
Identifying the Optimal Parameters to Express the Capacity–Activity Interrelationship of Community-Dwelling Older Adults Using Wearable Sensors



Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instrumentation
2.2.1. 6MWT
2.2.2. SPPB
2.2.3. Sway Test
2.2.4. TUG
2.2.5. Physical Activity Data
2.3. Testing Procedure
2.4. Data Analysis Procedure
2.4.1. Data Reduction
2.4.2. Cluster Analysis
2.4.3. Canonical Correlation Analysis
3. Results
3.1. Data Reduction
3.2. Clustering
3.2.1. Physical Activity
- Active duration: the total duration (minutes) of standing, shuffling, cycling, and walking combined;
- Movement intensity: the average movement intensity (m/s2) of active time;
- Lying-Standing: the number of transitions from lying to standing;
- Walking duration ≥ 20 s: the total (i.e., cumulative) duration (minutes) of walking periods greater than 20 s;
- Inactive periods: the number of sitting and lying periods combined.
3.2.2. Physical Capacity
- STS duration: time (in seconds) taken to complete one complete sit-to-stand cycle (sit-to-stand, stand, stand-to-sit, sit) at the participants’ fastest pace;
- Displacement: the mean (in mm) of the absolute AP and ML displacement during sway;
- 6MWT Distance: the total distance walking (m) during the 6MWT;
- STS power: the mean power (watts) of the sit to stand transition;
- StandToSitflex: the total flexion range (in degrees) of the trunk during the stand to sit transition.
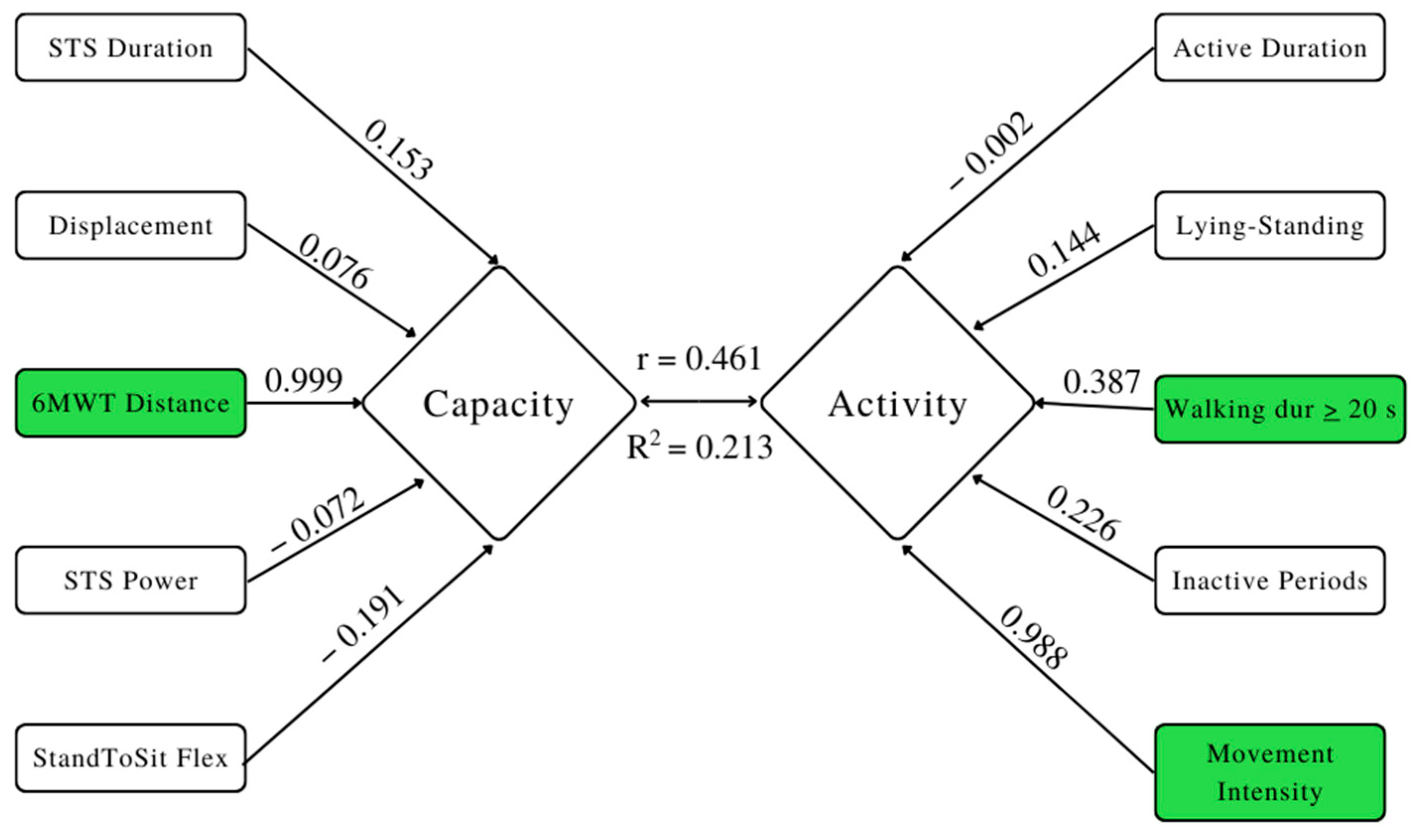
3.3. Canonical Correlation Analysis (CCA)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Canadian Medical Association. The State of Senior’s Health-Care in Canada. 2016. Available online: https://www.cma.ca/En/Lists/Medias/the-state-of-seniors-health-care-in-canada-september-2016.pdf (accessed on 1 August 2018).
- Statistics Canada. Canada’s Population Estimates: Age and Sex, July 1, 2018. 2019. Available online: https://www150.statcan.gc.ca/n1/daily-quotidien/190125/dq190125a-eng.pdf (accessed on 13 February 2019).
- La Grow, S.; Yeung, P.; Towers, A.; Alpass, F.; Stephens, C. The Impact of Mobility on Quality of Life among Older Persons. J. Aging Health 2013, 25, 723–736. [Google Scholar] [CrossRef] [PubMed]
- Webber, M.S.C.; Porter, M.M.; Menec, V.H. Mobility in Older Adults: A Comprehensive Framework. Gerontologist 2010, 50, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Helmrich, S.P.; Ragland, D.R.; Leung, R.W.; Paffenbarger, R.S. Physical Activity and Reduced Occurrence of Non-Insulin-Dependent Diabetes Mellitus. N. Engl. J. Med. 1991, 325, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E.; Jamnik, V.K.; Bredin, S.S.; McKenzie, D.C.; Stone, J.; Shephard, R.J.; Gledhill, N. Evidence-based risk assessment and recommendations for physical activity clearance: An introduction. Appl. Physiol. Nutr. Metab. 2011, 36, S1–S2. [Google Scholar] [CrossRef]
- Pahor, M.; Guralnik, J.M.; Ambrosius, W.T.; Blair, S.; Bonds, D.E.; Church, T.S.; Espeland, M.A.; Fielding, R.A.; Gill, T.; Groessl, E.J.; et al. Effect of Structured Physical Activity on Prevention of Major Mobility Disability in Older Adults. JAMA 2014, 311, 2387–2396. [Google Scholar] [CrossRef]
- Gill, T.M.; Guralnik, J.M.; Pahor, M.; Church, T.; Fielding, R.A.; King, A.C.; Marsh, A.P.; Newman, A.B.; Pellegrini, C.A.; Chen, S.H.; et al. Effect of structured physical activity on overall burden and transitions between states of major mobility disability in older persons: Secondary analysis of a randomized controlled trial. Ann. Intern. Med. 2017, 165, 833–840. [Google Scholar] [CrossRef]
- Iezonni, L. When Walking Fails: Mobility Problems of Adults with Chronic Conditions; University of California Press: Berkley, CA, USA, 2003. [Google Scholar]
- Walter-Ginzburg, A.; Guralnik, J.M.; Blumstein, T.; Gindin, J.; Baruch, M. Assistance with Personal Care Activities Among the Old-Old in Israel: A National Epidemiological Study. J. Am. Geriatr. Soc. 2001, 49, 1176–1184. [Google Scholar] [CrossRef]
- Nakano, M.M.; Otonari, T.S.; Takara, K.S.; Carmo, C.M.; Tanaka, C. Physical Performance, Balance, Mobility, and Muscle Strength Decline at Different Rates in Elderly People. J. Phys. Ther. Sci. 2014, 26, 583–586. [Google Scholar] [CrossRef]
- Distefano, G.; Standley, R.A.; Zhang, X.; Carnero, E.A.; Yi, F.; Cornnell, H.H.; Coen, P.M. Physical activity unveils the relationship between mitochondrial energetics, muscle quality, and physical function in older adults. J. Cachex Sarcopenia Muscle 2018, 9, 279–294. [Google Scholar] [CrossRef]
- Van Lummel, R.C.; Walgaard, S.; Pijnappels, M.; Elders, P.J.M.; Garcia-Aymerich, J.; Van Dieën, J.H.; Beek, P.J. Physical Performance and Physical Activity in Older Adults: Associated but Separate Domains of Physical Function in Old Age. PLoS ONE 2015, 10, e0144048. [Google Scholar] [CrossRef]
- Davis, J.C.; Bryan, S.; Best, J.R.; Li, L.C.; Hsu, C.L.; Gomez, C.; Vertes, K.A.; Liu-Ambrose, T. Mobility predicts change in older adults’ health-related quality of life: Evidence from a Vancouver falls prevention prospective cohort study. Health Qual. Life Outcomes 2015, 13, 101. [Google Scholar] [CrossRef] [PubMed]
- Santos, D.A.; Silva, A.M.; Baptista, F.; Santos, R.; Vale, S.; Mota, J.; Sardinha, L.B. Sedentary behaviour and physical activity are independently related to functional fitness in older adults. Exp. Gerontol. 2012, 47, 908–912. [Google Scholar] [CrossRef] [PubMed]
- Brach, J.S.; Simonsick, E.M.; Kritchevsky, S.; Yaffe, K.; Newman, A.B.; Health, Aging and Body Composition Study Research Group. The Association Between Physical Function and Lifestyle Activity and Exercise in the Health, Aging and Body Composition Study. J. Am. Geriatr. Soc. 2004, 52, 502–509. [Google Scholar] [CrossRef]
- Koolen, E.H.; van Hees, H.W.; van Lummel, R.C.; Dekhuijzen, R.; Djamin, R.S.; Spruit, M.A.; van’t Hul, A.J. “Can do” versus “do-do”: A novel concept to better understand physical functioning in patients with Chronic Obstructive Pulmonary Disease. J. Clin. Med. 2019, 8, 340. [Google Scholar] [CrossRef]
- Kasper, J.; Chan, K.; Freedman, V. Measuring physical capacity: An assessment of a composite measure using self-report and performance-based items. J. Aging Health 2017, 29, 289–309. [Google Scholar] [CrossRef]
- Stenholm, S.; Koster, A.; Valkeinen, H.; Patel, K.V.; Bandinelli, S.; Guralnik, J.M.; Ferrucci, L. Association of Physical Activity History With Physical Function and Mortality in Old Age. J. Gerontol. Ser. A 2015, 71, 496–501. [Google Scholar] [CrossRef] [PubMed]
- McRoberts: The Hague, The Netherlands. Available online: https://www.mcroberts.nl/products/ (accessed on 16 June 2019).
- Podsiadlo, D.; Richardson, S. The Timed “Up & Go”: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef] [PubMed]
- SAS Institute Inc. SAS Analytics Software, version 9.4m4; SAS Institute Inc.: Cary, NC, USA, 2016. [Google Scholar]
- IBM SPSS Statistics for Windows, version 25.0; IBM Corp.: Armonk, NY, USA, 2017.
- Berry, W.; Feldman, S. Multiple Regression in Practice (Quantitative Applications in the Social Sciences); SAGE Publications: Thousand Oaks, CA, USA, 1985. [Google Scholar]
- Vatcheva, K.; Lee, M.; McCormick, J.; Rahbar, M. Multicollinearity in regression analyses conducted in epidemiologic studies. Epidemiology 2016, 6, 227–242. [Google Scholar] [CrossRef]
- Bholowalia, P.; Kumar, A. EBK-Means: A clustering technique based on elbow method and k-means in WSN. Int. J. Comput. Appl. 2014, 105, 17–24. [Google Scholar]
- Harada, N.D.; Chiu, V.; Stewart, A.L. Mobility-related function in older adults: Assessment with a 6-minute walk test. Arch. Phys. Med. Rehabil. 1999, 80, 837–841. [Google Scholar] [CrossRef]
- Casanova, C.; Celli, B.R.; Barria, P.; Casas, A.; Cote, C.; de Torres, J.P.; Jardim, J.; Lopez, M.V.; Marin, J.M.; de Oca, M.M.; et al. The 6-min walk distance in healthy subjects: Reference standards from seven countries. Eur. Respir. J. 2010, 37, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Roman-Liu, D. Age-related changes in the range and velocity of postural sway. Arch. Gerontol. Geriatr. 2018, 77, 68–80. [Google Scholar] [CrossRef] [PubMed]
- Maki, B.E.; Holliday, P.J.; Topper, A.K. A Prospective Study of Postural Balance and Risk of Falling in An Ambulatory and Independent Elderly Population. J. Gerontol. 1994, 49, M72–M84. [Google Scholar] [CrossRef]
- Van Lummel, R.; Evers, J.; Niessen, M.; Beek, P.; van Dieen, J. Older adults with weaker muscle strength stand up from a sitting position with more dynamic trunk use. Sensors 2018, 18, 1235. [Google Scholar] [CrossRef] [PubMed]
- Lindemann, U.; Claus, H.; Stuber, M.; Augat, P.; Muche, R.; Nikolaus, T.; Becker, C. Measuring power during the sit-to-stand transfer. Eur. J. Appl. Physiol. 2003, 89, 466–470. [Google Scholar] [CrossRef]
- Swain, D.P.; Franklin, B.A. Comparison of Cardioprotective Benefits of Vigorous Versus Moderate Intensity Aerobic Exercise. Am. J. Cardiol. 2006, 97, 141–147. [Google Scholar] [CrossRef]
- Cornelissen, V.A.; Goetschalckx, K.; Verheyden, B.; Aubert, A.E.; Arnout, J.; Persu, A.; Rademakers, F.; Fagard, R.H. Effect of endurance training on blood pressure regulation, biomarkers and the heart in subjects at a higher age. Scand. J. Med. Sci. Sports 2010, 21, 526–534. [Google Scholar] [CrossRef]
- Serwe, K.M.; Swartz, A.M.; Hart, T.L.; Strath, S.J. Effectiveness of Long and Short Bout Walking on Increasing Physical Activity in Women. J. Womens Health 2011, 20, 247–253. [Google Scholar] [CrossRef]
- Woolf-May, K.; Kearney, E.; Owen, A.; Jones, D.; Davison, R.; Bird, S. The efficacy of accumulated short bouts versus single daily bouts of brisk waking in improving aerobic fitness and blood lipid profiles. Health Educ. Res. Theory Pract. 1999, 14, 803–815. [Google Scholar] [CrossRef]
- Diaz, K.; Howard, V.J.; Hutto, B.; Colabianchi, N.; Vena, J.E.; Safford, M.M.; Blair, S.N.; Hooker, S.P. Patterns of Sedentary Behavior and Mortality in U.S. Middle-Aged and Older Adults. Ann. Intern. Med. 2017, 167, 465–475. [Google Scholar] [CrossRef]
- Benatti, F.; Ried-Larsen, M. The effects of breaking up prolonged sitting time: A review of experimental studies. Med. Sci. Sports Exerc. 2015, 47, 2053–2061. [Google Scholar] [CrossRef] [PubMed]
- Sparling, P.B.; Howard, B.J.; Dunstan, D.; Owen, N. Recommendations for physical activity in older adults. BMJ 2015, 350, h100. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd ed.; U.S. Department of Health and Human Services: Washington, DC, USA, 2018.
- Mol, A.; Reijnierse, E.M.; Trappenburg, M.C.; van Wezel, R.J.A.; Maier, A.B.; Meskers, C.G.M. Rapid Systolic Blood Pressure Changes After Standing Up Associate With Impaired Physical Performance in Geriatric Outpatients. J. Am. Hear. Assoc. 2018, 7, e010060. [Google Scholar] [CrossRef] [PubMed]
- Edholm, P.; Nilsson, A.; Kadi, F. Physical function in older adults: Impacts of past and present physical activity behaviours. Scand. J. Med. Sci. Spor. 2019, 29, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Farhney, S.; Cheryl, K.; Dattilo, J.; Rusch, F. Effects of goal setting on activity level of senior exercisers with Osteoarthritis residing in the community. Therap. Recr. J. 2010, 44, 87–102. [Google Scholar]
- Bravata, D.M.; Smith-Spangler, C.; Sundaram, V.; Gienger, A.L.; Lin, N.; Lewis, R.; Stave, C.D.; Olkin, I.; Sirard, J.R. Using Pedometers to Increase Physical Activity and Improve Health: A systematic review. J. Am. Med. Assoc. 2007, 298, 2296–2304. [Google Scholar] [CrossRef]
- Sisson, S.B.; Camhi, S.M.; Church, T.S.; Tudor-Locke, C.; Johnson, W.; Katzmarzyk, P.T. Accelerometer-Determined Steps/Day and Metabolic Syndrome. Am. J. Prev. Med. 2010, 38, 575–582. [Google Scholar] [CrossRef]
- Pillay, J.; Kolbe-Alexander, T.; Proper, K.; Tomaz, S.; van Mechelen, W.; Lambert, E. Steps that count: Pedometer-measured physical activity, self-reported physical activity, and current physical guidelines—How do they relate? S. Afr. J. Sports Med. 2014, 26, 77–81. [Google Scholar] [CrossRef]


{kind=link}
| Age (Years) | Weight (kg) | Height (cm) | |
|---|---|---|---|
| Men (N = 21) | 73.29 ± 5.12 | 85.38 ± 21.89 | 172.38 ± 5.96 |
| Women (N = 55) | 74.35 ± 5.18 | 66.02 ± 10.16 | 159.87 ± 7.25 |
| Total (N = 76) | 74.05 ± 5.15 | 71.37 ± 16.58 | 163.33 ± 8.85 |
| 5 Clusters | R2 with: | |||
|---|---|---|---|---|
| Cluster | Variable | Own Cluster | Next Closest | 1-R2 Ratio |
| 1 | Active duration | 0.8430 | 0.3815 | 0.2538 |
| 2 | Movement intensity | 0.9792 | 0.0155 | 0.0211 |
| 3 | Lying-Standing | 0.6973 | 0.0546 | 0.3202 |
| 4 | Walking duration ≥ 20 s | 0.8775 | 0.2030 | 0.0607 |
| 5 | Inactive periods | 0.8837 | 0.0740 | 0.1255 |
| 5 Clusters | R-Squared with | |||
|---|---|---|---|---|
| Cluster | Variable | Own Cluster | Next Closest | 1-R2 Ratio |
| 1 | STS duration | 0.9354 | 0.0868 | 0.0707 |
| 2 | Displacement | 0.8770 | 0.0362 | 0.1276 |
| 3 | 6MWT distance | 0.7350 | 0.0463 | 0.2778 |
| 4 | STS power | 0.8140 | 0.0366 | 0.1931 |
| 5 | STS flex | 0.7452 | 0.1572 | 0.3024 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wright, E.; Chester, V.; Kuruganti, U. Identifying the Optimal Parameters to Express the Capacity–Activity Interrelationship of Community-Dwelling Older Adults Using Wearable Sensors. Sensors 2022, 22, 9648. https://doi.org/10.3390/s22249648
Wright E, Chester V, Kuruganti U. Identifying the Optimal Parameters to Express the Capacity–Activity Interrelationship of Community-Dwelling Older Adults Using Wearable Sensors. Sensors. 2022; 22(24):9648. https://doi.org/10.3390/s22249648
Chicago/Turabian StyleWright, Emily, Victoria Chester, and Usha Kuruganti. 2022. "Identifying the Optimal Parameters to Express the Capacity–Activity Interrelationship of Community-Dwelling Older Adults Using Wearable Sensors" Sensors 22, no. 24: 9648. https://doi.org/10.3390/s22249648
APA StyleWright, E., Chester, V., & Kuruganti, U. (2022). Identifying the Optimal Parameters to Express the Capacity–Activity Interrelationship of Community-Dwelling Older Adults Using Wearable Sensors. Sensors, 22(24), 9648. https://doi.org/10.3390/s22249648