
How Much Data Is Enough? A Reliable Methodology to Examine Long-Term Wearable Data Acquisition in Gait and Postural Sway

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
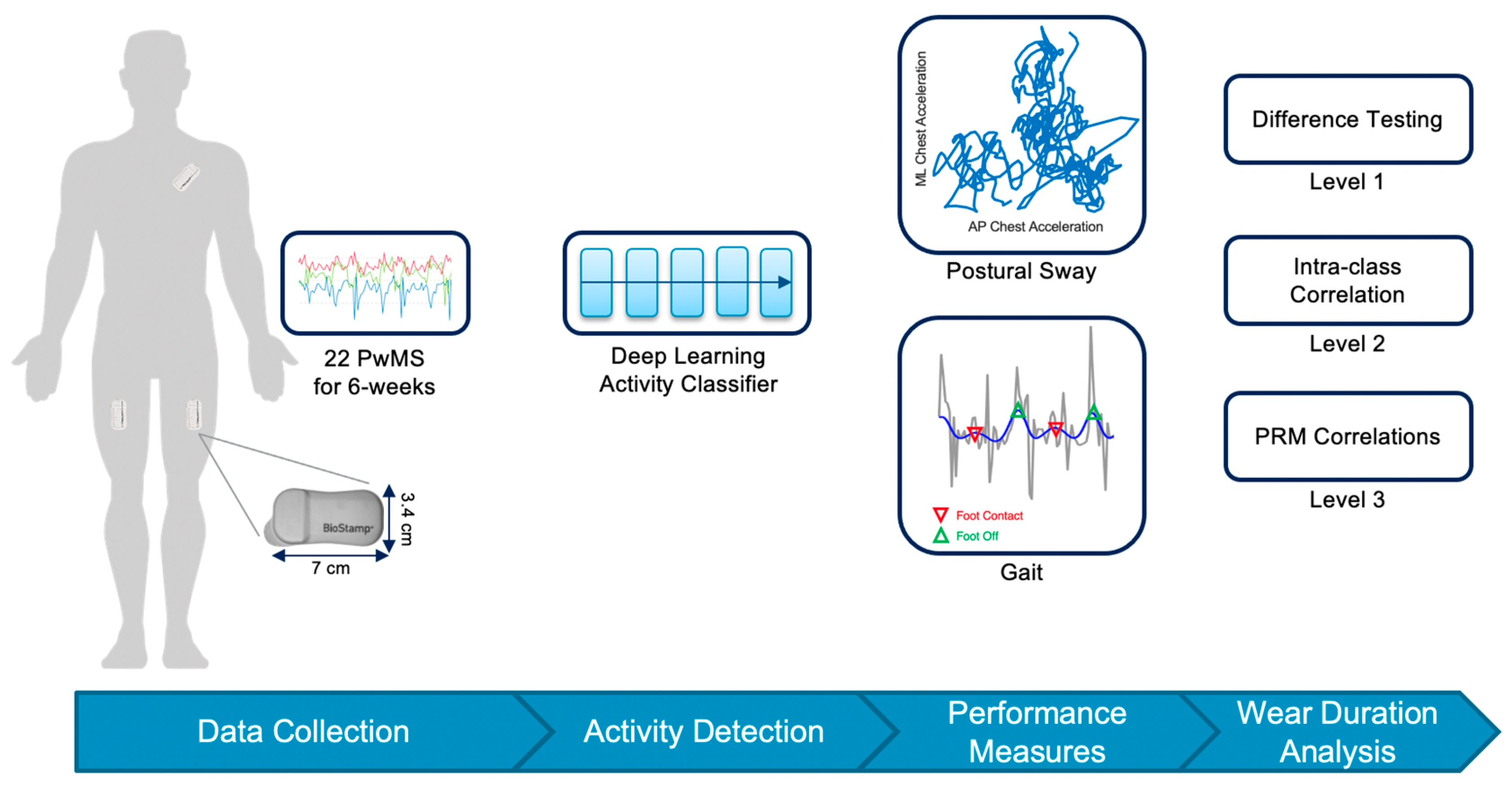
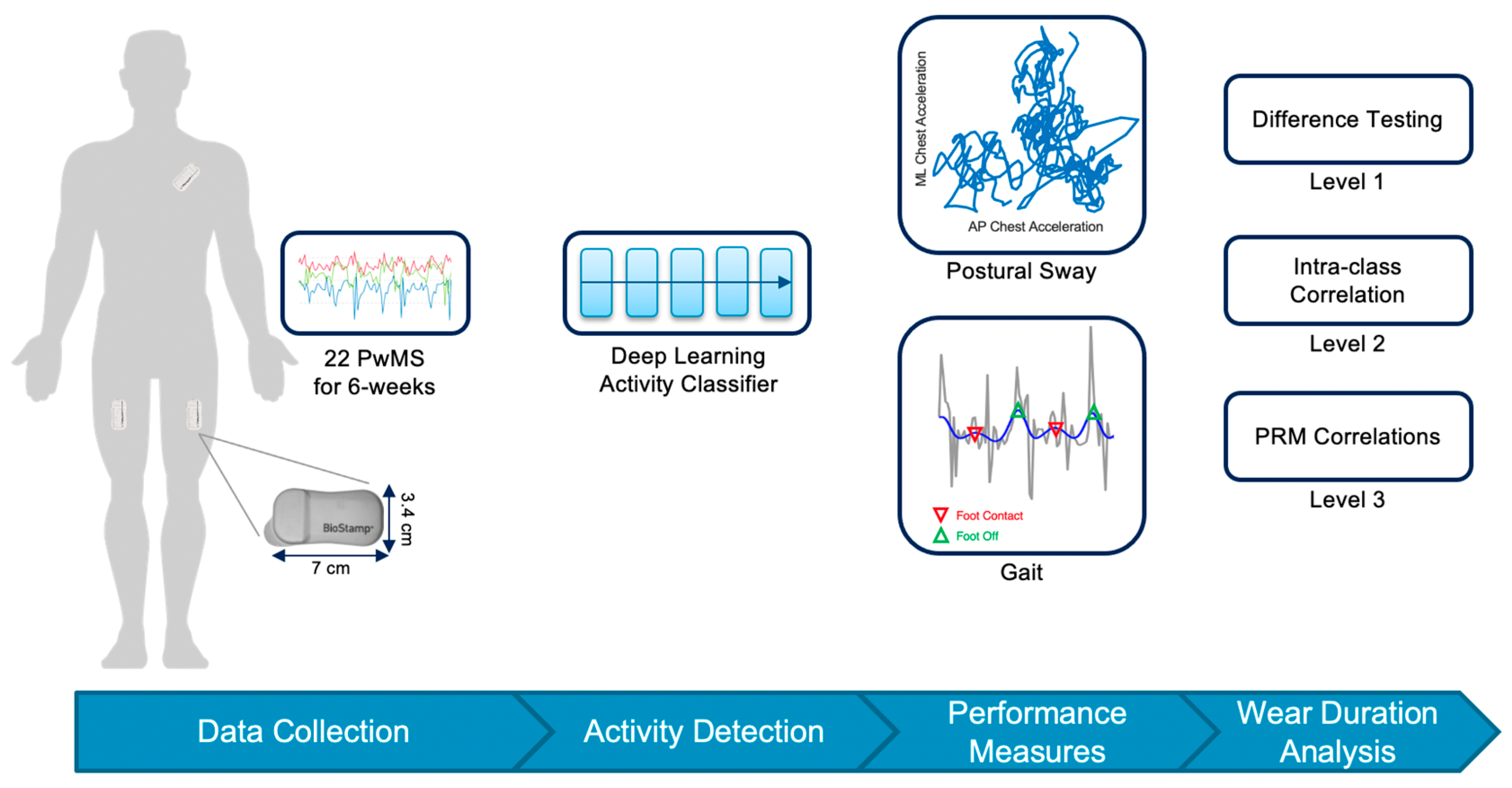
2.1. Participants and Protocol
2.2. Remote Analysis Pipeline
2.3. Wear-Time Analysis
3. Results
3.1. Difference Testing and Intra-Class Correlation for Gait Measures
3.2. Difference Testing and Intra-Class Correlation for Postural Sway Measures
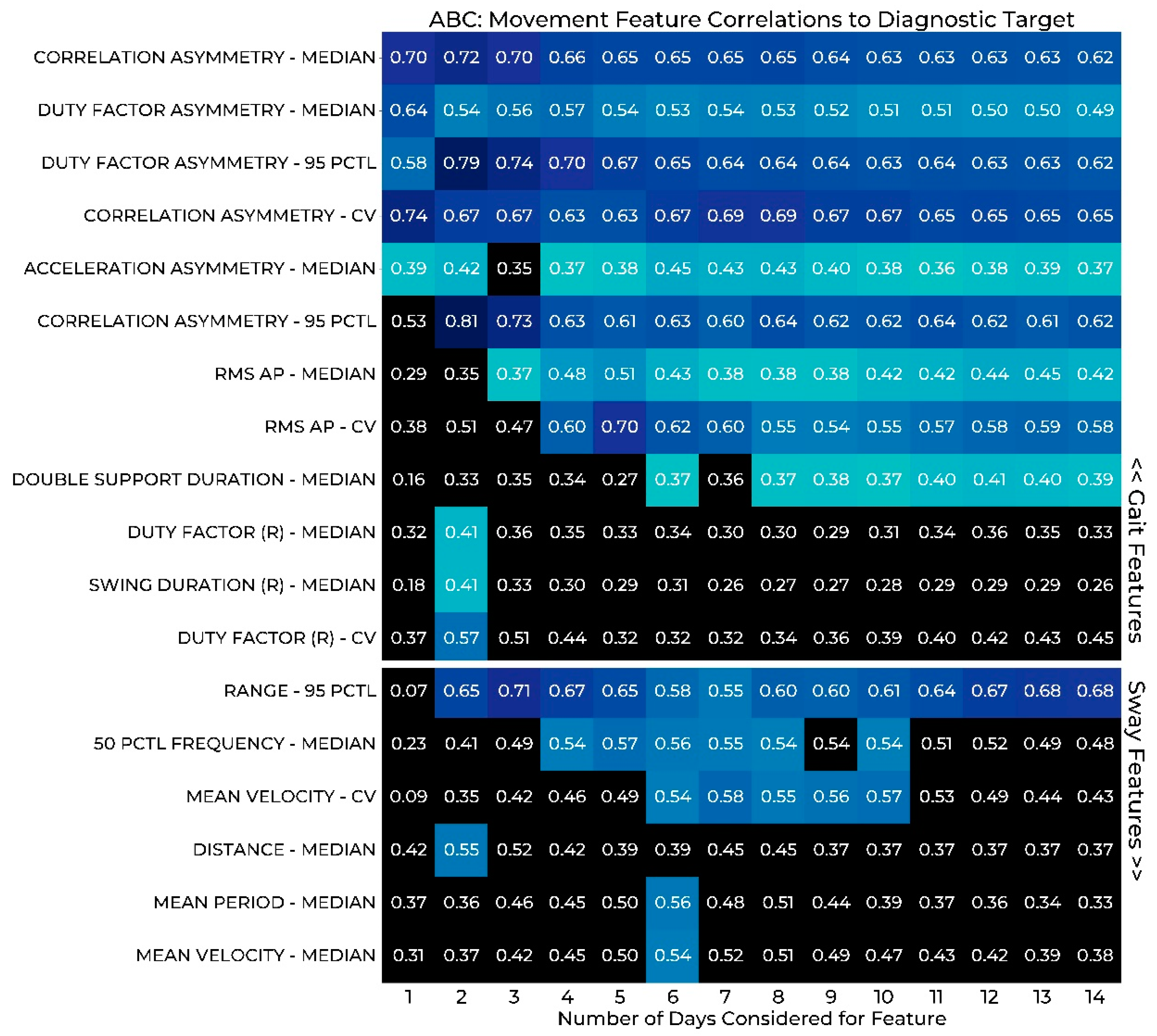
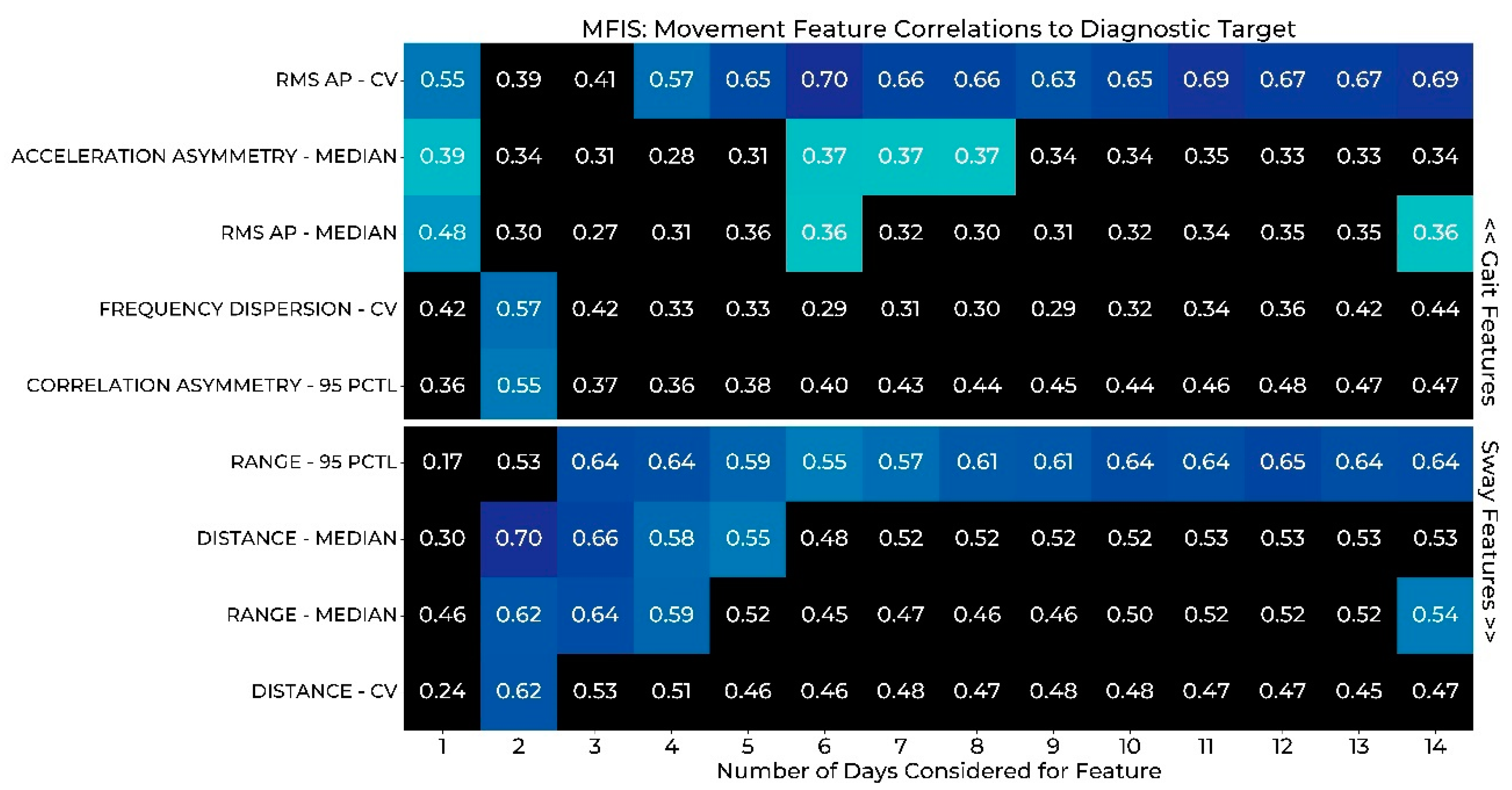
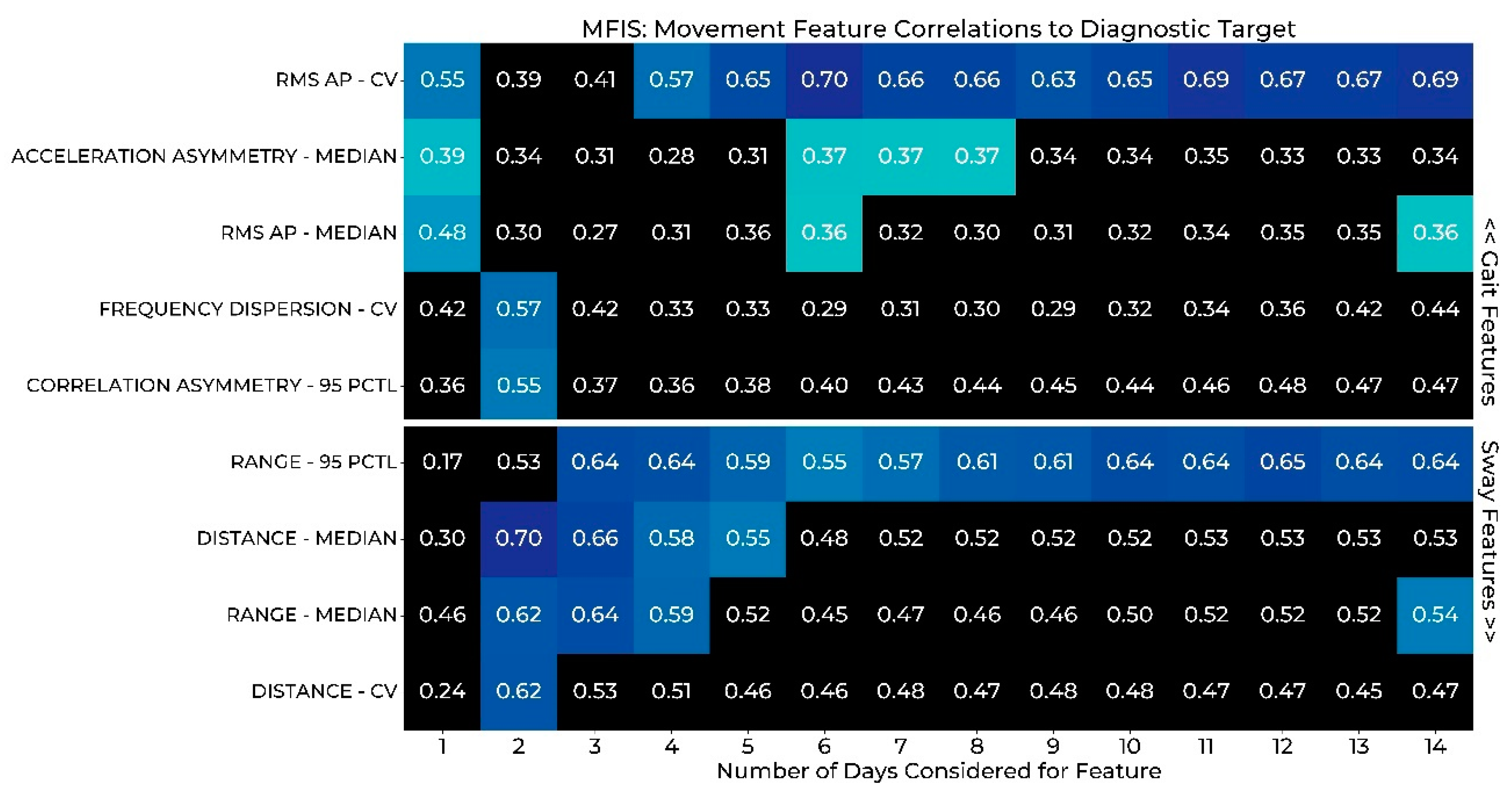
3.3. Correlation of Gait and Sway Features to PRMs
3.4. Analysis of Factors Impacting Wear Duration
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix A.1. Difference Testing Results

{kind=link}
{kind=link}
{kind=link}
| Gait Feature (14 Total) | 1D vs. 1W | 2D vs. 1W | 3D vs. 1W | WE vs. WD | 1W vs. 2W | 1W vs. 3W | 1W vs. 4W | 1W vs. 5W | 1W vs. 6W |
|---|---|---|---|---|---|---|---|---|---|
| Acceleration Asymmetry | |||||||||
| Correlation Asymmetry | |||||||||
| Double Support Duration | CV | ||||||||
| Duty Factor | |||||||||
| Duty Factor Asymmetry | |||||||||
| Entropy Ratio | |||||||||
| Entropy Ratio Asymmetry | |||||||||
| Frequency Dispersion ML | |||||||||
| Lyapunov Exponent AP | |||||||||
| Lyapunov Exponent ML | |||||||||
| RMS AP | |||||||||
| Stance Duration | |||||||||
| Stride Duration | |||||||||
| Swing Duration | CV | ||||||||
| Number of Significant Differences | 2-CV | 0-CV | 0-CV | 0-CV | 0-CV | 0-CV | 0-CV | 0-CV | 0-CV |
| 0-M | 0-M | 0-M | 0-M | 0-M | 0-M | 0-M | 0-M | 0-M | |
| 0–95th P | 0–95th P | 0–95th P | 0–95th P | 0–95th P | 0–95th P | 0–95th P | 0–95th P | 0–95th P |
| Sway Feature (13 Total) | 1D vs. 1W | 2D vs. 1W | 3D vs. 1W | WE vs. WD | 1W vs. 2W | 1W vs. 3W | 1W vs. 4W | 1W vs. 5W | 1W vs. 6W |
|---|---|---|---|---|---|---|---|---|---|
| Area | CV | ||||||||
| Centroidal Frequency | |||||||||
| Distance | |||||||||
| 50th Percentile Frequency | |||||||||
| 95th Percentile Frequency | |||||||||
| Frequency Dispersion | |||||||||
| Jerk | |||||||||
| Mean Period | CV | ||||||||
| Mean Velocity | |||||||||
| Path | |||||||||
| Power | CV | ||||||||
| Range | |||||||||
| RMS | |||||||||
| Number of Significant Differences | 3-CV | 0-CV | 0-CV | 0-CV | 0-CV | 0-CV | 0-CV | 0-CV | 0-CV |
| 0-M | 0-M | 0-M | 0-M | 0-M | 0-M | 0-M | 0-M | 0-M | |
| 0–95th P | 0–95th P | 0–95th P | 0–95th P | 0–95th P | 0–95th P | 0–95th P | 0–95th P | 0–95th P |
Appendix A.2. ICC Results
| Gait Feature (14 Total) | 1D vs. 1W | 2D vs. 1W | 3D vs. 1W | WE vs. WD | 1W vs. 2W | 1W vs. 3W | 1W vs. 4W | 1W vs. 5W | 1W vs. 6W |
|---|---|---|---|---|---|---|---|---|---|
| Acceleration Asymmetry | 0.92 | 0.95 | 0.98 | 0.96 | 0.99 | 0.97 | 0.96 | 0.95 | 0.98 |
| 0.89 | 0.97 | 0.98 | 0.94 | 0.98 | 0.97 | 0.94 | 0.93 | 0.98 | |
| 0.80 | 0.90 | 0.91 | 0.92 | 0.98 | 0.90 | 0.91 | 0.89 | 0.94 | |
| Correlation Asymmetry | 0.96 | 0.98 | 0.99 | 0.98 | 1.00 | 0.99 | 0.98 | 0.97 | 0.96 |
| 0.75 | 0.90 | 0.95 | 0.91 | 0.98 | 0.96 | 0.95 | 0.96 | 0.95 | |
| 0.94 | 0.96 | 0.98 | 0.95 | 0.98 | 0.98 | 0.96 | 0.93 | 0.96 | |
| Double Support Duration | 0.95 | 0.96 | 0.98 | 0.93 | 0.99 | 0.98 | 0.87 | 0.89 | 0.96 |
| 0.84 | 0.83 | 0.91 | 0.38 | 0.93 | 0.88 | 0.74 | 0.48 | 0.72 | |
| 0.62 | 0.84 | 0.98 | 0.60 | 0.96 | 0.92 | 0.87 | 0.78 | 0.79 | |
| Duty Factor | 0.96 | 0.98 | 0.99 | 0.98 | 0.98 | 0.97 | 0.91 | 0.95 | 0.93 |
| 0.70 | 0.94 | 0.97 | 0.96 | 0.99 | 0.96 | 0.95 | 0.86 | 0.89 | |
| 0.80 | 0.91 | 0.92 | 0.87 | 0.97 | 0.93 | 0.84 | 0.76 | 0.83 | |
| Duty Factor Asymmetry | 0.96 | 0.97 | 0.99 | 0.98 | 0.99 | 0.99 | 0.97 | 0.98 | 0.97 |
| 0.79 | 0.97 | 0.96 | 0.96 | 0.99 | 0.99 | 0.95 | 0.97 | 0.96 | |
| 0.89 | 0.94 | 0.97 | 0.96 | 0.97 | 0.97 | 0.95 | 0.94 | 0.96 | |
| Entropy Ratio | - | 0.84 | 0.85 | 0.71 | 0.98 | 0.95 | 0.62 | - | - |
| - | 0.91 | 0.96 | 0.91 | 0.98 | 0.97 | 0.81 | - | - | |
| - | 0.82 | 0.91 | 0.90 | 0.87 | 0.90 | 0.53 | - | - | |
| Entropy Ratio Asymmetry | - | 0.97 | 0.96 | 0.88 | 0.95 | 0.94 | 0.92 | - | - |
| - | 0.83 | 0.85 | 0.60 | 0.86 | 0.87 | 0.78 | - | - | |
| - | 0.45 | 0.72 | 0.32 | 0.91 | 0.85 | 0.39 | - | - | |
| Frequency Dispersion ML | 0.96 | 0.95 | 0.97 | 0.94 | 0.99 | 0.99 | 0.93 | 0.89 | 0.79 |
| 0.76 | 0.93 | 0.95 | 0.93 | 0.99 | 0.99 | 0.96 | 0.89 | 0.96 | |
| 0.87 | 0.94 | 0.98 | 0.87 | 0.98 | 0.98 | 0.91 | 0.84 | 0.94 | |
| Lyapunov Exponent AP | - | - | - | 0.57 | 0.99 | 0.97 | 0.83 | 0.66 | 0.89 |
| - | - | - | 0.71 | 0.97 | 0.97 | 0.73 | 0.44 | 0.93 | |
| - | - | - | 0.02 | 0.00 | 0.00 | 0.08 | 0.19 | 0.00 | |
| Lyapunov Exponent ML | - | - | - | 0.79 | 0.84 | 0.88 | 0.83 | 0.84 | 0.92 |
| - | - | - | 0.57 | 0.98 | 0.97 | 0.80 | 0.60 | 0.82 | |
| - | - | - | 0.15 | 0.57 | 0.07 | 0.53 | 0.00 | 0.00 | |
| RMS AP | 0.83 | 0.95 | 0.96 | 0.94 | 0.98 | 0.97 | 0.88 | 0.94 | 0.95 |
| 0.68 | 0.93 | 0.95 | 0.87 | 0.97 | 0.92 | 0.86 | 0.87 | 0.90 | |
| 0.83 | 0.88 | 0.94 | 0.86 | 0.95 | 0.95 | 0.64 | 0.83 | 0.91 | |
| Stance Duration | 0.89 | 0.95 | 0.98 | 0.89 | 0.99 | 0.98 | 0.93 | 0.94 | 0.98 |
| 0.53 | 0.96 | 0.96 | 0.90 | 0.99 | 0.98 | 0.94 | 0.88 | 0.92 | |
| 0.57 | 0.94 | 0.96 | 0.85 | 0.97 | 0.96 | 0.78 | 0.85 | 0.88 | |
| Stride Duration | 0.92 | 0.95 | 0.99 | 0.90 | 0.99 | 0.99 | 0.96 | 0.98 | 0.99 |
| 0.84 | 0.92 | 0.95 | 0.88 | 0.98 | 0.97 | 0.95 | 0.88 | 0.96 | |
| 0.45 | 0.90 | 0.96 | 0.81 | 0.97 | 0.95 | 0.84 | 0.90 | 0.94 | |
| Swing Duration | 0.97 | 0.98 | 0.99 | 0.96 | 0.99 | 0.98 | 0.93 | 0.96 | 0.97 |
| 0.82 | 0.91 | 0.92 | 0.92 | 0.96 | 0.93 | 0.82 | 0.80 | 0.87 | |
| 0.38 | 0.65 | 0.78 | 0.72 | 0.94 | 0.86 | 0.58 | 0.59 | 0.72 | |
| Number of Strong Correlations | 10 | 12 | 12 | 13 | 14 | 14 | 13 | 11 | 12 |
| 8 | 12 | 12 | 11 | 14 | 14 | 14 | 9 | 12 | |
| 6 | 10 | 12 | 10 | 12 | 12 | 8 | 9 | 10 |
| Sway Feature (13 Total) | 1D vs. 1W | 2D vs. 1W | 3D vs. 1W | WE vs. WD | 1W vs. 2W | 1W vs. 3W | 1W vs. 4W | 1W vs. 5W | 1W vs. 6W |
|---|---|---|---|---|---|---|---|---|---|
| Area | 0.49 | 0.86 | 0.94 | 0.93 | 0.96 | 0.94 | 0.84 | 0.87 | 0.93 |
| 0.40 | 0.38 | 0.95 | 0.91 | 0.98 | 0.95 | 0.92 | 0.81 | 0.96 | |
| 0.46 | 0.81 | 0.89 | 0.85 | 0.92 | 0.90 | 0.88 | 0.86 | 0.91 | |
| Centroidal Frequency | 0.84 | 0.96 | 0.99 | 0.95 | 1.00 | 0.99 | 0.97 | 0.98 | 0.99 |
| 0.73 | 0.90 | 0.97 | 0.88 | 0.99 | 0.99 | 0.96 | 0.97 | 0.98 | |
| 0.49 | 0.90 | 0.95 | 0.91 | 0.96 | 0.96 | 0.93 | 0.92 | 0.95 | |
| Distance | 0.75 | 0.94 | 0.97 | 0.94 | 0.97 | 0.97 | 0.83 | 0.89 | 0.94 |
| 0.46 | 0.86 | 0.95 | 0.76 | 0.96 | 0.92 | 0.89 | 0.88 | 0.92 | |
| 0.47 | 0.94 | 0.96 | 0.93 | 0.96 | 0.96 | 0.77 | 0.86 | 0.94 | |
| 50th Percentile Frequency | 0.80 | 0.96 | 0.99 | 0.96 | 0.98 | 0.97 | 0.94 | 0.95 | 0.96 |
| 0.74 | 0.94 | 0.98 | 0.94 | 0.98 | 0.98 | 0.94 | 0.96 | 0.97 | |
| 0.52 | 0.84 | 0.88 | 0.78 | 0.96 | 0.93 | 0.90 | 0.83 | 0.91 | |
| 95th Percentile Frequency | 0.74 | 0.97 | 0.99 | 0.97 | 0.98 | 0.96 | 0.95 | 0.94 | 0.96 |
| 0.64 | 0.94 | 0.98 | 0.94 | 0.98 | 0.98 | 0.95 | 0.97 | 0.98 | |
| 0.32 | 0.71 | 0.90 | 0.79 | 0.95 | 0.91 | 0.56 | 0.88 | 0.89 | |
| Frequency Dispersion | 0.64 | 0.95 | 0.96 | 0.95 | 0.98 | 0.98 | 0.91 | 0.93 | 0.97 |
| 0.66 | 0.91 | 0.96 | 0.89 | 0.97 | 0.95 | 0.93 | 0.92 | 0.94 | |
| 0.46 | 0.87 | 0.93 | 0.93 | 0.97 | 0.96 | 0.86 | 0.92 | 0.95 | |
| Jerk | 0.85 | 0.88 | 0.96 | 0.92 | 0.98 | 0.95 | 0.71 | 0.84 | 0.92 |
| 0.68 | 0.87 | 0.96 | 0.87 | 0.96 | 0.93 | 0.76 | 0.83 | 0.90 | |
| 0.27 | 0.79 | 0.87 | 0.90 | 0.93 | 0.91 | 0.87 | 0.83 | 0.90 | |
| Mean Period | 0.01 | 0.97 | 0.97 | 0.97 | 0.90 | 0.90 | 0.84 | 0.83 | 0.94 |
| 0.43 | 0.78 | 0.96 | 0.90 | 0.94 | 0.96 | 0.95 | 0.72 | 0.96 | |
| 0.56 | 0.67 | 0.87 | 0.49 | 0.84 | 0.83 | 0.40 | 0.41 | 0.75 | |
| Mean Velocity | 0.56 | 0.97 | 0.96 | 0.96 | 0.97 | 0.96 | 0.95 | 0.94 | 0.96 |
| 0.85 | 0.80 | 0.93 | 0.94 | 0.95 | 0.97 | 0.94 | 0.86 | 0.97 | |
| 0.72 | 0.94 | 0.97 | 0.90 | 0.92 | 0.90 | 0.76 | 0.93 | 0.88 | |
| Path | 0.51 | 0.97 | 0.96 | 0.98 | 0.97 | 0.96 | 0.95 | 0.93 | 0.96 |
| 0.84 | 0.79 | 0.94 | 0.94 | 0.95 | 0.97 | 0.94 | 0.86 | 0.97 | |
| 0.62 | 0.91 | 0.96 | 0.94 | 0.94 | 0.93 | 0.83 | 0.93 | 0.91 | |
| Power | 0.24 | 0.96 | 0.95 | 0.98 | 0.96 | 0.97 | 0.97 | 0.92 | 0.97 |
| 0.82 | 0.72 | 0.94 | 0.94 | 0.95 | 0.97 | 0.92 | 0.82 | 0.97 | |
| 0.77 | 0.91 | 0.96 | 0.93 | 0.94 | 0.92 | 0.76 | 0.92 | 0.88 | |
| Range | 0.65 | 0.91 | 0.94 | 0.94 | 0.97 | 0.97 | 0.82 | 0.88 | 0.96 |
| 0.48 | 0.94 | 0.97 | 0.95 | 0.98 | 0.96 | 0.88 | 0.91 | 0.94 | |
| 0.39 | 0.77 | 0.87 | 0.68 | 0.91 | 0.87 | 0.85 | 0.58 | 0.83 | |
| RMS | 0.49 | 0.97 | 0.96 | 0.97 | 0.97 | 0.97 | 0.95 | 0.93 | 0.97 |
| 0.83 | 0.79 | 0.95 | 0.94 | 0.95 | 0.97 | 0.93 | 0.86 | 0.98 | |
| 0.61 | 0.92 | 0.96 | 0.95 | 0.95 | 0.94 | 0.93 | 0.93 | 0.92 | |
| Number of Strong Correlations | 5 | 13 | 13 | 13 | 13 | 13 | 13 | 13 | 13 |
| 6 | 12 | 13 | 13 | 13 | 13 | 13 | 13 | 13 | |
| 1 | 12 | 13 | 11 | 13 | 13 | 11 | 11 | 13 |
References
- Gurchiek, R.D.; Choquette, R.H.; Beynnon, B.D.; Slauterbeck, J.R.; Tourville, T.W.; Toth, M.J.; McGinnis, R.S. Open-Source Remote Gait Analysis: A Post-Surgery Patient Monitoring Application. Sci. Rep. 2019, 9, 17966. [Google Scholar] [CrossRef] [PubMed]
- Meyer, B.M.; Tulipani, L.J.; Gurchiek, R.D.; Allen, D.A.; Adamowicz, L.; Larie, D.; Solomon, A.J.; Cheney, N.; McGinnis, R. Wearables and Deep Learning Classify Fall Risk from Gait in Multiple Sclerosis. IEEE J. Biomed. Health Inform. 2020, 25, 1824–1831. [Google Scholar] [CrossRef] [PubMed]
- Sun, R.; Moon, Y.; McGinnis, R.S.; Seagers, K.; Motl, R.W.; Sheth, N.; Wright, J.A.; Ghaffari, R.; Patel, S.; Sosnoff, J.J. Assessment of Postural Sway in Individuals with Multiple Sclerosis Using a Novel Wearable Inertial Sensor. Digit. Biomark. 2018, 2, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Tulipani, L.J.; Meyer, B.; Fox, S.; Solomon, A.J.; McGinnis, R.S. The Sit-to-Stand Transition as a Biomarker for Impairment: Comparison of Instrumented 30-Second Chair Stand Test and Daily Life Transitions in Multiple Sclerosis. IEEE Trans. Neural Syst. Rehabil. Eng. 2022, 30, 1213–1222. [Google Scholar] [CrossRef]
- McGinnis, R.S.; Mahadevan, N.; Moon, Y.; Seagers, K.; Sheth, N.; Jr, J.A.W.; DiCristofaro, S.; Silva, I.; Jortberg, E.; Ceruolo, M.; et al. A machine learning approach for gait speed estimation using skin-mounted wearable sensors: From healthy controls to individuals with multiple sclerosis. PLoS ONE 2017, 12, e0178366. [Google Scholar] [CrossRef]
- Gurchiek, R.D.; Rupasinghe Arachchige Don, H.S.; Pelawa Watagoda, L.C.R.; McGinnis, R.S.; van Werkhoven, H.; Needle, A.R.; McBride, J.M.; Arnholt, A.T. Sprint Assessment Using Machine Learning and a Wearable Accelerometer. J. Appl. Biomech. 2019, 35, 164–169. [Google Scholar] [CrossRef]
- Tulipani, L.J.; Meyer, B.; Allen, D.; Solomon, A.J.; McGinnis, R.S. Evaluation of unsupervised 30-second chair stand test performance assessed by wearable sensors to predict fall status in multiple sclerosis. Gait Posture 2022, 94, 19–25. [Google Scholar] [CrossRef]
- Tulipani, L.J.; Meyer, B.; Larie, D.; Solomon, A.J.; McGinnis, R.S. Metrics extracted from a single wearable sensor during sit-stand transitions relate to mobility impairment and fall risk in people with multiple sclerosis. Gait Posture 2020, 80, 361–366. [Google Scholar] [CrossRef]
- Frechette, M.L.; Meyer, B.M.; Tulipani, L.J.; Gurchiek, R.D.; McGinnis, R.S.; Sosnoff, J.J. Next Steps in Wearable Technology and Community Ambulation in Multiple Sclerosis. Curr. Neurol. Neurosci. Rep. 2019, 19, 80. [Google Scholar] [CrossRef]
- Bernhard, F.P.; Sartor, J.; Bettecken, K.; Hobert, M.A.; Arnold, C.; Weber, Y.G.; Poli, S.; Margraf, N.G.; Schlenstedt, C.; Hansen, C.; et al. Wearables for gait and balance assessment in the neurological ward—study design and first results of a prospective cross-sectional feasibility study with 384 inpatients. BMC Neurol. Lond. 2018, 18, 114. [Google Scholar] [CrossRef]
- McGinnis, R.S.; McGinnis, E.W.; Hruschak, J.; Lopez-Duran, N.L.; Fitzgerald, K.; Rosenblum, K.L.; Muzik, M. Rapid detection of internalizing diagnosis in young children enabled by wearable sensors and machine learning. PLoS ONE 2019, 14, e0210267. [Google Scholar] [CrossRef] [PubMed]
- Bellenger, C.R.; Miller, D.J.; Halson, S.L.; Roach, G.D.; Sargent, C. Wrist-Based Photoplethysmography Assessment of Heart Rate and Heart Rate Variability: Validation of WHOOP. Sensors 2021, 21, 3571. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, W.; Capodilupo, J.; Nicolae, A.; Aruh, R.; Liden, C.J.; Tom, B.T. Wearable Continuous Physiological Monitoring Device. U.S. Patent USD767768S1, 27 September 2016. [Google Scholar]
- Brumback, C.B.; Knight, D.W.; Park, J.; Axley, A.C.; Yuen, S.G.J. Biometric Monitoring Device with Contextually-or Environmentally-Dependent Display. U.S. Patent US8784271B2, 22 July 2014. [Google Scholar]
- Patel, M.; Pavic, A.; Goodwin, V.A. Wearable inertial sensors to measure gait and posture characteristic differences in older adult fallers and non-fallers: A scoping review. Gait Posture 2020, 76, 110–121. [Google Scholar] [CrossRef] [PubMed]
- Baker, N.; Gough, C.; Gordon, S.J. Inertial Sensor Reliability and Validity for Static and Dynamic Balance in Healthy Adults: A Systematic Review. Sensors 2021, 21, 5167. [Google Scholar] [CrossRef] [PubMed]
- Ghislieri, M.; Gastaldi, L.; Pastorelli, S.; Tadano, S.; Agostini, V. Wearable Inertial Sensors to Assess Standing Balance: A Systematic Review. Sensors 2019, 19, 4075. [Google Scholar] [CrossRef]
- Huisinga, J.M.; Mancini, M.; St. George, R.J.; Horak, F.B. Accelerometry Reveals Differences in Gait Variability Between Patients with Multiple Sclerosis and Healthy Controls. Ann. Biomed. Eng. 2013, 41, 1670–1679. [Google Scholar] [CrossRef]
- Sun, R.; Hsieh, K.L.; Sosnoff, J.J. Fall Risk Prediction in Multiple Sclerosis Using Postural Sway Measures: A Machine Learning Approach. Sci. Rep. 2019, 9, 16154. [Google Scholar] [CrossRef]
- Allali, G.; Laidet, M.; Herrmann, F.R.; Armand, S.; Elsworth-Edelsten, C.; Assal, F.; Lalive, P.H. Gait variability in multiple sclerosis: A better falls predictor than EDSS in patients with low disability. J. Neural Transm. 2016, 123, 447–450. [Google Scholar] [CrossRef]
- Storm, F.A.; Nair, K.P.S.; Clarke, A.J.; Van der Meulen, J.M.; Mazzà, C. Free-living and laboratory gait characteristics in patients with multiple sclerosis. PLoS ONE 2018, 13, e0196463. [Google Scholar] [CrossRef]
- Czech, M.D.; Psaltos, D.; Zhang, H.; Adamusiak, T.; Calicchio, M.; Kelekar, A.; Messere, A.; Van Dijk, K.R.A.; Ramos, V.; Demanuele, C.; et al. Age and environment-related differences in gait in healthy adults using wearables. Npj Digit. Med. 2020, 3, 127. [Google Scholar] [CrossRef]
- Cheng, Y.; Wang, K.; Xu, H.; Li, T.; Jin, Q.; Cui, D. Recent developments in sensors for wearable device applications. Anal. Bioanal. Chem. 2021, 413, 6037–6057. [Google Scholar] [CrossRef] [PubMed]
- Godkin, F.E.; Turner, E.; Demnati, Y.; Vert, A.; Roberts, A.; Swartz, R.H.; McLaughlin, P.M.; Weber, K.S.; Thai, V.; Beyer, K.B.; et al. Feasibility of a continuous, multi-sensor remote health monitoring approach in persons living with neurodegenerative disease. J. Neurol. 2021, 269, 2673–2686. [Google Scholar] [CrossRef] [PubMed]
- McGinnis, R.S.; McGinnis, E.W. Advancing Digital Medicine with Wearables in the Wild. Sensors 2022, 22, 4576. [Google Scholar] [CrossRef]
- Kasser, S.L.; Goldstein, A.; Wood, P.K.; Sibold, J. Symptom variability, affect and physical activity in ambulatory persons with multiple sclerosis: Understanding patterns and time-bound relationships. Disabil. Health J. 2017, 10, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Mueller, A.; Hoefling, H.A.; Muaremi, A.; Praestgaard, J.; Walsh, L.C.; Bunte, O.; Huber, R.M.; Fürmetz, J.; Keppler, A.M.; Schieker, M.; et al. Continuous Digital Monitoring of Walking Speed in Frail Elderly Patients: Noninterventional Validation Study and Longitudinal Clinical Trial. JMIR MHealth UHealth 2019, 7, e15191. [Google Scholar] [CrossRef]
- Adamowicz, L.; Karahanoglu, F.I.; Cicalo, C.; Zhang, H.; Demanuele, C.; Santamaria, M.; Cai, X.; Patel, S. Assessment of Sit-to-Stand Transfers during Daily Life Using an Accelerometer on the Lower Back. Sensors 2020, 20, 6618. [Google Scholar] [CrossRef]
- Hart, T.L.; Swartz, A.M.; Cashin, S.E.; Strath, S.J. How many days of monitoring predict physical activity and sedentary behaviour in older adults? Int. J. Behav. Nutr. Phys. Act. 2011, 8, 62. [Google Scholar] [CrossRef]
- Matthews, C.E.; Ainsworth, B.E.; Thompson, R.W.; Bassett, D.R. Sources of variance in daily physical activity levels as measured by an accelerometer. Med. Sci. Sports Exerc. 2002, 34, 1376–1381. [Google Scholar] [CrossRef]
- Gretebeck, R.J.; Montoye, H.J. Variability of some objective measures of physical activity. Med. Sci. Sports Exerc. 1992, 24, 1167–1172. [Google Scholar] [CrossRef]
- van Schooten, K.S.; Rispens, S.M.; Elders, P.J.; Lips, P.; van Dieën, J.H.; Pijnappels, M. Assessing physical activity in older adults: Required days of trunk accelerometer measurements for reliable estimation. J. Aging Phys. Act. 2015, 23, 9–17. [Google Scholar] [CrossRef]
- Kang, M.; Bjornson, K.; Barreira, T.V.; Ragan, B.G.; Song, K. The minimum number of days required to establish reliable physical activity estimates in children aged 2–15 years. Physiol. Meas. 2014, 35, 2229–2237. [Google Scholar] [CrossRef] [PubMed]
- Levin, S.; Jacobs, D.R.; Ainsworth, B.E.; Richardson, M.T.; Leon, A.S. Intra-individual variation and estimates of usual physical activity. Ann. Epidemiol. 1999, 9, 481–488. [Google Scholar] [CrossRef]
- Supratak, A.; Datta, G.; Gafson, A.R.; Nicholas, R.; Guo, Y.; Matthews, P.M. Remote Monitoring in the Home Validates Clinical Gait Measures for Multiple Sclerosis. Front. Neurol. 2018, 9, 561. [Google Scholar] [CrossRef] [PubMed]
- Powell, L.E.; Myers, A.M. The Activities-specific Balance Confidence (ABC) Scale. J. Gerontol. Ser. A 1995, 50A, M28–M34. [Google Scholar] [CrossRef] [PubMed]
- Modified Fatigue Impact Scale. Available online: https://www.sralab.org/rehabilitation-measures/modified-fatigue-impact-scale (accessed on 16 June 2020).
- Hobart, J.C.; Riazi, A.; Lamping, D.L.; Fitzpatrick, R.; Thompson, A.J. Measuring the impact of MS on walking ability: The 12-Item MS Walking Scale (MSWS-12). Neurology 2003, 60, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Jortberg, E.; Silva, I.; Bhatkar, V.; McGinnis, R.S.; Sen-Gupta, E.; Morey, B.; Wright, J.A.; Pindado, J.; Bianchi, M.T. A novel adhesive biosensor system for detecting respiration, cardiac, and limb movement signals during sleep: Validation with polysomnography. Nat. Sci. Sleep 2018, 10, 397–408. [Google Scholar] [CrossRef]
- Learmonth, Y.C.; Motl, R.W.; Sandroff, B.M.; Pula, J.H.; Cadavid, D. Validation of patient determined disease steps (PDDS) scale scores in persons with multiple sclerosis. BMC Neurol. 2013, 13, 37. [Google Scholar] [CrossRef]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444. [Google Scholar] [CrossRef]
- Chen, Y.; Zhong, K.; Zhang, J.; Sun, Q.; Zhao, X. LSTM Networks for Mobile Human Activity Recognition; Atlantis Press: Amsterdam, The Netherlands, 2016; pp. 50–53. [Google Scholar]
- Gurchiek, R.D.; Garabed, C.P.; McGinnis, R.S. Gait event detection using a thigh-worn accelerometer. Gait Posture 2020, 80, 214–216. [Google Scholar] [CrossRef]
- Craig, J.J.; Bruetsch, A.P.; Lynch, S.G.; Huisinga, J.M. The relationship between trunk and foot acceleration variability during walking shows minor changes in persons with multiple sclerosis. Clin. Biomech. 2017, 49, 16–21. [Google Scholar] [CrossRef]
- Mancini, M.; Salarian, A.; Carlson-Kuhta, P.; Zampieri, C.; King, L.; Chiari, L.; Horak, F.B. ISway: A sensitive, valid and reliable measure of postural control. J. NeuroEng. Rehabil. 2012, 9, 59. [Google Scholar] [CrossRef] [PubMed]
- Goldsack, J.C.; Coravos, A.; Bakker, J.P.; Bent, B.; Dowling, A.V.; Fitzer-Attas, C.; Godfrey, A.; Godino, J.G.; Gujar, N.; Izmailova, E.; et al. Verification, analytical validation, and clinical validation (V3): The foundation of determining fit-for-purpose for Biometric Monitoring Technologies (BioMeTs). NPJ Digit. Med. 2020, 3, 55. [Google Scholar] [CrossRef] [PubMed]
- Nilsagård, Y.; Carling, A.; Forsberg, A. Activities-Specific Balance Confidence in People with Multiple Sclerosis. Mult. Scler. Int. 2012, 2012, e613925. [Google Scholar] [CrossRef] [PubMed]
- Tajali, S.; Shaterzadeh-Yazdi, M.-J.; Negahban, H.; van Dieën, J.H.; Mehravar, M.; Majdinasab, N.; Saki-Malehi, A.; Mofateh, R. Predicting falls among patients with multiple sclerosis: Comparison of patient-reported outcomes and performance-based measures of lower extremity functions. Mult. Scler. Relat. Disord. 2017, 17, 69–74. [Google Scholar] [CrossRef]
- Téllez, N.; Río, J.; Tintoré, M.; Nos, C.; Galán, I.; Montalban, X. Does the Modified Fatigue Impact Scale offer a more comprehensive assessment of fatigue in MS? Mult. Scler. J. 2005, 11, 198–202. [Google Scholar] [CrossRef]
- Strober, L.B.; Bruce, J.M.; Arnett, P.A.; Alschuler, K.N.; DeLuca, J.; Chiaravalloti, N.; Lebkuecher, A.; Di Benedetto, M.; Cozart, J.; Thelen, J.; et al. Tired of not knowing what that fatigue score means? Normative data of the Modified Fatigue Impact Scale (MFIS). Mult. Scler. Relat. Disord. 2020, 46, 102576. [Google Scholar] [CrossRef] [PubMed]
- Kleinman, K.; Huang, S.S. Calculating Power by Bootstrap, with an Application to Cluster-Randomized Trials. eGEMs 2017, 4, 1202. [Google Scholar] [CrossRef] [Green Version]

| Comparison | Gait ICC | Gait Diff | Sway ICC | Sway Diff | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Median | 95th P | CV | Median | 95th P | CV | Median | 95th P | CV | Median | 95th P | CV | |
| 1 Day vs. 1 Week (n = 22) | 100 | 80 | 60 | 100 | 100 | 80 | 38 | 46 | 8 | 100 | 100 | 77 |
| 2 Days vs. 1 Week (n = 22) | 100 | 100 | 90 | 100 | 100 | 100 | 100 | 92 | 92 | 100 | 100 | 100 |
| 3 Days vs. 1 Week (n = 22) | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 |
| 2 Weeks vs. 1 Week (n = 22) | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 85 | 100 | 100 | 100 |
| 3 Weeks vs. 1 Week (n = 21) | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 |
| 4 Weeks vs. 1 Week (n = 21) | 100 | 90 | 80 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 |
| 5 Weeks vs. 1 Week (n = 21) | 100 | 90 | 90 | 100 | 100 | 100 | 100 | 100 | 85 | 100 | 100 | 100 |
| 6 Weeks vs. 1 Week (n = 19) | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 85 | 100 | 100 | 100 |
| Weekday vs. Weekend (n = 22) | 100 | 90 | 90 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 |
| Coefficient | Estimate | Standard Error | p-Value |
|---|---|---|---|
| Intercept | 4.41 | 0.53 | <0.01 |
| Log CV | 0.86 | 0.41 | 0.047 |
| Count | −0.011 | 0.0029 | <0.01 |
| Interaction (Log CV × Count) | −0.0040 | 0.0020 | 0.054 |
| R-Squared: 0.46; Adjusted R-Squared: 0.39 | |||
| Number of Observations: 27 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meyer, B.M.; Depetrillo, P.; Franco, J.; Donahue, N.; Fox, S.R.; O’Leary, A.; Loftness, B.C.; Gurchiek, R.D.; Buckley, M.; Solomon, A.J.; et al. How Much Data Is Enough? A Reliable Methodology to Examine Long-Term Wearable Data Acquisition in Gait and Postural Sway. Sensors 2022, 22, 6982. https://doi.org/10.3390/s22186982
Meyer BM, Depetrillo P, Franco J, Donahue N, Fox SR, O’Leary A, Loftness BC, Gurchiek RD, Buckley M, Solomon AJ, et al. How Much Data Is Enough? A Reliable Methodology to Examine Long-Term Wearable Data Acquisition in Gait and Postural Sway. Sensors. 2022; 22(18):6982. https://doi.org/10.3390/s22186982
Chicago/Turabian StyleMeyer, Brett M., Paolo Depetrillo, Jaime Franco, Nicole Donahue, Samantha R. Fox, Aisling O’Leary, Bryn C. Loftness, Reed D. Gurchiek, Maura Buckley, Andrew J. Solomon, and et al. 2022. "How Much Data Is Enough? A Reliable Methodology to Examine Long-Term Wearable Data Acquisition in Gait and Postural Sway" Sensors 22, no. 18: 6982. https://doi.org/10.3390/s22186982
APA StyleMeyer, B. M., Depetrillo, P., Franco, J., Donahue, N., Fox, S. R., O’Leary, A., Loftness, B. C., Gurchiek, R. D., Buckley, M., Solomon, A. J., Ng, S. K., Cheney, N., Ceruolo, M., & McGinnis, R. S. (2022). How Much Data Is Enough? A Reliable Methodology to Examine Long-Term Wearable Data Acquisition in Gait and Postural Sway. Sensors, 22(18), 6982. https://doi.org/10.3390/s22186982