
Validity of an iPhone App to Detect Prefrailty and Sarcopenia Syndromes in Community-Dwelling Older Adults: The Protocol for a Diagnostic Accuracy Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Protocol Registration
2.2. Eligibility Criteria
2.3. Participants Recruitment
2.4. General Data Collection
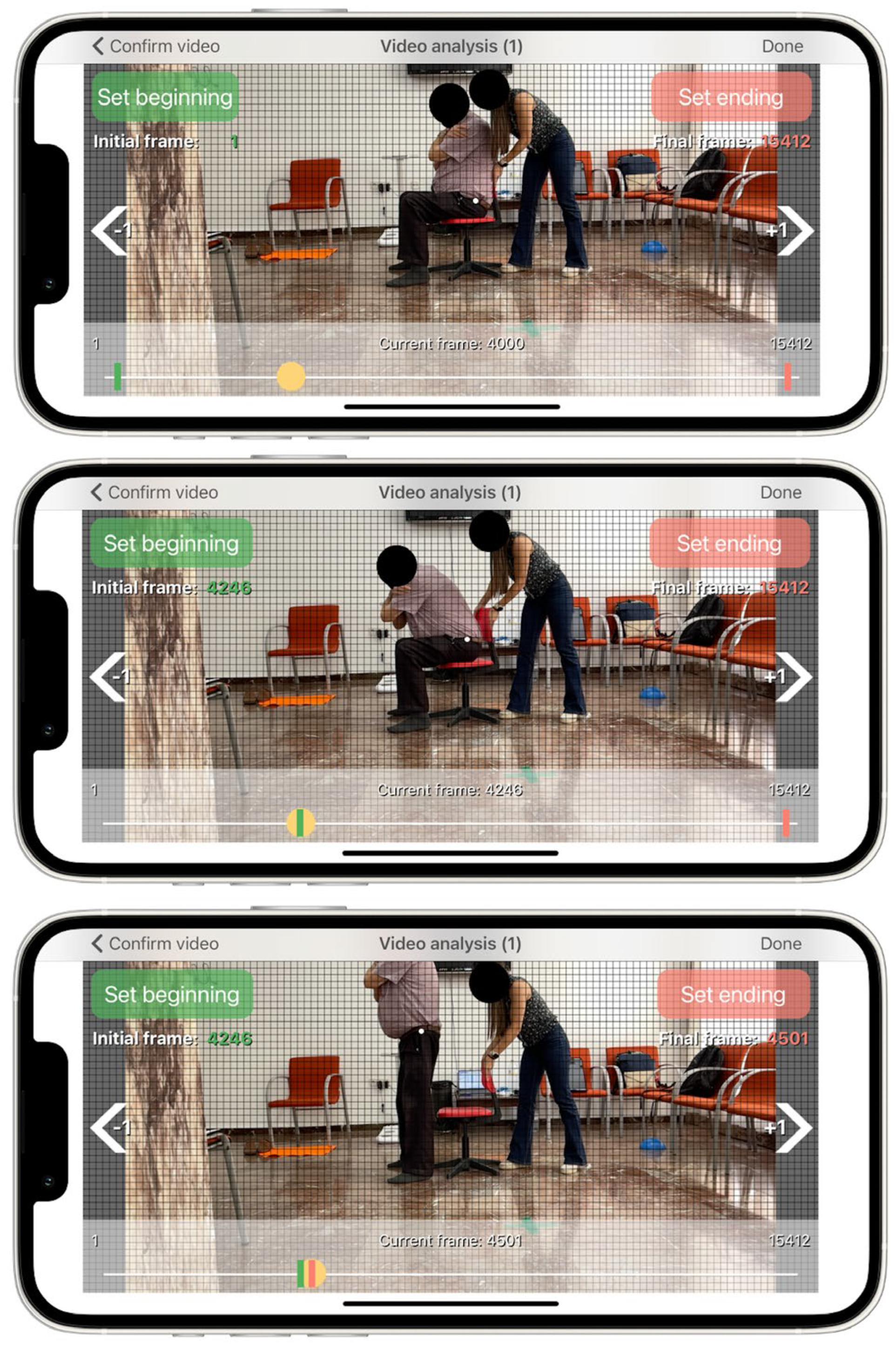
2.5. Index Test: Smartphone Mobile Application (App)
2.6. Reference Standard for Frailty Syndrome
2.7. Reference Standard for Sarcopenia
2.8. Sample Size Estimation
2.9. Statistical Analysis
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Domain | Question | List of Possible Answers |
|---|---|---|
| Health Status | Do you smoke? | Yes/No |
| Have you been diagnosed with one or more of these diseases? | Hypertension | |
| Diabetes Type I or II | ||
| Cardiovascular Disease | ||
| Chronic Obstructive Pulmonary Disease | ||
| Acute Myocardial Infarction | ||
| Cancer | ||
| Asthma | ||
| Bronchitis | ||
| Urinary Incontinence | ||
| Anemia | ||
| Thyroid Disease | ||
| Others | ||
| Do you take five or more pills a day? | Yes/No | |
| How is your health in general? | Very good | |
| Good | ||
| Fair | ||
| Bad | ||
| Very bad | ||
| Socioeconomic Status | Please, choose the option relative to your study level | None |
| Primary | ||
| Lower Secondary | ||
| Upper Secondary | ||
| Bachelor’s or equivalent | ||
| Master’s or equivalent | ||
| Doctorate’s or equivalent | ||
| Please, choose the option that better fits with your annual salary | 0–10,000 € | |
| 10,000–20,000 € | ||
| 20,000–30,000 € | ||
| 30,000–40,000 € | ||
| >40,000 € | ||
| Depression | Are you basically satisfied with your life? | Yes/No |
| Do you often get bored? | Yes/No | |
| Do you often feel helpless? | Yes/No | |
| Do you prefer staying at home instead of going out and doing new things? | Yes/No | |
| Is it hard for you to get started on new projects? | Yes/No | |
| Adverse Events | Have you experienced two or more falls during the last year? | Yes/No |
| Have you been hospitalized during the last year? | Yes/No |
References
- Ma, L. Current Situation of Frailty Screening Tools for Older Adults. J. Nutr. Health Aging 2019, 23, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European Consensus on Definition and Diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela, P.L.; Castillo-García, A.; Morales, J.S.; Izquierdo, M.; Serra-Rexach, J.A.; Santos-Lozano, A.; Lucia, A. Physical Exercise in the Oldest Old. Compr. Physiol. 2019, 9, 1281–1304. [Google Scholar] [CrossRef]
- Muscedere, J. Editorial: The Need to Implement Frailty in the International Classification of Disease (ICD). J. Frailty Aging 2020, 9, 2–3. [Google Scholar] [CrossRef] [PubMed]
- Petermann-Rocha, F.; Balntzi, V.; Gray, S.R.; Lara, J.; Ho, F.K.; Pell, J.P.; Celis-Morales, C. Global Prevalence of Sarcopenia and Severe Sarcopenia: A Systematic Review and Meta-Analysis. J. Cachexia Sarcopenia Muscle 2022, 13, 86–99. [Google Scholar] [CrossRef] [PubMed]
- Santos-Eggimann, B.; Cuénoud, P.; Spagnoli, J.; Junod, J. Prevalence of Frailty in Middle-Aged and Older Community-Dwelling Europeans Living in 10 Countries. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64, 675–681. [Google Scholar] [CrossRef]
- Thompson, M.Q.; Yu, S.; Tucker, G.R.; Adams, R.J.; Cesari, M.; Theou, O.; Visvanathan, R. Frailty and Sarcopenia in Combination Are More Predictive of Mortality than Either Condition Alone. Maturitas 2021, 144, 102–107. [Google Scholar] [CrossRef]
- Mori, H.; Tokuda, Y. Differences and Overlap between Sarcopenia and Physical Frailty in Older Community-Dwelling Japanese. Asia Pac. J. Clin. Nutr. 2019, 28, 157–165. [Google Scholar] [CrossRef]
- Davies, B.; García, F.; Ara, I.; Artalejo, F.R.; Rodriguez-Mañas, L.; Walter, S. Relationship Between Sarcopenia and Frailty in the Toledo Study of Healthy Aging: A Population Based Cross-Sectional Study. J. Am. Med. Dir. Assoc. 2018, 19, 282–286. [Google Scholar] [CrossRef]
- Davies, B.; Walter, S.; Rodríguez-Laso, A.; Carnicero Carreño, J.A.; García-García, F.J.; Álvarez-Bustos, A.; Rodríguez-Mañas, L. Differential Association of Frailty and Sarcopenia With Mortality and Disability: Insight Supporting Clinical Subtypes of Frailty. J. Am. Med. Dir. Assoc. 2022, in press. [Google Scholar] [CrossRef]
- Knudtson, M.D.; Klein, B.E.K.; Klein, R. Biomarkers of Aging and Falling: The Beaver Dam Eye Study. Arch. Gerontol. Geriatr. 2009, 49, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Millor, N.; Lecumberri, P.; Gomez, M.; Martinez, A.; Martinikorena, J.; Rodriguez-Manas, L.; Garcia-Garcia, F.J.; Izquierdo, M. Gait Velocity and Chair Sit-Stand-Sit Performance Improves Current Frailty-Status Identification. IEEE Trans. Neural Syst. Rehabil. Eng. Publ. IEEE Eng. Med. Biol. Soc. 2017, 25, 2018–2025. [Google Scholar] [CrossRef] [PubMed]
- Kera, T.; Kawai, H.; Takahashi, J.; Hirano, H.; Watanabe, Y.; Fujiwara, Y.; Ihara, K.; Kim, H.; Obuchi, S. Development of a Screening Formula for Sarcopenia Using Ground Reaction Force during Sit-to-Stand Motion. Gait Posture 2022, 93, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Cárdenas, J.D.; Rodríguez-Juan, J.J.; Smart, R.R.; Jakobi, J.M.; Jones, G.R. Validity and Reliability of an IPhone App to Assess Time, Velocity and Leg Power during a Sit-to-Stand Functional Performance Test. Gait Posture 2018, 59, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Orange, S.T.; Metcalfe, J.W.; Liefeith, A.; Jordan, A.R. Validity of Various Portable Devices to Measure Sit-to-Stand Velocity and Power in Older Adults. Gait Posture 2020, 76, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Ishii, S.; Tanaka, T.; Shibasaki, K.; Ouchi, Y.; Kikutani, T.; Higashiguchi, T.; Obuchi, S.P.; Ishikawa-Takata, K.; Hirano, H.; Kawai, H.; et al. Development of a Simple Screening Test for Sarcopenia in Older Adults. Geriatr. Gerontol. Int. 2014, 14 (Suppl. S1), 93–101. [Google Scholar] [CrossRef]
- Landi, F.; Onder, G.; Russo, A.; Liperoti, R.; Tosato, M.; Martone, A.M.; Capoluongo, E.; Bernabei, R. Calf Circumference, Frailty and Physical Performance among Older Adults Living in the Community. Clin. Nutr. Edinb. Scotl. 2014, 33, 539–544. [Google Scholar] [CrossRef]
- Bossuyt, P.M.; Reitsma, J.B.; Bruns, D.E.; Gatsonis, C.A.; Glasziou, P.P.; Irwig, L.; Lijmer, J.G.; Moher, D.; Rennie, D.; de Vet, H.C.W.; et al. STARD 2015: An Updated List of Essential Items for Reporting Diagnostic Accuracy Studies. BMJ 2015, 351, h5527. [Google Scholar] [CrossRef]
- Hu, F.-J.; Liu, H.; Liu, X.-L.; Jia, S.-L.; Hou, L.-S.; Xia, X.; Dong, B.-R. Mid-Upper Arm Circumference as an Alternative Screening Instrument to Appendicular Skeletal Muscle Mass Index for Diagnosing Sarcopenia. Clin. Interv. Aging 2021, 16, 1095–1104. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Ruiz-Comellas, A.; Pera, G.; Baena Díez, J.M.; Mundet Tudurí, X.; Alzamora Sas, T.; Elosua, R.; Torán Monserrat, P.; Heras, A.; Forés Raurell, R.; Fusté Gamisans, M.; et al. Validation of a Spanish Short Version of the Minnesota Leisure Time Physical Activity Questionnaire (VREM). Rev. Esp. Salud Publica 2012, 86, 495–508. [Google Scholar] [CrossRef]
- Sergi, G.; De Rui, M.; Veronese, N.; Bolzetta, F.; Berton, L.; Carraro, S.; Bano, G.; Coin, A.; Manzato, E.; Perissinotto, E. Assessing Appendicular Skeletal Muscle Mass with Bioelectrical Impedance Analysis in Free-Living Caucasian Older Adults. Clin. Nutr. Edinb. Scotl. 2015, 34, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A Short Physical Performance Battery Assessing Lower Extremity Function: Association with Self-Reported Disability and Prediction of Mortality and Nursing Home Admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef]
- Bujang, M.A.; Adnan, T.H. Requirements for Minimum Sample Size for Sensitivity and Specificity Analysis. J. Clin. Diagn. Res. JCDR 2016, 10, YE01–YE06. [Google Scholar] [CrossRef] [PubMed]
- Schenkman, M.; Riley, P.O.; Pieper, C. Sit to Stand from Progressively Lower Seat Heights -- Alterations in Angular Velocity. Clin. Biomech. Bristol Avon 1996, 11, 153–158. [Google Scholar] [CrossRef]
- Kuo, Y.-L. The Influence of Chair Seat Height on the Performance of Community-Dwelling Older Adults’ 30-Second Chair Stand Test. Aging Clin. Exp. Res. 2013, 25, 305–309. [Google Scholar] [CrossRef]
- Weiner, D.K.; Long, R.; Hughes, M.A.; Chandler, J.; Studenski, S. When Older Adults Face the Chair-Rise Challenge. A Study of Chair Height Availability and Height-Modified Chair-Rise Performance in the Elderly. J. Am. Geriatr. Soc. 1993, 41, 6–10. [Google Scholar] [CrossRef]
- Lindemann, U.; Claus, H.; Stuber, M.; Augat, P.; Muche, R.; Nikolaus, T.; Becker, C. Measuring Power during the Sit-to-Stand Transfer. Eur. J. Appl. Physiol. 2003, 89, 466–470. [Google Scholar] [CrossRef] [PubMed]
- Kralj, A.; Jaeger, R.J.; Munih, M. Analysis of Standing up and Sitting down in Humans: Definitions and Normative Data Presentation. J. Biomech. 1990, 23, 1123–1138. [Google Scholar] [CrossRef]
- Stevermer, C.A.; Gillette, J.C. Kinematic and Kinetic Indicators of Sit-to-Stand. J. Appl. Biomech. 2016, 32, 7–15. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montemurro, A.; Ruiz-Cárdenas, J.D.; Martínez-García, M.d.M.; Rodríguez-Juan, J.J. Validity of an iPhone App to Detect Prefrailty and Sarcopenia Syndromes in Community-Dwelling Older Adults: The Protocol for a Diagnostic Accuracy Study. Sensors 2022, 22, 6010. https://doi.org/10.3390/s22166010
Montemurro A, Ruiz-Cárdenas JD, Martínez-García MdM, Rodríguez-Juan JJ. Validity of an iPhone App to Detect Prefrailty and Sarcopenia Syndromes in Community-Dwelling Older Adults: The Protocol for a Diagnostic Accuracy Study. Sensors. 2022; 22(16):6010. https://doi.org/10.3390/s22166010
Chicago/Turabian StyleMontemurro, Alessio, Juan D. Ruiz-Cárdenas, María del Mar Martínez-García, and Juan J. Rodríguez-Juan. 2022. "Validity of an iPhone App to Detect Prefrailty and Sarcopenia Syndromes in Community-Dwelling Older Adults: The Protocol for a Diagnostic Accuracy Study" Sensors 22, no. 16: 6010. https://doi.org/10.3390/s22166010
APA StyleMontemurro, A., Ruiz-Cárdenas, J. D., Martínez-García, M. d. M., & Rodríguez-Juan, J. J. (2022). Validity of an iPhone App to Detect Prefrailty and Sarcopenia Syndromes in Community-Dwelling Older Adults: The Protocol for a Diagnostic Accuracy Study. Sensors, 22(16), 6010. https://doi.org/10.3390/s22166010