
Proposed Mobility Assessments with Simultaneous Full-Body Inertial Measurement Units and Optical Motion Capture in Healthy Adults and Neurological Patients for Future Validation Studies: Study Protocol

 ,
,  ,
,  add
Show full author list
add
Show full author list
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Participants
2.3. Clinical and Demographic Data
2.4. Disease Specific Scales
2.5. Equipment
2.6. Protocol
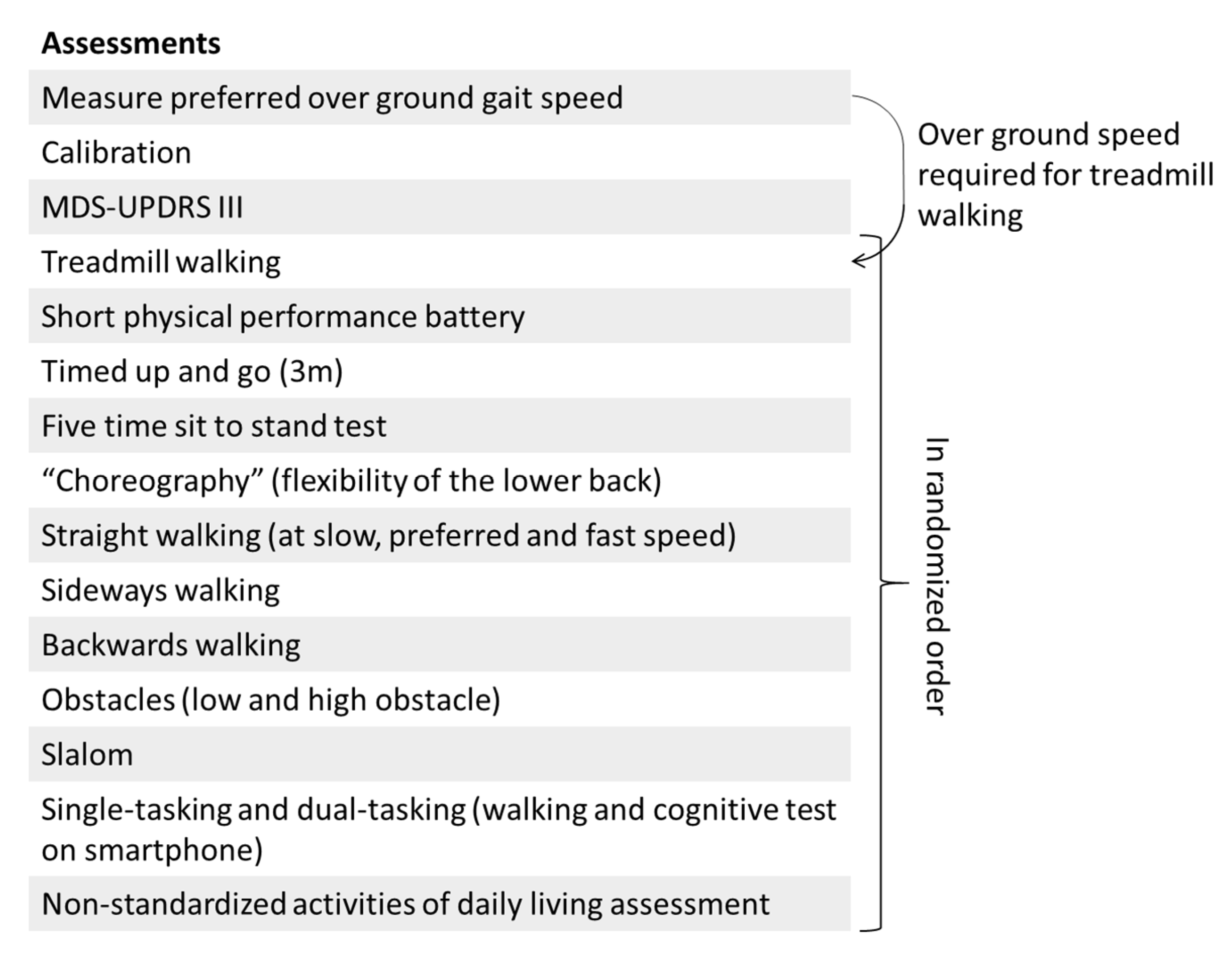
2.6.1. Standardized Mobility Assessments
- Treadmill walking. All participants will wear a safety harness that is suspended from the ceiling while walking at the treadmill. At the start of the treadmill trial, the speed of the treadmill will be gradually increased to a speed that is comfortable for the participant. The participant will walk for 60 s at this speed. Thereafter, the speed of the treadmill will be gradually adapted to the preferred over ground walking speed which is measured at the start of the protocol. The participant will walk again 60 s at this speed. A subset of the healthy young adults will participate in a split-belt protocol which is described in the Supplementary Material
- Short physical performance battery (SPPB)
- ○
- Side-by-side stand (“Please stand with your feet together for 10 s, try not to move your feet”)
- ○
- Semi-tandem stand (“Please stand with the heel of one foot touching the big toe of the other foot for 10 s, you can put either foot in front, try not to move your feet”)
- ○
- Tandem stand (“Please stand with the heel of one foot in front while touching the toes of your other foot, you can put either foot in front, try not to move your feet”)
- ○
- m gait (“Please stand with the toes of both feet on the starting line and walk over to the end of the walkway at your normal gait speed”)
- ○
- m gait (“Please stand again with the toes of both feet on the starting line and walk over to the end of the walkway at your normal gait speed”)
- ○
- Repeated chair Stand (“Please stand up straight five times in a row as fast as possible without using your arms”)
- Timed up and go (“Please stand up from the chair, walk at preferred speed towards the cone, turn around it in the direction of your preference, walk back and sit down”)
- Five time sit to stand test (“Please stand up straight five times in a row at your preferred speed without using your arms if possible”)
- “Choreography”: a series of movements related to the flexibility of the lower back (see Supplementary Material). The choreography contains flexion, extension and rotational movements of the back, as well as a combination of those movements (“Please perform the movements that are shown one by one on the pictures”)
- Straight walking
- ○
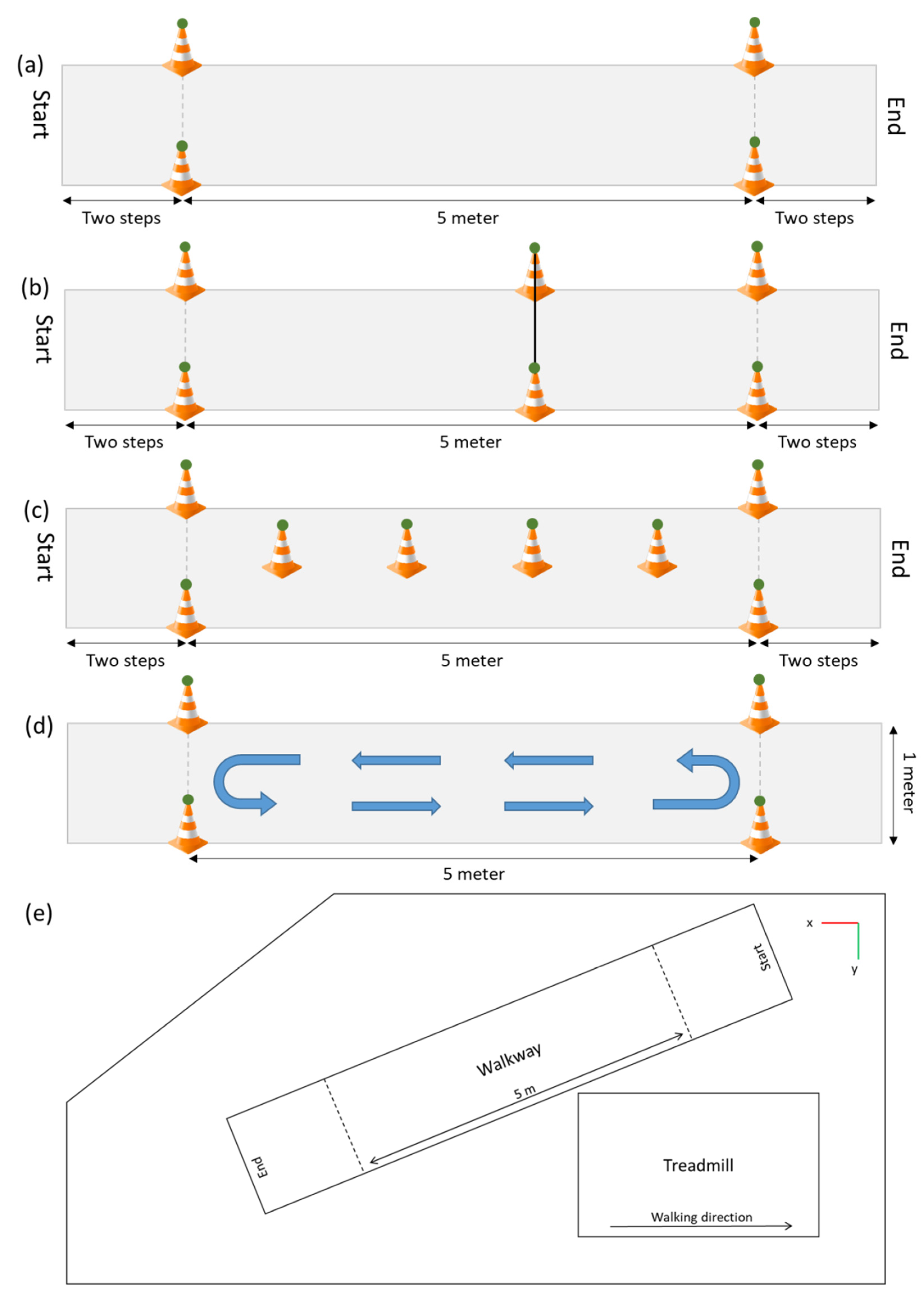
- Slow speed (“Please walk half of your normal walking speed”; Figure 3a)
- ○
- Preferred speed (“Please walk at your normal walking speed”)
- ○
- Fast speed (“Please walk as fast as possible, without running or falling”)
- Sideways walking (“Please walk sideways, do not cross your legs during this walk”)
- Backwards walking (“Please walk backwards at a speed that is comfortable for you”)
- Obstacles: an obstacle with a height of 10 cm, and one with a height of 20 cm will be placed at the three meter point with reflective markers on the top of each side (Figure 3b), and a forward walk will be performed once for each obstacle (“Please walk at your normal walking speed and step over the obstacle”)
- Slalom: cones will be placed every meter in the middle of the walkway. Each cone will have a reflective marker on top (“Please walk at your normal speed around the cones, do not step over them”; Figure 3d)Single and dual-tasking: It is know that the complexity of the dual-task influences the dual-task costs [31,32], therefore two tasks with different complexity will be performed. The first task will be a simple reaction time test where participants will have to tap on the screen as fast as possible after a black square appears on the screen. There are six time intervals ranging from 1000 to 2000 ms (increased in steps of 200 ms), which determines the time it will take for the black square to appear on the screen. Each time interval occurs four times and the order of the 24 options is randomized. The reaction time will be recorded. A more complex reaction time test that is more often used to measure the dual-task performance is the Stroop test [33,34,35]. The Stroop test also measures the cognitive inhibition [35,36]. In this study a numerical Stroop test will be performed. During this test two numbers will appear on the screen and the participants have to tap on the number that is highest in value.
- Within this test there are three conditions; (1) Neutral, the font size of both numbers is equal; (2) Congruent, the number highest in value has a larger font size; (3) Incongruent, the number highest in value has a smaller font size (Figure 4). In total 24 responses will be required, eight of each condition. The order in which the 24 options occur in the test is randomized. The reaction time as well as the accuracy will be recorded.
- ○
- Simple reaction time task on a smartphone while standing (“Please tap on the screen as fast as possible after a black square appears on the screen”)
- ○
- Numerical Stroop task on a smartphone while standing (“On the screen will appear each time two numbers, please tap on the largest number in value, not the largest number in size”)
- ○
- Walking up and down the 5 m walkway for 30 s, turning direction was not instructed (“Please walk up and down the walkway at your normal speed and stay within the area marked by the cones”; Figure 3d)
- ○
- Walking up and down the 5 m walkway and performing the simple reaction time test on the smartphone (“Please perform the simple reaction time test again as instructed before and walk up and down the walkway at your normal speed at the same moment”)
- ○
- Walking up and down the 5 m walkway and performing the Numerical Stroop test on the smartphone (“Please perform the numerical Stroop test again as instructed before and walk up and down the walkway at your normal speed at the same moment”)
2.6.2. Non-Standardized Activities of Daily Living Assessment
- Setting a table (plates, cutlery, glasses)
- Eating and drinking (including opening a bottle and pouring a drink)
- Cleaning a table
- Lifting/replacing objects from different heights
- Ironing and folding a T-shirt
- Tooth brushing
- Multiple chair rises
- Sitting and reading out loud
- Sitting and talking
- Opening a cabinet and taking objects out of it
2.7. Database and Data Availability
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abdo, W.F.; van de Warrenburg, B.P.C.; Burn, D.J.; Quinn, N.P.; Bloem, B.R. The clinical approach to movement disorders. Nat. Rev. Neurol. 2010, 6, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Rehman, R.Z.U.; Del Din, S.; Guan, Y.; Yarnall, A.J.; Shi, J.Q.; Rochester, L. Selecting clinically relevant gait characteristics for classification of early parkinson’s disease: A comprehensive machine learning approach. Sci. Rep. 2019, 9, 17269. [Google Scholar] [CrossRef] [Green Version]
- Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel, R.; et al. Movement disorder society-sponsored revision of the unified parkinson’s disease rating scale (MDS-UPDRS): Scale presentation and clinimetric testing results. Mov. Disord. 2008, 23, 2129–2170. [Google Scholar] [CrossRef] [PubMed]
- Curtze, C.; Nutt, J.G.; Carlson-Kuhta, P.; Mancini, M.; Horak, F.B. Levodopa is a double-edged sword for balance and gait in people with parkinson’s disease. Mov. Disord. 2015, 30, 1361–1370. [Google Scholar] [CrossRef]
- Ramsperger, R.; Meckler, S.; Heger, T.; van Uem, J.; Hucker, S.; Braatz, U.; Graessner, H.; Berg, D.; Manoli, Y.; Serrano, J.A.; et al. Continuous leg dyskinesia assessment in Parkinson’s disease-clinical validity and ecological effect. Park. Relat. Disord. 2016, 26, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Warmerdam, E.; Hausdorff, J.M.; Atrsaei, A.; Zhou, Y.; Mirelman, A.; Aminian, K.; Espay, A.J.; Hansen, C.; Evers, L.J.W.; Keller, A.; et al. Long-term unsupervised mobility assessment in movement disorders. Lancet Neurol. 2020, 19, 462–470. [Google Scholar] [CrossRef]
- Maetzler, W.; Rochester, L.; Bhidayasiri, R.; Espay, A.J.; Sánchez-Ferro, A.; van Uem, J.M.T. Modernizing daily function assessment in parkinson’s disease using capacity, perception, and performance measures. Mov. Disord. 2021, 36, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Ameen, M.S.; Cheung, L.M.; Hauser, T.; Hahn, M.A.; Schabus, M. About the accuracy and problems of consumer devices in the assessment of sleep. Sens. Switz. 2019, 19, 4160. [Google Scholar] [CrossRef] [Green Version]
- Imboden, M.T.; Nelson, M.B.; Kaminsky, L.A.; Montoye, A.H. Comparison of four Fitbit and Jawbone activity monitors with a research-grade Actigraph accelerometer for estimating physical activity and energy expenditure. Br. J. Sports Med. 2018, 52, 844–850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maetzler, W.; Klucken, J.; Horne, M. A clinical view on the development of technology-based tools in managing Parkinson’s disease. Mov. Disord. 2016, 31, 1263–1271. [Google Scholar] [CrossRef]
- Ghislieri, M.; Gastaldi, L.; Pastorelli, S.; Tadano, S.; Agostini, V. Wearable inertial sensors to assess standing balance: A systematic review. Sens. Switz. 2019, 19, 4075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibb, W.R.G.; Lees, A.J. The relevance of the Lewy body to the pathogenesis of idiopathic Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 1988, 51, 745–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Otto, J.C.; Gierthmühlen, J.; Kirchhofer, V.; Borzikowsky, C.; Baron, R. Validation of the questionnaire for symptom assessment in pain disorders for back pain patients (Q-SAP). Eur. J. Pain UK 2021, 25, 513–528. [Google Scholar] [CrossRef] [PubMed]
- Deyo, R.A.; Cherkin, D.C.; Ciol, M.A. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J. Clin. Epidemiol. 1992, 45, 613–619. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The montreal cognitive assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.S.; Kohlmann, T.; Janssen, M.F.; Buchholz, I. Psychometric properties of the EQ-5D-5L: A systematic review of the literature. Qual. Life Res. 2021, 30, 647–673. [Google Scholar] [CrossRef] [PubMed]
- Graf, C. Instrumental activities of daily living scale. Am. J. Nurs. 2008, 108, 52–62. [Google Scholar] [CrossRef] [Green Version]
- Haase, I.; Schwarz, A.; Burger, A.; Kladny, B. Der funktionsfragebogen hannover (FFbH) und die subskala “körperliche funktionsfähigkeit” aus dem SF-36 im vergleich. Rehabilitation 2001, 40, 40–42. [Google Scholar] [CrossRef]
- Malmstrom, T.K.; Miller, D.K.; Simonsick, E.M.; Ferrucci, L.; Morley, J.E. SARC-F: A symptom score to predict persons with sarcopenia at risk for poor functional outcomes. J. Cachexia Sarcopenia Muscle 2016, 7, 28–36. [Google Scholar] [CrossRef]
- Williamson, A.; Hoggart, B. Pain: A review of three commonly used pain rating scales. J. Clin. Nurs. 2005, 14, 798–804. [Google Scholar] [CrossRef] [PubMed]
- Pestronk, A.; Florence, J.; Levine, T.; Al-Lozi, M.T.; Lopate, G.; Miller, T.; Ramneantu, I.; Waheed, W.; Stambuk, M. Sensory exam with a quantitative tuning fork: Rapid, sensitive and predictive of SNAP amplitude. Neurology 2004, 62, 461–464. [Google Scholar] [CrossRef] [PubMed]
- Herlofson, K.; Larsen, J.P. Measuring fatigue in patients with Parkinson’s disease—The fatigue severity scale. Eur. J. Neurol. 2002, 9, 595–600. [Google Scholar] [CrossRef]
- Luszczynska, A.; Scholz, U.; Schwarzer, R. The general self-efficacy scale: Multicultural validation studies. J. Psychol. 2005, 139, 439–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism: Onset, progression, and mortality. Neurology 1967, 17, 427–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [Green Version]
- Brott, T.; Adams, H.P., Jr.; Olinger, C.P.; Marler, J.R.; Barsan, W.G.; Biller, J.; Spilker, J.; Holleran, R.; Eberle, R.; Hertzberg, V.; et al. Measurements of acute cerebral infarction. Stroke 1989, 20, 864–871. [Google Scholar] [CrossRef] [Green Version]
- Wu, G.; Siegler, S.; Allard, P.; Kirtley, C.; Leardini, A.; Rosenbaum, D.; Whittle, M.; D’Lima, D.D.; Cristofolini, L.; Witte, H.; et al. ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion—Part I: Ankle, hip, and spine. J. Biomech. 2002, 35, 543–548. [Google Scholar] [CrossRef]
- Wu, G.; Van Der Helm, F.C.T.; Veeger, H.E.J.; Makhsous, M.; Van Roy, P.; Anglin, C.; Nagels, J.; Karduna, A.R.; McQuade, K.; Wang, X.; et al. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion—Part II: Shoulder, elbow, wrist and hand. J. Biomech. 2005, 38, 981–992. [Google Scholar] [CrossRef]
- Robert-Lachaine, X.; Mecheri, H.; Larue, C.; Plamondon, A. Accuracy and repeatability of single-pose calibration of inertial measurement units for whole-body motion analysis. Gait Posture 2017, 54, 80–86. [Google Scholar] [CrossRef]
- Patel, P.; Lamar, M.; Bhatt, T. Effect of type of cognitive task and walking speed on cognitive-motor interference during dual-task walking. Neuroscience 2014, 260, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Hagner-Derengowska, M.; Kałuzny, K.; Hagner, W.; Kałuzna, A.; Kochański, B.; Borkowska, A.; Budzyński, J. The effect of two different cognitive tests on gait parameters during dual tasks in healthy postmenopausal women. BioMed Res. Int. 2016, 2016, 1205469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wollesen, B.; Voelcker-Rehage, C.; Regenbrecht, T.; Mattes, K. Influence of a visual-verbal Stroop test on standing and walking performance of older adults. Neuroscience 2016, 318, 166–177. [Google Scholar] [CrossRef]
- Strouwen, C.; Molenaar, E.A.L.M.; Münks, L.; Broeder, S.; Ginis, P.; Bloem, B.R.; Nieuwboer, A.; Heremans, E. Determinants of dual-task training effect size in parkinson disease: Who will benefit most? J. Neurol. Phys. Ther. 2019, 43, 3–11. [Google Scholar] [CrossRef]
- Perrochon, A.; Kemoun, G.; Watelain, E.; Dugué, B.; Berthoz, A. The “stroop walking task”: An innovative dual-task for the early detection of executive function impairment. Neurophysiol. Clin. 2015, 45, 181–190. [Google Scholar] [CrossRef]
- Stroop, J.R. Studies of interference in serial verbal reactions. J. Exp. Psychol. 1935, 18, 643–662. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)-A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faber, G.S.; Chang, C.C.; Kingma, I.; Dennerlein, J.T.; van Dieën, J.H. Estimating 3D L5/S1 moments and ground reaction forces during trunk bending using a full-body ambulatory inertial motion capture system. J. Biomech. 2016, 49, 904–912. [Google Scholar] [CrossRef] [Green Version]
- Mavor, M.P.; Ross, G.B.; Clouthier, A.L.; Karakolis, T.; Graham, R.B. Validation of an IMU suit for military-based tasks. Sens. Switz. 2020, 20, 4280. [Google Scholar] [CrossRef]
- Robert-Lachaine, X.; Mecheri, H.; Larue, C.; Plamondon, A. Validation of inertial measurement units with an optoelectronic system for whole-body motion analysis. Med. Biol. Eng. Comput. 2017, 55, 609–619. [Google Scholar] [CrossRef]
- Bourke, A.K.; Ihlen, E.A.F.; Bergquist, R.; Wik, P.B.; Vereijken, B.; Helbostad, J.L. A physical activity reference data-set recorded from older adults using body-worn inertial sensors and video technology—The ADAPT study data-set. Sensors 2017, 17, 559. [Google Scholar] [CrossRef] [Green Version]
- Delrobaei, M.; Baktash, N.; Gilmore, G.; McIsaac, K.; Jog, M. Using wearable technology to generate objective parkinson’s disease dyskinesia severity score: Possibilities for home monitoring. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 1853–1863. [Google Scholar] [CrossRef] [PubMed]
- Delrobaei, M.; Memar, S.; Pieterman, M.; Stratton, T.W.; McIsaac, K.; Jog, M. Towards remote monitoring of Parkinson’s disease tremor using wearable motion capture systems. J. Neurol. Sci. 2018, 384, 38–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robert-Lachaine, X.; Parent, G.; Fuentes, A.; Hagemeister, N.; Aissaoui, R. Inertial motion capture validation of 3D knee kinematics at various gait speed on the treadmill with a double-pose calibration. Gait Posture 2020, 77, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, U.; Balasukumaran, T.; Hoffman, J.; Springer, S. Agreement of gait events detection during treadmill backward walking by kinematic data and inertial motion units. Sensors 2020, 20, 6331. [Google Scholar] [CrossRef]
- Buckley, A.C.; Galna, B.; Rochester, L.; Mazz, C. Upper body accelerations as a biomarker of gait impairment in the early stages of Parkinson’s disease. Gait Posture 2019, 71, 289–295. [Google Scholar] [CrossRef]
- Turcato, A.M.; Godi, M.; Giardini, M.; Arcolin, I.; Nardone, A.; Giordano, A.; Schieppati, M. Abnormal gait pattern emerges during curved trajectories in high-functioning Parkinsonian patients walking in line at normal speed. PLoS ONE 2018, 13, e0197264. [Google Scholar] [CrossRef]
- Lamoth, C.J.; Van Deudekom, F.J.; Van Campen, J.P.; Appels, B.A.; De Vries, O.J.; Pijnappels, M. Gait stability and variability measures show effects of impaired cognition and dual tasking in frail people. J. Neuroeng. Rehabil. 2011, 8, 2. [Google Scholar] [CrossRef] [Green Version]
- Smith, E.; Cusack, T.; Cunningham, C.; Blake, C. The influence of a cognitive dual task on the gait parameters of healthy older adults: A systematic review and meta-analysis. J. Aging Phys. Act. 2017, 25, 671–686. [Google Scholar] [CrossRef]
- Fasano, A.; Schlenstedt, C.; Herzog, J.; Plotnik, M.; Rose, F.E.M.; Volkmann, J.; Deuschl, G. Split-belt locomotion in Parkinson’s disease links asymmetry, dyscoordination and sequence effect. Gait Posture 2016, 48, 6–12. [Google Scholar] [CrossRef]
- Pavasini, R.; Guralnik, J.; Brown, J.C.; di Bari, M.; Cesari, M.; Landi, F.; Vaes, B.; Legrand, D.; Verghese, J.; Wang, C.; et al. Short physical performance battery and all-cause mortality: Systematic review and meta-analysis. BMC Med. 2016, 14, 215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christopher, A.; Kraft, E.; Olenick, H.; Kiesling, R.; Doty, A. The reliability and validity of the timed up and go as a clinical tool in individuals with and without disabilities across a lifespan: A systematic review: Psychometric properties of the timed up and go. Disabil. Rehabil. 2019, 43, 1799–1813. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W.; Bubela, D.J.; Magasi, S.R.; Wang, Y.C.; Gershon, R.C. Sit-to-stand test: Performance and determinants across the age-span. Isokinet. Exerc. Sci. 2010, 18, 235–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atrsaei, A.; Dadashi, F.; Hansen, C.; Warmerdam, E.; Mariani, B.; Maetzler, W. Postural transitions detection and characterization in healthy and patient populations using a single waist sensor. J. Neuroeng. Rehabil. 2020, 17, 70. [Google Scholar] [CrossRef]
- Morris, R.; Stuart, S.; McBarron, G.; Fino, P.; Mancini, M.; Curtze, C. Validity of MobilityLab (version 2) for gait assessment in young adults, older adults and Parkinson’s disease. Physiol. Meas. 2019, 40, 095003. [Google Scholar] [CrossRef] [PubMed]
- Vienne-Jumeau, A.; Quijoux, F.; Vidal, P.P.; Ricard, D. Wearable inertial sensors provide reliable biomarkers of disease severity in multiple sclerosis: A systematic review and meta-analysis. Ann. Phys. Rehabil. Med. 2020, 63, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Uemura, K.; Yamada, M.; Nagai, K.; Ichihashi, N. Older adults at high risk of falling need more time for anticipatory postural adjustment in the precrossing phase of obstacle negotiation. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2011, 66, 904–909. [Google Scholar] [CrossRef] [PubMed]
- Pieruccini-Faria, F.; Montero-Odasso, M.; Newman, A. Obstacle negotiation, gait variability, and risk of falling: Results from the “gait and brain study”. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2019, 74, 1422–1428. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, B.A.; Faria, C.D.C.M.; Santos, M.P.; Swarowsky, A. Assessing timed up and go in Parkinson’s disease: Reliability and validity of timed up and go assessment of biomechanical strategies. J. Rehabil. Med. 2017, 49, 723–731. [Google Scholar] [CrossRef] [Green Version]
- Gaßner, H.; Marxreiter, F.; Steib, S.; Kohl, Z.; Schlachetzki, J.C.M.; Adler, W.; Eskofier, B.M.; Pfeifer, K.; Winkler, J.; Klucken, J. Gait and cognition in parkinson’s disease: Cognitive impairment is inadequately reflected by gait performance during dual task. Front. Neurol. 2017, 8, 550. [Google Scholar] [CrossRef] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Warmerdam, E.; Romijnders, R.; Geritz, J.; Elshehabi, M.; Maetzler, C.; Otto, J.C.; Reimer, M.; Stuerner, K.; Baron, R.; Paschen, S.; et al. Proposed Mobility Assessments with Simultaneous Full-Body Inertial Measurement Units and Optical Motion Capture in Healthy Adults and Neurological Patients for Future Validation Studies: Study Protocol. Sensors 2021, 21, 5833. https://doi.org/10.3390/s21175833
Warmerdam E, Romijnders R, Geritz J, Elshehabi M, Maetzler C, Otto JC, Reimer M, Stuerner K, Baron R, Paschen S, et al. Proposed Mobility Assessments with Simultaneous Full-Body Inertial Measurement Units and Optical Motion Capture in Healthy Adults and Neurological Patients for Future Validation Studies: Study Protocol. Sensors. 2021; 21(17):5833. https://doi.org/10.3390/s21175833
Chicago/Turabian StyleWarmerdam, Elke, Robbin Romijnders, Johanna Geritz, Morad Elshehabi, Corina Maetzler, Jan Carl Otto, Maren Reimer, Klarissa Stuerner, Ralf Baron, Steffen Paschen, and et al. 2021. "Proposed Mobility Assessments with Simultaneous Full-Body Inertial Measurement Units and Optical Motion Capture in Healthy Adults and Neurological Patients for Future Validation Studies: Study Protocol" Sensors 21, no. 17: 5833. https://doi.org/10.3390/s21175833
APA StyleWarmerdam, E., Romijnders, R., Geritz, J., Elshehabi, M., Maetzler, C., Otto, J. C., Reimer, M., Stuerner, K., Baron, R., Paschen, S., Beyer, T., Dopcke, D., Eiken, T., Ortmann, H., Peters, F., Recke, F. v. d., Riesen, M., Rohwedder, G., Schaade, A., ... Hansen, C. (2021). Proposed Mobility Assessments with Simultaneous Full-Body Inertial Measurement Units and Optical Motion Capture in Healthy Adults and Neurological Patients for Future Validation Studies: Study Protocol. Sensors, 21(17), 5833. https://doi.org/10.3390/s21175833