
State-of-the-Art Sensors for Remote Care of People with Dementia during a Pandemic: A Systematic Review






Abstract
:1. Introduction
2. Materials and Methods
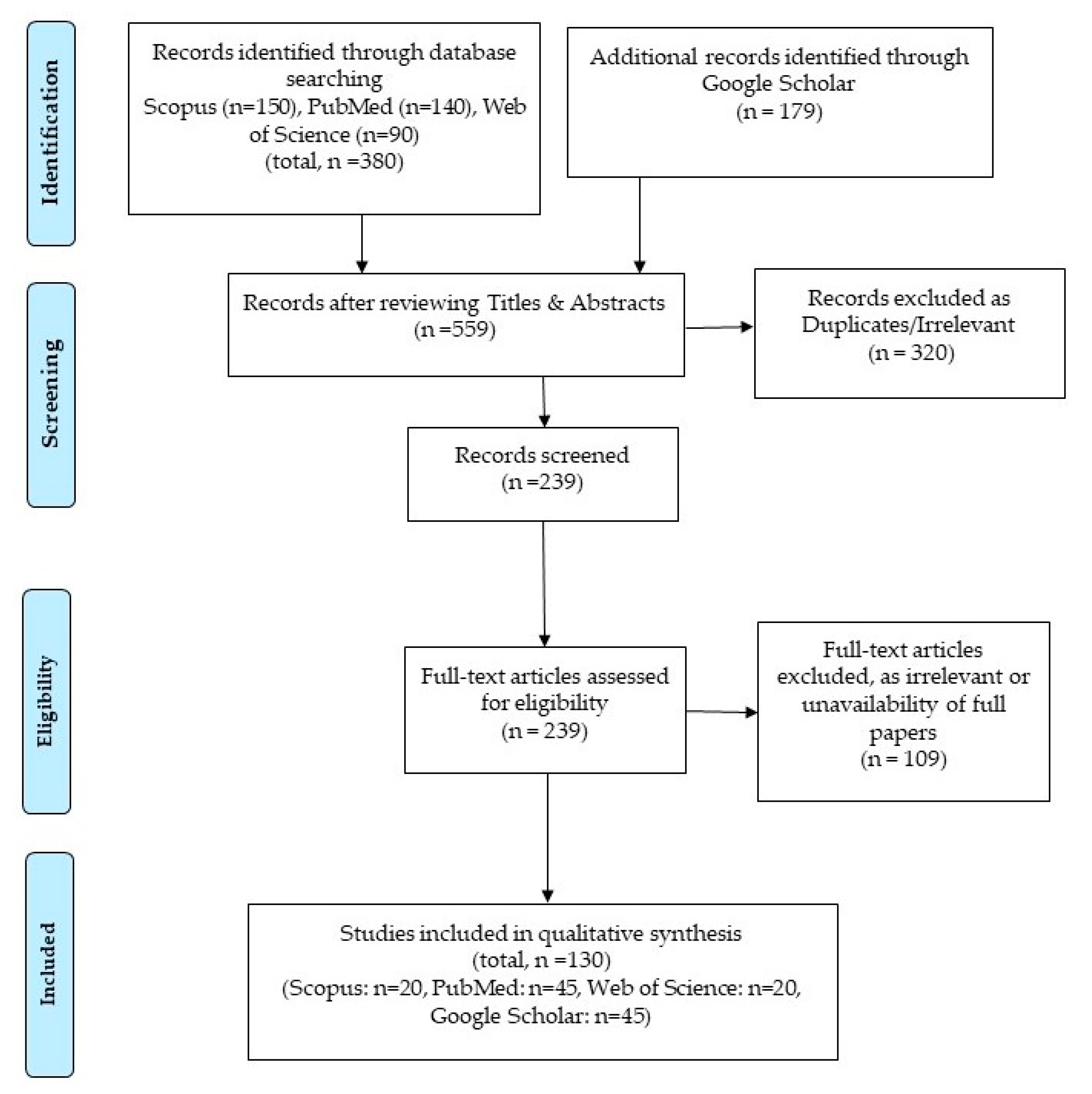
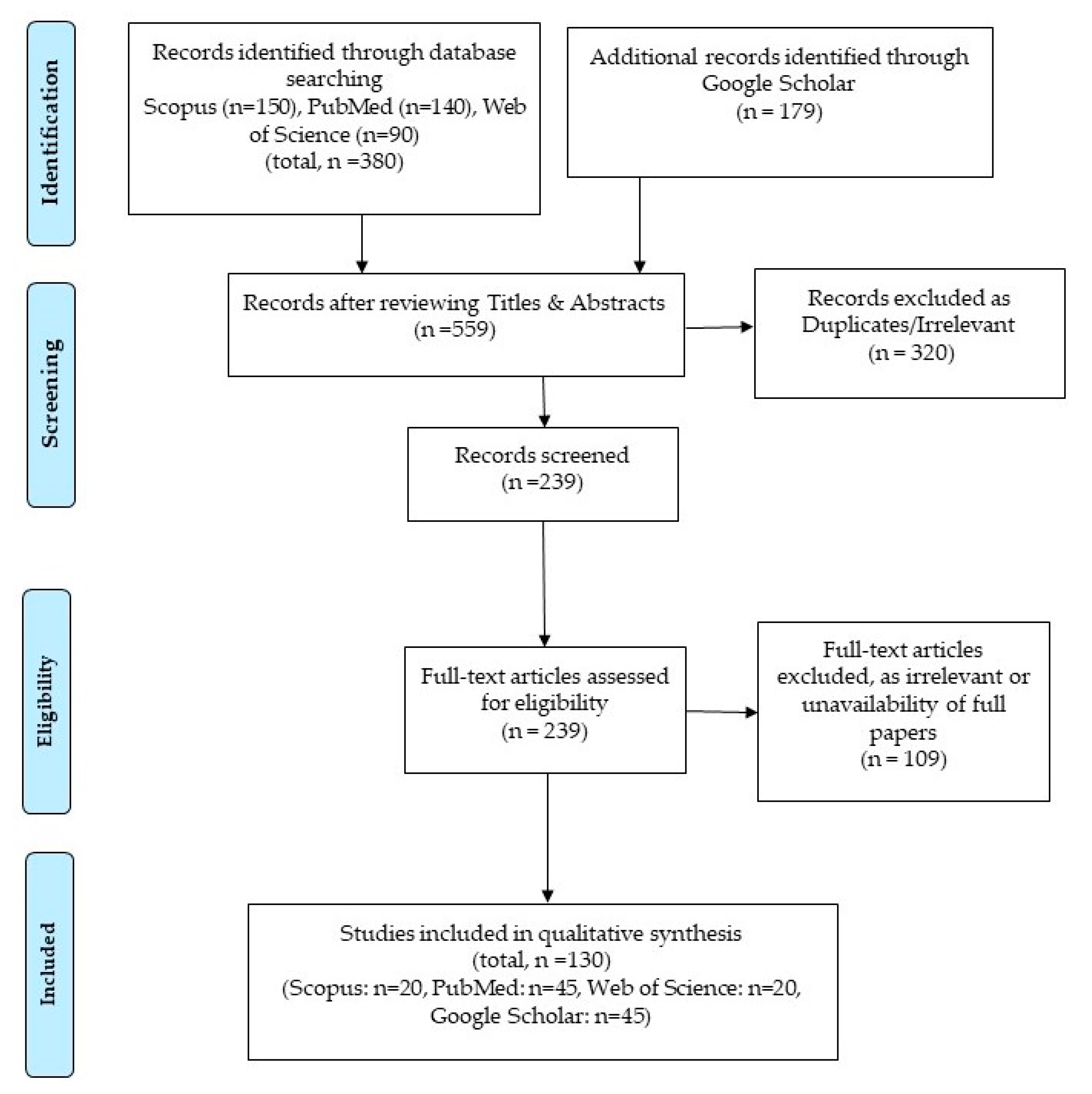
2.1. Search Strategy
2.2. Selection of Articles
2.3. Synthesis of Data

{kind=link}
| Device/Service | Category | Functionality |
|---|---|---|
| Cognitive Assistive Technologies (COACH, zero-effort technologies) [41,42,43] | Telecare | Prompt to PLWD on daily activities at home (such as hand washing). |
| Smart home [44,45,46,47,48,49,50,51,52,53,54] | Telecare | Analyse health, prompt for medication, support for cooking, dressing, clinical trials at home. |
| Avoiding hospitalization [55,56,57,58] | Telecare | Home care, (cost-effective, health safety, psychological stress). |
| Virtual visiting (Social robots) [9,19,36,51,59,60,61,62,63,64,65,66,67] | Telecare | Remote health check-up, reducing physical contact, cost-effective informal caregiving (supporting food preparation, eating, recreational activities). |
| Reminder systems [53,54,68,69] | Telecare | Memory support (alarm, communicator, diary, reminders), remote schedule prompter, medication regime support. |
| Video monitoring system [19,26,38,70,71,72,73,74] | Telecare | Audio-video conferencing with family and remote surveillance. |
| GPS-based devices [75,76] | Location | Monitoring geographic location of PLWD. |
| Safe walking [77,78,79,80] | Location | Navigation and route finding. |
| Smart phones with GPS [80,81] | Location | Navigation prompting with identification of indicators of disorientation for PLWD. |
| Exercising in virtual environments [82,83] | Location | Indoor exercising, navigating practice. |
| Health monitors [84,85] | Location | Health monitoring in outdoors activities. |
| Safety keys [86,87] | Safety and Security | Easy access to house. |
| Auto water controller [86,87] | Safety and Security | Automatically disables water flows. |
| Auto gas supply controller [86,87] | Safety and Security | Automatically disables gas supply. |
| Safe home (door alerts, video call, burglar alarm, automatic fire detectors) [88] | Safety and Security | Remote home surveillance. |
| Social alarm system (crime surveillance, fire alarm services, community safety, telehealth) [89,90] | Safety and Security | Social support to PLWD during emergency. |
| Pressure mats [91,92] | Safety and Security | Movement detection and automatic communication to the carer. |
| Telephone-blocker [86,93] | Safety and Security | Blocks unwanted calls automatically. |
| Item locator [10,24,94,95,96] | Safety & Security | Helps locate important items for PLWD. |
3. Results
- Telecare.
- Location.
- Safety and Security.
3.1. Telecare
3.1.1. Reducing Hospitalization
3.1.2. Virtual Visiting
3.1.3. Reminder Systems
3.1.4. Video Monitoring
3.2. Location
Health Monitors
- Tunstall: They primarily detect the impact and then the angle of tilt of the wearer. It generates an alarm after producing a 15 s warning, if horizontal. The alarm can be cancelled during the warning time. Some users find difficulty in wearing it all the time, for example, during bedtimes.
- Tele-alarm: These sensors consist of an accelerometer and a tiltmeter and can measure tilt continuously. Whenever the change in tilt is greater than 45 degrees and is followed by an impact, it generates an alarm. Unlike Tunstall, they can be worn at any time; however, they do not provide any warning of an impending fall.
- Technology in healthcare: It detects the rate of change of body tilt angle. The body tilt angle during a fall provides a measure for the change of posture. When the tilt rate is greater than 30 degrees/second, it generates an alarm.
3.3. Safety and Security
3.3.1. Home Security
3.3.2. Social Alarm Systems
3.3.3. Pressure Mats
3.3.4. Telephone Blockers
3.3.5. Item Locator
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hughes, J.C. Alzheimer’s and Other Dementias; Oxford University Press: Oxford, UK, 2011; ISBN 0199596557. [Google Scholar]
- Wittenberg, R.; Hu, B.; Barraza-Araiza, L.F.; Rehill, A. Projections of Older People with Dementia and Costs of Dementia Care in the United Kingdom, 2019–2040; CPEC Working Paper; London School of Economics: London, UK, 2019; pp. 1–79. [Google Scholar]
- WHO. Global Action Plan. on the Public Health Response to Dementia 2017–2025; WHO Document Production Services: Geneva, Switzerland, 2017. [Google Scholar]
- Chernbumroong, S.; Cang, S.; Atkins, A.; Yu, H. Elderly activities recognition and classification for applications in assisted living. Expert Syst. Appl. 2013, 40, 1662–1674. [Google Scholar] [CrossRef]
- Prince, M.; Knapp, M.; Guerchet, M.; McCrone, P.; Prina, M.; Comas-Herrera, A.; Wittenberg, R.; Adelaja, B.; Hu, B. Dementia UK: Update; Alzheimer’s Society: London, UK, 2014; Volume 1, pp. 6–86. [Google Scholar] [CrossRef]
- Chester, H.; Clarkson, P.; Davies, L.; Sutcliffe, C.; Davies, S.; Feast, A.; Hughes, J.; Challis, D. People with dementia and carer preferences for home support services in early-stage dementia. Aging Ment. Health 2018, 22, 270–279. [Google Scholar] [CrossRef]
- Improving Services and Support for People with Dementia; National Audit Office: London, UK, 2007; Volume 1, pp. 1–72.
- How Technology Can Help. Available online: https://www.alzheimers.org.uk/get-support/staying-independent/how-technology-can-help (accessed on 30 May 2021).
- Assistive Technology—Devices to Help with Everyday Living; Alzheimer’s Society: London, UK, 2014; Volume 1, pp. 1–17.
- Prince, M.; Wimo, A.; Guerchet, M.; Gemma-Claire, A.; Wu, Y.-T.; Prina, M. World Alzheimer Report 2015: The Global Impact of Dementia—An analysis of prevalence, incidence, cost and trends. Alzheimer’s Dis. Int. 2015. Available online: https://kclpure.kcl.ac.uk/portal/en/publications/world-alzheimer-report-2015--the-global-impact-of-dementia(ae525fda-1938-4892-8daa-a2222a672254).html (accessed on 6 July 2021).
- Cahill, S.; Begley, E.; Faulkner, J.P.; Hagen, I. “It gives me a sense of independence”—Findings from Ireland on the use and usefulness of assistive technology for people with dementia. Technol. Disabil. 2007, 19, 133–142. [Google Scholar] [CrossRef]
- Harmand, M.G.-C.; Meillon, C.; Rullier, L.; Avila-Funes, J.-A.; Bergua, V.; Dartigues, J.-F.; Amieva, H. Cognitive decline after entering a nursing home: A 22-year follow-up study of institutionalized and noninstitutionalized elderly people. J. Am. Med. Dir. Assoc. 2014, 15, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P. Depressive disorders in caregivers of dementia patients: A systematic review. Aging Ment. Health 2005, 9, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Bull, C.; Almond, T.; Christensen, H.; Fenech, M. Chronic stress and suboptimal nutrition is associated with chromosome instability in dementia family carers. Psychoneuroendocrinology 2017, 83, 89. [Google Scholar] [CrossRef]
- Canevelli, M.; Valletta, M.; Toccaceli Blasi, M.; Remoli, G.; Sarti, G.; Nuti, F.; Sciancalepore, F.; Ruberti, E.; Cesari, M.; Bruno, G. Facing Dementia During the COVID-19 Outbreak. J. Am. Geriatr. Soc. 2020, 68, 1673–1676. [Google Scholar] [CrossRef] [PubMed]
- Cheung, G.; Peri, K. Challenges to dementia care during COVID-19: Innovations in remote delivery of group Cognitive Stimu-lation Therapy. Aging Ment. Health 2021, 25, 977–979. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Li, T.; Barbarino, P.; Gauthier, S.; Brodaty, H.; Molinuevo, J.L.; Xie, H.; Sun, Y.; Yu, E.; Tang, Y. Dementia care during COVID-19. Lancet 2020, 395, 1190–1191. [Google Scholar] [CrossRef]
- Korczyn, A.D. Dementia in the COVID-19 period. J. Alzheimer’s Dis. 2020, 75, 1071. [Google Scholar] [CrossRef]
- Palgi, Y.; Shrira, A.; Ring, L.; Bodner, E.; Avidor, S.; Bergman, Y.; Cohen-Fridel, S.; Keisari, S.; Hoffman, Y. The loneliness pandemic: Loneliness and other concomitants of depression, anxiety and their comorbidity during the COVID-19 outbreak. J. Affect. Disord. 2020, 275, 109–111. [Google Scholar] [CrossRef] [PubMed]
- Tso, I.F.; Park, S. Alarming levels of psychiatric symptoms and the role of loneliness during the COVID-19 epidemic: A case study of Hong Kong. Psychiatry Res. 2020, 293, 113423. [Google Scholar] [CrossRef]
- Li, L.Z.; Wang, S. Prevalence and predictors of general psychiatric disorders and loneliness during COVID-19 in the United Kingdom. Psychiatry Res. 2020, 291, 113267. [Google Scholar] [CrossRef]
- Velayudhan, L.; Aarsland, D.; Ballard, C. Mental health of people living with dementia in care homes during COVID-19 pandemic. Int. Psychogeriatr. 2020, 32, 1253–1254. [Google Scholar] [CrossRef]
- Borges-Machado, F.; Barros, D.; Ribeiro, Ó.; Carvalho, J. The Effects of COVID-19 Home Confinement in Dementia Care: Phys-ical and Cognitive Decline, Severe Neuropsychiatric Symptoms and Increased Caregiving Burden. Am. J. Alzheimers. Dis. Other Dement. 2020, 35, 1533317520976720. [Google Scholar] [CrossRef]
- Cagnin, A.; Di Lorenzo, R.; Marra, C.; Bonanni, L.; Cupidi, C.; Laganà, V.; Rubino, E.; Vacca, A.; Provero, P.; Isella, V.; et al. Behavioral and psychological effects of coronavirus disease-19 quarantine in patients with dementia. Front. Psychiatry 2020, 11, 916. [Google Scholar] [CrossRef]
- Sutin, A.R.; Stephan, Y.; Luchetti, M.; Terracciano, A. Loneliness and risk of dementia. J. Gerontol. Ser. B 2020, 75, 1414–1422. [Google Scholar] [CrossRef]
- Williams, K.; Arthur, A.; Niedens, M.; Moushey, L.; Hutfles, L. In-Home Monitoring Support for Dementia Caregivers: A Feasibility Study. Clin. Nurs. Res. 2013, 22, 139–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, D.; Bharucha, A.J.; Wactlar, H.D. Intelligent video monitoring to improve safety of older persons. In Proceedings of the 2007 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 22–26 August 2007; pp. 3814–3817. [Google Scholar] [CrossRef]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- New Trial to Look at Reducing Transmission of Covid—19 in Care Homes. Available online: https://www.news-medical.net/news/20210127/New-trial-to-look-at-reducing-transmission-of-Covid-19-in-care-homes.aspx (accessed on 6 July 2021).
- Van den Heuvel, E.; Jowitt, F.; McIntyre, A. Awareness, requirements and barriers to use of Assistive Technology designed to enable independence of people suffering from Dementia (ATD). Technol. Disabil. 2012, 24, 139–148. [Google Scholar] [CrossRef] [Green Version]
- Burstein, A.A.; DaDalt, O.; Kramer, B.; D’Ambrosio, L.A.; Coughlin, J.F. Dementia caregivers and technology acceptance: Interest outstrips awareness. Gerontechnology 2015, 14, 45–56. [Google Scholar] [CrossRef]
- Gibson, G.; Dickinson, C.; Brittain, K.; Robinson, L. The everyday use of assistive technology by people with dementia and their family carers: A qualitative study. BMC Geriatr. 2015, 15, 89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooks, N.A. User’s responses to assistive devices for physical disability. Soc. Sci. Med. 1991, 32, 1417–1424. [Google Scholar] [CrossRef]
- Brims, L.; Oliver, K. Effectiveness of assistive technology in improving the safety of people with dementia: A systematic review and meta-analysis. Aging Ment. Health 2019, 23, 942–951. [Google Scholar] [CrossRef] [PubMed]
- Bharucha, A.J.; Anand, V.; Forlizzi, J.; Dew, M.A.; Reynolds, C.F., III; Stevens, S.; Wactlar, H. Intelligent assistive technology applications to dementia care: Current capabilities, limitations, and future challenges. Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2009, 17, 88–104. [Google Scholar] [CrossRef]
- Fleming, R.; Sum, S. Empirical studies on the effectiveness of assistive technology in the care of people with dementia: A systematic review. J. Assist. Technol. 2014, 8, 14–34. [Google Scholar] [CrossRef]
- Ienca, M.; Fabrice, J.; Elger, B.; Caon, M.; Scoccia Pappagallo, A.; Kressig, R.W.; Wangmo, T. Intelligent Assistive Technology for Alzheimer’s Disease and Other Dementias: A Systematic Review. J. Alzheimer’s Dis. 2017, 56, 1301–1340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sriram, V.; Jenkinson, C.; Peters, M. Informal carers’ experience of assistive technology use in dementia care at home: A systematic review. BMC Geriatr. 2019, 19, 160. [Google Scholar] [CrossRef] [Green Version]
- Huremović, D. Psychiatry of Pandemics; Springer: Berlin/Heidelberg, Germany, 2020; Volume 61, pp. 270–284. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Mihailidis, A.; Boger, J.N.; Craig, T.; Hoey, J. The COACH prompting system to assist older adults with dementia through handwashing: An efficacy study. BMC Geriatr. 2008, 8, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Begum, M.; Wang, R.; Huq, R.; Mihailidis, A. Performance of daily activities by older adults with dementia: The role of an assistive robot. In Proceedings of the 2013 IEEE 13th International Conference on Rehabilitation Robotics (ICORR), Seattle, WA, USA, 24–26 June 2013; IEEE: Piscataway, NJ, USA; pp. 1–8. [Google Scholar]
- Boger, J.; Young, V.; Hoey, J.; Jiancaro, T.; Mihailidis, A. Zero-Effort Technologies: Considerations, Challenges, and Use in Health, Wellness, and Rehabilitation. Synth. Lect. Assist. Rehabil. Health Technol. 2018, 8, i-118. [Google Scholar] [CrossRef]
- Cook, G.A.; Bailey, C.; Moyle, W. The impact of ICT-based telecare technology on quality of life of people with dementia: Review of the literature. In Proceedings of the 2013 6th International Conference on Human System Interactions (HSI), Sopot, Poland, 6–8 June 2013; pp. 614–619. [Google Scholar] [CrossRef]
- Sprint, G.; Cook, D.J.; Fritz, R.; Schmitter-Edgecombe, M. Using smart homes to detect and analyze health events. Computer 2016, 49, 29–37. [Google Scholar] [CrossRef]
- Amiribesheli, M.; Bouchachia, H. A tailored smart home for dementia care. J. Ambient Intell. Humaniz. Comput. 2018, 9, 1755–1782. [Google Scholar] [CrossRef] [Green Version]
- Orpwood, R.; Gibbs, C.; Adlam, T.; Faulkner, R.; Meegahawatte, D. The Gloucester smart house for people with dementia—user-interface aspects. In Designing a More Inclusive World; Springer: Berlin/Heidelberg, Germany, 2004; pp. 237–245. [Google Scholar]
- Pigot, H.; Mayers, A.; Giroux, S. The intelligent habitat and everyday life activity support. In Proceedings of the 5th International conference on Simulations in Biomedicine, Ljubljana, Slovenia, 2–4 April 2003; pp. 507–516. [Google Scholar] [CrossRef] [Green Version]
- Burleson, W.; Lozano, C.; Ravishankar, V.; Lee, J.; Mahoney, D. An assistive technology system that provides personalized dressing support for people living with dementia: Capability study. JMIR Med. Inform. 2018, 6, e21. [Google Scholar] [CrossRef] [Green Version]
- Hu, Y.; Tilke, D.; Adams, T.; Crandall, A.S.; Cook, D.J.; Schmitter-Edgecombe, M. Smart home in a box: Usability study for a large scale self-installation of smart home technologies. J. Reliab. Intell. Environ. 2016, 2, 93–106. [Google Scholar] [CrossRef] [Green Version]
- Kaye, J. Home-based technologies: A new paradigm for conducting dementia prevention trials. Alzheimer’s Dement. 2008, 4, S60–S66. [Google Scholar] [CrossRef] [PubMed]
- Teipel, S.; König, A.; Hoey, J.; Kaye, J.; Krüger, F.; Robillard, J.M.; Kirste, T.; Babiloni, C. Use of nonintrusive sensor-based information and communication technology for real-world evidence for clinical trials in dementia. Alzheimer’s Dement. 2018, 14, 1216–1231. [Google Scholar] [CrossRef]
- The Provision of Equipment to Older or Disabled People by the NHS and Social Services in England and Wales. Available online: http://www.opengrey.eu/item/display/10068/615326 (accessed on 6 July 2021).
- Audit Commission. Assisting Independence: Fully Equipped 2; Audit Commission: Wanchai, Hong Kong, China, 2002.
- Toot, S.; Devine, M.; Akporobaro, A.; Orrell, M. Causes of Hospital Admission for People with Dementia: A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2013, 14, 463–470. [Google Scholar] [CrossRef]
- Madir, J.; Madir, J. Using Technology to Deliver Health Services. In HealthTech; Edward Elgar Publishing: Cheltenham, UK, 2020; Volume 5, pp. 1–22. ISBN 9781839104893. [Google Scholar]
- Roy, N.; Baltus, G.; Fox, D.; Gemperle, F.; Goetz, J.; Hirsch, T.; Margaritis, D.; Montemerlo, M.; Pineau, J.; Schulte, J. Towards personal service robots for the elderly. In Proceedings of the Workshop on Interactive Robots and Entertainment (WIRE 2000), Pittsburgh, PA, USA, 30 April–1 May 2000; Volume 25, p. 184. [Google Scholar]
- Leonard, B.E.; Myint, A. Changes in the immune system in depression and dementia: Causal or coincidental effects? Dialogues Clin. Neurosci. 2006, 8, 163. [Google Scholar]
- Pineau, J.; Montemerlo, M.; Pollack, M.; Roy, N.; Thrun, S. Towards robotic assistants in nursing homes: Challenges and results. Rob. Auton. Syst. 2003, 42, 271–281. [Google Scholar] [CrossRef]
- Coradeschi, S.; Cesta, A.; Cortellessa, G.; Coraci, L.; Gonzalez, J.; Karlsson, L.; Furfari, F.; Loutfi, A.; Orlandini, A.; Palumbo, F.; et al. Giraffplus: Combining social interaction and long term monitoring for promoting independent living. In Proceedings of the 2013 6th International Conference on Human System Interactions (HSI), Sopot, Poland, 6–8 June 2013; IEEE: Piscataway, NJ, USA; pp. 578–585. [Google Scholar]
- Derek, M.; Chan, J.; Nejat, G. A socially assistive robot for meal-time cognitive interventions. J. Med. Devices 2012, 6, 017559. [Google Scholar] [CrossRef]
- Louie, W.-Y.G.; Li, J.; Mohamed, C.; Despond, F.; Lee, V.; Nejat, G. Tangy the robot bingo facilitator: A performance review. J. Med. Devices 2015, 9, 020936. [Google Scholar] [CrossRef]
- Chiu, T.; Marziali, E.; Colantonio, A.; Carswell, A.; Gruneir, M.; Tang, M.; Eysenbach, G. Internet-based caregiver support for Chinese Canadians taking care of a family member with Alzheimer disease and related dementia. Can. J. Aging La Rev. Can. Vieil. 2009, 28, 323–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Czaja, S.J.; Loewenstein, D.; Schulz, R.; Nair, S.N.; Perdomo, D. A videophone psychosocial intervention for dementia caregivers. Am. J. Geriatr. Psychiatry 2013, 21, 1071–1081. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, J.H.; Jhoo, J.H.; Lee, K.U.; Kim, K.W.; Lee, D.Y.; Woo, J.I. A telemedicine system as a care modality for dementia patients in Korea. Alzheimer Dis. Assoc. Disord. 2000, 14, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.Y.; Murphy, R.R.; Robinson, G.; Fredrickson, K.R.; Thielke, S.M.; Tsuang, D.W.; Borson, S. A Dementia Care Shared Medical Visit Model for Patients and Caregivers Using Telemedicine. J. Neuropsychiatry Clin. Neurosci. 2014, 26, 23–24. [Google Scholar]
- Ory, M.G.; Hoffman, R.R., III; Yee, J.L.; Tennstedt, S.; Schulz, R. Prevalence and Impact of Caregiving: A Detailed Comparison Between Dementia and Nondementia Caregivers. Gerontologist 1999, 39, 177–186. [Google Scholar] [CrossRef] [Green Version]
- Yasuda, K.; Kuwahara, N.; Kuwabara, K.; Morimoto, K.; Tetsutani, N. Daily assistance for individuals with dementia via videophone. Am. J. Alzheimers. Dis. Other Demen. 2013, 28, 508–516. [Google Scholar] [CrossRef]
- Tokunaga, S.; Horiuchi, H.; Takatsuka, H.; Saiki, S.; Matsumoto, S.; Nakamura, M.; Yasuda, K. Towards personalized and context-aware reminder service for people with dementia. In Proceedings of the 2016 International Joint Conference on Neural Networks (IJCNN), Vancouver, BC, Canada, 24–29 July 2016; pp. 946–2953. [Google Scholar] [CrossRef]
- D’Onofrio, G.; Sancarlo, D.; Ricciardi, F.; Panza, F.; Seripa, D.; Cavallo, F.; Giuliani, F.; Greco, A. Information and Communication Technologies for the Activities of Daily Living in Older Patients with Dementia: A Systematic Review. J. Alzheimer’s Dis. 2017, 57, 927–935. [Google Scholar] [CrossRef] [Green Version]
- Bayen, E.; Jacquemot, J.; Netscher, G.; Agrawal, P.; Tabb Noyce, L.; Bayen, A. Reduction in Fall Rate in Dementia Managed Care Through Video Incident Review: Pilot Study. J. Med. Internet. Res. 2017, 19, e339. [Google Scholar] [CrossRef]
- Hori, M.; Kubota, M.; Ando, K.; Kihara, T.; Takahashi, R.; Kinoshita, A. The effect of videophone communication (with skype and webcam) for elderly patients with dementia and their caregivers. Gan Kagaku Ryoho 2009, 36, 36. [Google Scholar]
- Van der Ploeg, E.S.; Eppingstall, B.; O’Connor, D.W. Internet video chat (Skype) family conversations as a treatment of agitation in nursing home residents with dementia. Int. Psychogeriatr. 2016, 28, 697–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, D.; Park, H.W.; Piao, M.; Ryu, K.H. The design and partial implementation of the dementia-aid monitoring system based on sensor network and cloud computing platform. In Applied Computing & Information Technology; Springer: Berlin/Heidelberg, Germany, 2016; pp. 85–100. [Google Scholar]
- Liu, L.; Miguel Cruz, A.; Ruptash, T.; Barnard, S.; Juzwishin, D. Acceptance of global positioning system (GPS) technology among dementia clients and family caregivers. J. Technol. Hum. Serv. 2017, 35, 99–119. [Google Scholar] [CrossRef]
- Lin, Y.J.; Chen, H.S.; Su, M.J. A Cloud based Bluetooth Low Energy tracking system for dementia patients. In Proceedings of the Eighth International Conference on Mobile Computing and Ubiquitous Networking (ICMU), Hakodate, Japan, 20–22 January 2015. [Google Scholar]
- Liao, L.; Patterson, D.J.; Fox, D.; Kautz, H. Learning and inferring transportation routines. Artif. Intell. 2007, 171, 311–331. [Google Scholar] [CrossRef] [Green Version]
- Wood, E.; Ward, G.; Woolham, J. The development of safer walking technology: A review. J. Assist. Technol. 2015, 9, 100–115. [Google Scholar] [CrossRef]
- Teipel, S.; Babiloni, C.; Hoey, J.; Kaye, J.; Kirste, T.; Burmeister, O.K. Information and communication technology solutions for outdoor navigation in dementia. Alzheimer’s Dement. 2016, 12, 695–707. [Google Scholar] [CrossRef] [Green Version]
- Kwan, R.Y.C.; Cheung, D.S.K.; Kor, P.P.-K. The use of smartphones for wayfinding by people with mild dementia. Dementia 2020, 19, 721–735. [Google Scholar] [CrossRef]
- Koldrack, P.; Teipel, S.J.; Kirste, T. Sensing disorientation of persons with dementia in outdoor wayfinding tasks using wearable sensors to enable situation-aware navigation assistance. Alzheimer’s Dement. 2016, 7, P160. [Google Scholar] [CrossRef]
- Schikhof, Y.; Wauben, L. Two types of stimuli in virtual cycling for people with dementia. Gerontechnology (Valkenswaard) 2016, 15, 163S. [Google Scholar]
- Blackman, T.; Van Schaik, P.; Martyr, A. Outdoor environments for people with dementia: An exploratory study using virtual reality. Ageing Soc. 2007, 27, 811–825. [Google Scholar] [CrossRef] [Green Version]
- Shin, D.; Shin, D.; Shin, D. Ubiquitous health management system with watch-type monitoring device for dementia patients. J. Appl. Math. 2014, 2014, 878741. [Google Scholar] [CrossRef]
- Doughty, K.; Lewis, R.; McIntosh, A. The design of a practical and reliable fall detector for community and institutional telecare. J. Telemed. Telecare 2000, 6, 150–154. [Google Scholar] [CrossRef]
- Gibson, G.; Newton, L.; Pritchard, G.; Finch, T.; Brittain, K.; Robinson, L. The provision of assistive technology products and services for people with dementia in the United Kingdom. Dementia 2016, 15, 681–701. [Google Scholar] [CrossRef] [Green Version]
- Olsson, A.; Engström, M.; Skovdahl, K.; Lampic, C. My, your and our needs for safety and security: Relatives’ reflections on using information and communication technology in dementia care. Scand. J. Caring Sci. 2012, 26, 104–112. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, B.; Bowen, M.E.; Keys, K.; Bulat, T. Safe home program: A suite of technologies to support extended home care of persons with dementia. Am. J. Alzheimer’s Dis. Other Dement. 2013, 28, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, M.; Nakashima, T. Features of the Japanese national dementia strategy in comparison with international dementia policies: How should a national dementia policy interact with the public health-and social-care systems? Alzheimer’s Dement. 2014, 10, 468–476. [Google Scholar] [CrossRef]
- Lauriks, S.; Reinersmann, A.; Van der Roest, H.G.; Meiland, F.J.M.; Davies, R.J.; Moelaert, F.; Mulvenna, M.D.; Nugent, C.D.; Dröes, R.-M. Review of ICT-based services for identified unmet needs in people with dementia. Ageing Res. Rev. 2007, 6, 223–246. [Google Scholar] [CrossRef]
- Murphy, J.; Gray, C.M.; van Achterberg, T.; Wyke, S.; Cox, S. The effectiveness of the Talking Mats framework in helping people with dementia to express their views on well-being. Dementia 2010, 9, 454–472. [Google Scholar] [CrossRef]
- Murphy, J.; Oliver, T. The use of Talking Mats to support people with dementia and their carers to make decisions together. Health Soc. Care Community 2013, 21, 171–180. [Google Scholar] [CrossRef]
- Chandaria, K. Shortchanged: Protecting People with Dementia from Financial Abuse; Alzheimer’s Society and National Institute for Health Research: London, UK, 2011; Volume 1, pp. 9–60. [Google Scholar]
- Maki, O.; Saarikalle, K.; Cahill, S.; Clarke, N.; Morbey, H.; Hayes, K. Enabling Technologies for People with Dementia. Available online: https://www.researchgate.net/profile/Nicholas-Clarke/publication/237782118_Enabling_Technologies_for_People_with_Dementia/links/542a909f0cf27e39fa8eaf4e/Enabling-Technologies-for-People-with-Dementia.pdf (accessed on 6 July 2021).
- Topo, P.; Saarikalle, K.; Mäki, O.; Parviainen, S. Enabling Technologies for People with Dementia, Report of Assessment Study in Finland. Methods 2004, 1, 1–46. [Google Scholar]
- Cash, M. At home with assistive technology. J. Dement. Care 2003, 11, 38. [Google Scholar]
- Evans, J.; Brown, M.; Coughlan, T.; Lawson, G.; Craven, M.P. A systematic review of dementia focused assistive technology. Lect. Notes Comput. Sci. (Incl. Subser. Lect. Notes Artif. Intell. Lect. Notes Bioinform.) 2015, 9170, 406–417. [Google Scholar] [CrossRef]
- Moyle, W. The promise of technology in the future of dementia care. Nat. Rev. Neurol. 2019, 15, 353–359. [Google Scholar] [CrossRef] [Green Version]
- Sanders, D.; Scott, P. Literature review: Technological interventions and their impact on quality of life for people living with dementia. BMJ Health Care Inform. 2020, 27, e100064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoel, V.; Feunou, C.M.; Wolf-Ostermann, K. Technology-driven solutions to prompt conversation, aid communication and support interaction for people with dementia and their caregivers: A systematic literature review. BMC Geriatr. 2021, 21, 157. [Google Scholar] [CrossRef]
- Leroi, I.; Woolham, J.; Gathercole, R.; Howard, R.; Dunk, B.; Fox, C.; O’Brien, J.; Bateman, A.; Poland, F.; Bentham, P.; et al. Does telecare prolong community living in dementia? A study protocol for a pragmatic, randomised controlled trial. Trials 2013, 14, 349. [Google Scholar] [CrossRef] [Green Version]
- Robinson, L.; Brittain, K.; Lindsay, S.; Jackson, D.; Olivier, P. Keeping in Touch Everyday (KITE) project: Developing assistive technologies with people with dementia and their carers to promote independence. Int. Psychogeriatr. 2009, 21, 494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardillo, E.; Sapienza, G.; Li, C.; Caddemi, A. Head Motion and Eyes Blinking Detection: A mm-Wave Radar for Assisting People with Neurodegenerative Disorders. In Proceedings of the 2020 50th European Microwave Conference (EuMC), Utrecht, The Netherlands, 12–14 January 2021; pp. 925–928. [Google Scholar] [CrossRef]
- Robillard, J.M.; Hoey, J. Emotion and motivation in cognitive assistive technologies for dementia. Computer 2018, 51, 24–34. [Google Scholar] [CrossRef]
- Wong-Lin, K.; McClean, P.L.; McCombe, N.; Kaur, D.; Sanchez-Bornot, J.M.; Gillespie, P.; Todd, S.; Finn, D.P.; Joshi, A.; Kane, J.; et al. Shaping a data-driven era in dementia care pathway through computational neurology approaches. BMC Med. 2020, 18, 398. [Google Scholar] [CrossRef]
- Shen, L.; Kennedy, D.; Preuss, N. The three NITRCs: Software, data and cloud computing for brain science and dementia research. Alzheimer’s Dement. 2013, 4, P78. [Google Scholar]
- Pot, A.M.; Willemse, B.M.; Horjus, S. A pilot study on the use of tracking technology: Feasibility, acceptability, and benefits for people in early stages of dementia and their informal caregivers. Aging Ment. Health 2012, 16, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Milne, H.; van der Pol, M.; McCloughan, L.; Hanley, J.; Mead, G.; Starr, J.; Sheikh, A.; McKinstry, B. The use of global positional satellite location in dementia: A feasibility study for a randomised controlled trial. BMC Psychiatry 2014, 14, 160. [Google Scholar] [CrossRef] [Green Version]
- Olsson, A.; Engström, M.; Åsenlöf, P.; Skovdahl, K.; Lampic, C. Effects of tracking technology on daily life of persons with dementia: Three experimental single-case studies. Am. J. Alzheimer’s Dis. Other Dement. 2015, 30, 29–40. [Google Scholar] [CrossRef] [PubMed]
- Holthe, T.; Jentoft, R.; Arntzen, C.; Thorsen, K. Benefits and burdens: Family caregivers’ experiences of assistive technology (AT) in everyday life with persons with young-onset dementia (YOD). Disabil. Rehabil. Assist. Technol. 2018, 13, 754–762. [Google Scholar] [CrossRef] [PubMed]
- Arntzen, C.; Holthe, T.; Jentoft, R. Tracing the successful incorporation of assistive technology into everyday life for younger people with dementia and family carers. Dementia 2016, 15, 646–662. [Google Scholar] [CrossRef]
- Riikonen, M.; Mäkelä, K.; Perälä, S. Safety and monitoring technologies for the homes of people with dementia. Gerontechnology 2010, 9, 32–45. [Google Scholar] [CrossRef]
- Øderud, T.; Landmark, B.; Eriksen, S.; Fossberg, A.B.; Aketun, S.; Omland, M.; Hem, K.-G.; Østensen, E.; Ausen, D. Persons with Dementia and Their Caregivers Using GPS. Stud. Health Technol. Inform. 2015, 217, 212–221. [Google Scholar]
- Olsson, A.; Engström, M.; Lampic, C.; Skovdahl, K. A passive positioning alarm used by persons with dementia and their spouses–a qualitative intervention study. BMC Geriatr. 2013, 13, 11. [Google Scholar] [CrossRef]
- O’Neill, D. Should patients with dementia who wander be electronically tagged? BMJ 2013, 346, 3606. [Google Scholar] [CrossRef] [PubMed]
- Zwijsen, S.A.; Niemeijer, A.R.; Hertogh, C.M.P.M. Ethics of using assistive technology in the care for community-dwelling elderly people: An overview of the literature. Aging Ment. Health 2011, 15, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Olsson, A.; Skovdahl, K.; Engström, M. Using diffusion of innovation theory to describe perceptions of a passive positioning alarm among persons with mild dementia: A repeated interview study. BMC Geriatr. 2016, 16, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Megges, H.; Freiesleben, S.D.; Lüdtke, V.; Rösch, C.; Peters, O. A longitudinal user study testing two locating systems in home dementia care. Alzheimer’s Dement. 2017, 13, P165–P166. [Google Scholar] [CrossRef]
- Godwin, B. The ethical evaluation of assistive technology for practitioners: A checklist arising from a participatory study with people with dementia, family and professionals. J. Assist. Technol. 2012, 6, 123–135. [Google Scholar] [CrossRef]
- Tchalla, A.E.; Lachal, F.; Cardinaud, N.; Saulnier, I.; Rialle, V.; Preux, P.-M.; Dantoine, T. Preventing and managing indoor falls with home-based technologies in mild and moderate Alzheimer’s disease patients: Pilot study in a community dwelling. Dement. Geriatr. Cogn. Disord. 2013, 36, 251–261. [Google Scholar] [CrossRef]
- Nauha, L.; Keränen, N.S.; Kangas, M.; Jämsä, T.; Reponen, J. Assistive technologies at home for people with a memory disorder. Dementia 2018, 17, 909–923. [Google Scholar] [CrossRef] [Green Version]
- Hall, A.; Wilson, C.B.; Stanmore, E.; Todd, C. Implementing monitoring technologies in care homes for people with dementia: A qualitative exploration using normalization process theory. Int. J. Nurs. Stud. 2017, 72, 60–70. [Google Scholar] [CrossRef] [PubMed]
- The Impact of COVID-19 on People Affected by Dementia. Available online: https://www.alzheimers.org.uk/sites/default/files/2020-08/The_Impact_of_COVID-19_on_People_Affected_By_Dementia.pdf (accessed on 6 July 2021).
- Cipriani, G.; Di Fiorino, M. Access to care for dementia patients suffering from COVID-19. Am. J. Geriatr. Psychiatry 2020, 28, 796–797. [Google Scholar] [CrossRef]
- Asghar, I.; Cang, S.; Yu, H. Usability evaluation of assistive technologies through qualitative research focusing on people with mild dementia. Comput. Hum. Behav. 2018, 79, 192–201. [Google Scholar] [CrossRef]
- Mallin, S.S.V.; de Carvalho, H.G. Assistive Technology and User-Centered Design: Emotion as element for innovation. Procedia Manuf. 2015, 3, 5570–5578. [Google Scholar] [CrossRef] [Green Version]
- Suijkerbuijk, S.; Nap, H.H.; Cornelisse, L.; Ijsselsteijn, W.A.; De Kort, Y.A.W.; Minkman, M.M.N.; Baglio, F. Active involvement of people with Dementia: A systematic review of studies developing supportive technologies. J. Alzheimer’s Dis. 2019, 69, 1041–1065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roelands, M.; Van Oost, P.; Buysse, A.; Depoorter, A. Awareness among community-dwelling elderly of assistive devices for mobility and self-care and attitudes towards their use. Soc. Sci. Med. 2002, 54, 1441–1451. [Google Scholar] [CrossRef]
- Deco, G.; Cruzat, J.; Cabral, J.; Tagliazucchi, E.; Laufs, H.; Logothetis, N.K.; Kringelbach, M.L. Awakening: Predicting external stimulation to force transitions between different brain states. Proc. Natl. Acad. Sci. USA 2019, 116, 18088–18097. [Google Scholar] [CrossRef] [Green Version]
- Meiland, F.; Reinersmann, A.; Bergvall-Kareborn, B.; Craig, D.; Moelaert, F.; Mulvenna, M.; Nugent, C.D.; Scully, T.; Bengtsson, J.; Dres, R.M. COGKNOW: Development of an ICT device to support people with dementia. J. Inf. Technol. Healthc. 2007, 5, 324–334. [Google Scholar]
- Certification-D—Certification of Technological Products for People with Dementia to Support SMEs in Innovation and Business Growth. Available online: https://www.nweurope.eu/projects/project-search/certification-d-certification-of-technological-products-for-people-with-dementia-to-support-smes-in-innovation-and-business-growth/ (accessed on 30 May 2021).
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Behera, C.K.; Condell, J.; Dora, S.; Gibson, D.S.; Leavey, G. State-of-the-Art Sensors for Remote Care of People with Dementia during a Pandemic: A Systematic Review. Sensors 2021, 21, 4688. https://doi.org/10.3390/s21144688
Behera CK, Condell J, Dora S, Gibson DS, Leavey G. State-of-the-Art Sensors for Remote Care of People with Dementia during a Pandemic: A Systematic Review. Sensors. 2021; 21(14):4688. https://doi.org/10.3390/s21144688
Chicago/Turabian StyleBehera, Chandan Kumar, Joan Condell, Shirin Dora, David S. Gibson, and Gerard Leavey. 2021. "State-of-the-Art Sensors for Remote Care of People with Dementia during a Pandemic: A Systematic Review" Sensors 21, no. 14: 4688. https://doi.org/10.3390/s21144688
APA StyleBehera, C. K., Condell, J., Dora, S., Gibson, D. S., & Leavey, G. (2021). State-of-the-Art Sensors for Remote Care of People with Dementia during a Pandemic: A Systematic Review. Sensors, 21(14), 4688. https://doi.org/10.3390/s21144688