
EEG-Based Prediction of the Recovery of Carotid Blood Flow during Cardiopulmonary Resuscitation in a Swine Model


Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Statement
2.2. Study Design and Setting
2.3. Experimental Animal and Housing
2.4. Surgical Preparation and Hemodynamic Measurements
2.5. EEG Signal Acquisition
2.6. Development of Machine-Learning Based Prediction Model
2.7. Performance Evaluation
3. Results
3.1. EEG Changes throughout the Experiments
3.2. EEG Parameters for Modeling
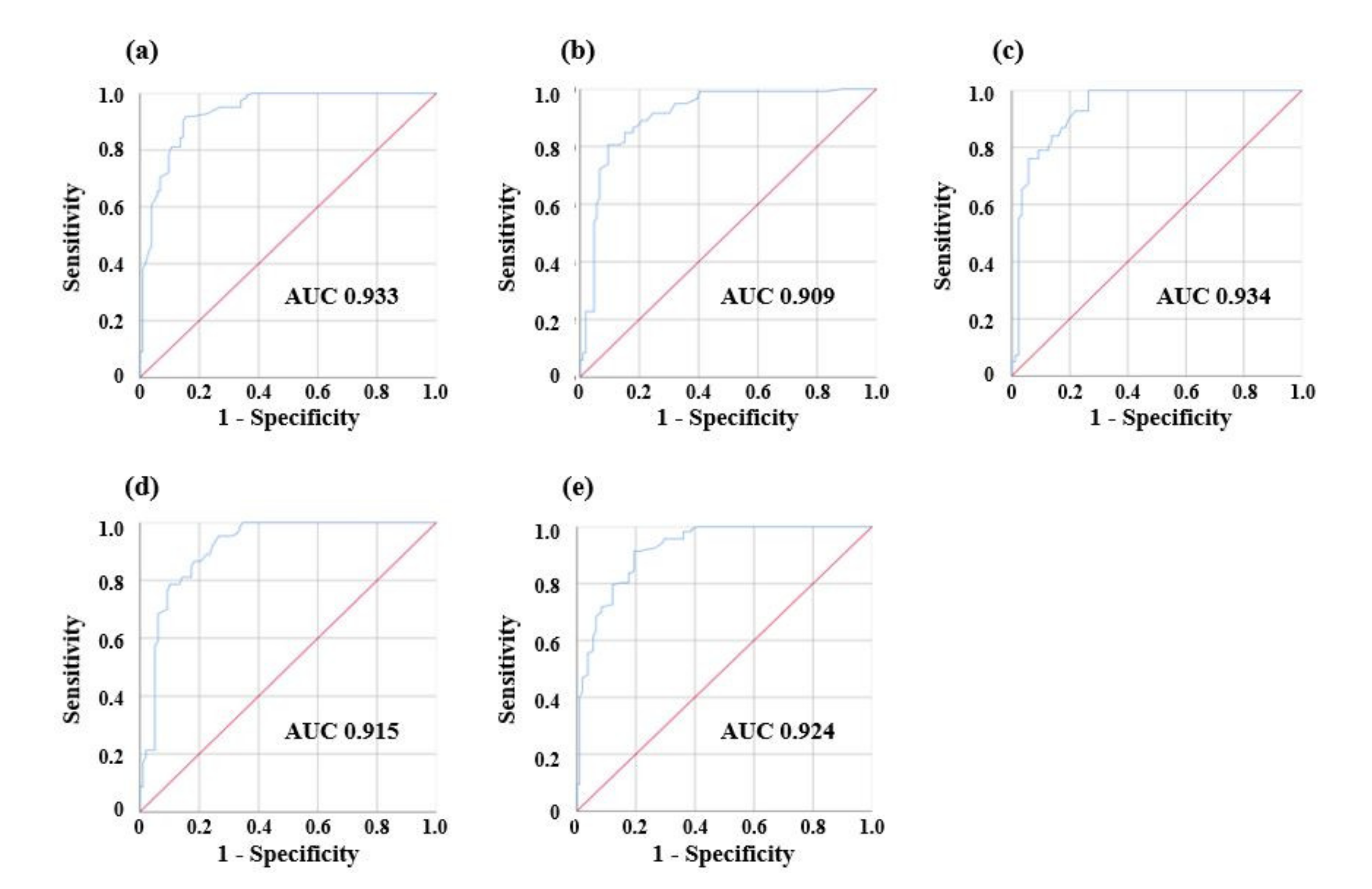
3.3. Performances of Prediction Models
4. Discussion
4.1. EEG Parameters and Classification Model of Performances
4.2. Clinical Implication and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sawyer, K.N.; Camp-Rogers, T.R.; Kotini-Shah, P.; Del Rios, M.; Gossip, M.R.; Moitra, V.K.; Haywood, K.L.; Dougherty, C.M.; Lubitz, S.A.; Rabinstein, A.A.; et al. Sudden Cardiac Arrest Survivorship: A Scientific Statement From the American Heart Association. Circulation 2020, 141, e654–e685. [Google Scholar] [CrossRef]
- Iwami, T.; Nichol, G.; Hiraide, A.; Hayashi, Y.; Nishiuchi, T.; Kajino, K.; Morita, H.; Yukioka, H.; Ikeuchi, H.; Sugimoto, H.; et al. Continuous Improvements in “Chain of Survival” Increased Survival After Out-of-Hospital Cardiac Arrests. Circulation 2009, 119, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.; Brown, L.L.; Duff, J.P.; Davidson, J.; Overly, F.; Tofil, N.M.; Peterson, D.T.; White, M.L.; Bhanji, F.; Bank, I.; et al. Improving Cardiopulmonary Resuscitation With a CPR Feedback Device and Refresher Simulations (CPR CARES Study). JAMA Pediatr. 2015, 169, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, S.M.; Farris, R.W.D.; Di Gennaro, J.L.; Roberts, J.S. Systematic Review and Meta-Analysis of End-Tidal Carbon Dioxide Values Associated With Return of Spontaneous Circulation During Cardiopulmonary Resuscitation. J. Intensiv. Care Med. 2014, 30, 426–435. [Google Scholar] [CrossRef] [PubMed]
- Sheak, K.R.; Wiebe, D.J.; Leary, M.; Babaeizadeh, S.; Yuen, T.C.; Zive, D.; Owens, P.C.; Edelson, D.P.; Daya, M.R.; Idris, A.H.; et al. Quantitative relationship between end-tidal carbon dioxide and CPR quality during both in-hospital and out-of-hospital cardiac arrest. Resuscitation 2015, 89, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Berg, K.M.; Cheng, A.; Panchal, A.R.; Topjian, A.A.; Aziz, K.; Bhanji, F.; Bigham, B.L.; Hirsch, K.G.; Hoover, A.V.; Kurz, M.C.; et al. Part 7: Systems of Care: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142, S580–S604. [Google Scholar] [CrossRef]
- Torgersen, J.; Strand, K.; Bjelland, T.W.; Klepstad, P.; Kvåle, R.; Søreide, E.; Wentzel-Larsen, T.; Flaatten, H. Cognitive dysfunction and health-related quality of life after a cardiac arrest and therapeutic hypothermia. Acta Anaesthesiol. Scand. 2010, 54, 721–728. [Google Scholar] [CrossRef]
- Aaslid, R.; Lundar, T.; Lindegaard, K.F.; Nornes, H. Estimation of Cerebral Perfusion Pressure from Arterial Blood Pressure and Transcranial Doppler Recordings. In Intracranial Pressure VI; Springer Science and Business Media LLC: Berlin/Heidelberg, Germany, 1986; pp. 226–229. [Google Scholar]
- Blumenstein, J.; Kempfert, J.; Walther, T.; Van Linden, A.; Fassl, J.; Borger, M.; Mohr, F.W. Cerebral Flow Pattern Monitoring by Transcranial Doppler during Cardiopulmonary Resuscitation. Anaesth. Intensiv. Care 2010, 38, 376–380. [Google Scholar] [CrossRef]
- Álvarez-Fernández, J.A.; Pérez-Quintero, R. Use of transcranial Doppler ultrasound in the management of post-cardiac arrest syndrome. Resuscitation 2009, 80, 1321–1322. [Google Scholar] [CrossRef]
- Schnaubelt, S.; Sulzgruber, P.; Menger, J.; Skhirtladze-Dworschak, K.; Sterz, F.; Dworschak, M. Regional cerebral oxygen saturation during cardiopulmonary resuscitation as a predictor of return of spontaneous circulation and favourable neurological outcome—A review of the current literature. Resuscitation 2018, 125, 39–47. [Google Scholar] [CrossRef]
- Reagan, E.M.; Nguyen, R.T.; Ravishankar, S.T.; Chabra, V.; Fuentes, B.; Spiegel, R.; Parnia, S. Monitoring the Relationship Between Changes in Cerebral Oxygenation and Electroencephalography Patterns During Cardiopulmonary Resuscitation. Crit. Care Med. 2018, 46, 757–763. [Google Scholar] [CrossRef]
- Azim, N.; Wang, C.Y. The use of bispectral index during a cardiopulmonary arrest: A potential predictor of cerebral perfusion. Anaesthesia 2004, 59, 610–612. [Google Scholar] [CrossRef] [PubMed]
- Meaney, P.A.; Bobrow, B.J.; Mancini, M.E.; Christenson, J.; de Caen, A.R.; Bhanji, F.; Abella, B.S.; Kleinman, M.E.; Edelson, D.P.; Berg, R.A.; et al. Cardiopulmonary resuscitation quality: Improving cardiac resuscitation outcomes both inside and outside the hospital: A consensus statement from the American Heart Association. Circulation 2013, 128, 417–435. [Google Scholar] [CrossRef]
- Friess, S.H.; Sutton, R.M.; French, B.; Bhalala, U.; Maltese, M.R.; Naim, M.Y.; Bratinov, G.; Rodriguez, S.A.; Weiland, T.R.; Garuccio, M.; et al. Hemodynamic directed CPR improves cerebral perfusion pressure and brain tissue oxygenation. Resuscitation 2014, 85, 1298–1303. [Google Scholar] [CrossRef]
- Lewis, L.M.; Stothert, J.; Standeven, J.; Chandel, B.; Kurtz, M.; Fortney, J. Correlation of end-tidal CO2 to cerebral perfusion during CPR. Ann. Emerg. Med. 1992, 21, 1131–1134. [Google Scholar] [CrossRef]
- Kim, H.; Kim, K.H.; Hong, K.J.; Ku, Y.; Shin, S.D.; Kim, H.C. Frontal EEG Changes with the Recovery of Carotid Blood Flow in a Cardiac Arrest Swine Model. Sensors 2020, 20, 3052. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.; Shin, S.D.; Song, K.J.; Park, Y.J.; Ryu, H.H.; Debaty, G.; Lurie, K.; Hong, K.J. The effect of resuscitation position on cerebral and coronary perfusion pressure during mechanical cardiopulmonary resuscitation in porcine cardiac arrest model. Resuscitation 2017, 113, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Covert, R.; Schreiber Torgerson, L.; Torgerson, R.; Miletich, D. Prediction of cerebral blood flow in fetal lambs by carotid artery ultrasonic flow transducer. Reprod. Fertil. Dev. 1996, 8, 157–162. [Google Scholar] [CrossRef]
- Mullie, A.; Lewi, P.; Van Hoeyweghen, R. Pre-CPR conditions and the final outcome of CPR. Resuscitation 1989, 17, S11–S21. [Google Scholar] [CrossRef]
- Peberdy, M.A.; Callaway, C.W.; Neumar, R.W.; Geocadin, R.G.; Zimmerman, J.L.; Donnino, M.; Gabrielli, A.; Silvers, S.M.; Zaritsky, A.L.; Merchant, R.; et al. Part 9: Post-Cardiac Arrest Care: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2010, 122, S768–S786. [Google Scholar] [CrossRef]
- National Research Council. Guide for the Care and Use of Laboratory Animals; National Academies Press: Washington, DC, USA, 2010. [Google Scholar]
- Newell, C.; Grier, S.; Soar, J. Airway and ventilation management during cardiopulmonary resuscitation and after successful resuscitation. Crit. Care 2018, 22, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Marshall, R.S. The functional relevance of cerebral hemodynamics: Why blood flow matters to the injured and recovering brain. Curr. Opin. Neurol. 2004, 17, 705–709. [Google Scholar] [CrossRef]
- Goldberger, J.; Hinton, G.E.; Roweis, S.T.; Salakhutdinov, R.R. Neighbourhood components analysis. In Proceedings of the Advances in Neural Information Processing Systems, Vancouver, BC, Canada, 5–8 December 2005; pp. 513–520. [Google Scholar]
- Tomioka, R.; Aihara, K.; Müller, K.-R. Logistic regression for single trial EEG classification. In Proceedings of the Advances in Neural Information Processing Systems, Vancouver, BC, Canada, 3–6 December 2007; pp. 1377–1384. [Google Scholar]
- Bhavsar, H.; Panchal, M.H. A review on support vector machine for data classification. Int. J. Adv. Res. Comput. Eng. Technol. 2012, 1, 185–189. [Google Scholar]
- Peterson, L.E. K-nearest neighbor. Scholarpedia 2009, 4, 1883. [Google Scholar] [CrossRef]
- Edla, D.R.; Mangalorekar, K.; Dhavalikar, G.; Dodia, S. Classification of EEG data for human mental state analysis using Random Forest Classifier. Procedia Comput. Sci. 2018, 132, 1523–1532. [Google Scholar] [CrossRef]
- Cybenko, G. Approximation by superpositions of a sigmoidal function. Math. Control. Signals Syst. 1989, 2, 303–314. [Google Scholar] [CrossRef]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic minority over-sampling technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Visa, S.; Ramsay, B.; Ralescu, A.L.; van der Knaap, E. Confusion Matrix-based Feature Selection. MAICS 2011, 710, 120–127. [Google Scholar]
- Goutte, C.; Gaussier, E. A probabilistic interpretation of precision, recall and F-score, with implication for evaluation. In Proceedings of the European Conference on Information Retrieval, Rome, Italy, 2–5 April 2005; Springer: Berlin/Heidelberg, Germany, 2005; pp. 345–359. [Google Scholar]
- Lund, A.; Secher, N.H.; Hirasawa, A.; Ogoh, S.; Hashimoto, T.; Schytz, H.W.; Ashina, M.; Sørensen, H. Ultrasound tagged near infrared spectroscopy does not detect hyperventilation-induced reduction in cerebral blood flow. Scand. J. Clin. Lab. Investig. 2015, 76, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Sandroni, C.; Parnia, S.; Nolan, J.P. Cerebral oximetry in cardiac arrest: A potential role but with limitations. Intensiv. Care Med. 2019, 45, 904–906. [Google Scholar] [CrossRef]
- De Vries, J.W.; Bakker, P.F.A.; Visser, G.H.; Diephuis, J.C.; Van Huffelen, A.C. Changes in Cerebral Oxygen Uptake and Cerebral Electrical Activity During Defibrillation Threshold Testing. Anesthesia Analg. 1998, 87, 16–20. [Google Scholar]
- LoSasso, T.J.; Muzzi, D.A.; Meyer, F.B.; Sharbrough, F.W. Electroencephalographic Monitoring of Cerebral Function During Asystole and Successful Cardiopulmonary Resuscitation. Anesthesia Analg. 1992, 75, 1021–1024. [Google Scholar] [CrossRef] [PubMed]
- Long, C.W.; Shah, N.K.; Loughlin, C.; Spydell, J.; Bedford, R.F. A comparison of EEG determinants of near-awakening from isoflurane and fentanyl anesthesia. Spectral edge, median power frequency, and delta ratio. Anesthesia Analg. 1989, 69, 169–173. [Google Scholar]
- Drummond, J.C.; Brann, C.A.; Perkins, D.E.; Wolfe, D.E. A comparison of median frequency, spectral edge frequency, a frequency band power ratio, total power, and dominance shift in the determination of depth of anesthesia. Acta Anaesthesiol. Scand. 1991, 35, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Mandrekar, J.N. Receiver Operating Characteristic Curve in Diagnostic Test Assessment. J. Thorac. Oncol. 2010, 5, 1315–1316. [Google Scholar] [CrossRef]
- Phelps, R.; Dumas, F.; Maynard, C.; Silver, J.; Rea, T. Cerebral Performance Category and Long-Term Prognosis Following Out-of-Hospital Cardiac Arrest. Crit. Care Med. 2013, 41, 1252–1257. [Google Scholar] [CrossRef]
- Zadini, F.; Newton, E.; Abdi, A.A.; Lenker, J.; Zadini, G.; Henderson, S.O. Use of the Trendelenburg Position in the Porcine Model Improves Carotid Flow During Cardiopulmonary Resuscitation. West. J. Emerg. Med. 2008, 9, 206–211. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Method | Measurement | Characteristics |
|---|---|---|---|
| Performance-oriented | Accelero-meter | Compression depth, rate | |
| Force sensor | Chest recoil | ||
| Patient-oriented | Capno-graphy | ETCO2 | |
| TCD | Velocity of CBF | ||
| NIRS | rSO2 | ||
| EEG | Cerebral electrical activity |
|
| CBF Recovery Degree | Class | Amount of Acquired Data in Each Experiment | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Test Number | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | Total | ||
| Lower (<30%) | group 0 | 0 | 40 | 0 | 0 | 44 | 0 | 2 | 33 | 119 | |
| Higher (≥30%) | group 1 | 15 | 1 | 28 | 12 | 1 | 14 | 35 | 0 | 106 | |
| All | Total amount | 15 | 41 | 28 | 12 | 45 | 14 | 37 | 33 | 225 | |
| EEG Parameters | Definition | NCA Feature Ranking | p-Value | Result of Selection |
|---|---|---|---|---|
| BSR | Burst suppression ratio | 18 | <0.001 | Excluded |
| Magnitude | Maximal amplitude during the epoch(unit: µV) | 11 | <0.001 | Selected |
| SynchFastSlow | Relative synchrony of fast and slow wave | 17 | 0.264 | Excluded |
| BetaR | log(P20–47 Hz/P11–20 Hz) | 4 | 0.864 | Excluded after Student’s t-test |
| DeltaR | log(P8–20 Hz/P1–4 Hz) | 5 | <0.001 | Selected |
| DAR | log(P1–4 Hz/P8–13 Hz) | 7 | <0.001 | Selected |
| DTABR | log(P1–8 Hz/P8–30 Hz) | 6 | <0.001 | Selected |
| BcSEF | Burst suppression ratio-compensated spectral edge frequency 95 | 1 | <0.001 | Selected |
| ExtraPR | P40–47 Hz/P1–47 Hz | 19 | 0.675 | Excluded |
| AlphaPR | P8–13 Hz/P1–47 Hz | 12 | 0.439 | Excluded |
| BetaPR | P13–30 Hz/P1–47 Hz | 16 | <0.001 | Excluded |
| DeltaPR | P1–4 Hz/P1–47 Hz | 3 | 0.014 | Selected |
| ThetaPR | P4–8 Hz/P1–47 Hz | 15 | <0.001 | Excluded |
| GammaPR | P30–47 Hz/P1–47 Hz | 13 | 0.001 | Excluded |
| Shannon entropy | 14 | 0.607 | Excluded | |
| Log energy entropy | 10 | <0.001 | Selected | |
| Spectral entropy | 2 | 0.013 | Selected | |
| Rényi entropy | 8 | <0.001 | Selected | |
| Ratio05 | Percentage of data whose amplitude is under ±5 µV | 20 | <0.001 | Excluded |
| BG_Alpha+ | P8–47 Hz/P1–47 Hz | 9 | <0.001 | Selected |
| EEG Parameters | Definition | Median (IQR) | p-Value | |
|---|---|---|---|---|
| Group 0 | Group 1 | |||
| Magnitude | Maximal amplitude during the epoch (unit: µV) | 4.08 (2.52 14.28) | 18.55 (15.72 22.29) | <0.001 |
| DeltaR | log(P8–20 Hz/P1–4 Hz) | 0.00 (−0.30 0.31) | 0.25 (−0.08 0.72) | <0.001 |
| DAR | log(P1–4 Hz/P8–13 Hz) | 0.20 (−0.10 0.49) | −0.07 (−0.42 0.36) | <0.001 |
| DeltaPR | log(P1–4 Hz/P1–47 Hz) | 0.28 (0.17 0.41) | 0.20 (0.08 0.41) | 0.014 |
| DTABR | log(P1–8 Hz/P8–30 Hz) | 0.18 (−0.10 0.45) | −0.06 (−0.31 0.21) | <0.001 |
| BcSEF | Burst suppression ratio-compensated spectral edge frequency 95 | 0.00 (0.00 19.50) | 27.0 (22.0 30.0) | <0.001 |
| BG_Alpha+ | P8–47 Hz/P1–47 Hz | 39.90 (26.54 55.94) | 54.53 (39.07 67.68) | <0.001 |
| Spectral entropy | 0.78 (0.76 0.80) | 0.79 (0.77 0.81) | 0.013 | |
| Rényientropy | 6.93 (5.57 9.06) | 9.83 (9.20 10.11) | <0.001 | |
| Log energyentropy | −241.24 (−1014.8 729.0) | 1122.30 (836.8 1304.1) | <0.001 | |
| Performance | LR | SVM | KNN | RF | MLP |
|---|---|---|---|---|---|
| Accuracy | 0.840 | 0.853 | 0.813 | 0.827 | 0.836 |
| Sensitivity | 0.782 | 0.807 | 0.689 | 0.748 | 0.798 |
| Specificity | 0.906 | 0.906 | 0.953 | 0.915 | 0.877 |
| Precision | 0.903 | 0.906 | 0.943 | 0.908 | 0.880 |
| F1 score | 0.838 | 0.853 | 0.796 | 0.820 | 0.837 |
| AUC | 0.933 | 0.909 | 0.934 | 0.915 | 0.924 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.; Kim, K.H.; Hong, K.J.; Ku, Y.; Shin, S.D.; Kim, H.C. EEG-Based Prediction of the Recovery of Carotid Blood Flow during Cardiopulmonary Resuscitation in a Swine Model. Sensors 2021, 21, 3650. https://doi.org/10.3390/s21113650
Kim H, Kim KH, Hong KJ, Ku Y, Shin SD, Kim HC. EEG-Based Prediction of the Recovery of Carotid Blood Flow during Cardiopulmonary Resuscitation in a Swine Model. Sensors. 2021; 21(11):3650. https://doi.org/10.3390/s21113650
Chicago/Turabian StyleKim, Heejin, Ki Hong Kim, Ki Jeong Hong, Yunseo Ku, Sang Do Shin, and Hee Chan Kim. 2021. "EEG-Based Prediction of the Recovery of Carotid Blood Flow during Cardiopulmonary Resuscitation in a Swine Model" Sensors 21, no. 11: 3650. https://doi.org/10.3390/s21113650
APA StyleKim, H., Kim, K. H., Hong, K. J., Ku, Y., Shin, S. D., & Kim, H. C. (2021). EEG-Based Prediction of the Recovery of Carotid Blood Flow during Cardiopulmonary Resuscitation in a Swine Model. Sensors, 21(11), 3650. https://doi.org/10.3390/s21113650