Effects of Whole-Body Electromyostimulation on Physical Fitness in Postmenopausal Women: A Randomized Controlled Trial

 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Experimental Approach
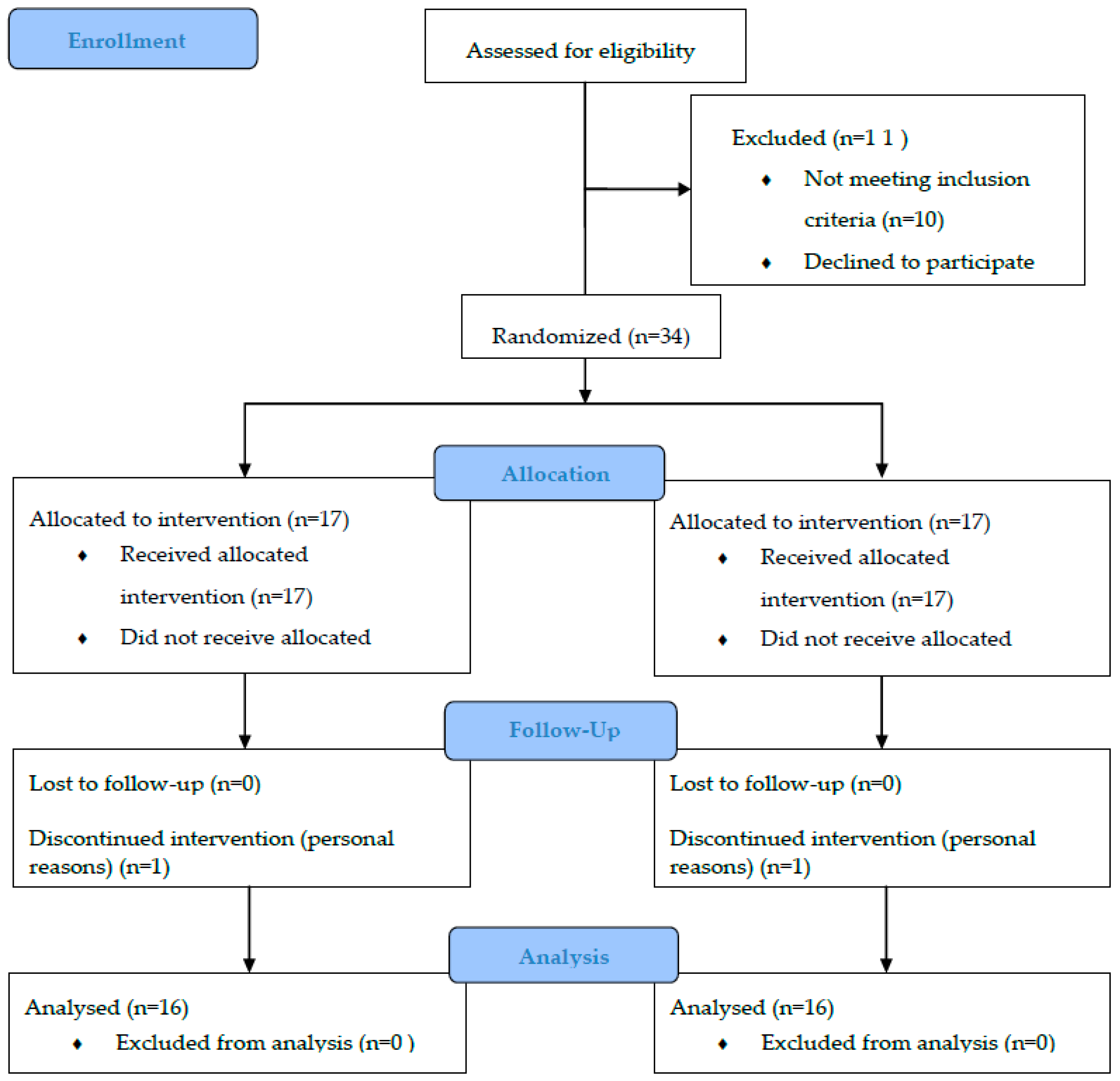
2.2. Participants
2.3. Menopause Status
2.4. Interventions
Harms
2.5. Patient and Public Involvement
2.6. Assessments
- Balance: “Flamingo test”. Participants started standing, with both feet on the ground. After the signal, they tried to stand on the sole of one foot. The time that the subject was able to stay in that posture up to a maximum of sixty seconds was recorded. The test was performed alternately, twice with each leg, and the best attempt of the four was registered.
- Leg strength: “Chair Stand Test”. The participant started from a sitting position with her arms crossed and the palms of her hands resting on her shoulders. The number of times she was able to get up and sit in 30 s was registered. The test was performed only once.
- Arm strength: “Arm Curl Test”. Participants sat on a bench holding 2.5 kg. The maximum number of elbow flexo-extension that the participant was able to execute in 30 s was registered. The test was performed once with each arm.
- Legs flexibility: “Chair Sit-and-Reach Test”. Participants began the test sitting, with one leg extended and the heel resting on the floor, while her hands were directed towards the toes of that leg. The existing distance, positive or negative, in centimeters, between the fingers and toes was measured. The test was performed once with each leg.
- Arms Flexibility: “Back Scratch Test”. The participant placed a hand over the shoulder of that same arm, and the opposite hand from the bottom up, trying to touch each other. The participant tried to touch or overlap the fingers of both hands. The distance in centimeters (positive or negative) between the fingertips of each hand was measured. The test was carried out twice, once with each arm.
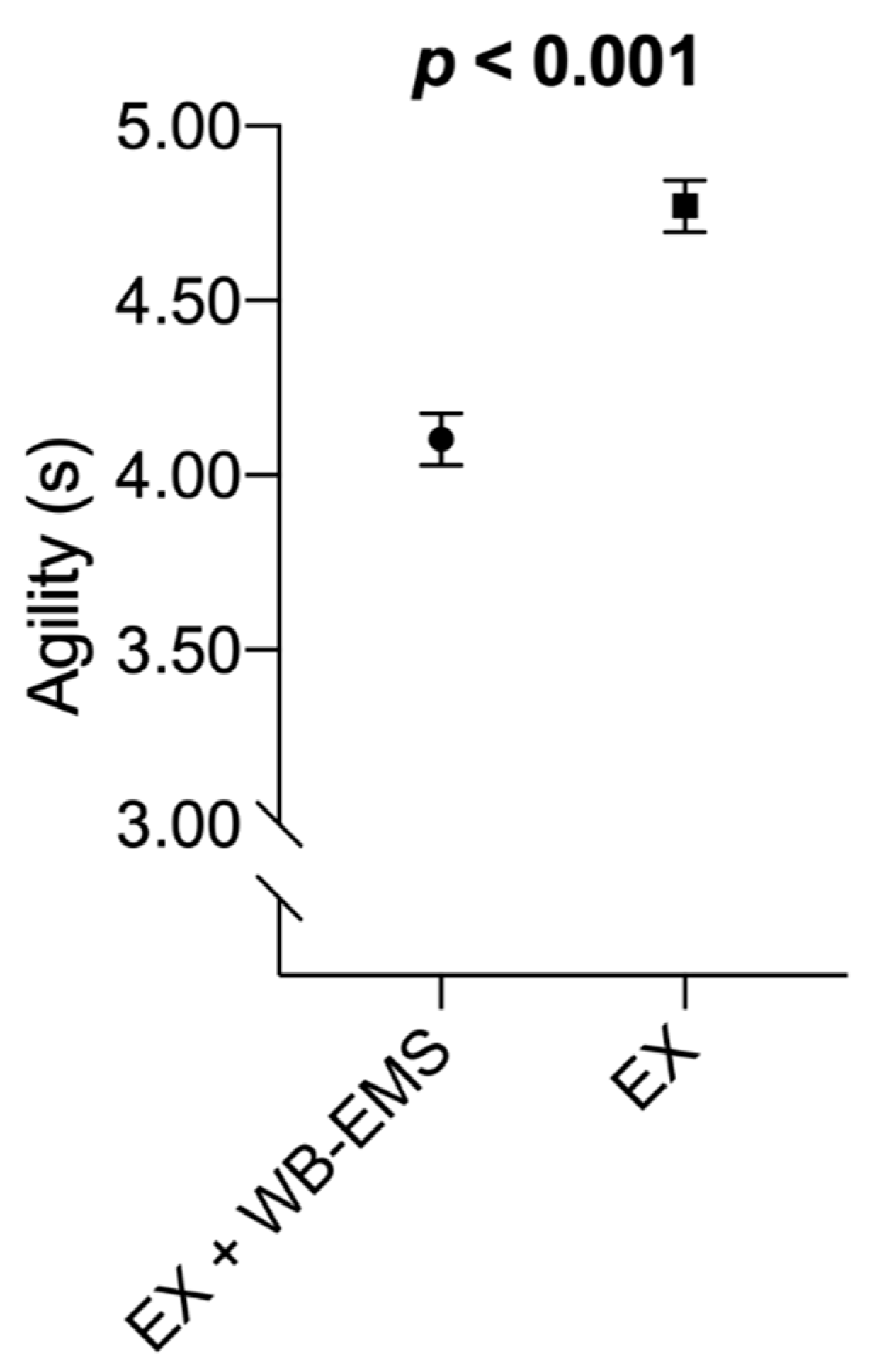
- Agility: “8-Foot Up-and-Go Test”. From a sitting position, the seconds that the participant took to get up, walk to a cone located 2.45 m, go around it, and sit down again were measured. The test was performed twice with at least one-minute rest between repetitions, and the best result was recorded.
- Speed: “Brisk Walking Test”. The time taken for each participant to walk 30 m was measured. Two repetitions were performed with a minute of rest between them. The best of both results was recorded.
- Cardiovascular resistance: “6-Minute Walk Test”. In a circuit of 46 m delineated by cones, the meters that each participant was able to cover walking for 6 min were registered.
2.7. Statistical Procedures
3. Results
- -
- Balance right leg
- -
- Balance left leg
- -
- Leg strength
- -
- Strength right arm
- -
- Strength left arm
- -
- Lower extremity flexibility
- -
- Upper extremity flexibility
- -
- Agility
- -
- Speed
- -
- Cardiovascular endurance
4. Discussion
4.1. Balance
4.2. Leg Strength
4.3. Arms Strength
4.4. Flexibility
4.5. Agility
4.6. Speed
4.7. Cardiovascular Endurance
4.8. Study Limitations
4.9. Practical Applications
4.10. Future Proposals
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kaushal, N.; Langlois, F.; Hagger, M.S.; Bherer, L. Investigating dose—Response effects of multimodal exercise programs on health-related quality of life in older adults. Clin. Interv. Aging 2019, 14, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C. Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1435–1445. [Google Scholar] [CrossRef] [PubMed]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K. The Physiology of Optimizing Health with a Focus on Exercise as Medicine. Annu. Rev. Physiol. 2019, 81, 607–627. [Google Scholar] [CrossRef]
- Orkaby, A.R.; Forman, D.E. Physical activity and CVD in older adults: An expert’s perspective. Expert Rev. Cardiovasc. Ther. 2018, 16, 1–10. [Google Scholar] [CrossRef]
- Bondarev, D.; Laakkonen, E.K.; Finni, T.; Kokko, K.; Kujala, U.M.; Aukee, P.; Kovanen, V.; Sipila, S. Physical performance in relation to menopause status and physical activity. Menopause 2018, 25, 1432–1441. [Google Scholar] [CrossRef]
- Abdulnour, J.; Doucet, E.; Brochu, M.; Lavoie, J.-M.; Strychar, I.; Rabasa-Lhoret, R.; Prud’homme, D. The effect of the menopausal transition on body composition and cardiometabolic risk factors: A Montreal-Ottawa New Emerging Team group study. Menopause 2012, 19, 760–767. [Google Scholar] [CrossRef]
- Guthrie, J.R.; Dennerstein, L.; Dudley, E.C. Weight gain and the menopause: A 5-year prospective study. Climacteric 1999, 2, 205–211. [Google Scholar] [CrossRef]
- Hodson, L.; Harnden, K.; Banerjee, R.; Real, B.; Marinou, K.; Karpe, F.; Fielding, B.A. Lower resting and total energy expenditure in postmenopausal compared with premenopausal women matched for abdominal obesity. J. Nutr. Sci. 2014, 3, e3. [Google Scholar] [CrossRef]
- Duval, K.; Prud’homme, D.; Rabasa-Lhoret, R.; Strychar, I.; Brochu, M.; Lavoie, J.-M.; Doucet, E. Effects of the menopausal transition on energy expenditure: A MONET Group Study. Eur. J. Clin. Nutr. 2013, 67, 407–411. [Google Scholar] [CrossRef]
- Lohne-Seiler, H.; Torstveit, M.K.; Anderssen, S.A. Training: Effects on Muscle Strength and Power in the Elderly. J. Aging Phys. Act. 2013, 21, 51–70. [Google Scholar] [CrossRef] [PubMed]
- Vechin, F.C.; Libardi, C.A.; Conceicao, M.S.; Damas, F.R.; Lixandrao, M.E.; Berton, R.P.B.; Tricoli, V.A.A.; Roschel, H.A.; Cavaglieri, C.R.; Chacon-Mikahil, M.P.T.; et al. Comparisons between low-intensity resistance training with blood flow restriction and high-intensity resistance training on quadriceps muscle mass and strength in elderly. J. Strength Cond. Res. 2015, 29, 1071–1076. [Google Scholar] [CrossRef] [PubMed]
- Narici, M.V.; Reeves, N.D.; Morse, C.I.; Maganaris, C.N. Muscular adaptations to resistance exercise in the elderly. J. Musculoskelet. Neuronal Interact. 2004, 4, 161–164. [Google Scholar] [PubMed]
- Rice, J.; Keogh, J.W.L. Power Training: Can it Improve Functional Performance in Older Adults? A Systematic Review. Int. J. Exerc. Sci. 2009, 2, 131–151. [Google Scholar]
- Park, J.; Han, D. Effects of high intensity aerobic exercise on treadmill on maximum-expiratory lung capacity of elderly women. J. Phys. Ther. Sci. 2017, 29, 1454–1457. [Google Scholar] [CrossRef]
- Osuka, Y.; Matsubara, M.; Hamasaki, A.; Hiramatsu, Y.; Ohshima, H.; Tanaka, K. Development of low-volume, high-intensity, aerobic-type interval training for elderly Japanese men: A feasibility study. Eur. Rev. Aging Phys. Act. 2017, 14, 1–8. [Google Scholar] [CrossRef]
- Li, K.; Fang, Y.; Zhou, Y.; Liu, H. Non-Invasive Stimulation-Based Tactile Sensation for Upper-Extremity Prosthesis: A Review. IEEE Sens. J. 2017, 17, 2625–2635. [Google Scholar] [CrossRef]
- Zhou, Y.; Fang, Y.; Gui, K.; Li, K.; Zhang, D.; Liu, H. SEMG Bias-Driven Functional Electrical Stimulation System for Upper-Limb Stroke Rehabilitation. IEEE Sens. J. 2018, 18, 6812–6821. [Google Scholar] [CrossRef]
- Filipovic, A.; Kleinoder, H.; Dormann, U.; Mester, J.; Klein Der, H.; Rmann, U.D.; Mester, J. Electromyostimulation—a Systematic Review of the Effects of Different Electromyostimulation Methods on Selected Strength Parameters in Trained and Elite Athletes. J. Strength Cond. Res. 2012, 26, 2600–2614. [Google Scholar] [CrossRef]
- Wiemspro—Electrostimulation for Fitness. Available online: https://wiemspro.com/?lang=es (accessed on 22 July 2019).
- Kemmler, W.; Teschler, M.; Weißenfels, A.; Bebenek, M.; Fröhlich, M.; Kohl, M.; von Stengel, S.; Weissenfels, A.; Bebenek, M.; Frohlich, M.; et al. Effects of whole-body electromyostimulation versus high-intensity resistance exercise on body composition and strength: A randomized controlled study. Evid.-Based Complement. Altern. Med. 2016, 2016, 9236809. [Google Scholar] [CrossRef]
- Schink, K.; Reljic, D.; Herrmann, H.J.; Meyer, J.; Mackensen, A.; Neurath, M.F.; Zopf, Y. Whole-Body Electromyostimulation Combined With Individualized Nutritional Support Improves Body Composition in Patients with Hematological Malignancies—A Pilot Study. Front. Physiol. 2018, 9, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Grimm, A.; Bebenek, M.; Kohl, M.; Von Stengel, S. Effects of Combined Whole-Body Electromyostimulation and Protein Supplementation on Local and Overall Muscle/Fat Distribution in Older Men with Sarcopenic Obesity: The Randomized Controlled Franconia Sarcopenic Obesity (FranSO) Study. Calcif. Tissue Int. 2018, 103, 266–277. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Bebenek, M.; Engelke, K.; von Stengel, S. Impact of whole-body electromyostimulation on body composition in elderly women at risk for sarcopenia: The Training and ElectroStimulation Trial (TEST-III). Age (Dordr.). 2014, 36, 395–406. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Schliffka, R.; Mayhew, J.L.; von Stengel, S. Effects of whole-body electromyostimulation on resting metabolic rate, body composition, and maximum strength in postmenopausal women: the Training and ElectroStimulation Trial. J. Strength Cond. Res. 2010, 24, 1880–1887. [Google Scholar] [CrossRef] [PubMed]
- von Stengel, S.; Bebenek, M.; Engelke, K.; Kemmler, W. Whole-body electromyostimulation to fight osteopenia in elderly females: The randomized controlled training and electrostimulation trial (TEST-III). J. Osteoporos. 2015, 2015, 643520. [Google Scholar] [CrossRef]
- Kemmler, W.; Teschler, M.; Weissenfels, A.; Bebenek, M.; von Stengel, S.; Kohl, M.; Freiberger, E.; Goisser, S.; Jakob, F.; Sieber, C.; et al. Whole-body electromyostimulation to fight sarcopenic obesity in community-dwelling older women at risk. Resultsof the randomized controlled FORMOsA-sarcopenic obesity study. Osteoporos. Int. 2016, 27, 3261–3270. [Google Scholar] [CrossRef]
- Schink, K.; Herrmann, H.J.; Schwappacher, R.; Meyer, J.; Orlemann, T.; Waldmann, E.; Wullich, B.; Kahlmeyer, A.; Fietkau, R.; Lubgan, D.; et al. Effects of whole-body electromyostimulation combined with individualized nutritional support on body composition in patients with advanced cancer: a controlled pilot trial. BMC Cancer 2018, 18, 886. [Google Scholar] [CrossRef]
- Kemmler, W.; Weissenfels, A.; Teschler, M.; Willert, S.; Bebenek, M.; Shojaa, M.; Kohl, M.; Freiberger, E.; Sieber, C.; von Stengel, S. Whole-body electromyostimulation and protein supplementation favorably affect sarcopenic obesity in community-dwelling older men at risk: The randomized controlled FranSO study. Clin. Interv. Aging 2017, 12, 1503–1513. [Google Scholar] [CrossRef]
- Amaro-Gahete, F.J.; De-la-O, A.; Sanchez-Delgado, G.; Robles-Gonzalez, L.; Jurado-Fasoli, L.; Ruiz, J.R.; Gutierrez, A. Functional Exercise Training and Undulating Periodization Enhances the Effect of Whole-Body Electromyostimulation Training on Running Performance. Front. Physiol. 2018, 9, 720. [Google Scholar] [CrossRef]
- Von Stengel, S.; Kemmler, W. Trainability of leg strength by whole-body electromyostimulation during adult lifespan: A study with male cohorts. Clin. Interv. Aging 2018, 13, 2495–2502. [Google Scholar] [CrossRef]
- Muñoz-arribas, A.; Mata, E.; Pedrero-chamizo, R.; Espino, L.; Gusi, N.; Villa, G.; Gonzalez-gross, M.; Casajús, J.A.; Ara, I.; Gómez-cabello, A. Obesidad sarcopénica y condición física en octogenarios; proyecto multicéntrico EXERNET. Nutr. Hosp. 2013, 28, 1877–1883. [Google Scholar] [PubMed]
- Schulz, K.F.; Altman, U.G.; Moher, D. CONSORT 2010 Statement. Obstet. Gynecol. 2010, 115, 1063–1070. [Google Scholar] [CrossRef] [PubMed]
- Moniker Privacy Services Random Team Generator—Split a List into Random Groups. Available online: https://www.randomlists.com/team-generator (accessed on 26 November 2019).
- Sjöström, M.; Oja, P.; Hagströmer, M.; Smith, B.J.; Bauman, A. Health-enhancing physical activity across European Union countries: The Eurobarometer study. J. Public Health (Bangkok) 2006, 14, 291–300. [Google Scholar] [CrossRef]
- Kovanen, V.; Aukee, P.; Kokko, K.; Finni, T.; Tarkka, I.M.; Tammelin, T.; Kujala, U.M.; Sipilä, S.; Laakkonen, E.K. Design and protocol of Estrogenic Regulation of Muscle Apoptosis (ERMA) study with 47 to 55-year-old women’s cohort: Novel results show menopause-related differences in blood count. Menopause 2018, 25, 1020–1032. [Google Scholar] [CrossRef] [PubMed]
- Aragão-Santos, J.C.; De Resende-Neto, A.G.; Nogueira, A.C.; Feitosa-Neta, M.D.L.; Brandão, L.H.A.; Chaves, L.M.D.S.; Da Silva-Grigoletto, M.E.; Feitosa-Neta, M.L. The effects of functional and traditional strength training on different strength parameters of elderly women: A randomized and controlled trial. J. Sports Med. Phys. Fit. 2019, 59, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Badillo, J.J.; Sanchez-Medina, L. Movement velocity as a measure of loading intensity in resistance training. Int. J. Sports Med. 2010, 31, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Wirtz, N.; Wahl, P.; Kleinöder, H.; Wechsler, K.; Achtzehn, S.; Mester, J. Acute metabolic, hormonal, and psychological responses to strength training with superimposed EMS at the beginning and the end of a 6 week training period. J. Musculoskelet. Neuronal Interact. 2015, 15, 325–332. [Google Scholar]
- Reed, J.L.; Pipe, A.L. The talk test: A useful tool for prescribing and monitoring exercise intensity. Curr. Opin. Cardiol. 2014, 29, 475–480. [Google Scholar] [CrossRef]
- Borg, G. Perceived exertion as an indicator of somatic stress. Scand. J. Rehabil. Med. 1970, 2, 92–98. [Google Scholar]
- Filipovic, A.; Klein Der, H.; Rmann, U.D.; Mester, J. Electromyostimulation—A Systematic Review of the Influence of Training Regimens and Stimulation Parameters on Effectiveness in Electromyostimulation Training of Selected Strength Parameters. J. Strength Cond. Res. 2011, 25, 3218–3238. [Google Scholar] [CrossRef]
- Doucet, B.M.; Lam, A.; Griffin, L. Neuromuscular electrical stimulation for skeletal muscle function. Yale J. Biol. Med. 2012, 85, 201–215. [Google Scholar] [PubMed]
- A Guide to the Use of Electrical Stimulation in Pediatric Nurodisbility. Association of Paediatric Chartered Physiotherapists. Available online: https://apcp.csp.org.uk/content/guide-use-electrical-stimulation-paedaitric-neurodisability (accessed on 19 December 2019).
- Deley, G.; Babault, N. Could low-frequency electromyostimulation training be an effective alternative to endurance training? An overview in one adult. J. Sport. Sci. Med. 2014, 13, 444–450. [Google Scholar]
- Petrofsky, J. The effect of the subcutaneous fat on the transfer of current through skin and into muscle. Med. Eng. Phys. 2008, 30, 1168–1176. [Google Scholar] [CrossRef] [PubMed]
- Sirola, J.; Rikkonen, T. Muscle performance after the menopause. J. Br. Menopause Soc. 2005, 11, 45–50. [Google Scholar] [CrossRef]
- Sagarra-Romero, L.; Vicente-Rodriguez, G.; Pedrero-Chamizo, R.; Vila-Maldonado, S.; Gusi, N.; Villa-Vicente, J.G.; Espino, L.; Gonzalez-Gross, M.; Casajus, J.A.; Ara, I.; et al. Is Sitting Time Related with Physical Fitness in Spanishelderly Population? The EXERNET Multicenter Study. J. Nutr. Health Aging 2019, 23, 401–407. [Google Scholar] [CrossRef]
- Vincent, W.J.; Weir, J.P. Statistics in Kinesiology; Human Kinetics: Champaign, IL, USA, 2012; ISBN 9781450402545. [Google Scholar]
- Field, A. Discovering Statistics Using IBM SPSS Statistics; SAGE Publications Ltd.: Thousand Oaks, CA, USA, 2017; ISBN 9781526419521. [Google Scholar]
- Orr, R.; Raymond, J.; Fiatarone Singh, M. Efficacy of progressive resistance training on balance performance in older adults: A systematic review of randomized controlled trials. Sports Med. 2008, 38, 317–343. [Google Scholar] [CrossRef]
- Marques, E.A.; Figueiredo, P.; Harris, T.B.; Wanderley, F.A.; Carvalho, J. Are resistance and aerobic exercise training equally effective at improving knee muscle strength and balance in older women? Arch. Gerontol. Geriatr. 2017, 68, 106–112. [Google Scholar] [CrossRef]
- Gonzalez, A.M.; Mangine, G.T.; Fragala, M.S.; Stout, J.R.; Beyer, K.S.; Bohner, J.D.; Emerson, N.S.; Hoffman, J.R. Resistance training improves single leg stance performance in older adults. Aging Clin. Exp. Res. 2014, 26, 89–92. [Google Scholar] [CrossRef]
- Joshua, A.M.; D’Souza, V.; Unnikrishnan, B.; Mithra, P.; Kamath, A.; Acharya, V.; Venugopal, A. Effectiveness of progressive resistance strength training versus traditional balance exercise in improving balance among the elderly - a randomised controlled trial. J. Clin. Diagn. Res. 2014, 8, 98–102. [Google Scholar] [CrossRef]
- Lustosa, L.P.; Silva, J.P.; Coelho, F.M.; Pereira, D.S.; Parentoni, A.N.; Pereira, L.S.M. Impact of resistance exercise program on functional capacity and muscular strength of knee extensor in pre-frail community-dwelling older women: A randomized crossover trial. Rev. Bras. Fisioter. 2011, 15, 318–324. [Google Scholar] [CrossRef]
- Kemmler, W.; von Stengel, S. Whole-body electromyostimulation as a means to impact muscle mass and abdominal body fat in lean, sedentary, older female adults: Subanalysis of the TEST-III trial. Clin. Interv. Aging 2013, 8, 1353–1364. [Google Scholar] [CrossRef] [PubMed]
- Pano-Rodriguez, A.; Beltran-Garrido, J.V.; Hernandez-Gonzalez, V.; Reverter-Masia, J. Effects of whole-body electromyostimulation on health and performance: A systematic review. BMC Complement. Altern. Med. 2019, 19, 87. [Google Scholar] [CrossRef] [PubMed]
- Asikainen, T.-M.; Kukkonen-Harjula, K.; Miilunpalo, S. Exercise for health for early postmenopausal women: a systematic review of randomised controlled trials. Sports Med. 2004, 34, 753–778. [Google Scholar] [CrossRef] [PubMed]
- Pollanen, E.; Sipila, S.; Alen, M.; Ronkainen, P.H.A.; Ankarberg-Lindgren, C.; Puolakka, J.; Suominen, H.; Hamalainen, E.; Turpeinen, U.; Konttinen, Y.T.; et al. Differential influence of peripheral and systemic sex steroids on skeletal muscle quality in pre- and postmenopausal women. Aging Cell 2011, 10, 650–660. [Google Scholar] [CrossRef] [PubMed]
- Perez-Bellmunt, A.; Casasayas, O.; Navarro, R.; Simon, M.; Martin, J.C.; Perez-Corbella, C.; Blasi, M.; Ortiz, S.; Alvarez, P.; Pacheco, L. Effectiveness of low-frequency electrical stimulation in proprioceptive neuromuscular facilitation techniques in healthy males: a randomized controlled trial. J. Sports Med. Phys. Fitness 2019, 59, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Filipovic, A.; Grau, M.; Kleinoeder, H.; Zimmer, P.; Hollmann, W.; Bloch, W. Effects of a Whole-Body Electrostimulation Program on Strength, Sprinting, Jumping, and Kicking Capacity in Elite Soccer Players. J. Sport. Sci. Med. 2016, 15, 639–648. [Google Scholar]
- Roth, G.A.; Forouzanfar, M.H.; Moran, A.E.; Barber, R.; Nguyen, G.; Feigin, V.L.; Naghavi, M.; Mensah, G.A.; Murray, C.J.L. Demographic and epidemiologic drivers of global cardiovascular mortality. N. Engl. J. Med. 2015, 372, 1333–1341. [Google Scholar] [CrossRef]
- Filipovic, A.; Kleinoder, H.; Pluck, D.; Hollmann, W.; Bloch, W.; Grau, M. Influence of Whole-Body Electrostimulation on Human Red Blood Cell Deformability. J. Strength Cond. Res. 2015, 29, 2570–2578. [Google Scholar] [CrossRef]
- Amaro-Gahete, F.J.; De-la-O, A.; Sanchez-Delgado, G.; Robles-Gonzalez, L.; Jurado-Fasoli, L.; Ruiz, J.R. Whole-Body Electromyostimulation Improves Performance-Related Parameters in Runners. Front. Physiol. 2018, 9, 1576. [Google Scholar] [CrossRef]
- Makar, O.; Siabrenko, G. Influence of physical activity on cardiovascular system and prevention of cardiovascular diseases (review). Georgian Med. News 2018, 285, 69–74. [Google Scholar]
- Morton, R.W.; Murphy, K.T.; Mckellar, S.R.; Schoenfeld, B.J.; Henselmans, M.; Helms, E.; Aragon, A.A.; Devries, M.C.; Banfield, L.; Krieger, J.W.; et al. A systematic review, meta-analysis and meta- regression of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength in healthy adults. Br. J. Sports Med. 2018, 52, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Chung, P.-K. Differences in Functional Fitness Among Older Adults with and Without Risk of Falling. Asian Nurs. Res. (Korean. Soc. Nurs. Sci). 2016, 10, 51–55. [Google Scholar] [CrossRef] [PubMed][Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 34) | EX + WB-EMS (n = 17) | EX (n = 17) | p-Value |
|---|---|---|---|---|
| Age (years) | 61.4 ± 4.0 | 63.1 ± 3,42 | 59.7 ± 3,82 | 0.011 |
| Body mass (kg) | 67.4 ± 10.8 | 67.7 ± 10.1 | 67.1 ± 10,8 | 0.866 |
| Height (cm) | 158.3 ± 5.3 | 159.9 ± 5.2 | 156.7 ± 5.0 | 0.614 |
| Body mass index (BMI, kg/m2) | 29.9 ± 4.1 | 26.5 ± 4.1 | 27.3 ± 4.2 | 0.220 |
| Outcome | Group | Pre | Post | Estimated Mean Difference [95% CI] | p (Time) | p (Group*time) |
|---|---|---|---|---|---|---|
| Balance right leg (s) | All | 47.82 ± 19.12 | 49.86 ± 18.07 | 2.05 [−4.82, 8.91] | 0.547 | 0.549 |
| EX + WB-EMS | 41.96 ± 19.49 | 41.87 ± 21.47 | 0.01 [−13.42, 13.43] | |||
| EX | 53.67 ± 17.39 | 57.75 ± 9.00 | 4.08 [−9.35, 17.51] | |||
| Balance left leg (s) | All | 44.12 ± 20.86 | 49.32 ± 17.60 | 5.22 [−2.58, 13.01] | 0.182 | 0.715 |
| EX + WB-EMS | 34.96 ± 22.94 | 41.59 ± 19.33 | 6.62 −8.62, 21.87] | |||
| EX | 53.24 ± 13.95 | 57.03 ± 11.79 | 3.81 [−11.44, 19.05] | |||
| Leg strength (reps.) | All | 13.66 ± 2.03 | 20.72 ± 4.88 | 7.06 [5.77, 8.34] | <0.001 | 0.016 |
| EX + WB-EMS | 13.50 ± 1.83 | 22.19 ± 4.79 | 8.68 [6.16, 11.22] | |||
| EX | 13.81 ± 2.26 | 19.25 ± 4.66 | 5.44 [2.91, 7.97] | |||
| Outcome | Group | Pre | Post | Estimated mean Difference [95% CI] | p (Time) | p (Group*time) |
| Strength right arm (reps.) | All | 15.53 ± 2.57 | 20.84 ± 2.65 | 5.32 [4.24, 6.38] | <0.001 | 0.031 |
| EX + WB-EMS | 14.81 ± 2.26 | 21.31 ± 3.05 | 6.50 [4.41, 8.59] | |||
| EX | 16.25 ± 2.72 | 20.38 ± 2.19 | 4.13 [2.03, 6.22] | |||
| Strength left arm (reps.) | All | 15.78 ± 2.46 | 21.25 ± 2.89 | 5.47 [4.58, 6.36] | <0.001 | 0.018 |
| EX + WB-EMS | 15.06 ± 1.73 | 21.63 ± 3.07 | 6.56 [4.82, 8.31] | |||
| EX | 16.50 ± 2.90 | 20.88 ± 2.73 | 4.38 [2.63, 6.12] | |||
| LE flexibility (cm) | All | −0.34 ± 7.45 | 1.94 ± 5.65 | 2.28 [0.70, 3.87] | 0.006 | 0.452 |
| EX + WB-EMS | −0.13 ± 5.61 | 2.75 ± 4.27 | 2.88 [−0.24, 5.99] | |||
| EX | −0.56 ± 9.12 | 1.13 ± 6.81 | 1.69 [−1.43, 4.80] | |||
| UE flexibility (cm) | All | 0.59 ± 5.99 | 2.20 ± 6.20 | 1.61 [−0.18, 3.40] | 0.076 | 0.818 |
| EX + WB-EMS | 0.62 ± 7.21 | 2.03 ± 7.51 | 1.41 [−2.09, 4.90] | |||
| EX | 0.56 ± 4.73 | 2.38 ± 4.79 | 1.81 [−1.68, 5.31] | |||
| Agility (s) | All | 5.16 ± 0.74 | 4.44 ± 0.46 | −0.72 [−0.88, −0.56] | <0.001 | <0.001 |
| EX + WB-EMS | 5.48 ± 0.73# | 4.26 ± 0.35 | −1.22 [−1.54, −0.90] | |||
| EX | 4.84 ± 0.62 | 4.62 ± 0.48 | −0.22 [−0.54, 0.10] | |||
| 30 m walk speed (s) | All | 14.08 ± 1.97 | 12.50 ± 1.49 | −1.58 [−1.92, −1.24] | <0.001 | 0.028 |
| EX + WB-EMS | 14.80 ± 1.89 | 12.85 ± 1.13 | −1.96 [−2.62, −1.30] | |||
| EX | 13.36 ± 1.83 | 12.16 ± 1.76 | −1.20 [−1.85, −0.54] | |||
| 6 min walk test (m) | All | 567.90 ± 57.32 | 658.50 ± 82.74 | 90.60 [73.96, 107.24] | <0.001 | <0.001 |
| EX + WB-EMS | 561.78 ± 54.58 | 717.31 ± 59.91 # | 155.54 [122.99, 188.08] | |||
| EX | 574.03 ± 61.09 | 599.69 ± 56.41 | 25.66 [−6.88, 58.21] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pano-Rodriguez, A.; Beltran-Garrido, J.V.; Hernandez-Gonzalez, V.; Reverter-Masia, J. Effects of Whole-Body Electromyostimulation on Physical Fitness in Postmenopausal Women: A Randomized Controlled Trial. Sensors 2020, 20, 1482. https://doi.org/10.3390/s20051482
Pano-Rodriguez A, Beltran-Garrido JV, Hernandez-Gonzalez V, Reverter-Masia J. Effects of Whole-Body Electromyostimulation on Physical Fitness in Postmenopausal Women: A Randomized Controlled Trial. Sensors. 2020; 20(5):1482. https://doi.org/10.3390/s20051482
Chicago/Turabian StylePano-Rodriguez, Alvaro, Jose Vicente Beltran-Garrido, Vicenç Hernandez-Gonzalez, and Joaquín Reverter-Masia. 2020. "Effects of Whole-Body Electromyostimulation on Physical Fitness in Postmenopausal Women: A Randomized Controlled Trial" Sensors 20, no. 5: 1482. https://doi.org/10.3390/s20051482
APA StylePano-Rodriguez, A., Beltran-Garrido, J. V., Hernandez-Gonzalez, V., & Reverter-Masia, J. (2020). Effects of Whole-Body Electromyostimulation on Physical Fitness in Postmenopausal Women: A Randomized Controlled Trial. Sensors, 20(5), 1482. https://doi.org/10.3390/s20051482