Effect of a Concurrent Cognitive Task, with Stabilizing Visual Information and Withdrawal, on Body Sway Adaptation of Parkinsonian’s Patients in an Off-Medication State: A Controlled Study

 ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Experiments
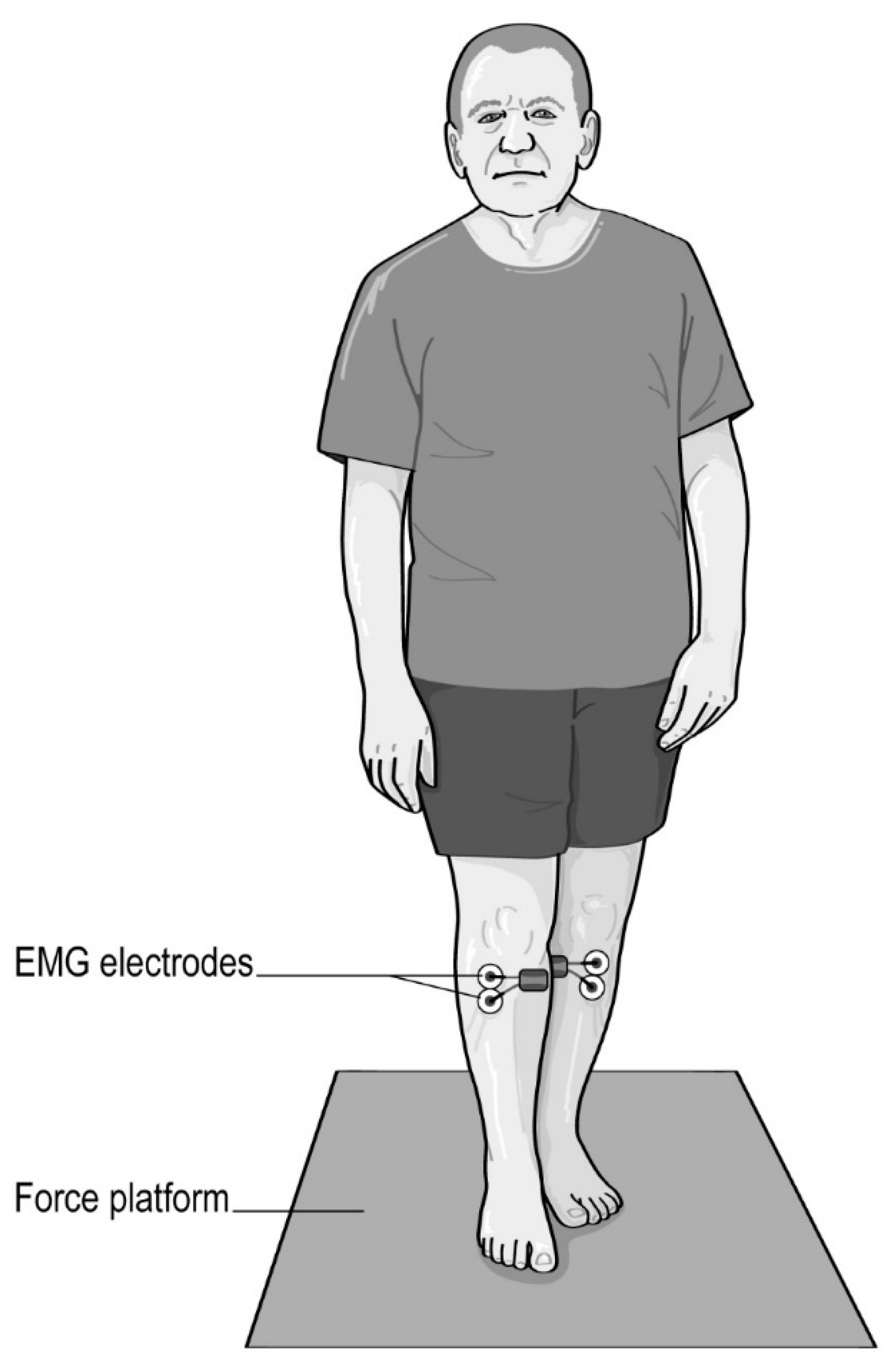
2.3. Instrumentation and Signal Analyses
2.4. Statistical Comparisons
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Ethical Statement
References
- Xia, R.; Mao, Z.-H. Progression of motor symptoms in Parkinson’s disease. Neurosci. Bull. 2012, 28, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Kamieniarz, A.; Michalska, J.; Brachman, A.; Pawłowski, M.; Słomka, K.J.; Juras, G. A posturographic procedure assessing balance disorders in Parkinson’s disease: A systematic review. Clin. Interv. Aging 2018, 13, 2301–2316. [Google Scholar] [CrossRef] [PubMed]
- Markovic, G.; Mikulic, P.; Kern, H.; Sarabon, N. Intra-session reliability of traditional and nonlinear time-series posturographic measures in a semi-tandem stance: A reference to age. Measurement 2014, 51, 124–132. [Google Scholar] [CrossRef]
- Geurts, A.C.H.; Boonstra, T.A.; Voermans, N.C.; Diender, M.G.; Weerdesteyn, V.; Bloem, B.R. Assessment of postural asymmetry in mild to moderate Parkinson’s disease. Gait Posture 2011, 33, 143–145. [Google Scholar] [CrossRef]
- Djaldetti, R.; Ziv, I.; Melamed, E. The mystery of motor asymmetry in Parkinson’s disease. Lancet Neurol. 2006, 5, 796–802. [Google Scholar] [CrossRef]
- Błaszczyk, J.W.; Orawiec, R.; Duda-Kłodowska, D.; Opala, G. Assessment of postural instability in patients with Parkinson’s disease. Exp. Brain Res. 2007, 183, 107–114. [Google Scholar] [CrossRef]
- Marchese, R.; Bove, M.; Abbruzzese, G. Effect of cognitive and motor tasks on postural stability in Parkinson’s disease: A posturographic study. Mov. Disord. Off. J. Mov. Disord. Soc. 2003, 18, 652–658. [Google Scholar] [CrossRef]
- Barbosa, A.F.; de Souza, C.O.; Chen, J.; Francato, D.V.; Caromano, F.A.; Chien, H.F.; Barbosa, E.R.; Greve, J.M.D.; Voos, M.C. The competition with a concurrent cognitive task affects posturographic measures in patients with Parkinson disease. Arq. Neuropsiquiatr. 2015, 73, 906–912. [Google Scholar] [CrossRef]
- Lacour, M.; Bernard-Demanze, L.; Dumitrescu, M. Posture control, aging, and attention resources: Models and posture-analysis methods. Neurophysiol. Clin. Clin. Neurophysiol. 2008, 38, 411–421. [Google Scholar] [CrossRef]
- Fernandes, Â.; Coelho, T.; Vitória, A.; Ferreira, A.; Santos, R.; Rocha, N.; Fernandes, L.; Tavares, J.M.R.S. Standing balance in individuals with Parkinson’s disease during single and dual-task conditions. Gait Posture 2015, 42, 323–328. [Google Scholar] [CrossRef]
- Holmes, J.D.; Jenkins, M.E.; Johnson, A.M.; Adams, S.G.; Spaulding, S.J. Dual-task interference: The effects of verbal cognitive tasks on upright postural stability in Parkinson’s disease. Park. Dis. 2010. [Google Scholar] [CrossRef] [PubMed]
- Rocchi, L.; Chiari, L.; Horak, F.B. Effects of deep brain stimulation and levodopa on postural sway in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2002, 73, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Beuter, A.; Hernández, R.; Rigal, R.; Modolo, J.; Blanchet, P.J. Postural sway and effect of levodopa in early Parkinson’s disease. Can. J. Neurol. Sci. 2008, 35, 65–68. [Google Scholar] [CrossRef]
- Curtze, C.; Nutt, J.G.; Carlson-Kuhta, P.; Mancini, M.; Horak, F.B. Levodopa is a double-edged sword for balance and gait in people with Parkinson’s disease. Mov. Dis. 2015, 30, 1361–1370. [Google Scholar] [CrossRef] [PubMed]
- Lang, K.C.; Hackney, M.E.; Ting, L.H.; McKay, J.L. Antagonist muscle activity during reactive balance responses is elevated in Parkinson’s disease and in balance impairment. PLoS ONE 2019, 14, e0211137. [Google Scholar] [CrossRef] [PubMed]
- Defer, G.L.; Widner, H.; Marié, R.M.; Rémy, P.; Levivier, M. Core assessment program for surgical interventional therapies in Parkinson’s disease (CAPSIT-PD). Mov. Disord. Off. J. Mov. Disord. Soc. 1999, 14, 572–584. [Google Scholar] [CrossRef]
- Caliandro, P.; Ferrarin, M.; Cioni, M.; Bentivoglio, A.R.; Minciotti, I.; D’Urso, P.I.; Tonali, P.A.; Padua, L. Levodopa effect on electromyographic activation patterns of tibialis anterior muscle during walking in Parkinson’s disease. Gait Posture 2011, 33, 436–441. [Google Scholar] [CrossRef]
- Saffer, M.; Kiemel, T.; Jeka, J. Coherence analysis of muscle activity during quiet stance. Exp. Brain. Res. 2008, 185, 215–226. [Google Scholar] [CrossRef]
- Hughes, A.J.; Ben-Shlomo, Y.; Daniel, S.E.; Lees, A.J. What features improve the accuracy of clinical diagnosis in Parkinson’s disease: A clinicopathologic study. Neurology 1992, 42, 1142–1146. [Google Scholar] [CrossRef]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism: Onset, progression and mortality. Neurology 1967, 17, 427–442. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel, R.; et al. Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale presentation and clinimetric testing results. Mov. Disord. 2008, 23, 2129–2170. [Google Scholar] [CrossRef] [PubMed]
- Chomiak, T.; Pereira, F.V.; Hu, B. The single-leg-stance test in Parkinson’s disease. J. Clin. Med. Res. 2015, 7, 182–185. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, H.; Allard, P.; Prince, F.; Labelle, H. Symmetry and limb dominance in able-bodied gait: A review. Gait Posture 2000, 12, 34–45. [Google Scholar] [CrossRef]
- Bonnet, C.T. Advantages and disadvantages of stiffness instructions when studying postural control. Gait Posture 2016, 46, 208–210. [Google Scholar] [CrossRef]
- Hansen, C.; Wei, Q.; Shieh, J.-S.; Fourcade, P.; Isableu, B.; Majed, L. Sample Entropy, Univariate, and Multivariate Multi-Scale Entropy in Comparison with Classical Postural Sway Parameters in Young Healthy Adults. Front. Hum. Neurosci. 2017, 11, 206. [Google Scholar] [CrossRef]
- Honeine, J.-L.; Crisafulli, O.; Schieppati, M. Body sway adaptation to addition but not withdrawal of stabilizing visual information is delayed by a concurrent cognitive task. J. Neurophysiol. 2017, 117, 777–785. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- Dault, M.C.; Yardley, L.; Frank, J.S. Does articulation contribute to modifications of postural control during dual-task paradigms? Cogn. Brain Res. 2003, 16, 434–440. [Google Scholar] [CrossRef]
- Torres-Oviedo, G.; Ting, L.H. Muscle synergies characterizing human postural responses. J. Neurophysiol. 2007, 98, 2144–2156. [Google Scholar] [CrossRef]
- Schieppati, M.; Hugon, M.; Grasso, M.; Nardone, A.; Galante, M. The limits of equilibrium in young and elderly normal subjects and in parkinsonians. Electroencephalogr. Clin. Neurophysiol. 1994, 93, 286–298. [Google Scholar] [CrossRef]
- Terra, M.B.; Rosa, P.C.; Torrecilha, L.A.; Costa, B.T.; Ferraz, H.B.; Santos, S.M.S. Impacto da doença de Parkinson na performance do equilíbrio em diferentes demandas atencionais. Fisioter. E Pesqui. 2016, 23, 410–415. [Google Scholar] [CrossRef]
- Rinalduzzi, S.; Trompetto, C.; Marinelli, L.; Alibardi, A.; Missori, P.; Fattapposta, F.; Pierelli, F.; Currà, A. Balance dysfunction in Parkinson’s disease. BioMed. Res. Int. 2015. [Google Scholar] [CrossRef] [PubMed]
- Vuillerme, N.; Nafati, G. How attentional focus on body sway affects postural control during quiet standing. Psychol. Res. 2007, 71, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Barbieri, F.A.; Polastri, P.F.; Baptista, A.M.; Lirani-Silva, E.; Simieli, L.; Orcioli-Silva, D.; Beretta, V.S.; Gobbi, L.T.B. Effects of disease severity and medication state on postural control asymmetry during challenging postural tasks in individuals with Parkinson’s disease. Hum. Mov. Sci. 2016, 46, 96–103. [Google Scholar] [CrossRef]
- Beretta, V.S.; Barbieri, F.A.; Orcioli-Silva, D.; Dos Santos, P.C.R.; Simieli, L.; Vitório, R.; Gobbi, L.T.B. Can Postural Control Asymmetry Predict Falls in People With Parkinson’s Disease? Motor Control 2018, 22, 449–461. [Google Scholar] [CrossRef]
- Rochester, L.; Galna, B.; Lord, S.; Burn, D. The nature of dual-task interference during gait in incident Parkinson’s disease. Neuroscience 2014, 265, 83–94. [Google Scholar] [CrossRef]
- Nieuwhof, F.; Bloem, B.R.; Reelick, M.F.; Aarts, E.; Maidan, I.; Mirelman, A.; Hausdorff, J.M.; Toni, I.; Helmich, R.C. Impaired dual tasking in Parkinson’s disease is associated with reduced focusing of cortico-striatal activity. Brain 2017, 140, 1384–1398. [Google Scholar] [CrossRef]
- Jazaeri, S.Z.; Azad, A.; Mehdizadeh, H.; Habibi, S.A.; Najafabadi, M.M.; Saberi, Z.S.; Rahimzadegan, H.; Moradi, S.; Behzadipour, S.; Parnianpour, M.; et al. The effects of anxiety and external attentional focus on postural control in patients with Parkinson’s disease. PLoS ONE 2018, 13, e0192168. [Google Scholar] [CrossRef]
- Piccoli, A.; Rossettini, G.; Cecchetto, S.; Viceconti, A.; Ristori, D.; Turolla, A.; Maselli, F.; Testa, M. Effect of Attentional Focus Instructions on Motor Learning and Performance of Patients with Central Nervous System and Musculoskeletal Disorders: A Systematic Review. J. Funct. Morphol. Kinesiol. 2018, 3, 40. [Google Scholar] [CrossRef]
- Wulf, G.; Landers, M.; Lewthwaite, R.; Töllner, T. External focus instructions reduce postural instability in individuals with Parkinson disease. Phys. Ther. 2009, 89, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Bargh, J.A.; Chartrand, T.L. The unbearable automaticity of being. Am. Psychol. 1999, 54, 462–479. [Google Scholar] [CrossRef]
- Workman, C.D.; Thrasher, T.A. The influence of dopaminergic medication on balance automaticity in Parkinson’s disease. Gait Posture 2019, 70, 98–103. [Google Scholar] [CrossRef]
- Beauchet, O.; Berrut, G. Gait and dual-task: Definition, interest, and perspectives in the elderly. Psychol. Neuropsychiatr. Vieil. 2006, 4, 215–225. [Google Scholar]
- Ruthruff, E.; Pashler, H.E.; Klaassen, A. Processing bottlenecks in dual-task performance: Structural limitation or strategic postponement? Psychon. Bull. Rev. 2001, 8, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Vette, A.H.; Sayenko, D.G.; Jones, M.; Abe, M.O.; Nakazawa, K.; Masani, K. Ankle muscle co-contractions during quiet standing are associated with decreased postural steadiness in the elderly. Gait Posture 2017, 55, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Nagai, K.; Yamada, M.; Mori, S.; Tanaka, B.; Uemura, K.; Aoyama, T.; Ichihashi, N.; Tsuboyama, T. Effect of the muscle coactivation during quiet standing on dynamic postural control in older adults. Arch. Gerontol. Geriatr. 2013, 56, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Honeine, J.-L.; Schieppati, M.; Gagey, O.; Do, M.-C. By counteracting gravity, triceps surae sets both kinematics and kinetics of gait. Physiol. Rep. 2014, 2, e00229. [Google Scholar] [CrossRef]
- Prieto Guerrero, A.; Espinosa Paredes, G. Linear and Non-Linear Stability Analysis in Boiling Water Reactors, 1st ed.; Woodhead Publishing: Duxford, UK, 2018; ISBN 978-0-08-102445-4. [Google Scholar]
- Stins, J.F.; Michielsen, M.E.; Roerdink, M.; Beek, P.J. Sway regularity reflects attentional involvement in postural control: Effects of expertise, vision and cognition. Gait Posture 2009, 30, 106–109. [Google Scholar] [CrossRef]
- Schniepp, R.; Wuehr, M.; Pradhan, C.; Novozhilov, S.; Krafczyk, S.; Brandt, T.; Jahn, K. Nonlinear variability of body sway in patients with phobic postural vertigo. Front. Neurol. 2013, 4, 115. [Google Scholar] [CrossRef]
- Dijkstra, B.W.; Bekkers, E.; Gilat, M.; de Rond, V.; Hardwick, R.M.; Nieuwboer, A. Functional neuroimaging of human postural control: A systematic review with meta-analysis. Neurosci. Biobehav. Rev. 2020, 115, 351–362. [Google Scholar] [CrossRef] [PubMed]
- Plummer, P.; Eskes, G. Measuring treatment effects on dual-task performance: A framework for research and clinical practice. Front. Hum. Neurosci. 2015, 9, 225. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patients with PD Mean (SD) [CI 95%] | Control Group Mean (SD) [CI 95%] | Between-Group Comparison p-Value | |
|---|---|---|---|
| Individuals (n) | 15 | 15 | |
| Age (years) | 67.7 (7.3) [63.6–71.7] | 24.9 (4.9) [22.1–27.6] | p < 0.01 |
| Height (m) | 1.67 (0.08) [1.62–1.71] | 1.77 (8.4) [1.72–1.82] | p < 0.01 |
| Weight (kg) | 67.8 (15.8) [59.1–76.5] | 69.8 (12.2) [63.0–76.5] | p > 0.05 |
| Body Mass Index (kg/m2) | 24.0 (3.8) [22.0–26.1] | 22.2 (2.4) [20.8–23.5] | p > 0.05 |
| Gender (F/M) | 9/6 | 7/8 | p > 0.05 |
| Dominant leg (L/R) | 3/12 | 2/13 | p > 0.05 |
| UPDRS motor examination | 24.5 (10.1) [18.9–30.0] | - | |
| UPDRS III Speech (item 3.1) | 0 (0) | - | |
| Sit-to-Stand in 15 s (n) | 8.1 (1.8) [7.1–9.1] | - | |
| Mini-Mental State Examination | 29.1 (1.5) [28.2–29.9] | - | |
| Berg Balance Scale (BBS) | 55.1 (2.1) [53. 9–56.2] | - | |
| Points in first 9 items of BBS (points) Disease Durations (years) | 36 (0) [36–36] 5.4 (3.4) [3.5–7.3] | - - | |
| Hoehn & Yahr Scale | 2 (0) | - |
| Eyes Open Single-Task | Eyes Open Dual-Task | Eyes Closed Single-Task | Eyes Closed Dual-Task | |
|---|---|---|---|---|
| COP Pathway (mm) | 1606 [933–2280] | 2105 [930–3279] | 2546 [1954–3139] *§ | 2874 [1745–4002] *§ |
| Ellipse Area 95% (mm2) | 101 [67–134] | 159 [84–234] | 283 [181–384] *§ | 296 [190–403] *§ |
| RMS ML (mm) | 3.7 [2.9–4.4] | 4.3 [3.2–5.5] | 6.5 [5.2–7.7] *§ | 6.2 [5.2–7.3] *§ |
| RMS AP (mm) | 1.4 [1.1–1.7] | 1.9 [1.2–2.5] | 2.5 [2.0–2.9] *§ | 2.5 [1.9–3.2] *§ |
| MeanFreq ML (Hz) | 0.011 [0.009–0.012] | 0.011 [0.009–0.012] | 0.010 [0.010–0.011] | 0.011 [0.009–0.012] |
| MedianFreq ML (Hz) | 0.018 [0.015–0.021] | 0.018 [0.015–0.021] | 0.017 [0.016–0.018] | 0.018 [0.015–0.021] |
| Mean Freq AP (Hz) | 0.010 [0.009–0.012] | 0.011 [0.009–0.012] | 0.010 [0.010–0.011] | 0.011 [0.009–0.012] |
| MedianFreq AP (Hz) | 0.018 [0.015–0.021] | 0.018 [0.015–0.021] | 0.017 [0.016–0.018] | 0.018 [0.015–0.021] |
| SampEn ML | 1.25 [1.23–1.27] | 1.24 [1.21–1.27] | 1.25 [1.23–1.27] | 1.25 [1.23–1.27] |
| SampEn AP | 1.26 [1.23–1.28] | 1.25 [1.22–1.28] | 1.26 [1.24–1.28] | 1.26 [1.24–1.29] |
| MSE ML | 6.05 [5.24–6.87] | 6.39 [5.31–7.46] * | 6.09 [5.35–6.83] * | 6.33 [5.42–7.24] * |
| MSE AP | 6.91 [6.03–7.79] | 7.28 [6.27–8.28] | 6.96 [6.06–7.86] * | 7.10 [6.12–8.07] * |
| MMSE | 20.52 (18.47–22.57] | 20.26 [18.12–22.41] | 20.95 [18.81–23.10] | 21.17 [19.17–23.17] |
| RMS Soleus-Forward (mV) | 955 [356–1284] | 998 [370–1267] | 1082 [396–1301] * | 1111 [432–1352] * |
| RMS Soleus-Backward (mV) | 1248 [551–1625] | 1319 [732–1667] | 1333 [632–2233] | 1517 [779–2195] * |
| RMS Tibialis Ant.-Forward (mV) | 1324 [367–2801] | 1543 [408–2817] | 1738 [615–3371] | 1679 [478–3662] |
| RMS Tibialis Ant.-Backward (mV) | 816 [312–2291] | 844 [249–1945] | 1334 [512–2416] *§ | 1204 [348–1967] *§ |
| RMS TFL-Forward (mV) | 613 [346–1048] | 657 [330–1179] | 685 [359–1119] | 777 [345–1330] * |
| RMS TFL-Backward (mV) | 746 [224–2103] | 668 [265–1367] | 842 [235–2343] | 807 [265–2423] |
| Correct answers (n) | 23.2 [18.9–27.5] | 21.7 [18.3–25.2] | ||
| Percentage of correct answers (%) | 88.9 [83.3–94.6] | 89.1 [84.1–94.0] |
| COP Pathway | EO-ST | EO-DT | EC-ST | EC-DT |
| EO-ST | 0.0021 | <0.0001 | <0.0001 | |
| EO-DT | 0.0021 | 0.0001 | <0.0001 | |
| EC-ST | <0.0001 | 0.0001 | 1.0000 | |
| EC-DT | <0.0001 | <0.0001 | 1.0000 | |
| Ellipse Area | EO-ST | EO-DT | EC-ST | EC-DT |
| EO-ST | 1.0000 | 0.0044 | 0.0040 | |
| EO-DT | 1.0000 | 0.0117 | 0.0107 | |
| EC-ST | 0.0044 | 0.0117 | 1.0000 | |
| EC-DT | 0.0040 | 0.0107 | 1.0000 | |
| MSE ML | EO-ST | EO-DT | EC-ST | EC-DT |
| EO-ST | 0.0105 | 0.0103 | 0.0004 | |
| EO-DT | 0.0105 | 1.0000 | 0.5911 | |
| EC-ST | 0.0103 | 1.0000 | 0.6011 | |
| EC-DT | 0.0004 | 0.5911 | 0.6011 | |
| MSE AP | EO-ST | EO-DT | EC-ST | EC-DT |
| EO-ST | 0.0552 | 0.0056 | 0.0012 | |
| EO-DT | 0.0552 | 1.0000 | 0.4000 | |
| EC-ST | 0.0056 | 1.0000 | 1.0000 | |
| EC-DT | 0.0012 | 0.4000 | 1.0000 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Delafontaine, A.; Hansen, C.; Marolleau, I.; Kratzenstein, S.; Gouelle, A. Effect of a Concurrent Cognitive Task, with Stabilizing Visual Information and Withdrawal, on Body Sway Adaptation of Parkinsonian’s Patients in an Off-Medication State: A Controlled Study. Sensors 2020, 20, 5059. https://doi.org/10.3390/s20185059
Delafontaine A, Hansen C, Marolleau I, Kratzenstein S, Gouelle A. Effect of a Concurrent Cognitive Task, with Stabilizing Visual Information and Withdrawal, on Body Sway Adaptation of Parkinsonian’s Patients in an Off-Medication State: A Controlled Study. Sensors. 2020; 20(18):5059. https://doi.org/10.3390/s20185059
Chicago/Turabian StyleDelafontaine, Arnaud, Clint Hansen, Iris Marolleau, Stefan Kratzenstein, and Arnaud Gouelle. 2020. "Effect of a Concurrent Cognitive Task, with Stabilizing Visual Information and Withdrawal, on Body Sway Adaptation of Parkinsonian’s Patients in an Off-Medication State: A Controlled Study" Sensors 20, no. 18: 5059. https://doi.org/10.3390/s20185059
APA StyleDelafontaine, A., Hansen, C., Marolleau, I., Kratzenstein, S., & Gouelle, A. (2020). Effect of a Concurrent Cognitive Task, with Stabilizing Visual Information and Withdrawal, on Body Sway Adaptation of Parkinsonian’s Patients in an Off-Medication State: A Controlled Study. Sensors, 20(18), 5059. https://doi.org/10.3390/s20185059