OBINTER: A Holistic Approach to Catalyse the Self-Management of Chronic Obesity

 , , ,
, , ,  ,
,  and
and 
Abstract
1. Introduction
2. Related Work
3. Materials and Methods
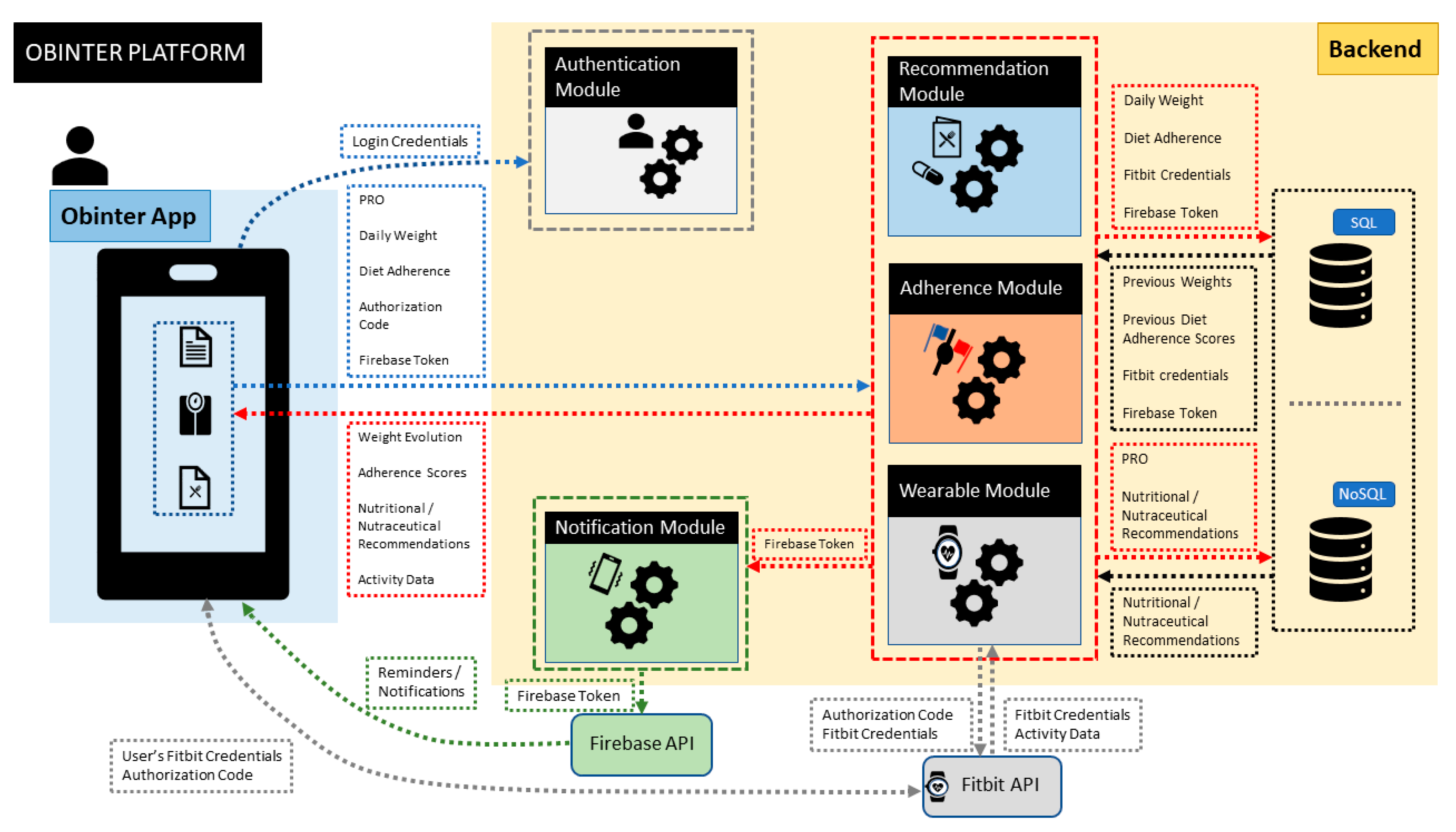
3.1. Platform
- i.
- Physical View
- ii.
- Development View
- iii.
- Logical View
3.2. Patient-Reported Outcomes (PROs)
- Assessing both the initial and final general patient background and current status using as PRO instrument a questionnaire (see Figure 3) designed by OBINTER’s research team that encompasses a multidisciplinary group of experts with relevant expertise in Digital Health, Nutrition, Endocrinology and Clinical Practice. The user responds to a life-habits questionnaire at the beginning and end of the study that is based on published, validated questionnaires in order to obtain information from the adult population regarding physical activity (IPAQ) [30] and Food Frequency intake [31]. The answers obtained in conjunction with red blood cell membrane lipidomic profiles [32] of each user are applied to generate personalized dietetic and nutraceutical recommendations. This process is detailed in Section 3.3.
- Gathering physical measurements that occur during the patient’s daily life using a wearable as PRO instrument that will accompany the user throughout the study. The specific measurements that are gathered as well as the integration mechanisms are further described in Section 3.5.
- Following up on treatment adherence and effectiveness using as PRO instrument questionnaires delivered directly to the users. These two aspects are described in greater detail in Section 3.4 and Section 3.6.
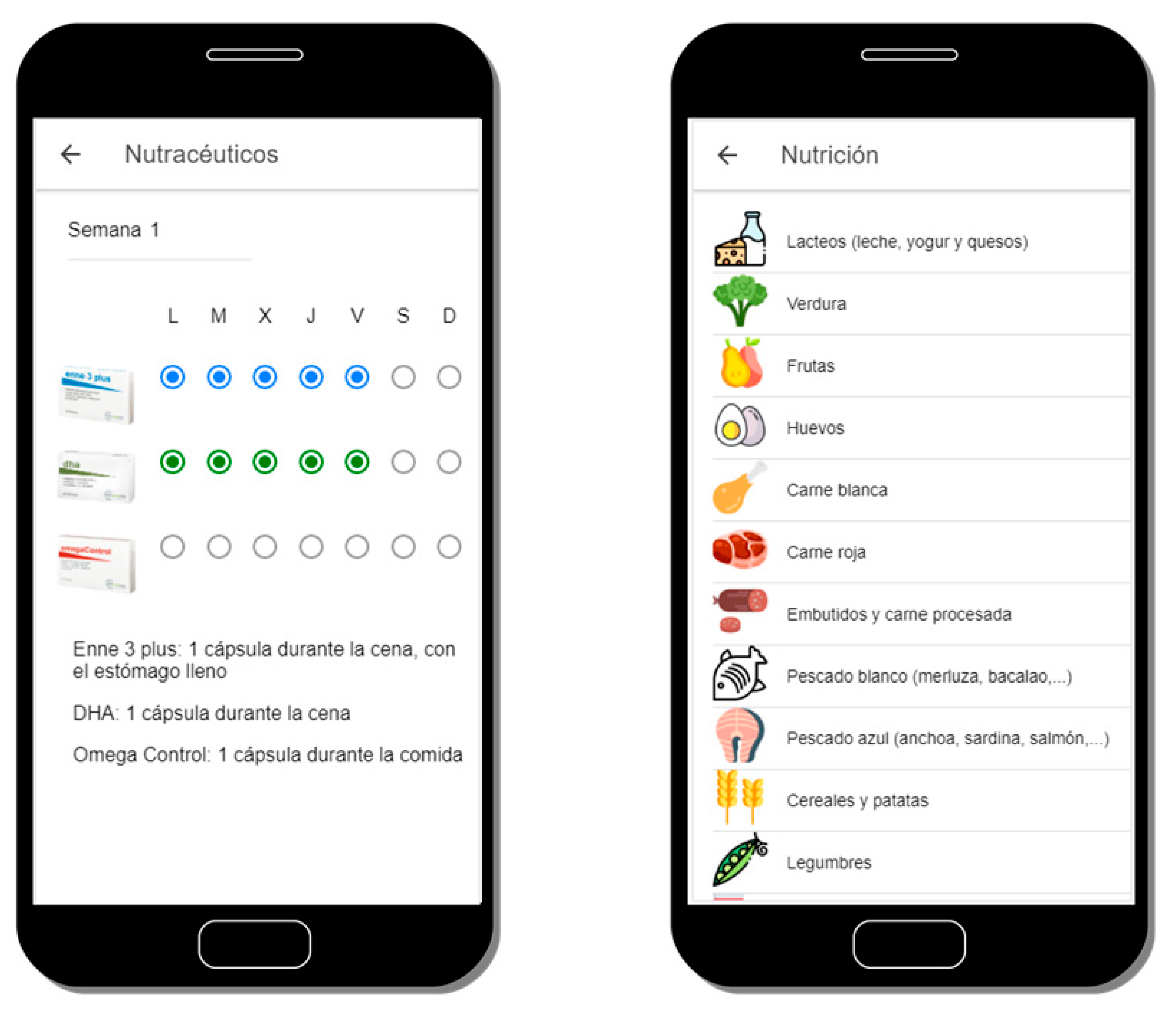
3.3. Personalized Dietetic and Nutraceutical Recommendations
3.4. Diet Adherence Control
3.5. Physical Activity Tracking
3.6. Weight Evolution Control
3.7. Adherence Strategy
- Methods of Measuring Adherence:
- ∘
- Patient questionnaires or patient self-reports are indirect methods that allow users to inform themselves about their status and progresses. The main disadvantage here, as it is in the traditional approach, is that results can be easily distorted by the patient. To mitigate this problem, the OBINTER platform checks user inputs before adding them to Information System trying to prevent the insertion of low-quality data by means of applying a different set of statistical methods or reference values, depending on the nature of the questionnaire, that could spot unusual values. For example, according to the NHS [39], a safe rate for losing weight is 0.5kg to 1kg each week, so values above/below them will be internally considered as unusual and suggested to be confirmed twice by the user.
- ∘
- Measurement of physical/physiologic markers (as an indirect method of measuring adherence). The integration of the wearable device becomes a relevant source of information to discover not only if users synchronize their data regularly, which would mean a regular interaction with the application, but also to explore and follow up on those parameters directly related to the obesity condition that might be a beacon for foreseeing low levels of adherence to the dietetic and nutraceutical recommendations.
- Methods for Improving Adherence:
- ∘
- Identify poor adherence: closely related to the methods for measuring adherence, but also complemented with other measurements such as login attempts or low personal scores in the virtual race (explained in next bullet). Since all the interactions carried out by the users within the system are tracked, OBINTER has mechanisms to detect poor adherence which is the first step to solving this issue.
- ∘
- Emphasize the value of the regimen and the effect of adherence: OBINTER’s participants are randomly assigned to a team with which they will run a virtual race “against” obesity (Figure 9). Users are informed that all their interactions and positive scores will contribute with additional virtual meters for their corresponding teams. This way, users are invited to relate compliance with a double positive purpose, therefore emphasizing the value of a good adherence. In addition, since users run in teams, we avoid that they view themselves as solely responsible for the task and simultaneously promote teamwork which has been proven as more effective than individual responsibility in multiple scenarios [40].
- ∘
- Provide simple, clear instructions and simplify the regimen as much as possible: best practices for designing an interface [41] have been adopted during OBINTER’s implementation process. The interface has been kept as simple as possible, always using common and consistent UI elements. Careful placement of items was done to help draw attention to the most important pieces of information. Internationalization issues were also considered, since the application is going to be tested in a two-official-languages country. In addition, nutraceutical and dietetic recommendations are depicted in a straightforward manner aimed at avoiding problematic misunderstandings.
- ∘
- Reinforce desirable behaviour and results when appropriate: to pursue this reinforcement, OBINTER’s platform makes use of its own notification system designed to remind the users the correct timeline physicians have designed for them to follow. Push notifications are delivered just before a scheduled relevant task. In addition, the timeline is always available the user’s consultations in the main section of the application. A second implementation has been carried out to reinforce desirable behaviour. This second implementation is a challenge delivery system that encourages users to achieve specific actions aimed to both advance in their obesity management and contribute to the teamwork, since the achievement of these challenges yields additional virtual meters for their teams (Figure 9).
3.8. User Evaluation Method
3.8.1. Study Design
- “I find the team competition system and challenge system motivating”;
- “The application can help me manage the different dimensions related to my overweight, in an orderly and easy way”;
- “I think that the proposed digital approach can help me manage my overweight and improve my well-being”.
3.8.2. Representative Tasks
3.8.3. Hardware and Software Requirements
3.8.4. Script-Driven Study
4. Results
4.1. User Evaluation Results
4.2. User Demographics
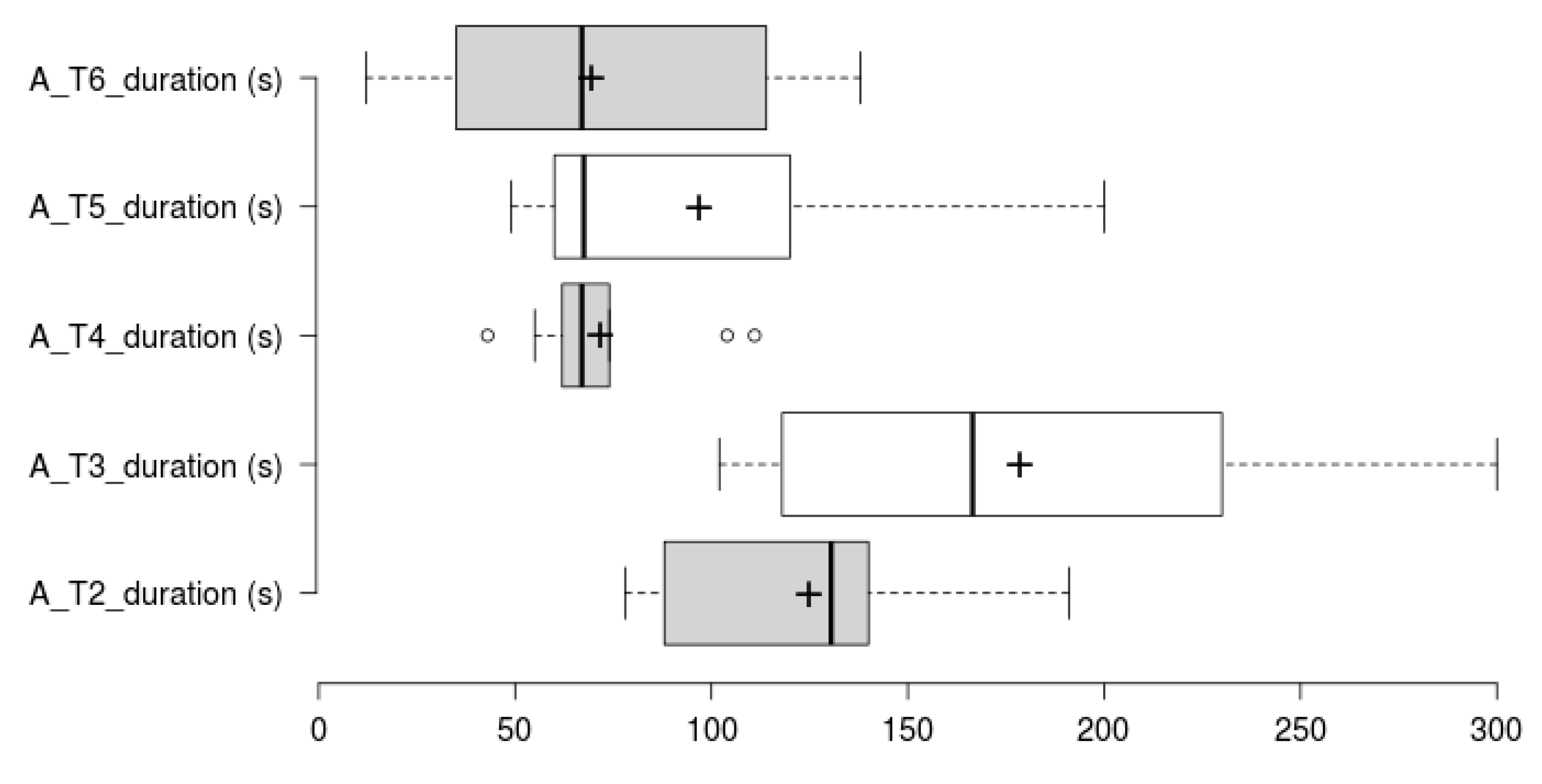
4.3. Task Completion and Times
4.4. SEQ Results Summary
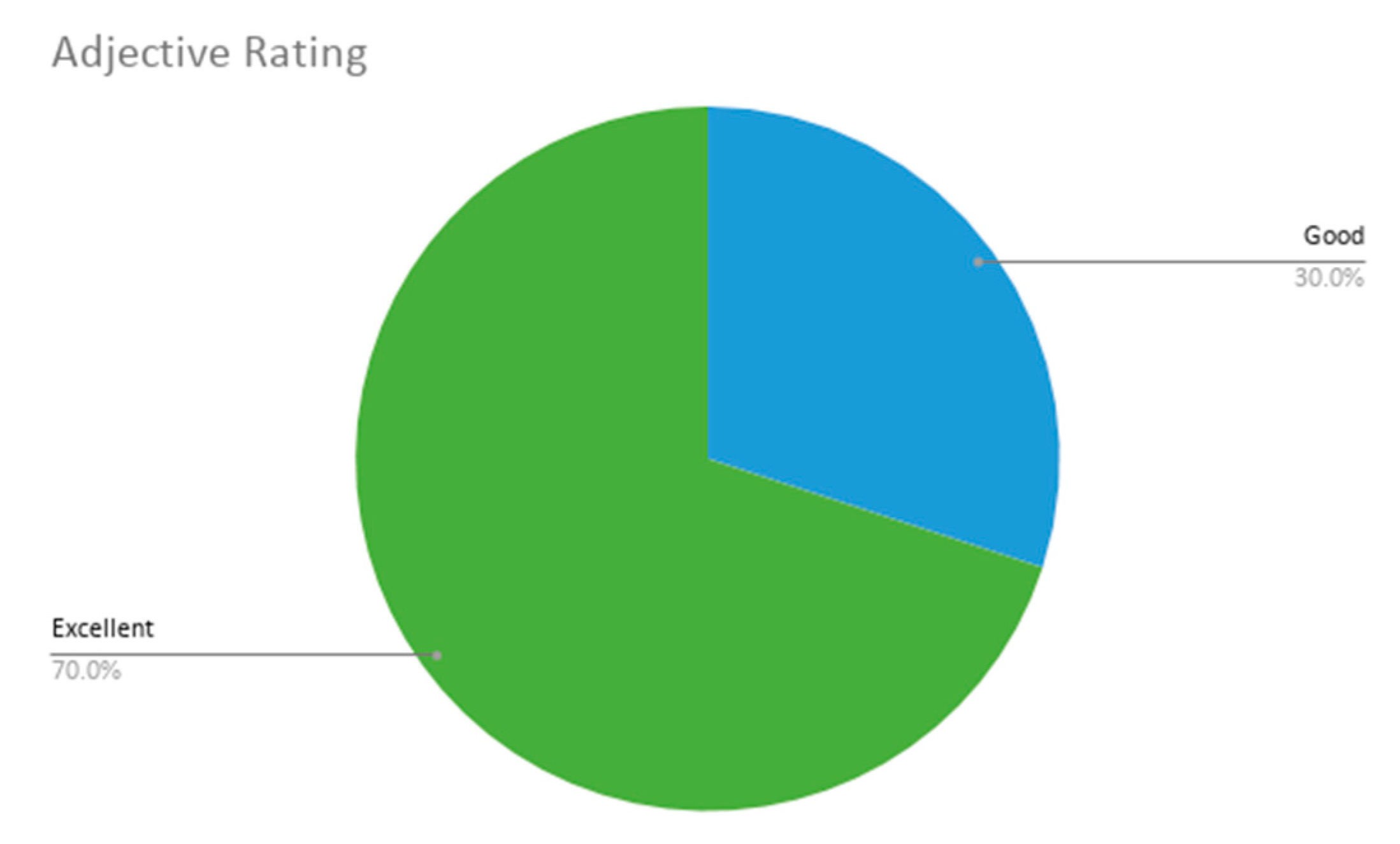
4.5. Extended SUS & Approach Acceptance Summary
4.6. Qualitative Results Summary
5. Discussion
6. Conclusions and Future Work
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Ethical Statement
References
- Rippe, J.M.; Crossley, S.; Ringer, R. Obesity as a Chronic Disease: Modern Medical and Lifestyle Management. J. Am. Diet. Assoc. 1998, 98, S9–S15. [Google Scholar] [CrossRef]
- Pi-Sunyer, X. The Medical Risks of Obesity. Postgrad. Med. 2009, 121, 21–33. [Google Scholar] [CrossRef]
- World Health Organization. Data and Statistics. 2020. Available online: https://www.euro.who.int/en/health-topics/noncommunicable-diseases/obesity/data-and-statistics (accessed on 29 July 2020).
- Kass, D.A.; Duggal, P.; Cingolani, O. Obesity could shift severe COVID-19 disease to younger ages. Lancet 2020, 395, 1544–1545. [Google Scholar] [CrossRef]
- Lighter-Fisher, J.; Phillips, M.; Hochman, S.; Sterling, S.; Johnson, D.; Francois, F.; Stachel, A. Obesity in Patients Younger Than 60 Years Is a Risk Factor for COVID-19 Hospital Admission. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Simonnet, A.; Chetboun, M.; Poissy, J.; Raverdy, V.; Noulette, J.; Duhamel, A.; Labreuche, J.; Mathieu, D.; Pattou, F.; Jourdain, M.; et al. High Prevalence of Obesity in Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) Requiring Invasive Mechanical Ventilation. Obesity 2020, 28, 1195–1199. [Google Scholar] [CrossRef]
- Scheen, A.J.; Marre, M.; Thivolet, C. Prognostic factors in patients with diabetes hospitalized for COVID-19: Findings from the CORONADO study and other recent reports. Diabetes Metab. 2020, 21. [Google Scholar] [CrossRef] [PubMed]
- Subhi, Y.; Bube, S.H.; Bojsen, S.R.; Thomsen, A.S.S.; Konge, L. Expert Involvement and Adherence to Medical Evidence in Medical Mobile Phone Apps: A Systematic Review. JMIR mHealth uHealth 2015, 3, e79. [Google Scholar] [CrossRef]
- Johns, D.J.; Hartmann-Boyce, J.; Jebb, S.A.; Aveyard, P. Diet or Exercise Interventions vs Combined Behavioral Weight Management Programs: A Systematic Review and Meta-Analysis of Direct Comparisons. J. Acad. Nutr. Diet. 2014, 114, 1557–1568. [Google Scholar] [CrossRef] [PubMed]
- Ifejika, N.L.; Bhadane, M.; Cai, C.C.; Noser, E.A.; Grotta, J.C.; Savitz, S.I. Use of a Smartphone-Based Mobile App for Weight Management in Obese Minority Stroke Survivors: Pilot Randomized Controlled Trial With Open Blinded End Point. JMIR mHealth uHealth 2020, 8, e17816. [Google Scholar] [CrossRef]
- Apiñaniz, A.; Cobos-Campos, R.; De Lafuente-Moríñigo, A.S.; Parraza, N.; Aizpuru, F.; Pérez, I.; Goicoechea, E.; Trápaga, N.; García, L. Effectiveness of randomized controlled trial of a mobile app to promote healthy lifestyle in obese and overweight patients. Fam. Pr. 2019, 36, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Bennett, G.G.; Steinberg, D.; Askew, S.; Levine, E.; Foley, P.; Batch, B.C.; Svetkey, L.P.; Bosworth, H.B.; Puleo, E.M.; Brewer, A.; et al. Effectiveness of an App and Provider Counseling for Obesity Treatment in Primary Care. Am. J. Prev. Med. 2018, 55, 777–786. [Google Scholar] [CrossRef] [PubMed]
- Simpson, S.A.; Matthews, L.; Pugmire, J.; McConnachie, A.; McIntosh, E.; Coulman, E.; Hughes, K.; Kelson, M.; Morgan-Trimmer, S.; Murphy, S.; et al. An app-, web- and social support-based weight loss intervention for adults with obesity: The HelpMeDoIt! feasibility RCT. Public Health Res. 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- Nikolaou, C.K.; Lean, M.E.J. Mobile applications for obesity and weight management: Current market characteristics. Int. J. Obes. 2016, 41, 200–202. [Google Scholar] [CrossRef] [PubMed]
- Payne, J.; Turk, M.T.; Kalarchian, M.A.; Pellegrini, C.A. Defining Adherence to Dietary Self-Monitoring Using a Mobile App: A Narrative Review. J. Acad. Nutr. Diet. 2018, 118, 2094–2119. [Google Scholar] [CrossRef]
- Thomas, J.G.; Bond, D.S. Review of Innovations in Digital Health Technology to Promote Weight Control. Curr. Diabetes Rep. 2014, 14. [Google Scholar] [CrossRef]
- Marcos, M.L.T.; Royo, M.J.P.; Domenech, N.R.; Presas, J.A.; Panisello, E.C.; Sadek, I.M.; Lopez, P.J.T. Efectos de una mejor adherencia a la dieta mediterránea por intervención digital (estudio MEDADIS) en pacientes con sobrepeso y obesidad. J. Negat. No Posit. Results 2017, 2, 94–100. [Google Scholar] [CrossRef]
- Hernández-Reyes, A.; Cámara-Martos, F.; Recio, G.M.; Molina-Luque, R.; Romero-Saldaña, M.; Rojas, R.M. Push Notifications From a Mobile App to Improve the Body Composition of Overweight or Obese Women: Randomized Controlled Trial. JMIR mHealth uHealth 2020, 8, e13747. [Google Scholar] [CrossRef]
- Fawcett, E.; Van Velthoven, M.H.; Meinert, E. Long-Term Weight Management Using Wearable Technology in Overweight and Obese Adults: Systematic Review. JMIR mHealth uHealth 2020, 8, e13461. [Google Scholar] [CrossRef]
- Yen, H.-Y.; Chiu, H.-L. The effectiveness of wearable technologies as physical activity interventions in weight control: A systematic review and meta-analysis of randomized controlled trials. Obes. Rev. 2019, 20, 1485–1493. [Google Scholar] [CrossRef]
- Tejpal, S.; Sanghera, N.; Manoharan, V.; Planas-Iglesias, J.; Myler, K.; Klein-Seetharaman, J. Towards personalised molecular feedback for weight loss. BMC Obes. 2019, 6, 20. [Google Scholar] [CrossRef]
- Frood, S.; Johnston, L.M.; Matteson, C.L.; Finegood, D.T. Obesity, Complexity, and the Role of the Health System. Curr. Obes. Rep. 2013, 2, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Pagoto, S.; Schneider, K.; Jojic, M.; DeBiasse, M.; Mann, D. Evidence-based strategies in weight-loss mobile apps. Am. J. Prev. Med. 2013, 45, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Kruchten, P. Architectural Blueprints—The “4+1” View Model of Software Architecture. IEEE Softw. 1995, 12, 42–50. [Google Scholar] [CrossRef]
- Cockburn, A. Hexagonal Architecture. Alistair Cockburn. 2020. Available online: https://alistair.cockburn.us/hexagonal-architecture/ (accessed on 29 July 2020).
- Yusuf, S. Ionic Framework by Example; Packt Publishing: Birmingham, UK, 2016. [Google Scholar]
- US Food and Drug Administration. Guidance for Industry. Patient-Reported Outcome Measures: Use in Medical Product Development to Support Labeling Claims. 2009. Available online: https://www.fda.gov/media/77832/download (accessed on 5 September 2020).
- The European Patients’ Academy on Therapeutic Innovation (EUPATI). Patient-Reported Outcomes (PROs) Assessment 2019. Available online: https://www.eupati.eu/clinical-development-and-trials/patient-reported-outcomes-pros-assessment/ (accessed on 24 July 2020).
- Locklear, T.; Abernethy, A.; Flynn, K.E.; Riley, W.; Johnson, L.L. Patient-Reported Outcomes. NIH Collaboratory Coordinating Center. 2014. Available online: https://dcricollab.dcri.duke.edu/sites/NIHKR/KR/PRO%20Resource%20Chapter.pdf (accessed on 5 September 2020).
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Ballart, J.D.; Piñol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martínez-González, M.Á.; Salas-Salvadó, J.; Martín-Moreno, J.M. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [PubMed]
- Ferreri, C.; Chatgilialoglu, C. Role of fatty acid-based functional lipidomics in the development of molecular diagnostic tools. Expert Rev. Mol. Diagn. 2012, 12, 767–780. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Luque, L.; Singh, M.; Ofli, F.; Mejova, Y.A.; Weber, I.; Aupetit, M.; Jreige, S.K.; Elmagarmid, A.; Srivastava, J.; Ahmedna, M. Implementing 360° Quantified Self for childhood obesity: feasibility study and experiences from a weight loss camp in Qatar. BMC Med. Inform. Decis. Mak. 2017, 17, 37. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Lagiou, P. Healthy Traditional Mediterranean Diet: An Expression of Culture, History, and Lifestyle. Nutr. Rev. 1997, 55, 383–389. [Google Scholar] [CrossRef]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.Á.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A Short Screener Is Valid for Assessing Mediterranean Diet Adherence among Older Spanish Men and Women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef]
- Fitbit. Fitbit Inspire and Inspire HR Fitness Trackers. 2020. Available online: https://www.fitbit.com/us/products/trackers/inspire (accessed on 24 July 2020).
- Sabaté, E. Adherence to Long-Term Therapies: Evidence for Action; WHO Press: Geneva, Switzerland, 2003. [Google Scholar]
- Osterberg, L.; Blaschke, T. Adherence to Medication. N. Engl. J. Med. 2005, 353, 487–497. [Google Scholar] [CrossRef]
- NHS. Start the NHS Weight Loss Plan. 2018. Available online: https://www.nhs.uk/live-well/healthy-weight/start-the-nhs-weight-loss-plan/ (accessed on 24 July 2020).
- Algashaam, N.M. Teamwork vs. Individual Responsibility. Int. J. Sci. Eng. Res. 2015, 6, 3. [Google Scholar]
- US Department of Health & Human Services. User Interface Design Basics. 2020. Available online: https://www.usability.gov/what-and-why/user-interface-design.html (accessed on 24 July 2020).
- Stinson, J.; McGrath, P.; Hodnett, E.; Feldman, B.; Duffy, C.; Huber, A.; Tucker, L.; Hetherington, R.; Tse, S.; Spiegel, L.; et al. Usability Testing of an Online Self-management Program for Adolescents With Juvenile Idiopathic Arthritis. J. Med. Internet Res. 2010, 12, e30. [Google Scholar] [CrossRef] [PubMed]
- Bond, R.R.; Finlay, D.D.; Nugent, C.D.; Moore, G.; Guldenring, D. A usability evaluation of medical software at an expert conference setting. Comput. Methods Programs Biomed. 2014, 113, 383–395. [Google Scholar] [CrossRef] [PubMed]
- Cleland, B.; Wallace, J.; Bond, R.; Muuraiskangas, S.; Pajula, J.; Epelde, G.; Arrúe, M.; Álvarez, R.; Black, M.; Mulvenna, M.D.; et al. Usability Evaluation of a Co-created Big Data Analytics Platform for Health Policy-Making. In Human Interface and the Management of Information. Visual Information and Knowledge Management. Lecture Notes in Computer Science; Yamamoto, S., Mori, H., Eds.; Springer: Berlin/Heidelberg, Germany, 2019; pp. 194–207. [Google Scholar] [CrossRef]
- Peute, L.W.P.; de Keizer, N.F.; Jaspers, M.W.M. The value of Retrospective and Concurrent Think Aloud in formative usability testing of a physician data query tool. J. Biomed. Inform. 2015, 55, 1–10. [Google Scholar] [CrossRef]
- Sauro, J. 10 Things to Know about the Single Ease Question (SEQ). MeasuringU. 2012. Available online: https://measuringu.com/seq10/ (accessed on 24 July 2020).
- Jordan, P.W.; Thomas, B.; McClelland, I.L.; Weerdmeester, B. Usability Evaluation in Industry; CRC Press: Boca Raton, FL, USA, 1996. [Google Scholar]
- Bangor, A. Determining What Individual SUS Scores Mean: Adding an Adjective Rating Scale. J. Usability Stud. 2009, 4, 10. [Google Scholar] [CrossRef]
- Hamilton, D.F.; Lane, J.V.; Gaston, P.; Patton, J.T.; Macdonald, D.J.; Simpson, A.H.R.W.; Howie, C.R.; Xie, L.; Yang, R.L. Assessing treatment outcomes using a single question. Bone Jt. J. 2014, 96, 622–628. [Google Scholar] [CrossRef]
- Lookback. Simple and Powerful User Research. Available online: https://lookback.io/ (accessed on 24 July 2020).
- Nielsen, J.; Landauer, T.K. A mathematical model of the finding of usability problems. In CHI ’93: Proceedings of the SIGCHI Conference on Human Factors in Computing Systems; ACM Press: New York, NY, USA, 1993; pp. 206–213. [Google Scholar] [CrossRef]
- Krug, S.; Matcho, M. Rocket Surgery Made Easy: The Do-It-Yourself Guide to Finding and Fixing Usability Problems; New Riders: Indianapolis, IN, USA, 2010. [Google Scholar]
- Lewis, J.R.; Sauro, J. The Factor Structure of the System Usability Scale. In Human Centered Design. Lecture Notes in Computer Science; Kurosu, M., Ed.; Springer: Berlin/Heidelberg, Germany, 2009; pp. 94–103. [Google Scholar] [CrossRef]
- Tullis, T.; Albert, B. Chapter 6: Self-Reported Metrics. In Measuring the User Experience, 2nd ed.; Tullis, T., Albert, B., Eds.; Morgan Kaufmann: Burlington, MA, USA, 2013; pp. 121–161. [Google Scholar] [CrossRef]
- Reichheld, F. The Ultimate Question: Driving Good Profits and True Growth, 1st ed.; Harvard Business School Press: Brighton, MA, USA, 2006. [Google Scholar]
- Young, S.W.H. Improving Library User Experience with A/B Testing: Principles and Process. J. Libr. User Exp. 2014. [Google Scholar] [CrossRef]
- Aslan, S.; Ciocca, G.; Schettini, R. Semantic Food Segmentation for Automatic Dietary Monitoring. In Proceedings of the IEEE 8th International Conference on Consumer Electronics, Berlin, Germany, 2–5 September 2018. [Google Scholar] [CrossRef]























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Approach | PRO | Personalized Dietetic/w/Metabolic Data | Diet Adherence Control | Weight Control | PA tracking | Push Notifi-cation | Adherence/Gaming Strategy |
|---|---|---|---|---|---|---|---|
| From [16] Livestrong | No | Not from experts/No | Yes | Yes | Not device | Yes | Yes |
| From [16] myWW app | No | Not from experts/No | No | Yes | Sync device | Yes | No |
| From [18] SMART MOVE | No | No/No | No | No | Not device | No | Yes |
| From [21] Digital Health Platform | Yes | Yes/Yes | No | Yes | Not device | No | No |
| From [23] Lose It! | No | Not from experts/No | Yes | Yes | Sync device | Yes | No |
| From [23] MyNetDiary | No | Not from experts/No | Yes | Yes | Sync device | Yes | No |
| From [23] MyFitnessPal | No | Not from experts/No | Yes | Yes | Sync device | Yes | No |
| OBINTER App | Yes | Yes/Yes | Yes | Yes | Sync device | Yes | Yes |
| Approach Dimensions | Task No. | Task Description |
|---|---|---|
| Patient-Reported Outcome | 1 | Fill initial questionnaire on patient’s background |
| Personalized Dietetic Recommendations, Personalized Nutraceutical Planning | 2 | Check background-based assigned diet and nutraceutical planning |
| Weight evolution Control, Diet Adherence Control | 3 | Fill weight and diet follow-up information |
| Physical activity tracking | 4 | Check steps number, burned calories and sedentary time |
| Adherence Strategy | 5 | Check assigned team and how well you are doing (adherence) |
| Adherence Strategy | 6 | Check, read and accept a proposed wellbeing challenge |
| Demographic | Result |
|---|---|
| Gender | 3 males, 7 females |
| Age | Mean 36.9 ± 12.02 years of age |
| Occupation | 2 Administrative Assistants, 3 Researchers, 1 Teacher, 2 Workers, 1 Insurance Expert, 1 Student |
| Primary Expertise | 1 Human Resources/1 Economics/3 Biomedicine/1 Languages/2 Manufacturing/1 Automotive/1 Computer Vision |
| First language | 4 Basque, 6 Spanish |
| Average computer usage per week | Mean 32.5 ± 14.64 |
| Average Internet usage per week | Mean 48.1 ± 31.67 |
| Average level of computer literacy | Mean 3.5 ± 1.08 |
| Mode: 4 | |
| Familiarity with diet/wellbeing tracking apps | Mean 1.8 ± 1.13 |
| Mode: 1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Álvarez, R.; Torres, J.; Artola, G.; Epelde, G.; Arranz, S.; Marrugat, G. OBINTER: A Holistic Approach to Catalyse the Self-Management of Chronic Obesity. Sensors 2020, 20, 5060. https://doi.org/10.3390/s20185060
Álvarez R, Torres J, Artola G, Epelde G, Arranz S, Marrugat G. OBINTER: A Holistic Approach to Catalyse the Self-Management of Chronic Obesity. Sensors. 2020; 20(18):5060. https://doi.org/10.3390/s20185060
Chicago/Turabian StyleÁlvarez, Roberto, Jordi Torres, Garazi Artola, Gorka Epelde, Sara Arranz, and Gerard Marrugat. 2020. "OBINTER: A Holistic Approach to Catalyse the Self-Management of Chronic Obesity" Sensors 20, no. 18: 5060. https://doi.org/10.3390/s20185060
APA StyleÁlvarez, R., Torres, J., Artola, G., Epelde, G., Arranz, S., & Marrugat, G. (2020). OBINTER: A Holistic Approach to Catalyse the Self-Management of Chronic Obesity. Sensors, 20(18), 5060. https://doi.org/10.3390/s20185060