Sensorized Assessment of Dynamic Locomotor Imagery in People with Stroke and Healthy Subjects

 ,
, 
 ,
,  , ,
, ,  ,
, 

Abstract
1. Introduction
2. Materials and Method
2.1. Participants
2.2. Procedures
2.2.1. Clinical Testing
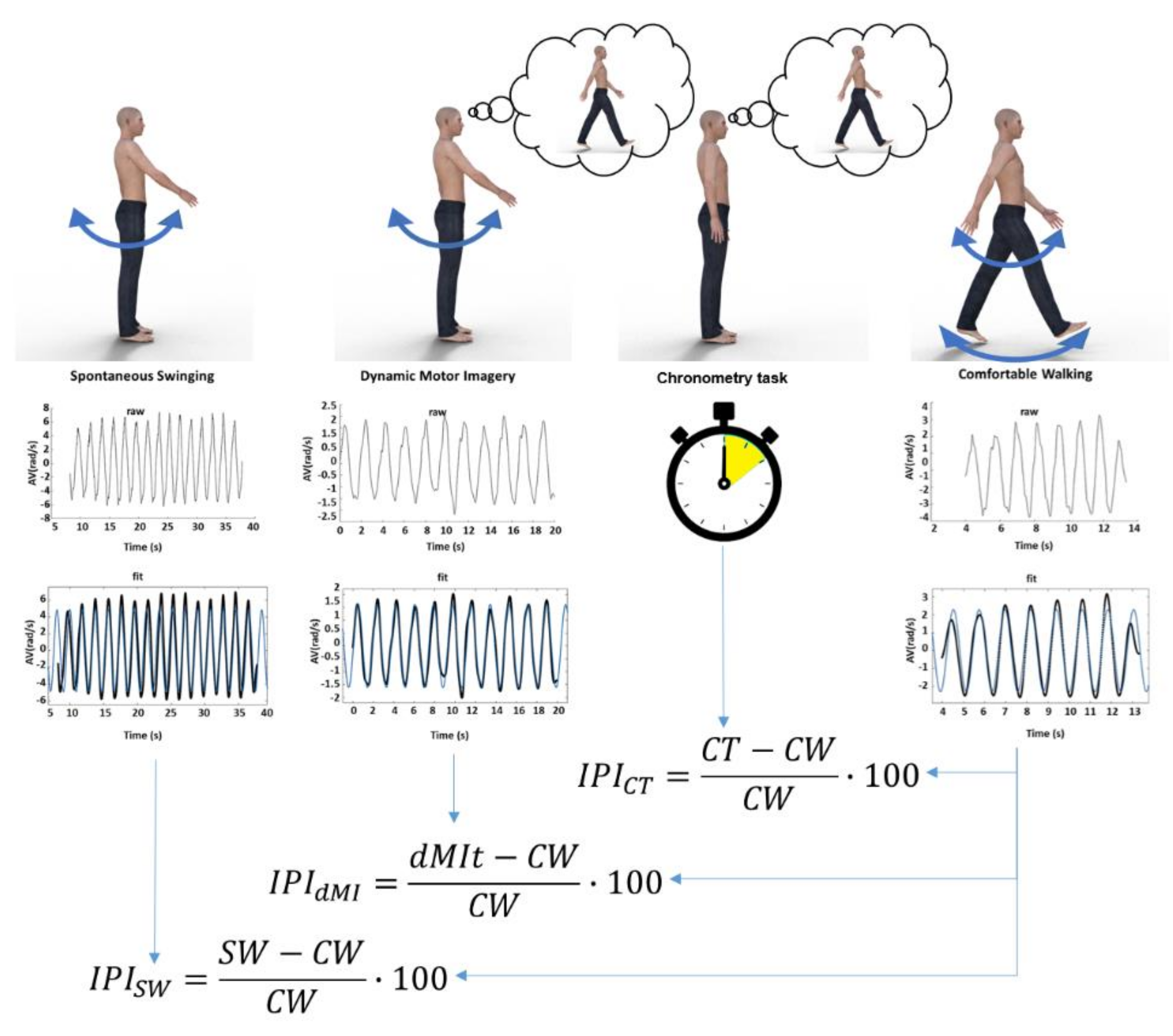
2.2.2. Motor Tasks and Setting
2.3. Apparatus of Wearable Inertial Sensors and Inertial Data Processing
2.4. Indices of Motor Imagery Performance
2.5. Statistical Analysis
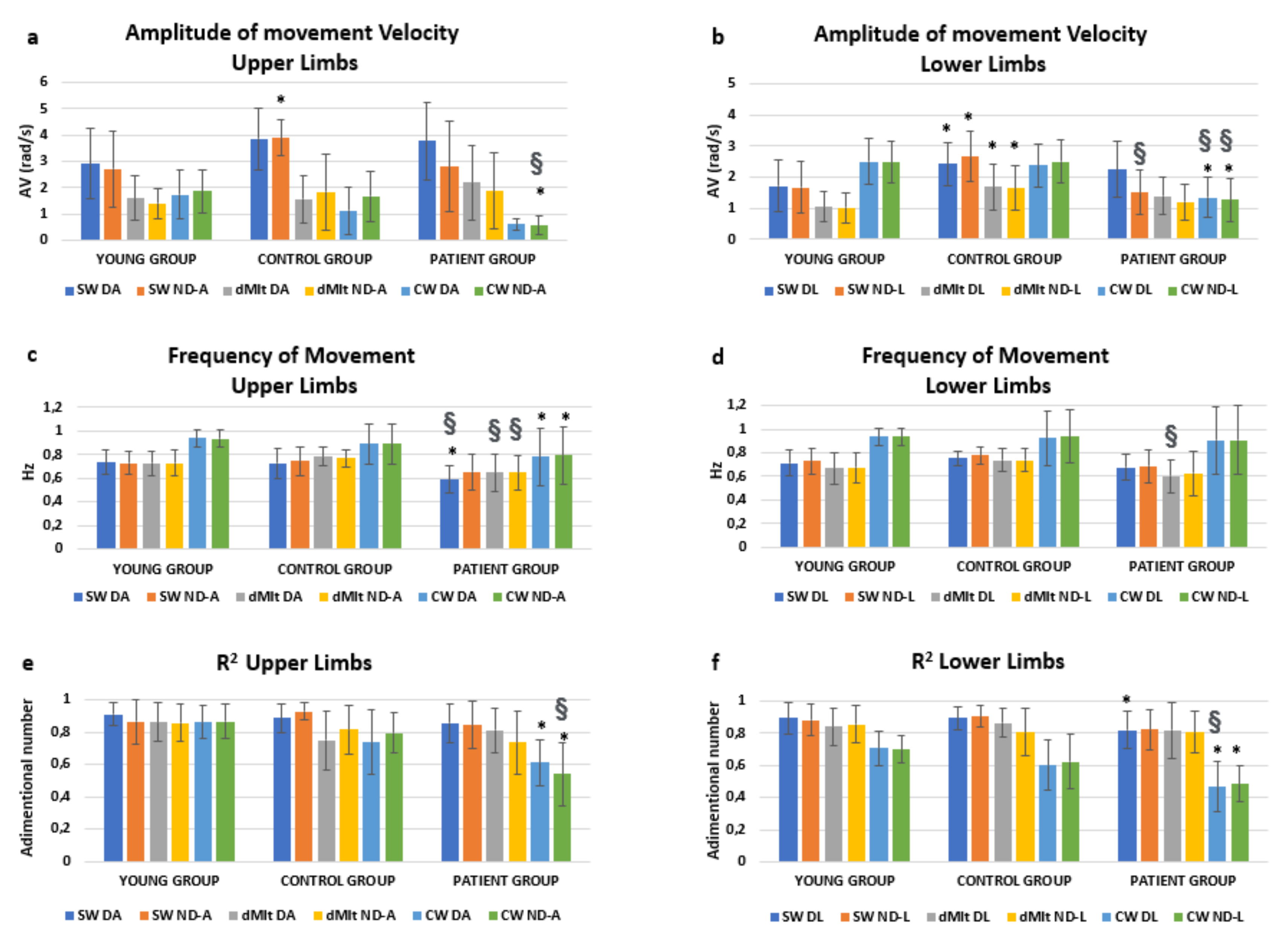
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Schuster-Amft, C.; Hilfiker, R.; Amft, O.; Scheidhauer, A.; Andrews, B.; Butler, J.; Kischka, U.; Ettlin, T. Best practice for motor imagery: A systematic literature review on motor imagery training elements in five different disciplines. BMC Med. 2011, 9, 75. [Google Scholar] [CrossRef]
- Jeannerod, M. The representing brain: Neural correlates of motor intention and imagery. Behav. Brain Sci. 1994, 17, 187–202. [Google Scholar] [CrossRef]
- Rodrigues, E.C.; Lemos, T.; Gouvea, B.; Volchan, E.; Imbiriba, L.; Vargas, C.D. Kinesthetic motor imagery modulates body sway. Neuroscience 2010, 169, 743–750. [Google Scholar] [CrossRef]
- Stins, J.F.; Schneider, I.K.; Koole, S.L.; Beek, P.J. The Influence of Motor Imagery on Postural Sway: Differential Effects of Type of Body Movement and Person Perspective. Adv. Cogn. Psychol. 2015, 11, 77–83. [Google Scholar] [CrossRef]
- Saimpont, A.; Malouin, F.; Tousignant, B.; Jackson, P.L. The influence of body configuration on motor imagery of walking in younger and older adults. Neuroscience 2012, 222, 49–57. [Google Scholar] [CrossRef]
- Fusco, A.; Gallotta, M.C.; Iosa, M.; Morone, G.; Iasevoli, L.; Trifoglio, D.; Saraceni, V.M.; Paolucci, S.; Baldari, C.; Guidetti, L. The dynamic motor imagery of locomotion is task-dependent in patients with stroke. Restor. Neurol. Neurosci. 2016, 34, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Guillot, A.; Moschberger, K.; Collet, C. Coupling movement with imagery as a new perspective for motor imagery practice. Behav. Brain Funct. 2013, 9, 8. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.J.; Radel, J.; Hanna-Pladdy, B. Improved function after combined physical and mental practice after stroke: A case of hemiparesis and apraxia. Am. J. Occup. Ther. 2011, 65, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Sacheli, L.M.; Zapparoli, L.; Preti, M.; De Santis, C.; Pelosi, C.; Ursino, N.; Zerbi, A.; Stucovitz, E.; Banfi, G.; Paulesu, E. A functional limitation to the lower limbs affects the neural bases of motor imagery of gait. NeuroImage Clin. 2018, 20, 177–187. [Google Scholar] [CrossRef]
- Thieme, H.; Bayn, M.; Wurg, M.; Zange, C.; Pohl, M.; Behrens, J. Mirror therapy for patients with severe arm paresis after stroke—A randomized controlled trial. Clin. Rehabil. 2013, 27, 314–324. [Google Scholar] [CrossRef]
- Gierlotka, M.; Labuz-Roszak, B.; Wojtyniak, B.; Lasek-Bal, A.; Zdrojewski, T.; Adamczyk-Sowa, M.; Chwojnicki, K.; Skrzypek, M.; Ciesla, D.; Gasior, M. Early and One-Year Outcomes of Acute Stroke in the Industrial Region of Poland During the Decade 2006–2015: The Silesian Stroke Registry. Neuroepidemiology 2018, 50, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Belda-Lois, J.M.; Horno, S.M.-D.; Bermejo-Bosch, I.; Moreno, J.C.; Pons, J.L.; Farina, D.; Iosa, M.; Molinari, M.; Tamburella, F.; Ramos-Murguialday, A.; et al. Rehabilitation of gait after stroke: A review towards a top-down approach. J. Neuroeng. Rehabil. 2011, 8, 66. [Google Scholar] [CrossRef] [PubMed]
- De Bartolo, D.; Morone, G.; Lupo, A.; Aloise, F.; Baricich, A.; Di Francesco, D.; Calderone, C.; Cisari, C.; Verdecchia, G.; Sandrini, G.; et al. From paper to informatics: The Post Soft Care-App, an easy-to-use and fast tool to help therapists identify unmet needs in stroke patients. Funct. Neurol. 2019, 33, 200–205. [Google Scholar]
- Iosa, M.; Bini, F.; Marinozzi, F.; Fusco, A.; Morone, G.; Koch, G.; Cinnera, A.M.; Bonnì, S.; Paolucci, S. Stability and Harmony of Gait in Patients with Subacute Stroke. J. Med. Biol. Eng. 2016, 36, 635–643. [Google Scholar] [CrossRef]
- Kantak, S.S.; Zahedi, N.; McGrath, R.L. Task-Dependent Bimanual Coordination After Stroke: Relationship with Sensorimotor Impairments. Arch. Phys. Med. Rehabil. 2016, 97, 798–806. [Google Scholar] [CrossRef]
- Plantin, J.; Pennati, G.V.; Roca, P.; Baron, J.-C.; Laurencikas, E.; Weber, K.; Godbolt, A.K.; Borg, J.; Lindberg, P.G. Quantitative Assessment of Hand Spasticity After Stroke: Imaging Correlates and Impact on Motor Recovery. Front. Neurol. 2019, 10, 836. [Google Scholar] [CrossRef]
- Jeon, H.J.; Hwang, B.Y. Effect of bilateral lower limb strengthening exercise on balance and walking in hemiparetic patients after stroke: A randomized controlled trial. J. Phys. Ther. Sci. 2018, 30, 277–281. [Google Scholar] [CrossRef]
- Li, S.; Francisco, G.E.; Zhou, P. Post-stroke Hemiplegic Gait: New Perspective and Insights. Front. Physiol. 2018, 9, 9. [Google Scholar] [CrossRef]
- Morone, G.; Annicchiarico, R.; Iosa, M.; Federici, A.; Paolucci, S.; Cortés, U.; Caltagirone, C. Overground walking training with the i-Walker, a robotic servo-assistive device, enhances balance in patients with subacute stroke: A randomized controlled trial. J. Neuroeng. Rehabil. 2016, 13, 47. [Google Scholar] [CrossRef]
- Morone, G.; Iosa, M.; Pratesi, L.; Paolucci, S. Can overestimation of walking ability increase the risk of falls in people in the subacute stage after stroke on their return home? Gait Posture 2014, 39, 965–970. [Google Scholar] [CrossRef]
- De Bartolo, D.; Spitoni, G.F.; Iosa, M.; Morone, G.; Ciancarelli, I.; Paolucci, S.; Antonucci, G. From movement to thought and back: A review on the role of cognitive factors influencing technological neurorehabilitation. Funct. Neurol. 2020, 34, 131–144. [Google Scholar]
- Dunsky, A.; Dickstein, R. Motor Imagery Training for Gait Rehabilitation of People with Post-Stroke Hemiparesis: Practical Applications and Protocols. Glob. J. Health Sci. 2018, 10, 66–78. [Google Scholar] [CrossRef]
- Vromen, A.; Verbunt, J.A.; Rasquin, S.; Wade, D.T. Motor imagery in patients with a right hemisphere stroke and unilateral neglect. Brain Inj. 2011, 25, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Ivanenko, Y.P.; Dominici, N.; Cappellini, G.; Dan, B.; Cheron, G.; Lacquaniti, F. Development of pendulum mechanism and kinematic coordination from the first unsupported steps in toddlers. J. Exp. Biol. 2004, 207, 3797–3810. [Google Scholar] [CrossRef]
- Wagenaar, R.C.; Van Emmerik, R. Resonant frequencies of arms and legs identify different walking patterns. J. Biomech. 2000, 33, 853–861. [Google Scholar] [CrossRef]
- Kilbreath, S.; Crosbie, J.; Canning, C.G.; Lee, M.-J. Inter-limb coordination in bimanual reach-to-grasp following stroke. Disabil. Rehabil. 2006, 28, 1435–1443. [Google Scholar] [CrossRef]
- Hollands, K.; Pelton, T.; Tyson, S.; Hollands, M.A.; Van Vliet, P. Interventions for coordination of walking following stroke: Systematic review. Gait Posture 2012, 35, 349–359. [Google Scholar] [CrossRef]
- Stephenson, J.L.; Lamontagne, A.; De Serres, S.J. The coordination of upper and lower limb movements during gait in healthy and stroke individuals. Gait Posture 2009, 29, 11–16. [Google Scholar] [CrossRef]
- Sousa, A.S.P.; Silva, A.; Santos, R.; Sousa, F.; Tavares, J.M.R.S.; Silva, M.A.F. Interlimb Coordination During the Stance Phase of Gait in Subjects with Stroke. Arch. Phys. Med. Rehabil. 2013, 94, 2515–2522. [Google Scholar] [CrossRef]
- Sousa, A.S.P.; Tavares, J.M.R.S. Interlimb Coordination During Step-to-Step Transition and Gait Performance. J. Mot. Behav. 2015, 47, 563–574. [Google Scholar] [CrossRef]
- Ford, M.P.; Wagenaar, R.C.; Newell, K.M. Arm constraint and walking in healthy adults. Gait Posture 2007, 26, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Moumdjian, L.; Buhmann, J.; Willems, I.; Feys, P.; Leman, M. Entrainment and Synchronization to Auditory Stimuli During Walking in Healthy and Neurological Populations: A Methodological Systematic Review. Front. Hum. Neurosci. 2018, 12, 263. [Google Scholar] [CrossRef] [PubMed]
- Secoli, R.; Milot, M.-H.; Rosati, G.; Reinkensmeyer, D.J. Effect of visual distraction and auditory feedback on patient effort during robot-assisted movement training after stroke. J. Neuroeng. Rehabil. 2011, 8, 21. [Google Scholar] [CrossRef] [PubMed]
- Iosa, M.; De Sanctis, M.; Summa, A.; Bergamini, E.; Morelli, D.; Vannozzi, G. Usefulness of Magnetoinertial Wearable Devices in Neurorehabilitation of Children with Cerebral Palsy. Appl. Bionics Biomech. 2018, 2018, 1–7. [Google Scholar] [CrossRef]
- Iosa, M.; Picerno, P.; Paolucci, S.; Morone, G. Wearable Inertial Sensors for Human Movement Analysis. Expert Rev. Med. Devices 2016, 13, 641–659. [Google Scholar] [CrossRef] [PubMed]
- Iosa, M.; Lupo, A.; Morone, G.; Baricich, A.; Picelli, A.; Panza, G.; Smania, N.; Cisari, C.; Sandrini, G.; Paolucci, S. Post Soft Care: Italian implementation of a post-stroke checklist software for primary care and identification of unmet needs in community-dwelling patients. Neurol. Sci. 2017, 39, 135–139. [Google Scholar] [CrossRef]
- Mathiowetz, V.; Volland, G.; Kashman, N.; Weber, K. Adult Norms for the Box and Block Test of Manual Dexterity. Am. J. Occup. Ther. 1985, 39, 386–391. [Google Scholar] [CrossRef]
- Iosa, M.; Fusco, A.; Morone, G.; Paolucci, S. Walking there: Environmental influence on walking-distance estimation. Behav. Brain Res. 2012, 226, 124–132. [Google Scholar] [CrossRef]
- Fusco, A.; Iasevoli, L.; Iosa, M.; Gallotta, M.C.; Padua, L.; Tucci, L.; Antonucci, G.; Baldari, C.; Guidetti, L. Dynamic motor imagery mentally simulates uncommon real locomotion better than static motor imagery both in young adults and elderly. PLoS ONE 2019, 14, e0218378. [Google Scholar] [CrossRef]
- Summa, A.; Vannozzi, G.; Bergamini, E.; Iosa, M.; Morelli, D.; Cappozzo, A. Multilevel Upper Body Movement Control during Gait in Children with Cerebral Palsy. PLoS ONE 2016, 11, e0151792. [Google Scholar] [CrossRef]
- Zwergal, A.; Linn, J.; Xiong, G.; Brandt, T.; Strupp, M.; Jahn, K. Aging of human supraspinal locomotor and postural control in fMRI. Neurobiol. Aging 2012, 33, 1073–1084. [Google Scholar] [CrossRef] [PubMed]
- Habib, M.K.; Watanabe, K.; Izumi, K. Biped Locomotion Using CPG with Sensory Interaction. In Proceedings of the 2009 IEEE International Symposium on Industrial Electronics, Seoul, Korea, 5–8 July 2009; IEEE: New York, NY, USA, 2009; pp. 1452–1457. [Google Scholar]
- Taylor, J.A.; Thoroughman, K.A. Motor Adaptation Scaled by the Difficulty of a Secondary Cognitive Task. PLoS ONE 2008, 3, e2485. [Google Scholar] [CrossRef] [PubMed]
- Iosa, M.; Fusco, A.; Marchetti, F.; Morone, G.; Caltagirone, C.; Paolucci, S.; Peppe, A. The Golden Ratio of Gait Harmony: Repetitive Proportions of Repetitive Gait Phases. BioMed Res. Int. 2013, 2013, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Iosa, M.; Morone, G.; Bini, F.; Fusco, A.; Paolucci, S.; Marinozzi, F. The connection between anthropometry and gait harmony unveiled through the lens of the golden ratio. Neurosci. Lett. 2016, 612, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Iosa, M.; De Bartolo, D.; Morone, G.; Boffi, T.; Mammucari, E.; Vannozzi, G.; Bini, F.; Marinozzi, F.; Antonucci, G.; Paolucci, S.; et al. Gait phase proportions in different locomotion tasks: The pivot role of golden ratio. Neurosci. Lett. 2019, 699, 127–133. [Google Scholar] [CrossRef]
- Patla, A.E.; Calvert, T.W.; Stein, R.B. Model of a pattern generator for locomotion in mammals. Am. J. Physiol. Integr. Am. J. Physiol. Regul. Integr. Comp. Physiol. 1985, 248, R484–R494. [Google Scholar] [CrossRef]
- Zehr, E.P.; Carroll, T.J.; Chua, R.; Collins, D.F.; Frigon, A.; Haridas, C.; Hundza, S.R.; Thompson, A.K. Possible contributions of CPG activity to the control of rhythmic human arm movement. Can. J. Physiol. Pharmacol. 2004, 82, 556–568. [Google Scholar] [CrossRef]
- MacLellan, M.J.; Ivanenko, Y.P.; Massaad, F.; Bruijn, S.M.; Duysens, J.; Lacquaniti, F. Muscle activation patterns are bilaterally linked during split-belt treadmill walking in humans. J. Neurophysiol. 2014, 111, 1541–1552. [Google Scholar] [CrossRef]
- Dzeladini, F.; Kieboom, J.V.D.; Ijspeert, A.J. The contribution of a central pattern generator in a reflex-based neuromuscular model. Front. Hum. Neurosci. 2014, 8, 371. [Google Scholar] [CrossRef]
- Ivanenko, Y.P.; Grasso, R.; Macellari, V.; Lacquaniti, F. Control of foot trajectory in human locomotion: Role of ground contact forces in simulated reduced gravity. J. Neurophysiol. 2002, 87, 3070–3089. [Google Scholar] [CrossRef]
- Sinai, M.J.; Ooi, T.L.; He, Z.J. Terrain influences the accurate judgement of distance. Nature 1998, 395, 497–500. [Google Scholar] [CrossRef] [PubMed]
- Dominici, N.; Daprati, E.; Nico, D.; Cappellini, G.; Ivanenko, Y.P.; Lacquaniti, F. Changes in the Limb Kinematics and Walking-Distance Estimation After Shank Elongation: Evidence for a Locomotor Body Schema? J. Neurophysiol. 2009, 101, 1419–1429. [Google Scholar] [CrossRef] [PubMed]
- Fàbrica, C.G.; Jerez-Mayorga, D.; Silva-Pereyra, V. Pendular energy transduction in the different phases of gait cycle in post-stroke subjects. Hum. Mov. Sci. 2019, 66, 521–528. [Google Scholar] [CrossRef] [PubMed]
- Ketcham, C.J.; Rodriguez, T.M.; Zihlman, K.A. Targeted Aiming Movements Are Compromised in Nonaffected Limb of Persons with Stroke. Neurorehabilit. Neural Repair 2007, 21, 388–397. [Google Scholar] [CrossRef] [PubMed]
- Pichiorri, F.; Morone, G.; Petti, M.; Toppi, J.; Pisotta, I.; Molinari, M.; Paolucci, S.; Inghilleri, M.; Astolfi, L.; Cincotti, F.; et al. Brain-computer interface boosts motor imagery practice during stroke recovery. Ann. Neurol. 2015, 77, 851–865. [Google Scholar] [CrossRef]
- Sterling, N.W.; Cusumano, J.P.; Shaham, N.; Piazza, S.J.; Liu, G.; Kong, L.; Du, G.; Lewis, M.M.; Huang, X. Dopaminergic modulation of arm swing during gait among Parkinson’s disease patients. J. Parkinson’s Dis. 2015, 5, 141–150. [Google Scholar] [CrossRef]
- Luria, A.R. The Working Brain. An Introduction to Neuropsychology, 1st ed.; Penguin: Middlesex, UK, 1973; p. 198. [Google Scholar]



{kind=link}
{kind=link}
| YG | CG | PG | p-Value | |
|---|---|---|---|---|
| Nr. of Participant | 27 | 15 | 15 | - |
| Nr. of Males | 13 | 8 | 9 | 0.715 |
| Age (years) | 25.1 ± 3.6 | 54.2 ± 15.3 | 53.9 ± 17.1 | 0.964 |
| Stature (cm) | 171.2 ± 7.8 | 168.3 ± 7.7 | 174.1 ± 8.8 | 0.065 |
| Upper Limb Length (cm) | 58.3 ± 3.5 | 57.3 ± 3.2 | 59.7 ± 4.2 | 0.723 |
| Arm Length (cm) | 32.2 ± 2.6 | 30.3 ± 2 | 31.4 ± 2.2 | 0.175 |
| Forearm Length (cm) | 26.6 ± 1.7 | 26.9 ± 1.4 | 28.3 ± 2.3 | 0.059 |
| Lower Limb Length (cm) | 81.15 ± 3.9 | 81.3 ± 5.1 | 85.14 ± 6.6 | 0.089 |
| Thigh Length (cm) | 40.4 ± 4.8 | 43.6 ± 3.4 | 46.1 ± 4.5 | 0.105 |
| Shank Length (cm) | 40.7 ± 3 | 37.6 ± 3.7 | 39.07 ± 3.1 | 0.281 |
| Clinical Assessment of Patients | Median | IQR |
|---|---|---|
| Times from stroke Functional Ambulation Categories | 37 4 | 70 1 |
| Tinetti Scale-Walk | 11 | 2 |
| Berg Balance Scale | 54 | 3.5 |
| Barthel Index | 100 | 2.5 |
| Motricity Index—Affected Upper Limb Motricity Index—Not Affected Upper Limb Motricity Index—Affected Lower Limb Motricity Index—Not Affected Lower Limb | 83 99 83 99 | 18.5 0 13 0 |
| Box and Blocs—Affected Hand Box and Blocs—Not Affected Hand | 30 47 | 34 11.5 |
| Kinesthetic and Visual Imagery Questionnaire | 97 | 22 |
| Parameter | Limbs | IPI | YG | CG | PG Unaffected | PG Affected | Between-Groups p: | |
|---|---|---|---|---|---|---|---|---|
| Speed Amplitude | Upper Limbs | SW | −111 ± 26% | −340 ± 76% | −578 ± 98% | −494 ± 91% | <0.001 | |
| dMIt | −16 ± 18% | −68 ± 24% | −298 ± 80% | −278 ± 59% | <0.001 | |||
| dMIt vs. SW | p | <0.001 | <0.001 | 0.002 | 0.006 | - | ||
| Lower Limbs | SW | 13 ± 12% | −9 ± 6% | −169 ± 75% | −28 ± 12% | <0.001 | ||
| dMIt | 52 ± 6% | 30 ± 6% | −42 ± 29% | −8 ± 12% | <0.001 | |||
| dMIt vs. SW | p | <0.001 | <0.001 | 0.001 | 0.012 | - | ||
| Frequency | Upper Limbs | SW | 22 ± 1% | 16 ± 3% | 18 ± 8% | 9 ± 10% | 0.238 | |
| dMIt | 22 ± 1% | 11 ± 2% | 9 ± 9% | 11 ± 9% | 0.001 | |||
| dMIt vs. SW | p | 0.901 | 0.056 | 0.020 | 0.910 | - | ||
| Lower Limbs | SW | 23 ± 1% | 14 ± 3% | 20 ± 6% | 20 ± 6% | 0.112 | ||
| dMIt | 28 ± 1% | 18 ± 3% | 29 ± 7% | 27 ± 8% | 0.014 | |||
| dMIt vs. SW | p | 0.002 | 0.120 | 0.001 | 0.027 | - | ||
| Waveform | Upper Limbs | SW | −4 ± 2% | −30 ± 12% | −49 ± 12% | −95 ± 36% | <0.001 | |
| dMIt | −1 ± 3% | −10 ± 9% | −42 ± 12% | −56 ± 20% | <0.001 | |||
| dMIt vs. SW | p | 0.012 | <0.001 | 0.112 | 0.017 | - | ||
| Lower Limbs | SW | −29 ± 3% | −55 ± 7% | −97 ± 23% | −79 ± 14% | <0.001 | ||
| dMIt | −22 ± 3% | −44 ± 7% | −97 ± 24% | −76 ± 13% | <0.001 | |||
| dMIt vs. SW | p | 0.014 | 0.028 | 0.776 | 0.910 | - | ||
| Chronometry Task | dMIt | 3 ± 5% | −2 ± 9% | 2 ± 16% | 0.941 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Bartolo, D.; Belluscio, V.; Vannozzi, G.; Morone, G.; Antonucci, G.; Giordani, G.; Santucci, S.; Resta, F.; Marinozzi, F.; Bini, F.; et al. Sensorized Assessment of Dynamic Locomotor Imagery in People with Stroke and Healthy Subjects. Sensors 2020, 20, 4545. https://doi.org/10.3390/s20164545
De Bartolo D, Belluscio V, Vannozzi G, Morone G, Antonucci G, Giordani G, Santucci S, Resta F, Marinozzi F, Bini F, et al. Sensorized Assessment of Dynamic Locomotor Imagery in People with Stroke and Healthy Subjects. Sensors. 2020; 20(16):4545. https://doi.org/10.3390/s20164545
Chicago/Turabian StyleDe Bartolo, Daniela, Valeria Belluscio, Giuseppe Vannozzi, Giovanni Morone, Gabriella Antonucci, Gianluca Giordani, Stefania Santucci, Federica Resta, Franco Marinozzi, Fabiano Bini, and et al. 2020. "Sensorized Assessment of Dynamic Locomotor Imagery in People with Stroke and Healthy Subjects" Sensors 20, no. 16: 4545. https://doi.org/10.3390/s20164545
APA StyleDe Bartolo, D., Belluscio, V., Vannozzi, G., Morone, G., Antonucci, G., Giordani, G., Santucci, S., Resta, F., Marinozzi, F., Bini, F., Paolucci, S., & Iosa, M. (2020). Sensorized Assessment of Dynamic Locomotor Imagery in People with Stroke and Healthy Subjects. Sensors, 20(16), 4545. https://doi.org/10.3390/s20164545