IL-12 and IL-18 Induction and Subsequent NKT Activation Effects of the Japanese Botanical Medicine Juzentaihoto

Abstract
1. Introduction
2. Materials and Methods
2.1. JTT
2.2. Patients
2.3. ELISA
2.4. Cell culture
2.5. Mice
2.6. Pathological inspection
2.7. TEM
2.8. Immunohistochemical staining (IHC)
2.9. In situ hybridization mRNA analysis (ISH)
2.10. Statistical study
3. Results
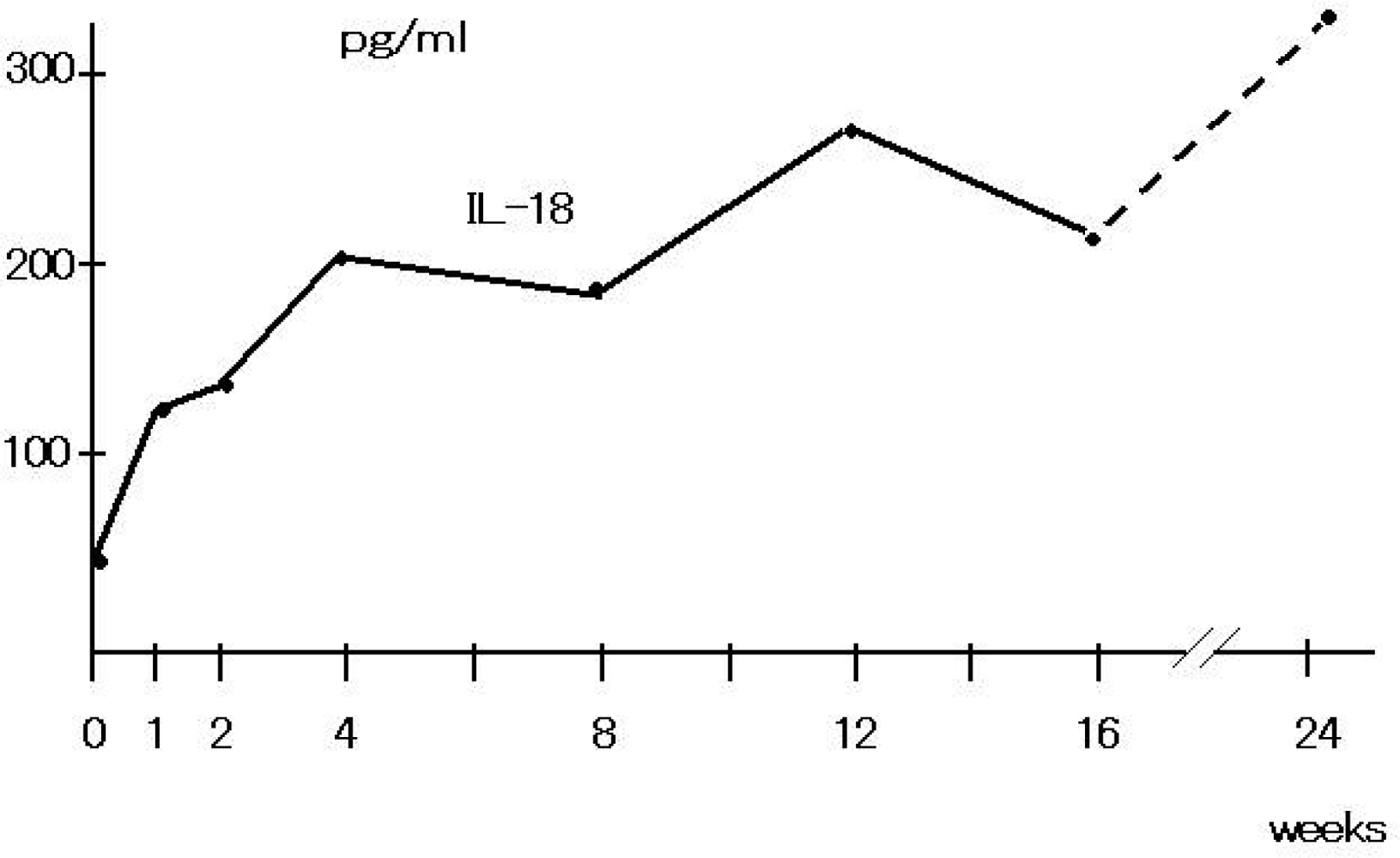
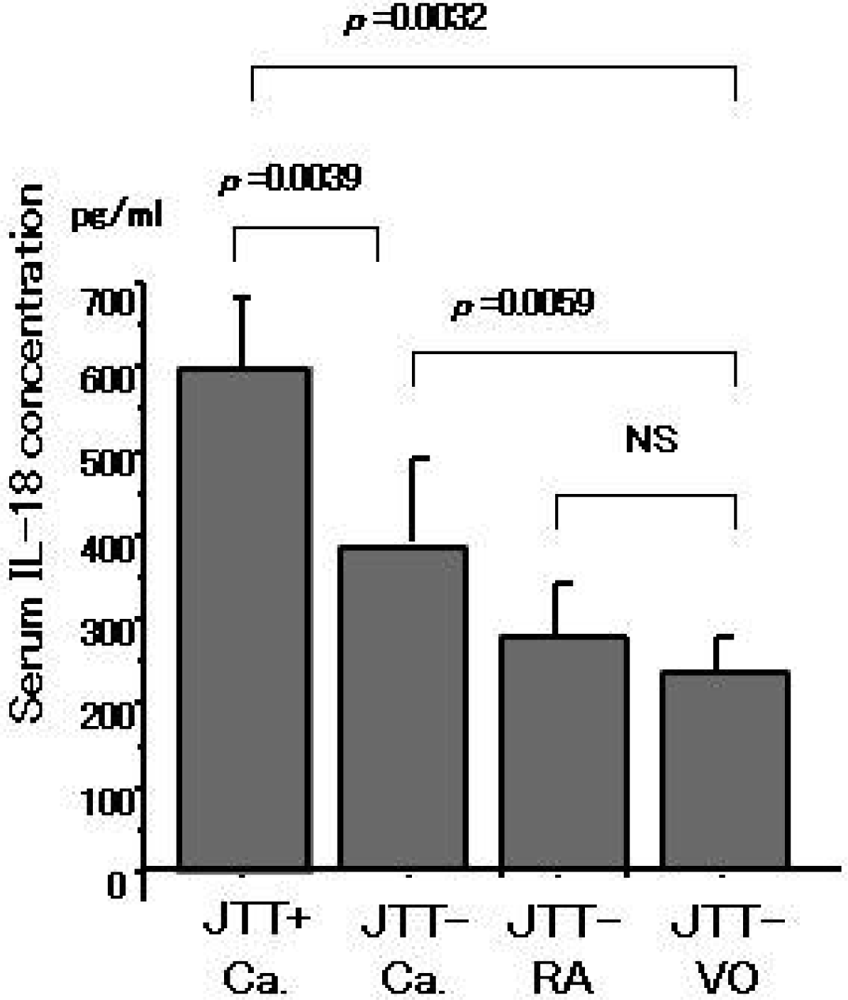
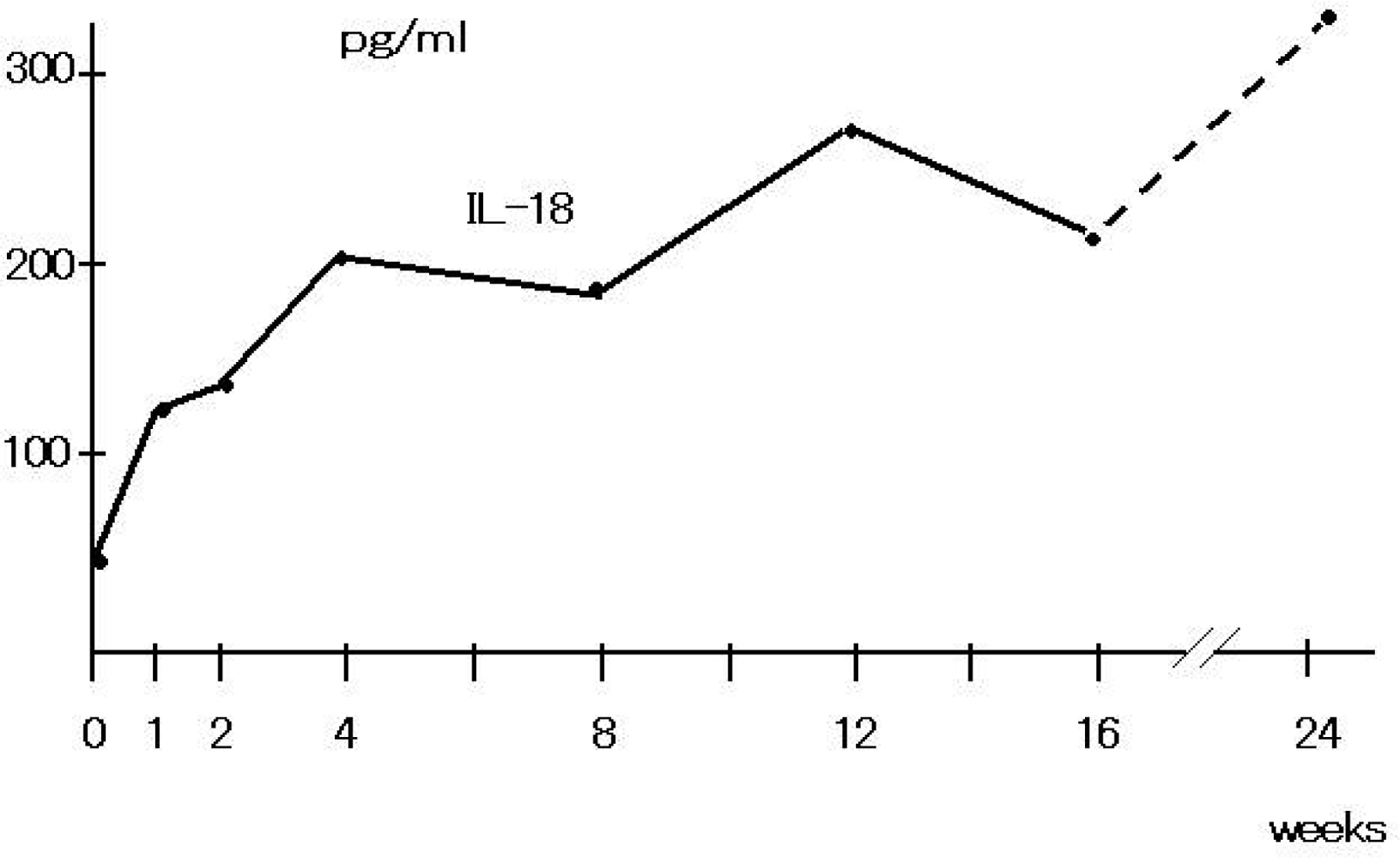
3.1. Serum cytokines
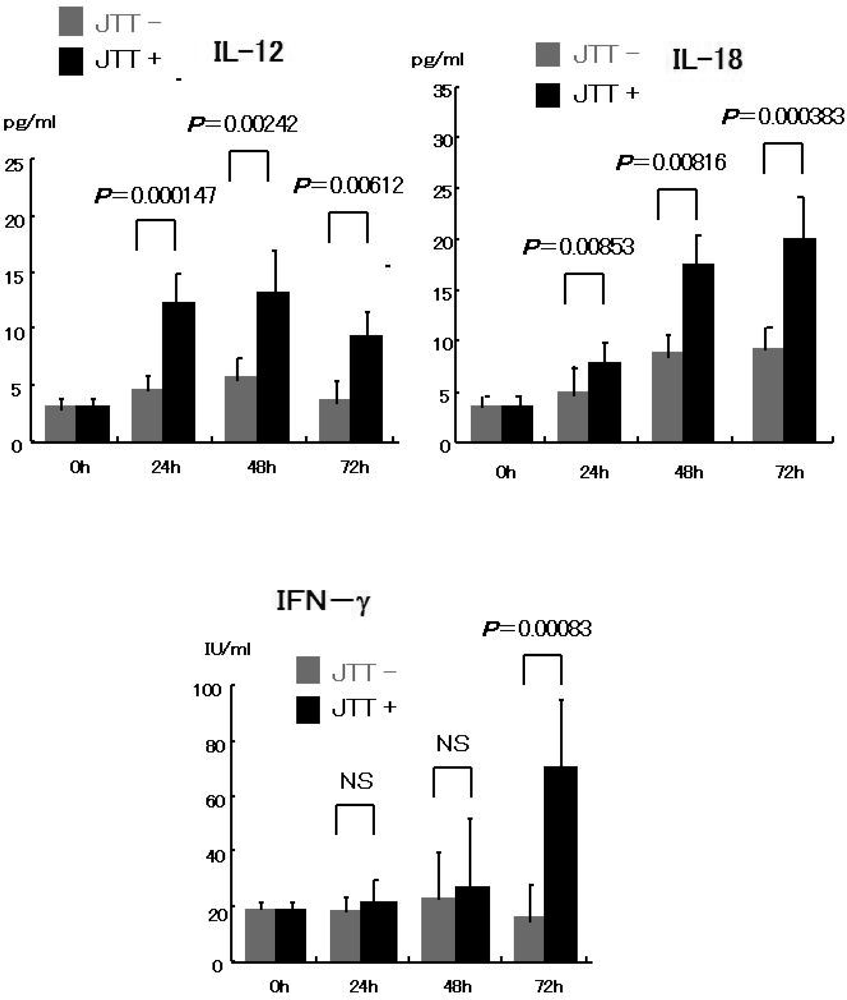
3.2. Cell culture
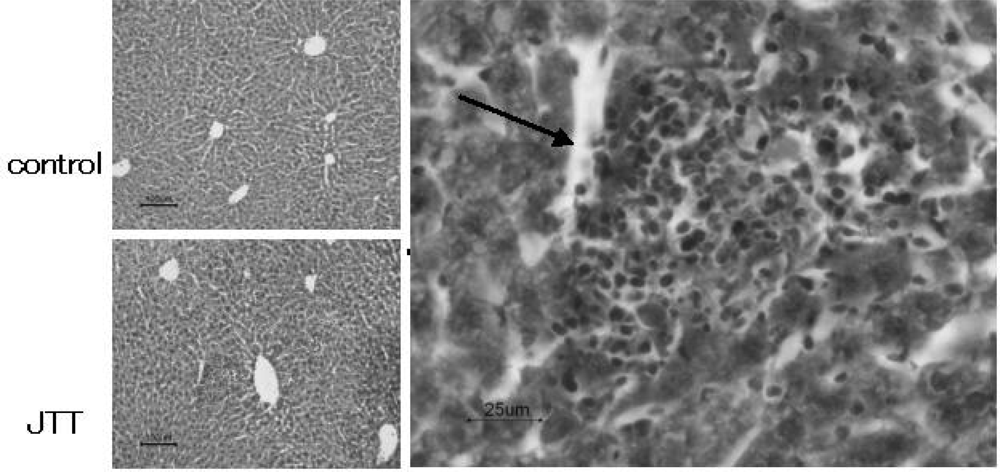
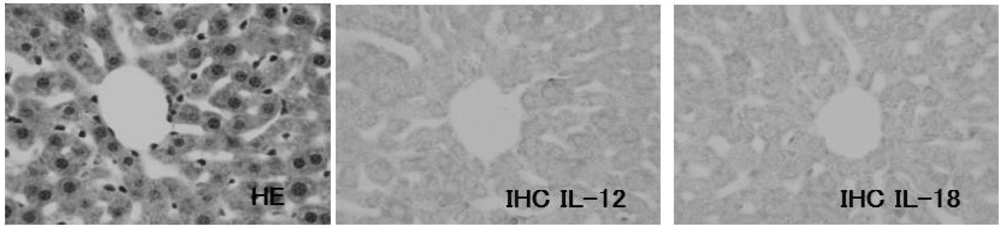
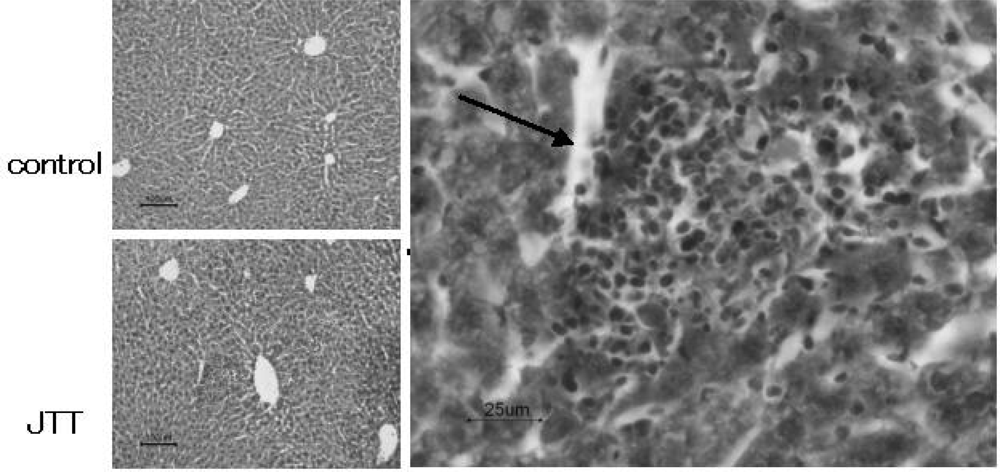
3.3. Pathological changes in liver
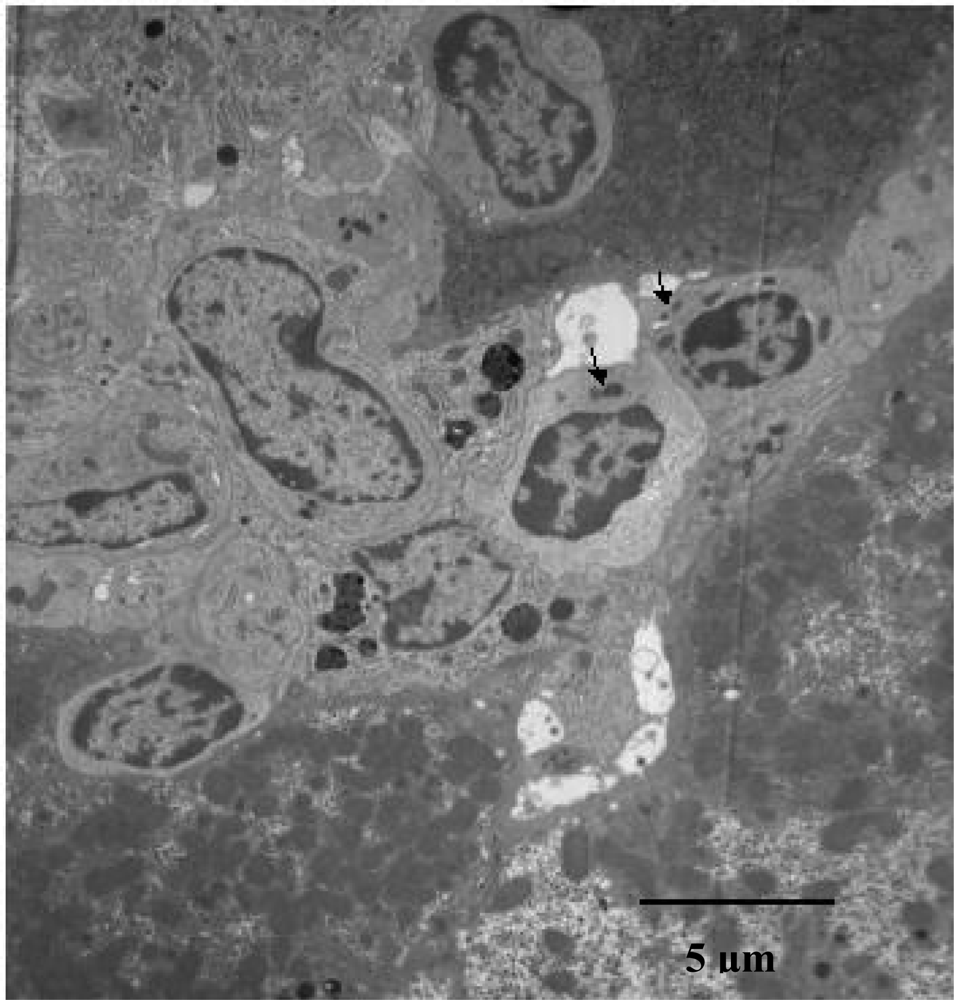
3.4. TEM findings
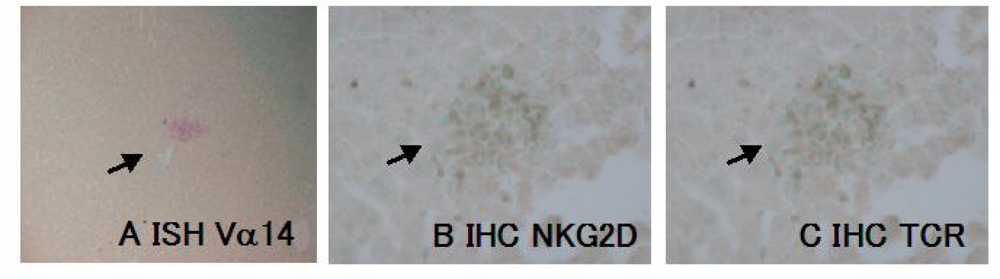
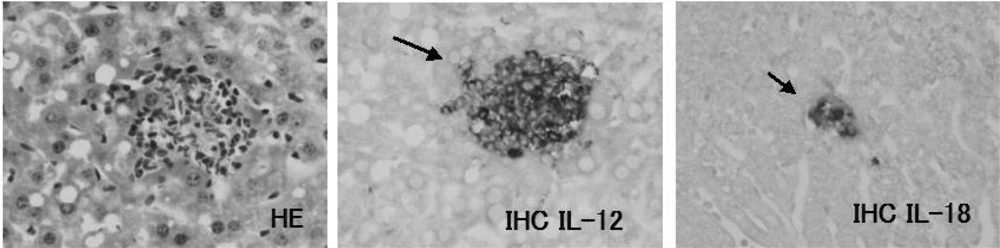
3.5. NKT infiltration in the JTT treated mice Liver
3.6. ISH for Va14
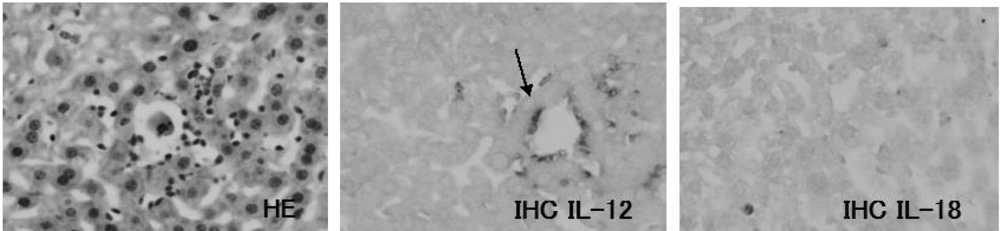
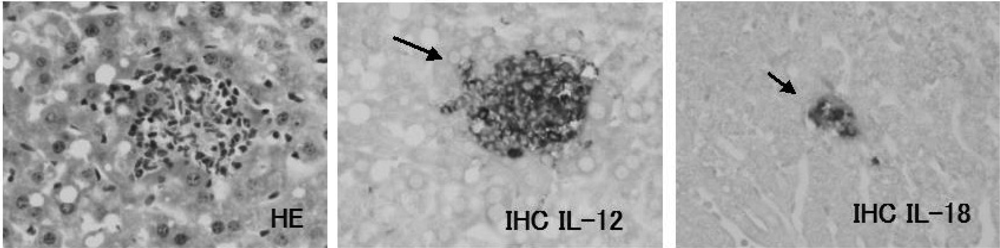
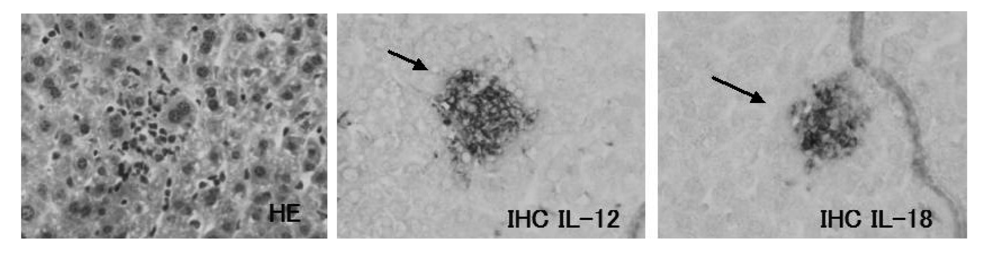
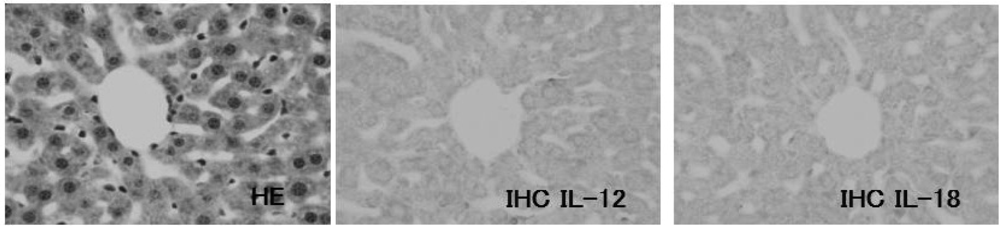
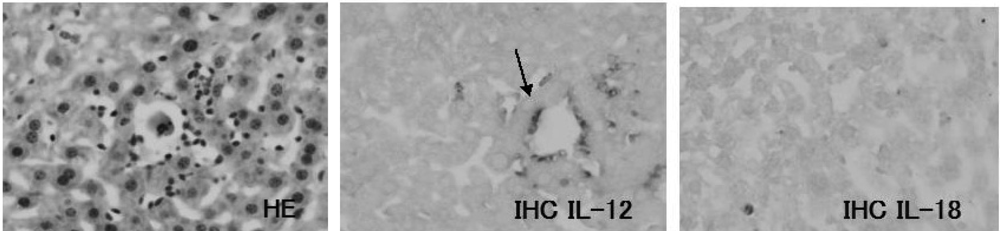
3.7. IL-12 expression on the JTT treated mice liver
3.8. IL-18 expression on the JTT treated mice liver
4. Discussion
Conclusions
Acknowledgments
References
- Akiba, T; Aoyama, R; Arai, M; Asaoka, T; Cyong, JC; Fukuta, Y; Fukuzawa, M; Goto, T; Hanawa, T; Hara, K. Introduction to KAMPO, Japanese Traditional Medicine; Sato, Y, Hanawa, T, Arai, M, Cyong, JC, Fukuzawa, M, Mitani, K, Ogihara, Y, Sakiyama, T, Shimada, Y, Toriizuka, K, Yamada, T, Eds.; Elsevier: Tokyo, Japan, 2005. [Google Scholar]
- Japanese Pharmacopoeia XV edition; Ministery of Health, Labour and Welfare; Aimi, N; Aoki, M; Aonuki, K; Aoyagi, N; Arakawa, Y; Arimoto, K; Ashizawa, K; Aso, S; Aso, Y; Emura, M; et al. (Eds.) 2006; pp. 1734–1735.
- Saiki, I; Yamaura, T; Ohnishi, Y; Hayakawa, Y; Komatsu, Y; Nunome, S. HPLC analysis of Juzen-taiho-to and its variant formulations and their antimetastatic efficacies. Chem Pharm Bull 1999, 47, 1170–1174. [Google Scholar]
- Hamada, M; Fujii, Y; Yamamoto, H; Miyazawa, Y; Shui, SH; Tung, CY; Yamaguchi, N. Effect of kampo medicine, zyuzentaihoto, on the immuno reactivity of tumor-bearing mice. J Ethnopharmacol 1988, 24, 311–320. [Google Scholar]
- Kiyohara, H; Takemoto, N; Komatsu, Y; Kawamura, H; Hosoya, E; Yamada, H. Characterization of mitogenic oeptic polysaccharides from kampo (Japanese herbal) medicine “Juzen-Taiho-To”. Planta Med 1991, 57, 254–259. [Google Scholar]
- Utsuyama, M; Seidlar, H; Kitagawa, M; Hirokawa, K. Immunological restoration and anti-tumor effect by Japanese herbal medicine in aged mice. Mechan Age Develop 2001, 122, 341–352. [Google Scholar]
- Saiki, I. A Kampo medicine “Juzen-taiho-to” prevention of malignant progression and metastasis of tumor cells and the mechanisms of action. Biol Pharm Bull 2000, 23, 677–688. [Google Scholar]
- Maruyama, H; Kawamura, H; Takemoto, N; Komatsu, Y; Aburada, M; Hosoya, E. Effect of Juzentaihoto on phagocytes. Jpn J Inflamation 1988, 8, 461–465. [Google Scholar]
- Haranaka, K; Satomi, N; Sakurai, A; Haranaka, R; Okada, N; Kobayashi, M. Antitumor activities and tumor necrosis factor producibility of traditional Chinese medicine and crude drugs. Cancer Immunol Immunother 1985, 20, 1–5. [Google Scholar]
- Kubota, A; Okamura, S; Shimoda, K. A traditional Chinese herbal medicine, Juzen-taiho-to, augments the production of granulocyte/macrophage colony-stimulating factor from human peripheral blood mononuclear cells in vitro. Int J Immunother 1992, 8, 191–195. [Google Scholar]
- Ohnishi, Y; Fujii, H; Hayakawa, Y; Sakukawa, R; Yamaura, T; Sakamoto, T; Tsukada, K; Fujimaki, M; Nunome, S; Komatsu, Y; Saiki, I. Oral administration of a Kampo(Japanese herbal) medicine Juzen-taiho-to inhibits liver metastasis of colon 26-L5 carcinoma cells. Jpn J Cancer Res 1998, 89, 206–213. [Google Scholar]
- Cui, J; Shin, T; Kawano, T; Sato, H; Kondo, E; Toura, I; Kaneko, Y; Koseki, H; Kanno, M; Taniguchi, M. Requirement for Vα14 T cells in IL-12-mediated rejection of tumors. Science 1997, 278, 1623–1626. [Google Scholar]
- Matsumoto, T; Sakurai, HM; Kiyohara, H; Yamada, H. Orally administered decoction of Kampo (Japanese herbal) medicine “Juzen -Taiho –To” modulates cytokine secretion and induces NKT cells in mouse liver. Immunopharmacology 2000, 46, 149–161. [Google Scholar]
- Adachi, Y; Koseki, H; Zulstra, M; Taniguchi, M. Positive selection of invariant Vα14+ T cells by non-major histocompatiblility complex-encoded class I-like molecules expressed on bone marrow-derived cells. Proc Natl Acad Sci 1995, 92, 1200–1204. [Google Scholar]
- Tsutsui, H; Matsui, K; Okamura, H; Nakanishi, K. Pathophysiological role of interleukin-18 in inflammatory liver disease. Immunol Rev 2000, 174, 192–209. [Google Scholar]
- Kobayashi, M; Fitz, L; Ryan, M; Hewick, MR; Clark, CS; Chan, S; Loudon, R; Sherman, F; Perussia, B; Trinchieri, G. Identification and purification of natural killer cell stimulatory factor, a cytokine with multiple biologic effects on human lymphocytes. J Exp Med 1989, 170, 827–845. [Google Scholar]
- Hsieh, SC; Macatonia, ES; Tripp, SC; Wolf, FS; O'Garra, A; Murphy, MK. Development of TH1 CD4+ T cells through IL-12 produced by Listeria-induced macrophages. Science 1993, 260, 547–549. [Google Scholar]
- Matsuda, T; Uzuki, M; Uchida, T; Nakamura, M; Tai, M; Shiraishi, N; Sazaki, N; Yakushiji, F; Tomiyama, J; Suzuki, S; et al. Induction of Mononuclear Cell Infiltration into Liver by the Japanese Herbal Medicine. Drugs Exp Clin Res 2005, 31, 207–214. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Crude Drugs | Scientific Name of Botanical Origin | Ratio |
|---|---|---|
| Astragali Radix | Astragalus membranaceus Bunge or A. mongholicus Bunge | 3.0 |
| Cinnamomi Cortex | Chinnamomum cassia Mlume or other species of the same genus | 3.0 |
| Rehmanniae Radix | Rehamannia glutinosa Liboschitz var. | 3.0 |
| Purpurea Makino or A. glutinosa Liboschitz | ||
| Paeoniae Radix | Paeonia lactiflora Pallas or allied plants | 3.0 |
| Cnidii Rhizoma | Cnidium officinale Makino | 3.0 |
| Atractylodis | Atractylodes launcea De Candolle or A. chinesis Koidzumi | 3.0 |
| Lanceae Rhizoma | ||
| Angelicae Radix | Angelica acutiloba Kitagawa or allied plants | 3.0 |
| Ginseng Radix | Panax ginseng C.A. Meyer | 3.0 |
| Hoelen | The sclerotium of Poria cocos Wolf | 3.0 |
| Glycyrrhizae Radix | Glycyrrhiza uralensis Fischier, G. grabra Linne, or other species of the same genus |
| Cytokine | Kit code | Production | Sensitivity |
|---|---|---|---|
| hIL-1 | RPN5971 | GE Imagination at Work | >4 pg/mL |
| hIL-2 | JIMRO IL-2 | Otsuka Pharma. Tokyo, Japan | >50 pg/mL |
| hIL-4 | S-4050 | R & D Systems Inc. MN, U.S.A. | >15 pg/mL |
| hIL-6 | D-6050 | R & D Systems Inc. MN, U.S.A. | >8 pg/mL |
| hIL-12 (supernatant) | EHIL12 | Pierce Biotech. Inc. IL, U.S.A | >3 pg/mL |
| hIL-12 (serum) | P1200 | R & D Systems Inc. MN, U.S.A. | >8 pg/mL |
| hIL-18 | #7260 | Med. Biologic. Lab. Nagoya, Japan | >12.5 pg/mL |
| hTNF-α | QTA00B | R & D Systems Inc. MN, U.S.A. | >0.5 pg/mL |
| hIFN-γ | IM1743 | Immunotech. Co. Marseille, France | >0.4 IU/mL |
| mIL-12 | M1270 | R & D Systems Inc. MN, U.S.A. | >2.5 pg/mL |
| mIL-18 | #7625 | Med. Biologic. Lab. Nagoya, Japan | >25 pg/mL |
| Antigen | Clone | Production |
|---|---|---|
| TCRαβ | MO073207 | Becton Dickinson Co. (NJ, U.S.A.) |
| NKG2D | 191004 | TECHNE (Staffordshire, U.K.) |
| IL-12 | C15.6 | Biosource International Inc. (CA. U.S.A.) |
| IL-18 | SC9464 | Santa Cruz Biotech. Inc. (CA. U.S.A.) |
Share and Cite
Fujiki, K.; Nakamura, M.; Matsuda, T.; Isogai, M.; Ikeda, M.; Yamamoto, Y.; Kitamura, M.; Sazaki, N.; Yakushiji, F.; Suzuki, S.; et al. IL-12 and IL-18 Induction and Subsequent NKT Activation Effects of the Japanese Botanical Medicine Juzentaihoto. Int. J. Mol. Sci. 2008, 9, 1142-1155. https://doi.org/10.3390/ijms9071142
Fujiki K, Nakamura M, Matsuda T, Isogai M, Ikeda M, Yamamoto Y, Kitamura M, Sazaki N, Yakushiji F, Suzuki S, et al. IL-12 and IL-18 Induction and Subsequent NKT Activation Effects of the Japanese Botanical Medicine Juzentaihoto. International Journal of Molecular Sciences. 2008; 9(7):1142-1155. https://doi.org/10.3390/ijms9071142
Chicago/Turabian StyleFujiki, Kazuhiko, Masanori Nakamura, Takako Matsuda, Mariko Isogai, Minako Ikeda, Yutaka Yamamoto, Mari Kitamura, Naoko Sazaki, Fumiatsu Yakushiji, Shinji Suzuki, and et al. 2008. "IL-12 and IL-18 Induction and Subsequent NKT Activation Effects of the Japanese Botanical Medicine Juzentaihoto" International Journal of Molecular Sciences 9, no. 7: 1142-1155. https://doi.org/10.3390/ijms9071142
APA StyleFujiki, K., Nakamura, M., Matsuda, T., Isogai, M., Ikeda, M., Yamamoto, Y., Kitamura, M., Sazaki, N., Yakushiji, F., Suzuki, S., Tomiyama, J., Uchida, T., & Taniguchi, K. (2008). IL-12 and IL-18 Induction and Subsequent NKT Activation Effects of the Japanese Botanical Medicine Juzentaihoto. International Journal of Molecular Sciences, 9(7), 1142-1155. https://doi.org/10.3390/ijms9071142