Abstract
Nonsyndromic cleft lip with or without cleft palate (NSCL ± P) is strongly associated with both environmental and genetic risk factors, but its genetic underpinnings remain partially known. While variants in interferon regulatory factor 6 (IRF6) are linked to NSCL ± P risk in populations from Asia and Europe, studies on the highly admixed Brazilian population are scarce and have produced ambiguous results. This study aimed to investigate the contribution of IRF6 variants to the risk of NSCL ± P. Five tag-single nucleotide polymorphisms (rs599021, rs2073485, rs2235375, rs7552506, and rs642961) were analyzed in a large multicenter cohort composed of 1006 patients with NSCL ± P and 942 healthy controls. Statistical analyses involved multiple logistic regression tests consideration the tri-hybrid genetic origin of the Brazilian population, under a Bonferroni p value correcting for multiple comparisons. The A allele (OR: 1.43, 95% CI: 1.22–1.67, p < 0.0001) and AA genotype (OR: 2.04, 95% CI: 1.46–2.86, p < 0.0001) frequencies of rs642961 were significantly associated with NSCL ± P risk. Stratified analyses indicated that the variant is associated with susceptibility to both nonsyndromic cleft lip only (NSCLO) and nonsyndromic cleft lip and palate (NSCLP). However, the association with NSCLO was primarily observed in patients with high African ancestry, whereas the association with NSCLP was predominantly seen in patients with high European ancestry. No significant associations were found for the other investigated variants. Our results support the notion that the IRF6 rs642961 variant represents a marker of susceptibility to NSCL ± P in the Brazilian population, and that genetic ancestry composition plays a central role in the association with the cleft type.
1. Introduction
Orofacial cleft, the most prevalent malformation affecting the face, results from fusion failures of the facial processes during early embryogenesis. Depending on the process involved in the failure, it is classified as cleft lip only (CLO), involving lack of fusion between the medial nasal and maxillary processes, cleft palate only (CPO), represented by non-fusion of the palatal shelves, which develop as bilateral outgrowths from the maxillary processes, or cleft lip and palate (CLP), due to nonunion of all these facial processes [1]. The similarities in both epidemiologic features and embryologic timing allows the combination of CLO and CLP in a unique group, called cleft lip with or without cleft palate (CL ± P). The majority of cases (approximately 70% of cases of CL ± P and 50% of cases of CPO) are isolated and sporadic in occurrence and classified as nonsyndromic, whereas the presence of rare genetic mutations characterizes the syndromic forms of orofacial clefts [2]. The incidence of nonsyndromic orofacial clefts is influenced by diverse factors, such as ethnicity, environmental exposures and socioeconomic status, and ranges from 1:500 to 1:2500 newborns [3].
The etiopathogenesis of nonsyndromic orofacial clefts is credited to a complex interplay of genetic, epigenetic, and environmental factors [4]. In recent decades, a plethora of studies, adopting varied genetic approaches, have identified diverse genes and loci of susceptibility to nonsyndromic orofacial clefts. Among the first described genes was interferon regulatory factor 6 (IRF6). Historically, IRF6 was targeted for investigation in nonsyndromic CL ± P (NSCL ± P) after mutations were detected in patients with Van der Woude syndrome, a Mendelian disorder that may include orofacial cleft in its clinical spectrum. The first study revealed an association of the genetic polymorphic variant rs2235371 with NSCL ± P [5], but a later study by the same group demonstrated the association of rs2235371 with NSCL ± P dependents on rs642961, a single nucleotide polymorphism (SNP) that abrogates the transcription factor AP-2a binding site in the promoter of IRF6 [6]. The association of rs642961 with NSCL ± P has been frequently replicated in Asian and European populations [7,8,9,10], but it was not confirmed in studies involving populations from Africa [11,12], Iran [13], Yemen [14] and Honduras [15], or in Hispanic and non-Hispanic white individuals living in the United States [16]. The association of IRF6 with NSCL ± P in the Brazilian population remains uncertain [17,18,19,20,21]. Together these findings provide evidence of the influence of ancestral origin on IRF6 risk, and highlight the importance of identifying both IRF6 common and population-specific candidate clinical variants of NSCL ± P. Accordingly, a recent study demonstrated that the IRF6 variant rs570516915, which is highly enriched in the Finnish population, is a risk factor for NSCPO [22].
Brazil, with a population surpassing 210 million, has one of the most genetically heterogeneous populations in the world, which is the result of more than 500 years of interethnic admixture between Native Americans, European colonizers, and African slaves [23]. The clinical influence of the genomic profile of the individual in the susceptibility of common and rare diseases has been demonstrated in different situations [24], including that of NSCL ± P [25]. The aim of the current study was to investigate the potential association of IRF6 genetic variants, selected by the tag-SNP strategy and represented by rs599021, rs2073485, rs2235375, rs7552506, and rs642961, with NSCL ± P in a large multicenter Brazilian case-control cohort.
2. Results
This study included 1006 patients with NSCL ± P, with 273 affected by NSCLO and 733 affected by NSCLP, and 942 healthy controls. There were no significant differences in genomic ancestry between the NSCL ± P group and controls. However, the NSCL ± P group included more men (56.7% vs. 46.5%; p < 0.0001) than the control group, and this difference was driven by the high proportion of males with NSCLP (Table 1). The genotyping call rate ranged from 98.4% to 99.7%, and the concordance in the validation sample, which was genotyped twice, was 100%. The genotype distributions of all variants adhered to HWE (Table 2).

Table 1.
Characteristics of the patients included in the study.
Table 2.
Characteristics of single nucleotide polymorphisms (SNP) in IRF6, including genome location, function, major and minor (in bold) alleles, genotyping call rate, and p value of the Hardy–Weinberg equilibrium (HWE) test.
Multiple logistic regression analyses considering the differences in sex and genomic ancestry proportions were used to compare allele and genotype distributions between the NSCL ± P and control groups. Although the SNP rs599021 has demonstrated some associations with a nominal p value (p < 0.05), only rs642961 was found to be associated with NSCL ± P risk, after adopting a p value for multiple comparisons of ≤0.01. The other SNPs (rs2073485, rs2235275, and rs7552506) showed no significant associations with NSCL ± P susceptibility (Table 3). Power analysis showed very good statistical power to detect association with the current sample size for all SNPs. The only variant that did not reach >99% was rs2235375, with a power of 84.6%.
Table 3.
Associations of IRF6 variants with the risk of nonsyndromic cleft lip with or without cleft palate (NSCL ± P). The values of p were adjusted for covariates (sex and genomic ancestry) by logistic regression analysis.
The presence of the rs642961 A allele was associated with an increased risk of NSCL ± P (OR:1.43, 95% CI: 1.22–1.67, p < 0.0001). Patients carrying the AA genotype exhibited a higher risk of NSCL ± P (OR: 2.04, 95% CI: 1.46–2.86, p < 0.0001), and both dominant (OR: 1.35, 95% CI: 1.12–1.64, p = 0.002) and recessive models (OR: 1.96, 95% CI: 1.40–2.72, p < 0.0001) further indicated an increased risk for NSCL ± P (Table 3). Next, we calculated the population attributable fraction (PAF), representing the proportion of NSCL ± P due to rs642961 A allele. The PAF for heterozygous carriers (GA genotype) was 7.47%, and for homozygous carriers (AA genotype) it was 25.92%.
To further explore the allele and genotype contribution of IRF6 variants to NSCL ± P susceptibility, a stratified analysis considering type of cleft was performed. The findings indicate that the A allele of rs642961 was associated with a significantly higher susceptibility to NSCLO (OR: 1.40, 95% CI: 1.11–1.77, p = 0.003) and NSCLP (OR: 1.44, 95% CI: 1.21–1.70, p < 0.0001) compared to the G allele (Table 4). For NSCLO, the AA genotype (OR: 1.92, 95% CI: 1.18–3.11, p = 0.01) and the recessive genetic model (GG + GA vs. AA) also showed a significant association (OR: 1.81, 95% CI: 1.13–2.91, p = 0.01), whereas the higher susceptibility to NSCLP was confirmed with the AA genotype (OR: 2.09, 95% CI: 1.46–2.99, p < 0.0001) and in the dominant (OR: 1.35, 95% CI: 1.09–1.66, p = 0.004) and recessive (OR: 2.01, 95% CI: 1.41–2.86, p < 0.0001) genetic models (Table 4).
Table 4.
Distribution of the IRF6 variants in nonsyndromic cleft lip only (NSCLO) and nonsyndromic cleft lip and palate (NSCLP). The p values were adjusted for covariates (sex and genomic ancestry) by logistic regression.
To strengthen our understanding of the contribution of rs642961 to NSCL ± P risk, ancestry-stratified analysis was performed, revealing noteworthy and specific associations for rs642961 (Table 5). For this analysis, aligning with the pioneer strategy proposed by Pena and collaborators [26], which has been successfully adopted by us in previous studies [27,28], individuals whose genome demonstrated a predominance of more than 20% African genetic markers were designated as having a high African ancestral background. Conversely, individuals whose genome exhibited high European markers and less than 20% of African markers were classified as possessing a high European ancestral background. The present results revealed that the association of the A allele (OR: 1.35, 95% CI: 1.14–1.61, p = 0.0006) with increased risk of NSCL ± P in patients exhibiting high European ancestry is due to the frequency of this allele in patients with NSCLP (OR: 1.40, 95% CI: 1.16–1.70, p = 0.0004). On the other hand, the susceptibility of NSCL ± P (OR: 1.79, 95% CI: 1.25–2.56, p = 0.001) in patients with high African ancestry is related to the predominance of the variant allele in NSCLO (OR: 2.32, 95% CI: 1.44–3.74, p = 0.0005).
Table 5.
Stratified analysis of IRF6 rs642961 based on ancestry of the samples. Samples were divided in relation to the genomic ancestry in high European genomic ancestry or high African genomic ancestry. The p values were adjusted for sex by logistic regression analysis.
3. Discussion
Although the mechanisms leading to the disruption of the embryological processes resulting in nonsyndromic orofacial clefts are complex and multifactorial, our understanding of the genetic components is evolving. To date, more than 50 loci/genes have been associated with nonsyndromic orofacial clefts, with many being validated in independent studies on diverse populations [29]. The validation of candidate variants for nonsyndromic orofacial clefts is essential, particularly in admixed populations such as the Brazilian population, because this allows an accurate estimation of the influence of population structure, avoiding the misinterpretation of risk scores calculated for other populations. After the identification that the common IRF6 rs642961 variant is related to increased odds for NSCL ± P, several studies explored its susceptibility and that of other IRF6 SNPs in the Brazilian population. The different genotyping methods, the small sample sizes, and the lack of control over the inference of the ancestry structure of the samples produced inconsistent and contradictory results. After combining the tag-SNP strategy, a large and multicenter sample and statistical analyses controlling individual ancestry structure, the results of the current study revealed that the presence of the rs642961 variant A allele increased the risk of NSCL ± P in the admixed Brazilian population.
The first Brazilian study exploring the association of IRF6 variants with NSCL ± P risk was reported by Paranaiba and colleagues in 2010 [17]. This study examined the variants rs2235371 and rs642961 in 177 samples of NSCL ± P and 126 controls by restriction fragment length polymorphism analysis, and revealed a lack of involvement of these IRF6 polymorphisms with NSCL ± P. Brito et al. [18] found that the A allele of rs642961 was not associated with NSCL ± P, but stratified analysis by cleft type showed a significant association with NSCLO, but not NSCLP. Interestingly, the authors discussed that the association was probably driven by the patients with cleft from a specific region of Brazil, where heritability was estimated to have an important influence on NSCL ± P risk. However, the patients with NSCLO in this cohort showed a higher African ancestry contribution than individuals of the control group. In a sample derived from subjects born in Bahia state, the Brazilian state with the highest historical immigration of Africans and a population that has the highest proportion of African genomic ancestry in Brazil, do Rego Borges et al. [19] observed that the frequency of the A risk allele of rs642961 was higher in the NSCL ± P group compared to the control group, but the significance did not withstand Bonferroni correction for multiple tests. The study conducted by Souza et al. [20], exploring 259 triads with patients with nonsyndromic orofacial clefts and their parents, which has the advantage of minimizing influence differences in the population stratification within and between groups, revealed that rs642961 is not associated with NSCL ± P in the Brazilian population, though the haplotype composed of the G allele of rs2235771 and the A allele of rs642961 was overtransmitted to patients when all types of clefts (NSCLO, NSCPO, and NSCLP) were combined. Bezerra et al. [21] observed no association between rs642961 and NSCL ± P, but the minor allele of rs2235771, which is frequently found in strong disequilibrium of linkage with rs642961, was associated with increased risk for NSCPO, but not NSCL ± P. However, the study included only 38 samples of NSCPO, and the p value was not corrected by multiple comparisons. Altogether, the variability of the results of the previous studies contrasting with the robust results reported here suggest that the lack of power of the samples may have limited the determination of the magnitude of the effects of rs642961 in previous studies. The result of the meta-analysis with these previous studies exploring rs642961 in the Brazilian population reinforces this evidence (Figure 1). The combination of 1089 samples of NSCL ± P and 1038 controls revealed low heterogeneity in the frequencies of the alleles across the individual studies, and yielded a pooled OR of 1.30 (95% CI: 1.08–1.56, p = 0.005).
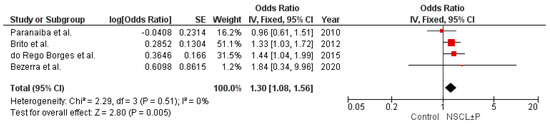
Figure 1.
Forest plot for the variant allele distribution of IRF6 rs642961 in the studies with the Brazilian population [17,18,19,21]. The meta-analysis was conducted using the Review Manager (RevMan, version 5.4.1, Cochrane), applying an inverse variance method with fixed effect model (I2 < 50%). The square markets indicate the odds ratio of the A allele for different studies, and the size of the marker correlates to the inverse variance of the effect estimate and indicates the weight of the study. The diamond data market indicates the pooled effect.
The studies presented here also revealed that the ancestry composition influences the association of rs642961 with the type of cleft. In the sample with high European ancestry, the susceptibility of the A allele was with NSCLP but not with NSCLO, whereas the association in patients with high African ancestry was only with NSCLO. In a population of more than 210 million, the highly heterogeneous and admixed structure constructed over 500 years of marriages from individuals from three main different roots (Amerindians, Europeans, and Africans) represents a factor with direct implications on the modulation of genetic risk factors for nonsyndromic orofacial clefts. However, this is the first study to show that genomic ancestry impacts on the association of a specific genetic variant with the type of cleft. The investigation of potential associations of NSCL ± P susceptibility signals identified by genome-wide studies in the Brazilian population revealed that rs227731 at 17q22, which may have regulatory effects on the NOG gene, a potent antagonist of bone morphogenetic proteins (BMP), and rs742071, an intronic variant of the PAX7 gene at 1p36, are associated with NSCL ± P in the Brazilian population due to the high frequency of the minor alleles in individuals of European ethnic background. On the other hand, rs1873147 at 15q22.2, an SNP located in an intergenic region that contains important sites with transcription activity, is involved in the pathogenesis of NSCL ± P in patients with a high percentage of African ancestry [25]. The variants rs3758249 at 9q22 and rs7078160 at 10q25.3 were reported as susceptibility loci for NSCL ± P in this Brazilian population with high African ancestry [19], which contrasts with a finding of no association of them with NSCL ± P in a Brazilian cohort with high European ancestry [30]. Likewise, the BMP rs2761887 polymorphism was only significantly associated with NSCL ± P in the Brazilian population enriched by African ancestry [28]. Collectively, these findings strongly support the notion that the intrinsic heterogeneity of the Brazilian population must be acknowledged in the design and interpretation of studies exploring the genetic basis of NSCL ± P. It is important to consider that the ancestry contribution of the subjects included in this study are in line with population genetic studies in Brazilians reporting most individuals have significant degrees of European and/or African ancestry, while Amerindian ancestry is mainly found in individuals of specific regions of Brazil [24,31].
It is important to recognize that the study has limitations and strengths. The multicenter design, enrolling samples from four of the five macroregions of Brazil, is at the same time a strength and a limitation. This approach brings a better representation of the Brazilian population, but the great variability among the different regions from which the samples were collected, particularly in relation to environment factors, potential gene-gene and gene-environment interactions, and heritability, may have influenced the results and the study was unable to control for these factors. Stratification of the sample is always related to loss of power, but in this particular situation, it did not prevent the identification of significant signals for both NSCLO and NSCLP. The strengths of the study include the use of a large sample size, the application of tag-SNP, which covered the presentative regions of IRF6, and a robust statistical approach with control for confounding effects including sex and ancestry proportions, with application of correction for multiple comparison tests.
4. Materials and Methods
4.1. Study Participants
This multicenter case-control study included patients with NSCL ± P and controls from four of the five Brazilian macroregions, who were recruited in the context of the Brazilian Oral Cleft Group (BOCG), a collaborative consortium committed to study risk factors associated with orofacial clefts. The centers associated with BOCG include the Centrinho do Hospital Santo Antônio das Obras Sociais Irmã Dulce in Salvador, Bahia, situated in the northeast region of Brazil; the Centro Pró-Sorriso at Hospital Alzira Velano, UNIFENAS, in Alfenas, Minas Gerais, located in the southeastern region; the Associação de Portadores de Fissura Lábio Palatal (APOFILAB) in Cascavel, Paraná, and the Centro de Atendimento Integral ao Fissurado Labiopalatal (CAIF) in Curitiba, both situated in the southern region, and the Centro de Reabilitação de Fissuras Orais do Hospital Geral e Maternidade de Cuiabá, located in the central-western region of Brazil. In those centers, all patients were screened to detect and exclude those with signs and symptoms of syndromes, and then only patients with NSCL ± P were included in the current study. The controls consisted of Brazilian individuals without orofacial cleft, family history of orofacial cleft or congenital abnormalities, from the same geographical areas as the cases. Control subjects were not related to the participating patients. The study protocol was approved by the institutional Research Ethics Committee (CAAE: 08452819.0.0000.5418), and all participants or their parents or legal guardians provided written informed consent.
4.2. Sample Size Estimation
For estimation of the sample size needed to reach a power of 80%, the Quanto software (version 1.2.4, [32]) was used. The calculation was performed with the following parameters: unmatched case-control study, gene only analysis, additive inheritance model, genetic effect of 1.3, minor allele frequency (MAF) of 0.137 (13.7%), two-sided type I error of 0.05, and Brazilian population risk (prevalence) of 0.00147. The genetic effect and MAF were calculated after a meta-analysis of four previous studies that explored rs642961 (details in the legend of Figure 1), the only IRF6 variant studied more than once in the Brazilian population [17,18,19,21]. With these parameters, the sample size required was 881 per group. The study included samples from 1006 patients with NSCL ± P and 942 healthy controls.
4.3. Genetic Polymorphism Selection
The selection of SNPs was performed using the tag-SNP approach to identify representative polymorphisms in IRF6. After configuring the Tagger program [33] to a pairwise algorithm, with a r2 ≥ 0.80 and MAF ≥ 0.10, 5 independent blocks exhibited genetic disequilibrium. From these blocks, we carefully selected the SNPs with the highest MAF value, giving preference to those that had undergone previous scrutiny in nonsyndromic orofacial clefts. The primary attributes of each SNP are depicted in Table 2.
4.4. SNP Genotyping
Desquamated oral mucosal cells obtained from oral swabs were subjected to genomic DNA extraction using a salt-out protocol previously described [34]. After DNA concentration determination using the NanoDrop™ 2000 spectrophotometer (Thermo Fisher Scientific, Waltham, MA, USA), 5 ng of genomic DNA were subjected to SNP genotyping with TaqMan 5′-exonuclease allelic discrimination assays (Assay-on-Demand, Applied Biosystems, Waltham, MA, USA) in the StepOnePlus real-time platform, following the manufacturer’s directions. For quality control, 10% of the samples were randomly selected and the reaction repeated.
4.5. Assessment of Genomic Ancestry
To determine the ancestral lineage of each individual, a panel of 40 biallelic short insertion–deletion polymorphisms (INDELs), previously validated as reliable indicators of ancestry within the Brazilian population [35], was genotyped and integrated into the analysis [36]. The Structure software (version 2.3.4) was employed to unravel the genomic ancestry inherent in each participant. This analytical process involved the application of a K = 3 model, duly considering the tri-hybrid origin that characterizes the Brazilian population.
4.6. Statistical Analysis
To evaluate the Hardy–Weinberg equilibrium (HWE) and differences in sex distribution, the chi-square test was applied. Proportions of genomic ancestry across groups were subjected to comparison using the Mann–Whitney test. To conduct multiple logistic regression analyses, the SNPassoc package (version 2.1-2) within the Rstudio program (version 3.5.1) [37] was used. These analyses were performed under unrestricted, dominant, and recessive genetic models. Statistical significance after Bonferroni correction for multiple comparisons was defined as p ≤ 0.01.
Power for detecting a p value ≤ 0.05 for each variant was calculated in the Quanto software (version 1.2.4, [32]), assuming a prevalence of NSCL ± P in Brazil of 0.00146 [38] and using the most conservative odd ratios (OR) reported in the literature. For rs2235375, the OR was derived from the meta-analysis performed by Golshan-Tafti et al. [39]. The population attributable fraction for rs642961 was calculated using Levin’s formula [40].
5. Conclusions
The findings of the current study ultimately provide evidence that the rs642961 polymorphism is associated with a significantly increased risk for NSCL ± P at both the allele and the genotype levels. The stratified analysis revealed that the association with NSCLO was driven by patients with high African ancestry and the association with NSCLP was dependent on patients with high European background. These findings not only enrich our understanding of the genetic basis of NSCL ± P, but also offer opportunities to dissect the roles of different IRF6 variants in the pathogenesis of this common and distressing congenital disease in admixed populations, such as those from the Latin American countries.
Author Contributions
Conceptualization, R.A.M., H.M.-J. and R.D.C.; methodology, R.A.M.; formal analysis, R.A.M. and R.D.C.; investigation, R.A.M. and R.D.C.; resources, D.R.B.M., S.R.d.A.R., L.E.R.V., R.S., J.F.-S., A.L.C.A.R. and Brazilian Oral Cleft Group; data curation, R.A.M., H.M.-J. and R.D.C.; writing—original draft preparation, R.A.M. and R.D.C.; writing—review and editing, all authors; supervision, R.D.C.; project administration, R.D.C.; funding acquisition, H.M.-J. and R.D.C. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by a research grant from the National Council for Scientific and Technological Development-CNPq (process #402994/2023-0 for R.D.C.), and from the Minas Gerais State Research Foundation-FAPEMIG (processes # APQ-00961-22 for D.R.B.M. and # RED-00073-23 for H.M.-J.).
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki. The study protocol was initially approved by each center associated to the Brazilian Oral Cleft Group, and then approved by the National Research Ethics Committee (CAAE: 08452819.0.0000.5418).
Informed Consent Statement
Informed consent was obtained from all subjects or their parents or legal guardians involved in the study.
Data Availability Statement
The data to support the findings of this study will be available on request from the corresponding author.
Conflicts of Interest
The authors declare no competing interests.
References
- Hammond, N.L.; Dixon, M.J. Revisiting the embryogenesis of lip and palate development. Oral Dis. 2022, 28, 1306–1326. [Google Scholar] [PubMed]
- Coletta, R.D.; Sunavala-Dossabhoy, G. Orofacial clefts: A compendium on non-syndromic cleft lip-cleft palate. Oral Dis. 2022, 28, 1301–1304. [Google Scholar]
- Dixon, M.J.; Marazita, M.L.; Beaty, T.H.; Murray, J.C. Cleft lip and palate: Understanding genetic and environmental influences. Nat. Rev. Genet. 2011, 12, 167–178. [Google Scholar] [PubMed]
- Alade, A.; Awotoye, W.; Butali, A. Genetic and epigenetic studies in non-syndromic oral clefts. Oral Dis. 2022, 28, 1339–1350. [Google Scholar] [CrossRef]
- Zucchero, T.M.; Cooper, M.E.; Maher, B.S.; Daack-Hirsch, S.; Nepomuceno, B.; Ribeiro, L.; Caprau, D.; Christensen, K.; Suzuki, Y.; Machida, J.; et al. Interferon regulatory factor 6 (IRF6) gene variants and the risk of isolated cleft lip or palate. N. Engl. J. Med. 2004, 351, 769–780. [Google Scholar]
- Rahimov, F.; Marazita, M.L.; Visel, A.; Cooper, M.E.; Hitchler, M.J.; Rubini, M.; Domann, F.E.; Govil, M.; Christensen, K.; Bille, C.; et al. Disruption of an AP-2alpha binding site in an IRF6 enhancer is associated with cleft lip. Nat. Genet. 2008, 40, 1341–1347. [Google Scholar] [CrossRef] [PubMed]
- Mostowska, A.; Hozyasz, K.K.; Wojcicki, P.; Biedziak, B.; Paradowska, P.; Jagodzinski, P.P. Association between genetic variants of reported candidate genes or regions and risk of cleft lip with or without cleft palate in the polish population. Birth Defects Res. A Clin. Mol. Teratol. 2010, 88, 538–545. [Google Scholar]
- Zhou, Q.; Li, M.; Zhu, W.; Guo, J.; Wang, Y.; Li, Y.; Li, S. Association between interferon regulatory factor 6 gene polymorphisms and nonsyndromic cleft lip with or without cleft palate in a chinese population. Cleft Palate Craniofac J. 2013, 50, 570–576. [Google Scholar] [CrossRef]
- Pegelow, M.; Koillinen, H.; Magnusson, M.; Fransson, I.; Unneberg, P.; Kere, J.; Karsten, A.; Peyrard-Janvid, M. Association and Mutation Analyses of the IRF6 Gene in Families With Nonsyndromic and Syndromic Cleft Lip and/or Cleft Palate. Cleft Palate Craniofac J. 2014, 51, 9–55. [Google Scholar]
- Wu-Chou, Y.H.; Lu, Y.C.; Chen, K.P.; Chang, H.F.; Lin, Y.T.; Lo, L.J. Association Studies Between Regulatory Regions of IRF6/TP63 Genes and Nonsyndromic Oral Clefts. Cleft Palate Craniofac. J. 2019, 56, 778–785. [Google Scholar]
- Butali, A.; Mossey, P.A.; Adeyemo, W.L.; Jezewski, P.A.; Onwuamah, C.K.; Ogunlewe, M.O.; Ugboko, V.I.; Adejuyigbe, O.; Adigun, A.I.; Abdur-Rahman, L.O.; et al. Genetic studies in the Nigerian population implicate an MSX1 mutation in complex oral facial clefting disorders. Cleft Palate Craniofac J. 2011, 48, 646–653. [Google Scholar]
- Figueiredo, J.C.; Ly, S.; Raimondi, H.; Magee, K.; Baurley, J.W.; Sanchez-Lara, P.A.; Ihenacho, U.; Yao, C.; Edlund, C.K.; van den Berg, D.; et al. Genetic risk factors for orofacial clefts in Central Africans and Southeast Asians. Am. J. Med. Genet. A 2014, 164A, 2572–2580. [Google Scholar] [PubMed]
- Nouri, N.; Memarzadeh, M.; Carinci, F.; Cura, F.; Scapoli, L.; Nouri, N.; Jafary, F.; Sedghi, M.; Sadri, L.; Salehi, M. Family-based association analysis between nonsyndromic cleft lip with or without cleft palate and IRF6 polymorphism in an Iranian population. Clin. Oral Investig. 2015, 19, 891–894. [Google Scholar]
- Aldhorae, K.A.; Böhmer, A.C.; Ludwig, K.U.; Esmail, A.H.; Al-Hebshi, N.N.; Lippke, B.; Gölz, L.; Nöthen, M.M.; Daratsianos, N.; Knapp, M.; et al. Nonsyndromic cleft lip with or without cleft palate in arab populations: Genetic analysis of 15 risk loci in a novel case-control sample recruited in Yemen. Birth Defects Res. A Clin. Mol. Teratol. 2014, 100, 307–313. [Google Scholar]
- Larrabee, Y.C.; Birkeland, A.C.; Kent, D.T.; Flores, C.; Su, G.H.; Lee, J.H.; Haddad, J., Jr. Association of common variants, not rare mutations, in IRF6 with nonsyndromic clefts in a Honduran population. Laryngoscope 2011, 121, 1756–1759. [Google Scholar] [PubMed]
- Blanton, S.H.; Burt, A.; Garcia, E.; Mulliken, J.B.; Stal, S.; Hecht, J.T. Ethnic heterogeneity of IRF6 AP-2a binding site promoter SNP association with nonsyndromic cleft lip and palate. Cleft Palate Craniofac J. 2010, 47, 574–577. [Google Scholar] [PubMed]
- Paranaíba, L.M.; Bufalino, A.; Martelli-Júnior, H.; de Barros, L.M.; Graner, E.; Coletta, R.D. Lack of association between IRF6 polymorphisms (rs2235371 and rs642961) and non-syndromic cleft lip and/or palate in a Brazilian population. Oral Dis. 2010, 16, 193–197. [Google Scholar]
- Brito, L.A.; Bassi, C.F.; Masotti, C.; Malcher, C.; Rocha, K.M.; Schlesinger, D.; Bueno, D.F.; Cruz, L.A.; Barbara, L.K.; Bertola, D.R.; et al. IRF6 is a risk factor for nonsyndromic cleft lip in the Brazilian population. Am. J. Med. Genet. A 2012, 158A, 2170–2175. [Google Scholar]
- do Rego Borges, A.; Sá, J.; Hoshi, R.; Viena, C.S.; Mariano, L.C.; de Castro Veiga, P.; Medrado, A.P.; Machado, R.A.; de Aquino, S.N.; Messetti, A.C.; et al. Genetic risk factors for nonsyndromic cleft lip with or without cleft palate in a Brazilian population with high African ancestry. Am. J. Med. Genet. A 2015, 167A, 2344–2349. [Google Scholar]
- de Souza, L.T.; Kowalski, T.W.; Ferrari, J.; Monlléo, I.L.; Ribeiro, E.M.; de Souza, J.; Fett-Conte, A.C.; de Araujo, T.K.; Gil-da-Silva-Lopes, V.L.; Ribeiro-Dos-Santos, Â.K.; et al. Study of IRF6 and 8q24 region in non-syndromic oral clefts in the Brazilian population. Oral Dis. 2016, 22, 241–245. [Google Scholar]
- Bezerra, J.F.; Silva, H.P.V.D.; Bortolin, R.H.; Luchessi, A.D.; Ururahy, M.A.G.; Loureiro, M.B.; Gil-da-Silva-Lopes, V.L.; Almeida, M.D.G.; Amaral, V.S.D.; Rezende, A.A. IRF6 polymorphisms in Brazilian patients with non-syndromic cleft lip with or without palate. Braz. J. Otorhinolaryngol. 2020, 86, 696–702. [Google Scholar] [PubMed]
- Rahimov, F.; Nieminen, P.; Kumari, P.; Juuri, E.; Nikopensius, T.; Paraiso, K.; German, J.; Karvanen, A.; Kals, M.; Elnahas, A.G.; et al. High incidence and geographic distribution of cleft palate in Finland are associated with the IRF6 gene. Nat. Commun. 2024, 15, 9568. [Google Scholar]
- Souza, A.M.; Resende, S.S.; Sousa, T.N.; Brito, C.F.A. A systematic scoping review of the genetic ancestry of the Brazilian population. Genet. Mol. Biol. 2019, 42, 495–508. [Google Scholar] [PubMed]
- Pereira, F.D.S.C.F.; Guimarães, R.M.; Lucidi, A.R.; Brum, D.G.; Paiva, C.L.A.; Alvarenga, R.M.P. A systematic literature review on the European, African and Amerindian genetic ancestry components on Brazilian health outcomes. Sci. Rep. 2019, 9, 8874. [Google Scholar]
- de Aquino, S.N.; Messetti, A.C.; Hoshi, R.; Borges, A.; Viena, C.S.; Reis, S.R.; Oliveira Swerts, M.S.; Graner, E.; Martelli-Júnior, H.; Coletta, R.D. Analysis of susceptibility polymorphisms for nonsyndromic cleft lip with or without cleft palate in the Brazilian population. Birth Defects Res. A Clin. Mol. Teratol. 2014, 100, 36–42. [Google Scholar]
- Pena, S.D.; Di Pietro, G.; Fuchshuber-Moraes, M.; Genro, J.P.; Hutz, M.H.; de Souza Kehdy, F.; Kohlrausch, F.; Magno, L.A.; Montenegro, R.C.; Moraes, M.O.; et al. The genomic ancestry of individuals from different geographical regions of Brazil is more uniform than expected. PLoS ONE 2011, 6, e17063. [Google Scholar]
- Machado, R.A.; de Oliveira, L.Q.R.; Rangel, A.L.C.A.; Reis, S.R.A.; Scariot, R.; Martelli, D.R.B.; Martelli-Júnior, H.; Coletta, R.D. Brazilian Multiethnic Association Study of Genetic Variant Interactions among FOS, CASP8, MMP2 and CRISPLD2 in the Risk of Nonsyndromic Cleft Lip with or without Cleft Palate. Dent. J. 2022, 11, 7. [Google Scholar] [CrossRef]
- Rocha de Oliveira, L.Q.; de Souza Nicolau, H.C.; Barbosa Martelli, D.R.; Martelli-Júnior, H.; Scariot, R.; Ayroza Rangel, A.L.C.; de Almeida Reis, S.R.; Coletta, R.D.; Machado, R.A. Ethnic Differences in the Brazilian Population Influence the Impact of BMP4 Genetic Variants on Susceptibility of Nonsyndromic Orofacial Clefts. Cleft Palate Craniofac J. 2024, 61, 1701–1712. [Google Scholar]
- Jia, Z.; Mukhopadhyay, N.; Yang, Z.; Butali, A.; Sun, J.; You, Y.; Yao, M.; Zhen, Q.; Ma, J.; He, M.; et al. Multi-ancestry Genome Wide Association Study Meta-analysis of Non-syndromic Orofacial Clefts. medRxiv 2024. [Google Scholar] [CrossRef]
- Bagordakis, E.; Paranaiba, L.M.; Brito, L.A.; de Aquino, S.N.; Messetti, A.C.; Martelli-Junior, H.; Swerts, M.S.; Graner, E.; Passos-Bueno, M.R.; Coletta, R.D. Polymorphisms at regions 1p22.1 (rs560426) and 8q24 (rs1530300) are risk markers for nonsyndromic cleft lip and/or palate in the Brazilian population. Am. J. Med. Genet. A 2013, 161A, 1177–1180. [Google Scholar]
- Pena, S.D.J.; Santos, F.R.; Tarazona-Santos, E. Genetic admixture in Brazil. Am. J. Med. Genet. C Semin. Med. Genet. 2020, 184, 928–938. [Google Scholar] [CrossRef] [PubMed]
- Gauderman, W.J. Sample size requirements for matched case-control studies of gene-environment interaction. Stat Med. 2002, 21, 35–50. [Google Scholar] [CrossRef] [PubMed]
- de Bakker, P.I.; Yelensky, R.; Pe’er, I.; Gabriel, S.B.; Daly, M.J.; Altshuler, D. Efficiency and power in genetic association studies. Nat. Genet. 2005, 37, 1217–1223. [Google Scholar] [CrossRef]
- Aidar, M.; Line, S.R. A simple and cost-effective protocol for DNA isolation from buccal epithelial cells. Braz. Dent. J. 2007, 18, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Bastos-Rodrigues, L.; Pimenta, J.R.; Pena, S.D. The genetic structure of human populations studied through short insertion-deletion polymorphisms. Ann. Hum. Genet. 2006, 70, 658–665. [Google Scholar] [CrossRef]
- Messetti, A.C.; Machado, R.A.; de Oliveira, C.E.; Martelli-Júnior, H.; de Almeida Reis, S.R.; Moreira, H.S.; Persuhn, D.C.; Wu, T.; Coletta, R.D. Brazilian multicenter study of association between polymorphisms in CRISPLD2 and JARID2 and non-syndromic oral clefts. J. Oral Pathol. Med. 2017, 46, 232–239. [Google Scholar] [CrossRef]
- RStudio Team. RStudio: Integrated Development for R; RStudio, PBC: Boston, MA, USA, 2020; Available online: http://www.rstudio.com/.
- Martelli-Junior, H.; Porto, L.V.; Martelli, D.R.; Bonan, P.R.; Freitas, A.B.; Della Coletta, R. Prevalence of nonsyndromic oral clefts in a reference hospital in the state of Minas Gerais, Brazil, between 2000–2005. Braz. Oral Res. 2007, 21, 314–317. [Google Scholar] [CrossRef]
- Golshan-Tafti, M.; Dastgheib, S.A.; Bahrami, R.; Aarafi, H.; Foroughi, E.; Mirjalili, S.R.; Kheirandish, N.; Aghasipour, M.; Shiri, A.; Azizi, S.; et al. A comprehensive consolidation of data on the relationship between IRF6 polymorphisms and non-syndromic cleft lip/palate susceptibility: From 79 case-control studies. J. Stomatol. Oral Maxillofac. Surg. 2024, 125, 101809. [Google Scholar] [CrossRef]
- Levin, M.L. The occurrence of lung cancer in man. Acta Unio Int. Contra Cancrum. 1953, 9, 531–541. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).