
Cardiovascular Biomarkers: Tools for Precision Diagnosis and Prognosis
 , ,
, ,
Abstract
1. Introduction
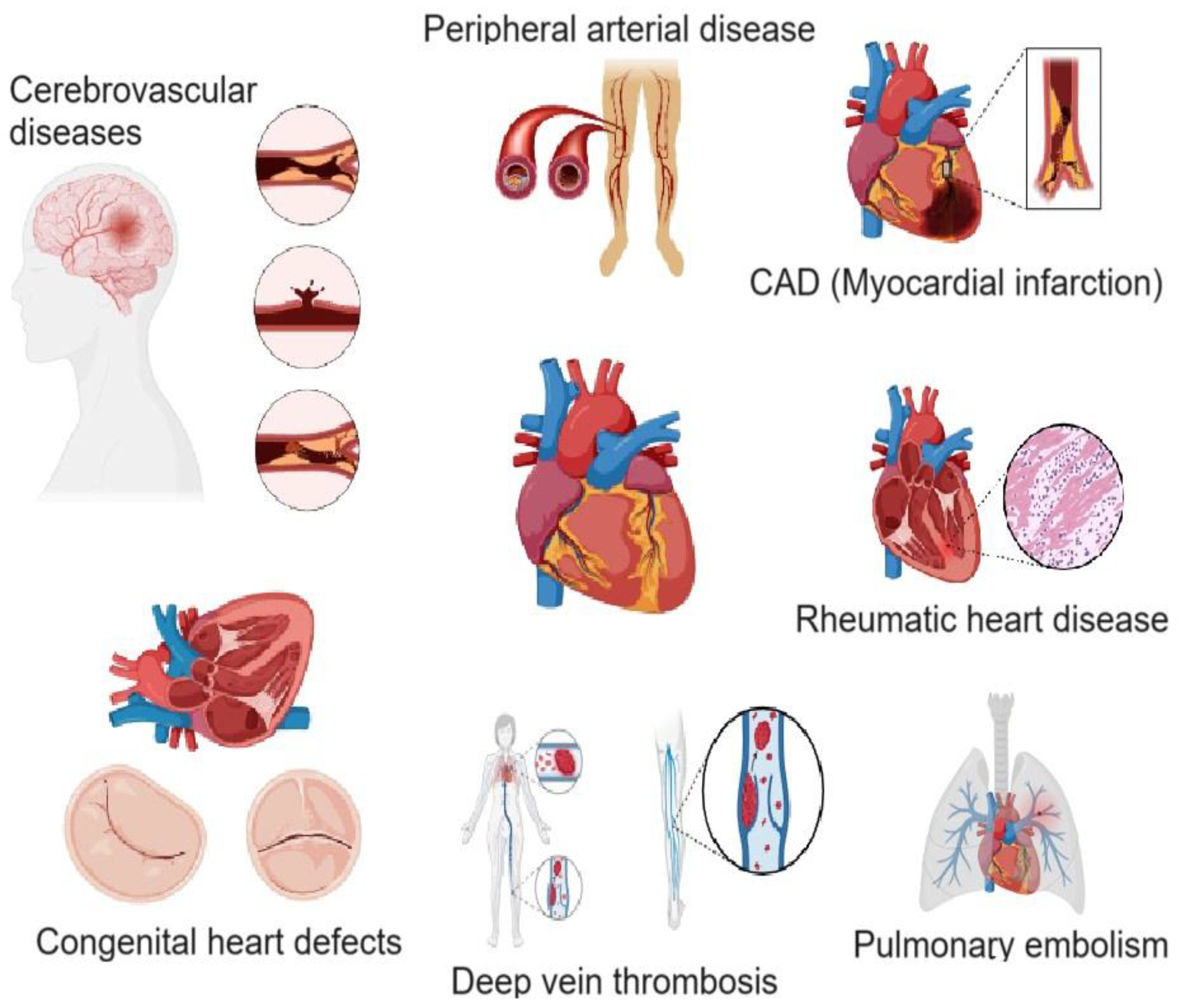
2. Cardiovascular Diseases
3. Diagnosis of CVDs and the Role of Biomarkers
4. Cardiac Biomarkers
4.1. Aspartate Aminotransferase (AST)
4.2. Creatine Kinase MB (CK-MB)
4.3. Lactate Dehydrogenase (LDH)
4.4. Carbonic Anhydrase III (CA-III)
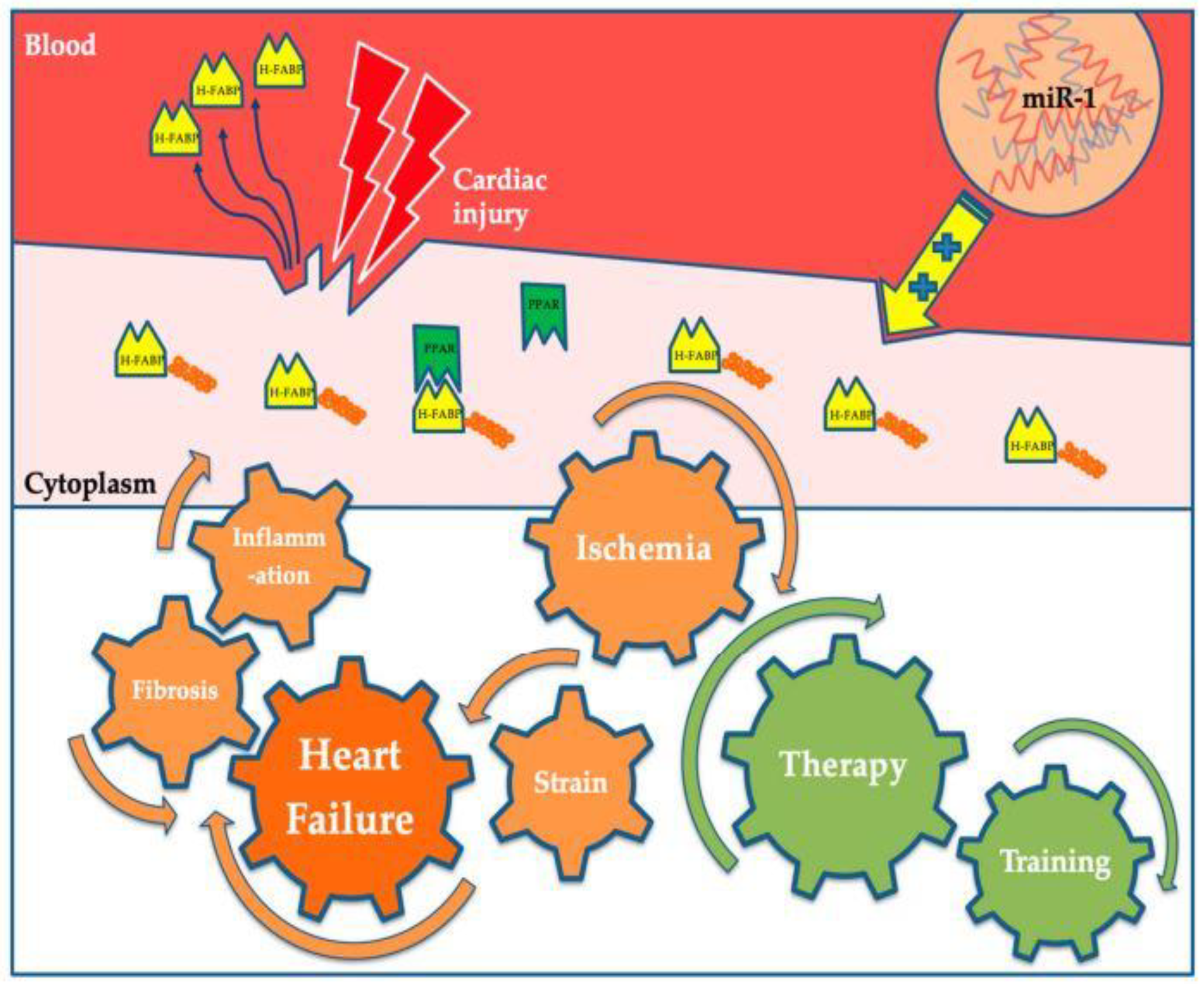
4.5. Heart-Type Fatty Acid-Binding Protein (H-FABP)
4.6. C-Reactive Protein (CRP)
4.7. Myeloperoxidase (MPO)
4.8. Cardiac Troponins
4.9. Hydroxybutyrate Dehydrogenase (HBDH)
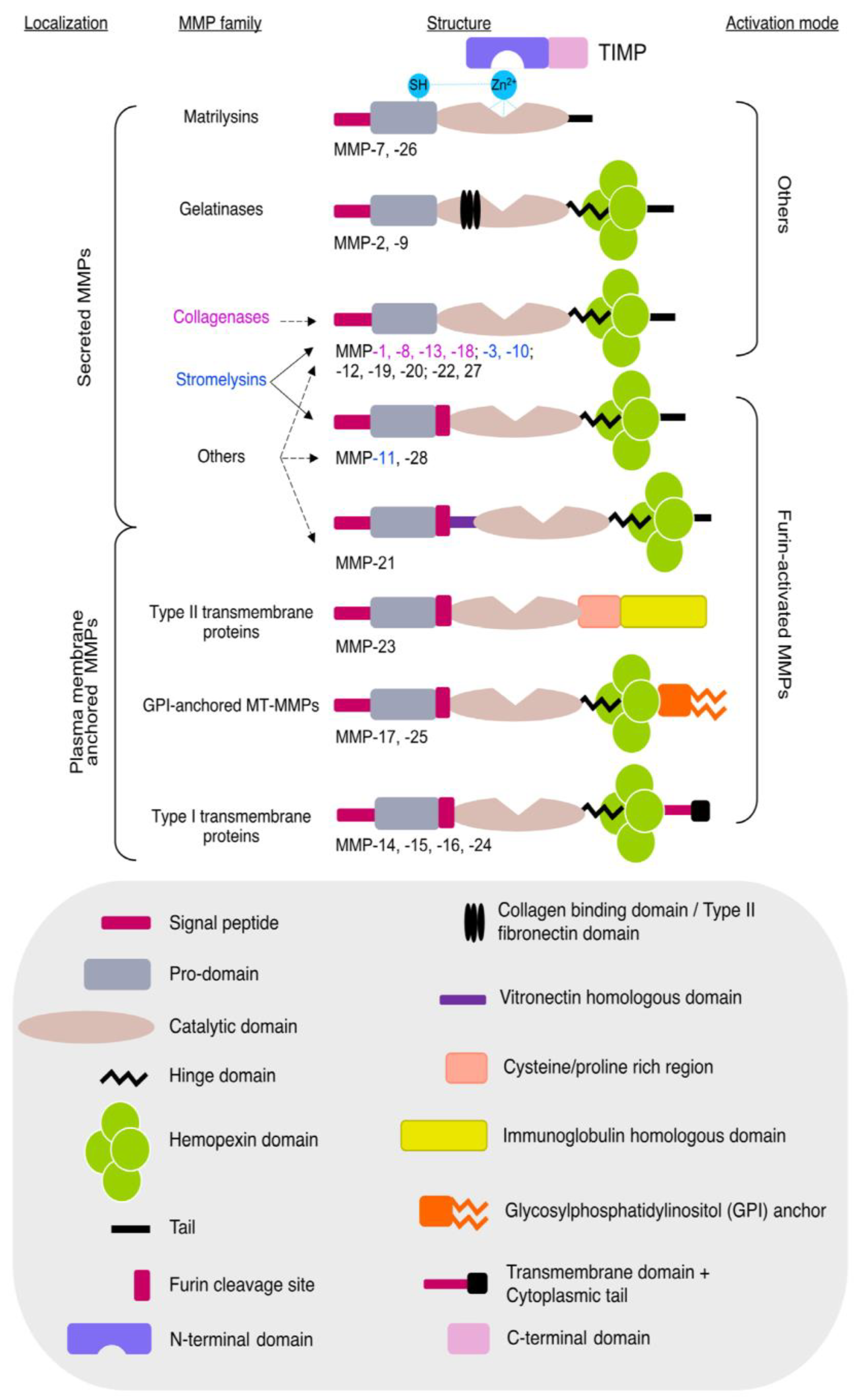
4.10. Matrix Metalloproteinases (MMPs) and Tissue Inhibitors of Metalloproteinases (TIMPs)
4.11. Fibrinogen Levels
4.12. Myoglobin
4.13. Ischemia-Modified Albumin (IMA)
4.14. Glycogen Phosphorylase Isoenzyme BB (GPBB)
4.15. Oxylipins
4.16. Lipoprotein-Associated Phospholipase A2 (Lp-PLA2)
4.17. B-Type Natriuretic Peptide (BNP) and N-Terminal Pro-B-Type Natriuretic Peptide (NT-proBNP)
4.18. Mid-Regional Pro-Atrial Natriuretic Peptide (MR-proANP) and Mid-Regional Pro-Adrenomedullin (MR-proADM)
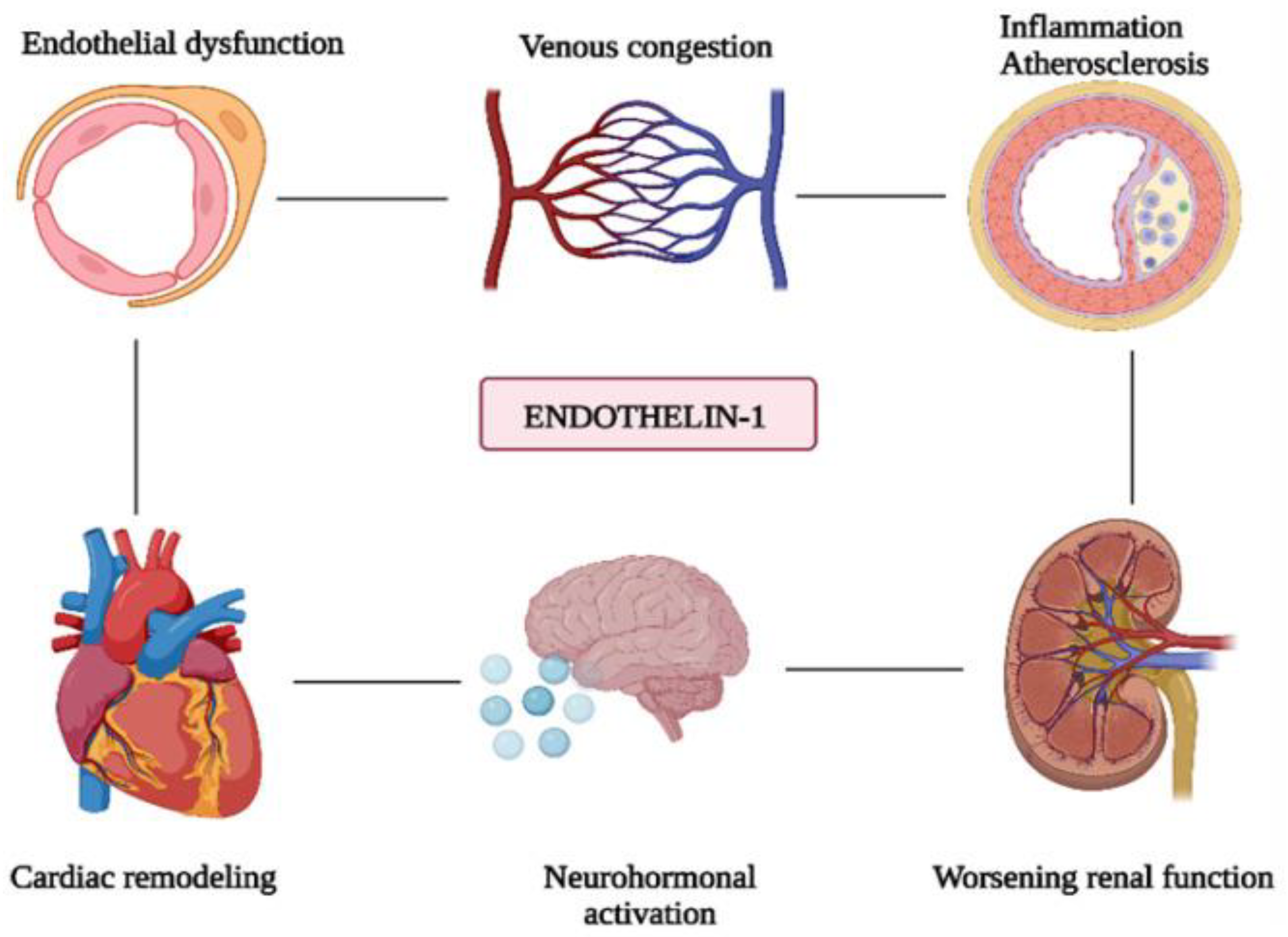
4.19. Endothelin-1 (ET-1)
4.20. Tumor Necrosis Factor-Alpha (TNFα)
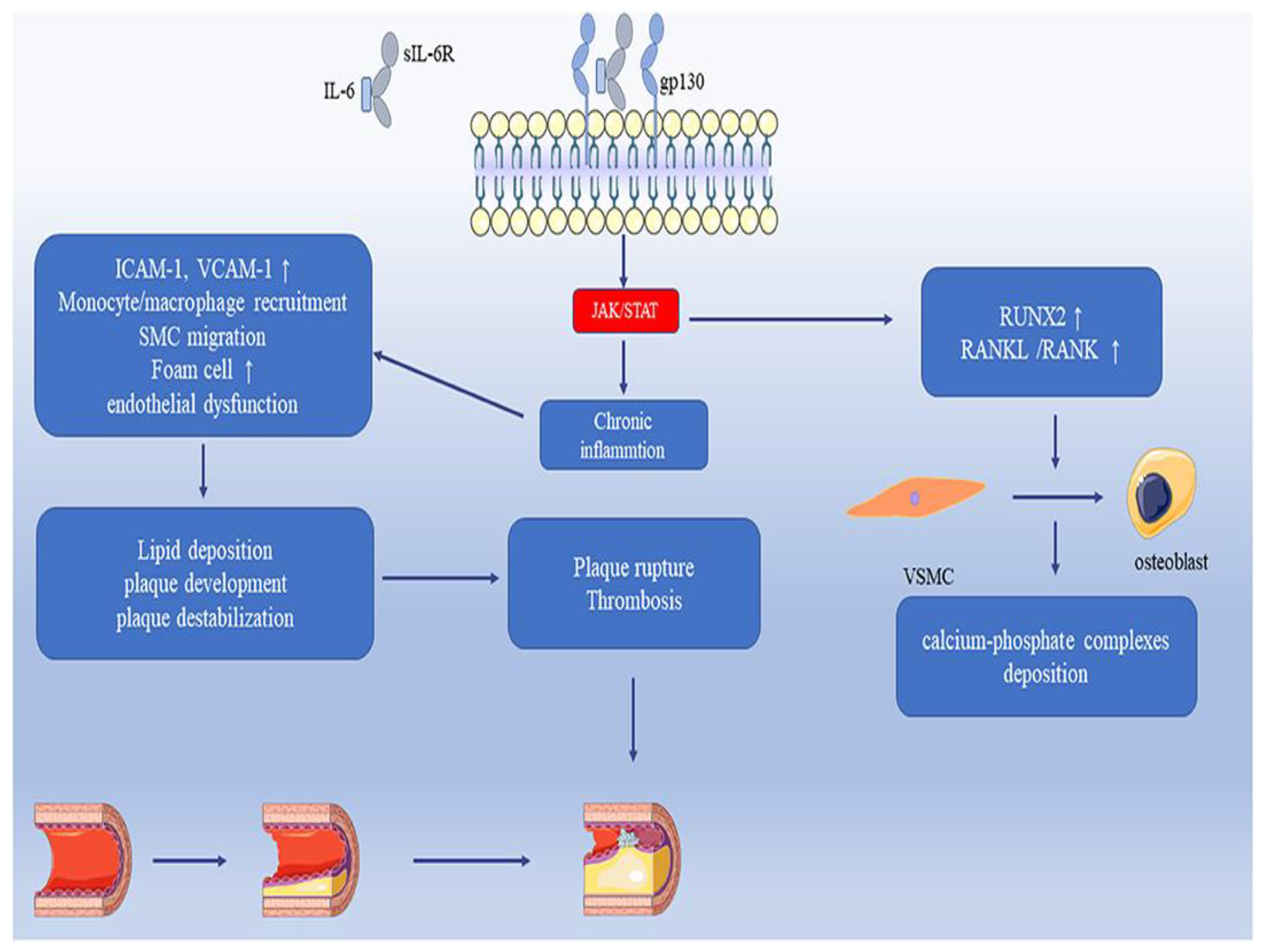
4.21. Interleukin-6 (IL-6)
4.22. Growth Differentiation Factor-15 (GDF-15)
4.23. Suppression of Tumorigenicity-2 (ST2)
4.24. Pentraxin 3 (PTX3)
4.25. Pregnancy-Associated Plasma Protein-A (PAPP-A)
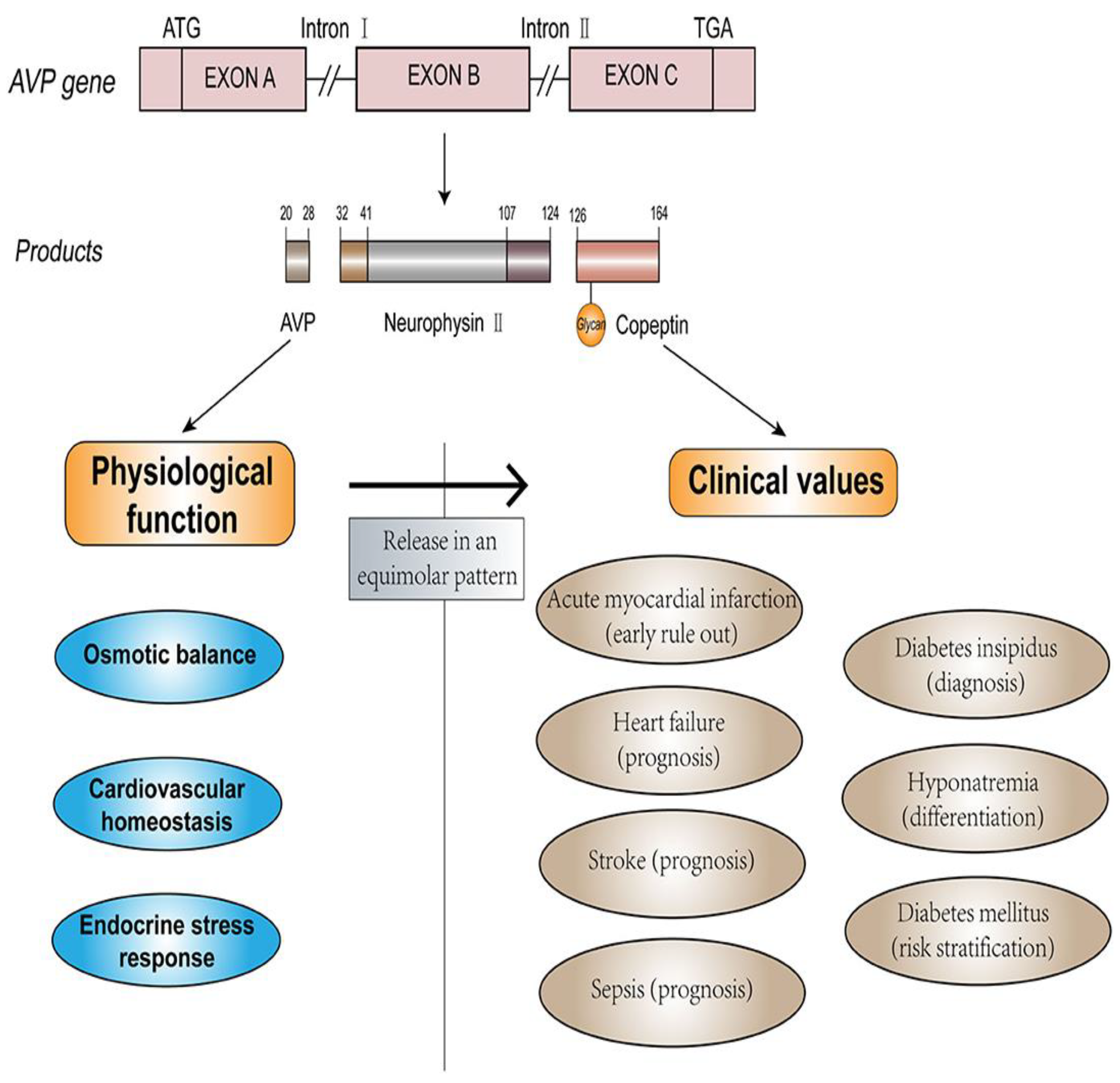
4.26. Copeptin
4.27. Galectin-3 (Gal-3)
4.28. Trimethylamine n-Oxide (TMAO)
4.29. MicroRNAs and Long Non-Coding RNAs
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gaziano, T.A. Cardiovascular diseases worldwide. Public Health Approach Cardiovasc. Dis. Prev. Manag. 2022, 1, 8–18. [Google Scholar]
- Wang, Y.; Wang, X.; Wang, C.; Zhou, J. Global, Regional, and National Burden of Cardiovascular Disease, 1990–2021: Results From the 2021 Global Burden of Disease Study. Cureus 2024, 16, e74333. [Google Scholar] [PubMed]
- Sun, B.; Wang, Z. A Short Review on Advances in Early Diagnosis and Treatment of Ischemic Stroke. Galen Med. J. 2023, 12, e2993. [Google Scholar] [PubMed]
- Ahmad, S.; Kumar, R. An update of new/potential cardiovascular markers: A narrative review. Mol. Biol. Rep. 2024, 51, 179. [Google Scholar] [CrossRef]
- Vasan, R.S. Biomarkers of cardiovascular disease: Molecular basis and practical considerations. Circulation 2006, 113, 2335–2362. [Google Scholar]
- Shao, C.; Wang, J.; Tian, J.; Tang, Y.D. Coronary Artery Disease: From Mechanism to Clinical Practice. In Coronary Artery Disease: Therapeutics and Drug Discovery; Wang, M., Ed.; Advances in Experimental Medicine and Biology; Springer: Singapore, 2020; Volume 1177. [Google Scholar] [CrossRef]
- Morley, R.L.; Sharma, A.; Horsch, A.D.; Hinchliffe, R.J. Peripheral artery disease. BMJ 2018, 360, j5842. [Google Scholar]
- Goldhaber, S.Z.; Bounameaux, H. Pulmonary embolism and deep vein thrombosis. Lancet 2012, 379, 1835–1846. [Google Scholar]
- Marijon, E.; Mirabel, M.; Celermajer, D.S.; Jouven, X. Rheumatic heart disease. Lancet 2012, 379, 953–964. [Google Scholar]
- Sun, R.; Liu, M.; Lu, L.; Zheng, Y.; Zhang, P. Congenital heart disease: Causes, diagnosis, symptoms, and treatments. Cell Biochem. Biophys. 2015, 72, 857–860. [Google Scholar]
- Netala, V.R.; Teertam, S.K.; Li, H.; Zhang, Z. A Comprehensive Review of Cardiovascular Disease Management: Cardiac Biomarkers, Imaging Modalities, Pharmacotherapy, Surgical Interventions, and Herbal Remedies. Cells 2024, 13, 1471. [Google Scholar] [CrossRef]
- Restrepo Tique, M.; Araque, O.; Sanchez-Echeverri, L.A. Technological Advances in the Diagnosis of Cardiovascular Disease: A Public Health Strategy. Int. J. Environ. Res. Public Health 2024, 21, 1083. [Google Scholar] [CrossRef] [PubMed]
- Jacob, R.; Khan, M. Cardiac Biomarkers: What Is and What Can Be. Indian J. Cardiovasc. Dis. Women WINCARS 2018, 3, 240–244. [Google Scholar] [CrossRef]
- Thupakula, S.; Nimmala, S.S.R.; Ravula, H.; Chekuri, S.; Padiya, R. Emerging biomarkers for the detection of cardiovascular diseases. Egypt Heart J. 2022, 74, 77. [Google Scholar] [CrossRef]
- Ladue, J.S.; Wroblewski, F.; Karmen, A. Serum glutamic oxaloacetic transaminase activity in human acute transmural myocardial infarction. Science 1954, 120, 497–499. [Google Scholar] [CrossRef] [PubMed]
- Aydin, S.; Ugur, K.; Aydin, S.; Sahin, I.; Yardim, M. Biomarkers in acute myocardial infarction: Current perspectives. Vasc. Health Risk Manag. 2019, 15, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wroblewski, F.; Ladue, J.S. Lactic dehydrogenase activity in blood. Proc. Soc. Exp. Biol. Med. 1955, 90, 210–213. [Google Scholar] [CrossRef]
- Feng, H.Z.; Jin, J.P. Transgenic expression of carbonic anhydrase III in cardiac muscle demonstrates a mechanism to tolerate acidosis. Am. J. Physiol. Cell Physiol. 2019, 317, C922–C931. [Google Scholar]
- Fliegel, L. Molecular biology of the myocardial Na+/H+ exchanger. J. Mol. Cell Cardiol. 2008, 44, 228–237. [Google Scholar] [CrossRef]
- Fliegel, L. Regulation of the Na+/H+ exchanger in the healthy and diseased myocardium. Exp. Opin. Ther. Targ. 2009, 13, 55–68. [Google Scholar]
- Otaki, Y.; Watanabe, T.; Kubota, I. Heart-type fatty acid-binding protein in cardiovascular disease: A systemic review. Clin. Chim. Acta 2017, 474, 44–53. [Google Scholar]
- Ye, X.D.; He, Y.; Wang, S.; Wong, G.T.; Irwin, M.G.; Xia, Z. Heart-type fatty acid binding protein (H-FABP) as a biomarker for acute myocardial injury and long-term post-ischemic prognosis. Acta Pharmacol. Sin. 2018, 39, 1155–1163. [Google Scholar] [CrossRef]
- Rezar, R.; Jirak, P.; Gschwandtner, M.; Derler, R.; Felder, T.K.; Haslinger, M.; Kopp, K.; Seelmaier, C.; Granitz, C.; Hoppe, U.C.; et al. Heart-Type Fatty Acid-Binding Protein (H-FABP) and its Role as a Biomarker in Heart Failure: What Do We Know So Far? J. Clin. Med. 2020, 9, 164. [Google Scholar] [CrossRef]
- Amezcua-Castillo, E.; González-Pacheco, H.; Sáenz-San Martín, A.; Méndez-Ocampo, P.; Gutierrez-Moctezuma, I.; Massó, F.; Sierra-Lara, D.; Springall, R.; Rodríguez, E.; Arias-Mendoza, A.; et al. C-Reactive Protein: The Quintessential Marker of Systemic Inflammation in Coronary Artery Disease-Advancing toward Precision Medicine. Biomedicines 2023, 11, 2444. [Google Scholar] [CrossRef] [PubMed]
- Cook, N.R.; Buring, J.E.; Ridker, P.M. The effect of including C-reactive protein in cardiovascular risk prediction models for women. Ann. Intern. Med. 2006, 145, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Hansson, G.K.; Hermansson, A. The immune system in atherosclerosis. Nat. Immunol. 2011, 12, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Frangie, C.; Daher, J. Role of myeloperoxidase in inflammation and atherosclerosis (Review). Biomed. Rep. 2022, 16, 53. [Google Scholar] [CrossRef] [PubMed]
- Anatoliotakis, N.; Deftereos, S.; Bouras, G.; Giannopoulos, G.; Tsounis, D.; Angelidis, C.; Kaoukis, A.; Stefanadis, C. Myeloperoxidase: Expressing inflammation and oxidative stress in cardiovascular disease. Curr. Top. Med. Chem. 2013, 13, 115–138. [Google Scholar] [CrossRef]
- Park, K.C.; Gaze, D.C.; Collinson, P.O.; Marber, M.S. Cardiac troponins: From myocardial infarction to chronic disease. Cardiovasc. Res. 2017, 113, 1708–1718. [Google Scholar] [CrossRef]
- Kaier, T.E.; Alaour, B.; Marber, M. Cardiac troponin and defining myocardial infarction. Cardiovasc. Res. 2021, 117, 2203–2215. [Google Scholar] [CrossRef]
- Zhang, Y.J.; Sun, Y.; Zhao, Y.B.; Ma, D. α-HBDH is a superior to LDH in predicting major adverse cardiovascular events in patients with acute aortic dissection. Heliyon 2024, 10, e29155. [Google Scholar] [CrossRef]
- Lee, S.; Koppensteiner, R.; Kopp, C.W.; Gremmel, T. α-Hydroxybutyrate dehydrogenase is associated with atherothrombotic events following infrainguinal angioplasty and stenting. Sci. Rep. 2019, 9, 18200. [Google Scholar]
- Molière, S.; Jaulin, A.; Tomasetto, C.-L.; Dali-Youcef, N. Roles of Matrix Metalloproteinases and Their Natural Inhibitors in Metabolism: Insights into Health and Disease. Int. J. Mol. Sci. 2023, 24, 10649. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Zheng, Y.J.; Gu, S.S.; Tan, J.L.; Paul, C.; Wang, Y.G.; Yang, H.T. Degradation of cardiac myosin light chain kinase by matrix metalloproteinase-2 contributes to myocardial contractile dysfunction during ischemia/reperfusion. J. Mol. Cell. Cardiol. 2014, 77, 102–112. [Google Scholar] [CrossRef] [PubMed]
- De Coux, A.; Lindsey, M.L.; Villarreal, F.; Garcia, R.A.; Schulz, R. Myocardial matrix metalloproteinase-2: Inside out and upside down. J. Mol. Cell. Cardiol. 2014, 77, 64–72. [Google Scholar] [CrossRef]
- Alp, E.; Yilmaz, A.; Tulmac, M.; Dikmen, A.U.; Cengel, A.; Yalcin, R.; Menevse, E.S. Analysis of MMP-7 and TIMP-2 gene polymorphisms in coronary artery disease and myocardial infarction: A Turkish case-control study. Kaohsiung J. Med. Sci. 2017, 33, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Macrae, F.L.; Swieringa, F.; Heemskerk, J.W.M.; Ariëns, R.A.S. High fibrinogen γ’ levels in patient plasma increase clot formation at arterial and venous shear. Blood Adv. 2021, 5, 3468–3477. [Google Scholar] [CrossRef]
- Appiah, D.; Schreiner, J.P.; MacLehose, R.F.; Folsom, A.R. Association of plasma γ’ fibrinogen with incident cardiovascular disease: The atherosclerosis risk in communities (ARIC) study. Arter. Thromb. Vasc. Biol. 2015, 35, 2700–2706. [Google Scholar] [CrossRef]
- Vaidya, H.C. Myoglobin: An early biochemical marker for the diagnosis of acute myocardial infarction. J. Clin. Immunoass. 1994, 17, 35–39. [Google Scholar]
- Gibler, W.B.; Gibler, C.D.; Weinshenker, E.; Abbottsmith, C.; Hedges, J.R.; Barsan, W.G.; Sperling, M.; Chen, I.W.; Embry, S.; Kereiakes, D. Myoglobin as an early indicator of acute myocardial infarction. Ann. Emerg. Med. 1987, 16, 851–856. [Google Scholar] [CrossRef] [PubMed]
- Mair, J.; Morandell, D.; Genser, N.; Lechleitner, P.; Dienstl, F.; Puschendorf, B. Equivalent early sensitivities of myoglobin, creatine kinase MB mass, creatine kinase isoform ratios, and cardiac troponins I and T for acute myocardial infarction. Clin. Chem. 1995, 41, 1266–1272. [Google Scholar] [CrossRef]
- Abadie, J.M.; Blassingame, C.L.; Bankson, D.D. Albumin cobalt binding assay to rule out acute coronary syndrome. Ann. Clin. Lab. Sci. 2005, 35, 66–72. [Google Scholar] [PubMed]
- Bhakthavatsala Reddy, C.; Cyriac, C.; Desle, H.B. Role of “Ischemia Modified Albumin” (IMA) in acute coronary syndromes. Indian Heart J. 2014, 66, 656–662. [Google Scholar] [CrossRef]
- Jawade, P.; Khillare, K.M.; Mangudkar, S.; Palange, A.; Dhadwad, J.; Deshmukh, M. A Comparative Study of Ischemia-Modified Albumin: A Promising Biomarker for Early Detection of Acute Coronary Syndrome (ACS). Cureus 2023, 15, e44357. [Google Scholar] [CrossRef]
- Rabitzsch, G.; Mair, J.; Lechleitner, P.; Noll, F.; Hofmann, U.; Krause, E.G.; Dienstl, F.; Puschendorf, B. Immunoenzymometric assay of human glycogen phosphorylase isoenzyme BB in diagnosis of ischemic myocardial injury. Clin. Chem. 1995, 41, 966–978. [Google Scholar] [CrossRef] [PubMed]
- Krause, E.G.; Rabitzsch, G.; Noll, F.; Mair, J.; Puschendorf, B. Glycogen phosphorylase isoenzyme BB in diagnosis of myocardial ischaemic injury and infarction. Mol. Cell Biochem. 1996, 60, 289–295. [Google Scholar] [CrossRef]
- Ghimire, A.; Giri, S.; Khanal, N.; Rayamajhi, S.; Thapa, A.; Bist, A.; Devkota, S. Diagnostic accuracy of glycogen phosphorylase BB for myocardial infarction: A systematic review and meta-analysis. J. Clin. Lab. Anal. 2022, 36, e24368. [Google Scholar] [CrossRef] [PubMed]
- Nayeem, M.A. Role of oxylipins in cardiovascular diseases. Acta Pharmacol. Sin. 2018, 39, 1142–1154. [Google Scholar] [CrossRef]
- Gabbs, M.; Leng, S.; Devassy, J.G.; Monirujjaman, M.; Aukema, H.M. Advances in our understanding of oxylipins derived from dietary PUFAs. Adv. Nutr. 2015, 6, 513–540. [Google Scholar]
- Wang, B.; Wu, L.; Chen, J.; Dong, L.; Chen, C.; Wen, Z.; Hu, J.; Fleming, I.; Wang, D. Metabolism pathways of arachidonic acids: Mechanisms and potential therapeutic targets. Signal Transduct. Target. Ther. 2021, 6, 94. [Google Scholar] [CrossRef]
- Tellis, C.C.; Tselepis, A.D. Pathophysiological role and clinical significance of lipoprotein-associated phospholipase A2 (Lp-PLA2) bound to LDL and HDL. Curr. Pharm. Des. 2014, 20, 6256–6269. [Google Scholar] [CrossRef]
- Munzel, T.; Gori, T. Lipoprotein-associated phospholipase A(2), a marker of vascular inflammation and systemic vulnerability. Eur. Heart J. 2009, 30, 2829–2831. [Google Scholar] [CrossRef] [PubMed]
- Zalewski, A.; Macphee, C. Role of lipoprotein-associated phospholipase A2 in atherosclerosis: Biology, epidemiology, and possible therapeutic target. Arter. Thromb. Vasc. Biol. 2005, 25, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Goetze, J.P.; Bruneau, B.G.; Ramos, H.R.; Ogawa, T.; De Bold, M.K.; De Bold, A.J. Cardiac natriuretic peptides. Nat. Rev. Cardiol. 2020, 17, 698–717. [Google Scholar] [CrossRef]
- Călburean, P.A.; Lupu, S.; Huțanu, A.; Oprica, M.; Opriș, D.R.; Stan, A.; Scurtu, A.C.; Aniței, D.; Harpa, M.; Brînzaniuc, K.; et al. Natriuretic peptides and soluble ST2 improves echocardiographic diagnosis of elevated left ventricular filling pressures. Sci. Rep. 2024, 14, 22171. [Google Scholar] [CrossRef]
- Weber, M.; Hamm, C. Role of B-type natriuretic peptide (BNP) and NT-proBNP in clinical routine. Heart 2006, 92, 843–849. [Google Scholar] [CrossRef]
- Cao, Z.; Jia, Y.; Zhu, B. BNP and NT-proBNP as Diagnostic Biomarkers for Cardiac Dysfunction in Both Clinical and Forensic Medicine. Int. J. Mol. Sci. 2019, 20, 1820. [Google Scholar] [CrossRef]
- Gohar, A.; Rutten, F.H.; den Ruijter, H.; Kelder, J.C.; von Haehling, S.; Anker, S.D.; Möckel, M.; Hoes, A.W. Mid-regional pro-atrial natriuretic peptide for the early detection of non-acute heart failure. Eur. J. Heart Fail. 2019, 21, 1219–1227. [Google Scholar] [CrossRef]
- Chioncel, O.; Butler, J. Mid-regional pro-atrial natriuretic peptide for diagnosis of heart failure in non-acute settings: Biomarkers plus clinical sense make good sense. Eur. J. Heart Fail. 2019, 21, 1228–1230. [Google Scholar]
- Potocki, M.; Ziller, R.; Mueller, C. Mid-Regional Pro-Adrenomedullin in Acute Heart Failure: A Better Biomarker or Just Another Biomarker? Curr. Heart Fail. Rep. 2012, 9, 244–251. [Google Scholar] [CrossRef]
- Khan, S.Q.; O’Brien, R.J.; Struck, J.; Quinn, P.; Morgenthaler, N.; Squire, I.; Davies, J.; Bergmann, A.; Ng, L.L. Prognostic value of midregional pro-adrenomedullin in patients with acute myocardial infarction: The lamp (leicester acute myocardial infarction peptide) study. J. Am. Coll. Cardiol. 2007, 49, 1525–1532. [Google Scholar]
- Dmour, B.A.; Costache, A.D.; Dmour, A.; Huzum, B.; Duca, Ș.T.; Chetran, A.; Miftode, R.Ș.; Afrăsânie, I.; Tuchiluș, C.; Cianga, C.M.; et al. Could Endothelin-1 Be a Promising Neurohormonal Biomarker in Acute Heart Failure? Diagnostics 2023, 13, 2277. [Google Scholar] [CrossRef] [PubMed]
- Dhaun, N.; Webb, D.J. Endothelins in cardiovascular biology and therapeutics. Nat. Rev. Cardiol. 2019, 16, 491–502. [Google Scholar] [CrossRef]
- Nishiyama, S.K.; Zhao, J.; Wray, D.W.; Richardson, R.S. Vascular function and endothelin-1: Tipping the balance between vasodilation and vasoconstriction. J. Appl. Physiol. 2017, 122, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Schumacher, S.M.; Naga Prasad, S.V. Tumor Necrosis Factor-α in Heart Failure: An Updated Review. Curr. Cardiol. Rep. 2018, 20, 117. [Google Scholar] [CrossRef]
- Urschel, K.; Cicha, I. TNF-α in the cardiovascular system: From physiology to therapy. Int. J. Interferon Cytokine Mediat. Res. 2015, 7, 9–25. [Google Scholar] [CrossRef]
- Dunlay, S.M.; Weston, S.A.; Redfield, M.M.; Killian, J.M.; Roger, V.L. Tumor necrosis factor-alpha and mortality in heart failure: A community study. Circulation 2008, 118, 625–631. [Google Scholar] [CrossRef]
- Rolski, F.; Błyszczuk, P. Complexity of TNF-? Signaling in Heart Disease. J. Clin. Med. 2020, 9, 3267. [Google Scholar] [CrossRef]
- Su, J.H.; Luo, M.Y.; Liang, N.; Gong, S.X.; Chen, W.; Huang, W.Q.; Tian, Y.; Wang, A.P. Interleukin-6: A Novel Target for Cardio-Cerebrovascular Diseases. Front. Pharmacol. 2021, 12, 745061. [Google Scholar] [CrossRef]
- Ridker, P.M.; Rane, M. Interleukin-6 Signaling and Anti-Interleukin-6 Therapeutics in Cardiovascular Disease. Circ. Res. 2021, 128, 1728–1746. [Google Scholar] [CrossRef]
- Mossmann, M.; Wainstein, M.V.; Mariani, S.; Machado, G.P.; de Araújo, G.N.; Andrades, M.; Gonçalves, S.C. Increased serum IL-6 is predictive of long-term cardiovascular events in high-risk patients submitted to coronary angiography: An observational study. Diabetol. Metab. Syndr. 2022, 14, 125. [Google Scholar] [CrossRef]
- Feng, Y.; Ye, D.; Wang, Z.; Pan, H.; Lu, X.; Wang, M.; Xu, Y.; Yu, J.; Zhang, J.; Zhao, M.; et al. The Role of Interleukin-6 Family Members in Cardiovascular Diseases. Front. Cardiovasc. Med. 2022, 9, 818890. [Google Scholar] [CrossRef]
- May, B.M.; Pimentel, M.; Zimerman, L.I.; Rohde, L.E. GDF-15 as a Biomarker in Cardiovascular Disease. Arq. Bras. Cardiol. 2021, 116, 494–500. [Google Scholar]
- Li, J.; Hu, X.; Xie, Z.; Li, J.; Huang, C.; Huang, Y. Overview of growth differentiation factor 15 (GDF15) in metabolic diseases. Biomed. Pharmacother. 2024, 176, 116809. [Google Scholar]
- Nyárády, B.B.; Kiss, L.Z.; Bagyura, Z.; Merkely, B.; Dósa, E.; Láng, O.; Kőhidai, L.; Pállinger, É. Growth and differentiation factor-15: A link between inflammaging and cardiovascular disease. Biomed. Pharmacother. 2024, 174, 116475. [Google Scholar]
- Di Candia, A.M.; De Avila, D.X.; Moreira, G.R.; Villacorta, H.; Maisel, A.S. Growth differentiation factor-15, a novel systemic biomarker of oxidative stress, inflammation, and cellular aging: Potential role in cardiovascular diseases. Am. Heart J. Plus Cardiol. Res. Pract. 2021, 9, 100046. [Google Scholar]
- Aimo, A.; Januzzi, J.L.; Bayes-Genis, A.; Vergaro, G.; Sciarrone, P.; Passino, C.; Emdin, M. Clinical and prognostic significance of sST2 in heart failure: JACC review topic of the week. J. Am. Coll. Cardiol. 2019, 74, 2193–2203. [Google Scholar]
- Jin, M.; Wei, S.; Gao, R.; Wang, K.; Xu, X.; Yao, W.; Zhang, H.; Zhou, Y.; Xu, D.; Zhou, F.; et al. Predictors of Long-Term Mortality in Patients With Acute Heart Failure. Int. Heart. J. 2017, 58, 409–415. [Google Scholar]
- Manzano-Fernández, S.; Januzzi, J.L.; Pastor-Pérez, F.J.; Bonaque-González, J.C.; Boronat-Garcia, M.; Pascual-Figal, D.A.; Montalban-Larrea, S.; Navarro-Peñalver, M.; Andreu-Cayuelas, J.M.; Valdés, M. Serial monitoring of soluble interleukin family member ST2 in patients with acutely decompensated heart failure. Cardiology 2012, 122, 158–166. [Google Scholar]
- Gul, I.; Yucel, O.; Zararsiz, A.; Demirpence, O.; Yucel, H.; Zorlu, A.; Yilmaz, M.B. Prognostic role of soluble suppression of tumorigenicity-2 on cardiovascular mortality in outpatients with heart failure. Anatol. J. Cardiol. 2017, 18, 200–205. [Google Scholar]
- Pfetsch, V.; Sanin, V.; Jaensch, A.; Dallmeier, D.; Mons, U.; Brenner, H.; Koenig, W.; Rothenbacher, D. Increased Plasma Concentrations of Soluble ST2 Independently Predict Mortality but not Cardiovascular Events in Stable Coronary Heart Disease Patients: 13-Year Follow-up of the KAROLA Study. Cardiovasc. Drugs Ther. 2017, 31, 167–177. [Google Scholar]
- Inoue, K.; Kodama, T.; Daida, H. Pentraxin 3: A novel biomarker for inflammatory cardiovascular disease. Int. J. Vasc. Med. 2012, 2012, 657025. [Google Scholar] [CrossRef] [PubMed]
- Ye, X.; Wang, Z.; Lei, W.; Shen, M.; Tang, J.; Xu, X.; Yang, Y.; Zhang, H. Pentraxin 3: A promising Therapeutic Target for Cardiovascular Diseases. Ageing Res. Rev. 2024, 93, 102163. [Google Scholar]
- Ristagno, G.; Fumagalli, F.; Bottazzi, B.; Mantovani, A.; Olivari, D.; Novelli, D.; Latini, R. Pentraxin 3 in Cardiovascular Disease. Front. Immunol. 2019, 10, 823. [Google Scholar] [CrossRef]
- Fornai, F.; Carrizzo, A.; Forte, M.; Ambrosio, M.; Damato, A.; Ferrucci, M.; Biagioni, F.; Busceti, C.; Puca, A.A. The inflammatory protein Pentraxin 3 in cardiovascular disease. Immun. Ageing 2016, 13, 25. [Google Scholar] [CrossRef] [PubMed]
- Conover, C.A.; Oxvig, C. The Pregnancy-Associated Plasma Protein-A (PAPP-A) Story. Endocr. Rev. 2023, 44, 1012–1028. [Google Scholar] [CrossRef] [PubMed]
- Ziviello, F.; Conte, S.; Cimmino, G.; Carlo Sasso, F.; Trimarco, B.; Cirillo, P. Pregnancy-associated plasma protein-A and its role in cardiovascular disease. Biology, experimental/clinical evidences and potential therapeutic approaches. Curr. Vasc. Pharmacol. 2017, 15, 197–206. [Google Scholar]
- Wang, J.; Tan, G.J.; Han, L.N.; Bai, Y.Y.; He, M.; Liu, H.B. Novel biomarkers for cardiovascular risk prediction. J. Geriatr. Cardiol. JGC 2017, 14, 135. [Google Scholar]
- Gururajan, P.; Gurumurthy, P.; Nayar, P.; Rao, G.S.N.; Babu, R.S.; Sarasabharati, A.; Cherian, K.M. Pregnancy associated plasma protein-A (PAPP-A) as an early marker for the diagnosis of acute coronary syndrome. Indian Heart J. 2012, 64, 141–145. [Google Scholar]
- Mu, D.; Cheng, J.; Qiu, L.; Cheng, X. Copeptin as a Diagnostic and Prognostic Biomarker in Cardiovascular Diseases. Front. Cardiovasc. Med. 2022, 9, 901990. [Google Scholar] [CrossRef]
- Łukaszyk, E.; Małyszko, J. Copeptin: Pathophysiology and potential clinical impact. Adv. Med. Sci. 2015, 60, 335–341. [Google Scholar]
- Morgenthaler, N.G. Copeptin: A biomarker of cardiovascular and renal function. Congest. Heart Fail. 2010, 16, S37–S44. [Google Scholar] [CrossRef] [PubMed]
- Zaborska, B.; Sikora-Frąc, M.; Smarż, K.; Pilichowska-Paszkiet, E.; Budaj, A.; Sitkiewicz, D.; Sygitowicz, G. The Role of Galectin-3 in Heart Failure-The Diagnostic, Prognostic and Therapeutic Potential-Where Do We Stand? Int. J. Mol. Sci. 2023, 24, 13111. [Google Scholar] [CrossRef]
- Zaborska, B.; Sygitowicz, G.; Smarż, K.; Pilichowska-Paszkiet, E.; Budaj, A. Galectin-3 is related to right ventricular dysfunction in heart failure patients with reduced ejection fraction and may affect exercise capacity. Sci. Rep. 2020, 10, 16682. [Google Scholar] [CrossRef]
- Amin, H.Z.; Amin, L.Z.; Wijaya, I.P. Galectin-3: A novel biomarker for the prognosis of heart failure. Clujul Med. 2017, 90, 129–132. [Google Scholar] [CrossRef] [PubMed]
- Filipe, M.D.; Meijers, W.C.; Van Der Velde, A.R.; De Boer, R.A. Galectin-3 and heart failure: Prognosis, prediction & clinical utility. Clin. Chim. Acta 2015, 443, 48–56. [Google Scholar] [PubMed]
- Velasquez, M.T.; Ramezani, A.; Manal, A.; Raj, D.S. Trimethylamine N-Oxide: The Good, the Bad and the Unknown. Toxins 2016, 8, 326. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.H.; Hazen, S.L. The contributory role of gut microbiota in cardiovascular disease. J. Clin. Investig. 2014, 124, 4204–4211. [Google Scholar] [CrossRef]
- Thomas, M.S.; Fernandez, M.L. Trimethylamine N-Oxide (TMAO), Diet and Cardiovascular Disease. Curr. Atheroscler. Rep. 2021, 23, 12. [Google Scholar] [CrossRef]
- Kanitsoraphan, C.; Rattanawong, P.; Charoensri, S.; Senthong, V. Trimethylamine N-Oxide and Risk of Cardiovascular Disease and Mortality. Curr. Nutr. Rep. 2018, 7, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Romaine, S.P.; Tomaszewski, M.; Condorelli, G.; Samani, N.J. MicroRNAs in cardiovascular disease: An introduction for clinicians. Heart 2015, 101, 921–928. [Google Scholar] [CrossRef]
- Searles, C.D. MicroRNAs and cardiovascular disease risk. Curr. Cardiol. Rep. 2024, 26, 51–60. [Google Scholar] [PubMed]
- Zhou, S.S.; Jin, J.P.; Wang, J.Q.; Zhang, Z.G.; Freedman, J.H.; Zheng, Y.; Cai, L. miRNAS in cardiovascular diseases: Potential biomarkers, therapeutic targets and challenges. Acta Pharmacol. Sin. 2018, 39, 1073–1084. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | Details |
|---|---|
| Biochemical role | Member of the phospholipase A2 superfamily; hydrolyzes oxidized phospholipids within lipoproteins, leading to the generation of proinflammatory mediators. |
| Primary source | Synthesized predominantly by inflammatory cells within atherosclerotic plaques. |
| Lipoprotein binding | Strong affinity for lipoprotein fractions, including HDL, LDL, and VLDL. This association highlights its role in lipid metabolism and atherogenesis. |
| Initial identification | Initially recognized as plasma platelet-activating factor acetylhydrolase (pPAF-AH) due to its ability to hydrolyze platelet-activating factor (PAF), a potent proinflammatory mediator. |
| Role in atherosclerosis | Contributes to vascular inflammation by hydrolyzing oxidized phospholipids in LDL, generating lysophosphatidylcholine and oxidized fatty acids, which promote plaque progression and instability. |
| Clinical significance | Elevated Lp-PLA2 levels are strongly associated with increased risk of cardiovascular diseases (CVDs), such as coronary heart disease (CHD), atherosclerosis, and ischemic stroke. |
| Diagnostic utility | Provides high specificity for vascular inflammation with minimal biological variability, making it a robust biomarker for assessing cardiovascular risk. |
| Prognostic implications | Elevated levels correlate with higher risks of cardiovascular events, plaque rupture, and future adverse outcomes. |
| Therapeutic potential | A potential therapeutic target due to its role in vascular inflammation and atherogenesis. Inhibitors of Lp-PLA2 are being investigated as possible interventions for reducing cardiovascular risk. |
| Inflammatory role | Mediates vascular inflammation through its regulatory effects on lipid metabolism and its proinflammatory activity within atherosclerotic plaques. |
| Utility in CVDs | Helps in diagnosing, prognosticating, and managing vascular diseases, particularly in patients predisposed to atherosclerosis, CHD, and ischemic stroke. |
| Advantages | High specificity for vascular inflammation; reflects the inflammatory state of atherosclerotic plaques; minimal biological variability. |
| Limitations | Elevated levels may reflect an inflammatory environment without necessarily pinpointing specific events, requiring integration with other clinical parameters for comprehensive assessment. |
| Feature | BNP | NT-proBNP |
|---|---|---|
| Source | Secreted by cardiac ventricles in response to stretch | Cleaved from proBNP during BNP synthesis |
| Molecular structure | Active hormone | Inactive fragment |
| Half-life | ~20 min | ~60–120 min |
| Stability | Less stable in blood samples | More stable in blood samples |
| Diagnostic role | Heart failure (HF) diagnosis, prognosis, and treatment monitoring | Heart failure diagnosis, prognosis, and treatment monitoring |
| Age impact | Less affected by age | Levels increase significantly with age |
| Renal impact | Moderately influenced by renal dysfunction | More significantly influenced by renal dysfunction |
| Reference ranges | <100 pg/mL typically indicates no HF | Age-specific cutoffs; <300 pg/mL often indicates no HF |
| Clinical use | Acute and chronic HF management | Acute and chronic HF management |
| Advantages | Directly reflects cardiac activity | Higher stability; useful for longer sample transport |
| Disadvantages | Short half-life, less stable | Age- and renal-dependent levels |
| Feature | MR-proANP | MR-proADM |
|---|---|---|
| Biochemical source | Derived from the stable N-terminal portion of pro-atrial natriuretic peptide (proANP). | A stable fragment of adrenomedullin, a peptide involved in vasodilation, natriuresis, and diuresis. |
| Primary role | Reflects atrial stretch and fluid overload, primarily linked to heart failure (HF). | Reflects vascular stress, endothelial dysfunction, and cardiovascular stress. |
| Stability | Highly stable in circulation due to its longer half-life compared to atrial natriuretic peptide (ANP). | Highly stable, offering reliable measurement and prognostic insights. |
| Diagnostic utility | Effective for diagnosing heart failure (HF), although slightly less sensitive than BNP and NT-proBNP. | Useful in acute and chronic HF, acute coronary syndrome (ACS), and acute myocardial infarction (AMI). Adds diagnostic value beyond natriuretic peptides. |
| Prognostic utility | Excels in long-term prognostic value, particularly in predicting mortality over five years in chronic HF. | Superior prognostic value in predicting mortality and cardiovascular events in HF, ACS, and AMI. Outperforms natriuretic peptides in risk stratification for mild-to-moderate HF. |
| Heart failure (HF) | Strongly associated with disease severity and mortality in chronic HF; valuable for monitoring disease progression and treatment efficacy. | Levels correlate with HF severity and NYHA class; provides predictive value for long-term outcomes and mortality. |
| Acute coronary syndrome (ACS) and AMI | Limited data on utility in ACS and AMI. | Independently associated with fatal and nonfatal cardiovascular events in ACS and AMI. Enhances risk stratification beyond traditional models and natriuretic peptides. |
| Screening potential | Effective for screening atrial fibrillation (AF), particularly in community populations, and identifying individuals at risk of developing AF. | Primarily used for prognostic and risk stratification purposes; limited use in AF screening. |
| Influencing factors | Levels influenced by age, BMI, race, and sex; despite variability, it remains reliable due to its stability. | Levels independent of renal function, age, and systolic blood pressure; remains highly predictive despite other clinical variations. |
| Advantages | Long half-life, stable, and highly prognostic for HF and atrial fibrillation risk. | Adds significant prognostic value to traditional risk models, particularly in ACS and AMI; strong correlation with cardiovascular stress and mortality. |
| Limitations | Diagnostic sensitivity slightly lower than BNP and NT-proBNP; levels vary with demographic and physiological factors. | Limited availability in routine clinical practice; specific role in AF screening not established. |
| Clinical utility | Valuable in chronic HF management, long-term mortality prediction, and AF screening. | Crucial for prognosticating HF, ACS, and AMI outcomes, particularly in mild-to-moderate HF; enhances risk models for predicting mortality and cardiovascular events. |
| Biomarker | Source | Half-Life | Detection Time Window | Specificity and Sensitivity | Factors Affecting Interpretation |
|---|---|---|---|---|---|
| Aspartate aminotransferase (AST) | Cardiac muscle, liver, and skeletal muscle | 17 ± 5 h | Rises in 6–12 h, peaks at 24–36 h, and normalizes in 3–7 days | Moderate sensitivity; low specificity for MI | Elevated in liver disease, muscle injury, and hemolysis |
| Creatine kinase MB (CK-MB) | Predominantly cardiac muscle and minor in skeletal muscle | ~12–24 h | Rises in 3–6 h, peaks at 18–24 h, and normalizes in 48–72 h | High specificity for MI; lower sensitivity than troponins | Skeletal muscle injury, renal failure, and chronic muscle diseases |
| Lactate dehydrogenase (LDH) | Cardiac muscle and red blood cells (LDH1 > LDH2 ratio indicative of MI) | ~9 h | Rises in 12–24 h, peaks in 2–3 days, and normalizes in 10–14 days | Low specificity; moderate sensitivity | Liver disease, hemolysis, malignancies, and strenuous exercise |
| Carbonic anhydrase III (CA-III) | Cardiac muscle and skeletal muscle | Not well established | Altered levels in oxidative stress and ischemia | Emerging biomarker; specificity/sensitivity under study | Ischemia, oxidative stress, and metabolic disorders |
| Heart-type fatty acid-binding protein (H-FABP) | Cardiac muscle | ~1–2 h | Detectable within 90 min, peaks at 6–8 h, and normalizes in 24–36 h | High sensitivity for early MI detection; moderate specificity | Skeletal muscle injury and renal dysfunction |
| C-reactive protein (CRP) | Produced in response to cardiac inflammation, vascular endothelium | 19 h | Increases within 6–12 h, peaks at 24–48 h, and remains elevated for days | High sensitivity for inflammation; low specificity for cardiac events | Chronic inflammation, infections, and autoimmune diseases |
| Myeloperoxidase (MPO) | Secreted by neutrophils and macrophages in atherosclerotic plaques | ~12–24 h | Detectable early in ACS and remains elevated for several days | High sensitivity for oxidative stress; moderate specificity for MI | Infections, systemic inflammation, and autoimmune diseases |
| Cardiac troponins (cTnI, cTnT) | Cardiac myocytes (specific to heart muscle) | cTnI: 2 h–1 day, cTnT: 2–14 days | Rises in 2–4 h, peaks at 12–24 h, and persists for 7–14 days (cTnT) | Gold standard for MI; high specificity and sensitivity | Chronic renal disease, heart failure, sepsis, and strenuous exercise |
| Hydroxybutyrate dehydrogenase (HBDH) | Cardiac muscle and red blood cells | ~10 h | Rises in 6–12 h, peaks at 48–72 h, and normalizes in 7–10 days | Moderate specificity; lower sensitivity than troponins | Liver disease, hemolysis, and muscle injury |
| Matrix metalloproteinases (MMPs) and TIMPs | Cardiac extracellular matrix and vascular smooth muscle cells | Hours to days | Chronically elevated in heart failure and atherosclerosis | High specificity for ECM remodeling; moderate sensitivity | Inflammation, cancer, and chronic heart diseases |
| Fibrinogen | Liver | ~3–5 days | Elevated in the presence of inflammation or cardiovascular risk | Moderate specificity; increased in inflammatory states | Liver disease (synthesis affected), inflammation, and malignancies |
| Myoglobin | Skeletal and cardiac muscle | 2–4 h | Detectable within 1–3 h, peaks at 6–9 h, and returns to baseline in 24 h | High sensitivity; low specificity | Skeletal muscle injury, renal failure, and exercise |
| Ischemia-modified albumin (IMA) | Serum albumin (modified by ischemia) | ~6 min | Detectable within minutes and peaks within 3–6 h | Moderate sensitivity and specificity for ischemia | Liver disease, infections, and oxidative stress conditions |
| Glycogen phosphorylase isoenzyme BB (GPBB) | Cardiac and brain tissue | ~1–3 h | Detectable within 1–4 h, peaks at 6–12 h, and normalizes in 24 h | High sensitivity; moderate specificity | Pregnancy, brain injury, and liver dysfunction |
| Oxylipins | Endothelial cells and inflammatory cells | Variable (minutes to hours) | Depends on lipid subtype | High specificity for endothelial function | Dietary intake and genetic polymorphisms |
| Lipoprotein-associated phospholipase A2 (Lp-PLA2) | Circulating with LDL and HDL | ~6 days | Chronic marker | High specificity for vascular inflammation | Affected by lipid-lowering therapies and metabolic syndrome |
| B-type natriuretic peptide (BNP) and NT-proBNP | Cardiac myocytes | BNP: ~20 min; NT-proBNP: ~90 min | Detectable within hours and peaks at 24–48 h | High specificity and sensitivity for HF | Affected by age, renal function, and obesity |
| Mid-regional pro-atrial natriuretic peptide (MR-proANP) | Cardiac atria | ~60 min | Detectable within hours, peaks within 24 h | High specificity, moderate sensitivity | Affected by renal dysfunction and age |
| Mid-regional pro-adrenomedullin (MR-proADM) | Endothelium, adrenal glands | ~22 min | Detectable early in sepsis, HF | High sensitivity, moderate specificity | Affected by inflammation and sepsis |
| Endothelin-1 (ET-1) | Endothelium | ~4–7 min | Detectable early in HF and hypertension | High specificity for endothelial dysfunction | Affected by renal disease and inflammatory conditions |
| Tumor necrosis factor-alpha (TNFα) | Immune cells | ~30 min | Chronic marker | High sensitivity, low specificity | Elevated in systemic inflammation, and cancer, infections |
| Myoglobin | Skeletal and cardiac muscle | 2–4 h | Detectable within 1–3 h, peaks at 6–9 h, and returns to baseline in 24 h | High sensitivity, low specificity | Skeletal muscle injury, renal failure, exercise |
| Ischemia-modified albumin (IMA) | Serum albumin (modified by ischemia) | ~6 min | Detectable within minutes and peaks within 3–6 h | Moderate sensitivity and specificity for ischemia | Liver disease, infections, and oxidative stress conditions |
| Interleukin-6 (IL-6) | Immune cells and endothelial cells | ~15–20 h | Peaks within 1–2 h and remains elevated for days | High sensitivity for inflammation, but low specificity for CVD alone | Chronic inflammatory diseases, infections, autoimmune disorders, and obesity |
| Growth differentiation factor-15 (GDF-15) | Cardiomyocytes and macrophages | ~4–6 h | Elevated in hours to days during acute and chronic cardiovascular conditions | High sensitivity for heart failure; moderate specificity for CVD | Kidney disease, aging, cancer, and metabolic disorders |
| Suppression of tumorigenicity-2 (ST2) | Cardiac fibroblasts and immune cells | ~1.5 h | Elevated in hours to days in acute and chronic heart failure; linked to adverse outcomes | High prognostic value in heart failure; moderate specificity for CAD | Infection, inflammatory diseases, and renal dysfunction |
| Pentraxin 3 (PTX3) | Endothelial cells, neutrophils, and macrophages | ~12–48 h | Peaks within hours and stays elevated for up to several days during acute myocardial infarction | High sensitivity for acute inflammation; moderate specificity for CAD | Sepsis, autoimmune diseases, and infections |
| Pregnancy-associated plasma protein-A (PAPP-A) | Vascular smooth muscle cells and macrophages | ~4 h | Elevated within hours to days in acute coronary syndromes and atherosclerosis progression | High specificity for unstable plaques; useful in CVD risk stratification | Renal dysfunction, pregnancy, and chronic inflammation |
| Copeptin | Secreted in equimolar amounts with AVP, from the posterior pituitary gland | 1–2 h | Within hours of acute myocardial infarction (AMI) onset; peaks on 1st day | High sensitivity for early AMI detection; good negative predictive value | Kidney function, age, and comorbidities like diabetes may affect copeptin levels. |
| Galectin-3 (Gal-3) | Secreted by activated macrophages, linked to fibrosis, inflammation, and remodeling | ~1–2 days | Elevated in both acute and chronic heart failure (HF); often detectable early | Moderate specificity for HF; high sensitivity for fibrosis and inflammation | Renal dysfunction can elevate levels; interpretation may vary with concurrent inflammation. |
| Trimethylamine N-oxide (TMAO) | Produced by gut microbiota from l-carnitine and choline metabolism | Several hours to days | Can be detected after consumption of dietary choline or l-carnitine, early in atherosclerosis | Moderate sensitivity for cardiovascular risk; linked to poor prognosis in CVD | Dietary intake, gut microbiota composition, and kidney function can influence TMAO levels. |
| MicroRNAs (miRNAs) | Released from cardiomyocytes, endothelial cells, and other cells during cardiovascular stress | Varies (hours to days) | Can be detected within hours of AMI or heart failure onset | High specificity for distinct CVDs; good sensitivity for early detection | Stable in plasma, but affected by collection and processing methods. Interference from other conditions can complicate interpretation. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Netala, V.R.; Hou, T.; Wang, Y.; Zhang, Z.; Teertam, S.K. Cardiovascular Biomarkers: Tools for Precision Diagnosis and Prognosis. Int. J. Mol. Sci. 2025, 26, 3218. https://doi.org/10.3390/ijms26073218
Netala VR, Hou T, Wang Y, Zhang Z, Teertam SK. Cardiovascular Biomarkers: Tools for Precision Diagnosis and Prognosis. International Journal of Molecular Sciences. 2025; 26(7):3218. https://doi.org/10.3390/ijms26073218
Chicago/Turabian StyleNetala, Vasudeva Reddy, Tianyu Hou, Yanbo Wang, Zhijun Zhang, and Sireesh Kumar Teertam. 2025. "Cardiovascular Biomarkers: Tools for Precision Diagnosis and Prognosis" International Journal of Molecular Sciences 26, no. 7: 3218. https://doi.org/10.3390/ijms26073218
APA StyleNetala, V. R., Hou, T., Wang, Y., Zhang, Z., & Teertam, S. K. (2025). Cardiovascular Biomarkers: Tools for Precision Diagnosis and Prognosis. International Journal of Molecular Sciences, 26(7), 3218. https://doi.org/10.3390/ijms26073218