
Angiotensin Dysregulation in Patients with Arterial Aneurysms


 ,
,
Abstract
1. Introduction
2. Results
2.1. Sample Characteristics
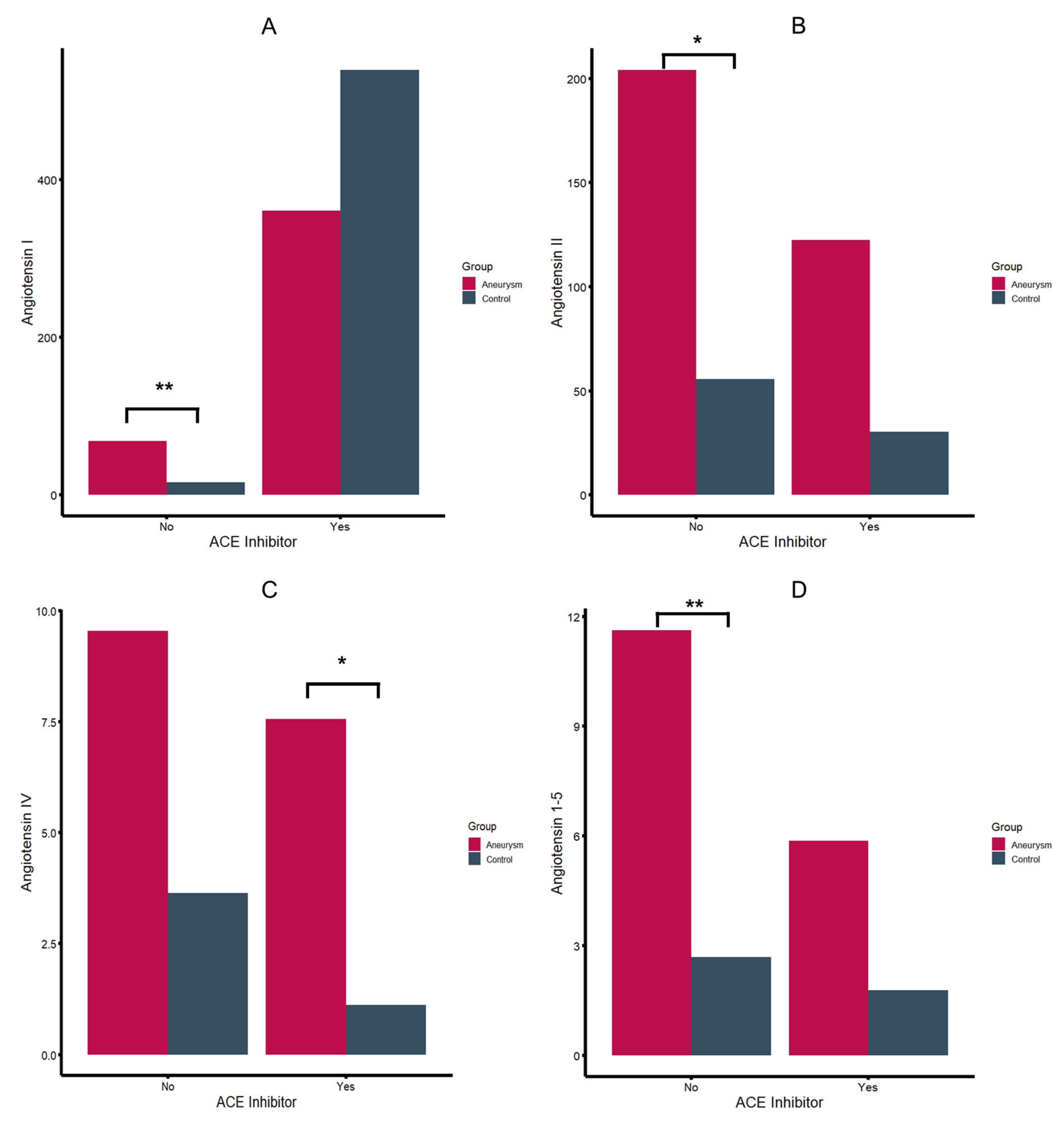
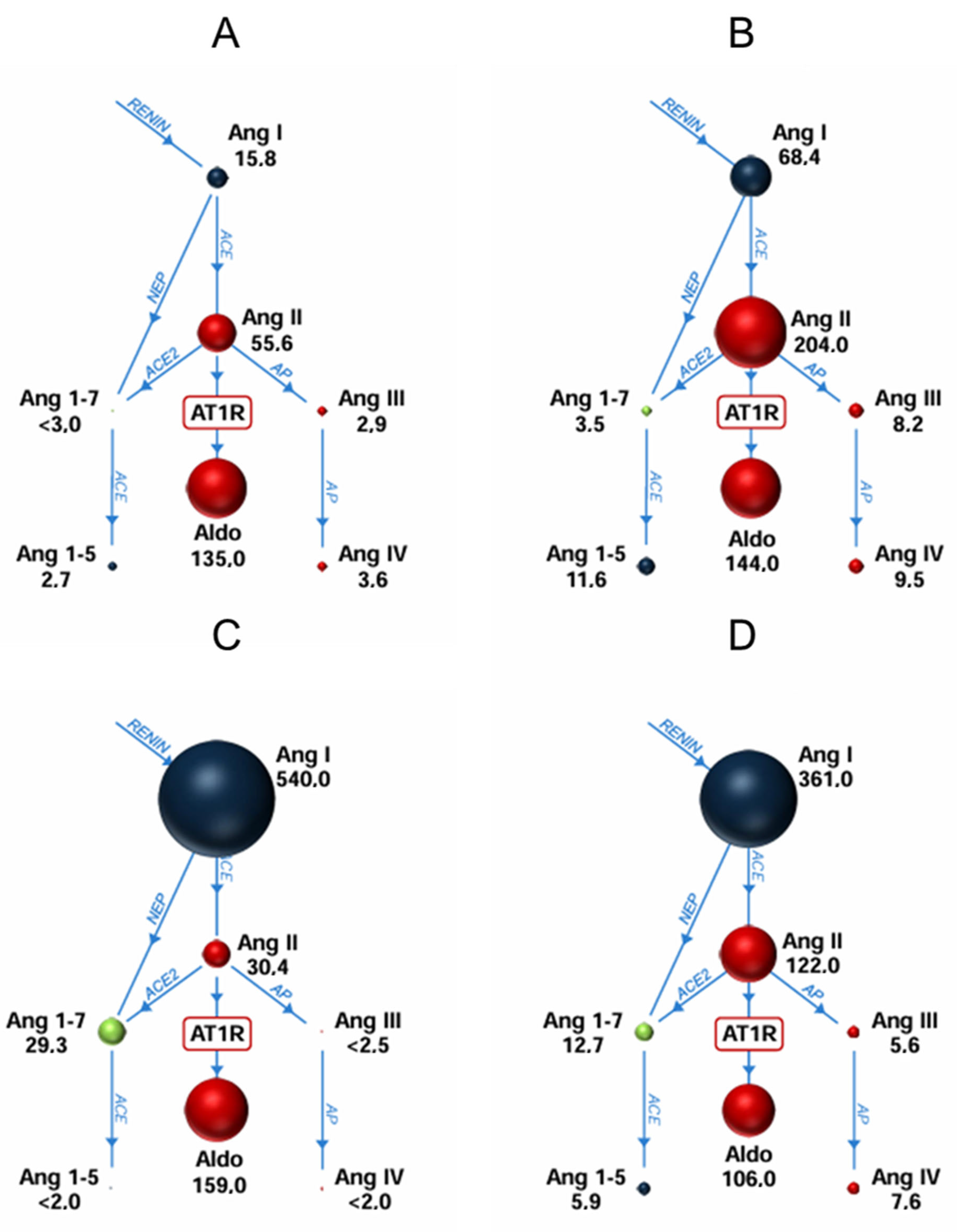
2.2. Systemic Angiotensin Quantification
2.3. Changes in RAS Profiles After Intervention
2.4. Tissue Samples
3. Discussion
Limitations
4. Materials and Methods
4.1. IRB Approval
4.2. Design and Study Participants
4.3. Material Harvested and Tissue Preparation
4.4. RAS Equilibrium Analysis and Enzyme Activities
4.5. Controls
4.6. Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Muscha Steckelings, U.; Bader, M. Renin-angiotensin system in aortic aneurysm still adding puzzle stones to an anything but complete picture. Hypertension 2018, 72, 579–581. [Google Scholar] [CrossRef] [PubMed]
- Tian, K.; Thanigaimani, S.; Gibson, K.; Golledge, J. Systematic Review Examining the Association Between Angiotensin Converting Enzyme Inhibitor or Angiotensin Receptor Blocker Prescription and Abdominal Aortic Aneurysm Growth and Events. Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 2024, 68, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Puertas-Umbert, L.; Almendra-Pegueros, R.; Jiménez-Altayó, F.; Sirvent, M.; Galán, M.; Martínez-González, J.; Rodríguez, C. Novel pharmacological approaches in abdominal aortic aneurysm. Clin. Sci. 2023, 137, 1167. [Google Scholar] [CrossRef]
- Jahangir, E.; Lipworth, L.; Edwards, T.L.; Kabagambe, E.K.; Mumma, M.T.; Mensah, G.A.; Fazio, S.; Blot, W.J.; Sampson, U.K.A. Smoking, sex, risk factors and abdominal aortic aneurysms: A prospective study of 18 782 persons aged above 65 years in the Southern Community Cohort Study. J. Epidemiol. Community Health 2015, 69, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Joergensen, T.M.M.; Christensen, K.; Lindholt, J.S.; Larsen, L.A.; Green, A.; Houlind, K. Editor’s Choice—High Heritability of Liability to Abdominal Aortic Aneurysms: A Population Based Twin Study. Eur. J. Vasc. Endovasc. Surg. 2016, 52, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Kobeissi, E.; Hibino, M.; Pan, H.; Aune, D. Blood pressure, hypertension and the risk of abdominal aortic aneurysms: A systematic review and meta-analysis of cohort studies. Eur. J. Epidemiol. 2019, 34, 547–555. [Google Scholar] [CrossRef]
- Sweeting, M.J.; Thompson, S.G.; Brown, L.C.; Powell, J.T. Meta-analysis of individual patient data to examine factors affecting growth and rupture of small abdominal aortic aneurysms. Br. J. Surg. 2012, 99, 655–665. [Google Scholar] [CrossRef]
- Sawada, H.; Lu, H.S.; Cassis, L.A.; Daugherty, A. Twenty Years of Studying AngII (Angiotensin II)-Induced Abdominal Aortic Pathologies in Mice: Continuing Questions and Challenges to Provide Insight into the Human Disease. Arterioscler. Thromb. Vasc. Biol. 2022, 42, 277–288. [Google Scholar]
- Rateri, D.L.; Howatt, D.A.; Moorleghen, J.J.; Charnigo, R.; Cassis, L.A.; Daugherty, A. Prolonged infusion of angiotensin II in apoE(-/-) mice promotes macrophage recruitment with continued expansion of abdominal aortic aneurysm. Am. J. Pathol. 2011, 179, 1542–1548. [Google Scholar] [CrossRef]
- Khoury, M.K.; Stranz, A.R.; Liu, B. Pathophysiology of Aortic Aneurysms: Insights from Animal Studies. Cardiol. Cardiovasc. Med. 2020, 4, 498–514. [Google Scholar] [CrossRef]
- Quintana, R.A.; Taylor, W.R. Cellular mechanisms of aortic aneurysm formation. Circ. Res. 2019, 124, 607–618. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Rateri, D.L.; Bruemmer, D.; Cassis, L.A.; Daugherty, A. Involvement of the renin-angiotensin system in abdominal and thoracic aortic aneurysms. Clin. Sci. 2012, 123, 531–543. [Google Scholar] [CrossRef] [PubMed]
- Golledge, J.; Muller, J.; Daugherty, A.; Norman, P. Abdominal Aortic Aneurysm. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 2605–2613. [Google Scholar] [CrossRef] [PubMed]
- Daugherty, A.; Manning, M.W.; Cassis, L.A. Angiotensin II promotes atherosclerotic lesions and aneurysms in apolipoprotein E–deficient mice. J. Clin. Investig. 2000, 105, 1605–1612. [Google Scholar] [CrossRef]
- Chappell, M.C. Biochemical evaluation of the renin-angiotensin system: The good, bad, and absolute? Am. J. Physiol. Heart Circ. Physiol. 2016, 310, H137–H152. [Google Scholar] [CrossRef]
- Santos, R.A.S.; Sampaio, W.O.; Alzamora, A.C.; Motta-Santos, D.; Alenina, N.; Bader, M.; Campagnole-Santos, M.J. The ACE2/Angiotensin-(1-7)/Mas axis of the renin-angiotensin system: Focus on Angiotensin-(1-7). Physiol. Rev. 2018, 98, 505–553. [Google Scholar] [CrossRef]
- Jadli, A.S.; Gomes, K.P.; Ballasy, N.N.; Wijesuriya, T.M.; Belke, D.; Fedak, P.W.M.; Patel, V.B. Inhibition of smooth muscle cell death by Angiotensin 1-7 protects against abdominal aortic aneurysm. Biosci. Rep. 2023, 43, BSR20230718. [Google Scholar] [CrossRef]
- Karasaki, K.; Kokubo, H.; Bumdelger, B.; Kaji, N.; Sakai, C.; Ishida, M.; Yoshizumi, M. Angiotensin II Type 1 Receptor Blocker Prevents Abdominal Aortic Aneurysm Progression in Osteoprotegerin-Deficient Mice via Upregulation of Angiotensin (1–7). J. Am. Heart Assoc. 2023, 12, e027589. [Google Scholar] [CrossRef]
- Van Rooyen, J.M.; Poglitsch, M.; Huisman, H.W.; Mels, C.M.C.; Kruger, R.; Malan, L.; Botha, S.; Lammertyn, L.; Gafane, L.; Schutte, A.E. Quantification of systemic renin-angiotensin system peptides of hypertensive black and white African men established from the RAS-Fingerprint®. J. Renin-Angiotensin-Aldosterone Syst. JRAAS 2016, 17, 1–7. [Google Scholar] [CrossRef]
- Kaschina, E.; Scholz, H.; Steckelings, U.M.; Sommerfeld, M.; Kemnitz, U.R.; Artuc, M.; Schmidt, S.; Unger, T. Transition from atherosclerosis to aortic aneurysm in humans coincides with an increased expression of RAS components. Atherosclerosis 2009, 205, 396–403. [Google Scholar] [CrossRef]
- Moltzer, E.; Essers, J.; Van Esch, J.H.M.; Roos-Hesselink, J.W.; Danser, A.H.J. The role of the renin-angiotensin system in thoracic aortic aneurysms: Clinical implications. Pharmacol. Ther. 2011, 131, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Q.; Heizhati, M.; Lin, M.; Wang, M.; Yao, X.; Gan, L.; Luo, Q.; Zhang, W.; Hong, J.; Yue, N.; et al. Higher Plasma Aldosterone Concentrations Are Associated with Elevated Risk of Aortic Dissection and Aneurysm: A Case-Control Study. Hypertension 2022, 79, 736–746. [Google Scholar] [CrossRef]
- van Thiel, B.S.; van der Pluijm, I.; te Riet, L.; Essers, J.; Danser, A.H.J. The renin-angiotensin system and its involvement in vascular disease. Eur. J. Pharmacol. 2015, 763, 3–14. [Google Scholar] [CrossRef]
- Crowley, S.D.; Navar, L.G.; Prieto, M.C.; Gurley, S.B.; Coffman, T.M. Kidney Renin–Angiotensin System: Lost in a RAS Cascade. Hypertension 2024, 81, 682–686. [Google Scholar] [CrossRef] [PubMed]
- Forrester, S.J.; Booz, G.W.; Sigmund, C.D.; Coffman, T.M.; Kawai, T.; Rizzo, V.; Scalia, R.; Eguchi, S. Angiotensin II signal transduction: An update on mechanisms of physiology and pathophysiology. Physiol. Rev. 2018, 98, 1627–1738. [Google Scholar] [CrossRef] [PubMed]
- Martyniak, A.; Tomasik, P.J. A New Perspective on the Renin-Angiotensin System. Diagnostics 2022, 13, 16. [Google Scholar] [CrossRef]
- Piqueras, L.; Sanz, M.J. Angiotensin II and leukocyte trafficking: New insights for an old vascular mediator. Role of redox-signaling pathways. Free Radic. Biol. Med. 2020, 157, 38–54. [Google Scholar] [CrossRef]
- Gibbons, G.H.; Pratt, R.E.; Dzau, V.J. Vascular smooth muscle cell hypertrophy vs. hyperplasia. Autocrine transforming growth factor-beta 1 expression determines growth response to angiotensin II. J. Clin. Investig. 1992, 90, 456–461. [Google Scholar] [CrossRef]
- Griendling, K.K.; Minieri, C.A.; Ollerenshaw, J.D.; Alexander, R.W. Angiotensin II stimulates NADH and NADPH oxidase activity in cultured vascular smooth muscle cells. Circ. Res. 1994, 74, 1141–1148. [Google Scholar] [CrossRef]
- Brasier, A.R.; Recinos, A.; Eledrisi, M.S.; Runge, M.S. Vascular inflammation and the renin-angiotensin system. Arterioscler. Thromb. Vasc. Biol. 2002, 22, 1257–1266. [Google Scholar] [CrossRef]
- Dell’italia, L.J.; Collawn, J.F.; Ferrario, C.M. Multifunctional role of chymase in acute and chronic tissue injury and remodeling. Circ. Res. 2018, 122, 319–336. [Google Scholar] [CrossRef] [PubMed]
- Reyes, S.; Varagic, J.; Ahmad, S.; VonCannon, J.; Kon, N.D.; Wang, H.; Groban, L.; Cheng, C.P.; Dell’Italia, L.J.; Ferrario, C.M. Novel Cardiac Intracrine Mechanisms Based on Ang-(1-12)/Chymase Axis Require a Revision of Therapeutic Approaches in Human Heart Disease. Curr. Hypertens. Rep. 2017, 19, 16. [Google Scholar] [CrossRef] [PubMed]
- Yugandhar, V.G.; Clark, M.A. Angiotensin III: A physiological relevant peptide of the renin angiotensin system. Peptides 2013, 46, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Chai, S.Y.; Fernando, R.; Peck, G.; Ye, S.Y.; Mendelsohn, F.A.O.; Jenkins, T.A.; Albiston, A.L. The angiotensin IV/AT4 receptor. Cell. Mol. Life Sci. 2004, 61, 2728–2737. [Google Scholar] [CrossRef] [PubMed]
- Lochard, N.; Thibault, G.; Silversides, D.W.; Touyz, R.M.; Reudelhuber, T.L. Chronic production of angiotensin IV in the brain leads to hypertension that is reversible with an angiotensin II AT1 receptor antagonist. Circ. Res. 2004, 94, 1451–1457. [Google Scholar] [CrossRef]
- Patel, V.B.; Zhong, J.C.; Grant, M.B.; Oudit, G.Y. Role of the ACE2/angiotensin 1-7 axis of the renin-angiotensin system in heart failure. Circ. Res. 2016, 118, 1313–1326. [Google Scholar] [CrossRef]
- Xue, F.; Yang, J.; Cheng, J.; Sui, W.; Cheng, C.; Li, H.; Zhang, M.; Zhang, J.; Xu, X.; Ma, J.; et al. Angiotensin-(1-7) mitigated angiotensin II-induced abdominal aortic aneurysms in apolipoprotein E-knockout mice. Br. J. Pharmacol. 2020, 177, 1719–1734. [Google Scholar] [CrossRef]
- Jadli, A.S.; Ballasy, N.N.; Gomes, K.P.; Mackay, C.D.A.; Meechem, M.; Wijesuriya, T.M.; Belke, D.; Thompson, J.; Fedak, P.W.M.; Patel, V.B. Attenuation of Smooth Muscle Cell Phenotypic Switching by Angiotensin 1-7 Protects against Thoracic Aortic Aneurysm. Int. J. Mol. Sci. 2022, 23, 15566. [Google Scholar] [CrossRef]
- Yu, L.; Yuan, K.; Phuong, H.T.A.; Park, B.M.; Kim, S.H. Angiotensin-(1-5), an active mediator of renin-angiotensin system, stimulates ANP secretion via Mas receptor. Peptides 2016, 86, 33–41. [Google Scholar] [CrossRef]
- Park, B.M.; Li, W.; Kim, S.H. Cardio-protective effects of angiotensin-(1-5) via mas receptor in rats against ischemic-perfusion injury. Peptides 2021, 139, 170516. [Google Scholar] [CrossRef]
- Miyake, T.; Miyake, T.; Shimizu, H.; Morishita, R. Inhibition of Aneurysm Progression by Direct Renin Inhibition in a Rabbit Model. Hypertension 2017, 70, 1201–1209. [Google Scholar] [CrossRef] [PubMed]
- Tomimori, Y.; Manno, A.; Tanaka, T.; Futamura-Takahashi, J.; Muto, T.; Nagahira, K. ASB17061, a novel chymase inhibitor, prevented the development of angiotensin II-induced abdominal aortic aneurysm in apolipoprotein E-deficient mice. Eur. J. Pharmacol. 2019, 856, 172403. [Google Scholar] [CrossRef] [PubMed]
- Lange, C.; Sommerfeld, M.; Namsolleck, P.; Kintscher, U.; Unger, T.; Kaschina, E. AT2R (angiotensin AT2 receptor) agonist, compound 21, prevents abdominal aortic aneurysm progression in the rat. Hypertension 2018, 72, E20–E29. [Google Scholar] [CrossRef] [PubMed]
- Ansary, T.M.; Nakano, D.; Nishiyama, A. Diuretic Effects of Sodium Glucose Cotransporter 2 Inhibitors and Their Influence on the Renin-Angiotensin System. Int. J. Mol. Sci. 2019, 20, 629. [Google Scholar] [CrossRef] [PubMed]
- Domenig, O.; Manzel, A.; Grobe, N.; Königshausen, E.; Kaltenecker, C.C.; Kovarik, J.J.; Stegbauer, J.; Gurley, S.B.; Van Oyen, D.; Antlanger, M.; et al. Neprilysin is a Mediator of Alternative Renin-Angiotensin-System Activation in the Murine and Human Kidney. Sci. Rep. 2016, 6, 33678. [Google Scholar] [CrossRef]
- Larouche-Lebel, É.; Loughran, K.A.; Huh, T.; Oyama, M.A. Effect of angiotensin receptor blockers and angiotensin converting enzyme 2 on plasma equilibrium angiotensin peptide concentrations in dogs with heart disease. J. Vet. Intern. Med. 2021, 35, 22–32. [Google Scholar] [CrossRef]
- Guo, Z.; Poglitsch, M.; McWhinney, B.C.; Ungerer, J.P.J.; Ahmed, A.H.; Gordon, R.D.; Wolley, M.; Stowasser, M. Measurement of Equilibrium Angiotensin II in the Diagnosis of Primary Aldosteronism. Clin. Chem. 2020, 66, 483–492. [Google Scholar] [CrossRef]
- Adin, D.; Atkins, C.; Domenig, O.; DeFrancesco, T.; Keene, B.; Tou, S.; Stern, J.A.; Meurs, K.M. Renin-angiotensin aldosterone profile before and after angiotensin-converting enzyme-inhibitor administration in dogs with angiotensin-converting enzyme gene polymorphism. J. Vet. Intern. Med. 2020, 34, 600–606. [Google Scholar] [CrossRef]
- Kaltenecker, C.C.; Domenig, O.; Kopecky, C.; Antlanger, M.; Poglitsch, M.; Berlakovich, G.; Kain, R.; Stegbauer, J.; Rahman, M.; Hellinger, R.; et al. Critical Role of Neprilysin in Kidney Angiotensin Metabolism. Circ. Res. 2020, 127, 593–606. [Google Scholar] [CrossRef]
- Antlanger, M.; Domenig, O.; Kaltenecker, C.C.; Kovarik, J.J.; Rathkolb, V.; Müller, M.M.; Schwaiger, E.; Hecking, M.; Poglitsch, M.; Säemann, M.D.; et al. Combined sodium glucose co-transporter-2 inhibitor and angiotensin-converting enzyme inhibition upregulates the renin-angiotensin system in chronic kidney disease with type 2 diabetes: Results of a randomized, double-blind, placebo-controlled exploratory trial. Diabetes Obes. Metab. 2022, 24, 816–826. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| ACE Inhibitor | No ACE Inhibitor | |||
|---|---|---|---|---|
| Aneurysm | Controls | Aneurysm | Controls | |
| N | 19 | 49 | 18 | 7 |
| Age | 71 (62–75) | 67 (57–75) | 76 (66–81) | 52 (50–63) |
| Sex (m:f) | 15 (78.9%):4 (21.1%) | 32 (65.3%):17 (34.7%) | 17 (94.4%):1 (5.6%) | 2 (28.6%):5 (71.4%) |
| BMI | 28.3 (4.8) | 28.9 (3.8) | 25.3 (3.7) | 27.5 (4.0) |
| Arterial hypertension | 19 (100%) | 49 (100%) | 9 (50.0%) | 4 (57.1%) |
| Diabetes | 2 (10.5%) | 25 (51.0%) | 6 (33.3%) | 2 (28.6%) |
| PAD | 4 (21.1%) | 5 (10.2%) | 4 (22.2%) | 4 (57.1%) |
| CHD | 9 (47.4%) | 10 (20.4%) | 2 (11.1%) | 1 (14.3%) |
| Chronic kidney disease | 8 (42.1%) | 46 (93.9%) | 4 (22.2%) | 1 (14.3%) |
| ACEi | No ACEi | |||||
|---|---|---|---|---|---|---|
| Aneurysm | Controls | p-Value | Aneurysm | Controls | p-Value | |
| N | 19 | 49 | - | 18 | 7 | - |
| Angiotensin 1–7 | 12.7 | 29.3 | 0.061 | 3.5 | 1.0 | 0.67 |
| Angiotensin 1–5 | 5.9 | 1.8 | 0.061 | 11.6 | 2.7 | 0.004 * |
| Angiotensin I (1–10) | 361 | 540 | 0.322 | 68.4 | 15.8 | 0.002 * |
| Angiotensin II (1–8) | 122 | 30.4 | 0.122 | 204 | 55.6 | 0.047 * |
| Angiotensin III (2–8) | 5.6 | 1.2 | 0.091 | 8.2 | 2.9 | 0.386 |
| Angiotensin IV (3–8) | 7.6 | 1.1 | 0.05 | 9.5 | 3.6 | 0.095 |
| Aldosterone | 106 | 159 | 0.147 | 144 | 135 | 0.745 |
| Neprilysin | 0.4 | 0.4 | 0.995 | 0.9 | 0.3 | 0.204 |
| ACE2 | 1.1 | 1.5 | 0.042 * | 1.5 | 1.1 | 0.458 |
| ACE | 0.9 | 0.3 | 0.067 | 2.8 | 4.5 | 0.064 |
| Renin | 483 | 570 | 0.64 | 273 | 71.5 | 0.014 * |
| ACEi | No ACEi | |||
|---|---|---|---|---|
| Pre | Post | Pre | Post | |
| N | 15 | 9 | 13 | 9 |
| Angiotensin 1–7 | 12.8 | 6.7 | 3.7 | 4.0 |
| Angiotensin 1–5 | 4.9 | 5.5 | 13.8 | 8.9 |
| Angiotensin I (1–10) | 408 | 112 | 75.6 | 116 |
| Angiotensin II (1–8) | 86.0 | 126 | 251 | 190 |
| Angiotensin III (2–8) | 3.5 | 7.1 | 10.8 | 8.3 |
| Angiotensin IV (3–8) | 5.6 | 8.0 | 11.7 | 9.8 |
| Aldosterone | 121 | 106 | 152 | 287 |
| Renin | 494 | 241 | 326 | 206 |
| ACE | 0.6 | 1.5 | 2.8 | 2.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leinweber, M.E.; Walter, C.; Assadian, A.; Kopecky, C.; Domenig, O.; Kovarik, J.J.; Hofmann, A.G. Angiotensin Dysregulation in Patients with Arterial Aneurysms. Int. J. Mol. Sci. 2025, 26, 1502. https://doi.org/10.3390/ijms26041502
Leinweber ME, Walter C, Assadian A, Kopecky C, Domenig O, Kovarik JJ, Hofmann AG. Angiotensin Dysregulation in Patients with Arterial Aneurysms. International Journal of Molecular Sciences. 2025; 26(4):1502. https://doi.org/10.3390/ijms26041502
Chicago/Turabian StyleLeinweber, Maria Elisabeth, Corinna Walter, Afshin Assadian, Chantal Kopecky, Oliver Domenig, Johannes Josef Kovarik, and Amun Georg Hofmann. 2025. "Angiotensin Dysregulation in Patients with Arterial Aneurysms" International Journal of Molecular Sciences 26, no. 4: 1502. https://doi.org/10.3390/ijms26041502
APA StyleLeinweber, M. E., Walter, C., Assadian, A., Kopecky, C., Domenig, O., Kovarik, J. J., & Hofmann, A. G. (2025). Angiotensin Dysregulation in Patients with Arterial Aneurysms. International Journal of Molecular Sciences, 26(4), 1502. https://doi.org/10.3390/ijms26041502