
Advancing Craniopharyngioma Management: A Systematic Review of Current Targeted Therapies and Future Perspectives

 ,
,  ,
, 
 ,
,  ,
,
Abstract
1. Introduction
2. Methods
2.1. Literature Review
2.2. Data Extraction
2.3. Outcomes
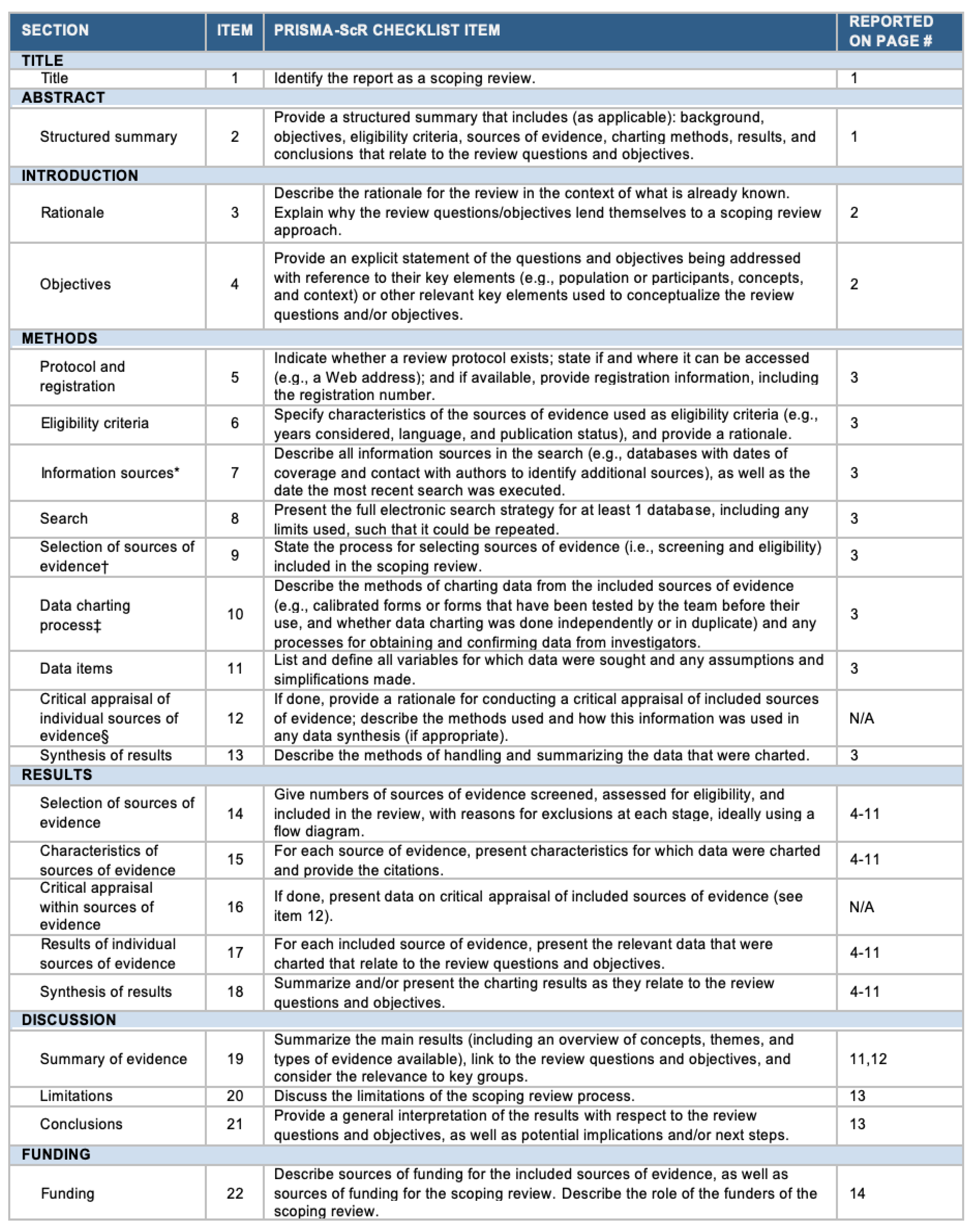
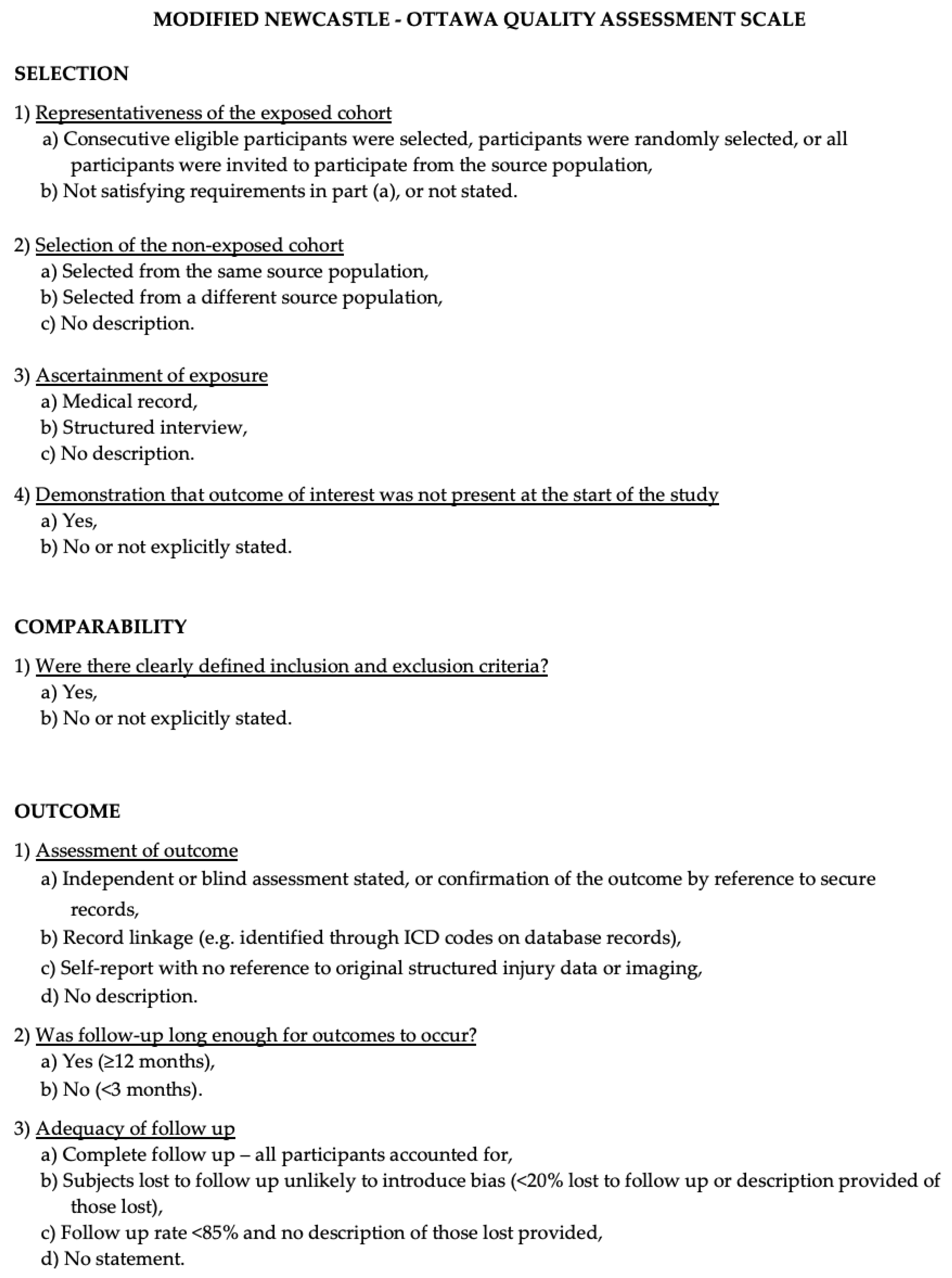
2.4. Risk of Bias Assessment
2.5. Statistical Analysis
3. Results and Discussion
3.1. Literature Review
3.2. Data Analysis
3.2.1. State of the Art of Adamantinomatous Craniopharyngioma-Targeted Therapies
3.2.2. State of the Art of Papillary Craniopharyngioma-Targeted Therapies
3.2.3. Overall Survival and Adverse Events
3.2.4. The Emerging Role of Stereotactic Radiosurgery Radioenhancers for the Management of Craniopharyngiomas
3.2.5. The Role of Targeted Therapies for Other Skull Base Lesions
3.2.6. Limitations and Future Directions
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Reyes, M.; Taghvaei, M.; Yu, S.; Sathe, A.; Collopy, S.; Prashant, G.N.; Evans, J.J.; Karsy, M. Targeted Therapy in the Management of Modern Craniopharyngiomas. Front. Biosci. 2022, 27, 136. [Google Scholar] [CrossRef] [PubMed]
- Calvanese, F.; Jacquesson, T.; Manet, R.; Vasiljevic, A.; Lasolle, H.; Ducray, F.; Raverot, G.; Jouanneau, E. Neoadjuvant B-RAF and MEK Inhibitor Targeted Therapy for Adult Papillary Craniopharyngiomas: A New Treatment Paradigm. Front. Endocrinol. 2022, 13, 882381. [Google Scholar] [CrossRef] [PubMed]
- Mrowczynski, O.D.; Langan, S.T.; Rizk, E.B. Craniopharyngiomas: A systematic review and evaluation of the current intratumoral treatment landscape. Clin. Neurol. Neurosurg. 2018, 166, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Whelan, R.; Hengartner, A.; Folzenlogen, Z.; Prince, E.; Hankinson, T.C. Adamantinomatous craniopharyngioma in the molecular age and the potential of targeted therapies: A review. Childs Nerv. Syst. 2020, 36, 1635–1642. [Google Scholar] [CrossRef] [PubMed]
- Hengartner, A.C.; Prince, E.; Vijmasi, T.; Hankinson, T.C. Adamantinomatous craniopharyngioma: Moving toward targeted therapies. Neurosurg. Focus. 2020, 48, E7. [Google Scholar] [CrossRef] [PubMed]
- Jannelli, G.; Calvanese, F.; Paun, L.; Raverot, G.; Jouanneau, E. Current Advances in Papillary Craniopharyngioma: State-of-the-Art Therapies and Overview of the Literature. Brain Sci. 2023, 13, 515. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of Non-Randomized Studies in Meta-Analysis|Request PDF. Available online: https://www.researchgate.net/publication/261773681_The_Newcastle-Ottawa_Scale_NOS_for_Assessing_the_Quality_of_Non-Randomized_Studies_in_Meta-Analysis (accessed on 19 July 2023).
- Jakacki, R.I.; Cohen, B.H.; Jamison, C.; Mathews, V.P.; Arenson, E.; Longee, D.C.; Hilden, J.; Cornelius, A.; Needle, M.; Heilman, D.; et al. Phase II evaluation of interferon-alpha-2a for progressive or recurrent craniopharyngiomas. J. Neurosurg. 2000, 92, 255–260. [Google Scholar] [CrossRef]
- Yeung, J.T.; Pollack, I.F.; Panigrahy, A.; Jakacki, R.I. Pegylated interferon-α-2b for children with recurrent craniopharyngioma. J. Neurosurg. Pediatr. 2012, 10, 498–503. [Google Scholar] [CrossRef]
- Grob, S.; Mirsky, D.M.; Donson, A.M.; Dahl, N.; Foreman, N.K.; Hoffman, L.M.; Hankinson, T.C.; Levy, J.M.M. Targeting IL-6 Is a Potential Treatment for Primary Cystic Craniopharyngioma. Front. Oncol. 2019, 9, 791. [Google Scholar] [CrossRef]
- Goldman, S.; Pollack, I.F.; Jakacki, R.I.; Billups, C.A.; Poussaint, Y.T.; Adesina, A.M.; Panigrahy, A.; Parsons, D.W.; Broniscer, A.; Robinson, G.W.; et al. Phase II study of peginterferon alpha-2b for patients with unresectable or recurrent craniopharyngiomas: A Pediatric Brain Tumor Consortium report. Neuro Oncol. 2020, 22, 1696–1704. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.; Allen, J.; Zagzag, D.; Wisoff, J.; Radmanesh, A.; Gindin, T.; Nicolaides, T. Radiologic response to MEK inhibition in a patient with a WNT-activated craniopharyngioma. Pediatr. Blood Cancer 2021, 68, e28753. [Google Scholar] [CrossRef] [PubMed]
- de Vos-Kerkhof, E.; Buis, D.R.; Lequin, M.H.; Bennebroek, C.A.; Aronica, E.; Hulleman, E.; Zwaveling-Soonawala, N.; van Santen, H.M.; Schouten-van Meeteren, A.Y.N. Tocilizumab for the fifth progression of cystic childhood craniopharyngioma—A case report. Front. Endocrinol. 2023, 14, 1225734. [Google Scholar] [CrossRef] [PubMed]
- De Rosa, A.; Calvanese, F.; Ducray, F.; Vasiljevic, A.; Manet, R.; Raverot, G.; Jouanneau, E. First evidence of anti-VEGF efficacy in an adult case of adamantinomatous craniopharyngioma: Case report and illustrative review. Ann. D’endocrinologie 2023, 84, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Brastianos, P.K.; Shankar, G.M.; Gill, C.M.; Taylor-Weiner, A.; Nayyar, N.; Panka, D.J.; Sullivan, R.J.; Frederick, D.T.; Abedalthagafi, M.; Jones, P.S.; et al. Dramatic Response of BRAF V600E Mutant Papillary Craniopharyngioma to Targeted Therapy. J. Natl. Cancer Inst. 2016, 108, djv310. [Google Scholar] [CrossRef]
- Aylwin, S.J.B.; Bodi, I.; Beaney, R. Pronounced response of papillary craniopharyngioma to treatment with vemurafenib, a BRAF inhibitor. Pituitary. 2016, 19, 544–546. [Google Scholar] [CrossRef]
- Roque, A.; Odia, Y. BRAF-V600E mutant papillary craniopharyngioma dramatically responds to combination BRAF and MEK inhibitors. CNS Oncol. 2017, 6, 95–99. [Google Scholar] [CrossRef]
- Rostami, E.; Witt Nyström, P.; Libard, S.; Wikström, J.; Casar-Borota, O.; Gudjonsson, O. Recurrent papillary craniopharyngioma with BRAFV600E mutation treated with neoadjuvant-targeted therapy. Acta Neurochir. 2017, 159, 2217–2221. [Google Scholar] [CrossRef]
- Himes, B.T.; Ruff, M.W.; Van Gompel, J.J.; Park, S.S.; Galanis, E.; Kaufmann, T.J.; Uhm, J.H. Recurrent papillary craniopharyngioma with BRAF V600E mutation treated with dabrafenib: Case report. J. Neurosurg. 2018, 130, 1299–1303. [Google Scholar] [CrossRef]
- Juratli, T.A.; Jones, P.S.; Wang, N.; Subramanian, M.; Aylwin, S.J.B.; Odia, Y.; Rostami, E.; Gudjonsson, O.; Shaw, B.L.; Cahill, D.P.; et al. Targeted treatment of papillary craniopharyngiomas harboring BRAF V600E mutations. Cancer 2019, 125, 2910–2914. [Google Scholar] [CrossRef]
- Rao, M.; Bhattacharjee, M.; Shepard, S.; Hsu, S. Newly diagnosed papillary craniopharyngioma with BRAF V600E mutation treated with single-agent selective BRAF inhibitor dabrafenib: A case report. Oncotarget 2019, 10, 6038–6042. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, A.; Mrowczynski, O.D.; Greene, A.; Ryan, S.; Chung, C.; Zacharia, B.E.; Glantz, M. Dual BRAF/MEK therapy in BRAF V600E-mutated primary brain tumors: A case series showing dramatic clinical and radiographic responses and a reduction in cutaneous toxicity. J. Neurosurg. 2019, 133, 1704–1709. [Google Scholar] [CrossRef] [PubMed]
- Di Stefano, A.L.; Guyon, D.; Sejean, K.; Feuvret, L.; Villa, C.; Berzero, G.; Bullet, V.D.; Halimi, E.; Boulin, A.; Baussart, B.; et al. Medical debulking with BRAF/MEK inhibitors in aggressive BRAF-mutant craniopharyngioma. Neurooncol Adv. 2020, 2, vdaa141. [Google Scholar] [CrossRef] [PubMed]
- Khaddour, K.; Chicoine, M.R.; Huang, J.; Dahiya, S.; Ansstas, G. Successful Use of BRAF/MEK Inhibitors as a Neoadjuvant Approach in the Definitive Treatment of Papillary Craniopharyngioma. J. Natl. Compr. Canc Netw. 2020, 18, 1590–1595. [Google Scholar] [CrossRef] [PubMed]
- Gopal, M.; Thakur, G.; Puduvalli, V. Initial Presentation of Papillary Craniopharyngioma with BRAF Mutation Treated with Adjuvant Chemotherapy (867). Neurology 2020, 94 (Suppl. S15), 867. Available online: https://n.neurology.org/content/94/15_Supplement/867 (accessed on 2 December 2023). [CrossRef]
- Butt, S.U.R.; Mejias, A.; Morelli, C.; Torga, G.; Happe, M.; Patrikidou, A.; Arkenau, H.T. BRAF/MEK inhibitors for BRAF V600E-mutant cancers in non-approved setting: A case series. Cancer Chemother. Pharmacol. 2021, 87, 437–441. [Google Scholar] [CrossRef] [PubMed]
- Chik, C.L.; van Landeghem, F.K.H.; Easaw, J.C.; Mehta, V. Aggressive Childhood-onset Papillary Craniopharyngioma Managed With Vemurafenib, a BRAF Inhibitor. J. Endocr. Soc. 2021, 5, bvab043. [Google Scholar] [CrossRef]
- Nussbaum, P.E.; Nussbaum, L.A.; Torok, C.M.; Patel, P.D.; Yesavage, T.A.; Nussbaum, E.S. Case report and literature review of BRAF-V600 inhibitors for treatment of papillary craniopharyngiomas: A potential treatment paradigm shift. J. Clin. Pharm. Ther. 2022, 47, 826–831. [Google Scholar] [CrossRef]
- Lin, A.L.; Tabar, V.; Young, R.J.; Geer, E.B. Dabrafenib as a diagnostic and therapeutic strategy for the non-surgical management of papillary craniopharyngioma. Pituitary 2023, 26, 482–487. [Google Scholar] [CrossRef]
- Brastianos, P.K.; Twohy, E.; Geyer, S.; Gerstner, E.R.; Kaufmann, T.J.; Tabrizi, S.; Kabat, B.; Thierauf, J.; Ruff, M.W.; Bota, D.A.; et al. BRAF–MEK Inhibition in Newly Diagnosed Papillary Craniopharyngiomas. N. Engl. J. Med. 2023, 389, 118–126. [Google Scholar] [CrossRef]
- Shah, S.N.; Kaki, P.C.; Shah, S.S.; Shah, S.A. Concurrent Radiation and Targeted Therapy for Papillary Craniopharyngioma: A Case Report. Cureus 2023, 15, e40190. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.P.; Wang, Y.L.; Wang, L.C.; Liu, Z.Y.; Fan, R.R.; Zan, X.; Liang, R.C.; Yang, J.L.; Zhou, L.X.; Xu, J.G. Case Report: Successful Use of BRAF/MEK Inhibitors in Aggressive BRAF-mutant Craniopharyngioma. World Neurosurg. 2023, 180, e117–e126. [Google Scholar] [CrossRef] [PubMed]
- De Rosa, A.; Pineda, J.; Cavallo, L.M.; Di Somma, A.; Romano, A.; Topczewski, T.E.; Somma, T.; Solari, D.; Enseñat, J.; Cappabianca, P.; et al. Endoscopic endo- and extra-orbital corridors for spheno-orbital region: Anatomic study with illustrative case. Acta Neurochir. 2019, 161, 1633–1646. [Google Scholar] [CrossRef] [PubMed]
- Ganau, M.; Foroni, R.I.; Gerosa, M.; Zivelonghi, E.; Longhi, M.; Nicolato, A. Radiosurgical options in neuro-oncology: A review on current tenets and future opportunities. Part. I: Therapeutic strategies. Tumori 2014, 100, 459–465. [Google Scholar] [CrossRef]
- Ganau, M.; Foroni, R.I.; Gerosa, M.; Ricciardi, G.K.; Longhi, M.; Nicolato, A. Radiosurgical options in neuro-oncology: A review on current tenets and future opportunities. Part. II: Adjuvant radiobiological tools. Tumori 2015, 101, 57–63. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Author, Year | Age (Years), Sex | Prior Treatment | Systemic Targeted Treatment | Next Treatment | Outcomes | Adverse Events | |
|---|---|---|---|---|---|---|---|
| Agents | Duration (Months) | ||||||
| Jakacki et al. [9] 2000 | 6.1, F | STR, cyst drainage, VPS | IFN-2α: induction phase: 8,000,000 U/m2 QD via SC injection for 16 weeks; maintenance phase: 8,000,000 U/m2 three times per week for an additional 32 weeks in patients without progressive disease at 16 weeks; Tylenol and/or a nonsteroidal anti-inflammatory agent were given 30 min before each INF dose during the 1st week. | 12 | RT | PD (25 months after initiation). | All patients had fever during the first few treatments, usually accompanied by chills and myalgias. Two patients with panhypopituitarism developed hypotension and lethargy with fever after the first or second dose of INF but recovered rapidly after receiving stress doses of steroid medications. One patient had refractory frontal lobe seizures shortly after starting treatment. One patient had hyperpigmentation; 11 lost weight during the induction phase. Most patients began to gain weight during the maintenance phase, although 3 continued to lose weight. All patients gained weight since discontinuing INF therapy. Mild nausea; constitutional symptoms lasting 1–2 days after each dose, which lessened over time. Transient constitutional symptoms after each dose, which improved over time; grade 2 transaminase elevation and mild thrombocytopenia. Nausea and occasional vomiting for 24 h after each injection; symptoms disappeared as treatment continued. |
| Jakacki et al. [9] 2000 | 10.2, F | STR, cyst drainage | 7 | N/A | PD (7 months after initiation). | ||
| Jakacki et al. [9] 2000 | 13.4, M | STR × 2, cyst drainage, RT, GTR | 12 | N/A | PD (37 months after initiation). | ||
| Jakacki et al. [9] 2000 | 19.2, M | STR, cyst drainage, RT | N/A | N/A | N/A | ||
| Jakacki et al. [9] 2000 | 11.4, M | STR | 12 | N/A | PD (22 months after initiation). | ||
| Jakacki et al. [9] 2000 | 7.1, M | STR | N/A | N/A | N/A | ||
| Jakacki et al. [9] 2000 | 4.2, F | STR, intracystic bleomycin | 12 | N/A | PD (21 months after initiation). | ||
| Jakacki et al. [9] 2000 | 4.2, M | STR, cyst drainage | 9 | N/A | PD (21 months after initiation). | ||
| Jakacki et al. [9] 2000 | 13.1, M | GTR, cyst drainage, STR × 2, RT | 12 | N/A | SD >29 months after initiation. | ||
| Jakacki et al. [9] 2000 | 11.6, M | GTR | 12 | N/A | SD (25 months after initiation). | ||
| Jakacki et al. [9] 2000 | 13.9, M | STR, RT | 12 | N/A | PR >30 months after initiation. | ||
| Jakacki et al. [9] 2000 | 13.3, M | GTR | 12 | N/A | CR > 22 months after initiation. | ||
| Jakacki et al. [9] 2000 | 11.9, M | GTR × 2, phosphorus-32 × 2 | 12 | N/A | PD 21 months after initiation. | ||
| Jakacki et al. [9] 2000 | 14.5, M | GTR × 2, STR, RT, cyst drainage | N/A | N/A | N/A | ||
| Jakacki et al. [9] 2000 | 19.8, F | STR × 4, phosphorus-32, RT, cyst drainage, bleomycin | 3 | N/A | PD 3 months after initiation. | ||
| Yeung et al. [10] 2012 | 9, F | GTR | Pegylated IFN-α-2b: initial dose 3 μg/kg as weekly SC injection. | 24 | N/A | CR; disease-free 120 months after initiation. | Mild nausea; constitutional symptoms lasting 1–2 days after each dose, which lessened over time. |
| Yeung et al. [10] 2012 | 14, M | STR, RT (54 Gy) | Pegylated IFN-α-2b: initial dose 3 μg/kg as weekly SC injection; reduced to 1.5 mg/kg/week after 6 months. | 24 | N/A | PR 60 months after initiation. | Transient constitutional symptoms after each dose, which improved over time; grade 2 transaminase elevation and mild thrombocytopenia. |
| Yeung et al. [10] 2012 | 13, M | GTR × 3 | Pegylated IFN-α-2b: initial dose 1 μg/kg as weekly SC injection. | 15 | N/A | CR 4 months after stopping treatment. | Nausea and occasional vomiting for 24 h after each injection; symptoms disappeared as treatment continued. |
| Yeung et al. [10] 2012 | 14, M | STR × 2 | Pegylated IFN-α-2b: initial dose 3 μg/kg as weekly SC injection. | 12 | phosphorus-32. | A 30% decrease in the cystic component after 4 months of treatment; at 12 months the cyst increased in size and the patient was taken off the study and referred for treatment with radioactive phosphorus. | Transient fatigue and fevers for 2 days after each dose, which improved over time. |
| Yeung et al. [10] 2012 | 15, F | GTR | Pegylated IFN-α-2b: initial dose 1 μg/kg as weekly SC injection. | 6 (ongoing to achieve 24 months). | N/A | SD (6 months after initiation). | N/A |
| Grob et al. [11] 2019 | 3, M | Intra-cystic IFN-α and bleomycin | TCZ: 12 mg/kg IV every 2 weeks; 9 months later, IV bevacizumab every 2 weeks was co-administered. | 28 (14 on combination therapy). | Six months off therapy, an MRI demonstrated an overall increase in cystic mass, so combination therapy was re-initiated; levetiracetam was administered for seizures. | Decrease in cystic disease 4 months after re-initiation of combination therapy. | Neutropenia (CTCAE v5, grade 3). |
| Grob et al. [11] 2019 | 7, M | Cyst aspirations, STR (MTA), RT (54 Gy), intra-cystic bleomycin. | TCZ: 12 mg/kg IV every 2 weeks. | 7 | N/A | PR (after 6 months of therapy, from 26 × 28 × 27 mm to 18 × 24 × 18 mm). | N/A |
| Goldman et al. [12] 2020 | 2–25 (18 Pts), M (8 Pts) F (10 Pts) | Stratum 1: patients treated with surgery alone and who had never received radiotherapy; stratum 2: patients who had previously received radiotherapy. | Weekly SC injection of pegylated interferon alpha-2b (either PEG-Intron or Sylatron, based on availability) at a dose of 1 µg/kg/week; 6 weekly doses constituted a course; treatment could continue without break for up to 18 courses. | 24 | N/A | Stratum 1.—only 1 patient met the protocol definition of PR; stratum 1 was closed prematurely. Stratum 2—None of the 11 patients attained the primary endpoint of objective radiographic response, and the study was closed. | The most frequently reported toxicities were: decreased white blood cells and neutrophils, elevated alanine aminotransferase (ALT)/aspartate aminotransferase, and fever. There were 12 grade 3 toxicities over the 141 cycles given. Two patients experienced a total of 4 episodes of neutropenia and one patient experienced 2 episodes of grade 3 increase in ALT. Two of the eighteen patients came off therapy due to toxicity: 1 patient (stratum 2) refused further study treatment secondary to grade 2 flu-like symptoms after receiving only a single dose of peginterferon, and another patient (stratum 1) came off treatment after 3 cycles due to grade 3 ALT elevation. One additional patient in stratum 2 was dose-reduced during cycle 5 secondary to grade 3 anorexia. |
| Patel et al. [13] 2021 | 26, F | VPS Surgery x8, CT, RT, GKRS. | Binimetinib: 45 mg BID → 30 mg BID → 30 mg in the morning and 15 mg in the evening due to adverse effects. | 8 | N/A | SD (since December 2019). | Furuncles/papulopustular rash on tights and buttocks, nail dystrophy, hyponatremia, venous stasis with poor wound healing, fatigue/daytime sleepiness, and weight gain. |
| Vos-Kerkhof et al. [14] 2023 | 15, F | EVD; Surgery: STR; STR (EEA × 1; MTA × 1) VPS STR (combined left transcranial and transsphenoidal approach). | TCZ (20 mg/mL) 800 mg every 2 weeks IV during 1 h. | 9 | N/A | SD (To date, from the start of TCZ, both the residual cystic and solid components of the craniopharyngioma have remained stable). | N/A |
| De Rosa et al. [15] 2023 | 84, M | STR, neuroendoscopic cyst fenestration. | Bevacizumab (10 mg/kg) every 2 weeks. | 3 | VMAT RT | PR (66.1% shrinkage: of tumor volume at 3 months). | N/A |
| Author, Year | Age (Years), Sex | Prior Treatment | Systemic Targeted Treatment | Next Treatment | Outcomes | Adverse Events | |
|---|---|---|---|---|---|---|---|
| Agents | Duration (Months) | ||||||
| Brastianos et al. [16] 2015 | 39, M | Multiple surgery STR (MTA × 4, EEA × 1) | Dabrafenib (150 mg, PO BID); trametinib (2 mg, PO QD) after 21 days | 1,7 (52 days) | Surgery: STR (EEA) for consolidation tumor. resection on treatment day 38; RT (50.4 Gy in 28 fractions). | SD (after 18 months). | Low-grade fever (1 day). |
| Aylwin et al. [17] 2016 | 57, F | Surgery: STR(EEA); STR(EEA)-RT; STR(EEA) | Vemurafenib 960 mg BID | 10 (3 months interruption after 3 months) | Antimicrobial therapy, surgical repair for CSF leak; re-started vemurafenib after a recurrence of the disease (6 weeks after treatment interruption) | PD (7 months after treatment initiation). | CSF leak, pneumocephalus, meningitis (due to tumor shrinkage). |
| Roque et al. [18] 2017 | 47, F | Surgery: PRc (MTA × 1); Ommaya catheter for cyst aspiration; RT (54 Gy in 30 fractions) | Dabrafenib (150 mg PO BID); trametinib (2 mg PO QD) | 7 | N/A | NCR (MRI—near disappearance of the tumor 7 months after treatment). | Initial intermittent fever. |
| Rostami et al. [19] 2017 | 65, M | Surgery: STR (EEA × 1) | Dabrafenib (150 mg BID); trametinib (2 mg QD) after 21 days | 3,5 (15 weeks) | RT | NCR (MRI—91% reduction), clinical improvement. | Drug-induced pyrexia needs treatment interruption. |
| Himes et al. [20] 2018 | 52, M | Surgery: STR (MTA × 1); RT (36 Gy in 12 fractions) | Dabrafenib (150 mg BID → 150 mg QD due to adverse effects → 225 mg QD) | 12 | N/A | SD (12 months off therapy) | Arthralgia |
| Juratli et al. [21] 2019 | 21, M | Surgery (biopsy) | Dabrafenib (150 mg BID), trametinib (2 mg QD) | 6 | N/A | PR (80–90% reduction in the solid and cystic portions within 6 months). | N/A |
| Rao et al. [22] 2019 | 35, M | Bilateral shunts for hydrocephalus STR (MTA × 1) | Dabrafenib (150 mg BID) | 24 | N/A | CR of the solid component (at 24 months). | N/A |
| Bernstein et al. [23] 2019 | 60, M | Surgery: STR × 4 RT | Dabrafenib (150 mg BID); trametinib (2 mg Q.H.S) after 14 days | 28 | N/A | CR at 28 months (100% tumor reduction at 2 months); best clinical response after 3 months. | Prominent and widespread verrucal keratoses 2 weeks after the start of dabrafenib; resolved after discontinuation of dabrafenib and the start of combination therapy. |
| Di Stefano et al. [24] 2020 | 55, F | Surgery: STR (EEA × 1) | Dabrafenib (150 mg PO BID), trametinib (2 mg PO QD) | 6,8 (208 days) | After 4.3 months of treatment, the patient underwent PBRT (52.2 Gy RBE in 29 fractions); dabrafenib and trametinib were discontinued 7 days before starting PBRT. | NCR (95% tumor reduction at 12, 7 months). | Grade 1 fatigue (CTCAE v4.0), coughing, and peripheral edema requiring temporary interruption of trametinib. |
| Khaddour et al. [25] 2020 | 39, M | Surgery: STR (EEA × 1) | Dabrafenib (150 mg PO BID), trametinib (2 mg PO QD); the treatment required interruption for 4 days due to adverse effects before later resuming the previous dosage. | 9 | Fractionated GKRS (Icon system; Elekta) over 5 daily fractions to a total of 25 Gy prescribed to the 50% isodose line; the maximum dose to the optic apparatus was 16 Gy. | In remission for 24 months. | Mild pyrexia (grade I fever according to CTCAE v5.0.). |
| Gopal et al. [26] 2020 | 44, M | Surgery: STR (MTA × 1) | Dabrafenib, trametinib | N/A | N/A | CR (MRI showed a decrease in size). | N/A |
| Butt et al. [27] 2021 | 32, F | Surgery: STR (MTA × 1); SRS; decompressive surgery | Dabrafenib (150 mg PO BID), trametinib (2 mg PO QD) | 3 | N/A | SD | Grade 2 fever; grade 2 rash. |
| Chik et al. [28] 2021 | 37, M | Surgery: STRc (EEA × 4) | Vemurafenib 960 mg BID; intermittent dose reduction after 3.7 months; 1.5-month interruption after 14.7 months. | 40 | STRc (MTA and EEA) RT (54 Gy/30 fractions) GKRS. | PR (MRI, 55% tumor reduction at 15 months); after the interruption, a similar reduction after 0.5 m. | Arthralgia, myalgia, elevated liver enzymes, and photosensitivity. |
| Nussbaum et al. [29] 2022 | 35, M | Surgery: STR (MTA × 1) | Initial dose: dabrafenib (75 mg, BID), trametinib (2 mg QD) Later dose: dabrafenib (250 mg BID) and trametinib (2 mg QD). | 27 | N/A | CR (>95% decrease in size after 21 months of treatment). | Iron deficiency, anemia, elevated values on liver function tests, the etiology of which is unclear. |
| Calvanese et al. [2] 2022 | 40, M | Surgery: NCR (EEA × 1) | Dabrafenib (150 mg BID), trametinib (2 mg QD). | 5 | Fractionated VMAT RT (52.2 Gy/29 fractions). | NCR (90% tumor reduction 12 months after RT). | N/A |
| Calvanese et al. [2] 2022 | 69, M | Biopsy | Dabrafenib 150 mg BID, trametinib 2 mg QD. | 4 | RT (52 Gy/30 fractions). | NCR (90% tumor reduction). | N/A |
| Lin et al. [30] 2023 | 59, M | N/A | Dabrafenib 150 mg BID, trametinib 2 mg QD; discontinued after 10 days due to pyrexia; the patient was continued on dabrafenib. | 6,8 | Dabrafenib 75 mg BID. | SD (after 3 months of follow-up). | Pyrexia increased longstanding palpitations, evaluated with 4-day Holter caused by paroxysmal atrial flutter. Dabrafenib has not been clearly associated with atrial arrhythmias. |
| Brastianos et al. [31] 2023 | 33–83 (16 Pts), M (7 Pts) F (9 Pts) | Cohort A: with/without surgery Cohort B: RT with/without other treatment (except for BRAF or MEK inhibitors). | Vemurafenib (960 mg PO BID) for 28 days in combination with cobimetinib (60 mg PO QD) for 21 days. | N/A | RT (×6 Pts) RT and surgery (×1 Pt) RT and dabrafenib (×1 Pt); off-protocol vemurafenib and cobimetinib (×1 Pt); no treatment (×7 Pts). | CR/PR (average reduction of 83%) in 15 Pts Nonresponse 1 Pt PFS 87% at 12 months and 58% at 24 months OS 100% both at 12 and 24 months. | Twelve patients had grade 3 adverse effects: rash, dehydration, increase in alkaline phosphatase levels, prolongation of corrected QT. Two patients had grade 4 adverse effects: 1 Pt → asymptomatic grade 4 increase in creatine kinase level 1 Pt → grade 4 hyperglicemia. |
| Shah et al. [32] 2023 | 57, F | Surgery: STR (EEA); IMRT (21,6 Gy in 12 fractions); STR; endoscopic transsphenoidal fenestration. | IMRT (37,8 Gy) in conjunction with 1 cycle of dabrafenib and trametinib. | N/A | Decadron (4 mg BID); gradual decadron taper to relieve brain edema. | CR (no evidence of disease recurrence 48 months after treatment). | Grade 2 acute CNS toxicity including marked fatigue and headaches, which responded to steroids; grade 2 excoriations; grade 3 vascular toxicity: diverticulitis complicated with pelvic abscess and pulmonary embolus. |
| Wu et al. [33] 2023 | 63, F | STR (MTA) GKRS (every 12 months) GTR. | Dabrafenib (150 mg BID) and trametinib (2 mg QD). | 3 | After a tumor-free period of 24 months, the disease recurred; the patient restarted combination therapy. | NCR (near 100% reduction size with tiny stable residual tumor) 3 months after treatment. | N/A |
| Wu et al. [33] 2023 | 75, M | STR (EEA) | Dabrafenib (150 mg BID) and trametinib (2 mg QD); the therapy was interrupted due to adverse effects. | 2 | N/A | PR (40% after 3 months). | Hyperglycemia and lower limb edema. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agosti, E.; Zeppieri, M.; Antonietti, S.; Piazza, A.; Ius, T.; Fontanella, M.M.; Fiorindi, A.; Panciani, P.P. Advancing Craniopharyngioma Management: A Systematic Review of Current Targeted Therapies and Future Perspectives. Int. J. Mol. Sci. 2024, 25, 723. https://doi.org/10.3390/ijms25020723
Agosti E, Zeppieri M, Antonietti S, Piazza A, Ius T, Fontanella MM, Fiorindi A, Panciani PP. Advancing Craniopharyngioma Management: A Systematic Review of Current Targeted Therapies and Future Perspectives. International Journal of Molecular Sciences. 2024; 25(2):723. https://doi.org/10.3390/ijms25020723
Chicago/Turabian StyleAgosti, Edoardo, Marco Zeppieri, Sara Antonietti, Amedeo Piazza, Tamara Ius, Marco Maria Fontanella, Alessandro Fiorindi, and Pier Paolo Panciani. 2024. "Advancing Craniopharyngioma Management: A Systematic Review of Current Targeted Therapies and Future Perspectives" International Journal of Molecular Sciences 25, no. 2: 723. https://doi.org/10.3390/ijms25020723
APA StyleAgosti, E., Zeppieri, M., Antonietti, S., Piazza, A., Ius, T., Fontanella, M. M., Fiorindi, A., & Panciani, P. P. (2024). Advancing Craniopharyngioma Management: A Systematic Review of Current Targeted Therapies and Future Perspectives. International Journal of Molecular Sciences, 25(2), 723. https://doi.org/10.3390/ijms25020723