

Transient Changes in Serum CEA, CA19-9, CRP, YKL-40, and IL-6 during Adjuvant Chemotherapy and Survival of Patients with Colorectal Cancer

 , , , ,
, , , ,
Abstract
1. Introduction
2. Results
2.1. Patient Characteristics
2.2. CEA Change Groups
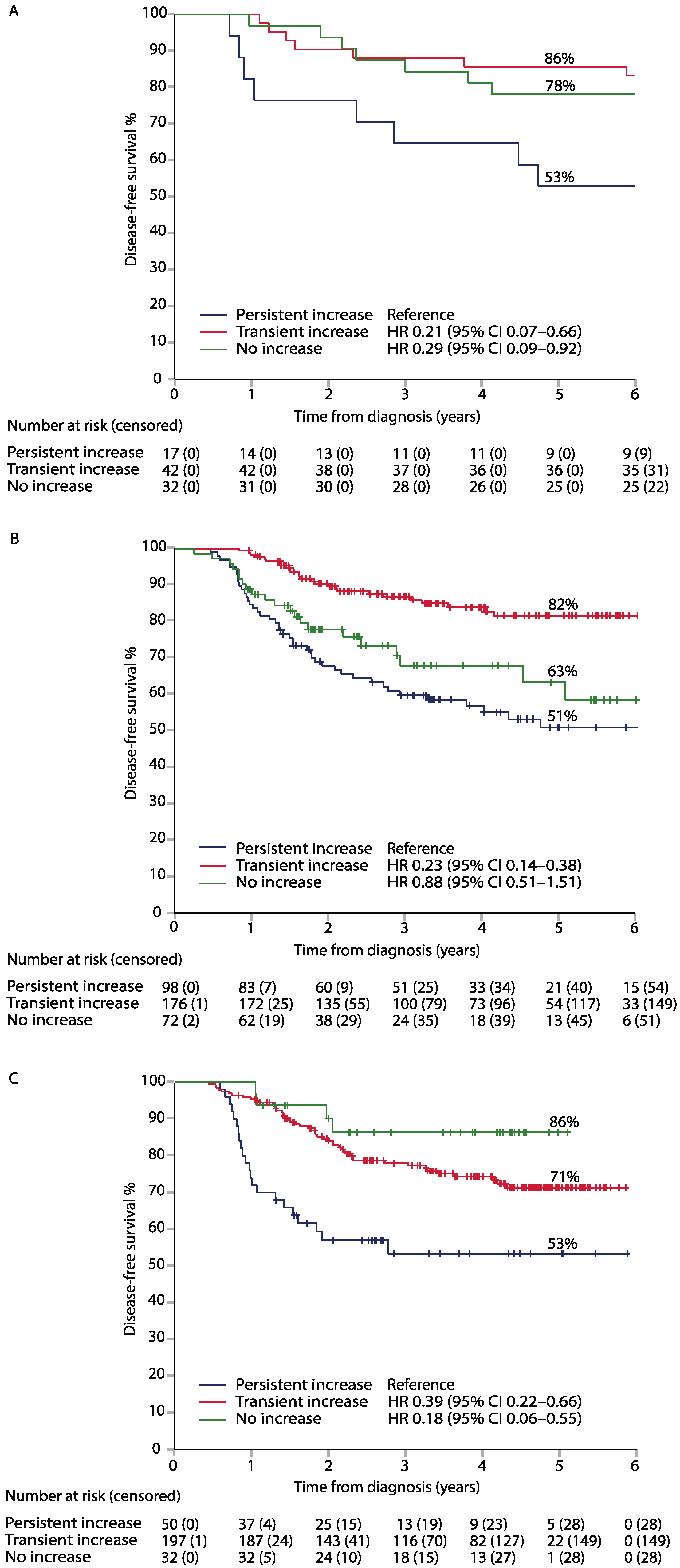
2.3. CEA Change and Survival
2.4. CA19-9, CRP, YKL-40, and IL-6
2.5. Association between Biomarker Kinetic Groups and Adverse Events during Adjuvant Therapy in the LIPSYT Study
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Blood Sampling
4.3. Serum Biomarker Assays
4.4. Biomarker Cut-Offs
4.5. Biomarker Changes with Time
4.6. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Taieb, J.; André, T.; Auclin, E. Refining adjuvant therapy for non-metastatic colon cancer, new standards and perspectives. Cancer Treat. Rev. 2019, 75, 1–11. [Google Scholar] [CrossRef]
- Benson, A.B.; Al-Hawary, M.M.; Azad, N.; Chen, Y.J.; Ciombor, K.K.; Cohen, S. NCCN Guidelines Version 4.2020 Colon Cancer NCCN Evidence Blocks TM Continue NCCN Guidelines Panel Disclosures; NCCN: Plymouth Meeting, PA, USA, 2020. [Google Scholar]
- Argilés, G.; Tabernero, J.; Labianca, R.; Hochhauser, D.; Salazar, R.; Iveson, T.; Laurent-Puig, P.; Quirke, P.; Yoshino, T.; Taieb, J.; et al. Localised colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2020, 31, 1291–1305. [Google Scholar] [CrossRef]
- Hall, C.; Clarke, L.; Pal, A.; Buchwald, P.; Eglinton, T.; Wakeman, C.; Frizelle, F. A Review of the Role of Carcinoembryonic Antigen in Clinical Practice. Ann. Coloproctol. 2019, 35, 294–305. [Google Scholar] [CrossRef]
- Hermunen, K.; Soveri, L.-M.; Boisen, M.K.; Mustonen, H.K.; Dehlendorff, C.; Haglund, C.H.; Johansen, J.S.; Osterlund, P. Postoperative serum CA19-9, YKL-40, CRP and IL-6 in combination with CEA as prognostic markers for recurrence and survival in colorectal cancer. Acta Oncol. 2020, 59, 1416–1423. [Google Scholar] [CrossRef]
- Goldstein, M.J.; Mitchell, E.P. Carcinoembryonic antigen in the staging and follow-up of patients with colorectal cancer. Cancer Investig. 2005, 23, 338–351. [Google Scholar] [CrossRef]
- Nicholson, B.D.; Shinkins, B.; Pathiraja, I.; Roberts, N.W.; James, T.J.; Mallett, S.; Perera, R.; Primrose, J.N.; Mant, D. Blood CEA levels for detecting recurrent colorectal cancer. Cochrane Database Syst. Rev. 2015, 12, CD011134. [Google Scholar] [CrossRef]
- Shinkins, B.; Nicholson, B.D.; Primrose, J.; Perera, R.; James, T.; Pugh, S.; Mant, D. The diagnostic accuracy of a single CEA blood test in detecting colorectal cancer recurrence: Results from the FACS trial. PLoS ONE 2017, 12, e0171810. [Google Scholar] [CrossRef]
- Okamura, R.; Hasegawa, S.; Hida, K.; Hoshino, N.; Kawada, K.; Sugihara, K.; Sakai, Y. Japanese Study Group for Postoperative Follow-up of Colorectal Cancer The role of periodic serum CA19-9 test in surveillance after colorectal cancer surgery. Int. J. Clin. Oncol. 2017, 22, 96–101. [Google Scholar] [CrossRef]
- Barillari, P.; Bolognese, A.; Chirletti, P.; Cardi, M.; Sammartino, P.; Stipa, V. Role of CEA, TPA, and Ca 19-9 in the early detection of localized and diffuse recurrent rectal cancer. Dis. Colon Rectum 1992, 35, 471–476. [Google Scholar] [CrossRef]
- Turano, M.; Delrio, P.; Rega, D.; Cammarota, F.; Polverino, A.; Duraturo, F.; Izzo, P.; De Rosa, M. Promising Colorectal Cancer Biomarkers for Precision Prevention and Therapy. Cancers 2019, 11, 1932. [Google Scholar] [CrossRef]
- Kawamura, Y.J.; Tokumitsu, A.; Mizokami, K.; Sasaki, J.; Tsujinaka, S.; Konishi, F. First Alert for Recurrence During Follow-up After Potentially Curative Resection for Colorectal Carcinoma: CA 19-9 Should Be Included in Surveillance Programs. Clin. Color. Cancer 2010, 9, 48–51. [Google Scholar] [CrossRef] [PubMed]
- Stiksma, J.; Grootendorst, D.C.; van der Linden, P.W.G. CA 19-9 as a marker in addition to CEA to monitor colorectal cancer. Clin. Color. Cancer 2014, 13, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Zhao, T.; Su, Z.; Li, Y.; Zhang, X.; You, Q. Chitinase-3 like-protein-1 function and its role in diseases. Signal Transduct. Target. Ther. 2020, 5, 201. [Google Scholar] [CrossRef] [PubMed]
- Yeo, I.; Lee, C.; Han, S.; Yun, J.; Hong, J. Roles of chitinase 3-like 1 in the development of cancer, neurodegenerative diseases, and inflammatory diseases. Pharmacol. Ther. 2019, 203, 107394. [Google Scholar] [CrossRef]
- Bian, B.; Li, L.; Yang, J.; Liu, Y.; Xie, G.; Zheng, Y.; Zeng, L.; Zeng, J.; Shen, L. Prognostic value of YKL-40 in solid tumors: A meta-analysis of 41 cohort studies. Cancer Cell Int. 2019, 19, 259. [Google Scholar] [CrossRef]
- Cintin, C.; Johansen, J.S.; Christensen, I.J.; Price, P.A.; Sørensen, S.; Nielsen, H.J. Serum YKL-40 and colorectal cancer. Br. J. Cancer 1999, 79, 1494–1499. [Google Scholar] [CrossRef]
- Nasr, R.; Salim Hammoud, M.; Nassar, F.; Mukherji, D.; Shamseddine, A.; Temraz, S. Inflammatory Markers and MicroRNAs: The Backstage Actors Influencing Prognosis in Colorectal Cancer Patients. Int. J. Mol. Sci. 2018, 19, 1867. [Google Scholar] [CrossRef]
- Vainer, N.; Dehlendorff, C.; Johansen, J.S.; Vainer, N.; Dehlendorff, C.; Johansen, J.S. Systematic literature review of IL-6 as a biomarker or treatment target in patients with gastric, bile duct, pancreatic and colorectal cancer. Oncotarget 2018, 9, 29820–29841. [Google Scholar] [CrossRef]
- Thomsen, M.; Kersten, C.; Sorbye, H.; Skovlund, E.; Glimelius, B.; Pfeiffer, P.; Johansen, J.; Kure, E.; Ikdahl, T.; Tveit, K.; et al. Interleukin-6 and C-reactive protein as prognostic biomarkers in metastatic colorectal cancer. Oncotarget 2016, 7, 5013–75022. [Google Scholar] [CrossRef]
- Dienstmann, R.; Salazar, R.; Tabernero, J. Personalizing colon cancer adjuvant therapy: Selecting optimal treatments for individual patients. J. Clin. Oncol. 2015, 33, 1787–1796. [Google Scholar] [CrossRef]
- Dasari, A.; Morris, V.K.; Allegra, C.J.; Atreya, C.; Benson, A.B.; Boland, P.; Chung, K.; Copur, M.S.; Corcoran, R.B.; Deming, D.A.; et al. ctDNA applications and integration in colorectal cancer: An NCI Colon and Rectal-Anal Task Forces whitepaper. Nat. Rev. Clin. Oncol. 2020, 17, 757–770. [Google Scholar] [CrossRef]
- Chakrabarti, S.; Xie, H.; Urrutia, R.; Mahipal, A. The Promise of Circulating Tumor DNA (ctDNA) in the Management of Early-Stage Colon Cancer: A Critical Review. Cancers 2020, 12, 2808. [Google Scholar] [CrossRef] [PubMed]
- Strimpakos, A.S.; Cunningham, D.; Mikropoulos, C.; Petkar, I.; Barbachano, Y.; Chau, I. The impact of carcinoembryonic antigen flare in patients with advanced colorectal cancer receiving first-line chemotherapy. Ann. Oncol. 2010, 21, 1013–1019. [Google Scholar] [CrossRef]
- Yu, P.; Zhou, M.; Qu, J.; Fu, L.; Li, X.; Cai, R.; Jin, B.; Teng, Y.; Liu, J.; Shi, J.; et al. The dynamic monitoring of CEA in response to chemotherapy and prognosis of mCRC patients. BMC Cancer 2018, 18, 1076. [Google Scholar] [CrossRef] [PubMed]
- Colloca, G.A.; Venturino, A.; Guarneri, D. Carcinoembryonic antigen reduction after medical treatment in patients with metastatic colorectal cancer: A systematic review and meta-analysis. Int. J. Color. Dis. 2019, 34, 657–666. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.-C.; Lin, J.-K.; Lin, T.-C.; Chen, W.-S.; Yang, S.-H.; Wang, H.-S.; Lan, Y.-T.; Lin, C.-C.; Jiang, J.-K.; Chang, S.-C. Concordance of Carcinoembryonic Antigen Ratio and Response Evaluation Criteria in Solid Tumors as Prognostic Surrogate Indicators of Metastatic Colorectal Cancer Patients Treated with Chemotherapy. Ann. Surg. Oncol. 2015, 22, 2262–2268. [Google Scholar] [CrossRef]
- Sørbye, H.; Dahl, O. Transient CEA increase at start of oxaliplatin combination therapy for metastatic colorectal cancer. Acta Oncol. 2004, 43, 495–498. [Google Scholar] [CrossRef]
- Yau, T.; Wong, H.; Chan, P.; Chan, T.; Mak, J.; Epstein, R.J. Transient Carcinoembryonic Antigen Elevations During Adjuvant Chemotherapy for Colorectal Cancer Reflect the Burden of Residual Micrometastatic Disease. Clin. Color. Cancer 2010, 9, 108–112. [Google Scholar] [CrossRef]
- Aldulaymi, B.; Christensen, I.J.; Sölétormos, G.; Jess, P.; Nielsen, S.E.; Brünner, N.; Nielsen, H.J. Changes in soluble CEA and TIMP-1 levels during adjuvant chemotherapy for stage III colon cancer. Anticancer Res. 2010, 30, 233–237. [Google Scholar]
- Lawrence, N.; Hinder, V.; Murray, M.; Macapagal, J.; Thompson, P.; Sharples, K.; Findlay, M. Transient elevation in serum carcinoembryonic antigen while on adjuvant chemotherapy for colon cancer: Is this of prognostic importance? Asia. Pac. J. Clin. Oncol. 2017, 13, e124–e131. [Google Scholar] [CrossRef]
- Shinkins, B.; Nicholson, B.D.; James, T.; Pathiraja, I.; Pugh, S.; Perera, R.; Primrose, J.; Mant, D. What carcinoembryonic antigen level should trigger further investigation during colorectal cancer follow-up? A systematic review and secondary analysis of a randomised controlled trial. Health Technol. Assess. 2017, 21, 1–60. [Google Scholar] [CrossRef] [PubMed]
- Moretto, R.; Rossini, D.; Conca, V.; Lonardi, S.; Rasola, C.; Antoniotti, C.; Santini, D.; Marmorino, F.; Tomasello, G.; Borelli, B.; et al. CEA increase as a marker of disease progression after first-line induction therapy in metastatic colorectal cancer patients. A pooled analysis of TRIBE and TRIBE2 studies. Br. J. Cancer 2021, 125, 839–845. [Google Scholar] [CrossRef] [PubMed]
- Duffy, M.J.; Lamerz, R.; Haglund, C.; Nicolini, A.; Kalousová, M.; Holubec, L.; Sturgeon, C. Tumor markers in colorectal cancer, gastric cancer and gastrointestinal stromal cancers: European group on tumor markers 2014 guidelines update. Int. J. Cancer 2014, 134, 2513–2522. [Google Scholar] [CrossRef] [PubMed]
- Locker, G.Y.; Hamilton, S.; Harris, J.; Jessup, J.M.; Kemeny, N.; Macdonald, J.S.; Somerfield, M.R.; Hayes, D.F.; Bast, R.C. ASCO ASCO 2006 update of recommendations for the use of tumor markers in gastrointestinal cancer. J. Clin. Oncol. 2006, 24, 5313–5327. [Google Scholar] [CrossRef]
- Vickers, A.J.; Brewster, S.F. PSA Velocity and Doubling Time in Diagnosis and Prognosis of Prostate Cancer. Br. J. Med. Surg. Urol. 2012, 5, 162–168. [Google Scholar] [CrossRef]
- Ailawadhi, S.; Sunga, A.; Rajput, A.; Yang, G.Y.; Smith, J.; Fakih, M. Chemotherapy-induced carcinoembryonic antigen surge in patients with metastatic colorectal cancer. Oncology 2006, 70, 49–53. [Google Scholar] [CrossRef]
- Li, Y.-H.; An, X.; Xiang, X.-J.; Wang, Z.-Q.; Wang, F.-H.; Feng, F.; Jiang, W.-Q.; He, Y.-J.; Xu, R.-H. Clinical significance of a transient increase in carcinoembryonic antigen and carbohydrate antigen 19-9 in patients with metastatic colorectal cancer receiving chemotherapy. Ai Zheng 2009, 28, 939–944. [Google Scholar] [CrossRef]
- An, X.; Ding, P.-R.; Xiang, X.-J.; Wang, Z.-Q.; Wang, F.-H.; Feng, F.; Jiang, W.-Q.; He, Y.-J.; Xu, R.-H.; Li, Y.-H. Carcinoembryonic antigen surge in metastatic colorectal cancer patients responding to irinotecan combination chemotherapy. Biomarkers 2010, 15, 243–248. [Google Scholar] [CrossRef]
- Ohtsukasa, S.; Okabe, S.; Yamashita, H.; Iwai, T.; Sugihara, K. Increased expression of CEA and MHC class I in colorectal cancer cell lines exposed to chemotherapy drugs. J. Cancer Res. Clin. Oncol. 2003, 129, 719–726. [Google Scholar] [CrossRef]
- Takahashi, N.; Shimada, T.; Ishibashi, Y.; Oyake, N.; Murakami, Y. Transient elevation of serum tumor markers in a patient with hypothyroidism. Am. J. Med. Sci. 2007, 333, 387–389. [Google Scholar] [CrossRef]
- Gardner, R.C.; Feinerman, A.E.; Kantrowitz, P.A.; Gottblatt, S.; Loewenstein, M.S.; Zamcheck, N. Serial carcinoembryonic antigen (CEA) blood levels in patients with ulcerative colitis. Am. J. Dig. Dis. 1978, 23, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Wang, J.; Liu, J.; Huang, S.; Xiong, B. Elevated carcinoembryonic antigen in patients with COVID-19 pneumonia. J. Cancer Res. Clin. Oncol. 2020, 146, 3385–3388. [Google Scholar] [CrossRef] [PubMed]
- Battaloglu, B.; Kaya, E.; Erdil, N.; Nisanoglu, V.; Kosar, F.; Ozgur, B.; Yildirim, B.; Karagoz, H. Does cardiopulmonary bypass alter plasma level of tumor markers? CA 125 and carcinoembryonic antigen. Thorac. Cardiovasc. Surg. 2002, 50, 201–203. [Google Scholar] [CrossRef] [PubMed]
- Polenakovic, M.; Sikole, A.; Dzikova, S.; Polenakovic, B.; Gelev, S. Acquired Renal Cystic Disease and Tumor Markers in Chronic Hemodialysis Patients. Int. J. Artif. Organs 1997, 20, 96–100. [Google Scholar] [CrossRef]
- Yasasever, V.; Dinçer, M.; Camlica, H.; Karaloğlu, D.; Dalay, N. Utility of CA 15-3 and CEA in monitoring breast cancer patients with bone metastases: Special emphasis on "spiking" phenomena. Clin. Biochem. 1997, 30, 53–56. [Google Scholar] [CrossRef]
- Yoshida, M.; Ogino, H.; Iwata, H.; Hattori, Y.; Hashimoto, S.; Nakajima, K.; Sasaki, S.; Hara, M.; Sekido, Y.; Mizoe, J.-E.; et al. Transient increases in serum α fetoprotein and protein induced by vitamin K antagonist II levels following proton therapy does not necessarily indicate progression of hepatocellular carcinoma. Oncol. Lett. 2019, 17, 3026–3034. [Google Scholar] [CrossRef]
- Horwich, A.; Peckham, M.J. Transient tumor marker elevation following chemotherapy for germ cell tumors of the testis. Cancer Treat. Rep. 1986, 70, 1329–1331. [Google Scholar]
- Kim, H.J.; Lee, K.; Kim, Y.J.; Oh, D.; Kim, J.H.; Im, S.; Lee, J.S. Chemotherapy-induced transient CEA and CA19-9 surges in patients with metastatic or recurrent gastric cancer. Acta Oncol. 2009, 48, 385–390. [Google Scholar] [CrossRef]
- Osterlund, P.; Ruotsalainen, T.; Korpela, R.; Saxelin, M.; Ollus, A.; Valta, P.; Kouri, M.; Elomaa, I.; Joensuu, H. Lactobacillus supplementation for diarrhoea related to chemotherapy of colorectal cancer: A randomised study. Br. J. Cancer 2007, 97, 1028–1034. [Google Scholar] [CrossRef]
- Heervä, E.; Väliaho, V.; Salminen, T.; Nieminen, L.; Carpelan, A.; Kurki, S.; Sundström, J.; Huhtinen, H.; Rantala, A.; Carpén, O.; et al. An easily adaptable validated risk score predicts cancer-specific survival in stage II colon cancer. Acta Oncol. 2020, 59, 1503–1507. [Google Scholar] [CrossRef]
- Hermunen, K.; Haglund, C.; Osterlund, P. CEA fluctuation during a single fluorouracil-based chemotherapy cycle for metastatic colorectal cancer. Anticancer Res. 2013, 33, 253–260. [Google Scholar] [PubMed]
- Bojesen, S.E.; Johansen, J.S.; Nordestgaard, B.G. Plasma YKL-40 levels in healthy subjects from the general population. Clin. Chim. Acta. 2011, 412, 709–712. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, L.S.; Christensen, I.J.; Lottenburger, T.; Svendsen, M.N.; Nielsen, H.J.; Nielsen, L.; Hørslev-Petersen, K.; Jensen, J.E.B.; Kollerup, G.; Johansen, J.S. Pre-analytical and biological variability in circulating interleukin 6 in healthy subjects and patients with rheumatoid arthritis. Biomarkers 2008, 13, 59–78. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | LIPSYT Patients | TAUH Patients | TUH Patients |
|---|---|---|---|
| n = 131 | n = 346 | n = 281 | |
| Age, median years (range) | 60 (31–76) | 67 (33–87) | 67 (28–84) |
| Age group, years (%) | |||
| <70 | 116 (89) | 217 (63) | 178 (64) |
| ≥70 | 15 (12) | 129 (37) | 101 (36) |
| Sex | |||
| Male | 70 (53) | 191 (55) | 149 (53) |
| Female | 61 (47) | 155 (45) | 130 (47) |
| Inflammatory disease a | |||
| No | 117 (89) | 329 (95) | 266 (95) |
| Yes | 14 (11) | 17 (5) | 13 (5) |
| Charlson comorbidity index | |||
| 0 | - | 205 (59) | 224 (80) |
| 1 | - | 107 (31) | 38 (80) |
| 2 or more | - | 34 (10) | 17 (6) |
| Smoking | |||
| Never | - | - | 155 (56) |
| Former/current | - | - | 107 (38) |
| Unknown | - | - | 17 (6) |
| Primary location | |||
| Right colon | 38 (29) | 105 (30) | 68 (24) |
| Left colon | 41 (31) | 97 (28) | 70 (25) |
| Rectal | 52 (40) | 144 (42) | 141 (51) |
| TNM stage b | |||
| IIA-B | 38 (29) | 84 (24) | 90 (32) |
| IIIA-C | 82 (63) | 259 (75) | 186 (67) |
| IV | 11 (8) | 3 (1) | 3 (1) |
| Grade | |||
| I-II | - | 251 (72%) | 212 (76) |
| III | - | 95 (28) | 67 (24) |
| Radiotherapy for rectal primary | |||
| No | 7 (13) | 41 (28) | 57 (40) |
| Preoperative 5 × 5 Gy | 8 (15) | 40 (28) | 50 (35) |
| Chemoradiation c | 37 (71) | 63 (44) | 34 (24) |
| Chemotherapy regimen | |||
| 5-FU + LV bolusinj d | 66 (50) | - | - |
| 5-FU + LV continuous inf | 65 (50) | - | - |
| Capecitabine | - | 155 (45) | 120 (43) |
| Capecitabine + oxaliplatin e | - | 190 (55) | 159 (57) |
| Biomarker | All | Transient Increase | No Increase | Persistent Increase |
|---|---|---|---|---|
| LIPSYT study | ||||
| CEA | ||||
| Patients, n (%) | 91 | 42 (46) | 32 (35) | 17 (19) |
| 0 months, Median (range) (µg/L) | 1.3 (0–4.5) | 1.6 (<0.5–3.8) | 1.0 (0–4.5) | 1.4 (<0.5–2.8) |
| 4 months, Median (range) (µg/L) | 2 (<0.5–6.6) | 2.4 (1.0–6.6) | 0.9 (<0.5–4.3) | 2.2 (0.6–4.5) |
| 8 months, Median (range) (µg/L) | 1.6 (<0.5–7.3) | 1.8 (<0.5–4.1) | 1.0 (<0.5–5.8) | 2.6 (0.9–7.3) |
| CA19-9 | ||||
| Patients, n (%) | 50 | 6 (12) | 38 (76) | 6 (12) |
| 0 months, Median (range) (kU/L) | <5 (<5–26) | 7 (<5–16) | <5 (<5–26) | 6 (<5–22) |
| 4 months, Median (range) (kU/L) | <5 (4–36) | 9 (6–27) | <5 (4–20) | 8 (5–34) |
| 8 months, Median (range) (kU/L) | 6 (4–333) | 8 (4–24) | <5 (4–25) | 13 (6–333) |
| CRP | ||||
| Patients, n (%) | 119 | 21 (18) | 95 (80) | 3 (3) |
| 0 months, Median (range)(mg/L) | 4 (4–10) | 4 (4–10) | 4 (4–10) | 4 (4–6) |
| 4 months, Median (range)(mg/L) | 4 (4–70) | 19 (7–70) | 4 (4–8) | 7 (7–10) |
| 8 months, Median (range)(mg/L) | 4 (1–15) | 4 (4–13) | 4 (1–15) | 10 (7–15) |
| YKL-40 | ||||
| Patients, n (%) | 92 | 52 (57) | 33 (36) | 7 (8) |
| 0 months, Median (range) (µg/L) | 49 (20–140) | 47 (20–130) | 46 (20–140) | 55 (38–115) |
| 4 months, Median (range) (µg/L) | 70 (20–267) | 100 (28–267) | 45 (20–110) | 87 (61–125) |
| 8 months, Median (range) (µg/L) | 56 (20–217) | 56 (20–217) | 44 (20–189) | 122 (68–176) |
| IL-6 | ||||
| Patients, n (%) | 97 | 42 (43) | 44 (45) | 11 (11) |
| 0 months, Median (range) (µg/L) | 2.0 (0.4–4.5) | 1.8 (0.4–4.5) | 2.3 (0.9–4.1) | 2.0 (0.8–3.9) |
| 4 months, Median (range) (µg/L) | 2.5 (0.6–24.9) | 3.9 (0.8–24.9) | 1.8 (0.6–3.4) | 2.6 (1.1–6.6) |
| 8 months, Median (range) (µg/L) | 1.7 (0.2–14.0) | 1.7 (0.7–5.7) | 1.7 (0.2–14.0) | 3.1 (1.6–11.3) |
| TAUH cohort | ||||
| CEA | ||||
| Patients, n (%) | 346 | 176 (51) | 72 (21) | 98 (28) |
| 0 months, Median (range) (µg/L) | 1.8 (0.3–5) | 1.8 (0.3–4.9) | 1.8 (0.7–4.9) | 1.8 (0.5–5) |
| 4 months, Median (range) (µg/L) | 2.8 (0.5–245) | 3.3 (0.8–28.2) | 1.8 (0.5–4.7) | 3.0 (0.6–245) |
| 8 months, Median (range) (µg/L) | 2.3 (0.5–655) | 2.2 (0.6–7.9) | 1.8 (0.5–45.3) | 3.2 (0.7–655) |
| CA19-9 | ||||
| Patients, n (%) | 104 | 48 (46) | 30 (29) | 26 (25) |
| 0 months, Median (range) (kU/L) | 7 (<5–24) | 8 (<5–20) | 6 (<5–23) | 8 (<5–24) |
| 4 months, Median (range) (kU/L) | 11 (<5–112) | 12 (6–63) | 5 (<5–24) | 13 (6–122) |
| 8 months, Median (range) (kU/L) | 8 (<5–2748) | 8 (<5–49) | 5 (<5–57) | 14 (6–2748) |
| CRP | ||||
| Patients, n (%) | 283 | 25 (9) | 237 (84) | 21 (7) |
| 0 months, Median (range)(mg/L) | 1 (1–10) | 1 (1–5) | 1 (1–10) | 1 (1–4) |
| 4 months, Median (range)(mg/L) | 1 (1–12) | 3 (1–10) | 1 (1–7) | 3 (1–12) |
| 8 months, Median (range)(mg/L) | 1 (1–255) | 1 (1–6) | 1 (1–255 a) | 6 (1–78) |
| TUH cohort | ||||
| CEA | ||||
| Patients, n (%) | 279 | 197 (71) | 32 (11) | 50 (18) |
| 0 months, Median (range)(µg/L) | 1.6 (0.2–5) | 1.5 (0.2–4.9) | 2.8 (0.9–5) | 1.5 (0.3–4.5) |
| 4 months, Median (range)(µg/L) | 2.9 (0.6–23) | 3.1 (0.9–23) | 2.3 (0.8–5) | 2.8 (0.6–19) |
| 8 months, Median (range)(µg/L) | 2.2 (0.2–38) | 2.0 (0.2–12) | 2.0 (0.4–8.4) | 3.0 (0.6–38) |
| Biomarker | All | Transient Increase | No Increase | Persistent Increase |
|---|---|---|---|---|
| CEA | ||||
| Patients, n (%) | 91 | 42 (46) | 32 (35) | 17 (19) |
| Relapses, n (%) | 20 (22) | 7 (17) | 5 (16) | 8 (47) |
| Non-CRC deaths, n (%) | 9 (10) | 4 (10) | 5 (16) | 0 (0) |
| Deaths (any cause) | 27 (30) | 10 (24) | 9 (28) | 8 (47) |
| 10-year DFS rate | 70% | 79% | 69% | 53% |
| 10-year OS rate | 73% | 81% | 72% | 53% |
| CA19-9 | ||||
| Patients, n (%) | 50 | 6 (12) | 38 (76) | 6 (12) |
| Relapses, n (%) | 23 (46) | 0 (0) | 19 (50) | 4 (67) |
| Non-CRC deaths, n (%) | 7 (14) | 1 (17) | 6 (16) | 0 (0) |
| Deaths (any cause) | 27 (54) | 1 (17) | 22 (58) | 4 (67) |
| 10-year DFS rate | 42% | 83% | 37% | 33% |
| 10-year OS rate | 46% | 83% | 42% | 33% |
| CRP | ||||
| Patients, n (%) | 119 | 21 (18) | 95 (80) | 3 (3) |
| Relapses, n (%) | 44 (37) | 6 (29) | 36 (38) | 2 (67) |
| Non-CRC deaths, n (%) | 11 (9) | 2 (10) | 8 (8) | 1 (33) |
| Deaths (any cause) | 50 (42) | 8 (38) | 39 (41) | 3 (100) |
| 10-year DFS rate | 56% | 62% | 57% | 0% |
| 10-year OS rate | 61% | 62% | 63% | 0% |
| YKL-40 | ||||
| Patients, n (%) | 92 | 52 (57) | 33 (36) | 7 (8) |
| Relapses, n (%) | 35 (28) | 14 (27) | 15 (45) | 6 (86) |
| Non-CRC deaths, n (%) | 8 (9) | 7 (13) | 1 (3) | 0 (0) |
| Deaths (any cause) | 39 (42) | 20 (38) | 14 (42) | 5 (71) |
| 10-year DFS rate | 54% | 62% | 52% | 14% |
| 10-year OS rate | 59% | 62% | 57% | 43% |
| IL-6 | ||||
| Patients, n (%) | 97 | 42 (43) | 44 (45) | 11 (11) |
| Relapses, n (%) | 38 (39) | 15 (36) | 17 (39) | 6 (55) |
| Non-CRC deaths, n (%) | 9 (9) | 4 (10) | 3 (7) | 2 (18) |
| Deaths (any cause) | 44 (45) | 19 (45) | 18 (41) | 7 (64) |
| 10-year DFS rate | 54% | 57% | 57% | 27% |
| 10-year OS rate | 58% | 57% | 64% | 36% |
| Transient Increase | No Increase | Persistent Increase | ||||
|---|---|---|---|---|---|---|
| HR a | 95% CI | HR a | 95% CI | |||
| LIPSYT study | ||||||
| CEA b | DFS | 0.21 | 0.07–0.66 | 0.29 | 0.09–0.92 | Reference |
| OS | 0.24 | 0.08–0.76 | 0.33 | 0.10–1.05 | ||
| CA19-9 c | DFS | 0.13 | 0.01–1.52 | 0.68 | 0.20–2.33 | Reference |
| OS | 0.11 | 0.01–1.22 | 0.67 | 0.20–2.27 | ||
| CRP d | DFS | 0.27 | 0.07–1.08 | 0.33 | 0.09–1.16 | Reference |
| OS | 0.25 | 0.06–1.01 | 0.30 | 0.08–1.06 | ||
| YKL-40 e | DFS | 0.21 | 0.06–0.73 | 0.34 | 0.10–1.12 | Reference |
| OS | 0.25 | 0.07–0.92 | 0.40 | 0.11–1.43 | ||
| IL-6 f | DFS | 0.40 | 0.16–1.02 | 0.40 | 0.16–1.02 | Reference |
| OS | 0.52 | 0.20–1.36 | 0.46 | 0.17–1.19 | ||
| TAUH cohort | ||||||
| CEA g | DFS | 0.23 | 0.14–0.38 | 0.88 | 0.51–1.51 | Reference |
| OS | 0.32 | 0.17–0.61 | 0.64 | 0.30–1.34 | ||
| CA19-9 h | DFS | 0.22 | 0.07–0.67 | 0.39 | 0.21–1.28 | Reference |
| OS | 0.10 | 0.02–0.65 | 0.19 | 0.03–1.18 | ||
| CRP i | DFS | 0.35 | 0.09–1.39 | 0.90 | 0.04–1.99 | Reference |
| OS | 0.70 | 0.12–4.03 | 1.13 | 0.39–3.24 | ||
| TUH cohort | ||||||
| CEA j | DFS | 0.39 | 0.22–0.66 | 0.18 | 0.09–0.92 | Reference |
| OS | 0.14 | 0.06–0.33 | 0.05 | 0.01–0.43 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lehtomäki, K.; Heervä, E.; Kellokumpu-Lehtinen, P.-L.; Mustonen, H.; Salminen, T.; Joensuu, H.; Hermunen, K.; Boisen, M.K.; Johansen, J.S.; Haglund, C.; et al. Transient Changes in Serum CEA, CA19-9, CRP, YKL-40, and IL-6 during Adjuvant Chemotherapy and Survival of Patients with Colorectal Cancer. Int. J. Mol. Sci. 2023, 24, 6753. https://doi.org/10.3390/ijms24076753
Lehtomäki K, Heervä E, Kellokumpu-Lehtinen P-L, Mustonen H, Salminen T, Joensuu H, Hermunen K, Boisen MK, Johansen JS, Haglund C, et al. Transient Changes in Serum CEA, CA19-9, CRP, YKL-40, and IL-6 during Adjuvant Chemotherapy and Survival of Patients with Colorectal Cancer. International Journal of Molecular Sciences. 2023; 24(7):6753. https://doi.org/10.3390/ijms24076753
Chicago/Turabian StyleLehtomäki, Kaisa, Eetu Heervä, Pirkko-Liisa Kellokumpu-Lehtinen, Harri Mustonen, Tapio Salminen, Heikki Joensuu, Kethe Hermunen, Mogens Karsbøl Boisen, Julia Sidenius Johansen, Caj Haglund, and et al. 2023. "Transient Changes in Serum CEA, CA19-9, CRP, YKL-40, and IL-6 during Adjuvant Chemotherapy and Survival of Patients with Colorectal Cancer" International Journal of Molecular Sciences 24, no. 7: 6753. https://doi.org/10.3390/ijms24076753
APA StyleLehtomäki, K., Heervä, E., Kellokumpu-Lehtinen, P.-L., Mustonen, H., Salminen, T., Joensuu, H., Hermunen, K., Boisen, M. K., Johansen, J. S., Haglund, C., & Osterlund, P. (2023). Transient Changes in Serum CEA, CA19-9, CRP, YKL-40, and IL-6 during Adjuvant Chemotherapy and Survival of Patients with Colorectal Cancer. International Journal of Molecular Sciences, 24(7), 6753. https://doi.org/10.3390/ijms24076753