
Extracellular Vesicles: The Future of Diagnosis in Solid Organ Transplantation?

 ,
,  ,
, 

Abstract
1. The Interest of EVs in Solid Organ Transplantation
1.1. The Thriving Field of Solid Organ Transplantation
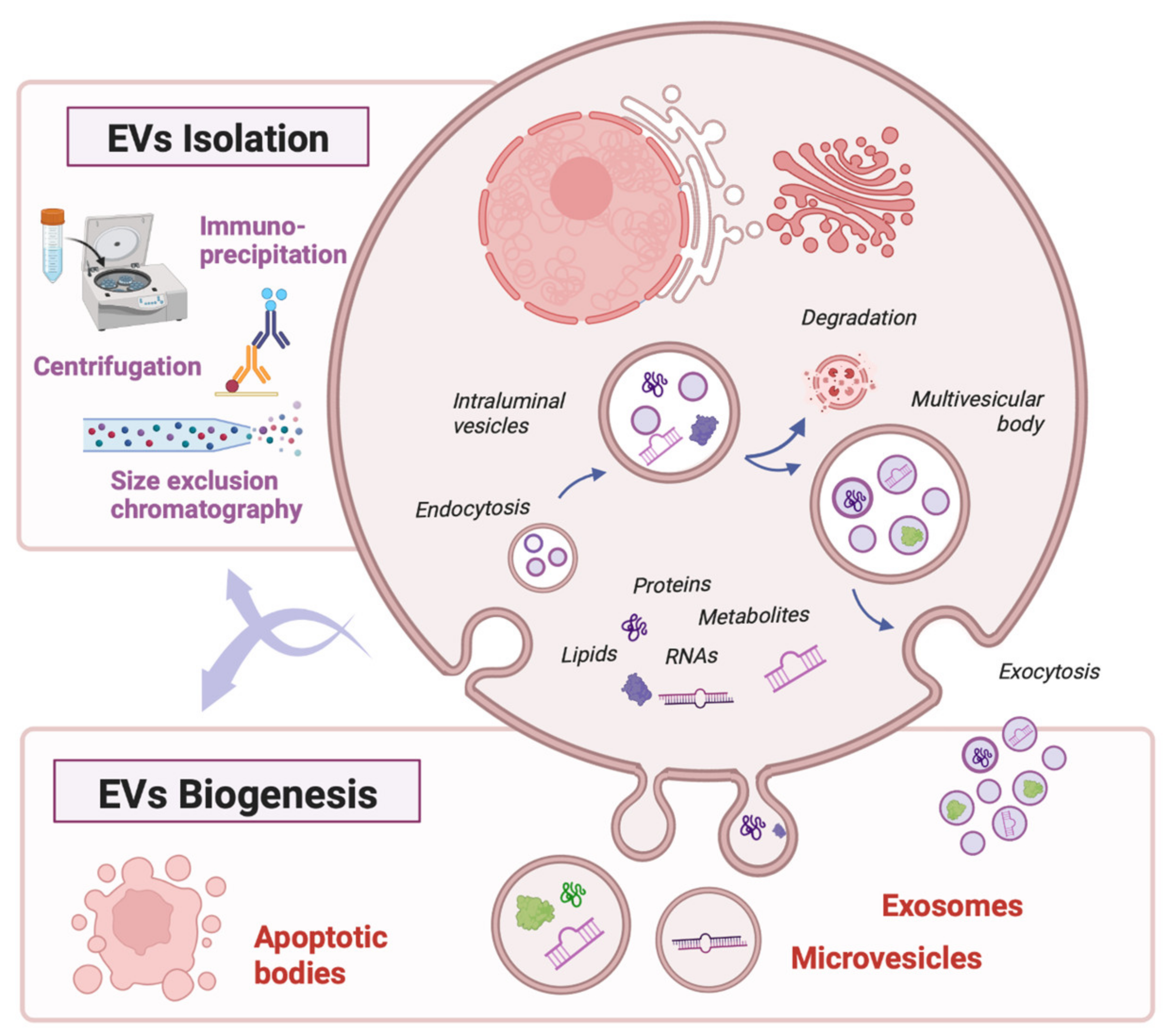
1.2. Intercellular Communication through Extracellular Vesicles
1.3. EVs as Stable, Organ-Specific Biomarkers of Health and Disease
2. EVs as Diagnostic Tools in Solid Organ Transplantation
2.1. Search Strategy
2.2. Preoperative and Postoperative Assessment of Donor Organ Function
2.3. Diagnosis of Graft Rejection
2.4. Diagnosis of Ischemia-Reperfusion Injury
2.5. Diagnosis of Immunosuppressive Drug Toxicity and Graft Infection
3. Opportunities and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barker, C.F.; Markmann, J.F. Historical Overview of Transplantation. Cold Spring Harb. Perspect. Med. 2013, 3, a014977. [Google Scholar] [CrossRef]
- Organización Nacional de Transplantes (ONT) NEWSLETTER. 2020. Available online: http://www.ont.gob.es/publicaciones/Documents/NEWSLETTER%202019_completo%20integrada%20cubierta.pdf (accessed on 3 January 2023).
- Black, C.K.; Termanini, K.M.; Aguirre, O.; Hawksworth, J.S.; Sosin, M. Solid organ transplantation in the 21st century. Ann. Transl. Med. 2018, 6, 409. [Google Scholar] [CrossRef]
- Wong, G.; Howard, K.; Chapman, J.R.; Chadban, S.; Cross, N.; Tong, A.; Webster, A.C.; Craig, J.C. Comparative Survival and Economic Benefits of De-ceased Donor Kidney Transplantation and Dialysis in People with Varying Ages and Co-Morbidities. PLoS ONE 2012, 7, e29591. [Google Scholar]
- Global Observatory on Donation and Transplantation. International Report on Organ Donation and Transplantation Activities: Executive Summary. 2021. Available online: http://www.transplant-observatory.org/wp-content/uploads/2021/06/GODT2019-data_web_updated-June-2021.pdf (accessed on 3 January 2023).
- Rana, A.; Gruessner, A.; Agopian, V.G.; Khalpey, Z.; Riaz, I.B.; Kaplan, B.; Halazun, K.J.; Busuttil, R.W.; Gruessner, R.W.G. Survival Benefit of Solid-Organ Transplant in the United States. JAMA Surg. 2015, 150, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Vanholder, R.; Domínguez-Gil, B.; Busic, M.; Cortez-Pinto, H.; Craig, J.C.; Jager, K.J.; Mahillo, B.; Stel, V.S.; Valentin, M.O.; Zoccali, C.; et al. Organ donation and transplantation: A multi-stakeholder call to action. Nat. Rev. Nephrol. 2021, 17, 554–568. [Google Scholar] [CrossRef]
- Rana, A.; Ackah, R.L.; Webb, G.J.; Halazun, K.J.; Vierling, J.M.; Liu, H.; Wu, M.-F.; Yoeli, D.; Kueht, M.; Mindikoglu, A.L.; et al. No Gains in Long-term Survival After Liver Transplantation Over the Past Three Decades. Ann. Surg. 2019, 269, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Coemans, M.; Süsal, C.; Döhler, B.; Anglicheau, D.; Giral, M.; Bestard, O.; Legendre, C.; Emonds, M.-P.; Kuypers, D.; Molenberghs, G.; et al. Analyses of the short- and long-term graft survival after kidney transplantation in Europe between 1986 and 2015. Kidney Int. 2018, 94, 964–973. [Google Scholar] [CrossRef]
- Lodhi, S.A.; Lamb, K.E.; Meier-Kriesche, H.U. Solid Organ Allograft Survival Improvement in the United States: The Long-Term Does Not Mirror the Dramatic Short-Term Success. Am. J. Transplant. 2011, 11, 1226–1235. [Google Scholar] [CrossRef]
- Joint Statement—EHKA. 2020. Available online: https://ekha.eu/wp-content/uploads/FINAL_14.01.2020_Joint-Statement-of-the-Thematic-Network-on-Organ-Donation-and-Transplantation.pdf (accessed on 3 January 2023).
- Berumen Sánchez, G.; Bunn, K.E.; Pua, H.H.; Rafat, M. Extracellular vesicles: Mediators of intercellular communication in tissue injury and disease. Cell Commun. Signal. 2021, 19, 104. [Google Scholar] [CrossRef]
- Stolp, J.; Zaitsu, M.; Wood, K.J. Immune Tolerance and Rejection in Organ Transplantation. Methods Protoc. 2019, 1899, 159–180. [Google Scholar] [CrossRef]
- Couch, Y.; Buzàs, E.I.; Di Vizio, D.; Gho, Y.S.; Harrison, P.; Hill, A.F.; Lötvall, J.; Raposo, G.; Stahl, P.D.; Théry, C.; et al. A brief history of nearly EV-erything—The rise and rise of extracellular vesicles. J. Extracell. Vesicles 2021, 10, e12144. [Google Scholar] [CrossRef]
- Lo, D.J.; Kaplan, B.; Kirk, A.D. Biomarkers for kidney transplant rejection. Nat. Rev. Nephrol. 2014, 10, 215–225. [Google Scholar] [CrossRef]
- Théry, C.; Witwer, K.W.; Aikawa, E.; Alcaraz, M.J.; Anderson, J.D.; Andriantsitohaina, R.; Antoniou, A.; Arab, T.; Archer, F.; Atkin-Smith, G.K.; et al. Minimal information for studies of extracellular vesicles 2018 (MISEV2018): A position statement of the International Society for Extracellular Vesicles and update of the MISEV2014 guidelines. J. Extracell. Vesicles 2018, 7, 1535750. [Google Scholar] [CrossRef] [PubMed]
- Witwer, K.W.; Théry, C. Extracellular vesicles or exosomes? On primacy, precision, and popularity influencing a choice of no-menclature. J. Extracell. Vesicles 2019, 8, 1648167. [Google Scholar] [CrossRef] [PubMed]
- van Niel, G.; D’Angelo, G.; Raposo, G. Shedding light on the cell biology of extracellular vesicles. Nat. Rev. Mol. Cell Biol. 2018, 19, 213–228. [Google Scholar] [CrossRef]
- Raposo, G.; Stoorvogel, W. Extracellular vesicles: Exosomes, microvesicles, and friends. J. Cell Biol. 2013, 200, 373–383. [Google Scholar] [CrossRef]
- Doyle, L.; Wang, M. Overview of Extracellular Vesicles, Their Origin, Composition, Purpose, and Methods for Exosome Isolation and Analysis. Cells 2019, 8, 727. [Google Scholar] [CrossRef]
- O’Brien, K.; Breyne, K.; Ughetto, S.; Laurent, L.C.; Breakefield, X.O. RNA delivery by extracellular vesicles in mammalian cells and its applications. Nat. Rev. Mol. Cell Biol. 2020, 21, 585–606. [Google Scholar] [CrossRef]
- Benichou, G.; Wang, M.; Ahrens, K.; Madsen, J.C. Extracellular vesicles in allograft rejection and tolerance. Cell. Immunol. 2020, 349, 104063. [Google Scholar] [CrossRef] [PubMed]
- Gasser, O.; Schifferli, J.A. Activated polymorphonuclear neutrophils disseminate anti-inflammatory microparticles by ectocytosis. Blood 2004, 104, 2543–2548. [Google Scholar] [CrossRef]
- Taraboletti, G.; D’Ascenzo, S.; Borsotti, P.; Giavazzi, R.; Pavan, A.; Dolo, V. Shedding of the Matrix Metalloproteinases MMP-2, MMP-9, and MT1-MMP as Membrane Vesicle-Associated Components by Endothelial Cells. Am. J. Pathol. 2002, 160, 673–680. [Google Scholar] [CrossRef] [PubMed]
- Keshtkar, S.; Azarpira, N.; Ghahremani, M.H. Mesenchymal stem cell-derived extracellular vesicles: Novel frontiers in regenerative medicine. Stem Cell Res. Ther. 2018, 9, 63. [Google Scholar] [CrossRef] [PubMed]
- Xia, W.; Xie, J.; Cai, Z.; Liu, X.; Wen, J.; Cui, Z.-K.; Zhao, R.; Zhou, X.; Chen, J.; Mao, X.; et al. Damaged brain accelerates bone healing by releasing small extracellular vesicles that target osteoprogenitors. Nat. Commun. 2021, 12, 6043. [Google Scholar] [CrossRef]
- Hur, Y.H.; Feng, S.; Wilson, K.F.; Cerione, R.A.; Antonyak, M.A. Embryonic Stem Cell-Derived Extracellular Vesicles Maintain ESC Stemness by Activating FAK. Dev. Cell 2021, 56, 277–291.e6. [Google Scholar] [CrossRef] [PubMed]
- Ratajczak, J.; Miękus, K.; Kucia, M.; Zhang, J.; Reca, R.; Dvorak, P.; Ratajczak, M.Z. Embryonic stem cell-derived microvesicles reprogram hematopoietic progenitors: Evidence for horizontal transfer of mRNA and protein delivery. Leukemia 2006, 20, 847–856. [Google Scholar] [CrossRef]
- Todorova, D.; Simoncini, S.; Lacroix, R.; Sabatier, F.; Dignat-George, F. Extracellular Vesicles in Angiogenesis. Circ. Res. 2017, 120, 1658–1673. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.K.; Song, K.S.; Chung, J.H.; Lee, K.R.; Lee, S.N. Platelet microparticles induce angiogenesis in vitro. Br. J. Haematol. 2004, 124, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Davila, M.; Amirkhosravi, A.; Coll, E.; Desai, H.; Robles, L.; Colon, J.; Baker, C.H.; Francis, J.L. Tissue factor-bearing microparticles derived from tumor cells: Impact on coagulation activation. J. Thromb. Haemost. 2008, 6, 1517–1524. [Google Scholar] [CrossRef]
- Raposo, G.; Nijman, H.W.; Stoorvogel, W.; Liejendekker, R.; Harding, C.V.; Melief, C.J.; Geuze, H.J. B lymphocytes secrete antigen-presenting vesicles. J. Exp. Med. 1996, 183, 1161–1172. [Google Scholar] [CrossRef]
- Mallegol, J.; Van Niel, G.; Lebreton, C.; Lepelletier, Y.; Candalh, C.; Dugave, C.; Heath, J.; Raposo, G.; Cerf-Bensussan, N.; Heyman, M. T84-Intestinal Epithelial Exosomes Bear MHC Class II/Peptide Complexes Potentiating Antigen Presentation by Dendritic Cells. Gastroenterology 2007, 132, 1866–1876. [Google Scholar] [CrossRef]
- Morelli, A.E.; Larregina, A.T.; Shufesky, W.J.; Sullivan, M.L.G.; Stolz, D.B.; Papworth, G.D.; Zahorchak, A.F.; Logar, A.J.; Wang, Z.; Watkins, S.C.; et al. Endocytosis, intracellular sorting, and processing of exosomes by dendritic cells. Blood 2004, 104, 3257–3266. [Google Scholar] [CrossRef] [PubMed]
- Hoshino, A.; Costa-Silva, B.; Shen, T.-L.; Rodrigues, G.; Hashimoto, A.; Mark, M.T.; Molina, H.; Kohsaka, S.; Di Giannatale, A.; Ceder, S.; et al. Tumour exosome integrins determine organotropic metastasis. Nature 2015, 527, 329–335. [Google Scholar] [CrossRef]
- Hu, M.; Li, J.; Liu, C.-G.; Goh, R.M.W.J.; Yu, F.; Ma, Z.; Wang, L. Noncoding RNAs of Extracellular Vesicles in Tumor Angiogenesis: From Biological Functions to Clinical Significance. Cells 2022, 11, 947. [Google Scholar] [CrossRef]
- Gabrielli, M.; Prada, I.; Joshi, P.; Falcicchia, C.; D’Arrigo, G.; Rutigliano, G.; Battocchio, E.; Zenatelli, R.; Tozzi, F.; Radeghieri, A.; et al. Microglial large extracellular vesicles propagate early synaptic dysfunction in Alzheimer’s disease. Brain 2022, 145, 2849–2868. [Google Scholar] [CrossRef]
- Peng, M.; Sun, R.; Hong, Y.; Wang, J.; Xie, Y.; Zhang, X.; Li, J.; Guo, H.; Xu, P.; Li, Y.; et al. Extracellular vesicles carrying proinflammatory factors may spread atherosclerosis to remote locations. Cell. Mol. Life Sci. 2022, 79, 430. [Google Scholar] [CrossRef] [PubMed]
- Mack, M.; Kleinschmidt, A.; Brühl, H.; Klier, C.; Nelson, P.J.; Cihak, J.; Plachý, J.; Stangassinger, M.; Erfle, V.; Schlöndorff, D. Transfer of the chemokine receptor CCR5 between cells by membrane-derived microparticles: A mechanism for cellular human immunodeficiency virus 1 infection. Nat. Med. 2000, 6, 769–775. [Google Scholar] [CrossRef]
- Cheng, L.; Hill, A.F. Therapeutically harnessing extracellular vesicles. Nat. Rev. Drug Discov. 2022, 21, 379–399. [Google Scholar] [CrossRef] [PubMed]
- Karpman, D.; Ståhl, A.-L.; Arvidsson, I. Extracellular vesicles in renal disease. Nat. Rev. Nephrol. 2017, 13, 545–562. [Google Scholar] [CrossRef]
- Zhou, H.; Pisitkun, T.; Aponte, A.; Yuen, P.; Hoffert, J.; Yasuda, H.; Hu, X.; Chawla, L.; Shen, R.-F.; Knepper, M.; et al. Exosomal Fetuin-A identified by proteomics: A novel urinary biomarker for detecting acute kidney injury. Kidney Int. 2006, 70, 1847–1857. [Google Scholar] [CrossRef]
- Zubiri, I.; Posada-Ayala, M.; Benito-Martin, A.; Maroto, A.S.; Martin-Lorenzo, M.; Cannata-Ortiz, P.; de la Cuesta, F.; Gonzalez-Calero, L.; Barderas, M.G.; Fernandez-Fernandez, B.; et al. Kidney tissue proteomics reveals regucalcin downregulation in response to diabetic nephropathy with reflection in urinary exosomes. Transl. Res. 2015, 166, 474–484.e4. [Google Scholar] [CrossRef]
- Duan, Z.-Y.; Cai, G.-Y.; Bu, R.; Lu, Y.; Hou, K.; Chen, X.-M. Selection of urinary sediment miRNAs as specific biomarkers of IgA nephropathy. Sci. Rep. 2016, 6, 23498. [Google Scholar] [CrossRef]
- Oh, J.G.; Lee, P.; Gordon, R.E.; Sahoo, S.; Kho, C.; Jeong, D. Analysis of extracellular vesicle miRNA profiles in heart failure. J. Cell. Mol. Med. 2020, 24, 7214–7227. [Google Scholar] [CrossRef]
- Zhang, Y.-N.; Vernooij, F.; Ibrahim, I.; Ooi, S.; Gijsberts, C.M.; Schoneveld, A.H.; Sen, K.W.; Den Ruijter, H.M.; Timmers, L.; Richards, A.M.; et al. Extracellular Vesicle Proteins Associated with Systemic Vascular Events Correlate with Heart Failure: An Observational Study in a Dyspnoea Cohort. PLoS ONE 2016, 11, e0148073. [Google Scholar] [CrossRef]
- Cuppoletti, A.; Roig, E.; Perez-Villa, F.; Marin, J.L.; Orús, J.; Vallejos, I.; Rivera, A.; Botta, C. Value of NT-proBNP Determinations in the Follow-Up of Heart Transplantation. Transplant. Proc. 2005, 37, 4033–4035. [Google Scholar] [CrossRef] [PubMed]
- Talha, S.; Charloux, A.; Piquard, F.; Geny, B. Brain natriuretic peptide and right heart dysfunction after heart transplantation. Clin. Transplant. 2017, 31, e12969. [Google Scholar] [CrossRef] [PubMed]
- Romero-García, N.; Huete-Acevedo, J.; Mas-Bargues, C.; Sanz-Ros, J.; Dromant, M.; Borrás, C. The Double-Edged Role of Extracellular Vesicles in the Hallmarks of Aging. Biomolecules 2023, 13, 165. [Google Scholar] [CrossRef]
- Ashcroft, J.; Leighton, P.; Elliott, T.R.; Hosgood, S.A.; Nicholson, M.L.; Kosmoliaptsis, V. Extracellular vesicles in kidney transplantation: A state-of-the-art review. Kidney Int. 2022, 101, 485–497. [Google Scholar] [CrossRef]
- Grange, C.; Bellucci, L.; Bussolati, B.; Ranghino, A. Potential Applications of Extracellular Vesicles in Solid Organ Transplantation. Cells 2020, 9, 369. [Google Scholar] [CrossRef] [PubMed]
- Mas-Bargues, C.; Borrás, C. Importance of stem cell culture conditions for their derived extracellular vesicles therapeutic effect. Free. Radic. Biol. Med. 2021, 168, 16–24. [Google Scholar] [CrossRef]
- Romero-García, N.; Mas-Bargues, C.; Huete-Acevedo, J.; Borrás, C. Extracellular Vesicles and Cellular Ageing; Springer International Publishing: Cham, Switzerland, 2023; pp. 271–311. [Google Scholar] [CrossRef]
- Sailliet, N.; Ullah, M.; Dupuy, A.; Silva, A.K.A.; Gazeau, F.; Le Mai, H.; Brouard, S. Extracellular Vesicles in Transplantation. Front. Immunol. 2022, 13, 179. [Google Scholar] [CrossRef]
- Mastoridis, S.; Londoño, M.C.; Kurt, A.; Kodela, E.; Crespo, E.; Mason, J.; Bestard, O.; Martínez-Llordella, M.; Sánchez-Fueyo, A. Impact of donor extracellular vesicle release on recipient cell “cross-dressing” following clinical liver and kidney transplantation. Am. J. Transplant. 2021, 21, 2387–2398. [Google Scholar] [CrossRef] [PubMed]
- Garg, N.; Poggio, E.D.; Mandelbrot, D. The Evaluation of Kidney Function in Living Kidney Donor Candidates. Kidney360 2021, 2, 1523–1530. [Google Scholar] [CrossRef] [PubMed]
- Mannon, R.B. Delayed Graft Function: The AKI of Kidney Transplantation. Nephron 2018, 140, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Turco, A.E.; Lam, W.; Rule, A.D.; Denic, A.; Lieske, J.C.; Miller, V.M.; Larson, J.J.; Kremers, W.K.; Jayachandran, M. Specific renal parenchymal-derived urinary extracellular vesicles identify age-associated structural changes in living donor kidneys. J. Extracell. Vesicles 2016, 5, 29642. [Google Scholar] [CrossRef] [PubMed]
- Lozano-Ramos, S.I.; Bancu, I.; Carreras-Planella, L.; Monguió-Tortajada, M.; Cañas, L.; Juega, J.; Bonet, J.; Armengol, M.P.; Lauzurica, R.; Borràs, F.E. Molecular profile of urine ex-tracellular vesicles from normo-functional kidneys reveal minimal differences between living and deceased donors. BMC Nephrol. 2018, 19, 189. [Google Scholar] [CrossRef] [PubMed]
- Gremmels, H.; de Jong, O.G.; Toorop, R.J.; Michielsen, L.; van Zuilen, A.D.; Vlassov, A.V.; Verhaar, M.C.; van Balkom, B.W. The Small RNA Repertoire of Small Extracellular Vesicles Isolated From Donor Kidney Preservation Fluid Provides a Source for Biomarker Discovery for Organ Quality and Posttransplantation Graft Function. Transplant. Direct. 2019, 5, e484. [Google Scholar] [CrossRef]
- Siedlecki, A.; Irish, W.; Brennan, D.C. Delayed Graft Function in the Kidney Transplant. Am. J. Transplant. 2011, 11, 2279–2296. [Google Scholar] [CrossRef]
- Dimuccio, V.; Ranghino, A.; Barbato, L.P.; Fop, F.; Biancone, L.; Camussi, G.; Bussolati, B. Urinary CD133+ Extracellular Vesicles Are Decreased in Kidney Transplanted Patients with Slow Graft Function and Vascular Damage. PLoS ONE 2014, 9, e104490. [Google Scholar] [CrossRef]
- Alvarez, S.; Suazo, C.; Boltansky, A.; Ursu, M.; Carvajal, D.; Innocenti, G.; Vukusich, A.; Hurtado, M.; Villanueva, S.; Carreño, J.; et al. Urinary Exosomes as a Source of Kidney Dysfunction Biomarker in Renal Transplantation. Transplant. Proc. 2013, 45, 3719–3723. [Google Scholar] [CrossRef] [PubMed]
- Peake, P.W.; Pianta, T.J.; Succar, L.; Fernando, M.; Pugh, D.J.; McNamara, K.; Endre, Z.H. A Comparison of the Ability of Levels of Urinary Biomarker Proteins and Exosomal mRNA to Predict Outcomes after Renal Transplantation. PLoS ONE 2014, 9, e98644. [Google Scholar] [CrossRef]
- Wang, J.; Li, X.; Wu, X.; Wang, Z.; Zhang, C.; Cao, G.; Yan, T. Expression Profiling of Exosomal miRNAs Derived from the Peripheral Blood of Kidney Recipients with DGF Using High-Throughput Sequencing. BioMed Res. Int. 2019, 2019, 1759697. [Google Scholar] [CrossRef] [PubMed]
- Al-Nedawi, K.; Haas-Neill, S.; Gangji, A.; Ribic, C.M.; Kapoor, A.; Margetts, P. Circulating microvesicle protein is associated with renal transplant outcome. Transpl. Immunol. 2019, 55, 101210. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Han, X.; Sun, Y.; He, X.; Xue, D. A circulating exosomal microRNA panel as a novel biomarker for monitoring post-transplant renal graft function. J. Cell. Mol. Med. 2020, 24, 12154–12163. [Google Scholar] [CrossRef] [PubMed]
- Matignon, M.; Ding, R.; Dadhania, D.M.; Mueller, F.B.; Hartono, C.; Snopkowski, C.; Li, C.; Lee, J.R.; Sjoberg, D.; Seshan, S.V.; et al. Urinary Cell mRNA Profiles and Differential Diagnosis of Acute Kidney Graft Dysfunction. J. Am. Soc. Nephrol. 2014, 25, 1586–1597. [Google Scholar] [CrossRef]
- Nankivell, B.J.; Alexander, S.I. Rejection of the Kidney Allograft. N. Engl. J. Med. 2010, 363, 1451–1462. [Google Scholar] [CrossRef]
- Potena, L.; Zuckermann, A.; Barberini, F.; Aliabadi-Zuckermann, A. Complications of Cardiac Transplantation. Curr. Cardiol. Rep. 2018, 20, 73. [Google Scholar] [CrossRef]
- Ronca, V.; Wootton, G.; Milani, C.; Cain, O. The Immunological Basis of Liver Allograft Rejection. Front. Immunol. 2020, 11, 2155. [Google Scholar] [CrossRef]
- Denton, M.D.; Magee, C.C.; Sayegh, M.H. Immunosuppressive strategies in transplantation. Lancet 1999, 353, 1083–1091. [Google Scholar] [CrossRef]
- Plattner, B.W.; Chen, P.; Cross, R.; Leavitt, M.A.; Killen, P.D.; Heung, M. Complications and adequacy of transplant kidney biopsies: A comparison of techniques. J. Vasc. Access 2018, 19, 291–296. [Google Scholar] [CrossRef]
- Vantyghem, M.-C.; Kerr-Conte, J.; Arnalsteen, L.; Sergent, G.; Defrance, F.; Gmyr, V.; Declerck, N.; Raverdy, V.; Vandewalle, B.; Pigny, P.; et al. Primary Graft Function, Metabolic Control, and Graft Survival After Islet Transplantation. Diabetes Care 2009, 32, 1473–1478. [Google Scholar] [CrossRef]
- Betjes, M.G.H.; Roelen, D.L.; van Agteren, M.; Gestel, J.K.-V. Causes of Kidney Graft Failure in a Cohort of Recipients With a Very Long-Time Follow-Up After Transplantation. Front. Med. 2022, 9, 842419. [Google Scholar] [CrossRef] [PubMed]
- Serón, D.; Moreso, F.; Fulladosa, X.; Hueso, M.; Carrera, M.; Grinyó, J.M. Reliability of chronic allograft nephropathy diagnosis in sequential protocol biopsies. Kidney Int. 2002, 61, 727–733. [Google Scholar] [CrossRef]
- Kim, M.J.; Lim, S.J.; Ko, Y.; Kwon, H.E.; Jung, J.H.; Kwon, H.; Go, H.; Park, Y.; Kim, T.-K.; Jung, M.; et al. Urinary Exosomal Cystatin C and Lipopolysaccharide Binding Protein as Biomarkers for Antibody−Mediated Rejection after Kidney Transplantation. Biomedicines 2022, 10, 2346. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.-H.; Lee, C.-H.; Kim, K.Y.; Jung, H.-Y.; Choi, J.-Y.; Cho, J.-H.; Park, S.-H.; Kim, Y.-L.; Baek, M.-C.; Park, J.B.; et al. Novel urinary exosomal biomarkers of acute T cell-mediated rejection in kidney transplant recipients: A cross-sectional study. PLoS ONE 2018, 13, e0204204. [Google Scholar] [CrossRef]
- Sigdel, T.K.; Ng, Y.W.; Elee, S.; Nicora, C.D.; Qian, W.-J.; Smith, R.D.; Camp, D.G.; Sarwal, M.M. Perturbations in the Urinary Exosome in Transplant Rejection. Front. Med. 2015, 1, 57. [Google Scholar] [CrossRef]
- El Fekih, R.; Hurley, J.; Tadigotla, V.; Alghamdi, A.; Srivastava, A.; Coticchia, C.; Choi, J.; Allos, H.; Yatim, K.; Alhaddad, J.; et al. Faculty Opinions recommendation of Discovery and Validation of a Urinary Exosome mRNA Signature for the Diagnosis of Human Kidney Transplant Rejection. J. Am. Soc. Nephrol. 2021, 32, 994–1004. [Google Scholar] [CrossRef]
- Park, J.; Lin, H.-Y.; Assaker, J.P.; Jeong, S.; Huang, C.-H.; Kurdi, A.; Lee, K.; Fraser, K.; Min, C.; Eskandari, S.; et al. Integrated Kidney Exosome Analysis for the Detection of Kidney Transplant Rejection. ACS Nano 2017, 11, 11041–11046. [Google Scholar] [CrossRef] [PubMed]
- Tower, C.M.; Reyes, M.; Nelson, K.; Leca, N.; Kieran, N.; Muczynski, K.; Jefferson, J.A.; Blosser, C.; Kukla, A.; Maurer, D.; et al. Plasma C4d+ Endothelial Microvesicles Increase in Acute Antibody-Mediated Rejection. Transplantation 2017, 101, 2235–2243. [Google Scholar] [CrossRef]
- Zhang, H.; Huang, E.; Kahwaji, J.; Nast, C.C.; Li, P.; Mirocha, J.; Thomas, D.L.; Ge, S.; Vo, A.A.; Jordan, S.C.; et al. Plasma Exosomes From HLA-Sensitized Kidney Transplant Recipients Contain mRNA Transcripts Which Predict Development of Antibody-Mediated Rejection. Transplantation 2017, 101, 2419–2428. [Google Scholar] [CrossRef] [PubMed]
- Takada, Y.; Kamimura, D.; Jiang, J.-J.; Higuchi, H.; Iwami, D.; Hotta, K.; Tanaka, Y.; Ota, M.; Higuchi, M.; Nishio, S.; et al. Increased urinary exosomal SYT17 levels in chronic active antibody-mediated rejection after kidney transplantation via the IL-6 amplifier. Int. Immunol. 2020, 32, 653–662. [Google Scholar] [CrossRef]
- Jung, H.-Y.; Lee, C.-H.; Choi, J.-Y.; Cho, J.-H.; Park, S.-H.; Kim, Y.-L.; Moon, P.-G.; Baek, M.-C.; Park, J.B.; Kim, Y.H.; et al. Potential urinary extracellular vesicle protein biomarkers of chronic active antibody-mediated rejection in kidney transplant recipients. J. Chromatogr. B 2020, 1138, 121958. [Google Scholar] [CrossRef]
- Yang, J.; Bi, L.; He, X.; Wang, Z.; Qian, Y.; Xiao, L.; Shi, B. Follicular Helper T Cell Derived Exosomes Promote B Cell Proliferation and Differentiation in Antibody-Mediated Rejection after Renal Transplantation. BioMed Res. Int. 2019, 2019, 6387924. [Google Scholar] [CrossRef] [PubMed]
- Zhang, A.B.; Peng, Y.F.; Jia, J.J.; Nie, Y.; Zhang, S.Y.; Xie, H.Y.; Zhou, L.; Zheng, S.S. Exosome-derived galectin-9 may be a novel predictor of rejection and prognosis after liver transplantation. J. Zhejiang Univ.-Sci. B 2019, 20, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Woud, W.W.; Hesselink, D.A.; Hoogduijn, M.J.; Baan, C.C.; Boer, K. Direct detection of circulating donor-derived extracellular vesicles in kidney transplant recipients. Sci. Rep. 2022, 12, 21973. [Google Scholar] [CrossRef] [PubMed]
- Vallabhajosyula, P.; Korutla, L.; Habertheuer, A.; Yu, M.; Rostami, S.; Yuan, C.X.; Reddy, S.; Liu, C.; Korutla, V.; Koeberlein, B.; et al. Tissue-specific exosome biomarkers for non-invasively monitoring immunologic rejection of transplanted tissue. J. Clin. Investig. 2017, 127, 1375–1391. [Google Scholar] [CrossRef]
- Lund, L.H.; Khush, K.K.; Cherikh, W.S.; Goldfarb, S.; Kucheryavaya, A.Y.; Levvey, B.J.; Meiser, B.; Rossano, J.W.; Chambers, D.C.; Yusen, R.D.; et al. The Registry of the International Society for Heart and Lung Transplantation: Thirty-fourth Adult Heart Transplantation Report-2017; Focus Theme: Allograft ischemic time. J. Heart Lung Transplant. Off. Publ. Int. Soc. Heart Transplant. 2017, 36, 1037–1046. [Google Scholar] [CrossRef]
- Nguyen, V.; Cantarovich, M.; Cecere, R.; Giannetti, N. Tricuspid Regurgitation After Cardiac Transplantation: How Many Biopsies Are Too Many? J. Heart Lung Transplant. 2005, 24, S227–S231. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, V.; Mansueto, G.; Coscioni, E.; Maiello, C.; Benincasa, G.; Napoli, C. Novel biomarkers useful in surveillance of graft rejection after heart transplantation. Transpl. Immunol. 2021, 67, 101406. [Google Scholar] [CrossRef] [PubMed]
- Habertheuer, A.; Korutla, L.; Rostami, S.; Reddy, S.; Lal, P.; Naji, A.; Vallabhajosyula, P. Donor tissue-specific exosome profiling enables noninvasive monitoring of acute rejection in mouse allogeneic heart transplantation. J. Thorac. Cardiovasc. Surg. 2018, 155, 2479–2489. [Google Scholar] [CrossRef] [PubMed]
- Castellani, C.; Burrello, J.; Fedrigo, M.; Burrello, A.; Bolis, S.; Di Silvestre, D.; Tona, F.; Bottio, T.; Biemmi, V.; Toscano, G.; et al. Circulating extracellular vesicles as non-invasive biomarker of rejection in heart transplant. J. Heart Lung Transplant. 2020, 39, 1136–1148. [Google Scholar] [CrossRef] [PubMed]
- Kennel, P.J.; Saha, A.; Maldonado, D.A.; Givens, R.; Brunjes, D.L.; Castillero, E.; Zhang, X.; Ji, R.; Yahi, A.; George, I.; et al. Serum exosomal protein profiling for the non-invasive detection of cardiac allograft rejection. J. Heart Lung Transplant. 2018, 37, 409–417. [Google Scholar] [CrossRef] [PubMed]
- Glanville, A.R.; Benden, C.; Bergeron, A.; Cheng, G.-S.; Gottlieb, J.; Lease, E.D.; Perch, M.; Todd, J.L.; Williams, K.M.; Verleden, G.M. Bronchiolitis obliterans syndrome after lung or haematopoietic stem cell transplantation: Current management and future directions. ERJ Open Res. 2022, 8, 00185-2022. [Google Scholar] [CrossRef]
- Al-Githmi, I.; Batawil, N.; Shigemura, N.; Hsin, M.; Lee, T.W.; He, G.-W.; Yim, A. Bronchiolitis obliterans following lung transplantation. Eur. J. Cardio-Thoracic Surg. 2006, 30, 846–851. [Google Scholar] [CrossRef] [PubMed]
- Glanville, A.R. The Role of Surveillance Bronchoscopy Post-Lung Transplantation. Semin. Respir. Crit. Care Med. 2013, 34, 414–420. [Google Scholar] [CrossRef]
- Gregson, A.L.; Hoji, A.; Injean, P.; Poynter, S.T.; Briones, C.; Palchevskiy, V.; Weigt, S.S.; Shino, M.Y.; Derhovanessian, A.; Sayah, D.; et al. Altered Exosomal RNA Profiles in Bronchoalveolar Lavage from Lung Transplants with Acute Rejection. Am. J. Respir. Crit. Care Med. 2015, 192, 1490–1503. [Google Scholar] [CrossRef] [PubMed]
- Gunasekaran, M.; Xu, Z.; Nayak, D.K.; Sharma, M.; Hachem, R.; Walia, R.; Bremner, R.M.; Smith, M.A.; Mohanakumar, T. Donor-Derived Exosomes With Lung Self-Antigens in Human Lung Allograft Rejection. Am. J. Transplant. 2017, 17, 474–484. [Google Scholar] [CrossRef]
- Marino, J.; Babiker-Mohamed, M.H.; Crosby-Bertorini, P.; Paster, J.T.; LeGuern, C.; Germana, S.; Abdi, R.; Uehara, M.; Kim, J.I.; Markmann, J.F.; et al. Donor exosomes rather than passenger leukocytes initiate alloreactive T cell responses after transplantation. Sci. Immunol. 2016, 1, aaf8759. [Google Scholar] [CrossRef]
- Becker, P.D.; Ratnasothy, K.; Sen, M.; Peng, Q.; Romano, M.; Bazoer, J.; Suvitra, E.; Stout, A.; Hylton, S.G.; Dorling, A.; et al. B lymphocytes contribute to indirect pathway T cell sensitization via acquisition of extracellular vesicles. Am. J. Transplant. 2020, 21, 1415–1426. [Google Scholar] [CrossRef]
- Eltzschig, H.K.; Eckle, T. Ischemia and reperfusion—From mechanism to translation. Nat. Med. 2011, 17, 1391–1401. [Google Scholar] [CrossRef]
- Sonoda, H.; Yokota-Ikeda, N.; Oshikawa, S.; Kanno, Y.; Yoshinaga, K.; Uchida, K.; Ueda, Y.; Kimiya, K.; Uezono, S.; Ueda, A.; et al. Decreased abundance of urinary exosomal aquaporin-1 in renal ischemia-reperfusion injury. Am. J. Physiol. Physiol. 2009, 297, F1006–F1016. [Google Scholar] [CrossRef]
- Oshikawa-Hori, S.; Yokota-Ikeda, N.; Sonoda, H.; Ikeda, M. Urinary extracellular vesicular release of aquaporins in patients with renal transplantation. BMC Nephrol. 2019, 20, 216. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.-L.; Lv, L.-L.; Tang, T.-T.; Wang, B.; Feng, Y.; Zhou, L.-T.; Cao, J.-Y.; Tang, R.-N.; Wu, M.; Liu, H.; et al. HIF-1α inducing exosomal microRNA-23a expression mediates the cross-talk between tubular epithelial cells and macrophages in tubulointerstitial inflammation. Kidney Int. 2019, 95, 388–404. [Google Scholar] [CrossRef]
- Ding, C.; Zheng, J.; Wang, B.; Li, Y.; Xiang, H.; Dou, M.; Qiao, Y.; Tian, P.; Ding, X.; Xue, W. Exosomal MicroRNA-374b-5p From Tubular Epithelial Cells Promoted M1 Macrophages Activation and Worsened Renal Ischemia/Reperfusion Injury. Front. Cell Dev. Biol. 2020, 8, 587693. [Google Scholar] [CrossRef] [PubMed]
- Azzi, J.R.; Sayegh, M.H.; Mallat, S.G. Calcineurin Inhibitors: 40 Years Later, Can’t Live Without. J. Immunol. 2013, 191, 5785–5791. [Google Scholar] [CrossRef] [PubMed]
- Carreras-Planella, L.; Juega, J.; Taco, O.; Cañas, L.; Franquesa, M.; Lauzurica, R.; Borràs, F.E. Proteomic Characterization of Urinary Ex-tracellular Vesicles from Kidney-Transplanted Patients Treated with Calcineurin Inhibitors. Int. J. Mol. Sci. 2020, 21, 7569. [Google Scholar] [CrossRef] [PubMed]
- Costa de Freitas, R.C.; Bortolin, R.H.; Vecchia Genvigir, F.D.; Bonezi, V.; Crespo Hirata, T.D.; Felipe, C.R.; Tedesco-Silva, H., Jr.; Medina-Pestana, J.O.; Cerda, A.; Doi, S.Q.; et al. Differentially expressed urinary exo-miRs and clinical outcomes in kidney recipients on short-term tacrolimus therapy: A pilot study. Epigenomics 2020, 12, 2019–2034. [Google Scholar] [CrossRef]
- Lucafò, M.; De Biasi, S.; Curci, D.; Norbedo, A.; Stocco, G.; Decorti, G. Extracellular Vesicles as Innovative Tools for AssessingAdverse Effects of Immunosuppressant Drugs. Curr. Med. Chem. 2022, 29, 3586–3600. [Google Scholar] [CrossRef]
- Karuthu, S.; Blumberg, E.A. Common Infections in Kidney Transplant Recipients. Clin. J. Am. Soc. Nephrol. 2012, 7, 2058–2070. [Google Scholar] [CrossRef]
- Buehrig, C.K.; Lager, D.J.; Stegall, M.D.; Kreps, M.A.; Kremers, W.K.; Gloor, J.M.; Schwab, T.R.; Velosa, J.A.; Fidler, M.E.; Larson, T.S.; et al. Influence of surveillance renal allograft biopsy on diagnosis and prognosis of polyomavirus-associated nephropathy. Kidney Int. 2003, 64, 665–673. [Google Scholar] [CrossRef]
- Pakfetrat, M.; Yaghobi, R.; Salmanpoor, Z.; Roozbeh, J.; Torabinezhad, S.; Kadkhodaei, S. Frequency of Polyomavirus BK Infection in Kidney Transplant Patients Suspected to Nephropathy. Int. J. Organ Transplant. Med. 2015, 6, 77–84. [Google Scholar]
- Huang, A.L.; Hendren, N.; Carter, S.; Larsen, C.; Garg, S.; La Hoz, R.; Farr, M. Biomarker-Based Assessment for Infectious Risk Before and After Heart Transplantation. Curr. Heart Fail. Rep. 2022, 19, 236–246. [Google Scholar] [CrossRef]
- Kim, M.H.; Lee, Y.H.; Seo, J.-W.; Moon, H.; Kim, J.S.; Kim, Y.G.; Jeong, K.-H.; Moon, J.-Y.; Lee, T.W.; Ihm, C.-G.; et al. Urinary exosomal viral microRNA as a marker of BK virus nephropathy in kidney transplant recipients. PLoS ONE 2017, 12, e0190068. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Zeng, G.; Randhawa, P.S. Detection of BKV encoded mature MicroRNAs in kidney transplant patients: Clinical and biologic insights. J. Clin. Virol. 2019, 119, 6–10. [Google Scholar] [CrossRef]
- Gunasekaran, M.; Bansal, S.; Ravichandran, R.; Sharma, M.; Perincheri, S.; Rodriguez, F.; Hachem, R.; Fisher, C.E.; Limaye, A.P.; Omar, A.; et al. Respiratory viral infection in lung transplantation induces exosomes that trigger chronic rejection. J. Heart Lung Transplant. 2020, 39, 379–388. [Google Scholar] [CrossRef]
- Braun, F.; Rinschen, M.; Buchner, D.; Bohl, K.; Plagmann, I.; Bachurski, D.; Späth, M.R.; Antczak, P.; Göbel, H.; Klein, C.; et al. The proteomic landscape of small urinary extracellular vesicles during kidney transplantation. J. Extracell. Vesicles 2020, 10, e12026. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Li, W.; Cao, L.; Wang, B.; Liu, C.; Qin, Y.; Guo, B.; Huang, C. Serum extracellular vesicle MicroRNAs as candidate biomarkers for acute rejection in patients subjected to liver transplant. Front. Genet. 2022, 13, 1015049. [Google Scholar] [CrossRef] [PubMed]
- Gunasekaran, M.; Sharma, M.; Hachem, R.; Bremner, R.; Smith, M.A.; Mohanakumar, T. Circulating Exosomes with Distinct Prop-erties during Chronic Lung Allograft Rejection. J. Immunol. 2018, 200, 2535–2541. [Google Scholar] [CrossRef]
- Erdbrügger, U.; Blijdorp, C.J.; Bijnsdorp, I.V.; Borràs, F.E.; Burger, D.; Bussolati, B.; Byrd, J.B.; Clayton, A.; Dear, J.W.; Falcón-Pérez, J.M.; et al. Urinary extracellular vesicles: A position paper by the Urine Task Force of the International Society for Extracellular Vesicles. J. Extracell. Vesicles 2021, 10, e12093. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Research Topic | Organ | Study Population | EVs Origin | EVs Component | Reported Outcomes | Reference |
|---|---|---|---|---|---|---|
| Preoperative donor organ assessment | Kidney | LD | Urinary EVs | Various membrane protein signatures | Kidneys with nephrosclerosis correlated to fewer podocyte, parietal, or tubular cell EVs, among others. Kidneys with nephron hypertrophy correlated to fewer mesangial or descending limbs of Henle’s loop cell EVs. | Turco A.E. et al. [58] |
| LD vs. DD | miRNAs analysis, miR-326 | No overall differences were found in EVs miRNA profiles of living and deceased donors in normofunctioning grafts at 1 year. Only miRNA-223, which targets pro-apoptotic protein Bcl-2, was found overexpressed in living donors. | Lozano-Ramos S.I. et al. [59] | |||
| Prediction of postoperative graft function | Kidney | Human TR with vs. without DFG | EVs in preservation fluid | Multiple miRNAs | Differences between the two groups were found in 10 miRNAs upon basic analysis, but differences were lost upon multiple testing correction. Groups were not successfully identified via unsupervised clustering in PCA. | Gremmels H. et al. [60] |
| Human TR with vs. without DFG | Urinary EVs | Membrane protein (CD133+ EVs) | Patients with DFG had a significant increase in the CD133+ extracellular vesicle subpopulation compared with patients with early graft function. CD133+ may reflect the activity of progenitor cells in damage repair. | Dimuccio V. et al. [62] | ||
| Human TR with vs. without DFG (from DD vs. LD) | NGAL | NGAL levels were higher in kidney recipients from DDs. NGAL levels are significantly higher in patients with DGF compared with early graft function. | Alvarez S. et al. [63] | |||
| Human TR | NGAL, cystatin C, and IL-18 mRNA | Free urinary NGAL and cystatin C were correlated with serum creatinine at day 7 post-transplant. However, a poor correlation between EV-contained NGAL, cystatin C, or IL-18 mRNA and serum creatinine was found. | Peake P.W. et al. [64] | |||
| Human TR | Proteomic analysis, phosphoenolpyruvate carboxykinase 2 (PCK2) | Proteomic profile 1-day post-transplant correlated with renal function at 1 year. PCK2 1-day post-transplant in uEVs, but not in renal tissue, could predict renal function at 1 year. | Braun F. et al. [119] | |||
| Human TR with vs. without DFG (from DD) | Plasma-derived EVs | hsa-miR-33a-5p, hsa-miR-98-5p, and hsa-miR-151a-5p | A total of 52 miRNAs were found to be overexpressed in DGF compared with early graft function; of them, the mentioned 3 miRNAs were coexpressed. hsa-miR-151a-5p was positively correlated with first-week markers of graft function. | Wang J. et al. [65] | ||
| Human TR with good vs. poor outcome based on eGFR | Proteomic analysis | Proteomic profile could differentiate patients with good outcomes from those with poor outcomes based on eGFR at 1 month. | Al-Nedawi K. et al. [66] | |||
| Human TR with vs. without DFG (eGFR < 60 mL/min/1.73 m2) vs. healthy controls | miRNA analysis (miR-21-5p, miR-210-3p, and miR-4639-5p) | The panel could accurately differentiate between subjects with chronic allograft dysfunction and normal graft function, with better performance than simple or double indicators (ROC-AUC 0.89). | Chen Y. et al. [67] | |||
| Diagnosis of acute graft rejection | Kidney | Human TR with vs. without acute rejection | Urinary EVs | mRNA analysis (CXCL11, STAT1, SERPINA1, BMP7, NAMPT, IFNGR1, and IL18BP, among others) | This panel outperforms eGRF in early diagnosis of acute graft rejection (ROC-AUC 0.93). Moreover, it can differentiate mechanism of rejection (TCMR vs. ABMR). | El Fekih R. et al. [80] |
| Human TR with vs. without ABMR vs. TCMR | Proteomic analysis, cystatin C (CST3), and lipopolysaccharide-binding protein (LBP) | The combination of EV-contained CST3 and LPS can accurately identify ABMR patients versus non-rejection patients (ROC-AUC 0.879 and 0.901, respectively), as well as to differentiate them from TCMR. | Kim M. et al. [77] | |||
| Human TR with vs. without TCMR | Proteomic analysis Tetraspanin 1 (TSPAN1) and hemopexin (HPX) | TSPAN1 and HPX were significantly overexpressed in TCMR patients. | Lim J.H. et al. [78] | |||
| Human TR with vs. without TCMR | T-cell-derived urinary EVs | Membrane protein (CD3) | Presence of T-cell-specific membrane marker CD3 could accurately predict TCMR (ROC-AUC 0.911). | Park J. et al. [81] | ||
| Human TR with vs. without AR | Whole urine urinary EVs | Proteomic analysis | Eleven proteins were overexpressed in AR, three of which (CLCA1, PROS1, and KIAA053) were specific to the EV fraction. | Sigdel T.K. et al. [79] | ||
| Human TR with vs. without ABMR | Plasma-derived EVs | Membrane markers (C4d+, CD144+, and annexin V+) | C4d+/CD144+ and C4d+/annexin V+ EV subpopulations were significantly increased in AR patients. Upon treatment, C4d+/CD144+ EVs significantly decreased. | Tower C.M. et al. [82] | ||
| Human TR with vs. without ABMR vs. TCMR | mRNA analysis | Six genes were overexpressed in ABMR patients. A combination of 4 genes (gp130, SH2D1B, TNFα, and CCL4) can accurately predict ABMR. | Zhang H. et al. [83] | |||
| Liver | Human TR with vs. without TCMR | Plasma-derived EVs | Multiple miRNAs | Expression of miRNAs was significantly different between AR and non-AR patients. miR-223 and let-7e-5p were up-regulated in AR patients, whereas miR-199a-3p was down-regulated. | Wang W. et al. [120] | |
| Human TR with vs. without TCMR | Plasma-derived EVs | Galectin-9 | Levels of galectin-9 were higher in patients with acute TCMR. | Zhang A. et al. [87] | ||
| Lung | Human TR with vs. without AR or BOS | Plasma-derived EVs BALF-derived EVs | Donor HLA; lung-associated self-antigens (collagen V [Col-V] and K alpha 1 tubulin [Kα1T]) miRNA analysis | EV-contained donor HLA and collagen V were significantly overexpressed in AR and BOS compared with healthy patients (p < 0.05). Collagen V was detected 3 months before AR and 6 months before BOS diagnosis. Differentially expressed immunoregulatory miRNAs were found for AR (miR-92a and miR-182) and BOL (previous ones and miR-142-5p and miR-155) compared with control. | Gunasekaran M. et al. [100] | |
| Human TR with vs. without AR | BALF-derived EVs | RNA analysis | Transcriptomic signatures were significantly different between patients with and without AR. Patients with AR showed overexpression of antigen-processing immune activation pathways. | Gregson A. et al. [99] | ||
| Heart | Mice TR with vs. without AR | Plasma-derived EVs | Total plasma EV concentration | Total plasma EV concentration remained stable in control group, while it significantly decreased in the AR group at grade 0R rejection on histology. The model proved accurate for early prediction of AR (ROC-AUC 0.934) before any histology changes are detected. | Habertheuer A. et al. [93] | |
| Human TR with vs. without ABMR vs. TCMR | Membrane proteins (37 proteins) | AR EVs had increased concentration and decreased diameter. AR overexpressed HLA-I, CD41b, ROR-1, and SSEA-4 compared with controls. TCMR overexpressed CD2 and CD3, while ABMR overexpressed HLA-II, CD-326, CD19, CD20, and CD-25. The diagnostic model built on these markers reached a high accuracy (ROC-AUC 0.865) | Castellani C. et al. [94] | |||
| Human TR with vs. without ABMR vs. TCMR | Proteomic analysis | A total of 45 EV-derived proteins were identified to differentiate 3 groups: control/heart failure group, heart transplant without rejection and, ABMR and TCMR. A total of 15 of them were differentially expressed between the 2 last groups (p < 0.05). Most of these proteins play a role in the immune response (complement activation, adaptive immunity, and coagulation). | Kennel P. et al. [95] | |||
| Pancreatic islets | Mice TR from human islets, with and without induced AR | Plasma-derived EVs from donor’s islets and recipient T cells | EVs concentration, proteomic analysis, and miRNA analysis | AR led to a decrease in donor EVs and an increase in T cell recipient EVs. Four proteins were differentially expressed in AR versus control: angiopoietin 1, HSC70, C3, and hemopexin. Changes in microRNA and proteomic profiles were detected in AR prior to clinical effects (hyperglycemia). | Vallabhajosyula P. et al. [89] | |
| Diagnosis of chronic graft rejection | Kidney | Human TR with chronic ABMR vs. healthy and other-cause damage (calcineurin inhibitors toxicity and interstitial fibrosis) | Urinary EVs | SYT17 | Chronic ABMR patients had significantly higher SYT17 than the other groups. SYT17 could predict chronic ABMR with higher accuracy than traditional laboratory parameters (ROC-AUC 0.82). | Takada Y. et al. [84] |
| Human TR with vs. without chronic ABMR | Proteomic analysis, APOA1, TTR, PIGR, HPX, AZGP1, and CP | Expression of the six proteins was increased in chronic rejection compared with long term graft survival. | Jung H.Y. et al. [85] | |||
| Human TR with chronic allograft disfunction, with vs. without ABMR | T helper cells and plasma-derived EVs | Membrane proteins (CD4, CXCR5, CXCR3, and CTLA4) | The CD4+ CXCR5+ CXCR3- EV subpopulation was higher in ABMR patients, while expression of CTLA-4 was lower in this group. | Yang J. et al. [86] | ||
| Lung | Human TR with vs. without BOS Mice immunized with EVs from patients with vs. without BOS | Plasma-derived EVs | Kα1T; Col-V MHC-II; costimulatory molecules, CD40, CD80, and CD86; and transcription factors (NF-κB, hypoxia-inducible factor 1-α, and IL-1R–associated kinase 1, among others) | The aforementioned proteins were overexpressed in BOS versus control patients. Mice treated with EVs from BOS patients developed a specific proinflammatory phenotype. | Gunasekaran M. et al. [121] | |
| Diagnosis of ischemia reperfusion injury | Kidney | Mice with vs. without IRI Mice with vs. without IRI | Plasma-derived renal EVs | miRNA-23a | IRI increased miRNA-23a, which plays a role in macrophage activation. Inhibition of miRNA-23a ameliorated inflammation in the renal parenchyma. | Li Z. et al. [106] |
| miR-374b-5p | Levels of miR-374b-5p were increased after IRI. Inhibition of miR-374b-5p would alleviate kidney injury, showing its role in the damage cascade. | Ding C. et al. [107] | ||||
| Rats with vs. without unilateral IRI | Urinary EVs | Aquaporin 1 (AQP1); fetuin-A | Glycosylated AQP1 secretion was significantly reduced in the first 6 h after IRI compared with controls or other causes of renal injury. AQP1 was also reduced in a TR patient 48 h after transplantation. | Sonoda H. et al. [104] | ||
| Diagnosis of infection | Kidney | Human TR with vs. without BK virus nephropathy | Urinary EVs | bkv-miR-B1-5p; bkv-miR-B1-5p/miR-16 | Levels of viral miRNA (bkv-miR-B1-5p and bkv-miR-B1-5p/miR-16) showed a significant correlation with urinary BK viral load, as well as to plasma BK viral load, and could accurately predict viruria (ROC-AUC 0.989 and 0.985, respectively). | Kim M. et al. [116] |
| Lung | Human TR with vs. without symptomatic respiratory tract infection Mice as recipients for EVs treatment | Plasma-derived renal EVs | Lung-associated self-antigens (collagen V [Col-V], K alpha 1 tubulin [Kα1T]), 20S proteasome, and viral antigens | EV-contained self-antigens and viral antigens were higher in recipients of symptomatic respiratory viral infections. Mice immunized with those EVs developed immune responses to self-antigens, such as fibrosis, small airway occlusion, and cellular infiltration. | Gunasekaran M. et al. [118] | |
| Immunosuppressive drug monitoring | Kidney | Human TR under calcineurin inhibitor treatment with vs. without chronic calcineurin inhibitor toxicity vs. interstitial fibrosis and tubular damage from other causes | Urinary EVs | Proteomic analysis, CTSZ, RAB8A and SERPINC1 | Members of the uroplakin and plakin families were significantly overexpressed in the group with calcineurin inhibitor toxicity. CTSZ, RAB8A, and SERPINC1 were significantly overexpressed in patients with toxicity compared with normally functioning ones. | Carreras-Planella L. et al. [109] |
| Human TR under various immunosuppressive therapies and tacrolimus therapy | miRNA analysis | Expression of miR-155-5p and miR-223-3p showed significant correlation with tacrolimus dose and could be used to monitor toxicity. miR-223-3p also correlated with serum creatinine. | Costa de Freitas R. et al. [110] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romero-García, N.; Huete-Acevedo, J.; Mas-Bargues, C.; Sanz-Ros, J.; Dromant, M.; Badenes, R.; Borrás, C. Extracellular Vesicles: The Future of Diagnosis in Solid Organ Transplantation? Int. J. Mol. Sci. 2023, 24, 5102. https://doi.org/10.3390/ijms24065102
Romero-García N, Huete-Acevedo J, Mas-Bargues C, Sanz-Ros J, Dromant M, Badenes R, Borrás C. Extracellular Vesicles: The Future of Diagnosis in Solid Organ Transplantation? International Journal of Molecular Sciences. 2023; 24(6):5102. https://doi.org/10.3390/ijms24065102
Chicago/Turabian StyleRomero-García, Nekane, Javier Huete-Acevedo, Cristina Mas-Bargues, Jorge Sanz-Ros, Mar Dromant, Rafael Badenes, and Consuelo Borrás. 2023. "Extracellular Vesicles: The Future of Diagnosis in Solid Organ Transplantation?" International Journal of Molecular Sciences 24, no. 6: 5102. https://doi.org/10.3390/ijms24065102
APA StyleRomero-García, N., Huete-Acevedo, J., Mas-Bargues, C., Sanz-Ros, J., Dromant, M., Badenes, R., & Borrás, C. (2023). Extracellular Vesicles: The Future of Diagnosis in Solid Organ Transplantation? International Journal of Molecular Sciences, 24(6), 5102. https://doi.org/10.3390/ijms24065102