
Comparison between [68Ga]Ga-PSMA-617 and [18F]FET PET as Imaging Biomarkers in Adult Recurrent Glioblastoma

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Patient Recruitment and Data Collection
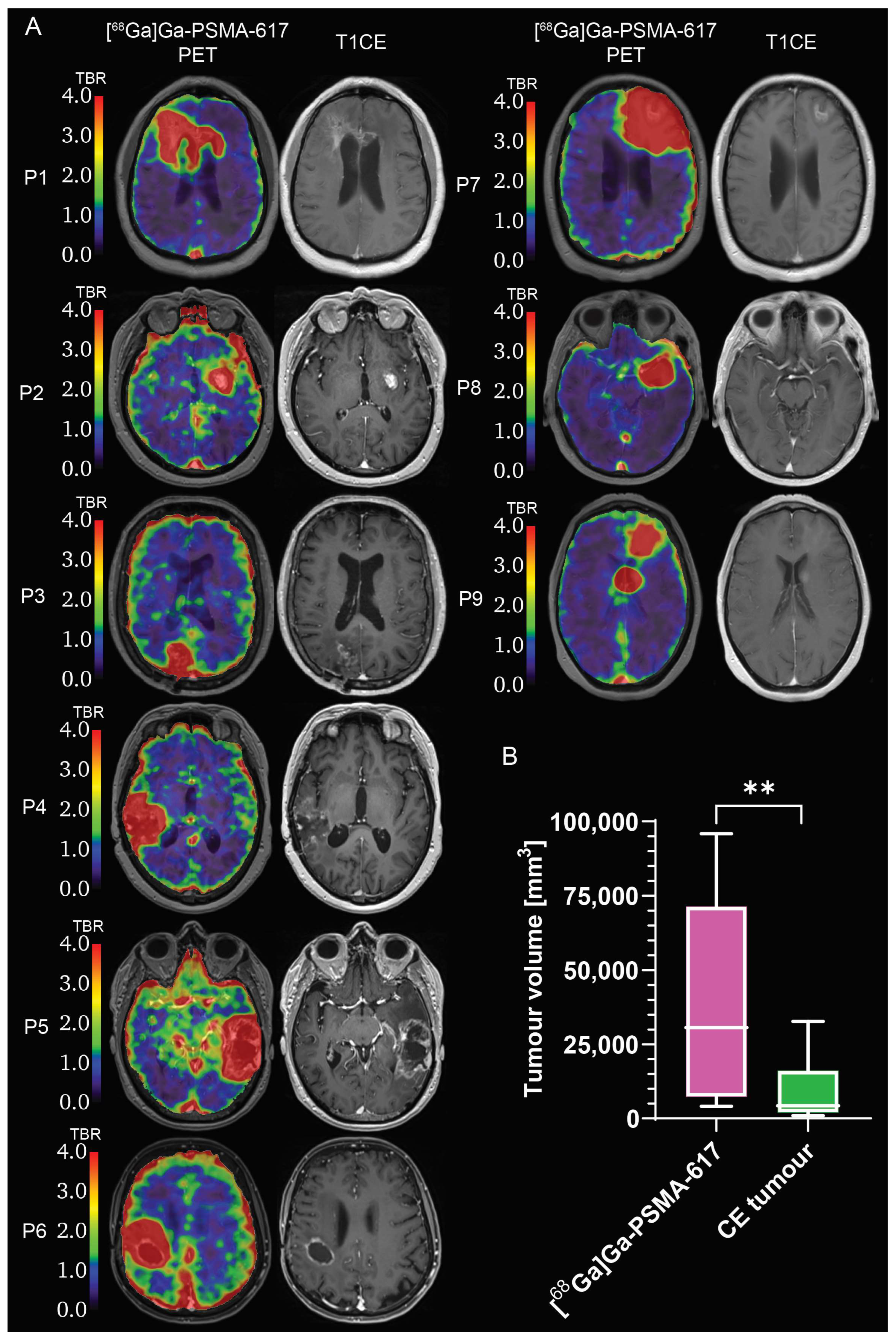
2.2. Evaluation of [68Ga]Ga-PSMA-617 Tumour Selectivity
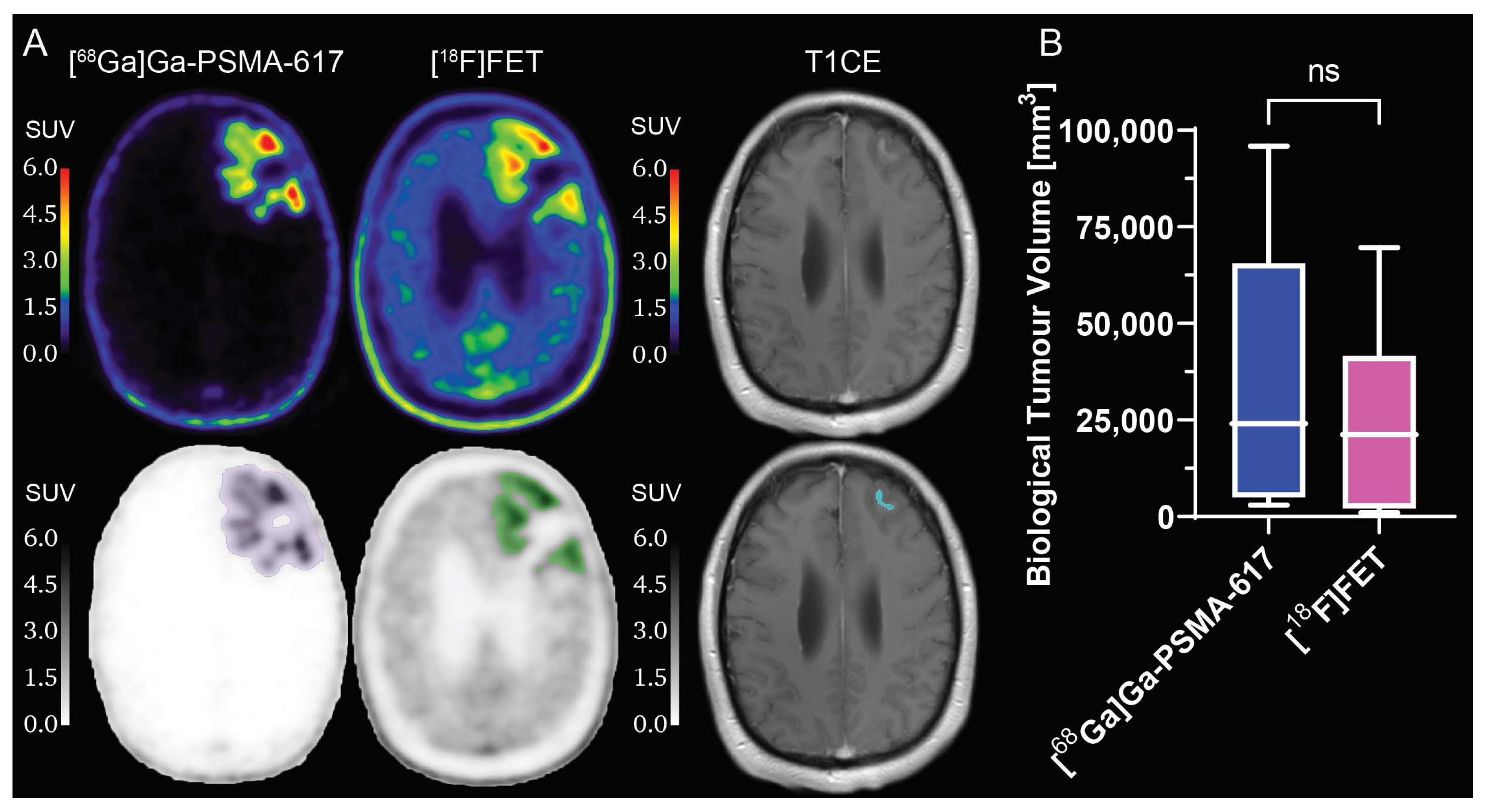
2.3. Comparison between [68Ga]Ga-PSMA-617 and [18F]FET Tumour Specificity
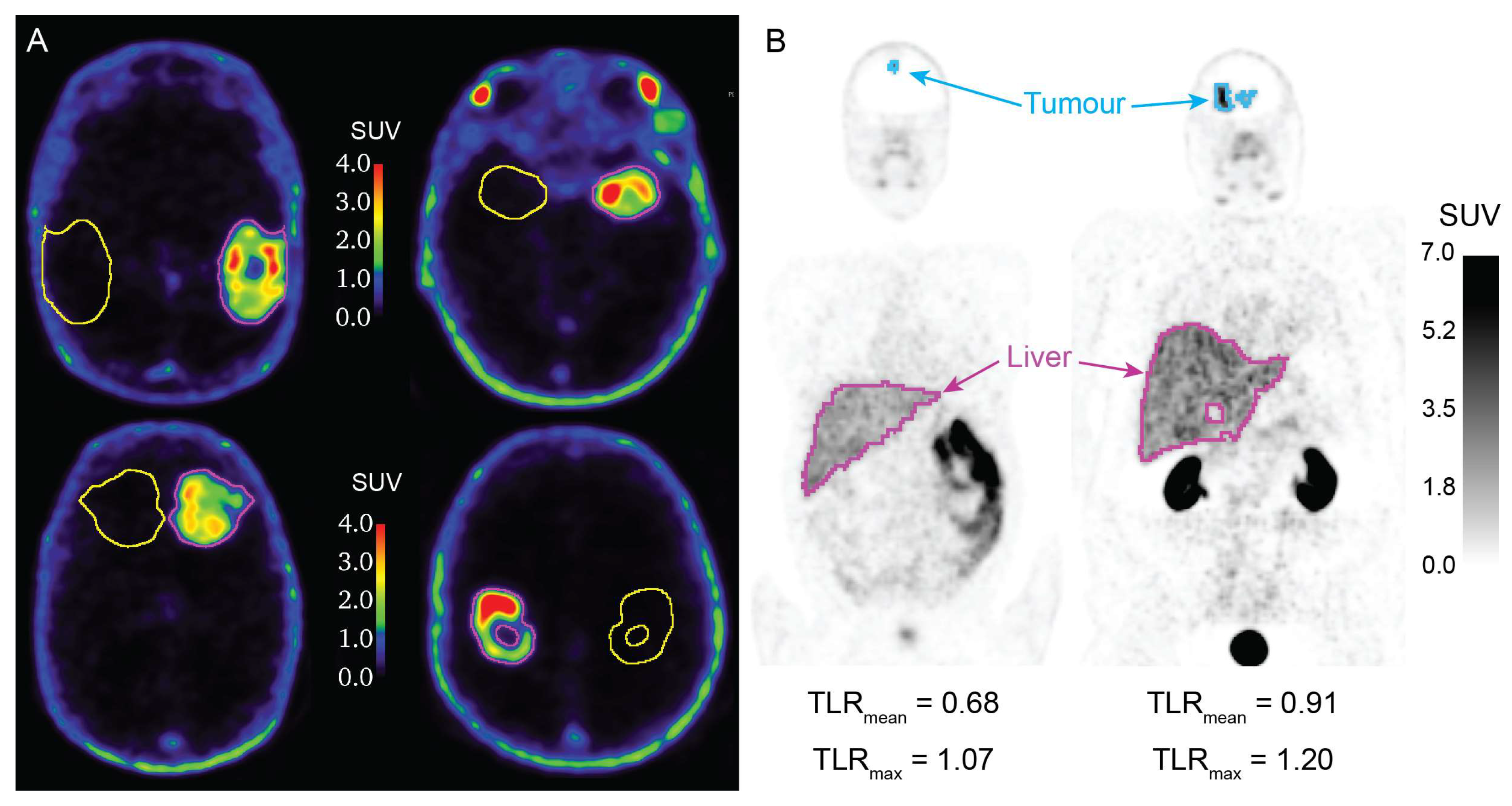
2.4. Evaluation of [68Ga]Ga-PSMA-617 Potential for Theranostics Application
3. Discussion
4. Materials and Methods
4.1. Clinical Trial Information
4.2. Eligibility Criteria
4.3. Study Plan
4.4. Radiolabeling and Positro Emission Tomography Imaging
4.5. Image Analysis
4.5.1. Pre-Processing
4.5.2. Segmentation
4.5.3. Metrics Calculation
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Silver:, D.A.; Pellicer, I.; Fair, W.R.; Heston, W.D.; Cordon-Cardo, C. Prostate-Specific Membrane Antigen Expression in Normal and Malignant Human Tissues. Clin. Cancer Res. 1997, 3, 81–85. [Google Scholar] [PubMed]
- Chang, S.S.; Reuter, V.E.; Heston, W.D.W.; Bander, N.H.; Grauer, L.S.; Gaudin, P.B. Five Different Anti-Prostate-Specific Membrane Antigen (PSMA) Antibodies Confirm PSMA Expression in Tumor-Associated Neovasculature. Cancer Res. 1999, 59, 3192–3198. [Google Scholar] [PubMed]
- Wernicke, A.G.; Edgar, M.A.; Lavi, E.; Liu, H.; Salerno, P.; Bander, N.H.; Gutin, P.H. Prostate-Specific Membrane Antigen as a Potential Novel Vascular Target for Treatment of Glioblastoma Multiforme. Arch. Pathol. Lab. Med. 2011, 135, 1486–1489. [Google Scholar] [CrossRef]
- Nomura, N.; Pastorino, S.; Jiang, P.; Lambert, G.; Crawford, J.R.; Gymnopoulos, M.; Piccioni, D.; Juarez, T.; Pingle, S.C.; Makale, M.; et al. Prostate Specific Membrane Antigen (PSMA) Expression in Primary Gliomas and Breast Cancer Brain Metastases. Cancer Cell Int. 2014, 14, 26. [Google Scholar] [CrossRef] [PubMed]
- Saffar, H.; Noohi, M.; Tavangar, S.M.; Saffar, H.; Azimi, S. Expression of Prostate-Specific Membrane Antigen (PSMA) in Brain Glioma and Its Correlation with Tumor Grade. Iran. J. Pathol. 2018, 13, 45–53. [Google Scholar] [CrossRef]
- Mahzouni, P.; Shavakhi, M. Prostate-Specific Membrane Antigen Expression in Neovasculature of Glioblastoma Multiforme. Adv. Biomed. Res. 2019, 8, 18. [Google Scholar] [CrossRef]
- Schwenck, J.; Tabatabai, G.; Skardelly, M.; Reischl, G.; Beschorner, R.; Pichler, B.; la Fougère, C. In Vivo Visualization of Prostate-Specific Membrane Antigen in Glioblastoma. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 170–171. [Google Scholar] [CrossRef]
- Sasikumar, A.; Joy, A.; Pillai, M.R.A.; Nanabala, R.; Anees K, M.; Jayaprakash, P.G.; Madhavan, J.; Nair, S. Diagnostic Value of 68Ga PSMA-11 PET/CT Imaging of Brain Tumors—Preliminary Analysis. Clin. Nucl. Med. 2017, 42, e41–e48. [Google Scholar] [CrossRef]
- Sasikumar, A.; Kashyap, R.; Joy, A.; Charan Patro, K.; Bhattacharya, P.; Reddy Pilaka, V.K.; Oommen, K.E.; Pillai, M.R.A. Utility of 68Ga-PSMA-11 PET/CT in Imaging of Glioma—A Pilot Study. Clin. Nucl. Med. 2018, 43, e304–e309. [Google Scholar] [CrossRef]
- Afshar-Oromieh, A.; Hetzheim, H.; Kratochwil, C.; Benesova, M.; Eder, M.; Neels, O.C.; Eisenhut, M.; Kübler, W.; Holland-Letz, T.; Giesel, F.L.; et al. The Theranostic PSMA Ligand PSMA-617 in the Diagnosis of Prostate Cancer by PET/CT: Biodistribution in Humans, Radiation Dosimetry, and First Evaluation of Tumor Lesions. J. Nucl. Med. 2015, 56, 1697–1705. [Google Scholar] [CrossRef]
- Wang, S.; Wang, J.; Liu, D.; Yang, D. The Value of 68Ga-PSMA-617 PET/CT in Differential Diagnosis between Low-Grade and High-Grade Gliomas. J. Nucl. Med. 2018, 59, 146. [Google Scholar]
- Kunikowska, J.; Kuliński, R.; Muylle, K.; Koziara, H.; Królicki, L. 68Ga–Prostate-Specific Membrane Antigen-11 PET/CT. Clin. Nucl. Med. 2020, 45, 11–18. [Google Scholar] [CrossRef]
- Kunikowska, J.; Charzyńska, I.; Kuliński, R.; Pawlak, D.; Maurin, M.; Królicki, L. Tumor Uptake in Glioblastoma Multiforme after IV Injection of [177Lu]Lu-PSMA-617. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1605–1606. [Google Scholar] [CrossRef]
- Coenen, H.H.; Elsinga, P.H.; Iwata, R.; Kilbourn, M.R.; Pillai, M.R.A.; Rajan, M.G.R.; Wagner, H.N.; Zaknun, J.J. Fluorine-18 Radiopharmaceuticals beyond [18F]FDG for Use in Oncology and Neurosciences. Nucl. Med. Biol. 2010, 37, 727–740. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; McConathy, J. Overview of PET Tracers for Brain Tumor Imaging. PET Clin. 2013, 8, 129–146. [Google Scholar] [CrossRef] [PubMed]
- Langen, K.-J.; Hamacher, K.; Weckesser, M.; Floeth, F.; Stoffels, G.; Bauer, D.; Coenen, H.H.; Pauleit, D. O-(2-[18F]Fluoroethyl)-l-Tyrosine: Uptake Mechanisms and Clinical Applications. Nucl. Med. Biol. 2006, 33, 287–294. [Google Scholar] [CrossRef]
- Traub-Weidinger, T.; Poetsch, N.; Woehrer, A.; Klebermass, E.M.; Bachnik, T.; Preusser, M.; Mischkulnig, M.; Kiesel, B.; Widhalm, G.; Mitterhauser, M.; et al. Psma Expression in 122 Treatment Naive Glioma Patients Related to Tumor Metabolism In11c-Methionine Pet and Survival. J. Pers. Med. 2021, 11, 624. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.K.; di Tomaso, E.; Duda, D.G.; Loeffler, J.S.; Sorensen, A.G.; Batchelor, T.T. Angiogenesis in Brain Tumours. Nat. Rev. Neurosci. 2007, 8, 610–622. [Google Scholar] [CrossRef]
- Tate, M.C.; Aghi, M.K. Biology of Angiogenesis and Invasion in Glioma. NeuroTherapeutics 2009, 6, 447–457. [Google Scholar] [CrossRef]
- Jensen, R.L. Brain Tumor Hypoxia: Tumorigenesis, Angiogenesis, Imaging, Pseudoprogression, and as a Therapeutic Target. J. Neurooncol. 2009, 92, 317–335. [Google Scholar] [CrossRef]
- Alberts, I.; Mingels, C.; Zacho, H.D.; Lanz, S.; Schöder, H.; Rominger, A.; Zwahlen, M.; Afshar-Oromieh, A. Comparing the Clinical Performance and Cost Efficacy of [68Ga]Ga-PSMA-11 and [18F]PSMA-1007 in the Diagnosis of Recurrent Prostate Cancer: A Markov Chain Decision Analysis. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 4252–4261. [Google Scholar] [CrossRef] [PubMed]
- Filss, C.P.; Albert, N.L.; Böning, G.; Kops, E.R.; Suchorska, B.; Stoffels, G.; Galldiks, N.; Shah, N.J.; Mottaghy, F.M.; Bartenstein, P.; et al. O-(2-[18F]Fluoroethyl)-l-Tyrosine PET in Gliomas: Influence of Data Processing in Different Centres. EJNMMI Res. 2017, 7, 64. [Google Scholar] [CrossRef] [PubMed]
- Lapa, C.; Linsenmann, T.; Monoranu, C.M.; Samnick, S.; Buck, A.K.; Bluemel, C.; Czernin, J.; Kessler, A.F.; Homola, G.A.; Ernestus, R.I.; et al. Comparison of the Amino Acid Tracers 18F-FET and 18F-DOPA in High-Grade Glioma Patients. J. Nucl. Med. 2014, 55, 1611–1616. [Google Scholar] [CrossRef]
- Pöpperl, G.; Götz, C.; Rachinger, W.; Gildehaus, F.J.; Tonn, J.C.; Tatsch, K. Value of O-(2-[18F]Fluoroethyl)-L-Tyrosine PET for the Diagnosis of Recurrent Glioma. Eur. J. Nucl. Med. Mol. Imaging 2004, 31, 1464–1470. [Google Scholar] [CrossRef] [PubMed]
- Rachinger, W.; Goetz, C.; Pöpperl, G.; Gildehaus, F.J.; Kreth, F.W.; Holtmannspötter, M.; Herms, J.; Koch, W.; Tatsch, K.; Tonn, J.-C.C. Positron Emission Tomography with O-(2-[18F]Fluoroethyl)-l-Tyrosine versus Magnetic Resonance Imaging in the Diagnosis of Recurrent Gliomas. Neurosurgery 2005, 57, 505–511. [Google Scholar] [CrossRef]
- Albert, N.L.; Weller, M.; Suchorska, B.; Galldiks, N.; Soffietti, R.; Kim, M.M.; La Fougère, C.; Pope, W.; Law, I.; Arbizu, J.; et al. Response Assessment in Neuro-Oncology Working Group and European Association for Neuro-Oncology Recommendations for the Clinical Use of PET Imaging in Gliomas. Neuro. Oncol. 2016, 18, 1199–1208. [Google Scholar] [CrossRef] [PubMed]
- Debus, C.; Waltenberger, M.; Floca, R.; Afshar-Oromieh, A.; Bougatf, N.; Adeberg, S.; Heiland, S.; Bendszus, M.; Wick, W.; Rieken, S.; et al. Impact of 18F-FET PET on Target Volume Definition and Tumor Progression of Recurrent High Grade Glioma Treated with Carbon-Ion Radiotherapy. Sci. Rep. 2018, 8, 7201. [Google Scholar] [CrossRef]
- Lowekamp, B.C.; Chen, D.T.; Ibáñez, L.; Blezek, D. The Design of SimpleITK. Front. Neuroinform. 2013, 7, 1–14. [Google Scholar] [CrossRef]
- Yaniv, Z.; Lowekamp, B.C.; Johnson, H.J.; Beare, R. SimpleITK Image-Analysis Notebooks: A Collaborative Environment for Education and Reproducible Research. J. Digit. Imaging 2018, 31, 290–303. [Google Scholar] [CrossRef]
- Beare, R.; Lowekamp, B.; Yaniv, Z. Image Segmentation, Registration and Characterization in R with SimpleITK. J. Stat. Softw. 2018, 86, 1–35. [Google Scholar] [CrossRef]
- Brighi, C. Genesis-GBM-001. Available online: https://doi.org/10.5281/zenodo.8124207 (accessed on 9 October 2023).
- Dcm2niix. Available online: https://github.com/rordenlab/dcm2niix (accessed on 20 September 2019).
- Laffon, E.; De Clermont, H.; Marthan, R. A Method of Adjusting SUV for Injection-Acquisition Time Differences in 18F-FDG PET Imaging. Eur. Radiol. 2011, 21, 2417–2424. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.M. Fast Robust Automated Brain Extraction. Hum. Brain Mapp. 2002, 17, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Brighi, C.; Puttick, S.; Li, S.; Keall, P.; Neville, K.; Waddington, D.; Bourgeat, P.; Gillman, A.; Fay, M. A Novel Semiautomated Method for Background Activity and Biological Tumour Volume Definition to Improve Standardisation of 18F-FET PET Imaging in Glioblastoma. EJNMMI Phys. 2022, 9, 9. [Google Scholar] [CrossRef] [PubMed]
- Hotta, M.; Gafita, A.; Murthy, V.; Benz, M.R.; Sonni, I.; Burger, I.A.; Eiber, M.; Emmett, L.; Farolfi, A.; Fendler, W.P.; et al. PSMA PET Tumor-to-Salivary Gland Ratio to Predict Response to [177Lu]PSMA Radioligand Therapy: An International Multicenter Retrospective Study. J. Nucl. Med. 2023, 64, 1024–1029. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Number | [18F]FET PET Scan [day month year] | [68Ga]Ga-PSMA-617 PET Scan [day month year] | Interval between Scans [days] |
|---|---|---|---|
| 1 | 11 October 2018 | 26 October 2018 | 15 |
| 2 | 9 September 2021 | 13 September 2021 | 4 |
| 3 | 15 November 2018 | 21 November 2018 | 6 |
| 4 | 29 November 2018 | 3 December 2018 | 4 |
| 5 | 8 November 2018 | 21 November 2018 | 13 |
| 6 | 13 November 2020 | 18 November 2020 | 5 |
| 7 | 13 November 2020 | 16 November 2020 | 3 |
| 8 | 24 January 2019 | 29 January 2019 | 5 |
| 9 | 28 March 2019 | 2 April 2019 | 5 |
| 10 | 15 July 2021 | 19 July 2021 | 4 |
| Patient Number | Tumour Volume [mm3] | SUVmean | SUVmax | TBRmean | TBRmax |
|---|---|---|---|---|---|
| 1 | 59,725 | 1.61 | 8.09 | 17.70 | 81.54 |
| 2 | 17,293 | 2.23 | 9.18 | 41.48 | 208.37 |
| 3 | 5070 | 0.79 | 1.96 | 27.39 | 112.88 |
| 4 | 4141 | 1.36 | 6.17 | 16.33 | 40.58 |
| 5 | 37,061 | 1.90 | 8.55 | 14.89 | 67.76 |
| 6 | 95,916 | 1.87 | 7.09 | 22.52 | 101.40 |
| 7 | 30,728 | 1.81 | 6.67 | 10.98 | 41.59 |
| 8 | 2956 | 1.68 | 7.28 | 19.23 | 70.85 |
| 9 | 83,177 | 1.90 | 8.35 | 22.76 | 98.65 |
| 10 | 9483 | 1.61 | 8.09 | 19.27 | 84.81 |
| Patient Number | Tumour Volume [mm3] | SUVmean | SUVmax | TBRmean | TBRmax |
|---|---|---|---|---|---|
| 1 | 39,765 | - | - | 2.26 | 4.86 |
| 2 | 9324 | 2.71 | 4.96 | 2.12 | 3.89 |
| 3 | 2080 | 5.36 | 7.73 | 2.14 | 3.08 |
| 4 | 974 | 2.41 | 2.76 | 1.83 | 2.09 |
| 5 | 14,211 | 2.98 | 4.87 | 2.05 | 3.34 |
| 6 | 47,071 | 3.20 | 6.44 | 2.22 | 4.46 |
| 7 | 33,819 | 2.35 | 4.44 | 2.22 | 4.19 |
| 8 | 1863 | 1.88 | 3.25 | 2.29 | 3.96 |
| 9 | 69,664 | 2.58 | 7.27 | 3.12 | 8.81 |
| 10 | 28,136 | 3.74 | 11.57 | 2.76 | 8.56 |
| Patient Number | [68Ga]Ga-PSMA-617 SUVmean | [68Ga]Ga-PSMA-617 SUVmax | [18F]FET SUVmean | [18F]FET SUVmax |
|---|---|---|---|---|
| 1 | 0.04 | 0.13 | - | - |
| 2 | 0.08 | 0.30 | 1.28 | 1.80 |
| 3 | 0.05 | 0.14 | 2.51 | 3.38 |
| 4 | 0.17 | 0.97 | 1.32 | 1.70 |
| 5 | 0.09 | 0.71 | 1.50 | 2.18 |
| 6 | 0.20 | 2.18 | 1.45 | 2.68 |
| 7 | 0.09 | 1.00 | 1.12 | 2.42 |
| 8 | 0.15 | 1.16 | 0.82 | 1.27 |
| 9 | 0.10 | 0.62 | 0.96 | 1.97 |
| 10 | 0.04 | 0.13 | 1.35 | 2.30 |
| Patient Number | TSGmean | TSGmax |
|---|---|---|
| 1 | 0.32 | 0.49 |
| 2 | 0.24 | 0.38 |
| 3 | 0.40 | 0.36 |
| 4 | 0.09 | 0.10 |
| 5 | 0.32 | 0.42 |
| 6 | 0.45 | 0.46 |
| 7 | 0.15 | 0.27 |
| 8 | 0.25 | 0.34 |
| 9 | 0.15 | 0.31 |
| 10 | 0.16 | 0.25 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brighi, C.; Puttick, S.; Woods, A.; Keall, P.; Tooney, P.A.; Waddington, D.E.J.; Sproule, V.; Rose, S.; Fay, M. Comparison between [68Ga]Ga-PSMA-617 and [18F]FET PET as Imaging Biomarkers in Adult Recurrent Glioblastoma. Int. J. Mol. Sci. 2023, 24, 16208. https://doi.org/10.3390/ijms242216208
Brighi C, Puttick S, Woods A, Keall P, Tooney PA, Waddington DEJ, Sproule V, Rose S, Fay M. Comparison between [68Ga]Ga-PSMA-617 and [18F]FET PET as Imaging Biomarkers in Adult Recurrent Glioblastoma. International Journal of Molecular Sciences. 2023; 24(22):16208. https://doi.org/10.3390/ijms242216208
Chicago/Turabian StyleBrighi, Caterina, Simon Puttick, Amanda Woods, Paul Keall, Paul A. Tooney, David E. J. Waddington, Vicki Sproule, Stephen Rose, and Michael Fay. 2023. "Comparison between [68Ga]Ga-PSMA-617 and [18F]FET PET as Imaging Biomarkers in Adult Recurrent Glioblastoma" International Journal of Molecular Sciences 24, no. 22: 16208. https://doi.org/10.3390/ijms242216208
APA StyleBrighi, C., Puttick, S., Woods, A., Keall, P., Tooney, P. A., Waddington, D. E. J., Sproule, V., Rose, S., & Fay, M. (2023). Comparison between [68Ga]Ga-PSMA-617 and [18F]FET PET as Imaging Biomarkers in Adult Recurrent Glioblastoma. International Journal of Molecular Sciences, 24(22), 16208. https://doi.org/10.3390/ijms242216208