

Statins in Children, an Update



Abstract
1. Introduction
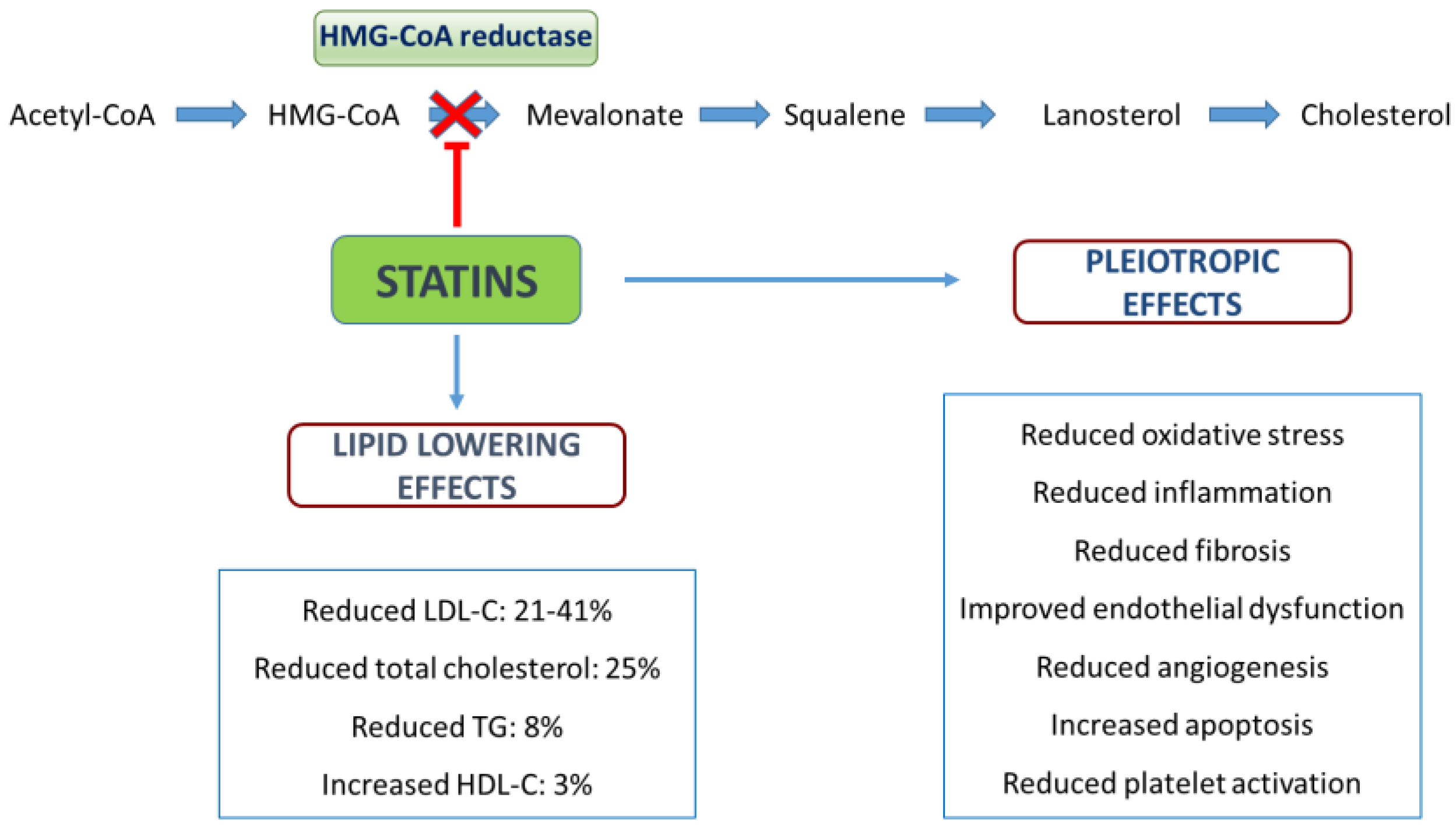
2. Cholesterol Metabolism and Mechanism of Action for Statins
3. Efficacy
4. Safety
5. Indications and Recommendations
6. Prescribing Statin Use in Youth
7. Surveillance
8. Limitations
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pahwa, R.; Jialal, I. Atherosclerosis. 2021 Sep 28. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation 2018, 137, e67–e492, Erratum in Circulation 2018, 137, e493. [Google Scholar] [CrossRef] [PubMed]
- Gatto, L.; Prati, F. Subclinical atherosclerosis: How and when to treat it? Eur. Heart J. Suppl. 2020, 22, E87–E90. [Google Scholar] [CrossRef] [PubMed]
- Ellulu, M.S.; Patimah, I.; Khaza’Ai, H.; Rahmat, A.; Abed, Y.; Ali, F. Atherosclerotic cardiovascular disease: A review of initiators and protective factors. Inflammopharmacology 2016, 24, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Linton, M.F.; Yancey, P.G.; Davies, S.S.; Jerome, W.G.; Linton, E.F.; Song, W.L.; Doran, A.C.; Vickers, K.C. The Role of Lipids and Lipoproteins in Atherosclerosis. In Endotext [Internet]; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., de Herder, W.W., Dhatariya, K., Dungan, K., Hershman, J.M., Hofland, J., Kalra, S., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- Burlutskaya, A.V.; Tril, V.E.; Polischuk, L.V.; Pokrovskii, V.M. Dyslipidemia in pediatrician’s practice. Rev. Cardiovasc. Med. 2021, 22, 817–834. [Google Scholar] [CrossRef]
- Baroncini, L.A.V.; Sylvestre, L.D.C.; Filho, R.P. Assessment of Intima-Media Thickness in Healthy Children Aged 1 to 15 Years. Arq. Bras. Cardiol. 2016, 106, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Gooty, V.D.; Sinaiko, A.R.; Ryder, J.; Dengel, D.R.; Jacobs, D.R.; Steinberger, J. Association Between Carotid Intima Media Thickness, Age, and Cardiovascular Risk Factors in Children and Adolescents. Metab. Syndr. Relat. Disord. 2018, 16, 122–126. [Google Scholar] [CrossRef]
- Briana, D.D.; Malamitsi-Puchner, A. Coronary Intimal Thickening Begins in Fetuses: Proof of Concept for the “Fetal Origins of Adult Disease” Hypothesis. Angiology 2019, 71, 89. [Google Scholar] [CrossRef]
- Guerri-Guttenberg, R.; Castilla, R.; Cao, G.; Azzato, F.; Ambrosio, G.; Milei, J. Coronary Intimal Thickening Begins in Fetuses and Progresses in Pediatric Population and Adolescents to Atherosclerosis. Angiology 2019, 71, 62–69. [Google Scholar] [CrossRef]
- Candelino, M.; Tagi, V.M.; Chiarelli, F. Cardiovascular risk in children: A burden for future generations. Ital. J. Pediatr. 2022, 48, 57. [Google Scholar] [CrossRef]
- Röhrl, C.; Stangl, H. Cholesterol metabolism—Physiological regulation and pathophysiological deregulation by the endoplasmic reticulum. Wien. Med. Wochenschr. 2018, 168, 280–285. [Google Scholar] [CrossRef]
- McMahan, C.A.; Gidding, S.S.; Malcom, G.T.; Tracy, R.E.; Strong, J.P.; McGill, H.C. Pathobiological Determinants of Atherosclerosis in Youth Research Group: Pathobiological Determinants of Atherosclerosis in Youth Risk Scores Are Associated with Early and Advanced Atherosclerosis. Pediatrics 2006, 118, 1447–1455. [Google Scholar] [CrossRef] [PubMed]
- Khoury, M.; McCrindle, B.W. The Rationale, Indications, Safety, and Use of Statins in the Pediatric Population. Can. J. Cardiol. 2020, 36, 1372–1383. [Google Scholar] [CrossRef]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: Executive Summary. J. Am. Coll. Cardiol. 2018, 73, 3168–3209, Erratum in J. Am. Coll. Cardiol. 2019, 73, 3234–3237. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the primary prevention of cardiovascular disease: A report of the american college of cardiology/American heart association task force on clinical practice guidelines. Circulation 2019, 140, e596–e646, Erratum in Circulation 2019, 140, e649–e650; Erratum in Circulation 2020, 141, e60; Erratum in Circulation 2020, 141, e774. [Google Scholar] [CrossRef] [PubMed]
- Trapani, L. Regulation and deregulation of cholesterol homeostasis: The liver as a metabolic “power station”. World J. Hepatol. 2012, 4, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Cerqueira, N.M.F.S.A.; Oliveira, E.F.; Gesto, D.S.; Santos-Martins, D.; Moreira, C.; Moorthy, H.N.; Ramos, M.J.; Fernandes, P.A. Cholesterol Biosynthesis: A Mechanistic Overview. Biochemistry 2016, 55, 5483–5506. [Google Scholar] [CrossRef] [PubMed]
- Feingold, K.R. Introduction to Lipids and Lipoproteins. In Endotext [Internet]; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., de Herder, W.W., Dhatariya, K., Dungan, K., Hershman, J.M., Hofland, J., Kalra, S., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- Lent-Schochet, D.; Jialal, I. Biochemistry, Lipoprotein Metabolism. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Ouimet, M.; Barrett, T.J.; Fisher, E.A. HDL and Reverse Cholesterol Transport. Circ. Res. 2019, 124, 1505–1518. [Google Scholar] [CrossRef] [PubMed]
- Pinal-Fernandez, I.; Casal-Dominguez, M.; Mammen, A.L. Statins: Pros and cons. Med. Clínica (Engl. Ed.) 2017, 150, 398–402. [Google Scholar] [CrossRef]
- Collins, R.; Reith, C.; Emberson, J.; Armitage, J.; Baigent, C.; Blackwell, L.; Blumenthal, R.; Danesh, J.; Smith, G.D.; DeMets, D.; et al. Interpretation of the evidence for the efficacy and safety of statin therapy. Lancet 2016, 388, 2532–2561, Erratum in Lancet 2017, 398, 602. [Google Scholar] [CrossRef]
- Istvan, E. Statin inhibition of HMG-CoA reductase: A 3-dimensional view. Atheroscler. Suppl. 2003, 4, 3–8. [Google Scholar] [CrossRef]
- Elkins, C.; Fruh, S.; Jones, L.; Bydalek, K. Clinical Practice Recommendations for Pediatric Dyslipidemia. J. Pediatr. Health Care 2019, 33, 494–504. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, M.; Amiri, S.; Pecic, S.; Machaj, F.; Rosik, J.; Łos, M.J.; Alizadeh, J.; Mahdian, R.; da Silva Rosa, S.C.; Schaafsma, D.; et al. Pleiotropic effects of statins: A focus on cancer. Biochim. Biophys. Acta (BBA) Mol. Basis Dis. 2020, 1866, 165968. [Google Scholar] [CrossRef]
- Zhang, Q.; Dong, J.; Yu, Z. Pleiotropic use of Statins as non-lipid-lowering drugs. Int. J. Biol. Sci. 2020, 16, 2704–2711. [Google Scholar] [CrossRef]
- Vuorio, A.; Kuoppala, J.; Kovanen, P.T.; Humphries, S.E.; Tonstad, S.; Wiegman, A.; Drogari, E.; Ramaswami, U. Statins for children with familial hypercholesterolemia. Cochrane Database Syst. Rev. 2017, 7, CD006401. [Google Scholar] [CrossRef]
- Radaelli, G.; Sausen, G.; Cesa, C.C.; Santos, F.D.S.; Portal, V.L.; Neyeloff, J.; Pellanda, L.C. Statin Treatments and Dosages in Children with Familial Hypercholesterolemia: Meta-Analysis. Arq. Bras. Cardiol. 2018, 111, 810–821. [Google Scholar] [CrossRef]
- Anagnostis, P.; Vaitsi, K.; Kleitsioti, P.; Mantsiou, C.; Pavlogiannis, K.; Athyros, V.G.; Mikhailidis, D.P.; Goulis, D.G. Efficacy and safety of statin use in children and adolescents with familial hypercholesterolaemia: A systematic review and meta-analysis of randomized-controlled trials. Endocrine 2020, 69, 249–261. [Google Scholar] [CrossRef]
- Fiorentino, R.; Chiarelli, F. Treatment of Dyslipidaemia in Children. Biomedicines 2021, 9, 1078. [Google Scholar] [CrossRef]
- Ferrari, F.; Martins, V.M.; Viviane, Z. Rochac Lipid Clinic Heart Institute (Incor), University of São Paulo Medical School Hospital, São Paulo, Brazil; Santos, R.D. Advances with lipid-lowering drugs for pediatric patients with familial hypercholesterolemia. Expert Opin. Pharmacother. 2020, 22, 483–495. [Google Scholar] [CrossRef]
- Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents; National Heart, Lung, and Blood Institute. Expert panel on integrated guidelines for cardiovascular health and risk reduction in children and adolescents: Summary report. Pediatrics 2011, 128 (Suppl. 5), S213–S256. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.L.; Wright, C.C.; Browne, B. Lipid-lowering medications for children and adolescents. J. Clin. Lipidol. 2015, 9, S67–S76. [Google Scholar] [CrossRef] [PubMed]
- Luirink, I.K.; Wiegman, A.; Kusters, D.M.; Hof, M.H.; Groothoff, J.W.; de Groot, E.; Kastelein, J.J.; Hutten, B.A. 20-Year Follow-up of Statins in Children with Familial Hypercholesterolemia. N. Engl. J. Med. 2019, 381, 1547–1556. [Google Scholar] [CrossRef] [PubMed]
- Mendelson, M.M.; Regh, T.; Chan, J.; Baker, A.; Ryan, H.H.; Palumbo, N.; Johnson, P.K.; Griggs, S.; Boghani, M.; Desai, N.K.; et al. Correlates of Achieving Statin Therapy Goals in Children and Adolescents with Dyslipidemia. J. Pediatr. 2016, 178, 149–155.e9. [Google Scholar] [CrossRef]
- Gidding, S.S.; Champagne, M.A.; De Ferranti, S.D.; Defesche, J.; Ito, M.K.; Knowles, J.W.; McCrindle, B.; Raal, F.; Rader, D.; Santos, R.D.; et al. The Agenda for Familial Hypercholesterolemia. Circulation 2015, 132, 2167–2192, Erratum in Circulation 2015, 132, e397. [Google Scholar] [CrossRef] [PubMed]
- Willeit, P.; Tschiderer, L.; Allara, E.; Reuber, K.; Seekircher, L.; Gao, L.; Liao, X.; Lonn, E.; Gerstein, H.C.; Yusuf, S.; et al. Carotid Intima-Media Thickness Progression as Surrogate Marker for Cardiovascular Risk. Circulation 2020, 142, 621–642. [Google Scholar] [CrossRef]
- Wiegman, A.; Hutten, B.A.; De Groot, E.; Rodenburg, J.; Bakker, H.D.; Büller, H.R.; Sijbrands, E.; Kastelein, J.J.P. Efficacy and Safety of Statin Therapy in Children with Familial Hypercholesterolemia. JAMA 2004, 292, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Rodenburg, J.; Vissers, M.N.; Wiegman, A.; van Trotsenburg, A.S.P.; Van Der Graaf, A.; De Groot, E.; Wijburg, F.A.; Kastelein, J.J.P.; Hutten, B.A. Statin Treatment in Children with Familial Hypercholesterolemia. Circulation 2007, 116, 664–668. [Google Scholar] [CrossRef]
- Kusters, D.M.; Avis, H.J.; De Groot, E.; Wijburg, F.A.; Kastelein, J.J.P.; Wiegman, A.; Hutten, B.A. Ten-Year Follow-up After Initiation of Statin Therapy in Children with Familial Hypercholesterolemia. JAMA 2014, 312, 1055–1057. [Google Scholar] [CrossRef]
- Wiegman, A.; Gidding, S.S.; Watts, G.F.; Chapman, M.J.; Ginsberg, H.N.; Cuchel, M.; Ose, L.; Averna, M.; Boileau, C.; Borén, J.; et al. Familial hypercholesterolaemia in children and adolescents: Gaining decades of life by optimizing detection and treatment. Eur. Heart J. 2015, 36, 2425–2437. [Google Scholar] [CrossRef]
- Vuorio, A.; Docherty, K.F.; Humphries, S.E.; Kuoppala, J.; Kovanen, P.T. Statin treatment of children with familial hypercholesterolemia—Trying to balance incomplete evidence of long-term safety and clinical accountability: Are we approaching a consensus? Atherosclerosis 2012, 226, 315–320. [Google Scholar] [CrossRef]
- Newman, C.B.; Preiss, D.; Tobert, J.A.; Jacobson, T.A.; Page, I.R.L.; Goldstein, L.B.; Chin, C.; Tannock, L.R.; Miller, M.; Raghuveer, G.; et al. Statin Safety and Associated Adverse Events: A Scientific Statement from the American Heart Association. Arter. Thromb. Vasc. Biol. 2019, 39, e38–e81, Erratum in Arter. Thromb. Vasc. Biol. 2019, 39, e158. [Google Scholar] [CrossRef]
- Mamann, N.; Lemale, J.; Karsenty, A.; Dubern, B.; Girardet, J.-P.; Tounian, P. Intermediate-Term Efficacy and Tolerance of Statins in Children. J. Pediatr. 2019, 210, 161–165. [Google Scholar] [CrossRef]
- Kavey, R.-E.W.; Manlhiot, C.; Runeckles, K.; Collins, T.; Gidding, S.S.; Demczko, M.; Clauss, S.; Harahsheh, A.S.; Mietus-Syder, M.; Khoury, M.; et al. Effectiveness and Safety of Statin Therapy in Children: A Real-World Clinical Practice Experience. CJC Open 2020, 2, 473–482. [Google Scholar] [CrossRef]
- Wiegman, A. Lipid Screening, Action, and Follow-up in Children and Adolescents. Curr. Cardiol. Rep. 2018, 20, 80. [Google Scholar] [CrossRef]
- Desai, N.K.; Mendelson, M.; Baker, A.; Ryan, H.H.; Griggs, S.; Boghani, M.; Yellen, E.; Buckley, L.; Gillman, M.W.; Zachariah, J.P.; et al. Hepatotoxicity of Statins as Determined by Serum Alanine Aminotransferase in a Pediatric Cohort with Dyslipidemia. J. Craniofacial Surg. 2019, 68, 175–181. [Google Scholar] [CrossRef]
- Gupta, A.; Thompson, D.; Whitehouse, A.; Collier, T.; Dahlof, B.; Poulter, N.; Collins, R.; Sever, P. Adverse events associated with unblinded, but not with blinded, statin therapy in the Anglo-Scandinavian Cardiac Outcomes Trial—Lipid-Lowering Arm (ASCOT-LLA): A randomised double-blind placebo-controlled trial and its non-randomised non-blind extension phase. Lancet 2017, 389, 2473–2481. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.K.; Mendelson, M.; Baker, A.; Ryan, H.H.; Warren, S.; Graham, D.; Griggs, S.S.; Desai, N.K.; Yellen, E.; Buckley, L.; et al. Statin-Associated Myopathy in a Pediatric Preventive Cardiology Practice. J. Pediatr. 2017, 185, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Corkins, M.R.; Daniels, S.R.; de Ferranti, S.D.; Golden, N.H.; Kim, J.H.; Magge, S.N.; Schwarzenberg, S.J. Nutrition in Children and Adolescents. Med. Clin. N. Am. 2016, 100, 1217–1235. [Google Scholar] [CrossRef] [PubMed]
- Eiland, L.S.; Luttrell, P.K. Use of Statins for Dyslipidemia in the Pediatric Population. J. Pediatr. Pharmacol. Ther. 2010, 15, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Cohen, H.; The Mighty Medic Satellite Research Group for Pediatric Dyslipidemia; Stefanutti, C. Current Approach to the Diagnosis and Treatment of Heterozygote and Homozygous FH Children and Adolescents. Curr. Atheroscler. Rep. 2021, 23, 30. [Google Scholar] [CrossRef] [PubMed]
- Vahedian-Azimi, A.; Makvandi, S.; Banach, M.; Reiner, Ž.; Sahebkar, A. Fetal toxicity associated with statins: A systematic review and meta-analysis. Atherosclerosis 2021, 327, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Maliachova, O. Familial Hypercholesterolemia in Children and Adolescents: Diagnosis and Treatment. Curr. Pharm. Des. 2019, 24, 3672–3677. [Google Scholar] [CrossRef] [PubMed]
- Farkouh, A.; Baumgärtel, C. Mini-review: Medication safety of red yeast rice products. Int. J. Gen. Med. 2019, 12, 167–171. [Google Scholar] [CrossRef]
- McCrindle, B.W.; Ose, L.; Marais, A. Efficacy and safety of atorvastatin in children and adolescents with familial hypercholesterolemia or severe hyperlipidemia: A multicenter, randomized, placebo-controlled trial. J. Pediatr. 2003, 143, 74–80. [Google Scholar] [CrossRef]
- Van Der Graaf, A.; Nierman, M.C.; Firth, J.C.; Wolmarans, K.H.; Marais, A.D.; De Groot, E. Efficacy and safety of fluvastatin in children and adolescents with heterozygous familial hypercholesterolaemia. Acta Paediatr. 2006, 95, 1461–1466. [Google Scholar] [CrossRef] [PubMed]
- Lambert, M.; Lupien, P.-J.; Gagné, C.; Lévy, E.; Blaichman, S.; Langlois, S.; Hayden, M.; Rose, V.; Clarke, J.T.R.; Wolfe, B.M.J.; et al. Treatment of Familial Hypercholesterolemia in Children and Adolescents: Effect of Lovastatin. Pediatrics 1996, 97, 619–628. [Google Scholar] [CrossRef]
- Stein, E.A.; Illingworth, D.R.; Kwiterovich, J.P.O.; Liacouras, C.A.; Siimes, M.A.; Jacobson, M.S.; Brewster, T.G.; Hopkins, P.; Davidson, M.; Graham, K.; et al. Efficacy and Safety of Lovastatin in Adolescent Males with Heterozygous Familial Hypercholesterolemia. JAMA 1999, 281, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Clauss, S.B.; Holmes, K.W.; Hopkins, P.; Stein, E.; Cho, M.; Tate, A.; Johnson-Levonas, A.O.; Kwiterovich, P.O. Efficacy and Safety of Lovastatin Therapy in Adolescent Girls with Heterozygous Familial Hypercholesterolemia. Pediatrics 2005, 116, 682–688. [Google Scholar] [CrossRef] [PubMed]
- Braamskamp, M.J.; Stefanutti, C.; Langslet, G.; Drogari, E.; Wiegman, A.; Hounslow, N.; Kastelein, J.J. Efficacy and Safety of Pitavastatin in Children and Adolescents at High Future Cardiovascular Risk. J. Pediatr. 2015, 167, 338–343.e5. [Google Scholar] [CrossRef]
- Knipscheer, H.C.; Boelen, C.C.A.; Kastelein, J.J.P.; Van Diermen, D.E.; Groenemeijer, B.E.; Ende, A.V.D.; Büller, H.R.; Bakker, H.D. Short-Term Efficacy and Safety of Pravastatin in 72 Children with Familial Hypercholesterolemia. Pediatr. Res. 1996, 39, 867–871, Erratum in Pediatr. Res. 1996, 40, 866. [Google Scholar] [CrossRef]
- Avis, H.J.; Hutten, B.A.; Gagné, C.; Langslet, G.; McCrindle, B.W.; Wiegman, A.; Hsia, J.; Kastelein, J.J.; Stein, E.A. Efficacy and Safety of Rosuvastatin Therapy for Children with Familial Hypercholesterolemia. J. Am. Coll. Cardiol. 2010, 55, 1121–1126. [Google Scholar] [CrossRef]
- Couture, P.; Brun, L.D.; Szots, F.; Lelièvre, M.; Gaudet, D.; Després, J.-P.; Simard, J.; Lupien, P.J.; Gagné, C. Association of Specific LDL Receptor Gene Mutations with Differential Plasma Lipoprotein Response to Simvastatin in Young French Canadians with Heterozygous Familial Hypercholesterolemia. Arter. Thromb. Vasc. Biol. 1998, 18, 1007–1012. [Google Scholar] [CrossRef]
- de Jongh, S.; Ose, L.; Szamosi, T.; Gagné, C.; Lambert, M.; Scott, R.; Perron, P.; Dobbelaere, D.; Saborio, M.; Tuohy, M.B.; et al. Efficacy and Safety of Statin Therapy in Children with Familial Hypercholesterolemia. Circulation 2002, 106, 2231–2237. [Google Scholar] [CrossRef] [PubMed]
- Bays, H.E.; Jones, P.H.; Orringer, C.E.; Brown, W.V.; Jacobson, T.A. National Lipid Association Annual Summary of Clinical Lipidology 2016. J. Clin. Lipidol. 2016, 10, S1–S43. [Google Scholar] [CrossRef]
- Miller, M.L.; Wright, C.C.; Rodriguez, B. Use of Lipid Lowering Medications in Youth. In Endotext [Internet]; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., de Herder, W.W., Dhatariya, K., Dungan, K., Hershman, J.M., Hofland, J., Kalra, S., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- De Ferranti, S.D.; Steinberger, J.; Ameduri, R.; Baker, A.; Gooding, H.; Kelly, A.S.; Mietus-Snyder, M.; Mitsnefes, M.M.; Peterson, A.L.; St-Pierre, J.; et al. Cardiovascular Risk Reduction in High-Risk Pediatric Patients: A Scientific Statement from the American Heart Association. Circulation 2019, 139, e603–e634. [Google Scholar] [CrossRef] [PubMed]
- NCEP Expert Panel on Blood Cholesterol Levels in Children and Adolescents. National Cholesterol Education Program (NCEP): Highlights of the report of the Expert Panel on Blood Cholesterol Levels in Children and Adolescents. Pediatrics 1992, 89, 495–501. [Google Scholar] [CrossRef]
- American Academy of Pediatrics; Committee on Nutrition. American Academy of Pediatrics. Committee on Nutrition. Cholesterol in childhood. Pediatrics 1998, 101, 141–147. [Google Scholar]
- McCrindle, B.W.; Urbina, E.M.; Dennison, B.A.; Jacobson, M.S.; Steinberger, J.; Rocchini, A.P.; Hayman, L.L.; Daniels, S.R. Drug Therapy of High-Risk Lipid Abnormalities in Children and Adolescents. Circulation 2007, 115, 1948–1967. [Google Scholar] [CrossRef]
- Ramaswami, U.; Humphries, S.E.; Priestley-Barnham, L.; Green, P.; Wald, D.S.; Capps, N.; Anderson, M.; Dale, P.; Morris, A.A. Current management of children and young people with heterozygous familial hypercholesterolaemia—HEART UK statement of care. Atherosclerosis 2019, 290, 1–8. [Google Scholar] [CrossRef]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS): The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur. Heart J. 2020, 41, 111–188, Erratum in Eur. Heart J. 2020, 41, 4255. [Google Scholar] [CrossRef]
- Cuchel, M.; Bruckert, E.; Ginsberg, H.N.; Raal, F.J.; Santos, R.D.; Hegele, R.A.; Kuivenhoven, J.A.; Nordestgaard, B.G.; Descamps, O.S.; Steinhagen-Thiessen, E.; et al. Homozigot ailevi hiperkolesterolemi: Klinisyenlerin taniyi ve klinik yönetimi geliştirmelerine yönelik yeni anlayişlar ve rehberlik. Avrupa Ateroskleroz Derneği’nin Ailevi Hiperkolesterolemi Üzerine Uzlaşi Paneli yazili görüşü [Homozygous familial hypercholesterolaemia: New insights and guidance for clinicians to improve detection and clinical management. A position paper from the Consensus Panel on Familial Hypercholesterolaemia of the European Atherosclerosis Society]. Turk Kardiyol. Dern. Ars. 2015, 43 (Suppl. 1), 1–14. (In Turkish) [Google Scholar]
- McGowan, M.P.; Dehkordi, S.H.H.; Moriarty, P.M.; Duell, P.B. Diagnosis and Treatment of Heterozygous Familial Hypercholesterolemia. J. Am. Heart Assoc. 2019, 8, e013225. [Google Scholar] [CrossRef] [PubMed]
- Awad, K.; Serban, M.-C.; Penson, P.; Mikhailidis, D.P.; Toth, P.P.; Jones, S.R.; Rizzo, M.; Howard, G.; Lip, G.Y.; Banach, M. Effects of morning vs evening statin administration on lipid profile: A systematic review and meta-analysis. J. Clin. Lipidol. 2017, 11, 972–985.e9. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.M. Dyslipidemia in Children and Adolescents: When and How to Diagnose and Treat? Pediatr. Gastroenterol. Hepatol. Nutr. 2014, 17, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Balla, S.; Ekpo, E.P.; Wilemon, K.A.; Knowles, J.W.; Rodriguez, F. Women Living with Familial Hypercholesterolemia: Challenges and Considerations Surrounding Their Care. Curr. Atheroscler. Rep. 2020, 22, 60. [Google Scholar] [CrossRef] [PubMed]
- Hirota, T.; Ieiri, I. Drug–drug interactions that interfere with statin metabolism. Expert Opin. Drug Metab. Toxicol. 2015, 11, 1435–1447. [Google Scholar] [CrossRef]
- Hu, P.; Dharmayat, K.I.; Stevens, C.A.; Sharabiani, M.T.; Jones, R.S.; Watts, G.F.; Genest, J.; Ray, K.; Vallejo-Vaz, A.J. Prevalence of Familial Hypercholesterolemia Among the General Population and Patients with Atherosclerotic Cardiovascular Disease. Circulation 2020, 141, 1742–1759. [Google Scholar] [CrossRef]
- Bouhairie, V.E.; Goldberg, C. Familial hypercholesterolemia. Clin. Cardiol. 2015, 33, 169–179. [Google Scholar] [CrossRef]
- Ramaswami, U.; Futema, M.; Bogsrud, M.P.; Holven, K.B.; van Lennep, J.R.; Wiegman, A.; Descamps, O.S.; Vrablik, M.; Freiberger, T.; Dieplinger, H.; et al. Comparison of the characteristics at diagnosis and treatment of children with heterozygous familial hypercholesterolaemia (FH) from eight European countries. Atherosclerosis 2019, 292, 178–187. [Google Scholar] [CrossRef]
- O’Gorman, C.; Conwell, L.; O’Neill, M.B. Considering statins for cholesterol-reduction in children if lifestyle and diet changes do not improve their health: A review of the risks and benefits. Vasc. Health Risk Manag. 2010, 7, 1–14. [Google Scholar] [CrossRef]
- Tada, H.; Takamura, M.; Kawashiri, M.-A. Familial Hypercholesterolemia: A Narrative Review on Diagnosis and Management Strategies for Children and Adolescents. Vasc. Health Risk Manag. 2021, 17, 59–67. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Drug | Potency | Pediatric FDA Approvals | Age | Dose | Mean LDL-C % Reduction | Supporting Studies |
|---|---|---|---|---|---|---|
| Atorvastatin | High-potency | Heterozygous FH | 10–17 years | 10–20 mg/day | 40% | McCrindle et al. [57] |
| Fluvastatin | Low-potency | Heterozygous FH | 10–16 years | 20–80 mg/day | 34% | Van der Graaf et al. [58] |
| Lovastatin | Low-potency | Heterozygous FH | 10–17 years | 10–40 mg/day | 17–37% | Lambert et al. [59] Stein et al. [60] Clauss et al. [61] |
| Pitavastatin | High-potency | Heterozygous FH | ≥8 years | 1–4 mg/day | 23–39% | Braamskamp M.J. et al. [62] |
| Pravastatin | Low-potency | Heterozygous FH | 8–18 years | 20 mg (8–13 years) | 23–33% | Knipscheer et al. [63] |
| 40 mg (14–18 years) | ||||||
| Rosuvastatin | High-potency | Heterozygous FH | 8–17 years | 5–20 mg/day | 38–50% | Avis et al. [64] |
| Homozygous FH | ≥7 years | |||||
| Simvastatin | Moderate-potency | Heterozygous FH | 10–17 years | 10–40 mg/day | 31–41% | Couture et al. [65] de Jongh et al. [66] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiorentino, R.; Chiarelli, F. Statins in Children, an Update. Int. J. Mol. Sci. 2023, 24, 1366. https://doi.org/10.3390/ijms24021366
Fiorentino R, Chiarelli F. Statins in Children, an Update. International Journal of Molecular Sciences. 2023; 24(2):1366. https://doi.org/10.3390/ijms24021366
Chicago/Turabian StyleFiorentino, Riccardo, and Francesco Chiarelli. 2023. "Statins in Children, an Update" International Journal of Molecular Sciences 24, no. 2: 1366. https://doi.org/10.3390/ijms24021366
APA StyleFiorentino, R., & Chiarelli, F. (2023). Statins in Children, an Update. International Journal of Molecular Sciences, 24(2), 1366. https://doi.org/10.3390/ijms24021366