
Enhanced Innate and Acquired Immune Responses in Systemic Sclerosis Primary Peripheral Blood Mononuclear Cells (PBMCs)
 ,
,  , and
, and 
Abstract
:1. Introduction
2. Results
2.1. Basic Clinical Parameters of Participants
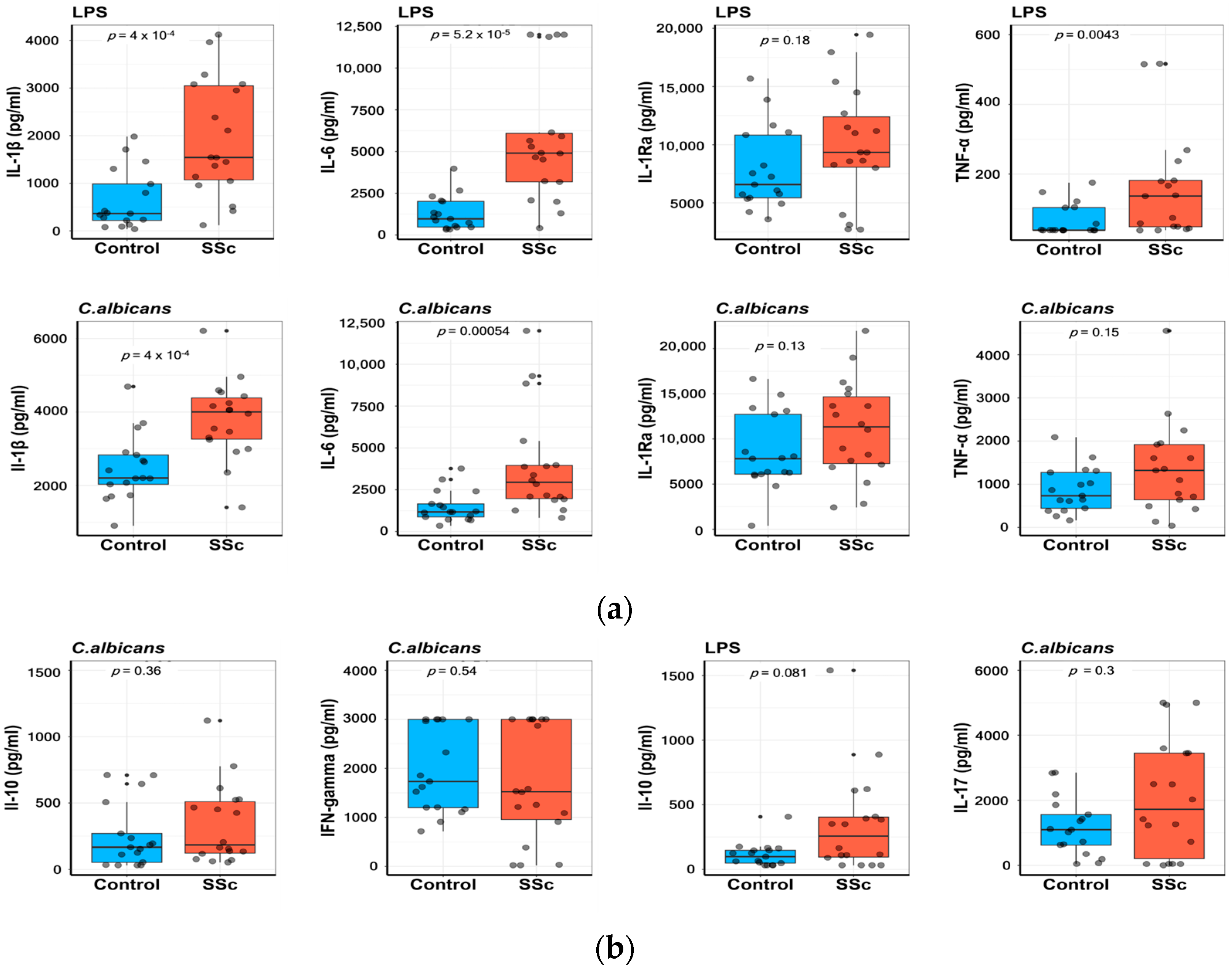
2.2. Patients with SSc Show Elevated Ex Vivo Cytokine Production Capacity
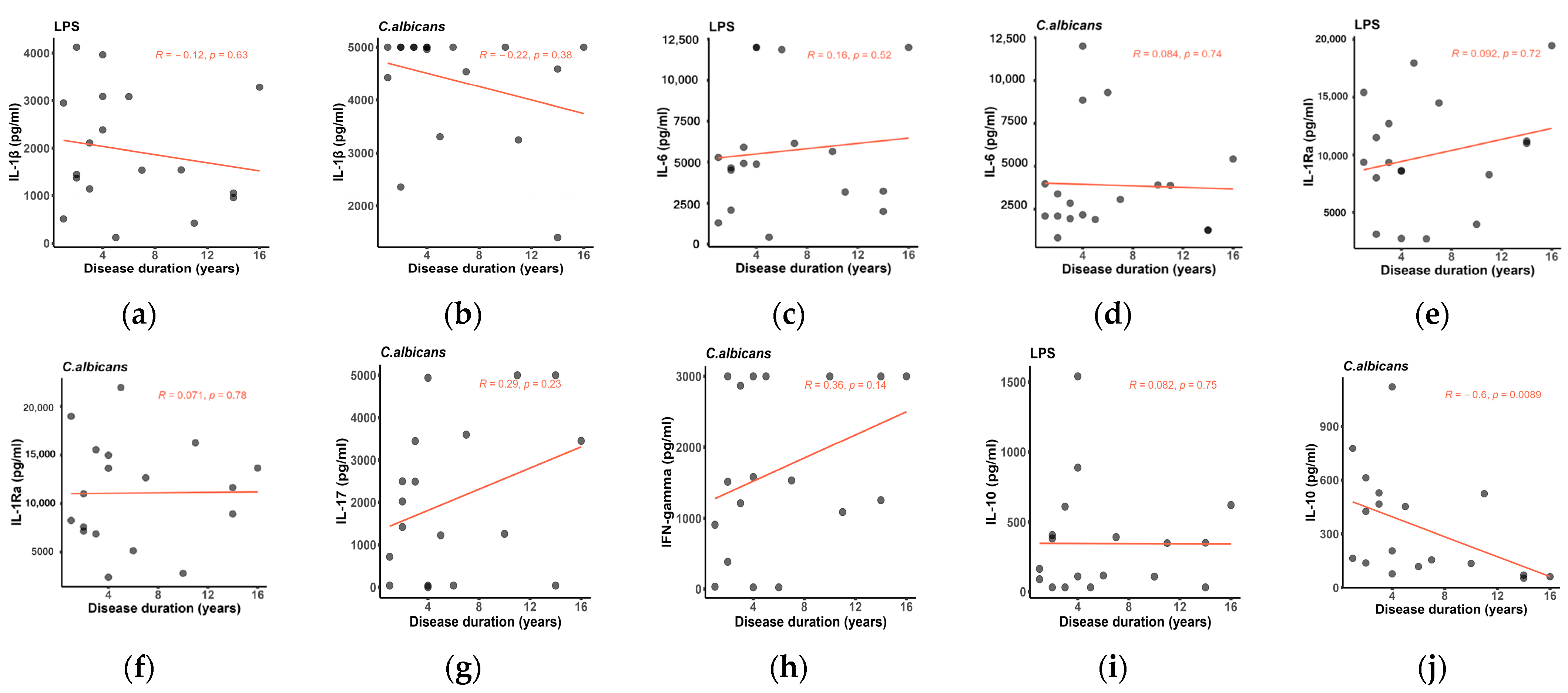
2.3. Assessment of Cytokine Production in Correlation to Disease Duration
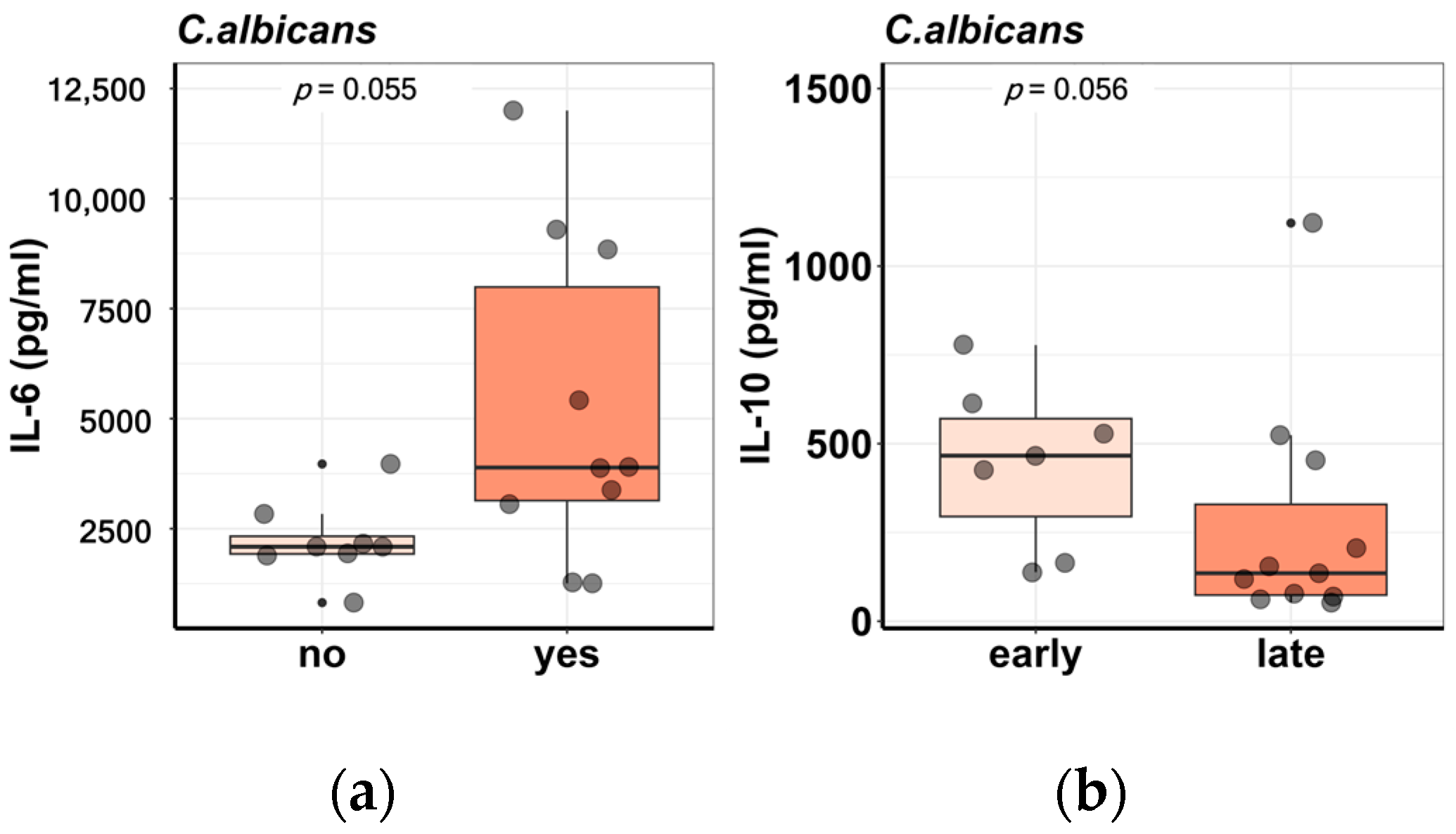
2.4. Cytokine Production in Relationship to SSc Subphenotypes
3. Discussion
4. Materials and Methods
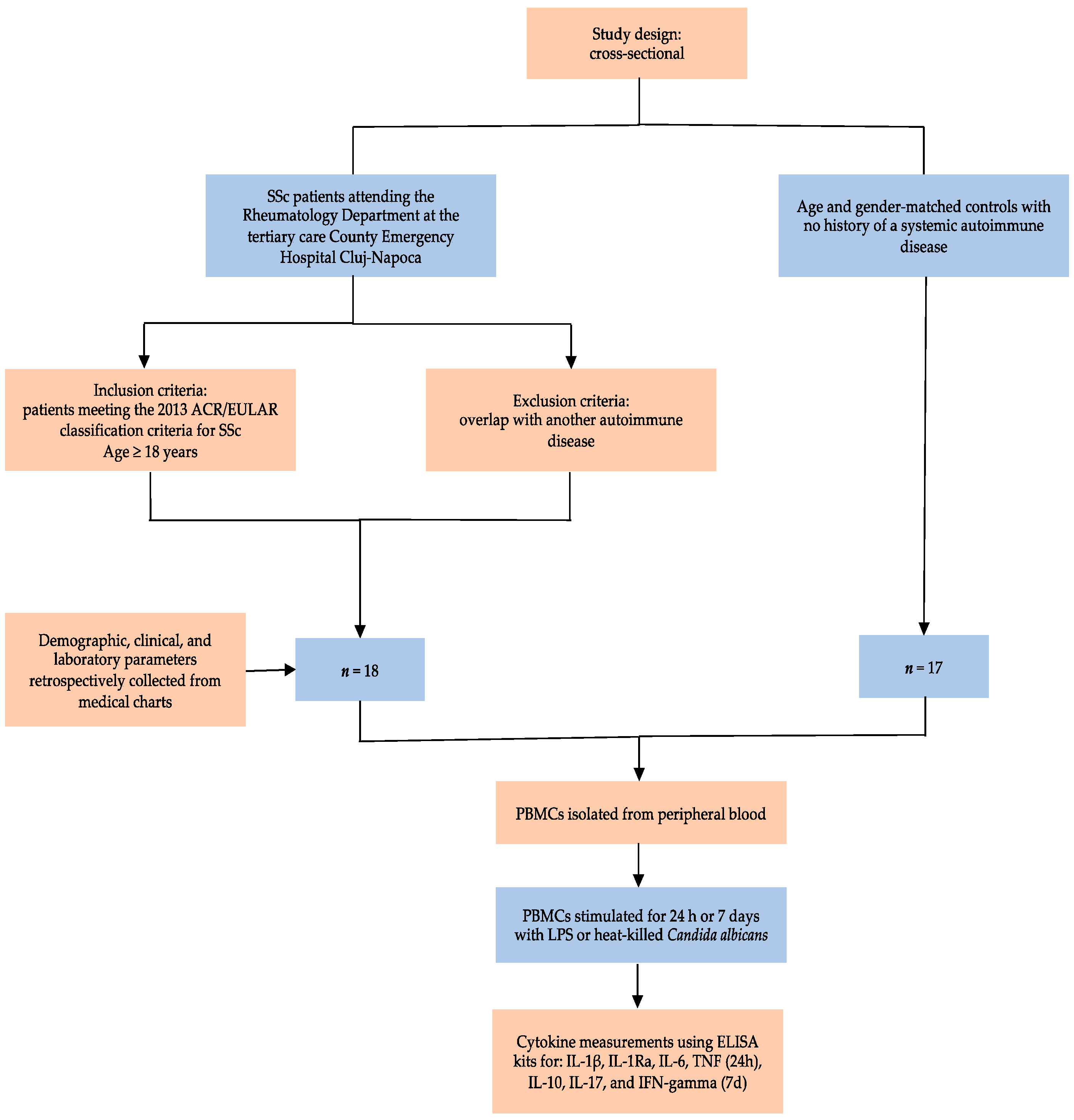
4.1. Study Design, Participants, and Variables
4.2. Cell Preparation and Culture Conditions
4.3. Cytokine Measurements
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Truchetet, M.E.; Brembilla, N.C.; Chizzolini, C. Current Concepts on the Pathogenesis of Systemic Sclerosis. Clin. Rev. Allergy Immunol. 2023, 64, 262–283. [Google Scholar] [CrossRef] [PubMed]
- Frasca, L.; Lande, R. Toll-like receptors in mediating pathogenesis in systemic sclerosis. Clin. Exp. Immunol. 2020, 201, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Benfaremo, D.; Svegliati, S.; Paolini, C.; Agarbati, S.; Moroncini, G. Systemic Sclerosis: From Pathophysiology to Novel Therapeutic Approaches. Biomedicines 2022, 10, 163. [Google Scholar] [CrossRef] [PubMed]
- Laurent, P.; Sisirak, V.; Lazaro, E.; Richez, C.; Duffau, P.; Blanco, P.; Truchetet, M.-E.; Contin-Bordes, C. Innate Immunity in Systemic Sclerosis Fibrosis: Recent Advances. Front. Immunol. 2018, 9, 1702. [Google Scholar] [CrossRef] [PubMed]
- Kania, G.; Rudnik, M.; Distler, O. Involvement of the myeloid cell compartment in fibrogenesis and systemic sclerosis. Nat. Rev. Rheumatol. 2019, 15, 288–302. [Google Scholar] [CrossRef]
- Bhandari, R.; Ball, M.S.; Martyanov, V.; Popovich, D.; Schaafsma, E.; Han, S.; ElTanbouly, M.; Orzechowski, N.M.; Carns, M.; Arroyo, E.; et al. Profibrotic Activation of Human Macrophages in Systemic Sclerosis. Arthritis Rheumatol. 2020, 72, 1160–1169. [Google Scholar] [CrossRef]
- Brown, M.; Postlethwaite, A.E.; Myers, L.K.; Hasty, K.A. Supernatants from culture of type I collagen-stimulated PBMC from patients with cutaneous systemic sclerosis versus localized scleroderma demonstrate suppression of MMP-1 by fibroblasts. Clin. Rheumatol. 2012, 31, 973–981. [Google Scholar] [CrossRef]
- De Almeida, A.R.; Dantas, A.T.; de Oliveira Gonçalves, M.E.; Chêne, C.; Jeljeli, M.; Chouzenoux, S.; Thomas, M.; Cunha, E.G.C.; de Azevedo Valadares, L.D.; de Melo Gomes, J.V.; et al. PPARγ partial agonist LPSF/GQ-16 prevents dermal and pulmonary fibrosis in HOCl-induced systemic sclerosis (SSc) and modulates cytokine production in PBMC of SSc patients. Inflammopharmacology 2023. [Google Scholar] [CrossRef]
- Liu, C.; Chu, D.; Kalantar-Zadeh, K.; George, J.; Young, H.A.; Liu, G. Cytokines: From Clinical Significance to Quantification. Adv. Sci. Weinh. Baden-Wurtt. Ger. 2021, 8, e2004433. [Google Scholar] [CrossRef]
- Raja, J.; Denton, C.P. Cytokines in the immunopathology of systemic sclerosis. Semin. Immunopathol. 2015, 37, 543–557. [Google Scholar] [CrossRef]
- Kantor, T.V.; Friberg, D.; Medsger, T.A.; Buckingham, R.B.; Whiteside, T.L. Cytokine production and serum levels in systemic sclerosis. Clin. Immunol. Immunopathol. 1992, 65, 278–285. [Google Scholar] [CrossRef]
- Dantas, A.T.; de Almeida, A.R.; Sampaio, M.C.P.D.; Cordeiro, M.F.; Oliveira, P.S.S.d.; Mariz, H.d.A.; Pereira, M.C.; Rego, M.J.B.d.M.; Pitta, I.d.R.; Duarte, A.L.B.P.; et al. Different profile of cytokine production in patients with systemic sclerosis and association with clinical manifestations. Immunol. Lett. 2018, 198, 12–16. [Google Scholar] [CrossRef]
- Umehara, H.; Kumagai, S.; Murakami, M.; Suginoshita, T.; Tanaka, K.; Hashida, S.; Ishikawa, E.; Imura, H. Enhanced production of interleukin-1 and tumor necrosis factor alpha by cultured peripheral blood monocytes from patients with scleroderma. Arthritis Rheum. 1990, 33, 893–897. [Google Scholar] [CrossRef]
- LeRoy, E.C.; Medsger, T.A. Criteria for the classification of early systemic sclerosis. J. Rheumatol. 2001, 28, 1573–1576. [Google Scholar] [PubMed]
- Gourh, P.; Arnett, F.C.; Assassi, S.; Tan, F.K.; Huang, M.; Diekman, L.; Mayes, M.D.; Reveille, J.D.; Agarwal, S.K. Plasma cytokine profiles in systemic sclerosis: Associations with autoantibody subsets and clinical manifestations. Arthritis Res. Ther. 2009, 11, R147. [Google Scholar] [CrossRef] [PubMed]
- Roumm, A.D.; Whiteside, T.L.; Medsger, T.A.; Rodnan, G.P. Lymphocytes in the skin of patients with progressive systemic sclerosis. Quantification, subtyping, and clinical correlations. Arthritis Rheum. 1984, 27, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Mavalia, C.; Scaletti, C.; Romagnani, P.; Carossino, A.M.; Pignone, A.; Emmi, L.; Pupilli, C.; Pizzolo, G.; Maggi, E.; Romagnani, S. Type 2 helper T-cell predominance and high CD30 expression in systemic sclerosis. Am. J. Pathol. 1997, 151, 1751–1758. [Google Scholar]
- York, M.R.; Nagai, T.; Mangini, A.J.; Lemaire, R.; van Seventer, J.M.; Lafyatis, R. A macrophage marker, Siglec-1, is increased on circulating monocytes in patients with systemic sclerosis and induced by type I interferons and toll-like receptor agonists. Arthritis Rheum. 2007, 56, 1010–1020. [Google Scholar] [CrossRef]
- Duan, H.; Fleming, J.; Pritchard, D.K.; Amon, L.M.; Xue, J.; Arnett, H.A.; Chen, G.; Breen, P.; Buckner, J.H.; Molitor, J.A.; et al. Combined analysis of monocyte and lymphocyte messenger RNA expression with serum protein profiles in patients with scleroderma. Arthritis Rheum. 2008, 58, 1465–1474. [Google Scholar] [CrossRef]
- Lakos, G.; Melichian, D.; Wu, M.; Varga, J. Increased bleomycin-induced skin fibrosis in mice lacking the Th1-specific transcription factor T-bet. Pathobiol. J. Immunopathol. Mol. Cell. Biol. 2006, 73, 224–237. [Google Scholar] [CrossRef]
- Scala, E.; Pallotta, S.; Frezzolini, A.; Abeni, D.; Barbieri, C.; Sampogna, F.; De Pità, O.; Puddu, P.; Paganelli, R.; Russo, G. Cytokine and chemokine levels in systemic sclerosis: Relationship with cutaneous and internal organ involvement. Clin. Exp. Immunol. 2004, 138, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Janahi, E.M.A.; Das, S.; Bhattacharya, S.N.; Haque, S.; Akhter, N.; Jawed, A.; Wahid, M.; Mandal, R.K.; Lohani, M.; Areeshi, M.Y.; et al. Cytomegalovirus aggravates the autoimmune phenomenon in systemic autoimmune diseases. Microb. Pathog. 2018, 120, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Magied, R.A.; Kamel, S.R.; Said, A.F.; Ali, H.M.; Abdel Gawad, E.A.; Moussa, M.M. Serum interleukin-6 in systemic sclerosis and its correlation with disease parameters and cardiopulmonary involvement. Sarcoidosis Vasc. Diffuse Lung Dis. Off. J. WASOG 2016, 33, 321–330. [Google Scholar] [CrossRef]
- Lin, X.; Ding, M.; Chen, T.; Min, S.; Wang, D.; Jiang, G. Peripheral blood IL-6 levels in systemic sclerosis patients: Correlation between IL-6 levels and clinical phenotypes. J. Cosmet. Dermatol. 2022, 21, 6086–6091. [Google Scholar] [CrossRef] [PubMed]
- Sato, S.; Hasegawa, M.; Takehara, K. Serum levels of interleukin-6 and interleukin-10 correlate with total skin thickness score in patients with systemic sclerosis. J. Dermatol. Sci. 2001, 27, 140–146. [Google Scholar] [CrossRef]
- Zhou, Y.; Fu, B.; Zheng, X.; Wang, D.; Zhao, C.; Qi, Y.; Sun, R.; Tian, Z.; Xu, X.; Wei, H. Pathogenic T-cells and inflammatory monocytes incite inflammatory storms in severe COVID-19 patients. Natl. Sci. Rev. 2020, 7, 998–1002. [Google Scholar] [CrossRef]
- Szabo, R.; Petrisor, C.; Bodolea, C.; Simon, R.; Maries, I.; Tranca, S.; Mocan, T. Hyperferritinemia, Low Circulating Iron and Elevated Hepcidin May Negatively Impact Outcome in COVID-19 Patients: A Pilot Study. Antioxidants 2022, 11, 1364. [Google Scholar] [CrossRef]
- Chikhoune, L.; Brousseau, T.; Morell-Dubois, S.; Farhat, M.M.; Maillard, H.; Ledoult, E.; Lambert, M.; Yelnik, C.; Sanges, S.; Sobanski, V.; et al. Association between Routine Laboratory Parameters and the Severity and Progression of Systemic Sclerosis. J. Clin. Med. 2022, 11, 5087. [Google Scholar] [CrossRef]
- Li, H.; Zhang, X.; Yu, L.; Shang, J.; Fan, J.; Feng, X.; Zhang, R.; Ren, J.; Guo, Q.; Duan, X. Comparing clinical characteristics of systemic sclerosis with or without interstitial lung disease: A cross-sectional study from a single center of the Chinese Rheumatism Data Center. Front. Med. 2022, 9, 1061738. [Google Scholar] [CrossRef]
- Zhu, L.; Fu, X.; Chen, X.; Han, X.; Dong, P. M2 macrophages induce EMT through the TGF-β/Smad2 signaling pathway. Cell Biol. Int. 2017, 41, 960–968. [Google Scholar] [CrossRef]
- Saraiva, M.; Vieira, P.; O’Garra, A. Biology and therapeutic potential of interleukin-10. J. Exp. Med. 2020, 217, e20190418. [Google Scholar] [CrossRef] [PubMed]
- Steen, E.H.; Wang, X.; Balaji, S.; Butte, M.J.; Bollyky, P.L.; Keswani, S.G. The Role of the Anti-Inflammatory Cytokine Interleukin-10 in Tissue Fibrosis. Adv. Wound Care 2020, 9, 184–198. [Google Scholar] [CrossRef] [PubMed]
- Laurent, P.; Allard, B.; Manicki, P.; Jolivel, V.; Levionnois, E.; Jeljeli, M.; Henrot, P.; Izotte, J.; Leleu, D.; Groppi, A.; et al. TGFβ promotes low IL10-producing ILC2 with profibrotic ability involved in skin fibrosis in systemic sclerosis. Ann. Rheum. Dis. 2021, 80, 1594–1603. [Google Scholar] [CrossRef]
- Xing, X.; Li, A.; Tan, H.; Zhou, Y. IFN-γ+ IL-17+ Th17 cells regulate fibrosis through secreting IL-21 in systemic scleroderma. J. Cell. Mol. Med. 2020, 24, 13600–13608. [Google Scholar] [CrossRef] [PubMed]
- Mora, V.P.; Loaiza, R.A.; Soto, J.A.; Bohmwald, K.; Kalergis, A.M. Involvement of trained immunity during autoimmune responses. J. Autoimmun. 2023, 137, 102956. [Google Scholar] [CrossRef]
- Nica, V.; Popp, R.A.; Crișan, T.O.; Joosten, L.A.B. The future clinical implications of trained immunity. Expert Rev. Clin. Immunol. 2022, 18, 1125–1134. [Google Scholar] [CrossRef]
- Crișan, T.O.; Netea, M.G.; Joosten, L.A.B. Innate immune memory: Implications for host responses to damage-associated molecular patterns. Eur. J. Immunol. 2016, 46, 817–828. [Google Scholar] [CrossRef]
- Ochando, J.; Mulder, W.J.M.; Madsen, J.C.; Netea, M.G.; Duivenvoorden, R. Trained immunity—Basic concepts and contributions to immunopathology. Nat. Rev. Nephrol. 2023, 19, 23–37. [Google Scholar] [CrossRef]
- Badii, M.; Gaal, O.; Popp, R.A.; Crișan, T.O.; Joosten, L.A.B. Trained immunity and inflammation in rheumatic diseases. Joint Bone Spine 2022, 89, 105364. [Google Scholar] [CrossRef]
- Jeljeli, M.; Riccio, L.G.C.; Doridot, L.; Chêne, C.; Nicco, C.; Chouzenoux, S.; Deletang, Q.; Allanore, Y.; Kavian, N.; Batteux, F. Trained immunity modulates inflammation-induced fibrosis. Nat. Commun. 2019, 10, 5670. [Google Scholar] [CrossRef]
- Kamada, R.; Yang, W.; Zhang, Y.; Patel, M.C.; Yang, Y.; Ouda, R.; Dey, A.; Wakabayashi, Y.; Sakaguchi, K.; Fujita, T.; et al. Interferon stimulation creates chromatin marks and establishes transcriptional memory. Proc. Natl. Acad. Sci. USA 2018, 115, E9162–E9171. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.-C.; Quintin, J.; Cramer, R.A.; Shepardson, K.M.; Saeed, S.; Kumar, V.; Giamarellos-Bourboulis, E.J.; Martens, J.H.A.; Rao, N.A.; Aghajanirefah, A.; et al. mTOR- and HIF-1α-mediated aerobic glycolysis as metabolic basis for trained immunity. Science 2014, 345, 1250684. [Google Scholar] [CrossRef] [PubMed]
- Arts, R.J.W.; Carvalho, A.; La Rocca, C.; Palma, C.; Rodrigues, F.; Silvestre, R.; Kleinnijenhuis, J.; Lachmandas, E.; Gonçalves, L.G.; Belinha, A.; et al. Immunometabolic Pathways in BCG-Induced Trained Immunity. Cell Rep. 2016, 17, 2562–2571. [Google Scholar] [CrossRef]
- Moreno-Moral, A.; Bagnati, M.; Koturan, S.; Ko, J.-H.; Fonseca, C.; Harmston, N.; Game, L.; Martin, J.; Ong, V.; Abraham, D.J.; et al. Changes in macrophage transcriptome associate with systemic sclerosis and mediate GSDMA contribution to disease risk. Ann. Rheum. Dis. 2018, 77, 596–601. [Google Scholar] [CrossRef] [PubMed]
- Gur, C.; Wang, S.-Y.; Sheban, F.; Zada, M.; Li, B.; Kharouf, F.; Peleg, H.; Aamar, S.; Yalin, A.; Kirschenbaum, D.; et al. LGR5 expressing skin fibroblasts define a major cellular hub perturbed in scleroderma. Cell 2022, 185, 1373–1388.e20. [Google Scholar] [CrossRef]
- Galiè, N.; Humbert, M.; Vachiery, J.-L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Vonk Noordegraaf, A.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Kardiol. Pol. 2015, 73, 1127–1206. [Google Scholar] [CrossRef]
- Hudson, M.; Ghossein, C.; Steen, V. Scleroderma renal crisis. Presse Medicale 2021, 50, 104063. Available online: https://pubmed.ncbi.nlm.nih.gov/33548376/ (accessed on 12 September 2023). [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | N | SSc, N = 18 1 |
|---|---|---|
| Age (years) | 18 | 50 (45, 56) |
| Gender | 18 | |
| female | 18 (100%) | |
| Disease duration (years) | 18 | 4.0 (2.2, 9.2) |
| Disease duration (early ≤3 years; late 3 years) | 18 | |
| early | 7 (39%) | |
| late | 11 (61%) | |
| SSc subtype | 18 | |
| diffuse cutaneous | 9 (50%) | |
| limited cutaneous | 8 (44%) | |
| sine scleroderma | 1 (6%) | |
| Esophagitis | 15 | 6 (40%) |
| unknown | 3 | |
| ILD | 18 | 11 (61%) |
| Arrhythmias requiring therapy | 18 | 1 (5.6%) |
| Arthritis | 18 | 1 (5.6%) |
| Digital ulcers | 18 | |
| current | 5 (28%) | |
| never | 8 (44%) | |
| previous | 5 (28%) | |
| Calcinosis | 18 | 4 (22%) |
| Telangiectasia | 18 | 8 (44%) |
| mRSS | 16 | 5.5 (4.0, 8.8) |
| unknown | 2 | |
| ANA | 18 | |
| negative | 1 (6%) | |
| positive | 17 (94%) | |
| Anti-Scl-70 | 18 | |
| negative | 7 (39%) | |
| positive | 11 (61%) | |
| Anti-centromere | 6 | |
| negative | 1 (17%) | |
| positive | 5 (83%) | |
| unknown | 12 | |
| Rheumatoid factor | 17 | |
| negative | 12 (70%) | |
| positive | 5 (30%) | |
| unknown | 1 | |
| CRP (mg/dL) | 18 | 0.19 (0.14, 0.33) |
| ESR (mm/h) | 18 | 9 (6,15) |
| Uric acid (mg/dL) | 17 | 4 (3.28–5.1) |
| unknown | 1 | |
| FVC (% predicted) | 8 | 93 (88–96.5) |
| unknown | 10 | |
| DLCO (% predicted) | 6 | 66 (66–74) |
| unknown | 12 | |
| LVEF (%) | 13 | 62 (59–65) |
| unknown | 5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szabo, I.; Badii, M.; Gaál, I.O.; Szabo, R.; Popp, R.A.; Joosten, L.A.B.; Crişan, T.O.; Rednic, S. Enhanced Innate and Acquired Immune Responses in Systemic Sclerosis Primary Peripheral Blood Mononuclear Cells (PBMCs). Int. J. Mol. Sci. 2023, 24, 14438. https://doi.org/10.3390/ijms241914438
Szabo I, Badii M, Gaál IO, Szabo R, Popp RA, Joosten LAB, Crişan TO, Rednic S. Enhanced Innate and Acquired Immune Responses in Systemic Sclerosis Primary Peripheral Blood Mononuclear Cells (PBMCs). International Journal of Molecular Sciences. 2023; 24(19):14438. https://doi.org/10.3390/ijms241914438
Chicago/Turabian StyleSzabo, Iulia, Medeea Badii, Ildikó O. Gaál, Robert Szabo, Radu A. Popp, Leo A. B. Joosten, Tania O. Crişan, and Simona Rednic. 2023. "Enhanced Innate and Acquired Immune Responses in Systemic Sclerosis Primary Peripheral Blood Mononuclear Cells (PBMCs)" International Journal of Molecular Sciences 24, no. 19: 14438. https://doi.org/10.3390/ijms241914438
APA StyleSzabo, I., Badii, M., Gaál, I. O., Szabo, R., Popp, R. A., Joosten, L. A. B., Crişan, T. O., & Rednic, S. (2023). Enhanced Innate and Acquired Immune Responses in Systemic Sclerosis Primary Peripheral Blood Mononuclear Cells (PBMCs). International Journal of Molecular Sciences, 24(19), 14438. https://doi.org/10.3390/ijms241914438