

Objective Physical Function in the Alzheimer’s Disease Continuum: Association with Cerebrospinal Fluid Biomarkers in the ALBION Study

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Results
2.1. Baseline Demographic and Clinical Characteristics
2.2. CSF Biomarkers and Physical Function Parameters in Different Groups
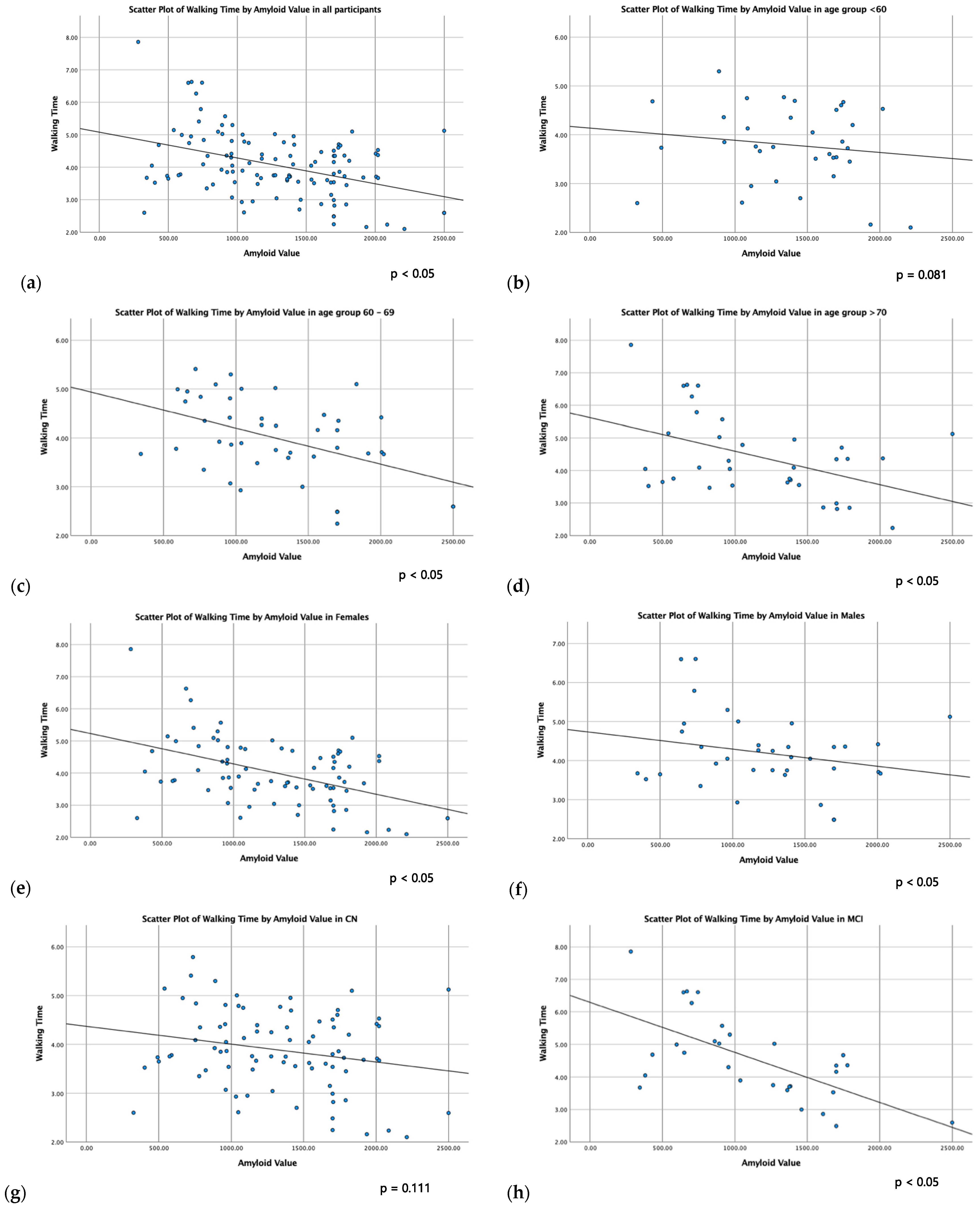
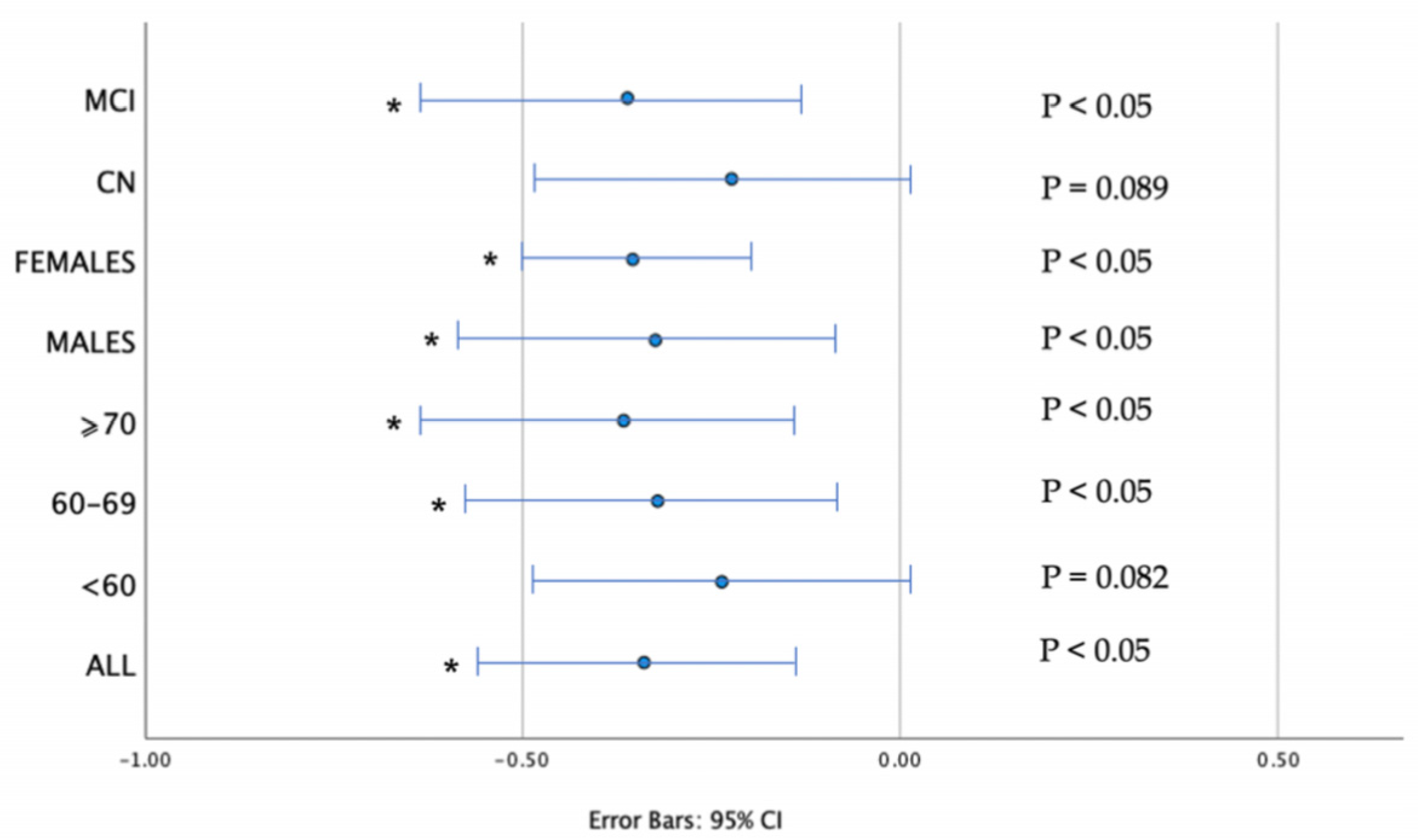
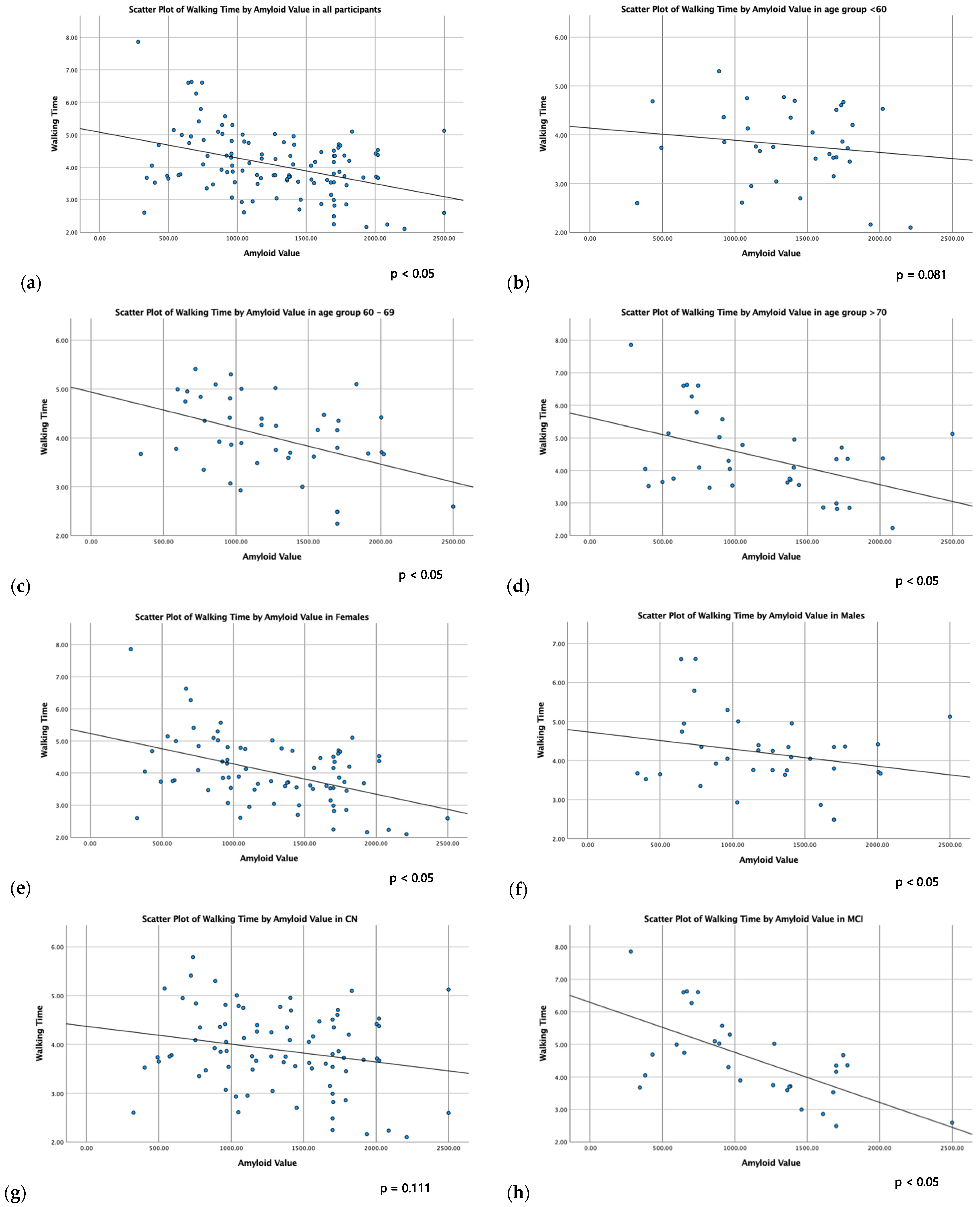
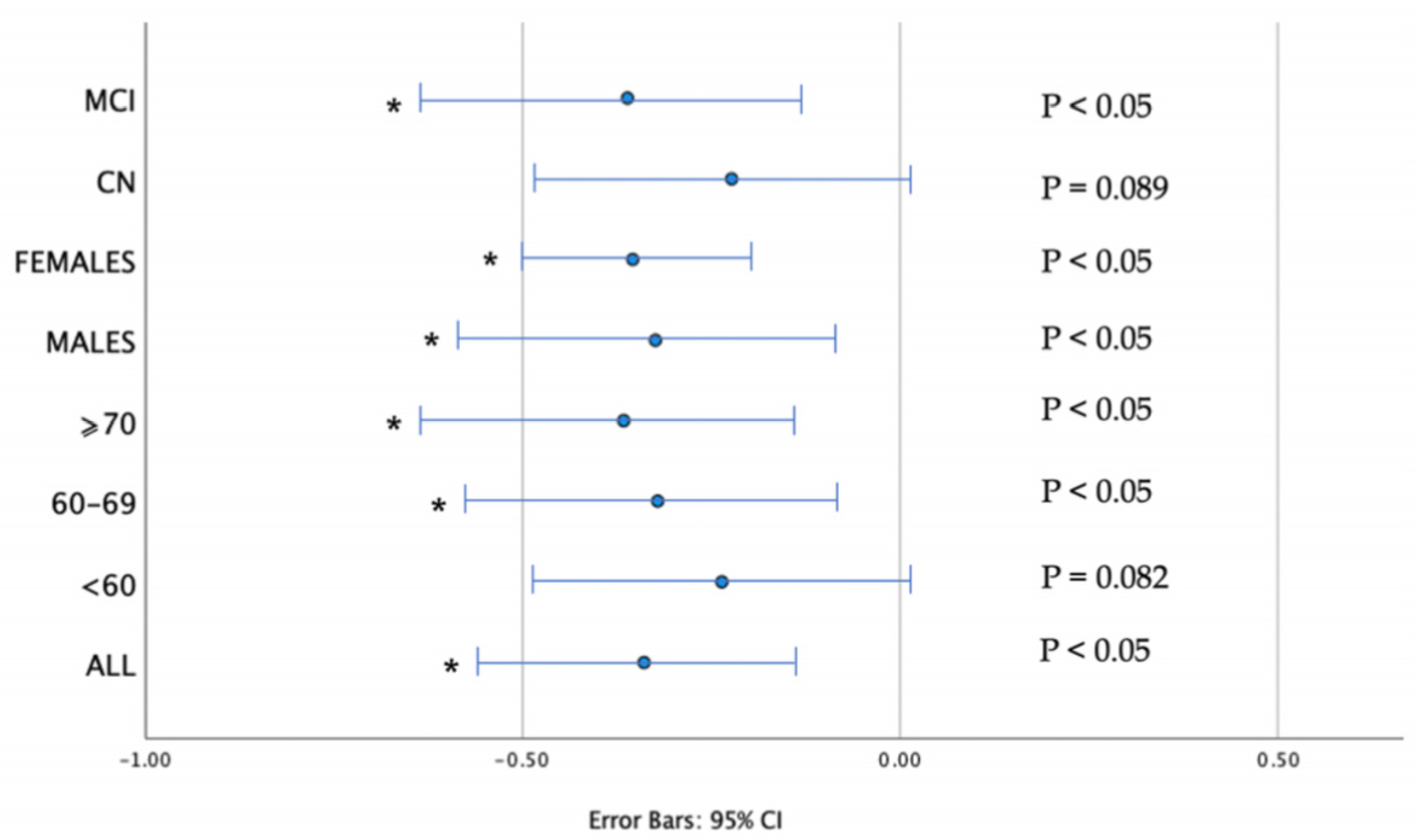
2.3. CSF Biomarkers in Relation to Physical Function Parameters
3. Discussion
4. Materials and Methods
4.1. Participants and Study Design
4.2. Diagnostic Procedures
4.2.1. Neurological and Neuropsychological Evaluation
4.2.2. Cerebrospinal Fluid (CSF) Analysis
4.2.3. Blood Analysis—ApoE Genotyping
4.2.4. Physical Function Parameters Assessment
4.3. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jack, C.R., Jr.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimer’s Dement. 2018, 14, 535–562. [Google Scholar] [CrossRef] [PubMed]
- Tahami Monfared, A.A.; Fu, S.; Hummel, N.; Qi, L.; Chandak, A.; Zhang, R.; Zhang, Q. Estimating Transition Probabilities Across the Alzheimer’s Disease Continuum Using a Nationally Representative Real-World Database in the United States. Neurol. Ther. 2023, 12, 1235–1255. [Google Scholar] [CrossRef] [PubMed]
- Jack, C.R., Jr.; Knopman, D.S.; Jagust, W.J.; Shaw, L.M.; Aisen, P.S.; Weiner, M.W.; Petersen, R.C.; Trojanowski, J.Q. Hypothetical model of dynamic biomarkers of the Alzheimer’s pathological cascade. Lancet Neurol. 2010, 9, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Donohue, M.C.; Sperling, R.A.; Petersen, R.; Sun, C.K.; Weiner, M.W.; Aisen, P.S. Alzheimer’s Disease Neuroimaging Initiative. Association between elevated brain amyloid and subsequent cognitive decline among cognitively normal persons. JAMA 2017, 317, 2305–2316. [Google Scholar] [CrossRef]
- Villemagne, V.L.; Burnham, S.; Bourgeat, P.; Brown, B.; Ellis, K.A.; Salvado, O.; Szoeke, C.; Macaulay, S.L.; Martins, R.; Maruff, P.; et al. Australian Imaging Biomarkers and Lifestyle (AIBL) Research Group. Amyloid β deposition, neurodegeneration, and cognitive decline in sporadic Alzheimer’s disease: A prospective cohort study. Lancet Neurol. 2013, 12, 357–367. [Google Scholar] [CrossRef]
- Bejanin, A.; Schonhaut, D.R.; La Joie, R.; Kramer, J.H.; Baker, S.L.; Sosa, N.; Ayakta, N.; Cantwell, A.; Janabi, M.; Lauriola, M.; et al. Tau pathology and neurodegeneration contribute to cognitive impairment in Alzheimer’s disease. Brain 2017, 140, 3286–3300. [Google Scholar] [CrossRef]
- Harman, D. Alzheimer’s disease pathogenesis: Role of aging. Ann. N. Y. Acad. Sci. 2006, 1067, 454–460. [Google Scholar] [CrossRef]
- Carvalho, A.; Rea, I.M.; Parimon, T.; Cusack, B.J. Physical activity and cognitive function in individuals over 60 years of age: A systematic review. Clin. Interv. Aging. 2014, 9, 661–682. [Google Scholar] [CrossRef]
- Boyle, P.A.; Buchman, A.S.; Wilson, R.S.; Leurgans, S.E.; Bennett, D.A. Physical frailty is associated with incident mild cognitive impairment in community-based older persons. J. Am. Geriatr. Soc. 2010, 58, 248–255. [Google Scholar] [CrossRef]
- Choi, J.; Park, J.; Lee, B.I.; Shin, K.J.; Yoo, S.; Kim, H.; Jang, W.; Kim, J.S.; Youn, J.; Oh, E. The Correlation between Cognition Screening Scores and Gait Status from Three-Dimensional Gait Analysis. J. Clin. Neurol. 2019, 15, 152–158. [Google Scholar] [CrossRef]
- Filardi, M.; Barone, R.; Bramato, G.; Nigro, S.; Tafuri, B.; Frisullo, M.E.; Zecca, C.; Tortelli, R.; Logroscino, G. The Relationship Between Muscle Strength and Cognitive Performance Across Alzheimer’s Disease Clinical Continuum. Front. Neurol. 2022, 13, 833087. [Google Scholar] [CrossRef]
- Clouston, S.A.; Brewster, P.; Kuh, D.; Richards, M.; Cooper, R.; Hardy, R.; Rubin, M.S.; Hofer, S.M. The dynamic relationship between physical function and cognition in longitudinal aging cohorts. Epidemiol. Rev. 2013, 35, 33–50. [Google Scholar] [CrossRef]
- De la Rosa, A.; Olaso-Gonzalez, G.; Arc-Chagnaud, C.; Millan, F.; Salvador-Pascual, A.; García-Lucerga, C.; Blasco-Lafarga, C.; Garcia-Dominguez, E.; Carretero, A.; Correas, A.G.; et al. Physical exercise in the prevention and treatment of Alzheimer’s disease. J. Sport. Health Sci. 2020, 9, 394–404. [Google Scholar] [CrossRef] [PubMed]
- Nuzum, H.; Stickel, A.; Corona, M.; Zeller, M.; Melrose, R.J.; Wilkins, S.S. Potential Benefits of Physical Activity in MCI and Dementia. Behav. Neurol. 2020, 2020, 7807856. [Google Scholar] [CrossRef]
- Buchman, A.S.; Yu, L.; Wilson, R.S.; Schneider, J.A.; Bennett, D.A. Association of brain pathology with the progression of frailty in older adults. Neurology 2013, 80, 2055–2061. [Google Scholar] [CrossRef]
- Fujisawa, C.; Umegaki, H.; Okamoto, K.; Nakashima, H.; Kuzuya, M.; Toba, K.; Sakurai, T. Physical Function Differences Between the Stages from Normal Cognition to Moderate Alzheimer Disease. J. Am. Med. Dir. Assoc. 2017, 18, e9–e368. [Google Scholar] [CrossRef]
- Cedervall, Y.; Halvorsen, K.; Aberg, A.C. A longitudinal study of gait function and characteristics of gait disturbance in individuals with Alzheimer’s disease. Gait Posture 2014, 39, 1022–1027. [Google Scholar] [CrossRef] [PubMed]
- Hausdorff, J.M.; Buchman, A.S. What links gait speed and MCI with dementia? A fresh look at the association between motor and cognitive function. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 409–411. [Google Scholar] [CrossRef] [PubMed]
- Su, H.; Sun, X.; Li, F.; Guo, Q. Association between handgrip strength and cognition in a Chinese population with Alzheimer’s disease and mild cognitive impairment. BMC Geriatr. 2021, 21, 459. [Google Scholar] [CrossRef] [PubMed]
- Song, R.; Fan, X.; Seo, J. Physical and cognitive function to explain the quality of life among older adults with cognitive impairment: Exploring cognitive function as a mediator. BMC Psychol. 2023, 11, 51. [Google Scholar] [CrossRef]
- Tangen, G.G.; Sverdrup, K.; Taraldsen, K.; Persson, K.; Engedal, K.; Bekkhus-Wetterberg, P.; Knapskog, A.B. Mobility and associations with levels of cerebrospinal fluid amyloid β and tau in a memory clinic cohort. Front. Aging. Neurosci. 2023, 15, 1101306. [Google Scholar] [CrossRef] [PubMed]
- Muurling, M.; Rhodius-Meester, H.F.M.; Pärkkä, J.; van Gils, M.; Frederiksen, K.S.; Bruun, M.; Hasselbalch, S.G.; Soininen, H.; Herukka, S.K.; Merjae, H.; et al. Gait Disturbances are Associated with Increased Cognitive Impairment and Cerebrospinal Fluid Tau Levels in a Memory Clinic Cohort. J. Alzheimers Dis. 2020, 76, 1061–1070. [Google Scholar] [CrossRef] [PubMed]
- Knapstad, M.K.; Steihaug, O.M.; Aaslund, M.K.; Nakling, A.; Naterstad, I.F.; Fladby, T.; Aarsland, D.; Giil, L.M. Reduced Walking Speed in Subjective and Mild Cognitive Impairment: A Cross-Sectional Study. J. Geriatr. Phys. Ther. 2019, 42, E122–E128. [Google Scholar] [CrossRef] [PubMed]
- Koychev, I.; Galna, B.; Zetterberg, H.; Lawson, J.; Zamboni, G.; Ridha, B.H.; Rowe, J.B.; Thomas, A.; Howard, R.; Malhotra, P.; et al. Aβ42/Aβ40 and Aβ42/Aβ38 Ratios Are Associated with Measures of Gait Variability and Activities of Daily Living in Mild Alzheimer’s Disease: A Pilot Study. J. Alzheimers Dis. 2018, 65, 1377–1383. [Google Scholar] [CrossRef]
- Nadkarni, N.K.; Perera, S.; Snitz, B.E.; Mathis, C.A.; Price, J.; Williamson, J.D.; DeKosky, S.T.; Klunk, W.E.; Lopez, O.L. Association of Brain Amyloid-β with Slow Gait in Elderly Individuals without Dementia: Influence of Cognition and Apolipoprotein E ε4 Genotype. JAMA Neurol. 2017, 74, 82–90. [Google Scholar] [CrossRef]
- Wennberg, A.M.V.; Savica, R.; Hagen, C.E.; Roberts, R.O.; Knopman, D.S.; Hollman, J.H.; Vemuri, P.; Jack, C.R., Jr.; Petersen, R.C.; Mielke, M.M. Cerebral Amyloid Deposition Is Associated with Gait Parameters in the Mayo Clinic Study of Aging. J. Am. Geriatr. Soc. 2017, 65, 792–799. [Google Scholar] [CrossRef] [PubMed]
- Yoon, D.H.; Lee, J.Y.; Shin, S.A.; Kim, Y.K.; Song, W. Physical Frailty and Amyloid-β Deposits in the Brains of Older Adults with Cognitive Frailty. J. Clin. Med. 2018, 7, 169. [Google Scholar] [CrossRef]
- Dao, E.; Hsiung, G.R.; Sossi, V.; Tam, R.; Shahinfard, E.; Nicklin, E.; Al Keridy, W.; Liu-Ambrose, T. Cerebral Amyloid-β Deposition Is Associated with Impaired Gait Speed and Lower Extremity Function. J. Alzheimers Dis. 2019, 71, S41–S49. [Google Scholar] [CrossRef]
- Tian, Q.; Bair, W.N.; Resnick, S.M.; Bilgel, M.; Wong, D.F.; Studenski, S.A. β-amyloid deposition is associated with gait variability in usual aging. Gait Posture 2018, 61, 346–352. [Google Scholar] [CrossRef]
- Tian, Q.; Resnick, S.M.; Bilgel, M.; Wong, D.F.; Ferrucci, L.; Studenski, S.A. β-Amyloid Burden Predicts Lower Extremity Performance Decline in Cognitively Unimpaired Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 716–723. [Google Scholar] [CrossRef]
- Wennberg, A.M.V.; Lesnick, T.G.; Schwarz, C.G.; Savica, R.; Hagen, C.E.; Roberts, R.O.; Knopman, D.S.; Hollman, J.H.; Vemuri, P.; Jack, C.R., Jr.; et al. Longitudinal Association Between Brain Amyloid-Beta and Gait in the Mayo Clinic Study of Aging. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 1244–1250. [Google Scholar] [CrossRef]
- Barnett, J.H.; Hachinski, V.; Blackwell, A.D. Cognitive health begins at conception: Addressing dementia as a lifelong and preventable condition. BMC Med. 2013, 11, 246. [Google Scholar] [CrossRef] [PubMed]
- Figgins, E.; Pieruccini-Faria, F.; Speechley, M.; Montero-Odasso, M. Potentially modifiable risk factors for slow gait in community-dwelling older adults: A systematic review. Ageing Res. Rev. 2021, 66, 101253. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhou, W.; Cassidy, R.M.; Su, H.; Su, Y.; Zhang, X.; Alzheimer’s Disease Neuroimaging Initiative. Risk factors for amyloid positivity in older people reporting significant memory concern. Compr. Psychiatry 2018, 80, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Justin, B.N.; Turek, M.; Hakim, A.M. Heart disease as a risk factor for dementia. Clin. Epidemiol. 2013, 5, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Gottesman, R.F.; Schneider, A.L.; Zhou, Y.; Coresh, J.; Green, E.; Gupta, N.; Knopman, D.S.; Mintz, A.; Rahmim, A.; Sharrett, A.R.; et al. Association Between Midlife Vascular Risk Factors and Estimated Brain Amyloid Deposition. JAMA 2017, 317, 1443–1450. [Google Scholar] [CrossRef]
- Zlokovic, B.V. Cerebrovascular effects of apolipoprotein E: Implications for Alzheimer disease. JAMA Neurol. 2013, 70, 440–444. [Google Scholar] [CrossRef]
- Takakusaki, K. Functional Neuroanatomy for Posture and Gait Control. J. Mov. Disord. 2017, 10, 1–17. [Google Scholar] [CrossRef]
- Del Campo, N.; Payoux, P.; Djilali, A.; Delrieu, J.; Hoogendijk, E.O.; Rolland, Y.; Cesari, M.; Weiner, M.W.; Andrieu, S.; Vellas, B.; et al. Relationship of regional brain β-amyloid to gait speed. Neurology 2016, 86, 36–43. [Google Scholar] [CrossRef]
- Hedden, T.; Van Dijk, K.R.; Becker, J.A.; Mehta, A.; Sperling, R.A.; Johnson, K.A.; Buckner, R.L. Disruption of functional connectivity in clinically normal older adults harboring amyloid burden. J. Neurosci. 2009, 29, 12686–12694. [Google Scholar] [CrossRef]
- Legdeur, N.; Badissi, M.; Yaqub, M.; Beker, N.; Sudre, C.H.; Ten Kate, M.; Gordon, M.F.; Novak, G.; Barkhof, F.; van Berckel, B.N.M.; et al. What Determines Cognitive Functioning in the Oldest-Old? The EMIF-AD 90+ Study. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 76, 1499–1511. [Google Scholar] [CrossRef]
- Lo, O.Y.; Manor, B. Measuring Gait to Monitor Cognitive Function in Older Adults: An Important Step in the Right Direction. Neurology 2023, 101, 10–11. [Google Scholar] [CrossRef]
- Doecke, J.D.; Ward, L.; Burnham, S.C.; Villemagne, V.L.; Li, Q.X.; Collins, S.; Fowler, C.J.; Manuilova, E.; Widmann, M.; Rainey-Smith, S.R.; et al. Elecsys CSF biomarker immunoassays demonstrate concordance with amyloid-PET imaging. Alzheimers Res. Ther. 2020, 12, 36. [Google Scholar] [CrossRef]
- Scarmeas, N.; Daskalaki, A.; Kalligerou, F.; Ntanasi, E.; Mamalaki, E.; Gargalionis, A.N.; Patas, K.; Chatzipanagiotou, S.; Yannakoulia, M.; Constantinides, V.C. Initial Data and a Clinical Diagnosis Transition for the Aiginition Longitudinal Biomarker Investigation of Neurodegeneration (ALBION) Study. Medicina 2022, 58, 1179. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C. Mild cognitive impairment as a diagnostic entity. J. Intern. Med. 2004, 256, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Kalligerou, F.; Ntanasi, E.; Voskou, P.; Velonakis, G.; Karavasilis, E.; Mamalaki, E.; Kyrozis, A.; Sigala, E.; Economou, N.T.; Patas, K.; et al. Aiginition Longitudinal Biomarker Investigation of Neurodegeneration (ALBION): Study design, cohort description, and preliminary data. Postgrad. Med. 2019, 131, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”. A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Mioshi, E.; Dawson, K.; Mitchell, J.; Arnold, R.; Hodges, J.R. The Addenbrooke’s Cognitive Examination Revised (ACE-R): A brief cognitive test battery for dementia screening. Int. J. Geriatr. Psychiatry 2006, 21, 1078–1085. [Google Scholar] [CrossRef]
- Petersen, R.C.; Doody, R.; Kurz, A.; Mohs, R.C.; Morris, J.C.; Rabins, P.V.; Ritchie, K.; Rossor, M.; Thal, L.; Winblad, B. Current concepts in mild cognitive impairment. Arch. Neurol. 2001, 58, 1985–1992. [Google Scholar] [CrossRef]
- Teunissen, C.E.; Tumani, H.; Engelborghs, S.; Mollenhauer, B. Biobanking of CSF: International standardization to optimize biomarker development. Clin. Biochem. 2014, 47, 288–292. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| All (n = 163) | CN 1 (n = 112) | MCI 2 (n = 51) | p-Value | |
|---|---|---|---|---|
| Sex, female (%) | 109 (66.9) | 76 (67.9) | 36 (70.6) | 0.722 |
| Age, y, mean ± SD 3 | 64.3 ± 9.2 | 62.8 ± 9.2 | 67.6 ± 8.2 | 0.002 |
| Education, y 4, Mean ± SD | 13.3 ± 3.8 | 13.8 ± 3.7 | 12.3 ± 4.1 | 0.016 |
| Family History of Dementia, n (%) | 75 (46.0) | 53 (47.3) | 22 (43.1) | 0.734 |
| MMSE 5, Mean ± SD | 28.1 ± 1.8 | 28.9 ± 1.2 | 26.4 ± 1.8 | <0.001 |
| ACE 6 score, Mean ± SD | 90.0 ± 7.7 | 93.6 ± 4.5 | 81.9 ± 7.1 | <0.001 |
| ApoE4 carrier, positive (%) | 44 (28.0) n = 157 | 22 (20.6) n = 107 | 22 (44.0) n = 50 | 0.004 |
| Walking Time, s 7, Mean ± SD | 4.73 ± 1.76 (n = 114) | 4.33 ± 1.04 (n = 81) | 5.82 ± 2.65 (n = 33) | <0.001 |
| Grip Strength, kg 8, Mean ± SD | 25.7 ± 8.9 (n = 143) | 26.8 ± 9.3 (n = 98) | 23.3 ± 7.8 (n = 45) | 0.032 |
| CSF Aβ42, Mean ± SD | 1161.6 ± 529.4 | 1240.0 ± 508.5 | 989.2 ± 538.3 | 0.005 |
| CSF Tau, Mean ± SD | 230.4 ± 172.5 | 218.0 ± 196.9 | 257.9 ± 96.5 | 0.171 |
| CSF PhTau, Mean ± SD | 19.2 ± 9.9 | 17.2 ± 8.9 | 23.6 ± 10.7 | <0.001 |
| Age Groups | Sex Groups | ApoE4 Groups | ||||
|---|---|---|---|---|---|---|
| <65 | ≥65 | Males | Females | Carriers | Non-Carriers | |
| N = 163 | 78 | 85 | 54 | 109 | 44 | 113 |
| CSF Aβ42, mean ± SD 1, p-Value | 1278.0 ± 478.6 | 1054.8 ± 553.5 | 1122.5 ± 536.3 | 1181.0 ± 527.3 | 882.3 ± 428.8 | 1276.8 ± 524.1 |
| 0.007 | 0.508 | <0.001 | ||||
| CSF Tau, mean ± SD, p-Value | 193.9 ± 96.2 | 264.0 ± 215.8 | 235.3 ± 99.3 | 228.0 ± 199.5 | 324.2 ± 281.2 | 196.2 ± 88.4 |
| 0.009 | 0.801 | <0.001 | ||||
| CSF PhTau, mean ± SD, p-Value | 16.3 ± 9.4 | 21.9 ± 9.7 | 21.0 ± 9.1 | 18.3 ± 10.3 | 26.0 ± 11.9 | 16.7 ± 7.9 |
| <0.001 | 0.801 | <0.001 | ||||
| N = 114 | 56 | 58 | 36 | 78 | 25 | 83 |
| Walking Time, s 2, mean ± SD, p-Value | 4.53 ± 2.13 | 4.93 ± 1.29 | 4.25 ± 0.90 | 4.96 ± 2.00 | 4.80 ± 1.25 | 4.76 ± 1.91 |
| 0.220 | 0.045 | 0.884 | ||||
| N = 143 | 69 | 74 | 43 | 100 | 38 | 99 |
| Grip Strength, kg 3, mean ± SD, p-Value | 26.0 ± 9.0 | 25.4 ± 8.9 | 35.8 ± 8.2 | 21.4 ± 4.7 | 22.9 ± 8.2 | 26.6 ± 9.0 |
| 0.348 | <0.001 | 0.034 | ||||
| Walking Time | All | Age Groups | Age Groups | Sex Groups | Clinical Groups | |||||
| <65 | ≥65 | <60 | 60–69 | ≥70 | Males | Females | CN 1 | MCI 2 | ||
| N= | 114 | 56 | 58 | 37 | 44 | 36 | 36 | 78 | 81 | 33 |
| CSF Aβ42 rs 3 (p) | −0.288 (<0.05) | −0.241 (<0.05) | −0.318 (<0.05) | −0.183 (0.081) | −0.261 (<0.05) | −0.312 (<0.05) | −0.281 (<0.05) | −0.295 (<0.05) | −0.151 (0.111) | −0.343 (<0.05) |
| CSF Tau rs (p) | 0.111 (0.091) | 0.039 (0.773) | 0.077 (0.565) | 0.052 (0.724) | 0.031 (0.818) | 0.066 (0.663) | 0.061 (0.663) | 0.148 (0.124) | 0.029 (0.764) | 0.274 (0.052) |
| CSF PhTau rs (p) | 0.115 (0.143) | 0.063 (0.643) | 0.017 (0.901) | 0.015 (0.836) | 0.007 (0.957) | 0.087 (0.532) | 0.119 (0.390) | 0.127 (0.190) | 0.019 (0.845) | 0.215 (0.130) |
| Grip Strength | All | Age Groups | Age Groups | Sex Groups | Clinical Groups | |||||
| <65 | ≥65 | <60 | 60–69 | ≥70 | Males | Females | CN | MCI | ||
| N= | 143 | 69 | 74 | 46 | 55 | 57 | 43 | 100 | 98 | 45 |
| CSF Aβ42 rs (p) | 0.044 (0.597) | 0.062 (0.613) | 0.049 (0.681) | 0.020 (0.989) | 0.051 (0.716) | 0.061 (0.687) | 0.037 (0.815) | 0.051 (0.612) | 0.128 (0.180) | 0.079 (0.434) |
| CSF Tau rs (p) | −0.060 (0.472) | −0.051 (0.677) | −0.223 (0.056) | −0.048 (0.756) | −0.060 (0.666) | −0.123 (0.416) | −0.362 (<0.05) | −0.058 (0.566) | −0.085 (0.371) | −0.053 (0.605) |
| CSF PhTau rs (p) | −0.103 (0.221) | −0.088 (0.471) | −0.180 (0.127) | −0.03 (0.987) | −0.09 (0.948) | −0.08 (0.599) | −0.432 (<0.05) | −0.116 (0.249) | −0.118 (0.217) | −0.116 (0.254) |
| Walking Time | All | Age Groups | Age Groups | Sex Groups | Clinical Groups | |||||
| <65 | ≥65 | <60 | 60–69 | ≥70 | Males | Females | CN 1 | MCI 2 | ||
| N= | 114 | 56 | 58 | 37 | 44 | 36 | 36 | 78 | 81 | 33 |
| CSF Aβ42 b 3 (p) | −0.346 (<0.05) | −0.332 (<0.05) | −0.365 (<0.05) | −0.236 (0.082) | −0.323 (<0.05) | −0.360 (<0.05) | −0.342 (<0.05) | −0.365 (<0.05) | −0.223 (0.089) | −0.387 (<0.05) |
| CSF Tau b (p) | 0.031 (0.759) | 0.012 (0.942) | 0.015 (0.852)) | 0.065 (0.757) | 0.143 (0.371) | 0.067 (0.775) | 0.061 (0.663) | 0.054 (0.668) | 0.049 (0.664) | 0.163 (0.253) |
| CSF PhTau b (p) | 0.031 (0.787) | 0.047 (0.778) | 0.073 (0.633 | 0.099 (0.623) | 0.074 (0.638) | 0.089 (0.720) | 0.119 (0.390) | 0.043 (0.769) | 0.028 (0.746) | 0.118 (0.331) |
| Grip Strength | All | Age Groups | Age Groups | Sex Groups | Clinical Groups | |||||
| <65 | ≥65 | <60 | 60–69 | ≥70 | Males | Females | CN | MCI | ||
| N= | 143 | 69 | 74 | 46 | 55 | 57 | 43 | 100 | 98 | 45 |
| CSF Aβ42 b (p) | 0.128 (0.180) | 0.068 (0.368) | 0.70 (0.606) | 0.144 (0.334) | 0.157 (0.250) | 0.075 (0.561) | 0.033 (0.813) | 0.062 (0.527) | 0.155 (0.107) | 0.203 (0.152) |
| CSF Tau b (p) | −0.011 (0.853) | −0.031 (0.733) | −0.055 (0.670) | −0.130 (0.364) | −0.044 (0.582) | −0.253 (0.206) | −0.246 (0.125) | −0.089 (0.396) | −0.013 (0.841) | −0.016 (0.899) |
| CSF PhTau b (p) | −0.073 (0.246) | −0.018 (0.84) | −0.128 (0.132) | −0.113 (0.427) | −0.053 (0.509) | −0.130 (0.296) | −0.274 (0.098) | −0.05 (0.968) | −0.115 (0.088) | −0.070 (0.572) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sampatakakis, S.N.; Mamalaki, E.; Ntanasi, E.; Kalligerou, F.; Liampas, I.; Yannakoulia, M.; Gargalionis, A.N.; Scarmeas, N. Objective Physical Function in the Alzheimer’s Disease Continuum: Association with Cerebrospinal Fluid Biomarkers in the ALBION Study. Int. J. Mol. Sci. 2023, 24, 14079. https://doi.org/10.3390/ijms241814079
Sampatakakis SN, Mamalaki E, Ntanasi E, Kalligerou F, Liampas I, Yannakoulia M, Gargalionis AN, Scarmeas N. Objective Physical Function in the Alzheimer’s Disease Continuum: Association with Cerebrospinal Fluid Biomarkers in the ALBION Study. International Journal of Molecular Sciences. 2023; 24(18):14079. https://doi.org/10.3390/ijms241814079
Chicago/Turabian StyleSampatakakis, Stefanos N., Eirini Mamalaki, Eva Ntanasi, Faidra Kalligerou, Ioannis Liampas, Mary Yannakoulia, Antonios N. Gargalionis, and Nikolaos Scarmeas. 2023. "Objective Physical Function in the Alzheimer’s Disease Continuum: Association with Cerebrospinal Fluid Biomarkers in the ALBION Study" International Journal of Molecular Sciences 24, no. 18: 14079. https://doi.org/10.3390/ijms241814079
APA StyleSampatakakis, S. N., Mamalaki, E., Ntanasi, E., Kalligerou, F., Liampas, I., Yannakoulia, M., Gargalionis, A. N., & Scarmeas, N. (2023). Objective Physical Function in the Alzheimer’s Disease Continuum: Association with Cerebrospinal Fluid Biomarkers in the ALBION Study. International Journal of Molecular Sciences, 24(18), 14079. https://doi.org/10.3390/ijms241814079