
Influence of Physiological Variables and Comorbidities on Plasma Aβ40, Aβ42, and p-tau181 Levels in Cognitively Unimpaired Individuals

 , , , ,
, , , ,  ,
,
Abstract
1. Introduction
2. Results
2.1. Sample Description
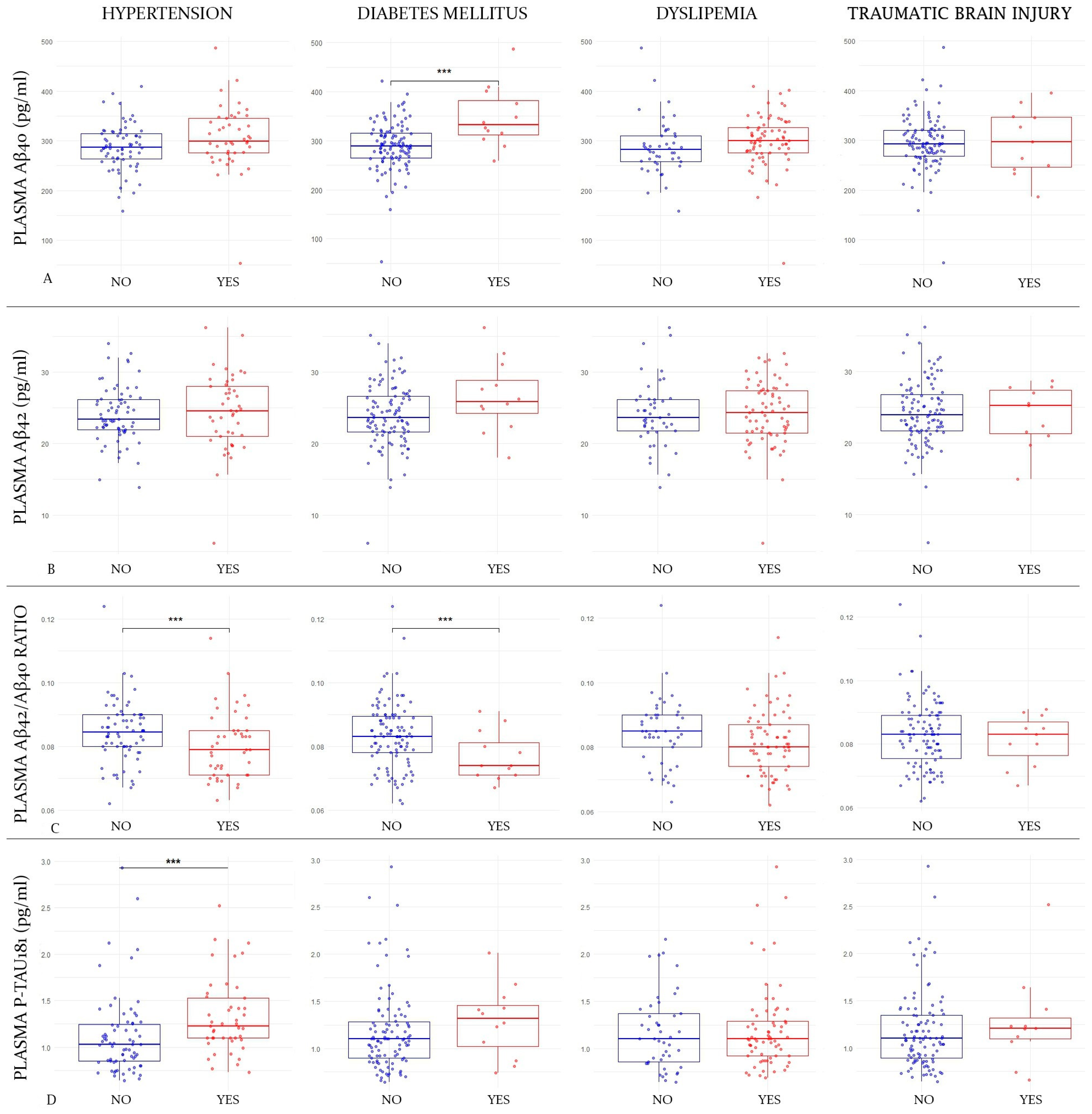
2.2. Influence of Comorbidity Status on Plasma Markers
2.3. Influence of Comorbidity Status on CSF Markers
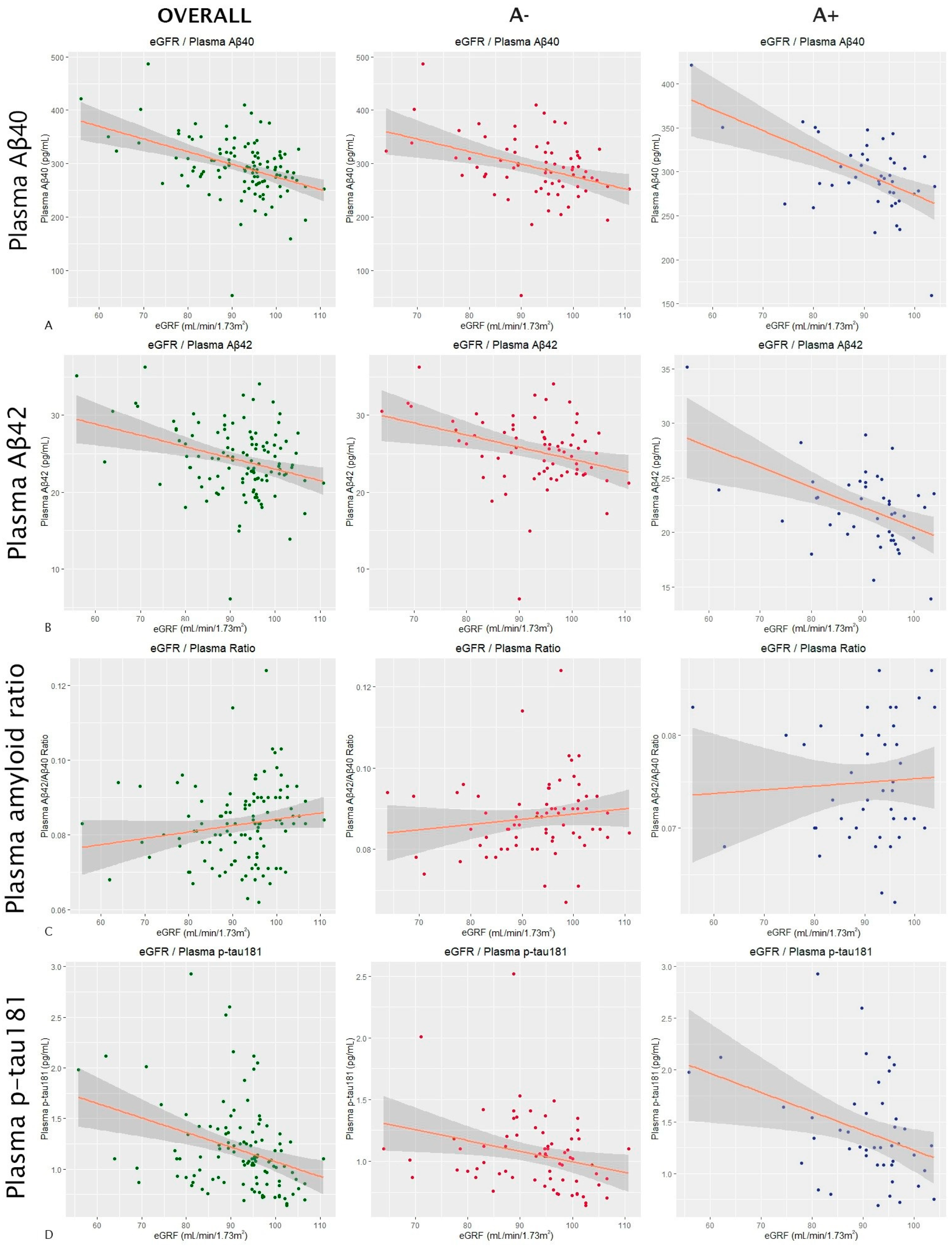
2.4. Influence of Biometric and Biochemical Variables on Plasma Markers
2.5. Influence of Biometric and Biochemical Variables on CSF Markers
3. Discussion
4. Material and Methods
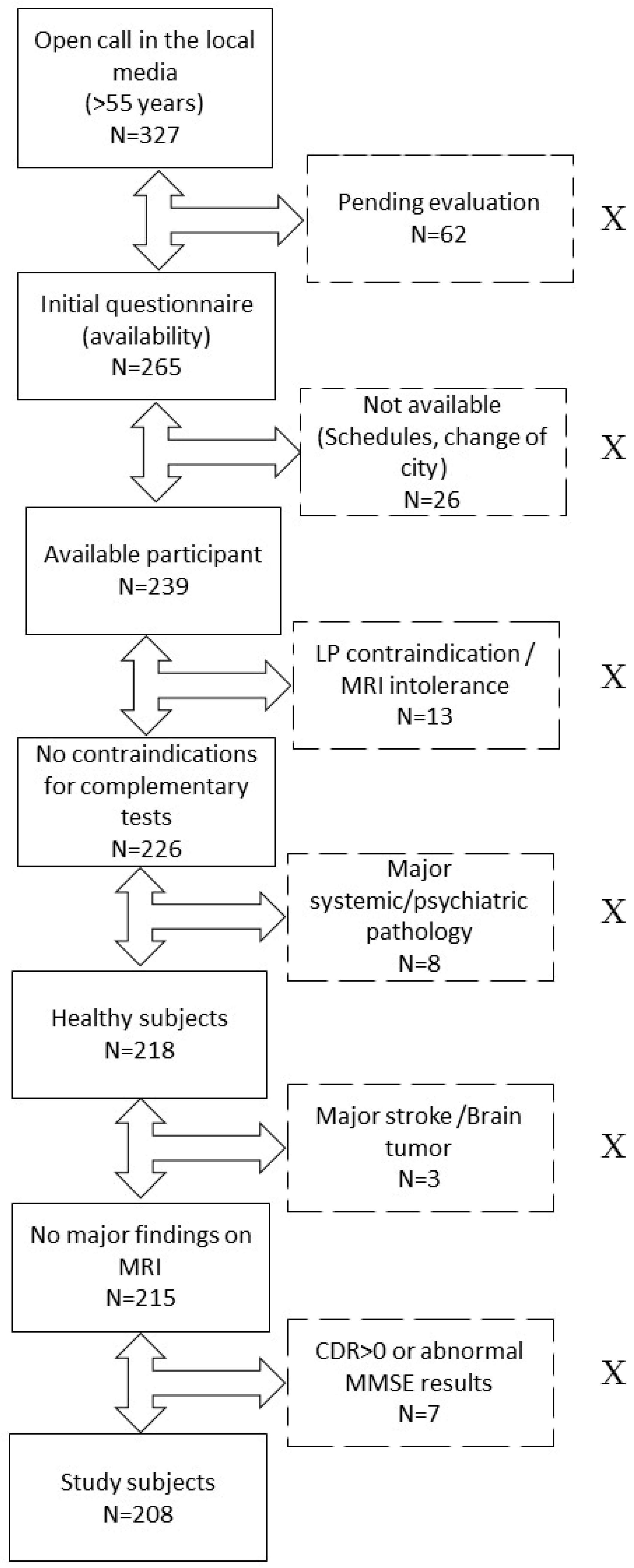
4.1. Participants
4.2. Cognitive Evaluation
4.3. ApoE Status
4.4. Sample Pre-Analysis
4.5. Biomarker Analysis
4.6. Comorbidity Assessment
4.7. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alzheimer’s Association. 2023 Alzheimer’s disease facts and figures. Alzheimers Dement. 2023, 19, 1598–1695. [Google Scholar] [CrossRef]
- Berg, L.; McKeel, D.W.; Miller, J.P.; Storandt, M.; Rubin, E.H.; Morris, J.C.; Baty, J.; Coats, M.; Norton, J.; Goate, A.M.; et al. Clinicopathologic studies in cognitively healthy aging and Alzheimer’s disease: Relation of histologic markers to dementia severity, age, sex, and apolipoprotein E genotype. Arch. Neurol. 1998, 55, 326–335. [Google Scholar] [CrossRef]
- Jack, C.R., Jr.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimers Dement. 2018, 14, 535–562. [Google Scholar] [CrossRef]
- Leuzy, A.; Cullen, N.C.; Mattsson-Carlgren, N.; Hansson, O. Current advances in plasma and cerebrospinal fluid biomarkers in Alzheimer’s disease. Curr. Opin. Neurol. 2021, 34, 266–274. [Google Scholar] [CrossRef]
- Li, Y.; Schindler, S.E.; Bollinger, J.G.; Ovod, V.; Mawuenyega, K.G.; Weiner, M.W.; Shaw, L.M.; Masters, C.L.; Fowler, C.J.; Trojanowski, J.Q.; et al. Validation of Plasma Amyloid-β 42/40 for Detecting Alzheimer Disease Amyloid Plaques. Neurology 2022, 98, e688–e699. [Google Scholar] [CrossRef]
- Brum, W.S.; Ashton, N.J.; Simrén, J.; di Molfetta, G.; Karikari, T.K.; Benedet, A.L.; Zimmer, E.R.; Lantero-Rodriguez, J.; Montoliu-Gaya, L.; Jeromin, A.; et al. Biological variation estimates of Alzheimer’s disease plasma biomarkers in healthy individuals. Alzheimers Dement. 2023. Published online November 20. [Google Scholar] [CrossRef] [PubMed]
- O’Bryant, S.E.; Petersen, M.; Hall, J.; Johnson, L.A. HABS-HD Study Team. Medical comorbidities and ethnicity impact plasma Alzheimer’s disease biomarkers: Important considerations for clinical trials and practice. Alzheimers Dement. 2023, 19, 36–43. [Google Scholar] [CrossRef] [PubMed]
- She, M.; Shang, S.; Hu, N.; Chen, C.; Dang, L.; Gao, L.; Wei, S.; Huo, K.; Wang, J.; Wang, J.; et al. Blood Pressure Level Is Associated With Changes in Plasma Aβ1 -40 and Aβ1-42 Levels: A Cross-sectional Study Conducted in the Suburbs of Xi’an, China. Front. Aging Neurosci. 2021, 13, 650679. [Google Scholar] [CrossRef] [PubMed]
- Gronewold, J.; Klafki, H.-W.; Baldelli, E.; Kaltwasser, B.; Seidel, U.K.; Todica, O.; Volsek, M.; Haußmann, U.; Wiltfang, J.; Kribben, A.; et al. Factors Responsible for Plasma β-Amyloid Accumulation in Chronic Kidney Disease. Mol. Neurobiol. 2016, 53, 3136–3145. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.-L.; Yao, X.-Q.; Lei, L.; Jin, W.-S.; Bai, Y.-D.; Zeng, G.-H.; Shi, A.-Y.; Liang, J.; Zhu, L.; Liu, Y.-H.; et al. Associations of Blood and Cerebrospinal Fluid Aβ and tau Levels with Renal Function. Mol. Neurobiol. 2023, 60, 5343–5351. [Google Scholar] [CrossRef] [PubMed]
- Syrjanen, J.A.; Campbell, M.R.; Algeciras-Schimnich, A.; Vemuri, P.; Graff-Radford, J.; Machulda, M.M.; Bu, G.; Knopman, D.S.; Jack, C.R., Jr.; Petersen, R.C.; et al. Associations of amyloid and neurodegeneration plasma biomarkers with comorbidities. Alzheimers Dement. 2022, 18, 1128–1140. [Google Scholar] [CrossRef]
- Tian, D.-Y.; Cheng, Y.; Zhuang, Z.-Q.; He, C.-Y.; Pan, Q.-G.; Tang, M.-Z.; Hu, X.-L.; Shen, Y.-Y.; Wang, Y.-R.; Chen, S.-H.; et al. Physiological clearance of amyloid-beta by the kidney and its therapeutic potential for Alzheimer’s disease. Mol. Psychiatry 2021, 26, 6074–6082. [Google Scholar] [CrossRef]
- European Alzheimer’s & Dementia Biobank Mendelian Randomization (EADB-MR) Collaboration; Luo, J.; Thomassen, J.Q.; Bellenguez, C.; Grenier-Boley, B.; de Rojas, I.; Castillo, A.; Parveen, K.; Küçükali, F.; Nicolas, A.; et al. Genetic Associations Between Modifiable Risk Factors and Alzheimer Disease. JAMA Netw. Open 2023, 6, e2313734. [Google Scholar] [CrossRef]
- Martínez-Dubarbie, F.; Guerra-Ruiz, A.; López-García, S.; Lage, C.; Fernández-Matarrubia, M.; Infante, J.; Pozueta-Cantudo, A.; García-Martínez, M.; Corrales-Pardo, A.; Bravo, M.; et al. Accuracy of plasma Aβ40, Aβ42, and p-tau181 to detect CSF Alzheimer’s pathological changes in cognitively unimpaired subjects using the Lumipulse automated platform. Alzheimers Res. Ther. 2023, 15, 163. [Google Scholar] [CrossRef]
- Hajjar, I.; Yang, Z.; Okafor, M.; Liu, C.; Waligorska, T.; Goldstein, F.C.; Shaw, L.M. Association of Plasma and Cerebrospinal Fluid Alzheimer Disease Biomarkers with Race and the Role of Genetic Ancestry, Vascular Comorbidities, and Neighborhood Factors. JAMA Netw. Open 2022, 5, e2235068. [Google Scholar] [CrossRef] [PubMed]
- Schindler, S.E.; Karikari, T.K.; Ashton, N.J.; Henson, R.L.; Yarasheski, K.E.; West, T.; Meyer, M.R.; Kirmess, K.M.; Li, Y.; Saef, B.; et al. Effect of Race on Prediction of Brain Amyloidosis by Plasma Aβ42/Aβ40, Phosphorylated Tau, and Neurofilament Light. Neurology 2022, 99, e245–e257. [Google Scholar] [CrossRef] [PubMed]
- Ramanan, V.K.; Graff-Radford, J.; Syrjanen, J.; Shir, D.; Algeciras-Schimnich, A.; Lucas, J.; Martens, Y.A.; Carrasquillo, M.M.; Day, G.S.; Ertekin-Taner, N.; et al. Association of Plasma Biomarkers of Alzheimer Disease With Cognition and Medical Comorbidities in a Biracial Cohort. Neurology 2023, 101, e1402–e1411. [Google Scholar] [CrossRef] [PubMed]
- Brum, W.S.; Docherty, K.F.; Ashton, N.J.; Zetterberg, H.; Hansson, O.; McMurray, J.J.V.; Blennow, K. Effect of Neprilysin Inhibition on Alzheimer Disease Plasma Biomarkers: A Secondary Analysis of a Randomized Clinical Trial. JAMA Neurol. 2023. Published online December 18. [Google Scholar] [CrossRef]
- López-De-Eguileta, A.; López-García, S.; Lage, C.; Pozueta, A.; García-Martínez, M.; Kazimierczak, M.; Bravo, M.; Irure, J.; López-Hoyos, M.; Muñoz-Cacho, P.; et al. The retinal ganglion cell layer reflects neurodegenerative changes in cognitively unimpaired individuals. Alzheimers Res. Ther. 2022, 14, 57. [Google Scholar] [CrossRef]
- Morris, J.C. The Clinical Dementia Rating (CDR): Current version and scoring rules. Neurology 1993, 43, 2412–2414. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Mattsson, N.; Andreasson, U.; Persson, S.; Arai, H.; Batish, S.D.; Bernardini, S.; Bocchio-Chiavetto, L.; Blankenstein, M.A.; Carrillo, M.C.; Chalbot, S.; et al. The Alzheimer’s Association external quality control program for cerebrospinal fluid biomarkers. Alzheimers Dement. 2011, 7, 386–395.e6. [Google Scholar] [CrossRef] [PubMed]
- Teunissen, C.E.; Tumani, H.; Engelborghs, S.; Mollenhauer, B. Biobanking of CSF: International standardization to optimize biomarker development. Clin. Biochem. 2014, 47, 288–292. [Google Scholar] [CrossRef]
- Verberk, I.M.W.; Misdorp, E.O.; Koelewijn, J.; Ball, A.J.; Blennow, K.; Dage, J.L.; Fandos, N.; Hansson, O.; Hirtz, C.; Janelidze, S.; et al. Characterization of pre-analytical sample handling effects on a panel of Alzheimer’s disease-related blood-based biomarkers: Results from the Standardization of Alzheimer’s Blood Biomarkers (SABB) working group. Alzheimers Dement. 2022, 18, 1484–1497. [Google Scholar] [CrossRef] [PubMed]
- Gobom, J.; Parnetti, L.; Rosa-Neto, P.; Vyhnalek, M.; Gauthier, S.; Cataldi, S.; Lerch, O.; Laczo, J.; Cechova, K.; Clarin, M.; et al. Validation of the LUMIPULSE automated immunoassay for the measurement of core AD biomarkers in cerebrospinal fluid. Clin. Chem. Lab Med. 2022, 60, 207–219. [Google Scholar] [CrossRef] [PubMed]
- Bayart, J.-L.; Hanseeuw, B.; Ivanoiu, A.; van Pesch, V. Analytical and clinical performances of the automated Lumipulse cerebrospinal fluid Aβ42 and T-Tau assays for Alzheimer’s disease diagnosis. J. Neurol. 2019, 266, 2304–2311. [Google Scholar] [CrossRef]
- De Meyer, G.; Shapiro, F.; Vanderstichele, H.; Vanmechelen, E.; Engelborghs, S.; De Deyn, P.P.; Coart, E.; Hansson, O.; Minthon, L.; Zetterberg, H.; et al. Diagnosis-independent Alzheimer disease biomarker signature in cognitively normal elderly people. Arch. Neurol. 2010, 67, 949–956. [Google Scholar] [CrossRef]
- Clifford, R.J., Jr.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Feldman, H.H.; Frisoni, G.B.; Hampel, H.; Jagust, W.J.; Johnson, K.A.; Knopman, D.S.; et al. A/T/N: An unbiased descriptive classification scheme for Alzheimer disease biomarkers. Neurology 2016, 87, 539–547. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Characteristic | Overall n = 208 | Females n = 136 | Males n = 72 |
|---|---|---|---|
| Females/Males (%) | 65.4% | 34.6% | |
| Age, median (IQR) | 64 (60–69) | 64 (59–68) | 68 (62–73) |
| ApoE ε4 carrier, n. (%) | 63 (30.3%) | 42 (30.9%) | 21 (29.2%) |
| MMSE (0–30), median (IQR) | 29 (28–30) | 29 (28–30) | 29 (28–30) |
| Education (years), median (IQR) | 12 (12–18) | 12 (12–18) | 12 (8–18) |
| Comorbidities | |||
| Hypertension (% yes) | 39.1 | 27.3 | 64.9 |
| Diabetes (% yes) | 10.4 | 11.7 | 8.1 |
| Dyslipidemia (% yes) | 60.9 | 59.7 | 62.2 |
| Traumatic Brain Injury (% yes) | 8.2 | 9.1 | 10.8 |
| Body Mass Index, median (IQR), {reference values}, kg/m2 | 26.3 (23.6–29.5) {18.5–24.9} | 25.8 (23.2–28.7) | 28.1 (25.3–30.3) |
| Systolic Blood Pressure, mean (SD), {reference values}, mmHg | 144.2 (15.1) {120–139} | 141.8 (15.8) | 148.7 (12.2) |
| Diastolic Blood Pressure, mean (SD), {reference values}, mmHg | 84.4 (10.1) {80–90} | 83.0 (9.5) | 86.9 (10.6) |
| eGFR, median (IQR), {reference values}, mL/min/1.73 m2 | 94.5 (87.3–97.9) {>60} | 94.8 (89.4–99.1) | 90.6 (82.9–95.3) |
| Glucose, median (IQR), {reference values}, mg/dL | 93 (86–100) {74–109} | 93 (86–97) | 93 (87–105) |
| Total cholesterol, mean (SD), {reference values}, mg/dL | 197.3 (36.9) {150–240} | 206.8 (34.4) | 177.5 (34.8) |
| LDL cholesterol, mean (SD), {reference values}, mg/dL | 118.6 (30.3) {100–129} | 123.8 (29.9) | 107.8 (28.7) |
| HDL cholesterol, mean (SD), {reference values}, mg/dL | 58.2 (15.4) {40–59} | 63.1 (14.6) | 48.1 (12.0) |
| AST, median (IQR), {reference values}, U/L | 22 (20–25) {14–35} | 22 (19–25) | 23 (21–26) |
| ALT, median (IQR), {reference values}, U/L | 20 (16–25) {10–49} | 19 (16–23) | 23 (18–27) |
| GGT, median (IQR), {reference values}, U/L | 20 (13–30) {6–73} | 16 (13–24) | 27 (21–37) |
| ALP, mean (SD), {reference values}, U/L | 67.8 (17.7) {46–116} | 70.2 (18.3) | 63.0 (15.8) |
| Total Bilirubin, median (IQR), {reference values}, mg/dL | 0.6 (0.4–0.7) {0.2–1.1} | 0.5 (0.4–0.6) | 0.6 (0.5–0.8) |
| Plasma Albumin, mean (SD), {reference values}, g/dL | 4.3 (0.2) {3.8–5.1} | 4.3 (0.2) | 4.2 (0.2) |
| Plasma Biomarkers | |||
| Aβ40, median (IQR), pg/mL | 292.8 (266–318) | 293.5 (268.8–319.8) | 282.9 (262.7–327.0) |
| Aβ42, median (IQR), pg/mL | 23.6 (21.5–26.3) | 24.7 (22.2–27.0) | 22.8 (20.1–26.7) |
| Ratio Aβ42/40, median (IQR) | 0.082 (0.074–0.089) | 0.084 (0.079–0.09) | 0.079 (0.071–0.084) |
| P-tau181, median (IQR), pg/mL | 1.1 (0.9–1.4) | 1.1 (0.9–1.3) | 1.2 (1.0–1.5) |
| CSF Biomarkers | |||
| Aβ40, mean (SD), pg/mL | 10,850.7 (3191.4) | 10,640.7 (3256.7) | 11,649.6 (3096.3) |
| Aβ42, median (IQR), pg/mL | 819.5 (577–1037) | 761 (565–1013) | 782 (501–1157) |
| Ratio Aβ42/40, median (IQR) | 0.084 (0.065–0.093) | 0.082 (0.069–0.090) | 0.078 (0.048–0.088) |
| P-tau181, median (IQR), pg/mL | 37.5 (30.4–54.3) | 35.5 (27–47.2) | 51.6 (35.8–61.6) |
| ATN group, n. (%) | |||
| A−T−N− | 135 (64.9%) | 91 (66.9%) | 44 (61.1%) |
| A+T−N− | 50 (24%) | 34 (25%) | 16 (22.2%) |
| A−T+N− | 1 (0.5%) | 1 (0.7%) | 0 |
| A+T+Nx | 22 (10.6%) | 10 (7.3%) | 12 (16.7) |
| Aβ40 (pg/mL) | Aβ42 (pg/mL) | Aβ42/Aβ40 | p-tau181 (pg/mL) | ||
|---|---|---|---|---|---|
| eGFR (mL/min/1.73 m2) | Estimate | −2.39 | −0.21 | 0.00001 | −0.037 |
| p-value | <0.0001 | <0.0001 | 0.83 | 0.39 | |
| BMI (kg/m2) | Estimate | 0.39 | −0.05 | −0.0002 | 0.01 |
| p-value | 0.74 | 0.60 | 0.23 | 0.22 | |
| Glucose (mg/dL) | Estimate | 0.23 | 0.02 | 0.00001 | −0.001 |
| p-value | 0.25 | 0.19 | 0.99 | 0.45 | |
| GGT (U/L) | Estimate | −0.32 | −0.04 | 0.00006 | −0.0002 |
| p-value | 0.25 | 0.08 | 0.18 | 0.89 | |
| AST (U/L) | Estimate | −2.67 | −0.15 | 0.0003 | 0.003 |
| p-value | 0.004 | 0.059 | 0.09 | 0.60 | |
| ALT (U/L) | Estimate | −0.87 | −0.05 | 0.00006 | −0.003 |
| p-value | 0.14 | 0.31 | 0.57 | 0.47 | |
| ALP (U/L) | Estimate | −0.22 | 0.02 | 0.0001 | −0.002 |
| p-value | 0.44 | 0.32 | 0.005 | 0.33 | |
| Total Bilirubin (mg/dL) | Estimate | −12.07 | −0.73 | 0.0001 | −0.05 |
| p-value | 0.49 | 0.62 | 0.97 | 0.65 | |
| Albumin (g/dL) | Estimate | 22.15 | 0.54 | −0.004 | 0.07 |
| p-value | 0.35 | 0.79 | 0.28 | 0.66 | |
| Total Cholesterol (mg/dL) | Estimate | −0.27 | −0.02 | −0.00001 | −0.0006 |
| p-value | 0.06 | 0.04 | 0.46 | 0.56 | |
| LDLc (mg/dL) | Estimate | −0.20 | −0.02 | −0.00003 | −0.0003 |
| p-value | 0.23 | 0.12 | 0.31 | 0.76 | |
| HDLc (mg/dL) | Estimate | −0.94 | −0.07 | 0.00003 | −0.001 |
| p-value | 0.008 | 0.02 | 0.68 | 0.63 | |
| SBP (mmHg) | Estimate | −0.38 | −0.03 | 0.000002 | 0.001 |
| p-value | 0.27 | 0.20 | 0.97 | 0.64 | |
| DBP (mmHg) | Estimate | −0.28 | −0.04 | −0.00003 | −0.0008 |
| p-value | 0.59 | 0.30 | 0.71 | 0.83 | |
| Aβ40 (pg/mL) | Aβ42 (pg/mL) | Aβ42/Aβ40 | p-tau181 (pg/mL) | ||
|---|---|---|---|---|---|
| eGFR (mL/min/1.73 m2) | Estimate | 73.71 | 3.87 | −0.0001 | 0.47 |
| p-value | 0.039 | 0.32 | 0.60 | 0.12 | |
| BMI (kg/m2) | Estimate | −150.32 | −9.42 | 0.0001 | −0.76 |
| p-value | 0.027 | 0.20 | 0.73 | 0.19 | |
| Glucose (mg/dL) | Estimate | 1.24 | 0.78 | 0.00005 | −0.16 |
| p-value | 0.91 | 0.54 | 0.46 | 0.09 | |
| GGT (U/L) | Estimate | −0.24 | −3.24 | −0.0002 | 0.05 |
| p-value | 0.98 | 0.06 | 0.027 | 0.71 | |
| AST (U/L) | Estimate | −83.1 | −4.79 | 0.0001 | −0.63 |
| p-value | 0.13 | 0.42 | 0.63 | 0.18 | |
| ALT (U/L) | Estimate | 4.27 | 1.37 | 0.00006 | −0.36 |
| p-value | 0.90 | 0.71 | 0.78 | 0.22 | |
| ALP (U/L) | Estimate | 1.77 | 4.59 | 0.0003 | −0.37 |
| p-value | 0.91 | 0.01 | 0.0002 | 0.009 | |
| Total Bilirubin (mg/dL) | Estimate | −1459.05 | −191.07 | −0.004 | 6.08 |
| p-value | 0.15 | 0.08 | 0.51 | 0.48 | |
| Albumin (g/dL) | Estimate | 712.7 | −9.20 | −0.006 | −4.04 |
| p-value | 0.60 | 0.95 | 0.51 | 0.73 | |
| Total Cholesterol (mg/dL) | Estimate | −15.5 | −2.38 | −0.00009 | 0.038 |
| p-value | 0.07 | 0.009 | 0.09 | 0.59 | |
| LDLc (mg/dL) | Estimate | −15.08 | −2.79 | 0.0001 | 0.05 |
| p-value | 0.13 | 0.009 | 0.056 | 0.55 | |
| HDLc (mg/dL) | Estimate | −15.7 | −1.37 | 0.000006 | 0.18 |
| p-value | 0.46 | 0.55 | 0.96 | 0.30 | |
| SBP (mmHg) | Estimate | −28.59 | −2.34 | −0.000001 | −0.08 |
| p-value | 0.15 | 0.28 | 0.99 | 0.67 | |
| DBP (mmHg) | Estimate | −17.04 | −0.79 | 0.00008 | −0.34 |
| p-value | 0.58 | 0.81 | 0.67 | 0.19 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Dubarbie, F.; Guerra-Ruiz, A.; López-García, S.; Irure-Ventura, J.; Lage, C.; Fernández-Matarrubia, M.; Pozueta-Cantudo, A.; García-Martínez, M.; Corrales-Pardo, A.; Bravo, M.; et al. Influence of Physiological Variables and Comorbidities on Plasma Aβ40, Aβ42, and p-tau181 Levels in Cognitively Unimpaired Individuals. Int. J. Mol. Sci. 2024, 25, 1481. https://doi.org/10.3390/ijms25031481
Martínez-Dubarbie F, Guerra-Ruiz A, López-García S, Irure-Ventura J, Lage C, Fernández-Matarrubia M, Pozueta-Cantudo A, García-Martínez M, Corrales-Pardo A, Bravo M, et al. Influence of Physiological Variables and Comorbidities on Plasma Aβ40, Aβ42, and p-tau181 Levels in Cognitively Unimpaired Individuals. International Journal of Molecular Sciences. 2024; 25(3):1481. https://doi.org/10.3390/ijms25031481
Chicago/Turabian StyleMartínez-Dubarbie, Francisco, Armando Guerra-Ruiz, Sara López-García, Juan Irure-Ventura, Carmen Lage, Marta Fernández-Matarrubia, Ana Pozueta-Cantudo, María García-Martínez, Andrea Corrales-Pardo, María Bravo, and et al. 2024. "Influence of Physiological Variables and Comorbidities on Plasma Aβ40, Aβ42, and p-tau181 Levels in Cognitively Unimpaired Individuals" International Journal of Molecular Sciences 25, no. 3: 1481. https://doi.org/10.3390/ijms25031481
APA StyleMartínez-Dubarbie, F., Guerra-Ruiz, A., López-García, S., Irure-Ventura, J., Lage, C., Fernández-Matarrubia, M., Pozueta-Cantudo, A., García-Martínez, M., Corrales-Pardo, A., Bravo, M., Martín-Arroyo, J., Infante, J., López-Hoyos, M., García-Unzueta, M. T., Sánchez-Juan, P., & Rodríguez-Rodríguez, E. (2024). Influence of Physiological Variables and Comorbidities on Plasma Aβ40, Aβ42, and p-tau181 Levels in Cognitively Unimpaired Individuals. International Journal of Molecular Sciences, 25(3), 1481. https://doi.org/10.3390/ijms25031481