
Association of CETP Gene Polymorphisms and Haplotypes with Cardiovascular Risk

 , ,
, , 
Abstract
1. Introduction
2. Results
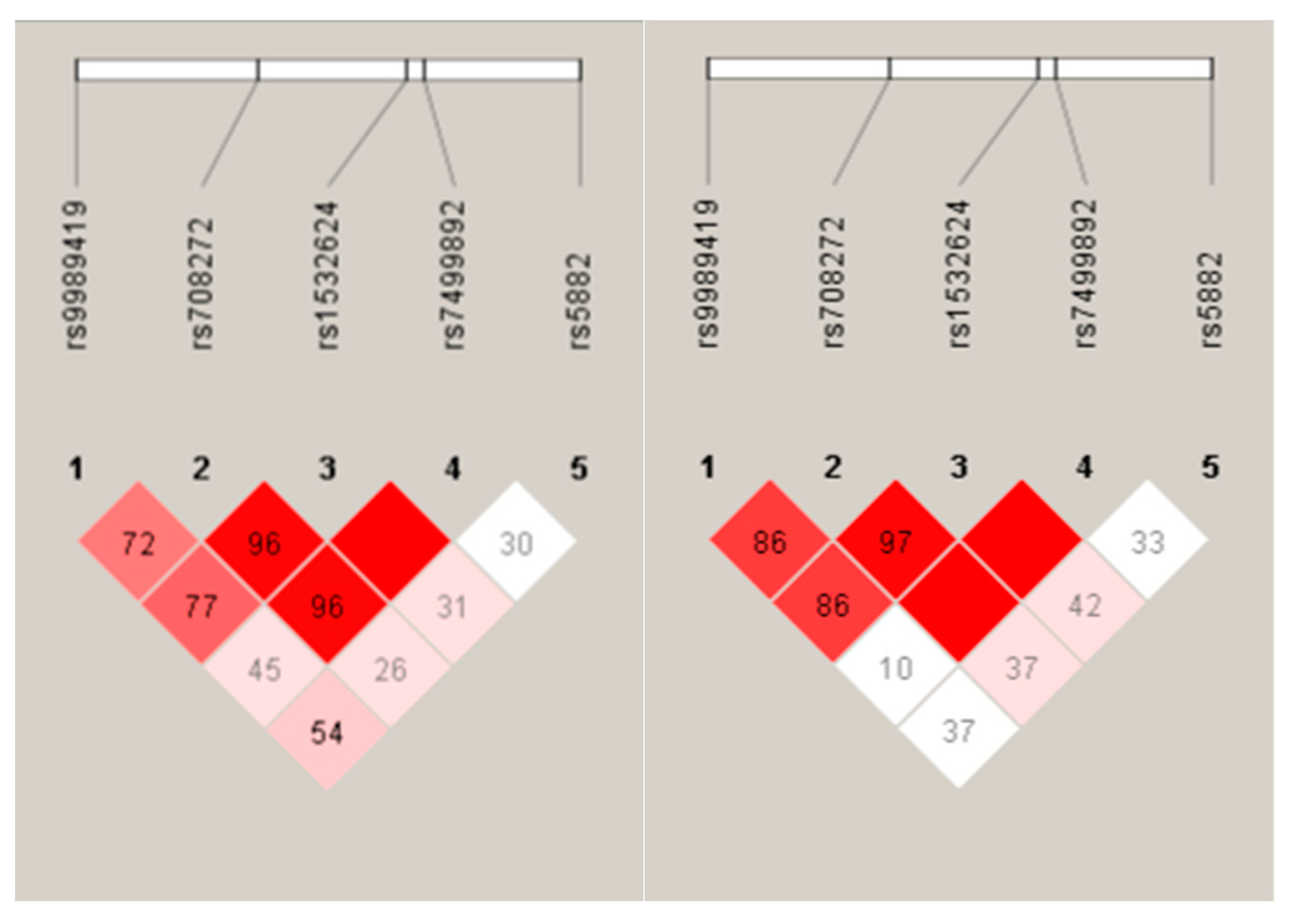
2.1. Characteristics of Study Subpopulations, Results of Hardy–Weinberg Equilibrium (HWE), Linkage Disequilibrium (LD), and Allele and Haplotype Frequencies by Analyses
2.2. Association of CETP Gene Polymorphisms and Their Haplotypes with the Estimated Cardiovascular Risk by SCORE and FRSs
2.3. Effect of SNPs and Haplotypes Significantly Associated with CVR on TG and HDL-C Levels and HDL Subfraction Profile
3. Discussion
4. Materials and Methods
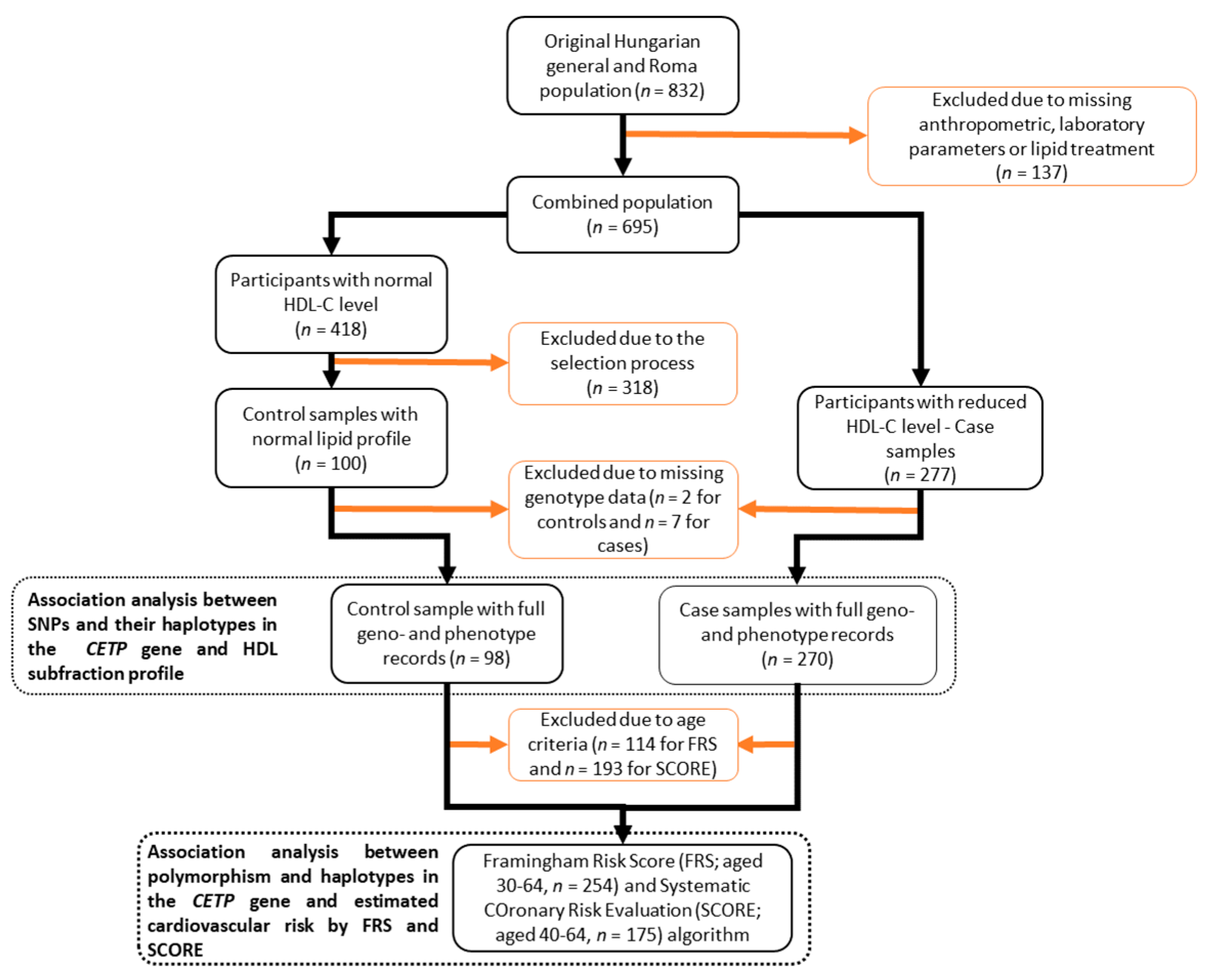
4.1. Study Design and Populations
4.2. Analysis of HDL Subfractions
4.3. Estimation of the Cardiovascular Risk by FRS and SCORE in Study Populations
4.4. DNA Isolation, Selection of SNPs, and Genotyping
4.5. Statistical Analyses
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cardiovascular Diseases (CVDs). Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-%28cvds%29 (accessed on 25 April 2023).
- Vaduganathan, M.; Mensah, G.A.; Turco, J.V.; Fuster, V.; Roth, G.A. The Global Burden of Cardiovascular Diseases and Risk A Compass for Future Health. J. Am. Coll. Cardiol. 2022, 80, 2361–2371. [Google Scholar] [CrossRef]
- Libby, P. The forgotten majority: Unfinished business in cardiovascular risk reduction. J. Am. Coll. Cardiol. 2005, 46, 1225–1228. [Google Scholar] [CrossRef]
- Knowles, J.W.; Ashley, E.A. Cardiovascular disease: The rise of the genetic risk score. PLoS Med. 2018, 15, e1002546. [Google Scholar] [CrossRef]
- Damen, J.A.; Hooft, L.; Schuit, E.; Debray, T.P.; Collins, G.S.; Tzoulaki, I.; Lassale, C.M.; Siontis, G.C.; Chiocchia, V.; Roberts, C.; et al. Prediction models for cardiovascular disease risk in the general population: Systematic review. BMJ 2016, 353, i2416. [Google Scholar] [CrossRef]
- D’Agostino, R.B., Sr.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel, W.B. General cardiovascular risk profile for use in primary care: The Framingham Heart Study. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef] [PubMed]
- Conroy, R.M.; Pyorala, K.; Fitzgerald, A.P.; Sans, S.; Menotti, A.; De Backer, G.; De Bacquer, D.; Ducimetiere, P.; Jousilahti, P.; Keil, U.; et al. Estimation of ten-year risk of fatal cardiovascular disease in Europe: The SCORE project. Eur. Heart J. 2003, 24, 987–1003. [Google Scholar] [CrossRef] [PubMed]
- Gordon, D.J.; Probstfield, J.L.; Garrison, R.J.; Neaton, J.D.; Castelli, W.P.; Knoke, J.D.; Jacobs, D.R., Jr.; Bangdiwala, S.; Tyroler, H.A. High-density lipoprotein cholesterol and cardiovascular disease. Four prospective American studies. Circulation 1989, 79, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Emerging Risk Factors, C.; Di Angelantonio, E.; Sarwar, N.; Perry, P.; Kaptoge, S.; Ray, K.K.; Thompson, A.; Wood, A.M.; Lewington, S.; Sattar, N.; et al. Major lipids, apolipoproteins, and risk of vascular disease. JAMA 2009, 302, 1993–2000. [Google Scholar] [CrossRef]
- Voight, B.F.; Peloso, G.M.; Orho-Melander, M. Plasma HDL cholesterol and risk of myocardial infarction: A mendelian randomisation study (vol 380, pg 572, 2012). Lancet 2012, 380, 564. [Google Scholar]
- Nordestgaard, B.G.; Madsen, C.M.; Varbo, A. Extreme High High-Density Lipoprotein Cholesterol Is Paradoxically Associated with High Mortality in Men and Women: Two Prospective Cohort Studies. Atherosclerosis 2017, 263, E89. [Google Scholar] [CrossRef]
- Rye, K.A.; Bursill, C.A.; Lambert, G.; Tabet, F.; Barter, P.J. The metabolism and anti-atherogenic properties of HDL. J. Lipid Res. 2009, 50, S195–S200. [Google Scholar] [CrossRef] [PubMed]
- Cuchel, M.; Rader, D.J. Macrophage reverse cholesterol transport: Key to the regression of atherosclerosis? Circulation 2006, 113, 2548–2555. [Google Scholar] [CrossRef] [PubMed]
- Barbagallo, C.M.; Averna, M.R.; Frada, G.; Noto, D.; Cavera, G.; Notarbartolo, A. Lipoprotein profile and high-density lipoproteins: Subfractions distribution in centenarians. Gerontology 1998, 44, 106–110. [Google Scholar] [CrossRef]
- Generoso, G.; Bensenor, I.M.; Santos, R.D.; Staniak, H.L.; Sharovsky, R.; Santos, I.S.; Goulart, A.C.; Jones, S.R.; Kulkarni, K.R.; Blaha, M.J.; et al. High-density Lipoprotein-cholesterol Subfractions and Coronary Artery Calcium: The ELSA-Brasil Study. Arch. Med. Res. 2019, 50, 362–367. [Google Scholar] [CrossRef]
- Maeda, S.; Nakanishi, S.; Yoneda, M.; Awaya, T.; Yamane, K.; Hirano, T.; Kohno, N. Associations between Small Dense LDL, HDL Subfractions (HDL2, HDL3) and Risk of Atherosclerosis in Japanese-Americans. J. Atheroscler. Thromb. 2012, 19, 444–452. [Google Scholar] [CrossRef] [PubMed]
- Oravec, S.; Dostal, E.; Dukat, A.; Gavornik, P.; Kucera, M.; Gruber, K. HDL subfractions analysis: A new laboratory diagnostic assay for patients with cardiovascular diseases and dyslipoproteinemia. Neuroendocrinol. Lett. 2011, 32, 502–509. [Google Scholar]
- Arsenault, B.J.; Lemieux, I.; Despres, J.P.; Gagnon, P.; Wareham, N.J.; Stroes, E.S.; Kastelein, J.J.; Khaw, K.T.; Boekholdt, S.M. HDL particle size and the risk of coronary heart disease in apparently healthy men and women: The EPIC-Norfolk prospective population study. Atherosclerosis 2009, 206, 276–281. [Google Scholar] [CrossRef]
- Zarkesh, M.; Daneshpour, M.S.; Faam, B.; Fallah, M.S.; Hosseinzadeh, N.; Guity, K.; Hosseinpanah, F.; Momenan, A.A.; Azizi, F. Heritability of the metabolic syndrome and its components in the Tehran Lipid and Glucose Study (TLGS). Genet. Res. 2012, 94, 331–337. [Google Scholar] [CrossRef]
- Schmidt, A.F.; Hunt, N.B.; Gordillo-Maranon, M.; Charoen, P.; Drenos, F.; Kivimaki, M.; Lawlor, D.A.; Giambartolomei, C.; Papacosta, O.; Chaturvedi, N.; et al. Cholesteryl ester transfer protein (CETP) as a drug target for cardiovascular disease. Nat. Commun. 2021, 12, 5640. [Google Scholar] [CrossRef]
- Ouimet, M.; Barrett, T.J.; Fisher, E.A. HDL and Reverse Cholesterol Transport. Circ. Res. 2019, 124, 1505–1518. [Google Scholar] [CrossRef]
- Nurmohamed, N.S.; Ditmarsch, M.; Kastelein, J.J.P. Cholesteryl ester transfer protein inhibitors: From high-density lipoprotein cholesterol to low-density lipoprotein cholesterol lowering agents? Cardiovasc. Res. 2022, 118, 2919–2931. [Google Scholar] [CrossRef]
- Barter, P.J.; Brewer, H.B., Jr.; Chapman, M.J.; Hennekens, C.H.; Rader, D.J.; Tall, A.R. Cholesteryl ester transfer protein: A novel target for raising HDL and inhibiting atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 160–167. [Google Scholar] [CrossRef]
- Schwartz, C.C.; VandenBroek, J.M.; Cooper, P.S. Lipoprotein cholesteryl ester production, transfer, and output in vivo in humans. J. Lipid Res. 2004, 45, 1594–1607. [Google Scholar] [CrossRef] [PubMed]
- Klerkx, A.H.; de Grooth, G.J.; Zwinderman, A.H.; Jukema, J.W.; Kuivenhoven, J.A.; Kastelein, J.J. Cholesteryl ester transfer protein concentration is associated with progression of atherosclerosis and response to pravastatin in men with coronary artery disease (REGRESS). Eur. J. Clin. Investig. 2004, 34, 21–28. [Google Scholar] [CrossRef] [PubMed]
- de Grooth, G.J.; Smilde, T.J.; Van Wissen, S.; Klerkx, A.H.; Zwinderman, A.H.; Fruchart, J.C.; Kastelein, J.J.; Stalenhoef, A.F.; Kuivenhoven, J.A. The relationship between cholesteryl ester transfer protein levels and risk factor profile in patients with familial hypercholesterolemia. Atherosclerosis 2004, 173, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Tosheska, K.; Labudovic, D.; Jovanova, S.; Jaglikovski, B.; Alabakovska, S. Cholesteryl ester transfer protein, low density lipoprotein particle size and intima media thickness in patients with coronary heart disease. Bosn. J. Basic Med. Sci. 2011, 11, 169–173. [Google Scholar] [CrossRef]
- Piko, P.; Fiatal, S.; Kosa, Z.; Sandor, J.; Adany, R. Genetic factors exist behind the high prevalence of reduced high-density lipoprotein cholesterol levels in the Roma population. Atherosclerosis 2017, 263, 119–126. [Google Scholar] [CrossRef]
- Piko, P.; Fiatal, S.; Kosa, Z.; Sandor, J.; Adany, R. Generalizability and applicability of results obtained from populations of European descent regarding the effect direction and size of HDL-C level-associated genetic variants to the Hungarian general and Roma populations. Gene 2019, 686, 187–193. [Google Scholar] [CrossRef]
- Piko, P.; Fiatal, S.; Werissa, N.A.; Bekele, B.B.; Racz, G.; Kosa, Z.; Sandor, J.; Adany, R. The Effect of Haplotypes in the CETP and LIPC Genes on the Triglycerides to HDL-C Ratio and Its Components in the Roma and Hungarian General Populations. Genes 2020, 11, 56. [Google Scholar] [CrossRef]
- Piko, P.; Kosa, Z.; Sandor, J.; Seres, I.; Paragh, G.; Adany, R. The profile of HDL-C subfractions and their association with cardiovascular risk in the Hungarian general and Roma populations. Sci. Rep. 2022, 12, 10915. [Google Scholar] [CrossRef]
- Wang, J.; Wang, L.J.; Zhong, Y.; Gu, P.; Shao, J.Q.; Jiang, S.S.; Gong, J.B. CETP gene polymorphisms and risk of coronary atherosclerosis in a Chinese population. Lipids Health Dis. 2013, 12, 176. [Google Scholar] [CrossRef] [PubMed]
- Todur, S.P.; Ashavaid, T.F. Association of CETP and LIPC Gene Polymorphisms with HDL and LDL Sub-fraction Levels in a Group of Indian Subjects: A Cross-Sectional Study. Indian J. Clin. Biochem. 2013, 28, 116–123. [Google Scholar] [CrossRef]
- Guo, S.; Hu, Y.; Ding, Y.; Liu, J.; Zhang, M.; Ma, R.; Guo, H.; Wang, K.; He, J.; Yan, Y.; et al. Association between Eight Functional Polymorphisms and Haplotypes in the Cholesterol Ester Transfer Protein (CETP) Gene and Dyslipidemia in National Minority Adults in the Far West Region of China. Int. J. Environ. Res. Public Health 2015, 12, 15979–15992. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Kim, J.Q.; Kim, J.; Oh, H.; Park, M. Studies on the plasma lipid profiles, and LCAT and CETP activities according to hyperlipoproteinemia phenotypes (HLP). Atherosclerosis 2001, 159, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Winkelmann, B.R.; Hoffmann, M.M.; Nauck, M.; Kumar, A.M.; Nandabalan, K.; Judson, R.S.; Boehm, B.O.; Tall, A.R.; Ruano, G.; Marz, W. Haplotypes of the cholesteryl ester transfer protein gene predict lipid-modifying response to statin therapy. Pharmacogenom. J. 2003, 3, 284–296. [Google Scholar] [CrossRef]
- Bercovich, D.; Friedlander, Y.; Korem, S.; Houminer, A.; Hoffman, A.; Kleinberg, L.; Shochat, C.; Leitersdorf, E.; Meiner, V. The association of common SNPs and haplotypes in the CETP and MDR1 genes with lipids response to fluvastatin in familial hypercholesterolemia. Atherosclerosis 2006, 185, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Raina, J.K.; Sharma, M.; Panjaliya, R.K.; Dogra, V.; Bakaya, A.; Kumar, P. Association of ESR1 (rs2234693 and rs9340799), CETP (rs708272), MTHFR (rs1801133 and rs2274976) and MS (rs185087) polymorphisms with Coronary Artery Disease (CAD). BMC Cardiovasc. Disord. 2020, 20, 340. [Google Scholar] [CrossRef]
- Vargas-Alarcon, G.; Perez-Mendez, O.; Posadas-Sanchez, R.; Pena-Duque, M.A.; Martinez-Rios, M.A.; Delgadillo-Rodriguez, H.; Fragoso, J.M. The rs4783961 and rs708272 genetic variants of the CETP gene are associated with coronary artery disease, but not with restenosis after coronary stenting. Arch. Cardiol. Mex. 2022, 92, 334–341. [Google Scholar] [CrossRef]
- Tall, A.R.; Yvan-Charvet, L.; Wang, N. The failure of torcetrapib: Was it the molecule or the mechanism? Arterioscler. Thromb. Vasc. Biol. 2007, 27, 257–260. [Google Scholar] [CrossRef]
- Robinson, J.G. Dalcetrapib: A review of Phase II data. Expert Opin. Investig. Drugs 2010, 19, 795–805. [Google Scholar] [CrossRef]
- Gutstein, D.E.; Krishna, R.; Johns, D.; Surks, H.K.; Dansky, H.M.; Shah, S.; Mitchel, Y.B.; Arena, J.; Wagner, J.A. Anacetrapib, a novel CETP inhibitor: Pursuing a new approach to cardiovascular risk reduction. Clin. Pharmacol. Ther. 2012, 91, 109–122. [Google Scholar] [CrossRef] [PubMed]
- Lincoff, A.M.; Nicholls, S.J.; Riesmeyer, J.S.; Barter, P.J.; Brewer, H.B.; Fox, K.A.A.; Gibson, C.M.; Granger, C.; Menon, V.; Montalescot, G.; et al. Evacetrapib and Cardiovascular Outcomes in High-Risk Vascular Disease. N. Engl. J. Med. 2017, 376, 1933–1942. [Google Scholar] [CrossRef] [PubMed]
- Sammons, E.; Hopewell, J.C.; Chen, F.; Stevens, W.; Wallendszus, K.; Valdes-Marquez, E.; Dayanandan, R.; Knott, C.; Murphy, K.; Wincott, E.; et al. Long-term safety and efficacy of anacetrapib in patients with atherosclerotic vascular disease. Eur. Heart J. 2022, 43, 1416–1424. [Google Scholar] [CrossRef]
- Dangas, K.; Navar, A.M.; Kastelein, J.J.P. The effect of CETP inhibitors on new-onset diabetes: A systematic review and meta-analysis. Eur. Heart J. Cardiovasc. Pharmacother. 2022, 8, 622–632. [Google Scholar] [CrossRef]
- Ditmarsch, M.; Kling, D.; Curcio, D.; Alp, N.; Kastelein, J.; Davidson, M. Obicetrapib Lowers LDL-C in Patients Taking High Intensity Statins—Results from the ROSE Clinical Trial. J. Clin. Lipidol. 2022, 16, e67–e68. [Google Scholar] [CrossRef]
- Santana, K.G.; Righetti, R.F.; Breda, C.N.S.; Dominguez-Amorocho, O.A.; Ramalho, T.; Dantas, F.E.B.; Nunes, V.S.; Tiberio, I.; Soriano, F.G.; Camara, N.O.S.; et al. Cholesterol-Ester Transfer Protein Alters M1 and M2 Macrophage Polarization and Worsens Experimental Elastase-Induced Pulmonary Emphysema. Front. Immunol. 2021, 12, 684076. [Google Scholar] [CrossRef] [PubMed]
- Venancio, T.M.; Machado, R.M.; Castoldi, A.; Amano, M.T.; Nunes, V.S.; Quintao, E.C.; Camara, N.O.; Soriano, F.G.; Cazita, P.M. CETP Lowers TLR4 Expression Which Attenuates the Inflammatory Response Induced by LPS and Polymicrobial Sepsis. Mediators Inflamm. 2016, 2016, 1784014. [Google Scholar] [CrossRef]
- Wanschel, A.; Guizoni, D.M.; Lorza-Gil, E.; Salerno, A.G.; Paiva, A.A.; Dorighello, G.G.; Davel, A.P.; Balkan, W.; Hare, J.M.; Oliveira, H.C.F. The Presence of Cholesteryl Ester Transfer Protein (CETP) in Endothelial Cells Generates Vascular Oxidative Stress and Endothelial Dysfunction. Biomolecules 2021, 11, 69. [Google Scholar] [CrossRef]
- Chantepie, S.; Bochem, A.E.; Chapman, M.J.; Hovingh, G.K.; Kontush, A. High-density lipoprotein (HDL) particle subpopulations in heterozygous cholesteryl ester transfer protein (CETP) deficiency: Maintenance of antioxidative activity. PLoS ONE 2012, 7, e49336. [Google Scholar] [CrossRef]
- Dorighello, G.G.; Assis, L.H.P.; Rentz, T.; Morari, J.; Santana, M.F.M.; Passarelli, M.; Ridgway, N.D.; Vercesi, A.E.; Oliveira, H.C.F. Novel Role of CETP in Macrophages: Reduction of Mitochondrial Oxidants Production and Modulation of Cell Immune-Metabolic Profile. Antioxidants 2022, 11, 1734. [Google Scholar] [CrossRef]
- Schechter, C.B.; Barzilai, N.; Crandall, J.P.; Atzmon, G. Cholesteryl ester transfer protein (CETP) genotype and reduced CETP levels associated with decreased prevalence of hypertension. Mayo Clin. Proc. 2010, 85, 522–526. [Google Scholar] [CrossRef]
- Hatakeyama, K. CETP Activity: A Link between Lipid Metabolism and Coagulation System. J. Atheroscler. Thromb. 2016, 23, 1144–1146. [Google Scholar] [CrossRef]
- Deguchi, H.; Fernandez, J.A.; Griffin, J.H. Plasma cholesteryl ester transfer protein and blood coagulability. Thromb. Haemost. 2007, 98, 1160–1164. [Google Scholar] [CrossRef] [PubMed]
- Li-Gao, R.; Mook-Kanamori, D.O.; Cannegieter, S.C.; Willems van Dijk, K.; Rosendaal, F.R.; van Hylckama Vlieg, A. The association of genetic variants in the cholesteryl ester transfer protein gene with hemostatic factors and a first venous thrombosis. J. Thromb. Haemost. 2019, 17, 1535–1543. [Google Scholar] [CrossRef] [PubMed]
- Adany, R.; Piko, P.; Fiatal, S.; Kosa, Z.; Sandor, J.; Biro, E.; Kosa, K.; Paragh, G.; Bacsne Baba, E.; Veres-Balajti, I.; et al. Prevalence of Insulin Resistance in the Hungarian General and Roma Populations as Defined by Using Data Generated in a Complex Health (Interview and Examination) Survey. Int. J. Environ. Res. Public Health 2020, 17, 4833. [Google Scholar] [CrossRef] [PubMed]
- Hintzpeter, B.; Finger, J.D.; Allen, J.; Kuhnert, R.; Seeling, S.; Thelen, J.; Lange, C. European Health Interview Survey (EHIS) 2—Background and study methodology. J. Health Monit. 2019, 4, 66–79. [Google Scholar] [CrossRef]
- Chary, A.; Hedayati, M. Review of Laboratory Methods to Determine HDL and LDL Subclasses and Their Clinical Importance. Rev. Cardiovasc. Med. 2022, 23, 147. [Google Scholar] [CrossRef]
- Wilson, P.W.; D’Agostino, R.B.; Levy, D.; Belanger, A.M.; Silbershatz, H.; Kannel, W.B. Prediction of coronary heart disease using risk factor categories. Circulation 1998, 97, 1837–1847. [Google Scholar] [CrossRef]
- Grundy, S.M.; Becker, D.; Clark, L.T.; Cooper, R.S.; Denke, M.A.; Howard, W.J.; Hunninghake, D.B.; Illingworth, R.; Luepker, R.V.; McBride, P.; et al. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) Final Report. Circulation 2002, 106, 3143–3421. [Google Scholar] [CrossRef]
- Piko, P.; Kosa, Z.; Sandor, J.; Adany, R. Comparative risk assessment for the development of cardiovascular diseases in the Hungarian general and Roma population. Sci. Rep. 2021, 11, 3085. [Google Scholar] [CrossRef]
- Machiela, M.J.; Chanock, S.J. LDlink: A web-based application for exploring population-specific haplotype structure and linking correlated alleles of possible functional variants. Bioinformatics 2015, 31, 3555–3557. [Google Scholar] [CrossRef] [PubMed]
- Sole, X.; Guino, E.; Valls, J.; Iniesta, R.; Moreno, V. SNPStats: A web tool for the analysis of association studies. Bioinformatics 2006, 22, 1928–1929. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| A | Control (n = 52) | Case (n = 124) | p-Value |
| Average (Std. Dev.) | |||
| Age (years) | 51.23 (0.90) | 49.66 (0.59) | 0.164 |
| BMI (kg/m2) | 25.14 (0.77) | 29.29 (0.55) | <0.001 * |
| Systolic blood pressure (mmHg) | 130.10 (2.40) | 127.15 (1.46) | 0.214 |
| Fasting glucose (mmol/L) | 5.55 (0.29) | 5.47 (0.15) | 0.844 |
| Total cholesterol (mmol/L) | 4.59 (0.09) | 5.05 (0.10) | 0.004 * |
| Triacylglycerol (mmol/L) | 0.97 (0.04) | 2.08 (0.10) | <0.001 * |
| High-density lipoprotein Cholesterol (mmol/L) | 1.62 (0.05) | 1.01 (0.02) | <0.001 * |
| Prevalence in % (95%CI) | p-value | ||
| Roma | 50.00 (36.72–63.28) | 54.03 (45.25–62.63) | 0.625 |
| Women | 48.08 (34.91–61.45) | 75.81 (67.73–82.69) | <0.001 * |
| Current smoker | 49.02 (35.67–62.48) | 55.28 (46.46–63.86) | 0.451 |
| Treated for high blood pressure | 28.85 (17.92–42.05) | 36.29 (28.22–44.99) | 0.342 |
| Treated for diabetes | 11.54 (4.96–22.24) | 10.48 (6.01–16.78) | 0.837 |
| B | Control (n = 64) | Case (n = 191) | p-Value |
| Average (Std. Dev.) | |||
| Age (years) | 48.12 (1.10) | 44.29 (0.67) | 0.004 * |
| BMI (kg/m2) | 24.78 (0.67) | 29.07 (0.45) | <0.001 * |
| Systolic blood pressure (mmHg) | 128.57 (2.08) | 124.59 (1.14) | 0.049 * |
| Fasting glucose (mmol/L) | 5.28 (0.25) | 5.26 (0.11) | 0.950 |
| Total cholesterol (mmol/L) | 4.55 (0.08) | 4.91 (0.08) | 0.013 * |
| Triacylglycerol (mmol/L) | 0.94 (0.04) | 2.04 (0.08) | <0.001 * |
| High-density lipoprotein cholesterol (mmol/L) | 1.63 (0.05) | 1.01 (0.01) | <0.001 * |
| Prevalence in % (95%CI) | p-value | ||
| Roma | 50.00 (37.98–62.02) | 45.03 (38.09–52.11) | 0.490 |
| Women | 48.44 (36.49–60.52) | 72.77 (66.15–78.71) | <0.001 * |
| Current smoker | 49.21 (37.13–61.35) | 56.84 (49.74–63.74) | 0.291 |
| Treated for high blood pressure | 25.00 (15.65–36.55) | 30.89 (24.66–37.69) | 0.371 |
| Treated for diabetes | 9.38 (4.01–18.30) | 7.85 (4.66–12.31) | 0.702 |
| Control (n = 96) | Case (n = 270) | p-Value | |
|---|---|---|---|
| Average (Std. Dev.) | |||
| Age (years) | 41.82 (1.34) | 40.45 (0.72) | 0.382 |
| BMI (kg/m2) | 24.06 (0.53) | 28.80 (0.37) | <0.001 * |
| Systolic blood pressure (mmHg) | 124.85 (1.71) | 123.02 (0.94) | 0.272 |
| Fasting glucose (mmol/L) | 5.09 (0.19) | 5.23 (0.10) | 0.381 |
| Total cholesterol (mmol/L) | 4.38 (0.07) | 4.80 (0.07) | 0.001 * |
| Triacylglycerol (mmol/L) | 0.90 (0.03) | 1.95 (0.07) | <0.001 * |
| High-density lipoprotein cholesterol (mmol/L) | 1.60 (0.04) | 1.01 (0.01) | <0.001 * |
| Prevalence in % (95%CI) | p-value | ||
| Roma | 51.04 (41.14–60.89) | 58.52 (52.58–64.28) | 0.204 |
| Women | 48.96 (39.11–58.86) | 73.33 (67.83–78.34) | <0.001 * |
| Current smoker | 48.42 (38.55–58.39) | 57.25 (51.29–63.06) | 0.137 |
| Treated for high blood pressure | 20.83 (13.65–29.75) | 27.41 (22.35–32.95) | 0.205 |
| Treated for diabetes | 7.29 (3.32–13.78) | 7.04 (4.44–10.55) | 0.934 |
| SCORE (n = 176) | FRSCHD and FRSCVD (n = 255) | HDL Subfractions’ Profile (n = 366) | |
|---|---|---|---|
| SNPs (minor/major allele) | Frequency in % | ||
| rs1532624 (A/C) | 27.27/72.73 | 29.71/70.29 | 30.33/69.67 |
| rs5882 (G/A) | 28.69/71.31 | 28.82/71.18 | 28.76/71.24 |
| rs708272 (A/G) | 29.26/70.74 | 31.37/68.63 | 31.76/68.24 |
| rs7499892 (T/C) | 36.08/63.92 | 33.34/66.66 | 33.74/66.26 |
| rs9989419 (G/A) | 46.45/53.55 | 47.06/52.94 | 48.84/51.16 |
| Haplotypes (H) | Prevalence in % | ||
| H1 (AGACG) | 22.29 | 22.27 | 23.13 |
| H2 (AAACG) | 13.76 | 14.50 | 14.74 |
| H3 (CAGCA) | 14.79 | 15.73 | 14.04 |
| H4 (CAGCG) | 8.86 | 8.46 | 9.03 |
| H5 (CAGTA) | 16.79 | 14.90 | 15.90 |
| H6 (CGGCA) | 5.26 | 5.67 | 6.20 |
| H7 (AAACA) | 2.37 | 2.87 | 2.76 |
| H8 (CGGTG) | 5.65 | 5.22 | 4.78 |
| H9 (CGGCG) | 3.25 | 3.49 | 3.14 |
| H10 (CAGTG) | 2.72 | 2.38 | 2.84 |
| Model I. | SCORE | FRSCHD | FRSCVD | |||
| β (Std. Dev.) | p-Value | β (Std. Dev.) | p-Value | β (Std. Dev.) | p-Value | |
| rs1532624 (C allele) | 0.190 (0.130) | 0.144 | 0.445 (0.205) | 0.031 * | 0.916 (0.384) | 0.018 * |
| rs5882 (A allele) | 0.141 (0.120) | 0.243 | 0.318 (0.201) | 0.116 | 0.442 (0.381) | 0.248 |
| rs708272 (G allele) | 0.159 (0.124) | 0.201 | 0.467 (0.199) | 0.020 * | 0.916 (0.372) | 0.014 * |
| rs7499892 (T allele) | 0.260 (0.143) | 0.070 | 0.774 (0.250) | 0.002 ** | 1.580 (0.467) | <0.001 ** |
| rs9989419 (A allele) | 0.133 (0.118) | 0.262 | 0.276 (0.195) | 0.159 | 0.308 (0.368) | 0.403 |
| Model II. | SCORE | FRSCHD | FRSCVD | |||
| β (std. dev.) | p-value | β (std. dev.) | p-value | β (std. dev.) | p-value | |
| rs1532624 (C allele) | 0.090 (0.123) | 0.467 | 0.357 (0.203) | 0.080 | 0.641 0.376) | 0.089 |
| rs5882 (A allele) | 0.049 (0.113) | 0.669 | 0.269 (0.198) | 0.175 | 0.262 (0.368) | 0.477 |
| rs708272 (G allele) | 0.067 (0.117) | 0.571 | 0.389 (0.197) | 0.050 * | 0.671 (0.363) | 0.066 |
| rs7499892 (T allele) | 0.192 (0.133) | 0.151 | 0.693 (0.246) | 0.005 ** | 1.344 (0.452) | 0.003 ** |
| rs9989419 (A allele) | 0.031 (0.111) | 0.780 | 0.136 (0.195) | 0.488 | −0.067 (0.361) | 0.853 |
| Model III. | SCORE | FRSCHD | FRSCVD | |||
| β (std. dev.) | p-value | β (std. dev.) | p-value | β (std. dev.) | p-value | |
| rs1532624 (C allele) | 0.061 (0.122) | 0.616 | 0.320 (0.184) | 0.084 | 0.581 (0.350) | 0.098 |
| rs5882 (A allele) | 0.043 (0.111) | 0.700 | 0.120 (0.181) | 0.506 | 0.018 80.345) | 0.960 |
| rs708272 (G allele) | 0.055 (0.115) | 0.637 | 0.400 (0.178) | 0.026 * | 0.694 (0.337) | 0.040 * |
| rs7499892 (T allele) | 0.156 (0.132) | 0.240 | 0.454 (0.227) | 0.046 * | 0.978 (0.428) | 0.023 * |
| rs9989419 (A allele) | 0.015 80.109) | 0.891 | 0.121 (0.177) | 0.496 | −0.091 (0.336) | 0.787 |
| H1 | H2 | H3 | H4 | H5 | H6 | H7 | H8 | H9 | H10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| rs1532624 | A | A | C | C | C | C | A | C | C | C |
| rs5882 | G | A | A | A | A | G | A | G | G | A |
| rs708272 | A | A | G | G | G | G | A | G | G | G |
| rs7499892 | C | C | C | C | T | C | C | T | C | T |
| rs9989419 | G | G | A | G | A | A | A | G | G | G |
| Model I. | β (95%CI), p-value | |||||||||
| SCORE | Ref. | N.S. | N.S. | N.S. | 0.43 (0.05–0.81) p = 0.028 * | N.S. | N.S. | 0.82 (0.18–1.46) p = 0.012 * | N.S. | N.S. |
| FRSCHD | N.S. | N.S. | N.S. | 0.98 (0.30- 1.64) p = 0.003 * | N.S. | 1.79 (0.27–3.31) p = 0.022 * | 1.48 (0.30–2.66) p = 0.014 * | N.S. | N.S. | |
| FRSCVD | N.S. | N.S. | N.S. | 1.93 (0.69–3.16) p = 0.002 * | N.S. | N.S. | 3.04 (0.92–5.17) p = 0.005 * | N.S. | N.S. | |
| Model II. | Β (95%CI), p-value | |||||||||
| SCORE | Ref. | N.S. | N.S. | N.S. | N.S. | N.S. | N.S. | 0.62 (0.01–1.24) p = 0.047 * | N.S. | N.S. |
| FRSCHD | N.S. | N.S. | N.S. | 0.80 (0.14–1.45) p = 0.017 * | N.S. | 1.63 (0.18–3.09) p = 0.028 * | 1.27 (0.11–2.44) p = 0.033 * | N.S. | N.S. | |
| FRSCVD | N.S. | N.S. | N.S. | 1.46 (0.25–2.66) p = 0.018 * | N.S. | N.S. | 2.97 (1.00–4.94) p = 0.003 * | N.S. | N.S. | |
| Model III | β (95%CI), p-value | |||||||||
| SCORE | Ref. | N.S. | N.S. | N.S. | N.S. | N.S. | N.S. | N.S. | N.S. | N.S. |
| FRSCHD | N.S. | N.S. | N.S. | N.S. | N.S. | 1.43 (0.15–2.71) p = 0.029 * | N.S. | N.S. | N.S. | |
| FRSCVD | N.S. | N.S. | N.S. | N.S. | N.S. | N.S. | 2.29 (0.29–4.28) p = 0.025 * | N.S. | N.S. | |
| H1 | H5 | H7 | H8 | |
|---|---|---|---|---|
| rs1532624 | A | C | A | C |
| rs5882 | G | A | A | G |
| rs708272 | A | G | A | G |
| rs7499892 | C | T | C | T |
| rs9989419 | G | A | A | G |
| β (95%CI) | ||||
| TG | Ref. | 0.43 (0.16–0.69) p = 0.002 ** | N.S. | N.S. |
| HDL-C | Ref. | −0.12 (−0.20–−0.04), p = 0.004 ** | N.S. | N.S. |
| HDL-1 | Ref. | N.S. | N.S. | −0.02 (−0.04–−0.00) p = 0.030 * |
| HDL-2 | N.S. | N.S. | N.S. | |
| HDL-3 | N.S. | −0.04 (−0.08–−0.01) p = 0.024 * | N.S. | |
| HDL-4 | N.S. | N.S. | N.S. | |
| HDL-5 | N.S. | −0.01 (−0.02–0.00) p = 0.020 * | N.S. | |
| HDL-6 | −0.03 (−0.04–−0.01) p = 0.003 ** | N.S. | N.S. | |
| HDL-7 | −0.01 (−0.02–0.00) p = 0.002 ** | N.S. | −0.01 (−0.03–0.00) p = 0.019 * | |
| HDL-8 | −0.01 (−0.02–0.00) p = 0.001 ** | N.S. | −0.01 (−0.02–0.00) p = 0.012 * | |
| HDL-9 | −0.01 (−0.01–0.00) p = 0.019 * | N.S. | N.S. | |
| HDL-10 | N.S. | N.S. | N.S. | |
| Large HDL | Ref. | N.S. | N.S. | N.S. |
| Interm. HDL | −0.05 (−0.09–−0.02) p = 0.008 * | N.S. | N.S. | |
| Small HDL | N.S. | N.S. | N.S. | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piko, P.; Jenei, T.; Kosa, Z.; Sandor, J.; Kovacs, N.; Seres, I.; Paragh, G.; Adany, R. Association of CETP Gene Polymorphisms and Haplotypes with Cardiovascular Risk. Int. J. Mol. Sci. 2023, 24, 10281. https://doi.org/10.3390/ijms241210281
Piko P, Jenei T, Kosa Z, Sandor J, Kovacs N, Seres I, Paragh G, Adany R. Association of CETP Gene Polymorphisms and Haplotypes with Cardiovascular Risk. International Journal of Molecular Sciences. 2023; 24(12):10281. https://doi.org/10.3390/ijms241210281
Chicago/Turabian StylePiko, Peter, Tibor Jenei, Zsigmond Kosa, Janos Sandor, Nora Kovacs, Ildiko Seres, Gyorgy Paragh, and Roza Adany. 2023. "Association of CETP Gene Polymorphisms and Haplotypes with Cardiovascular Risk" International Journal of Molecular Sciences 24, no. 12: 10281. https://doi.org/10.3390/ijms241210281
APA StylePiko, P., Jenei, T., Kosa, Z., Sandor, J., Kovacs, N., Seres, I., Paragh, G., & Adany, R. (2023). Association of CETP Gene Polymorphisms and Haplotypes with Cardiovascular Risk. International Journal of Molecular Sciences, 24(12), 10281. https://doi.org/10.3390/ijms241210281