
High Expression Levels of miR-21-5p in Younger Hospitalized COVID-19 Patients Are Associated with Mortality and Critical Disease

 , , ,
, , ,  ,
,  ,
,  , ,
, , 
Abstract
1. Introduction
2. Results
2.1. The miR-21-5p and miR-146a-5p and Their Relation with Mortality in Patients with COVID-19
2.2. The miR-21-5p and miR-146a-5p Expression between Patients with Severe and Critical COVID-19
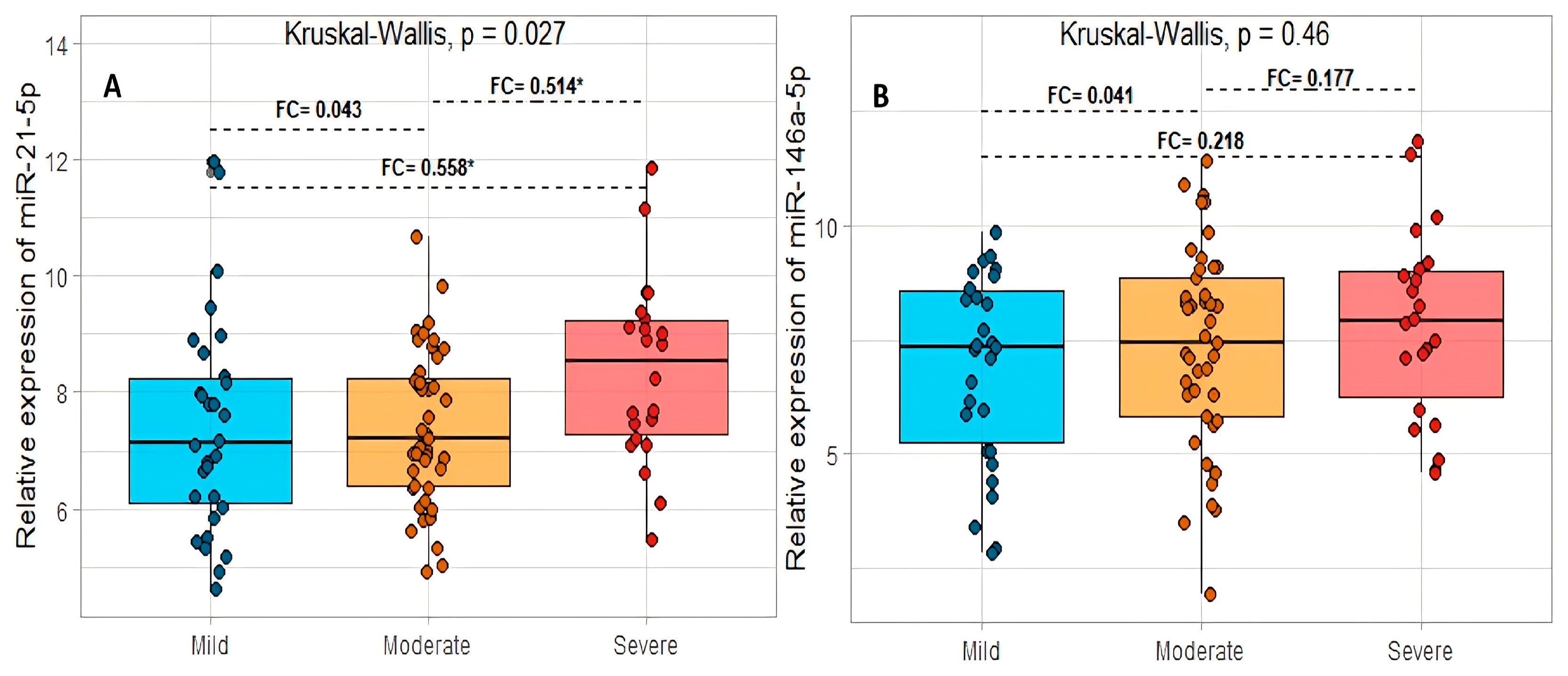
2.3. The miR-21-5p and miR-146a-5p and Their Relation to a Grade of Acute Respiratory Distress Syndrome in COVID-19
2.4. miRNA Relation to Comorbidities in Patients with Severe and Critical Disease in COVID-19
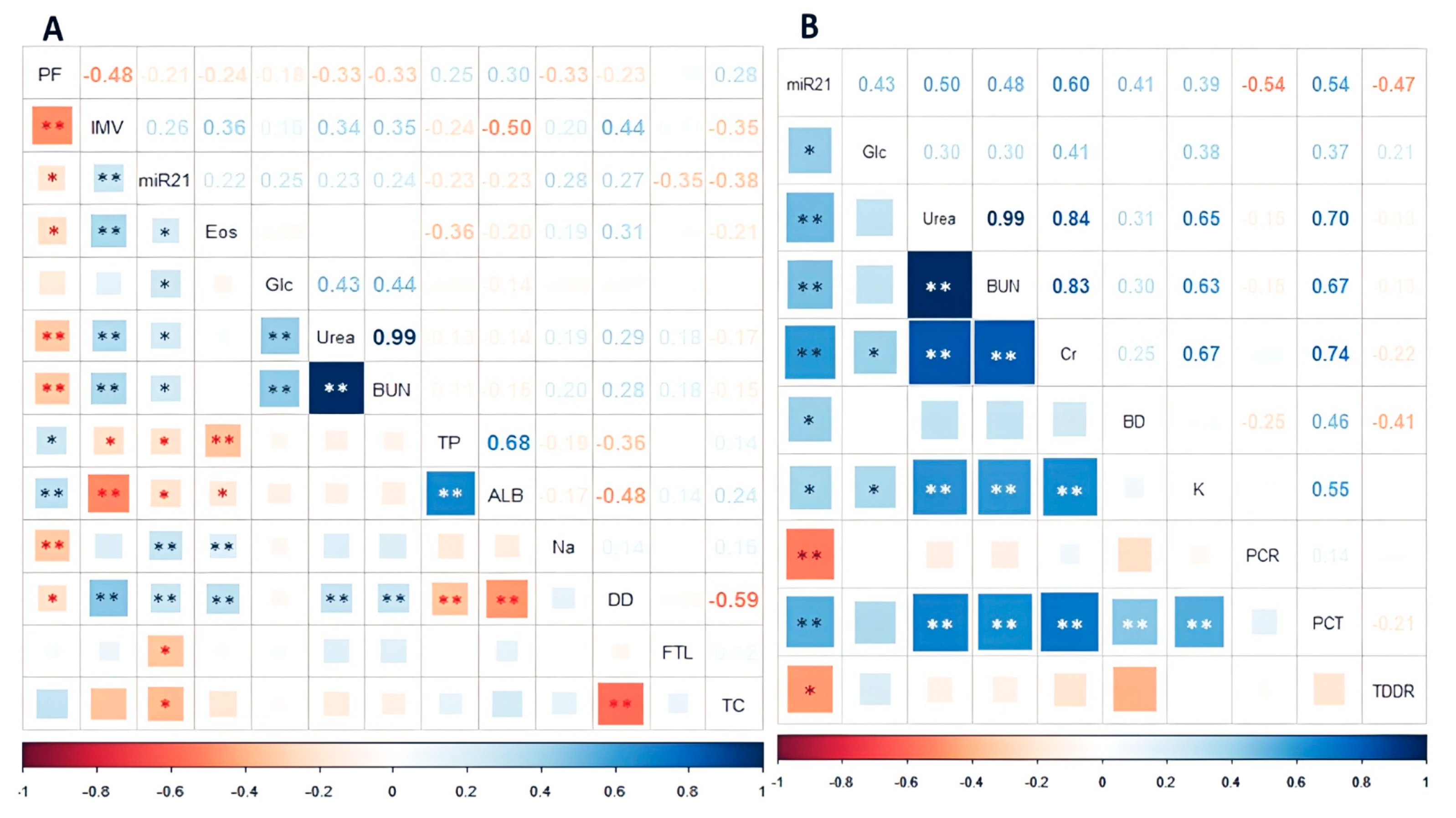
2.5. Correlation between miRNA Relative Expression and Clinical and Laboratory Variables
2.6. Receiver Operating Characteristic Curve Analysis of miR-21-5p and miR-146a-5p and Mortality in COVID-19 Patients
3. Discussion
4. Materials and Methods
4.1. Study Population
- Mild ARDS level: 200 mmHg < PaO2/FiO2 ≤ 300 mmHg.
- Moderate ARDS: 100 mmHg < PaO2/FiO2 ≤ 200 mmHg.
- Severe ARDS: PaO2/FiO2 ≤ 100 mmHg.
4.2. Statement of Ethics
4.3. Obtaining Blood Samples and RNA Isolation
4.4. RT-PCR and Polymerase Chain Reaction for miRNA Analysis
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mathieu, E.; Ritchie, H.; Rodés-Guirao, L.; Appel, C.; Gavrilov, D.; Giattino, C.; Hasell, J.; Macdonald, B.; Dattani, S.; Beltekian, D.; et al. Coronavirus Pandemic (COVID-19). Our World in Data 2020. Available online: https://ourworldindata.org/coronavirus (accessed on 6 October 2022).
- Grasselli, G.; Greco, M.; Zanella, A.; Albano, G.; Antonelli, M.; Bellani, G.; Bonanomi, E.; Cabrini, L.; Carlesso, E.; Castelli, G.; et al. Risk Factors Associated With Mortality Among Patients With COVID-19 in Intensive Care Units in Lombardy, Italy. JAMA Intern. Med. 2020, 180, 1345–1355. [Google Scholar] [CrossRef]
- Kim, L.; Garg, S.; O’halloran, A.; Whitaker, M.; Pham, H.; Anderson, E.J.; Armistead, I.; Bennett, N.M.; Billing, L.; Como-Sabetti, K.; et al. Risk Factors for Intensive Care Unit Admission and In-hospital Mortality Among Hospitalized Adults Identified through the US Coronavirus Disease 2019 (COVID-19)-Associated Hospitalization Surveillance Network (COVID-NET). Clin. Infect. Dis. 2020, 72, e206–e214. [Google Scholar] [CrossRef] [PubMed]
- Lighter, J.; Phillips, M.; Hochman, S.; Sterling, S.; Johnson, D.; Francois, F.; Stachel, A. Obesity in Patients Younger Than 60 Years Is a Risk Factor for COVID-19 Hospital Admission. Clin. Infect. Dis. 2020, 71, 896–897. [Google Scholar] [CrossRef]
- Mishra, R.; Kumar, A.; Ingle, H.; Kumar, H. The Interplay Between Viral-Derived miRNAs and Host Immunity During Infection. Front. Immunol. 2020, 10, 3079. [Google Scholar] [CrossRef]
- Silverio, A.; Di Maio, M.; Citro, R.; Esposito, L.; Iuliano, G.; Bellino, M.; Baldi, C.; De Luca, G.; Ciccarelli, M.; Vecchione, C.; et al. Cardiovascular risk factors and mortality in hospitalized patients with COVID-19: Systematic review and meta-analysis of 45 studies and 18,300 patients. BMC Cardiovasc. Disord. 2021, 21, 23. [Google Scholar] [CrossRef]
- Secretaría de Salud. Comunicados Técnicos Diarios COVID-19. 2021. Available online: https://www.gob.mx/salud/documentos/comunicados-tecnicos-diarios-covid19 (accessed on 24 July 2022).
- Secetarias Municipais e Estaduais de Saúde. Painel CoronaVirus. Ministério de Saúde. 2022. Available online: https://covid.saude.gov.br/ (accessed on 24 August 2022).
- Ministerio de Salud Chile. Plan de acción Coronavirus COVID-19. Red Pública de Salud Gratuita. 2022. Available online: https://www.minsal.cl/nuevo-coronavirus-2019-ncov/casos-confirmados-en-chile-covid-19/ (accessed on 23 August 2022).
- Baruch, P.J.; Aubert, R.; Ferrer, M.; Sanchez, L.; Dagorn, G.; Breteau, P. COVID-19: Le Tableau de Bord de l’epidémie. Les Décoderus 2022. Available online: https://www.lemonde.fr/les-decodeurs/article/2022/09/14/covid-19-le-tableau-de-bord-de-l-epidemie_6038751_4355775.html (accessed on 24 August 2022).
- Palacios, Y.; Ruiz, A.; Ramón-Luing, L.A.; Ocaña-Guzman, R.; Barreto-Rodriguez, O.; Sánchez-Monciváis, A.; Tecuatzi-Cadena, B.; Regalado-García, A.G.; Pineda-Gudiño, R.D.; García-Martínez, A.; et al. Severe COVID-19 Patients Show an Increase in Soluble TNFR1 and ADAM17, with a Relationship to Mortality. Int. J. Mol. Sci. 2021, 22, 8423. [Google Scholar] [CrossRef] [PubMed]
- Fricke-Galindo, I.; Martínez-Morales, A.; Chávez-Galán, L.; Ocaña-Guzmán, R.; Buendía-Roldán, I.; Pérez-Rubio, G.; Hernández-Zenteno, R.D.J.; Verónica-Aguilar, A.; Alarcón-Dionet, A.; Aguilar-Duran, H.; et al. IFNAR2 relevance in the clinical outcome of individuals with severe COVID-19. Front. Immunol. 2022, 13, 4031. [Google Scholar] [CrossRef]
- Fricke-Galindo, I.; Buendia-Roldan, I.; Chavez-Galan, L.; Pérez-Rubio, G.; Hernández-Zenteno, R.D.J.; Ramos-Martinez, E.; Zazueta-Márquez, A.; Reyes-Melendres, F.; Alarcón-Dionet, A.; Guzmán-Vargas, J.; et al. SERPINE1 rs6092 Variant Is Related to Plasma Coagulation Proteins in Patients with Severe COVID-19 from a Tertiary Care Hospital. Biology 2022, 11, 595. [Google Scholar] [CrossRef] [PubMed]
- Friedman, R.C.; Farh, K.K.-H.; Burge, C.B.; Bartel, D.P. Most mammalian mRNAs are conserved targets of microRNAs. Genome Res. 2009, 19, 92–105. [Google Scholar] [CrossRef]
- Krol, J.; Loedige, I.; Filipowicz, W. The widespread regulation of microRNA biogenesis, function and decay. Nat. Rev. Genet. 2010, 11, 597–610. [Google Scholar] [CrossRef]
- Keikha, R.; Hashemi-Shahri, S.M.; Jebali, A. The relative expression of miR-31, miR-29, miR-126, and miR-17 and their mRNA targets in the serum of COVID-19 patients with different grades during hospitalization. Eur. J. Med. Res. 2021, 26, 75. [Google Scholar] [CrossRef] [PubMed]
- de Gonzalo-Calvo, D.; Dávalos, A.; Montero, A.; García-González, A.; Tyshkovska, I.; González-Medina, A.; Soares, S.M.A.; Martínez-Camblor, P.; Casas-Agustench, P.; Rabadán, M.; et al. Circulating inflammatory miRNA signature in response to different doses of aerobic exercise. J. Appl. Physiol. 2015, 119, 124–134. [Google Scholar] [CrossRef]
- Bautista-Becerril, B.; Pérez-Dimas, G.; Sommerhalder-Nava, P.C.; Hanono, A.; Martínez-Cisneros, J.A.; Zarate-Maldonado, B.; Muñoz-Soria, E.; Aquino-Gálvez, A.; Castillejos-López, M.; Juárez-Cisneros, A.; et al. miRNAs, from Evolutionary Junk to Possible Prognostic Markers and Therapeutic Targets in COVID-19. Viruses 2021, 14, 41. [Google Scholar] [CrossRef] [PubMed]
- Donyavi, T.; Bokharaei-Salim, F.; Baghi, H.B.; Khanaliha, K.; Janat-Makan, M.A.; Karimi, B.; Nahand, J.S.; Mirzaei, H.; Khatami, A.; Garshasbi, S.; et al. Acute and post-acute phase of COVID-19: Analyzing expression patterns of miRNA-29a-3p, 146a-3p, 155–5p, and let-7b-3p in PBMC. Int. Immunopharmacol. 2021, 97, 107641. [Google Scholar] [CrossRef]
- Fayyad-Kazan, M.; Makki, R.; Skafi, N.; El Homsi, M.; Hamade, A.; El Majzoub, R.; Hamade, E.; Fayyad-Kazan, H.; Badran, B. Circulating miRNAs: Potential diagnostic role for coronavirus disease 2019 (COVID-19). Infect. Genet. Evol. 2021, 94, 105020. [Google Scholar] [CrossRef]
- Zhang, S.; Amahong, K.; Sun, X.; Lian, X.; Liu, J.; Sun, H.; Lou, Y.; Zhu, F.; Qiu, Y. The miRNA: A small but powerful RNA for COVID-19. Brief. Bioinform. 2021, 22, 1137–1149. [Google Scholar] [CrossRef]
- Garg, A.; Seeliger, B.; Derda, A.A.; Xiao, K.; Gietz, A.; Scherf, K.; Sonnenschein, K.; Pink, I.; Hoeper, M.M.; Welte, T.; et al. Circulating cardiovascular microRNAs in critically ill COVID-19 patients. Eur. J. Heart Fail. 2021, 23, 468–475. [Google Scholar] [CrossRef]
- Alizadehsani, R.; Sani, Z.A.; Behjati, M.; Roshanzamir, Z.; Hussain, S.; Abedini, N.; Hasanzadeh, F.; Khosravi, A.; Shoeibi, A.; Roshanzamir, M.; et al. Risk factors prediction, clinical outcomes, and mortality in COVID-19 patients. J. Med. Virol. 2020, 93, 2307–2320. [Google Scholar] [CrossRef]
- Dessie, Z.G.; Zewotir, T. Mortality-related risk factors of COVID-19: A systematic review and meta-analysis of 42 studies and 423,117 patients. BMC Infect. Dis. 2021, 21, 855. [Google Scholar] [CrossRef]
- Gao, Y.-D.; Ding, M.; Dong, X.; Zhang, J.-J.; Azkur, A.K.; Azkur, D.; Gan, H.; Sun, Y.-L.; Fu, W.; Li, W.; et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.; Gao, Y.; Li, Z.; Miao, Y.; Huang, Z.; Liu, X.; Xie, L.; Li, H.; Wen, W.; Zheng, Y.; et al. The noncoding and coding transcriptional landscape of the peripheral immune response in patients with COVID-19. Clin. Transl. Med. 2020, 10, e200. [Google Scholar] [CrossRef]
- Jiang, C.; Guo, Y.; Yu, H.; Lu, S.; Meng, L. Pleiotropic microRNA-21 in pulmonary remodeling: Novel insights for molecular mechanism and present advancements. Allergy Asthma Clin. Immunol. 2019, 15, 33. [Google Scholar] [CrossRef]
- Sheedy, F.J. Turning 21: Induction of miR-21 as a Key Switch in the Inflammatory Response. Front. Immunol. 2015, 6, 19. [Google Scholar] [CrossRef]
- Xue, Z.; Xi, Q.; Liu, H.; Guo, X.; Zhang, J.; Zhang, Z.; Li, Y.; Yang, G.; Zhou, D.; Yang, H.; et al. miR-21 promotes NLRP3 inflammasome activation to mediate pyroptosis and endotoxic shock. Cell Death Dis. 2019, 10, 461. [Google Scholar] [CrossRef]
- Sekar, D. Implications of microRNA 21 and its involvement in the treatment of different type of arthritis. Mol. Cell. Biochem. 2020, 476, 941–947. [Google Scholar] [CrossRef] [PubMed]
- Choi, B.; Kim, H.-A.; Suh, C.-H.; Byun, H.O.; Jung, J.-Y.; Sohn, S. The Relevance of miRNA-21 in HSV-Induced Inflammation in a Mouse Model. Int. J. Mol. Sci. 2015, 16, 7413–7427. [Google Scholar] [CrossRef] [PubMed]
- Kumarswamy, R.; Volkmann, I.; Thum, T. Regulation and function of miRNA-21 in health and disease. RNA Biol. 2011, 8, 706–713. [Google Scholar] [CrossRef]
- Peacock, O.; Lee, A.C.; Cameron, F.; Tarbox, R.; Vafadar-Isfahani, N.; Tufarelli, C.; Lund, J.N. Inflammation and MiR-21 Pathways Functionally Interact to Downregulate PDCD4 in Colorectal Cancer. PLoS ONE 2014, 9, e110267. [Google Scholar] [CrossRef]
- Hur, J.; Rhee, C.K.; Lee, S.Y.; Kim, Y.K.; Kang, J.Y. MicroRNA-21 inhibition attenuates airway inflammation and remodelling by modulating the transforming growth factor β–Smad7 pathway. Korean J. Intern. Med. 2021, 36, 706–720. [Google Scholar] [CrossRef] [PubMed]
- Bejerano, T.; Etzion, S.; Elyagon, S.; Etzion, Y.; Cohen, S. Nanoparticle Delivery of miRNA-21 Mimic to Cardiac Macrophages Improves Myocardial Remodeling after Myocardial Infarction. Nano Lett. 2018, 18, 5885–5891. [Google Scholar] [CrossRef]
- Hijmans, J.G.; Diehl, K.J.; Bammert, T.D.; Kavlich, P.J.; Lincenberg, G.M.; Greiner, J.J.; Stauffer, B.L.; DeSouza, C.A. Association between hypertension and circulating vascular-related microRNAs. J. Hum. Hypertens. 2018, 32, 440–447. [Google Scholar] [CrossRef]
- Roganović, J. Downregulation of microRNA-146a in diabetes, obesity and hypertension may contribute to severe COVID-19. Med. Hypotheses 2020, 146, 110448. [Google Scholar] [CrossRef]
- Lian, H.; Cai, H.; Zhang, H.; Ding, X.; Wang, X.; Zhang, S. The Prediction Value of D-Dimer on Prognosis in Intensive Care Unit among Old Patients (≥65 Years): A 9-Year Single-Center Retrospective Study of 9261 Cases. Oxidative Med. Cell. Longev. 2022, 2022, 2238985. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Karn, E.; Trivedi, K.; Kumar, P.; Chauhan, G.; Kumari, A.; Pant, P.; Munisamy, M.; Prakash, J.; Sarkar, P.G.; et al. Procalcitonin as a predictive marker in COVID-19: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0272840. [Google Scholar] [CrossRef]
- Minata, M.; Harada, K.H.; Yamaguchi, T.; Fujitani, T.; Nakagawa, H. Diabetes Mellitus May Exacerbate Liver Injury in Patients with COVID-19: A Single-Center, Observational, Retrospective Study. Diabetes Ther. 2022, 13, 1847–1860. [Google Scholar] [CrossRef] [PubMed]
- Smadja, D.M.; Fellous, B.A.; Bonnet, G.; Hauw-Berlemont, C.; Sutter, W.; Beauvais, A.; Fauvel, C.; Philippe, A.; Weizman, O.; Mika, D.; et al. D-dimer, BNP/NT-pro-BNP, and creatinine are reliable decision-making biomarkers in life-sustaining therapies withholding and withdrawing during COVID-19 outbreak. Front. Cardiovasc. Med. 2022, 9, 935333. [Google Scholar] [CrossRef] [PubMed]
- Pál, K.; Molnar, A.A.; Huțanu, A.; Szederjesi, J.; Branea, I.; Timár, Á.; Dobreanu, M. Inflammatory Biomarkers Associated with In-Hospital Mortality in Critical COVID-19 Patients. Int. J. Mol. Sci. 2022, 23, 10423. [Google Scholar] [CrossRef]
- Giannella, A.; Riccetti, S.; Sinigaglia, A.; Piubelli, C.; Razzaboni, E.; Di Battista, P.; Agostini, M.; Molin, E.D.; Manganelli, R.; Gobbi, F.; et al. Circulating microRNA signatures associated with disease severity and outcome in COVID-19 patients. Front. Immunol. 2022, 13, 968991. [Google Scholar] [CrossRef]
- Jenike, A.E.; Halushka, M.K. miR-21: A non-specific biomarker of all maladies. Biomark. Res. 2021, 9, 18. [Google Scholar] [CrossRef]
- Visacri, M.B.; Nicoletti, A.S.; Pincinato, E.C.; Loren, P.; Saavedra, N.; Saavedra, K.; Salazar, L.A.; Moriel, P. Role of miRNAs as biomarkers of COVID-19: A scoping review of the status and future directions for research in this field. Biomark. Med. 2021, 15, 1785–1795. [Google Scholar] [CrossRef]
- Gutiérrez-Pérez, I.A.; Buendía-Roldán, I.; Pérez-Rubio, G.; Chávez-Galán, L.; Hernández-Zenteno, R.D.J.; Aguilar-Duran, H.; Fricke-Galindo, I.; Zaragoza-García, O.; Falfán-Valencia, R.; Guzmán-Guzmán, I.P. Outcome predictors in COVID-19: An analysis of emergent systemic inflammation indices in Mexican population. Front. Med. 2022, 9, 1000147. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Gómez, B.; Leopoldo Rodríguez-Weber, F.; Díaz-Greene, E.J. Fisiología plaquetaria, agregometría plaquetaria y su utilidad clínica. Med. Interna Mex. 2018, 34, 244–263. [Google Scholar]
- Amezcua-Guerra, L.M. Anotaciones breves sobre el síndrome de liberación de citocinas y el bloqueo terapéutico de la interleucina-6 en SARS-CoV-2/COVID-19. Arch. Cardiol. Mex 2021, 90, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Dorrello, N.V.; Peschiaroli, A.; Guardavaccaro, D.; Colburn, N.H.; Sherman, N.E.; Pagano, M. S6K1- and βTRCP-Mediated Degradation of PDCD4 Promotes Protein Translation and Cell Growth. Science 2006, 314, 467–471. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, A.; Vencken, S.; De Santi, C.; Raoof, R.; Henshall, D.; Linnane, B.; McNally, P.; Greene, C. An investigation of miR-21 and the TLR4/PDCD4 axis in CF bronchial epithelium. Mol. Pathol. Funct. Genom. Eur. Respir. Soc. 2020, 56, 915. [Google Scholar] [CrossRef]
- Huang, G.; Yao, Q.; Ye, Z.; Huang, Y.; Zhang, C.; Jiang, Y.; Xi, X. Gender Differential Expression of AR/miR-21 Signaling Axis and Its Protective Effect on Renal Ischemia-Reperfusion Injury. Front. Cell Dev. Biol. 2022, 10, 861327. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Lu, C.; Qian, Y.; Li, H.; Tan, Y.; Cai, L.; Weng, H. Urinary miR-21 as a potential biomarker of hypertensive kidney injury and fibrosis. Sci. Rep. 2017, 7, 17737. [Google Scholar] [CrossRef]
- Chuppa, S.; Liang, M.; Liu, P.; Liu, Y.; Casati, M.C.; Cowley, A.W.; Patullo, L.; Kriegel, A.J. MicroRNA-21 regulates peroxisome proliferator–activated receptor alpha, a molecular mechanism of cardiac pathology in Cardiorenal Syndrome Type 4. Kidney Int. 2017, 93, 375–389. [Google Scholar] [CrossRef]
- Li, J.; Bai, J.; Tuerdi, N.; Liu, K. Long non-coding RNA MEG3 promotes tumor necrosis factor-alpha induced oxidative stress and apoptosis in interstitial cells of cajal via targeting the microRNA-21 /I-kappa-B-kinase beta axis. Bioengineered 2022, 13, 8676–8688. [Google Scholar] [CrossRef]
- Na, L.; Ding, H.; Xing, E.; Zhang, Y.; Gao, J.; Liu, B.; Yu, J.; Zhao, Y. The predictive value of microRNA-21 for sepsis risk and its correlation with disease severity, systemic inflammation, and 28-day mortality in sepsis patients. J. Clin. Lab. Anal. 2019, 34, e23103. [Google Scholar] [CrossRef]
- Burgos-Blasco, B.; Güemes-Villahoz, N.; Santiago, J.L.; Fernandez-Vigo, J.I.; Espino-Paisán, L.; Sarriá, B.; García-Feijoo, J.; Martinez-De-La-Casa, J.M. Hypercytokinemia in COVID-19: Tear cytokine profile in hospitalized COVID-19 patients. Exp. Eye Res. 2020, 200, 108253. [Google Scholar] [CrossRef] [PubMed]
- Lucas, C.; Wong, P.; Klein, J.; Castro, T.B.R.; Silva, J.; Sundaram, M.; Ellingson, M.K.; Mao, T.; Oh, J.E.; Israelow, B.; et al. Longitudinal analyses reveal immunological misfiring in severe COVID-19. Nature 2020, 584, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Bhimraj, A.; Morgan, R.L.; Hirsch Shumaker, A.; Baden, L.; Chi-Chung Cheng, V.; Edwards, K.M.; Gallagher, J.C.; Gandhi, R.T.; Muller, W.J.; Nakamura, M.M.; et al. IDSA Guidelines on the Treatment and Management of Patients with COVID-19. IDSA 2022. Available online: https://www.idsociety.org/practice-guideline/covid-19-guideline-treatment-and-management/ (accessed on 2 October 2022).
- World Health Organization. WHO Characterizes COVID-19 as a Pandemic. Pan American Health Organization 2020. Available online: https://www.paho.org/en/news/11-3-2020-who-characterizes-covid-19-pandemic (accessed on 19 March 2021).
- Kirschner, M.B.; Edelman, J.B.; Kao, S.C.-H.; Vallely, M.P.; Van Zandwijk, N.; Reid, G. The Impact of Hemolysis on Cell-Free microRNA Biomarkers. Front. Genet. 2013, 4, 94. [Google Scholar] [CrossRef] [PubMed]
- Kirschner, M.B.; Kao, S.C.; Edelman, J.J.; Armstrong, N.J.; Vallely, M.P.; van Zandwijk, N.; Reid, G. Haemolysis during Sample Preparation Alters microRNA Content of Plasma. PLoS ONE 2011, 6, e24145. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Severe n = 32 | Critical n = 65 | p-Value |
|---|---|---|---|
| Age, years | 41.5 (31–46) | 43 (38–52) | 0.047 |
| Sex (n, %) | |||
| Female | 11 (34.4) | 13 (20) | 0.139 |
| Male | 21 (65.6) | 52 (80) | |
| BMI, kg/m2 | 27.91 (24.55–30.39) | 29.40 (27.10–34.16) | 0.027 |
| BMI classification (n, %) | |||
| Normal weight | 12 (37.5) | 13 (20) | 0.084 |
| Overweight | 9 (28.1) | 20 (30.8) | 0.974 |
| Obesity | 11 (34.4) | 32 (49.2) | 0.196 |
| Symptoms onset, days | 8 (7–10) | 8 (7–12) | 0.266 |
| PaO2/FiO2 ratio | 210 (161–248) | 129 (80–169) | 0.001 |
| Classification PaO2/FiO2 ratio (n, %) | |||
| Mild | 18 (56.2) | 12 (18.5) | 0.003 |
| Moderate | 14 (43.8) | 31 (47.7) | 0.829 |
| Severe | 0 (0) | 22 (33.8) | 0.001 |
| Comorbidities | |||
| T2DM | 10 (31.3) | 15 (23.1) | 0.461 |
| SAH | 8 (25) | 14 (21.5) | 0.797 |
| Cardiovascular disease | 1 (3.1) | 1 (1.5) | 0.533 |
| Respiratory disease | 3 (9.4) | 1 (1.5) | 0.115 |
| Tobacco smoking | 11 (34.4) | 22 (33.8) | 0.566 |
| Characteristics | Survivors n = 65 | Non-Survivors n = 32 | p-Value |
|---|---|---|---|
| Age, years | 42 (32–48) | 48.5 (41–52) | 0.007 |
| Sex (n, %) | |||
| Female | 18 (27.7) | 6 (18.8) | 0.454 |
| Male | 47 (72.3) | 26 (81.2) | |
| PaO2/FiO2 ratio | 160 (106–225) | 143.65 (68.42–195) | 0.143 |
| Classification PaO2/FiO2 ratio (n, %) | |||
| Mild | 22 (33.8) | 8 (25) | 0.484 |
| Moderate | 31 (47.7) | 14 (43.8) | 0.829 |
| Severe | 12 (18.5) | 10 (31.3) | 0.198 |
| IMV | 32 (49.2) | 32 (100) | 0.001 |
| Length IMV, days | 6 (1–16) | 23.50 (15–34) | 0.001 |
| miR-21-5p | ||||
| Variable | Cut-Off | Odds Ratio | 95% CI | p-Value |
| Mortality | 8.237 | 4.129 | 1.658–10.227 | 0.020 |
| Severity | 8.191 | 5.639 | 1.774–17.914 | 0.002 |
| Need of IMV | 8.191 | 6.007 | 1.892–19.075 | 0.001 |
| miR-146a-5p | ||||
| Variable | Cut-Off | Odds Ratio | 95% CI | p-Value |
| Mortality | 5.884 | 2.577 | 0.869–7.640 | 0.081 |
| Severity | 9.148 | 2.654 | 0.703–10.010 | 0.138 |
| Need of IMV | 4.851 | 2.480 | 0.755–6.696 | 0.140 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bautista-Becerril, B.; Nava-Quiroz, K.J.; Muñoz-Soria, E.; Camarena, Á.; Fricke-Galindo, I.; Buendia-Roldan, I.; Pérez-Rubio, G.; Chavez-Galán, L.; Pérez-Torres, K.; Téllez-Quijada, F.; et al. High Expression Levels of miR-21-5p in Younger Hospitalized COVID-19 Patients Are Associated with Mortality and Critical Disease. Int. J. Mol. Sci. 2023, 24, 10112. https://doi.org/10.3390/ijms241210112
Bautista-Becerril B, Nava-Quiroz KJ, Muñoz-Soria E, Camarena Á, Fricke-Galindo I, Buendia-Roldan I, Pérez-Rubio G, Chavez-Galán L, Pérez-Torres K, Téllez-Quijada F, et al. High Expression Levels of miR-21-5p in Younger Hospitalized COVID-19 Patients Are Associated with Mortality and Critical Disease. International Journal of Molecular Sciences. 2023; 24(12):10112. https://doi.org/10.3390/ijms241210112
Chicago/Turabian StyleBautista-Becerril, Brandon, Karol J. Nava-Quiroz, Evangelina Muñoz-Soria, Ángel Camarena, Ingrid Fricke-Galindo, Ivette Buendia-Roldan, Gloria Pérez-Rubio, Leslie Chavez-Galán, Karina Pérez-Torres, Fernanda Téllez-Quijada, and et al. 2023. "High Expression Levels of miR-21-5p in Younger Hospitalized COVID-19 Patients Are Associated with Mortality and Critical Disease" International Journal of Molecular Sciences 24, no. 12: 10112. https://doi.org/10.3390/ijms241210112
APA StyleBautista-Becerril, B., Nava-Quiroz, K. J., Muñoz-Soria, E., Camarena, Á., Fricke-Galindo, I., Buendia-Roldan, I., Pérez-Rubio, G., Chavez-Galán, L., Pérez-Torres, K., Téllez-Quijada, F., Márquez-García, E., Moncada-Morales, A., Hernández-Zenteno, R. d. J., Jaime-Capetillo, M. E., & Falfán-Valencia, R. (2023). High Expression Levels of miR-21-5p in Younger Hospitalized COVID-19 Patients Are Associated with Mortality and Critical Disease. International Journal of Molecular Sciences, 24(12), 10112. https://doi.org/10.3390/ijms241210112