
In Vitro and In Vivo Evaluation of Injectable Strontium-Modified Calcium Phosphate Cement for Bone Defect Repair in Rats
 , ,
, ,
Abstract
1. Introduction
2. Results
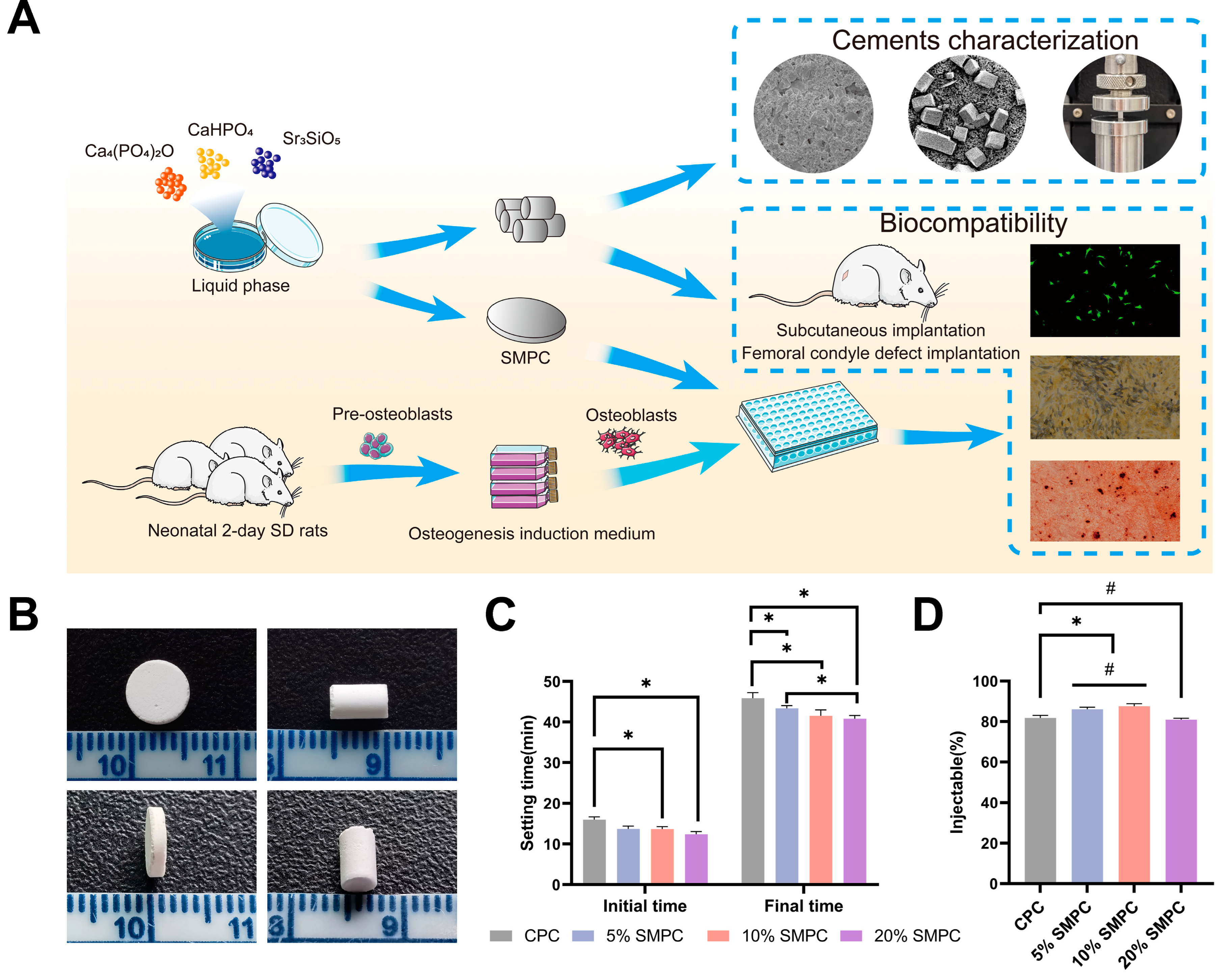
2.1. Cement Production, Setting Time, and Injectability
2.2. Phase Composition
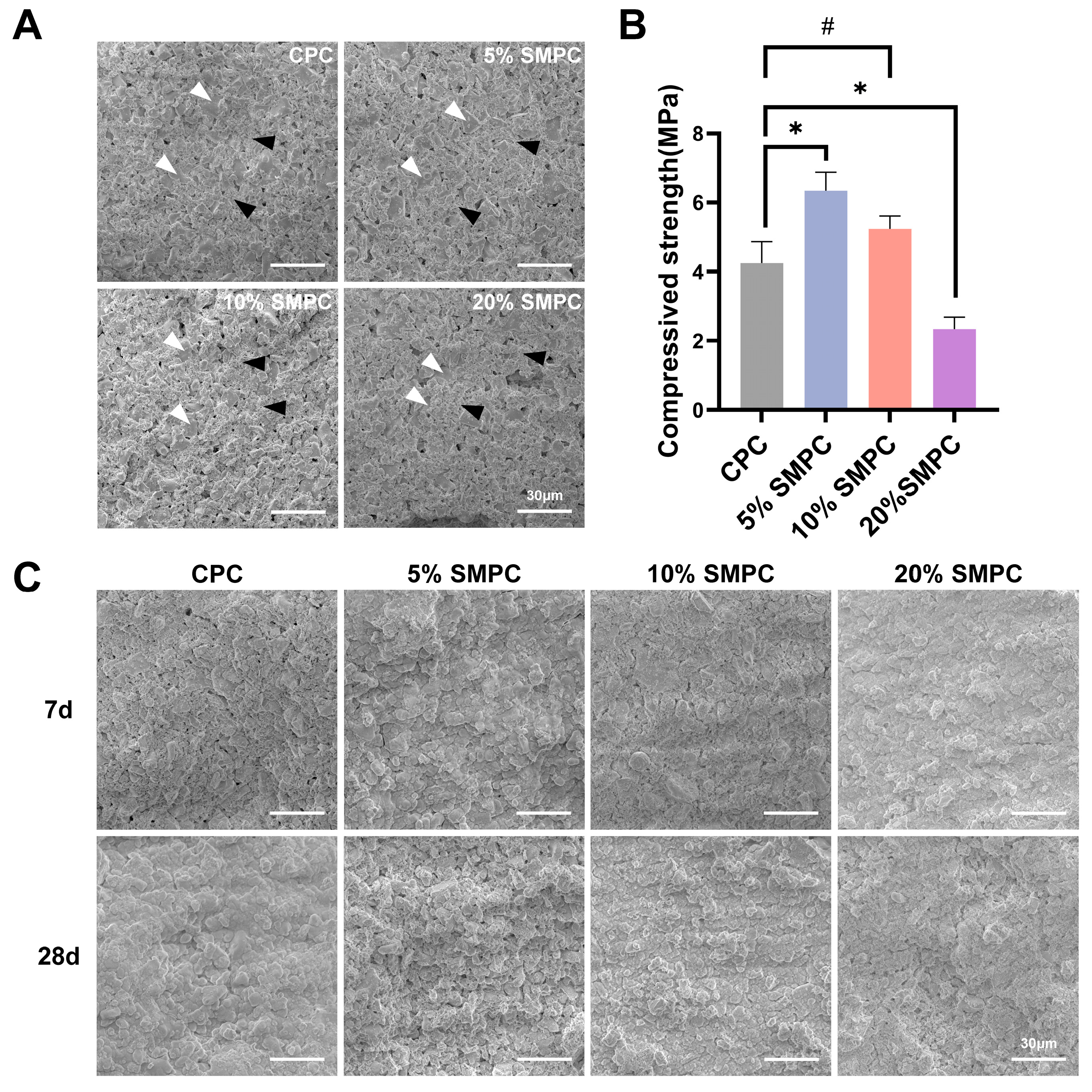
2.3. Microstructure and Mechanical Properties of Cements
2.4. Degradation and Biomineralization In Vitro
2.5. Toxicity and Adhesion Assessments
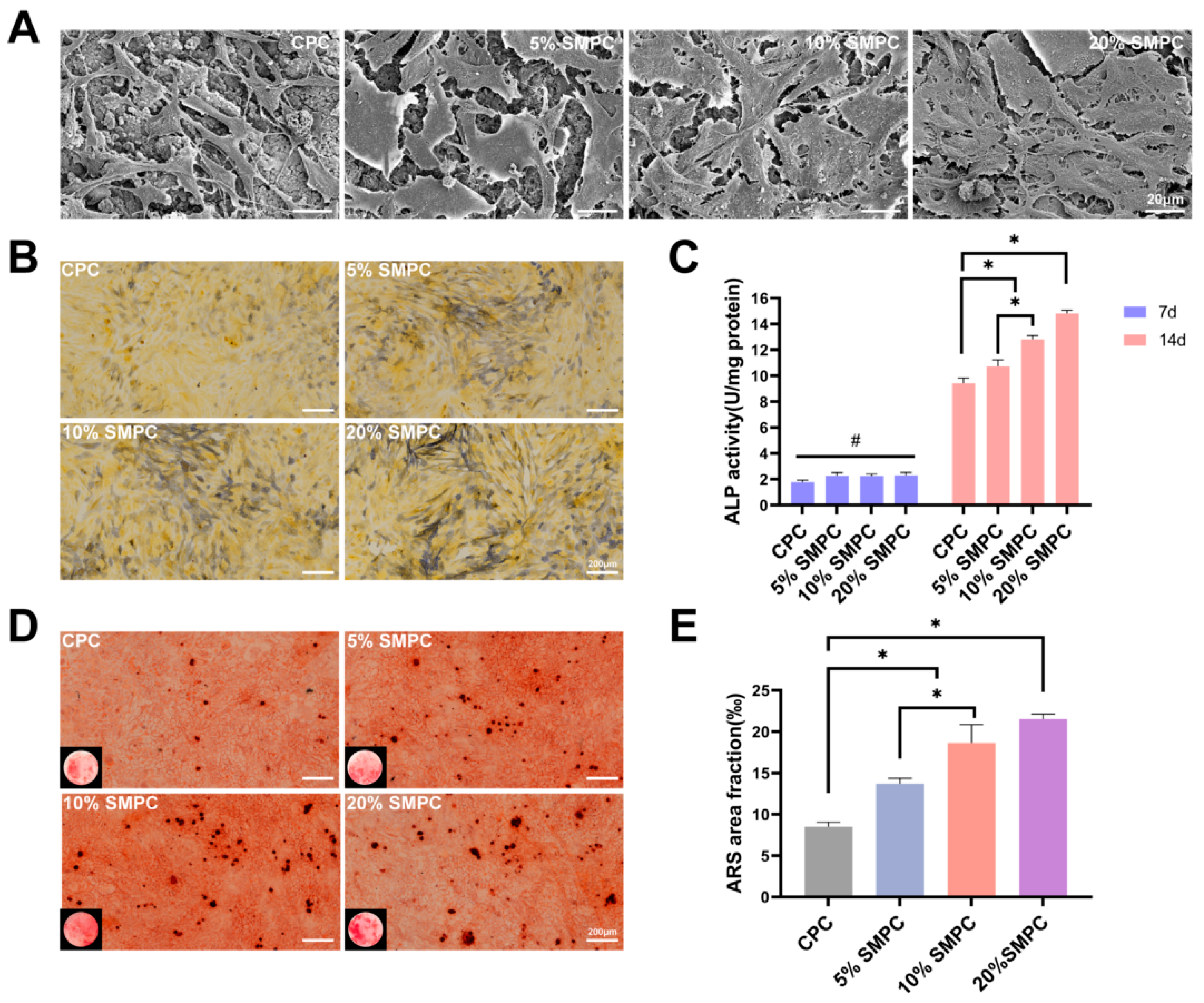
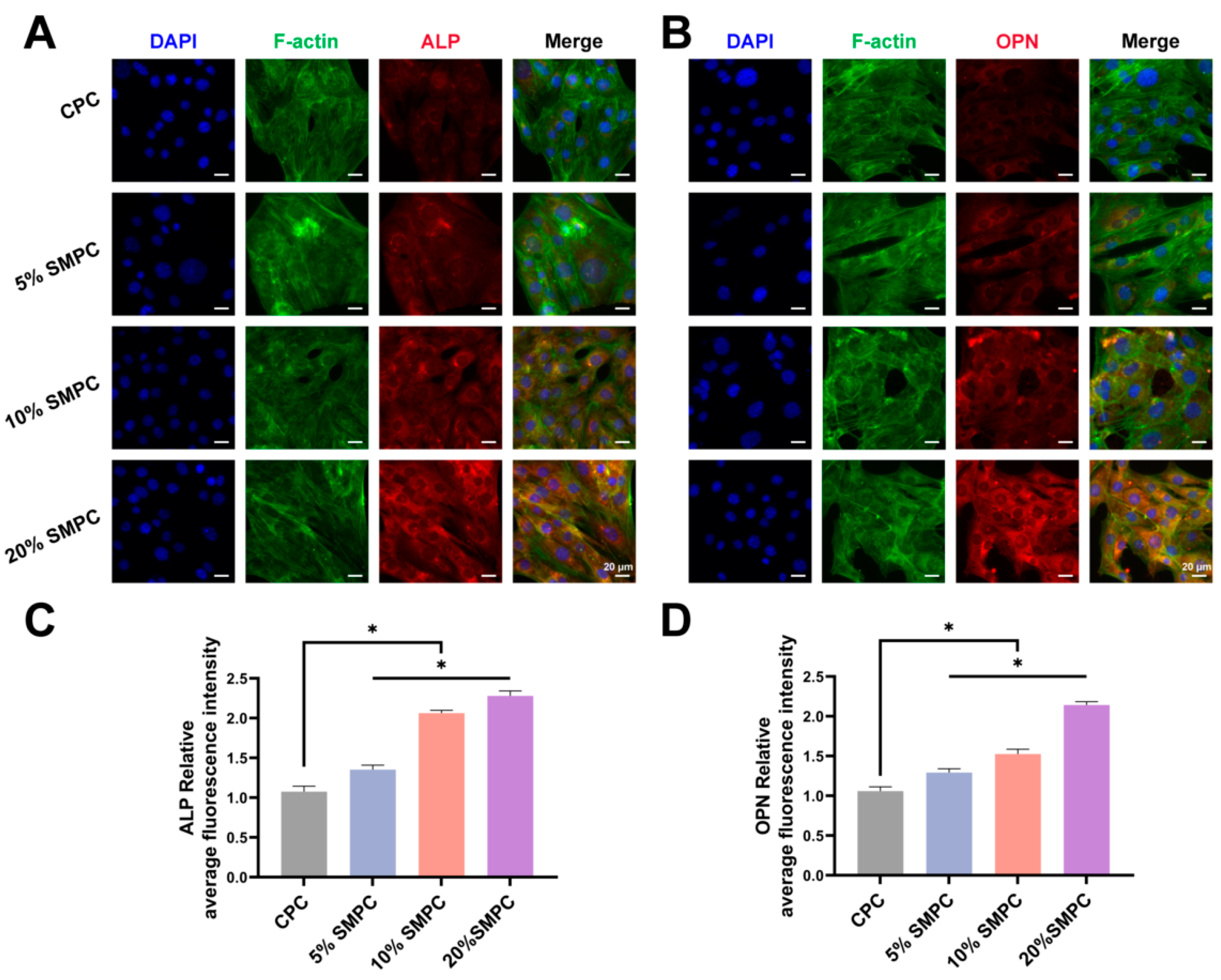
2.6. Proliferation and Osteogenic Capability Test
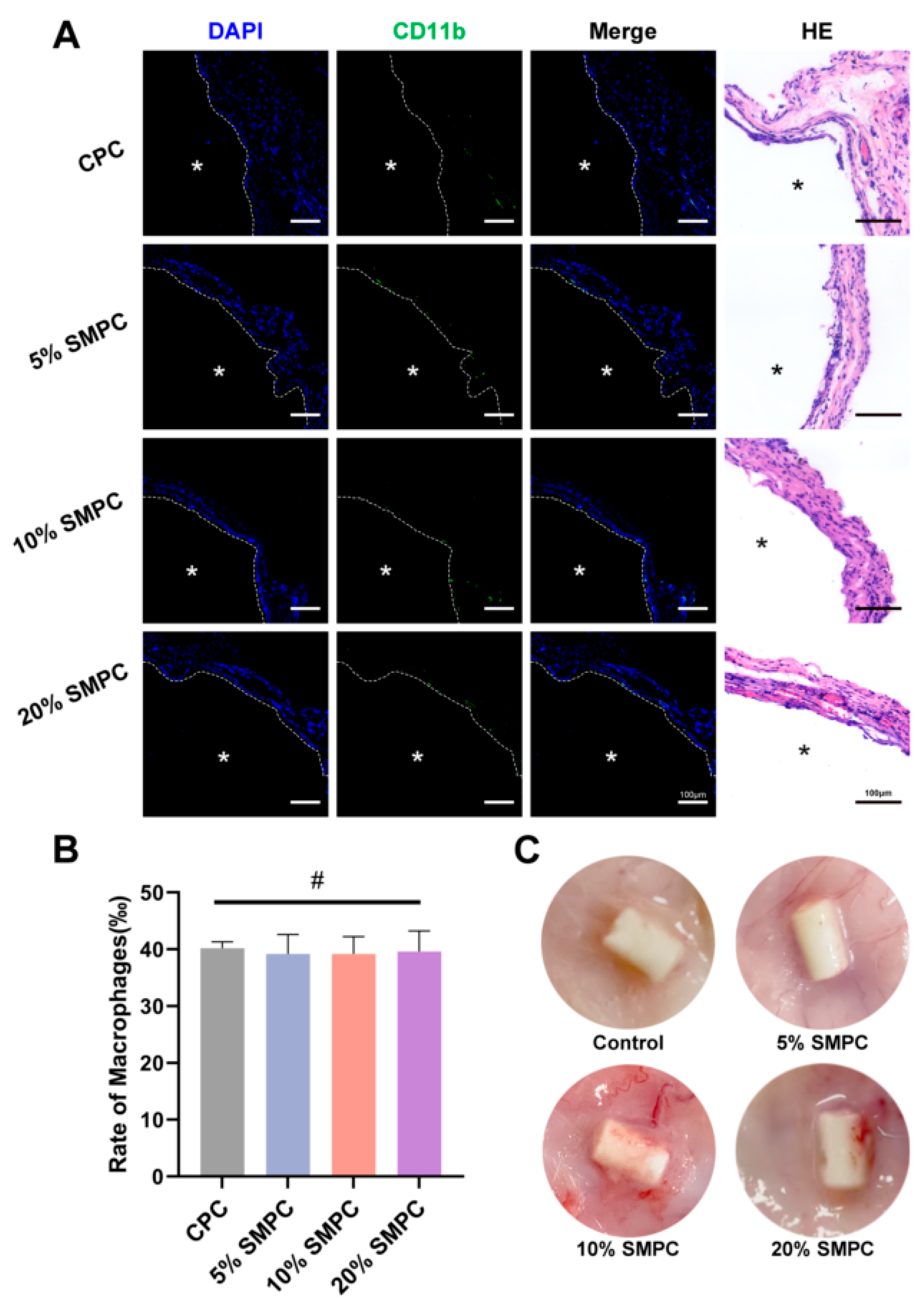
2.7. Local Inflammatory Response
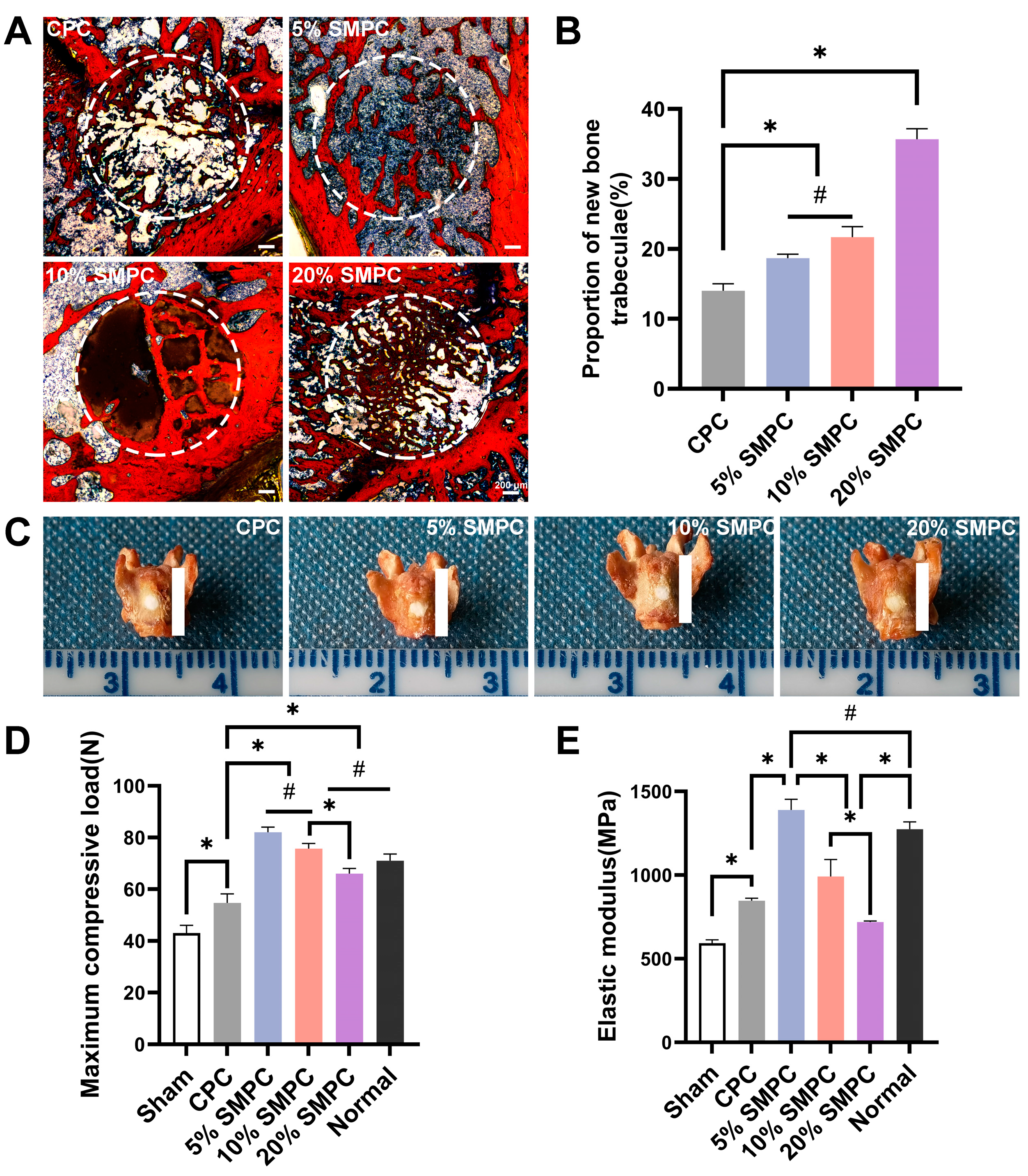
2.8. Osteogenic Ability Assessment In Vivo
2.9. Biomechanical Properties of Isolated Bone
3. Discussion
4. Materials and Methods
4.1. Fabrication of the CPC and SMPC
4.2. Characterization of Cement
4.2.1. Setting Time and Injectability
4.2.2. X-ray Diffraction and Mechanical Characterization
4.2.3. In Vitro Degradation and Biomineralization
4.3. Biocompatibility and Osteogenic Differentiation In Vitro
4.3.1. Osteoblast Culture
4.3.2. Cell Proliferation and Viability
4.3.3. Alkaline Phosphatase (ALP) Activity and Staining
4.3.4. Cell Adhesion and Microstructure
4.3.5. Alizarin Red S Staining
4.3.6. Immunofluorescence Analysis
4.4. In Vivo Experiments
4.4.1. Animal Surgery
4.4.2. Biomechanical Testing of Isolated Bone
4.4.3. Histological and Immunofluorescence Analysis
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Buchbinder, R.; Johnston, R.V.; Rischin, K.J.; Homik, J.; Jones, C.A.; Golmohammadi, K.; Kallmes, D.F. Percutaneous vertebroplasty for osteoporotic vertebral compression fracture. Cochrane Database Syst. Rev. 2018, 4, CD006349. [Google Scholar] [CrossRef] [PubMed]
- Ballane, G.; Cauley, J.A.; Luckey, M.M.; El-Hajj Fuleihan, G. Worldwide prevalence and incidence of osteoporotic vertebral fractures. Osteoporo.s Int. 2017, 28, 1531–1542. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, C.L.; Chutkan, N.B.; Choma, T.J.; Orr, R.D. Management of the Elderly With Vertebral Compression Fractures. Neurosurgery 2015, 77 (Suppl. S4), S33–S45. [Google Scholar] [CrossRef] [PubMed]
- Szczesny, G.; Kopec, M.; Politis, D.J.; Kowalewski, Z.L.; Lazarski, A.; Szolc, T. A Review on Biomaterials for Orthopaedic Surgery and Traumatology: From Past to Present. Materials 2022, 15, 3622. [Google Scholar] [CrossRef]
- Lu, Q.; Liu, C.; Wang, D.; Liu, H.; Yang, H.; Yang, L. Biomechanical evaluation of calcium phosphate-based nanocomposite versus polymethylmethacrylate cement for percutaneous kyphoplasty. Spine J. 2019, 19, 1871–1884. [Google Scholar] [CrossRef]
- Belkoff, S.M.; Molloy, S. Temperature measurement during polymerization of polymethylmethacrylate cement used for vertebroplasty. Spine 2003, 28, 1555–1559. [Google Scholar] [CrossRef]
- Grafe, I.A.; Baier, M.; Noldge, G.; Weiss, C.; Da Fonseca, K.; Hillmeier, J.; Libicher, M.; Rudofsky, G.; Metzner, C.; Nawroth, P.; et al. Calcium-phosphate and polymethylmethacrylate cement in long-term outcome after kyphoplasty of painful osteoporotic vertebral fractures. Spine 2008, 33, 1284–1290. [Google Scholar] [CrossRef]
- Legeros, R.Z. Apatite calcium phosphate: Possible restrative materials. J. Dent. Res. 1982, 61, 343. [Google Scholar]
- Brown, W.E. A new calcium phosphate settimg cement. J. Dent. Res. 1983, 62, 672. [Google Scholar]
- Weiner, S.; Traub, W. Bone structure: From angstroms to microns. Faseb. J. 1992, 6, 879–885. [Google Scholar] [CrossRef]
- Rho, J.Y.; Kuhn-Spearing, L.; Zioupos, P. Mechanical properties and the hierarchical structure of bone. Med. Eng. Phys. 1998, 20, 92–102. [Google Scholar] [CrossRef] [PubMed]
- Schroter, L.; Kaiser, F.; Stein, S.; Gbureck, U.; Ignatius, A. Biological and mechanical performance and degradation characteristics of calcium phosphate cements in large animals and humans. Acta. Biomater. 2020, 117, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Zhao, L.; Chen, W.; Liu, X.; Weir, M.D.; Xu, H.H. Stem Cells and Calcium Phosphate Cement Scaffolds for Bone Regeneration. J. Dent. Res. 2014, 93, 618–625. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.H.; Wang, P.; Wang, L.; Bao, C.; Chen, Q.; Weir, M.D.; Chow, L.C.; Zhao, L.; Zhou, X.; Reynolds, M.A. Calcium phosphate cements for bone engineering and their biological properties. Bone. Res. 2017, 5, 17056. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Huang, S.; Zou, R.; Gao, X.; Ruan, J.; Weir, M.D.; Reynolds, M.A.; Qin, W.; Chang, X.; Fu, H.; et al. Calcium phosphate cement scaffold with stem cell co-culture and prevascularization for dental and craniofacial bone tissue engineering. Dent. Mater. 2019, 35, 1031–1041. [Google Scholar] [CrossRef]
- Chen, W.; Thein-Han, W.; Weir, M.D.; Chen, Q.; Xu, H.H. Prevascularization of biofunctional calcium phosphate cement for dental and craniofacial repairs. Dent. Mater. 2014, 30, 535–544. [Google Scholar] [CrossRef]
- Jeong, J.; Kim, J.H.; Shim, J.H.; Hwang, N.S.; Heo, C.Y. Bioactive calcium phosphate materials and applications in bone regeneration. Biomater. Res. 2019, 23, 4. [Google Scholar] [CrossRef]
- Samavedi, S.; Whittington, A.R.; Goldstein, A.S. Calcium phosphate ceramics in bone tissue engineering: A review of properties and their influence on cell behavior. Acta. Biomater. 2013, 9, 8037–8045. [Google Scholar] [CrossRef]
- Zuo, Y.; Yang, F.; Wolke, J.G.; Li, Y.; Jansen, J.A. Incorporation of biodegradable electrospun fibers into calcium phosphate cement for bone regeneration. Acta. Biomater. 2010, 6, 1238–1247. [Google Scholar] [CrossRef]
- Wu, J.; Jiang, L.J.; Ju, L.P.; Zhang, Y.; Li, M.; Liu, X.; Qu, X.Y. A novel compound bone articular repair material combining deproteinized osteoarticulation with calcium phosphate cement and BMP-9. Mater. Des. 2021, 210, 110021. [Google Scholar] [CrossRef]
- Ruhe, P.Q.; Kroese-Deutman, H.C.; Wolke, J.G.; Spauwen, P.H.; Jansen, J.A. Bone inductive properties of rhBMP-2 loaded porous calcium phosphate cement implants in cranial defects in rabbits. Biomaterials 2004, 25, 2123–2132. [Google Scholar] [CrossRef] [PubMed]
- Kroese-Deutman, H.C.; Ruhe, P.Q.; Spauwen, P.H.; Jansen, J.A. Bone inductive properties of rhBMP-2 loaded porous calcium phosphate cement implants inserted at an ectopic site in rabbits. Biomaterials 2005, 26, 1131–1138. [Google Scholar] [CrossRef] [PubMed]
- Felix-Ilemhenbhio, F.; Pickering, G.A.E.; Kiss-Toth, E.; Wilkinson, J.M. Pathophysiology and Emerging Molecular Therapeutic Targets in Heterotopic Ossification. Int. J. Mol. Sci. 2022, 23, 6983. [Google Scholar] [CrossRef]
- Link, D.P.; van den Dolder, J.; Jurgens, W.J.; Wolke, J.G.; Jansen, J.A. Mechanical evaluation of implanted calcium phosphate cement incorporated with PLGA microparticles. Biomaterials 2006, 27, 4941–4947. [Google Scholar] [CrossRef]
- Liao, H.; Walboomers, X.F.; Habraken, W.J.; Zhang, Z.; Li, Y.; Grijpma, D.W.; Mikos, A.G.; Wolke, J.G.; Jansen, J.A. Injectable calcium phosphate cement with PLGA, gelatin and PTMC microspheres in a rabbit femoral defect. Acta. Biomater. 2011, 7, 1752–1759. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Wang, K.; Ma, T.; Huang, L.; Xia, B.; Zhu, S.; Yang, Y.; Liu, Z.; Quan, X.; Luo, K.; et al. Noncovalent Bonding of RGD and YIGSR to an Electrospun Poly(epsilon-Caprolactone) Conduit through Peptide Self-Assembly to Synergistically Promote Sciatic Nerve Regeneration in Rats. Adv. Health Mater. 2017, 6, 1600860. [Google Scholar] [CrossRef] [PubMed]
- Versieck, J. Trace elements in human body fluids and tissues. Crit. Rev. Clin. Lab. Sci. 1985, 22, 97–184. [Google Scholar] [CrossRef]
- Zhang, J.; Ma, X.; Lin, D.; Shi, H.; Yuan, Y.; Tang, W.; Zhou, H.; Guo, H.; Qian, J.; Liu, C. Magnesium modification of a calcium phosphate cement alters bone marrow stromal cell behavior via an integrin-mediated mechanism. Biomaterials 2015, 53, 251–264. [Google Scholar] [CrossRef]
- Tan, S.; Wang, Y.; Du, Y.; Xiao, Y.; Zhang, S. Injectable bone cement with magnesium-containing microspheres enhances osteogenesis via anti-inflammatory immunoregulation. Bioact. Mater. 2021, 6, 3411–3423. [Google Scholar] [CrossRef]
- Kuhlmann, J.; Bartsch, I.; Willbold, E.; Schuchardt, S.; Holz, O.; Hort, N.; Hoche, D.; Heineman, W.R.; Witte, F. Fast escape of hydrogen from gas cavities around corroding magnesium implants. Acta. Biomater. 2013, 9, 8714–8721. [Google Scholar] [CrossRef]
- Lu, T.; Zhang, J.; Yuan, X.; Tang, C.; Wang, X.; Zhang, Y.; Xiong, K.; Ye, J. Enhanced osteogenesis and angiogenesis of calcium phosphate cement incorporated with zinc silicate by synergy effect of zinc and silicon ions. Mater. Sci. Eng. C Mater. Biol. Appl. 2021, 131, 112490. [Google Scholar] [CrossRef] [PubMed]
- Xue, W.; Dahlquist, K.; Banerjee, A.; Bandyopadhyay, A.; Bose, S. Synthesis and characterization of tricalcium phosphate with Zn and Mg based dopants. J. Mater. Sci. Mater. Med. 2008, 19, 2669–2677. [Google Scholar] [CrossRef] [PubMed]
- Fosmire, G.J. Zinc toxicity. Am. J. Clin. Nutr. 1990, 51, 225–227. [Google Scholar] [CrossRef] [PubMed]
- Lode, A.; Heiss, C.; Knapp, G.; Thomas, J.; Nies, B.; Gelinsky, M.; Schumacher, M. Strontium-modified premixed calcium phosphate cements for the therapy of osteoporotic bone defects. Acta. Biomater. 2018, 65, 475–485. [Google Scholar] [CrossRef] [PubMed]
- Bonnelye, E.; Chabadel, A.; Saltel, F.; Jurdic, P. Dual effect of strontium ranelate: Stimulation of osteoblast differentiation and inhibition of osteoclast formation and resorption in vitro. Bone 2008, 42, 129–138. [Google Scholar] [CrossRef]
- Chen, F.; Tian, L.; Pu, X.; Zeng, Q.; Xiao, Y.; Chen, X.; Zhang, X. Enhanced ectopic bone formation by strontium-substituted calcium phosphate ceramics through regulation of osteoclastogenesis and osteoblastogenesis. Biomater. Sci. 2022, 10, 5925–5937. [Google Scholar] [CrossRef]
- Lavet, C.; Mabilleau, G.; Chappard, D.; Rizzoli, R.; Ammann, P. Strontium ranelate stimulates trabecular bone formation in a rat tibial bone defect healing process. Osteoporos. Int. 2017, 28, 3475–3487. [Google Scholar] [CrossRef]
- O’Donnell, S.; Cranney, A.; Wells, G.A.; Adachi, J.D.; Reginster, J.Y. Strontium ranelate for preventing and treating postmenopausal osteoporosis. Cochrane Database Syst. Rev. 2006, 4, CD005326. [Google Scholar] [CrossRef]
- Singh, S.S.; Roy, A.; Lee, B.; Parekh, S.; Kumta, P.N. Murine osteoblastic and osteoclastic differentiation on strontium releasing hydroxyapatite forming cements. Mater. Sci. Eng. C Mater. Biol. Appl. 2016, 63, 429–438. [Google Scholar] [CrossRef]
- Guo, X.; Wei, S.; Lu, M.; Shao, Z.; Lu, J.; Xia, L.; Lin, K.; Zou, D. Dose-dependent Effects of Strontium Ranelate on Ovariectomy Rat Bone Marrow Mesenchymal Stem Cells and Human Umbilical Vein Endothelial Cells. Int. J. Biol. Sci. 2016, 12, 1511–1522. [Google Scholar] [CrossRef]
- Zhang, J.; Liu, W.; Schnitzler, V.; Tancret, F.; Bouler, J.M. Calcium phosphate cements for bone substitution: Chemistry, handling and mechanical properties. Acta. Biomater. 2014, 10, 1035–1049. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Engqvist, H.; Persson, C. A ready-to-use acidic, brushite-forming calcium phosphate cement. Acta. Biomater. 2018, 81, 304–314. [Google Scholar] [CrossRef] [PubMed]
- del Real, R.P.; Wolke, J.G.; Vallet-Regi, M.; Jansen, J.A. A new method to produce macropores in calcium phosphate cements. Biomaterials 2002, 23, 3673–3680. [Google Scholar] [CrossRef]
- Nouda, S.; Tomita, S.; Kin, A.; Kawahara, K.; Kinoshita, M. Adjacent vertebral body fracture following vertebroplasty with polymethylmethacrylate or calcium phosphate cement: Biomechanical evaluation of the cadaveric spine. Spine 2009, 34, 2613–2618. [Google Scholar] [CrossRef]
- Schumacher, M.; Henss, A.; Rohnke, M.; Gelinsky, M. A novel and easy-to-prepare strontium(II) modified calcium phosphate bone cement with enhanced mechanical properties. Acta. Biomater. 2013, 9, 7536–7544. [Google Scholar] [CrossRef] [PubMed]
- Hamdan Alkhraisat, M.; Moseke, C.; Blanco, L.; Barralet, J.E.; Lopez-Carbacos, E.; Gbureck, U. Strontium modified biocements with zero order release kinetics. Biomaterials 2008, 29, 4691–4697. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Tang, Z.; Wu, K.; Bai, Y.; Lin, X.; Yang, H.; Yang, Q.; Wang, Z.; Ni, X.; Liu, H.; et al. Strontium-calcium phosphate hybrid cement with enhanced osteogenic and angiogenic properties for vascularised bone regeneration. J. Mater. Chem. B 2021, 9, 5982–5997. [Google Scholar] [CrossRef]
- Masaeli, R.; Jafarzadeh Kashi, T.S.; Dinarvand, R.; Rakhshan, V.; Shahoon, H.; Hooshmand, B.; Mashhadi Abbas, F.; Raz, M.; Rajabnejad, A.; Eslami, H.; et al. Efficacy of the biomaterials 3wt%-nanostrontium-hydroxyapatite-enhanced calcium phosphate cement (nanoSr-CPC) and nanoSr-CPC-incorporated simvastatin-loaded poly(lactic-co-glycolic-acid) microspheres in osteogenesis improvement: An explorative multi-phase experimental in vitro/vivo study. Mater. Sci. Eng. C Mater. Biol. Appl. 2016, 69, 171–183. [Google Scholar] [CrossRef]
- D’Onofrio, A.; Kent, N.W.; Shahdad, S.A.; Hill, R.G. Development of novel strontium containing bioactive glass based calcium phosphate cement. Dent. Mater. 2016, 32, 703–712. [Google Scholar] [CrossRef]
- Lin, Z.; Cao, Y.; Zou, J.; Zhu, F.; Gao, Y.; Zheng, X.; Wang, H.; Zhang, T.; Wu, T. Improved osteogenesis and angiogenesis of a novel copper ions doped calcium phosphate cement. Mater. Sci. Eng. C Mater. Biol. Appl. 2020, 114, 111032. [Google Scholar] [CrossRef]
- Kolodziejska, B.; Stepien, N.; Kolmas, J. The Influence of Strontium on Bone Tissue Metabolism and Its Application in Osteoporosis Treatment. Int. J. Mol. Sci. 2021, 22, 6564. [Google Scholar] [CrossRef] [PubMed]
- Geng, Y.; Mosyak, L.; Kurinov, I.; Zuo, H.; Sturchler, E.; Cheng, T.C.; Subramanyam, P.; Brown, A.P.; Brennan, S.C.; Mun, H.C.; et al. Structural mechanism of ligand activation in human calcium-sensing receptor. Elife 2016, 5, e13662. [Google Scholar] [CrossRef] [PubMed]
- Mountziaris, P.M.; Spicer, P.P.; Kasper, F.K.; Mikos, A.G. Harnessing and modulating inflammation in strategies for bone regeneration. Tissue Eng. Part B Rev. 2011, 17, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Jia, S.; Tian, F.; Gao, X.; Wang, Z.; Zhu, L.; Hao, D. Effects of calcium phosphate cement combined with hyaluronic acid/curcumin on the proliferation and osteogenesis of osteoblasts. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2021, 35, 104–110. [Google Scholar] [CrossRef]
- Zhu, L.; Jia, S.J.; Liu, T.J.; Yan, L.; Huang, D.G.; Wang, Z.Y.; Chen, S.; Zhang, Z.P.; Zeng, W.; Zhang, Y.; et al. Aligned PCL Fiber Conduits Immobilized with Nerve Growth Factor Gradients Enhance and Direct Sciatic Nerve Regeneration. Adv. Funct. Mater. 2020, 30, 2002610. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample | Sr (Atomic %) | P (Atomic %) | Ca (Atomic %) | Si (Atomic %) |
|---|---|---|---|---|
| Control (CPC) | - | 37.45 | 62.55 | - |
| 5% SMPC | 7.52 | 33.74 | 56.37 | 2.37 |
| 10% SMPC | 7.78 | 31.93 | 57.81 | 2.48 |
| 20% SMPC | 8.17 | 30.76 | 58.45 | 2.62 |
| Sample | TTCP (wt%) | DCPA (wt%) | TS (wt%) |
|---|---|---|---|
| Control (CPC) | 72.91 | 27.09 | ─ |
| 5% SMPC | 69.27 | 35.73 | 5.00 |
| 10% SMPC | 65.62 | 24.38 | 10.00 |
| 20% SMPC | 58.33 | 21.67 | 20.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, H.; Zhu, L.; Tian, F.; Wang, C.; Wu, W.; Lu, B.; Yan, L.; Jia, S.; Hao, D. In Vitro and In Vivo Evaluation of Injectable Strontium-Modified Calcium Phosphate Cement for Bone Defect Repair in Rats. Int. J. Mol. Sci. 2023, 24, 568. https://doi.org/10.3390/ijms24010568
Xu H, Zhu L, Tian F, Wang C, Wu W, Lu B, Yan L, Jia S, Hao D. In Vitro and In Vivo Evaluation of Injectable Strontium-Modified Calcium Phosphate Cement for Bone Defect Repair in Rats. International Journal of Molecular Sciences. 2023; 24(1):568. https://doi.org/10.3390/ijms24010568
Chicago/Turabian StyleXu, Hailiang, Lei Zhu, Fang Tian, Chengwen Wang, Weidong Wu, Botao Lu, Liang Yan, Shuaijun Jia, and Dingjun Hao. 2023. "In Vitro and In Vivo Evaluation of Injectable Strontium-Modified Calcium Phosphate Cement for Bone Defect Repair in Rats" International Journal of Molecular Sciences 24, no. 1: 568. https://doi.org/10.3390/ijms24010568
APA StyleXu, H., Zhu, L., Tian, F., Wang, C., Wu, W., Lu, B., Yan, L., Jia, S., & Hao, D. (2023). In Vitro and In Vivo Evaluation of Injectable Strontium-Modified Calcium Phosphate Cement for Bone Defect Repair in Rats. International Journal of Molecular Sciences, 24(1), 568. https://doi.org/10.3390/ijms24010568