
Changes in T-Cell Subpopulations and Cytokine Levels in Patients with Treatment-Resistant Depression—A Preliminary Study


Abstract
1. Introduction
2. Results
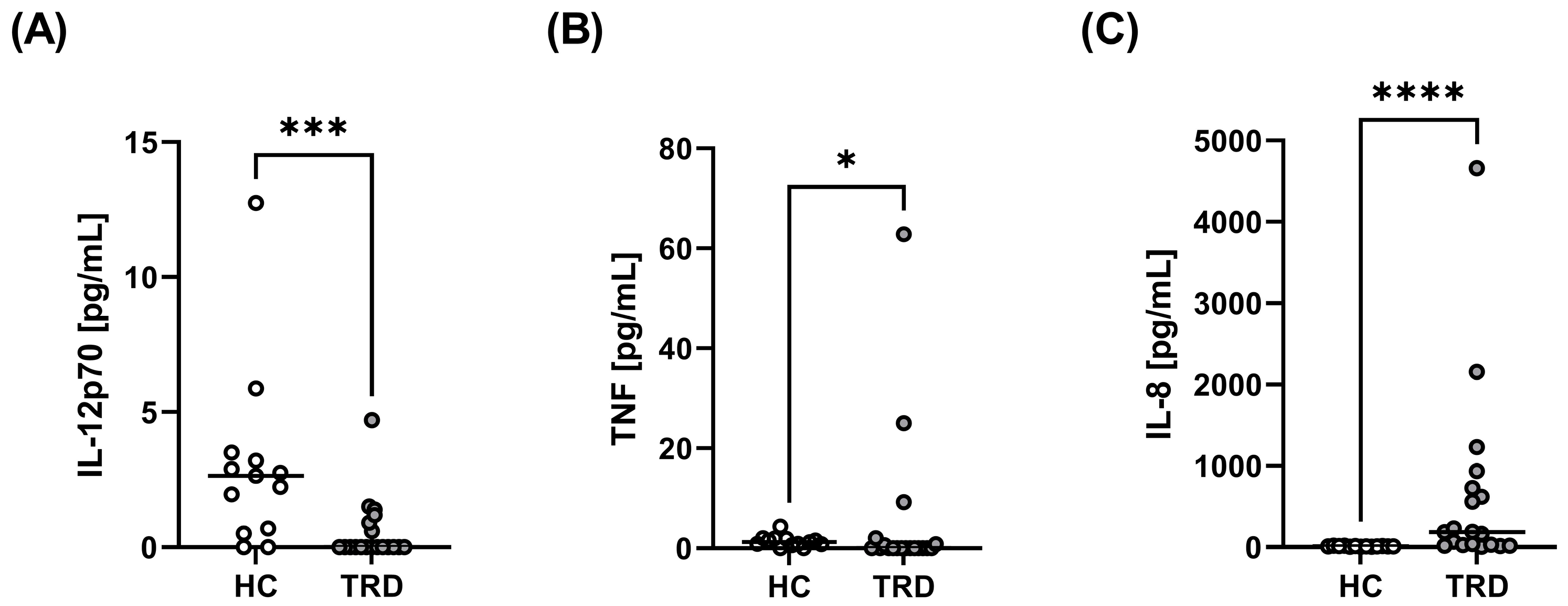
2.1. Comparison of T-Cell Subpopulations and Serum Cytokine Levels between TRD Patients and Healthy People
2.2. Correlations between Immunological and Clinical Parameters
2.3. Correlations between Immunological Parameters
3. Discussion
4. Materials and Methods
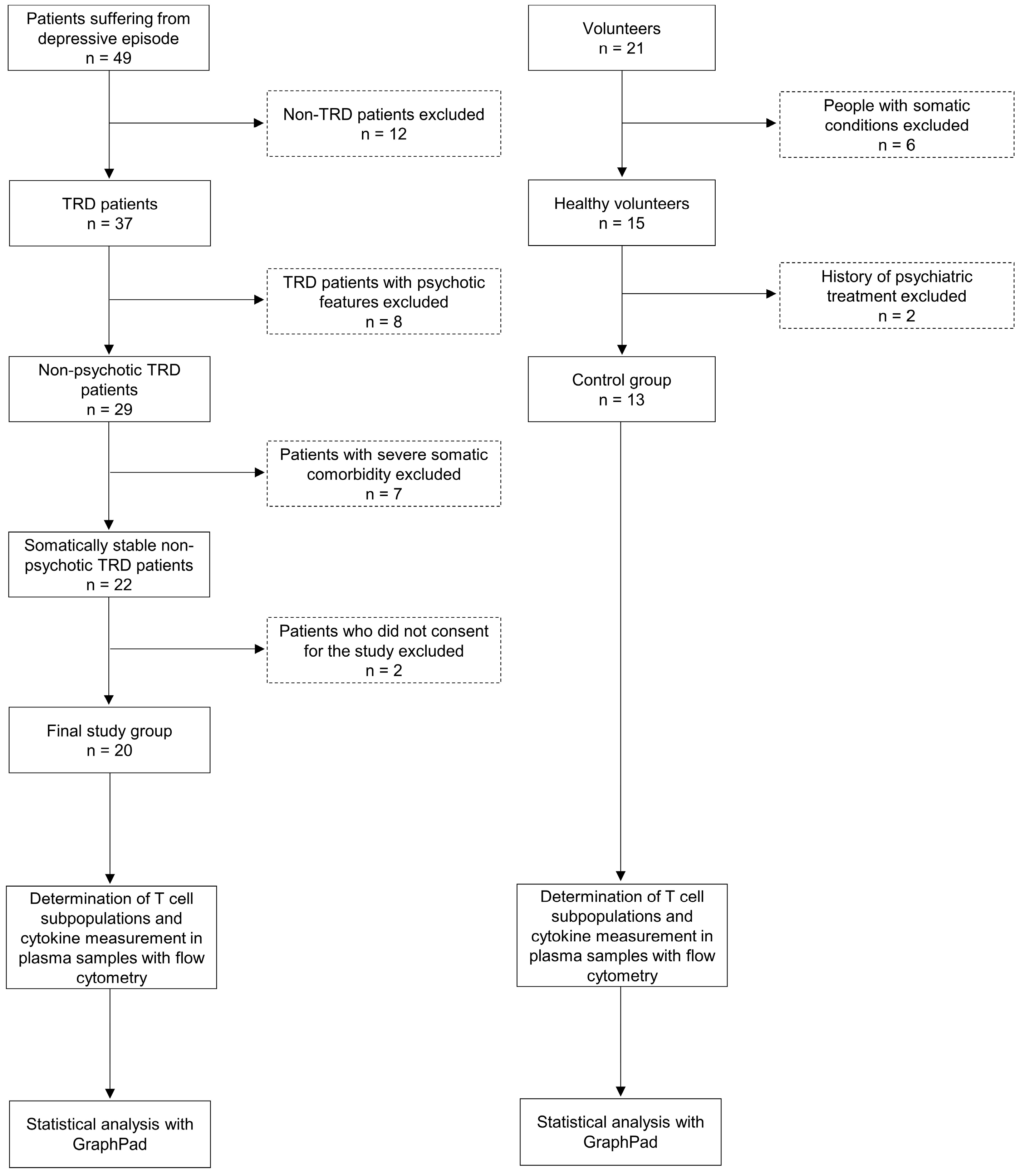
4.1. Study Groups
4.2. Ex Vivo Determination of T-Cell Subpopulations
4.3. Cytokine Measurement in Plasma Samples
4.4. Analysis and Statistics
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pariante, C.M. Psychoneuroimmunology or immunopsychiatry? Lancet Psychiatry 2015, 2, 197–199. [Google Scholar] [CrossRef] [PubMed]
- Dowlati, Y.; Herrmann, N.; Swardfager, W.; Liu, H.; Sham, L.; Reim, E.K.; Lanctôt, K.L. A meta-analysis of cytokines in major depression. Biol. Psychiatry 2010, 67, 446–457. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Ho, R.C.; Mak, A. Interleukin (IL)-6, tumour necrosis factor alpha (TNF-α) and soluble interleukin-2 receptors (sIL-2R) are elevated in patients with major depressive disorder: A meta-analysis and meta-regression. J. Affect. Disord. 2012, 139, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Strawbridge, R.; Arnone, D.; Danese, A.; Papadopoulos, A.; Herane Vives, A.; Cleare, A.J. Inflammation and clinical response to treatment in depression: A meta-analysis. Eur. Neuropsychopharmacol. 2015, 25, 1532–1543. [Google Scholar] [CrossRef] [PubMed]
- Alcocer-Gómez, E.; Casas-Barquero, N.; Williams, M.R.; Romero-Guillena, S.L.; Cañadas-Lozano, D.; Bullón, P.; Sánchez-Alcazar, J.A.; Navarro-Pando, J.M.; Cordero, M.D. Antidepressants induce autophagy dependent-NLRP3-inflammasome inhibition in Major depressive disorder. Pharmacol. Res. 2017, 121, 114–121. [Google Scholar] [CrossRef]
- Dahl, J.; Ormstad, H.; Aass, H.C.; Malt, U.F.; Bendz, L.T.; Sandvik, L.; Brundin, L.; Andreassen, O.A. The plasma levels of various cytokines are increased during ongoing depression and are reduced to normal levels after recovery. Psychoneuroendocrinology 2014, 45, 77–86. [Google Scholar] [CrossRef]
- Pérez-Sánchez, G.; Becerril-Villanueva, E.; Arreola, R.; Martínez-Levy, G.; Hernández-Gutiérrez, M.E.; Velasco-Velásquez, M.A.; Alvarez-Herrera, S.; Cruz-Fuentes, C.; Palacios, L.; de la Peña, F.; et al. Inflammatory Profiles in Depressed Adolescents Treated with Fluoxetine: An 8-Week Follow-up Open Study. Mediat. Inflamm. 2018, 2018, 4074051. [Google Scholar] [CrossRef]
- Demir, S.; Atli, A.; Bulut, M.; İbiloğlu, A.O.; Güneş, M.; Kaya, M.C.; Demirpençe, Ö.; Sır, A. Neutrophil-lymphocyte ratio in patients with major depressive disorder undergoing no pharmacological therapy. Neuropsychiatr. Dis. Treat. 2015, 11, 2253–2258. [Google Scholar] [CrossRef]
- Grosse, L.; Carvalho, L.A.; Birkenhager, T.K.; Hoogendijk, W.J.; Kushner, S.A.; Drexhage, H.A.; Bergink, V. Circulating cytotoxic T cells and natural killer cells as potential predictors for antidepressant response in melancholic depression. Restoration of T regulatory cell populations after antidepressant therapy. Psychopharmacology 2016, 233, 1679–1688. [Google Scholar] [CrossRef]
- Schmidt, F.M.; Lichtblau, N.; Minkwitz, J.; Chittka, T.; Thormann, J.; Kirkby, K.C.; Sander, C.; Mergl, R.; Faßhauer, M.; Stumvoll, M.; et al. Cytokine levels in depressed and non-depressed subjects, and masking effects of obesity. J. Psychiatr. Res. 2014, 55, 29–34. [Google Scholar] [CrossRef]
- Müller, N.; Hofschuster, E.; Ackenheil, M.; Mempel, W.; Eckstein, R. Investigations of the cellular immunity during depression and the free interval: Evidence for an immune activation in affective psychosis. Prog. Neuropsychopharmacol. Biol. Psychiatry 1993, 17, 713–730. [Google Scholar] [CrossRef] [PubMed]
- Maes, M.; Stevens, W.; DeClerck, L.; Bridts, C.; Peeters, D.; Schotte, C.; Cosyns, P. Immune disorders in depression: Higher T helper/T suppressor-cytotoxic cell ratio. Acta Psychiatr. Scand. 1992, 86, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Zorrilla, E.P.; Luborsky, L.; McKay, J.R.; Rosenthal, R.; Houldin, A.; Tax, A.; McCorkle, R.; Seligman, D.A.; Schmidt, K. The relationship of depression and stressors to immunological assays: A meta-analytic review. Brain Behav. Immun. 2001, 15, 199–226. [Google Scholar] [CrossRef] [PubMed]
- Başterzi, A.D.; Yazici, K.; Buturak, V.; Cimen, B.; Yazici, A.; Eskandari, G.; Tot Acar, S.; Taşdelen, B. Effects of venlafaxine and fluoxetine on lymphocyte subsets in patients with major depressive disorder: A flow cytometric analysis. Prog. Neuropsychopharmacol. Biol. Psychiatry 2010, 34, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Patas, K.; Willing, A.; Demiralay, C.; Engler, J.B.; Lupu, A.; Ramien, C.; Schäfer, T.; Gach, C.; Stumm, L.; Chan, K.; et al. T Cell Phenotype and T Cell Receptor Repertoire in Patients with Major Depressive Disorder. Front. Immunol. 2018, 9, 291. [Google Scholar] [CrossRef]
- Ivanova, S.A.; Semke, V.Y.; Vetlugina, T.P.; Rakitina, N.M.; Kudyakova, T.A.; Simutkin, G.G. Signs of apoptosis of immunocompetent cells in patients with depression. Neurosci. Behav. Physiol. 2007, 37, 527–530. [Google Scholar] [CrossRef]
- Szuster-Ciesielska, A.; Słotwińska, M.; Stachura, A.; Marmurowska-Michałowska, H.; Dubas-Slemp, H.; Bojarska-Junak, A.; Kandefer-Szerszeń, M. Accelerated apoptosis of blood leukocytes and oxidative stress in blood of patients with major depression. Prog. Neuropsychopharmacol. Biol. Psychiatry 2008, 32, 686–694. [Google Scholar] [CrossRef]
- Duggal, N.A.; Upton, J.; Phillips, A.C.; Hampson, P.; Lord, J.M. Depressive symptoms post hip fracture in older adults are associated with phenotypic and functional alterations in T cells. Immun. Ageing 2014, 11, 25. [Google Scholar] [CrossRef]
- Pietruczuk, K.; Jakuszkowiak, K.; Landowski, J.; Witkowski, J.M. Comparison of chosen immune system parameters in patients suffering from depression and healthy donors. Psychiatria 2005, 2, 210–216. [Google Scholar]
- Maes, M.; Bosmans, E.; Suy, E.; Vandervorst, C.; De Jonckheere, C.; Raus, J. Immune disturbances during major depression: Upregulated expression of interleukin-2 receptors. Neuropsychobiology 1990, 24, 115–120. [Google Scholar] [CrossRef]
- Lee, K.M.; Kim, Y.K. The role of IL-12 and TGF-beta1 in the pathophysiology of major depressive disorder. Int. Immunopharmacol. 2006, 6, 1298–1304. [Google Scholar] [CrossRef] [PubMed]
- Myint, A.M.; Leonard, B.E.; Steinbusch, H.W.; Kim, Y.K. Th1, Th2, and Th3 cytokine alterations in major depression. J. Affect. Disord. 2005, 88, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Jiang, T.; Chen, P.; Ouyang, J.; Xu, G.; Zeng, Z.; Sun, Y. Emerging tendency towards autoimmune process in major depressive patients: A novel insight from Th17 cells. Psychiatry Res. 2011, 188, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Davami, M.H.; Baharlou, R.; Ahmadi Vasmehjani, A.; Ghanizadeh, A.; Keshtkar, M.; Dezhkam, I.; Atashzar, M.R. Elevated IL-17 and TGF-β Serum Levels: A Positive Correlation between T-helper 17 Cell-Related Pro-Inflammatory Responses with Major Depressive Disorder. Basic Clin. Neurosci. 2016, 7, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Xiao, B.; Qiu, W.; Yang, L.; Hu, B.; Tian, X.; Yang, H. Altered expression of CD4+CD25+ regulatory T cells and its 5-HT1a receptor in patients with major depression disorder. J. Affect. Disord. 2010, 124, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Modabbernia, A.; Taslimi, S.; Brietzke, E.; Ashrafi, M. Cytokine alterations in bipolar disorder: A meta-analysis of 30 studies. Biol. Psychiatry 2013, 74, 15–25. [Google Scholar] [CrossRef]
- Misiak, B.; Bartoli, F.; Carrà, G.; Małecka, M.; Samochowiec, J.; Jarosz, K.; Banik, A.; Stańczykiewicz, B. Chemokine alterations in bipolar disorder: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 870–877. [Google Scholar] [CrossRef]
- do Prado, C.H.; Rizzo, L.B.; Wieck, A.; Lopes, R.P.; Teixeira, A.L.; Grassi-Oliveira, R.; Bauer, M.E. Reduced regulatory T cells are associated with higher levels of Th1/TH17 cytokines and activated MAPK in type 1 bipolar disorder. Psychoneuroendocrinology 2013, 38, 667–676. [Google Scholar] [CrossRef]
- Drexhage, R.C.; Hoogenboezem, T.H.; Versnel, M.A.; Berghout, A.; Nolen, W.A.; Drexhage, H.A. The activation of monocyte and T cell networks in patients with bipolar disorder. Brain Behav. Immun. 2011, 25, 1206–1213. [Google Scholar] [CrossRef]
- Becking, K.; Haarman, B.C.M.; Grosse, L.; Nolen, W.A.; Claes, S.; Arolt, V.; Schoevers, R.A.; Drexhage, H.A. The circulating levels of CD4+ T helper cells are higher in bipolar disorder as compared to major depressive disorder. J. Neuroimmunol. 2018, 319, 28–36. [Google Scholar] [CrossRef]
- Barbosa, I.G.; Rocha, N.P.; Assis, F.; Vieira, É.L.; Soares, J.C.; Bauer, M.E.; Teixeira, A.L. Monocyte and lymphocyte activation in bipolar disorder: A new piece in the puzzle of immune dysfunction in mood disorders. Int. J. Neuropsychopharmacol. 2014, 18, pyu021. [Google Scholar] [CrossRef] [PubMed]
- Gaynes, B.N.; Rush, A.J.; Trivedi, M.H.; Wisniewski, S.R.; Spencer, D.; Fava, M. The STAR*D study: Treating depression in the real world. Clevel. Clin. J. Med. 2008, 75, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Berlim, M.T.; Turecki, G. Definition, assessment, and staging of treatment-resistant refractory major depression: A review of current concepts and methods. Can. J. Psychiatry 2007, 52, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Poon, S.H.; Sim, K.; Baldessarini, R.J. Pharmacological approaches for treatment-resistant bipolar disorder. Curr. Neuropharmacol. 2015, 13, 592–604. [Google Scholar] [CrossRef]
- Strawbridge, R.; Hodsoll, J.; Powell, T.R.; Hotopf, M.; Hatch, S.L.; Breen, G.; Cleare, A.J. Inflammatory profiles of severe treatment-resistant depression. J. Affect. Disord. 2019, 246, 42–51. [Google Scholar] [CrossRef]
- Yamasaki, K.; Hasegawa, T.; Takeda, M. Serum level of soluble interleukin 6 receptor is a useful biomarker for identification of treatment-resistant major depressive disorder. Neuropsychopharmacol. Rep. 2020, 40, 130–137. [Google Scholar] [CrossRef]
- Sowa-Kućma, M.; Styczeń, K.; Siwek, M.; Misztak, P.; Nowak, R.J.; Dudek, D.; Rybakowski, J.K.; Nowak, G.; Maes, M. Lipid Peroxidation and Immune Biomarkers Are Associated with Major Depression and Its Phenotypes, Including Treatment-Resistant Depression and Melancholia. Neurotox. Res. 2018, 33, 448–460. [Google Scholar] [CrossRef]
- Wu, X.; Dai, B.; Yan, F.; Chen, Y.; Xu, Y.; Xia, Q.; Zhang, X. Serum Cortisol, Nesfatin-1, and IL-1β: Potential Diagnostic Biomarkers in Elderly Patients with Treatment-Resistant Depression. Clin. Interv. Aging 2022, 17, 567–576. [Google Scholar] [CrossRef]
- Park, M.; Newman, L.E.; Gold, P.W.; Luckenbaugh, D.A.; Yuan, P.; Machado-Vieira, R.; Zarate, C.A., Jr. Change in cytokine levels is not associated with rapid antidepressant response to ketamine in treatment-resistant depression. J. Psychiatr. Res. 2017, 84, 113–118. [Google Scholar] [CrossRef]
- Murata, S.; Murphy, M.; Hoppensteadt, D.; Fareed, J.; Welborn, A.; Halaris, A. Effects of adjunctive inflammatory modulation on IL-1β in treatment resistant bipolar depression. Brain Behav. Immun. 2020, 87, 369–376. [Google Scholar] [CrossRef]
- Kiraly, D.D.; Horn, S.R.; Van Dam, N.T.; Costi, S.; Schwartz, J.; Kim-Schulze, S.; Patel, M.; Hodes, G.E.; Russo, S.J.; Merad, M.; et al. Altered peripheral immune profiles in treatment-resistant depression: Response to ketamine and prediction of treatment outcome. Transl. Psychiatry 2017, 7, e1065. [Google Scholar] [CrossRef] [PubMed]
- Furman, D.; Campisi, J.; Verdin, E.; Carrera-Bastos, P.; Targ, S.; Franceschi, C.; Ferrucci, L.; Gilroy, D.W.; Fasano, A.; Miller, G.W.; et al. Chronic inflammation in the etiology of disease across the life span. Nat. Med. 2019, 25, 1822–1832. [Google Scholar] [CrossRef] [PubMed]
- Diez-Ruiz, A.; Tilz, G.P.; Zangerle, R.; Baier-Bitterlich, G.; Wachter, H.; Fuchs, D. Soluble receptors for tumour necrosis factor in clinical laboratory diagnosis. Eur. J. Haematol. 1995, 54, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Eley, B.S.; Batty, D.W. The basic immunology of tuberculosis. In Tuberculosis a Comprehensive Clinical Reference; Schaaf, H.S., Zumla, A.I., Eds.; Elsevier Health Sciences: Philadelphia, PA, USA, 2009; pp. 75–86. [Google Scholar]
- Cosma, N.C.; Üsekes, B.; Otto, L.R.; Gerike, S.; Heuser, I.; Regen, F.; Hellmann-Regen, J. M1/M2 polarization in major depressive disorder: Disentangling state from trait effects in an individualized cell-culture-based approach. Brain Behav. Immun. 2021, 94, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Ehrlich, L.C.; Hu, S.; Sheng, W.S.; Sutton, R.L.; Rockswold, G.L.; Peterson, P.K.; Chao, C.C. Cytokine regulation of human microglial cell IL-8 production. J. Immunol. 1998, 160, 1944–1948. [Google Scholar] [PubMed]
- Taub, D.D.; Anver, M.; Oppenheim, J.J.; Longo, D.L.; Murphy, W.J. T lymphocyte recruitment by interleukin-8 (IL-8). IL-8-induced degranulation of neutrophils releases potent chemoattractants for human T lymphocytes both in vitro and in vivo. J. Clin. Investig. 1996, 97, 1931–1941. [Google Scholar] [CrossRef]
- Kofod, J.; Elfving, B.; Nielsen, E.H.; Mors, O.; Köhler-Forsberg, O. Depression and inflammation: Correlation between changes in inflammatory markers with antidepressant response and long-term prognosis. Eur. Neuropsychopharmacol. 2022, 54, 116–125. [Google Scholar] [CrossRef]
- Huet, L.; Delgado, I.; Dexpert, S.; Sauvant, J.; Aouizerate, B.; Beau, C.; Forestier, D.; Ledaguenel, P.; Magne, E.; Capuron, L. Relationship between body mass index and neuropsychiatric symptoms: Evidence and inflammatory correlates. Brain Behav. Immun. 2021, 94, 104–110. [Google Scholar] [CrossRef]
- Berlin, I.; Lavergne, F. Relationship between body-mass index and depressive symptoms in patients with major depression. Eur. Psychiatry 2003, 18, 85–88. [Google Scholar] [CrossRef]
- Yu, J.Y.; Choi, W.J.; Lee, H.S.; Lee, J.W. Relationship between inflammatory markers and visceral obesity in obese and overweight Korean adults: An observational study. Medicine 2019, 98, e14740. [Google Scholar] [CrossRef]
- Cibrián, D.; Sánchez-Madrid, F. CD69: From activation marker to metabolic gatekeeper. Eur. J. Immunol. 2017, 47, 946–953. [Google Scholar] [CrossRef] [PubMed]
- Du, J.; Wei, L.; Li, G.; Hua, M.; Sun, Y.; Wang, D.; Han, K.; Yan, Y.; Song, C.; Song, R.; et al. Persistent High Percentage of HLA-DR+CD38high CD8+ T Cells Associated with Immune Disorder and Disease Severity of COVID-19. Front. Immunol. 2021, 12, 735125. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HC (n = 13) | TRD (n = 20) | p Value | |
|---|---|---|---|
| Sex (male/female) | 7/6 | 9/11 | 0.728 |
| Age (years) | 51 ± 17.63 | 47.50 ± 19.03 | 0.509 |
| BMI (kg/m2) | 24.47 ± 5.34 | 28.24 ± 6.27 | 0.115 |
| Length of current episode (weeks) | n.a. | 38 ± 6.08 | n.a. |
| MADRS | n.a. | 30.2 ± 1.49 | n.a. |
| Medication * | |||
| SSRIs | n.a. | 5 | n.a. |
| SNRIs | n.a. | 7 | n.a. |
| SARIs | n.a. | 2 | n.a. |
| NaSSAs | n.a. | 6 | n.a. |
| TCAs | n.a. | 2 | n.a. |
| Atypical antipsychotics | n.a. | 10 | n.a. |
| Antiepileptic drugs | n.a. | 5 | n.a. |
| Low-potency antipsychotics | n.a. | 4 | n.a. |
| Lithium | n.a. | 6 | n.a. |
| HC | TRD | p Value | |
|---|---|---|---|
| CD3+ (%) | 75.66 (62.2; 80.82) | 74.35 (43.3; 83.6) | 0.407 |
| CD3+CD4+ cells (%) | 61.4 (44.54; 76.88) | 67 (48.8; 82.5) | 0.286 |
| CD3+CD8+ cells (%) | 32.8 (17.01; 48) | 32.65 (13.2; 48.5) | 0.630 |
| CD4+/CD8+ ratio | 1.95 (1.08; 3.95) | 2.05 (1.03; 6.25) | 0.964 |
| CD3+CD4+ CD28+ cells (%) | 59.02 (38.98; 69.81) | 60 (36.7; 82.1) | 0.434 |
| CD3+CD4+CD25+ cells (%) | 13.16 (5.08; 24.3) | 6.99 (1.42; 43.6) | 0.006 |
| CD3+CD4+CD69+ cells (%) | 0.63 (0.04; 12.5) | 0.4 (0.03; 20) | 0.242 |
| CD3+CD4+CD95+ cells (%) | 35.8 (18.3; 53.33) | 29.1 (17; 45.8) | 0.080 |
| CD3+CD4+HLA-DR+ cells (%) | 1.68 (0.44; 7.18) | 1.11 (0.09; 20.5) | 0.715 |
| CD3+CD8+CD28+ cells (%) | 17.71 (9.59; 28.1) | 18.95 (11.2; 35.3) | 0.377 |
| CD3+CD8+CD25+ cells (%) | 0.64 (0.06; 4.84) | 0.39 (0.06; 3.82) | 0.191 |
| CD3+CD8+CD69+ cells (%) | 0.44 (0.07; 2.92) | 0.45 (0.01; 2.44) | 0.805 |
| CD3+CD8+CD95+ cells (%) | 30.3 (14.23; 48.56) | 18.2 (9.11; 35.1) | 0.024 |
| CD3+CD8+HLA-DR+ cells (%) | 2.79 (0.92; 13.5) | 8.8 (0.57; 15.9) | 0.059 |
| IL-12p70 (pg/mL) | 2.65 (0; 12.74) | 0 (0; 4.7) | 0.001 |
| TNF-α (pg/mL) | 1.2 (0; 4.36) | 0 (0; 62.8) | 0.025 |
| IL-10 (pg/mL) | 2.7 (0; 6.15) | 1.8 (0; 5.6) | 0.153 |
| IL-6 (pg/mL) | 2.89 (0; 22.57) | 2.8 (0; 110.4) | 0.726 |
| IL-1β (pg/mL) | 2.26 (0; 18.3) | 0.7 (0.0; 12.6) | 0.133 |
| IL-8 (pg/mL) | 11.33 (5.5; 20.2) | 185.9 (8.1; 4660) | <0.0001 |
| r | p Value | |
|---|---|---|
| CD3+ (%) | −0.160 | 0.500 |
| CD3+CD4+ cells (%) | 0.620 | 0.004 |
| CD3+CD8+ cells (%) | −0.599 | 0.005 |
| CD4+/CD8+ ratio | 0.604 | 0.005 |
| CD3+CD4+CD28+ cells (%) | 0.364 | 0.115 |
| CD3+CD4+CD25+ cells (%) | 0.007 | 0.977 |
| CD3+CD4+CD69+ cells (%) | 0.303 | 0.222 |
| CD3+CD4+CD95+ cells (%) | 0.482 | 0.052 |
| CD3+CD4+HLA-DR+ cells (%) | 0.230 | 0.359 |
| CD3+CD8+ CD28+ cells (%) | −0.358 | 0.121 |
| CD3+CD8+CD25+ cells (%) | −0.052 | 0.826 |
| CD3+CD8+CD69+ cells (%) | 0.040 | 0.875 |
| CD3+CD8+CD95+ cells (%) | −0.249 | 0.332 |
| CD3+CD8+HLA-DR+ cells (%) | −0.102 | 0,686 |
| IL-12p70 (pg/mL) | 0.208 | 0.394 |
| TNF-α (pg/mL) | 0.127 | 0.605 |
| IL-10 (pg/mL) | −0.273 | 0.259 |
| IL-6 (pg/mL) | 0.142 | 0.562 |
| IL-1β (pg/mL) | 0.058 | 0.815 |
| IL-8 (pg/mL) | −0.031 | 0.901 |
| IL-12p70 (pg/mL) | TNF-α (pg/mL) | IL-10 (pg/mL) | IL-6 (pg/mL) | IL-1β (pg/mL) | IL-8 (pg/mL) | |
|---|---|---|---|---|---|---|
| CD3+ (%) | −0.195 | −0.233 | 0.218 | −0.045 | 0.061 | −0.168 |
| CD3+CD4+ cells (%) | −0.006 | 0.049 | −0.473 | 0.091 | 0.072 | 0.226 |
| CD3+CD8+ cells (%) | 0.040 | −0.03 | 0.468 | −0.087 | −0.037 | −0.242 |
| CD4+/CD8+ ratio | −0.023 | 0.039 | −0.470 | 0.092 | 0.054 | 0.234 |
| CD3+CD4+CD28+ cells (%) | 0.168 | −0.089 | −0.312 | 0.133 | 0.214 | 0.135 |
| CD3+CD4+CD25+ cells (%) | 0.396 | 0.013 | 0.236 | 0.258 | 0.573 | 0.363 |
| CD3+CD4+CD69+ cells (%) | 0.401 | 0.470 | 0.046 | 0.395 | 0.592 | 0.564 |
| CD3+CD4+CD95+ cells (%) | −0.064 | −0.029 | −0.304 | 0.272 | 0.139 | −0.085 |
| CD3+CD4+HLA-DR+ cells (%) | −0.066 | 0.119 | −0.378 | 0.219 | 0.416 | 0.544 |
| CD3+CD8+CD28+ cells (%) | 0.295 | −0.056 | 0.190 | −0.172 | 0.236 | −0.188 |
| CD3+CD8+CD25+ cells (%) | 0.336 | −0.018 | 0.242 | 0.236 | 0.301 | −0.182 |
| CD3+CD8+CD69+ cells (%) | −0.104 | 0.040 | 0.165 | 0.088 | 0.124 | 0.239 |
| CD3+CD8+CD95+ cells (%) | 0.224 | 0.132 | 0.579 | 0.573 | 0.327 | 0.003 |
| CD3+CD8+HLA-DR+ cells (%) | 0.075 | −0.072 | −0.183 | −0.022 | 0.248 | 0.088 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szałach, Ł.P.; Cubała, W.J.; Lisowska, K.A. Changes in T-Cell Subpopulations and Cytokine Levels in Patients with Treatment-Resistant Depression—A Preliminary Study. Int. J. Mol. Sci. 2023, 24, 479. https://doi.org/10.3390/ijms24010479
Szałach ŁP, Cubała WJ, Lisowska KA. Changes in T-Cell Subpopulations and Cytokine Levels in Patients with Treatment-Resistant Depression—A Preliminary Study. International Journal of Molecular Sciences. 2023; 24(1):479. https://doi.org/10.3390/ijms24010479
Chicago/Turabian StyleSzałach, Łukasz Piotr, Wiesław Jerzy Cubała, and Katarzyna Aleksandra Lisowska. 2023. "Changes in T-Cell Subpopulations and Cytokine Levels in Patients with Treatment-Resistant Depression—A Preliminary Study" International Journal of Molecular Sciences 24, no. 1: 479. https://doi.org/10.3390/ijms24010479
APA StyleSzałach, Ł. P., Cubała, W. J., & Lisowska, K. A. (2023). Changes in T-Cell Subpopulations and Cytokine Levels in Patients with Treatment-Resistant Depression—A Preliminary Study. International Journal of Molecular Sciences, 24(1), 479. https://doi.org/10.3390/ijms24010479