
Albumin Binds Doxorubicin via Self–Assembling Dyes as Specific Polymolecular Ligands

 , ,
, ,
Abstract
:1. Introduction
2. Results
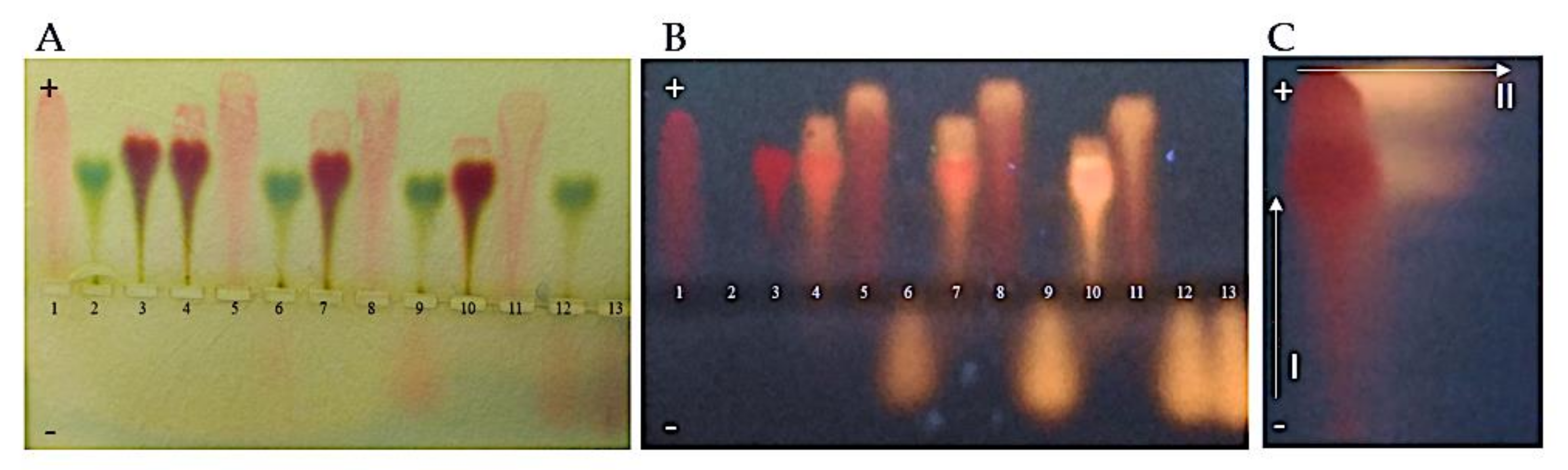
2.1. Dox Forms Complexes with CR (CR–Dox), Which Are Bound by Albumin. Agarose Gel Electrophoresis and Chromatographic Analysis
2.2. Increasing the Amount of Dox in the BSA–CR–Dox Complex Increases the Size of This Complex. Gel–Filtration Chromatography (BioGel P–300): Elution Volumes of CR and CR–Dox Complexes with Albumin
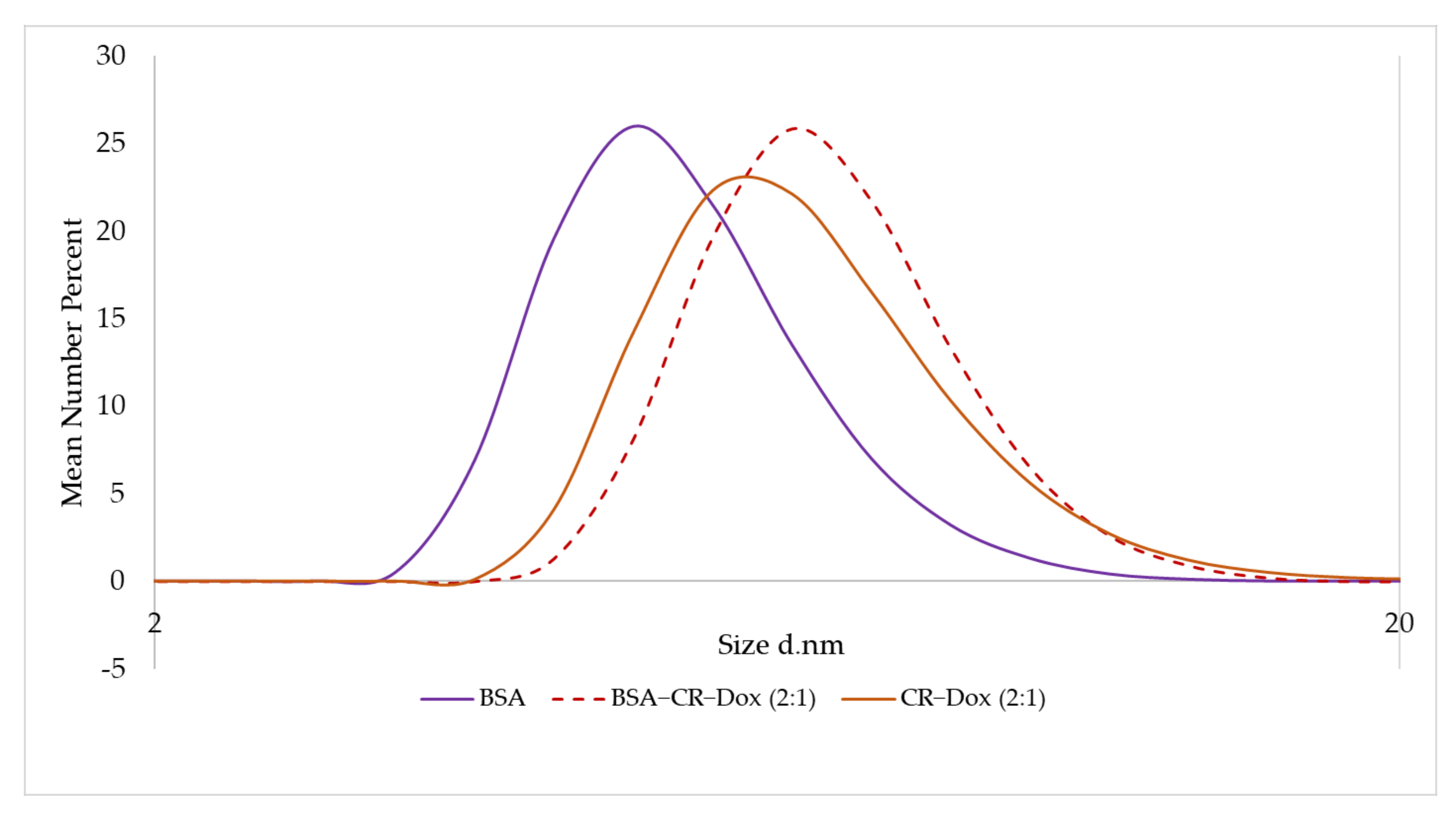
2.3. DLS Analysis
2.3.1. CR–Dox (2:1) Complexes Are of the Same Size as BSA–CR–Dox Complexes (CR–Dox = 2:1)
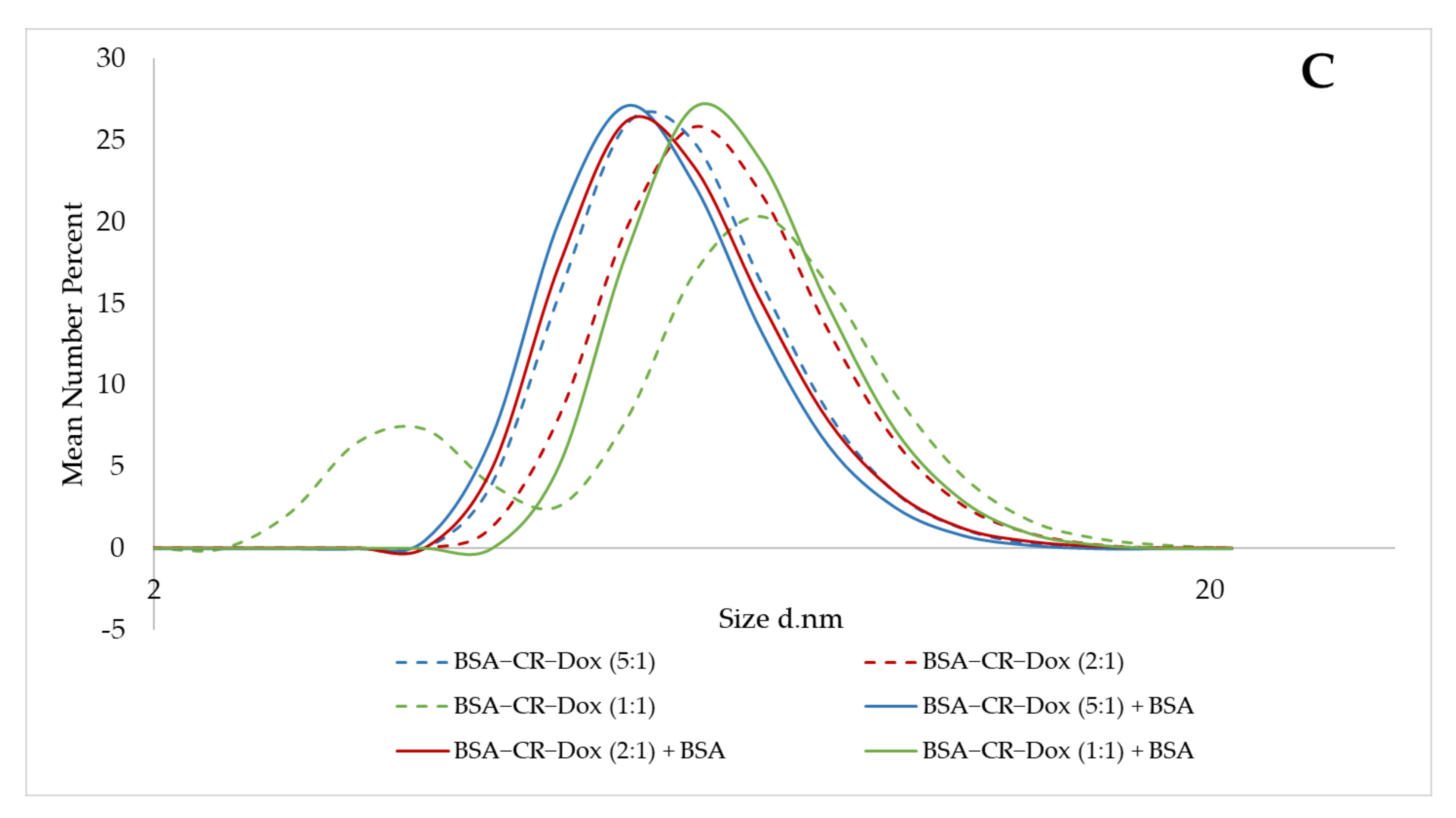
2.3.2. Assessment of CR–Dox Binding to Albumin—Additional Albumin Is Not Bridged with CR–Dox
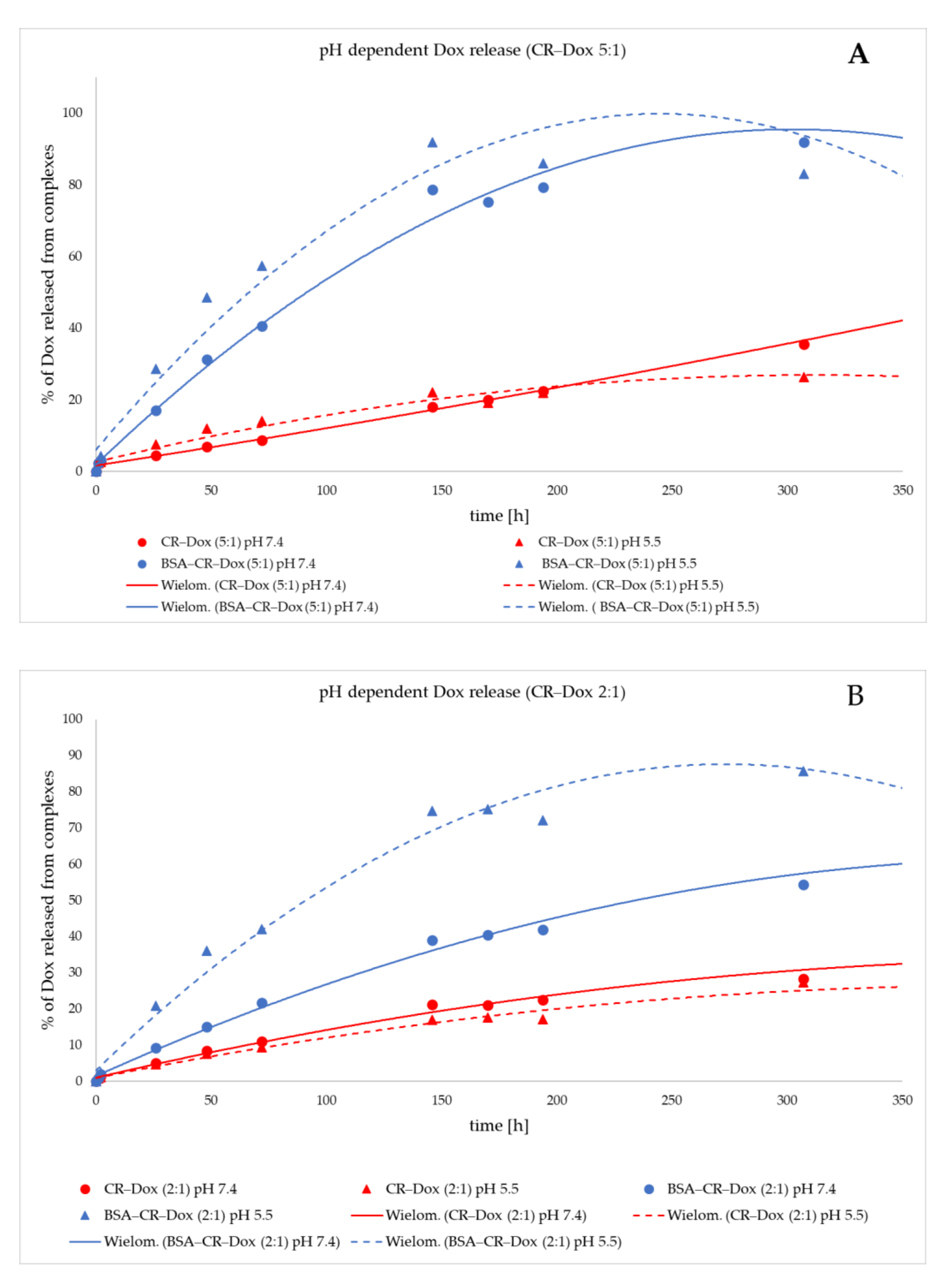
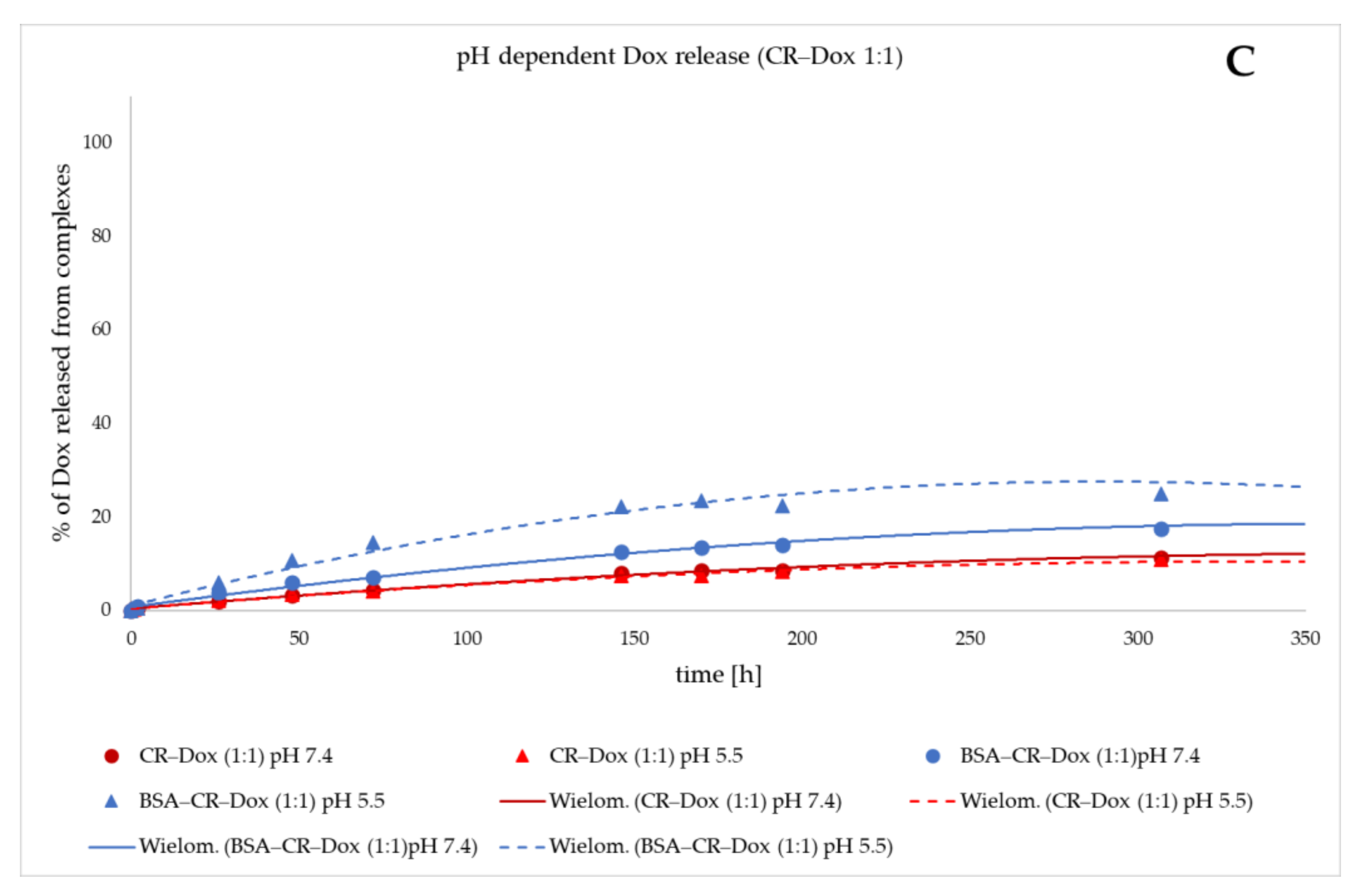
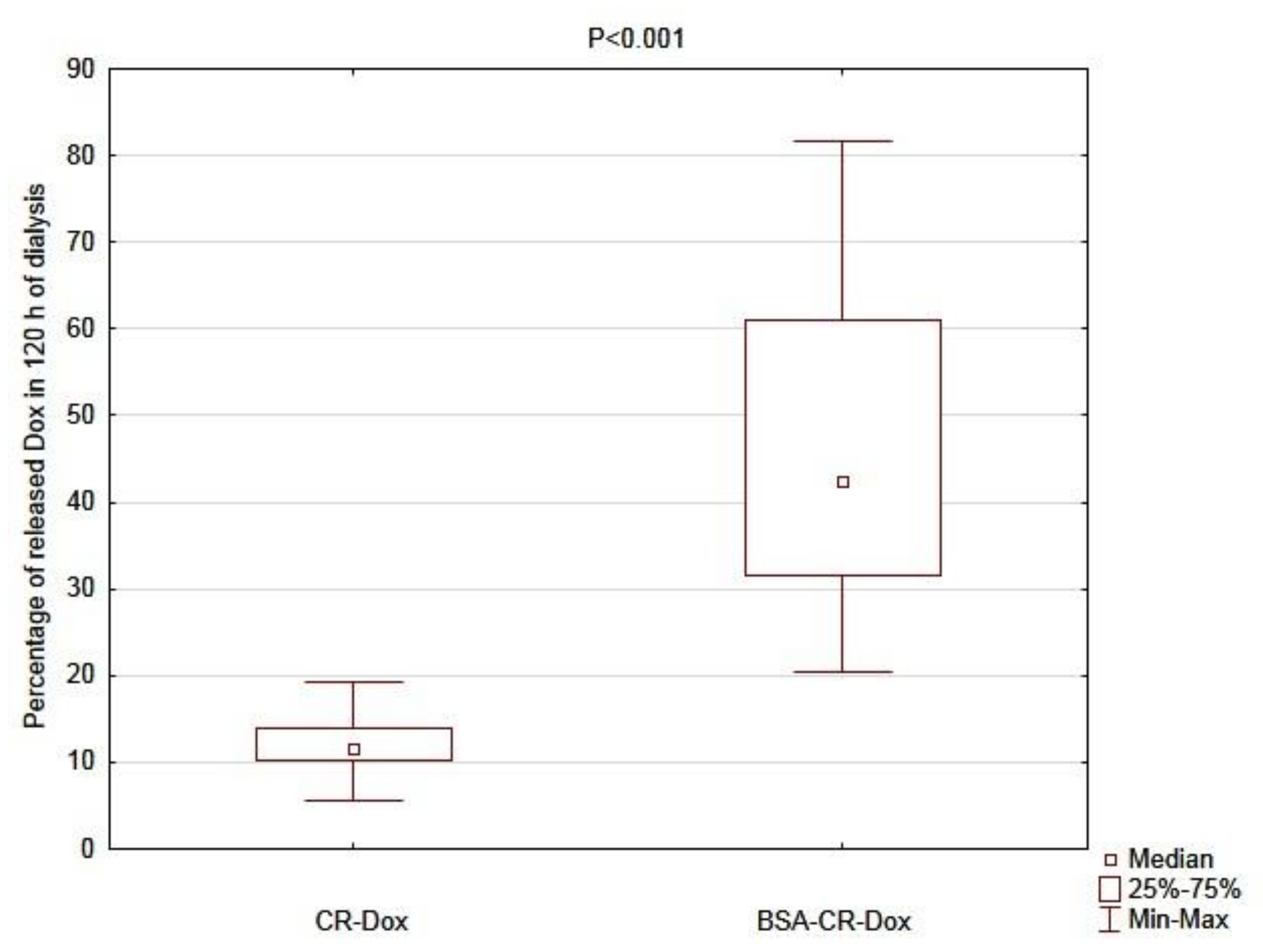
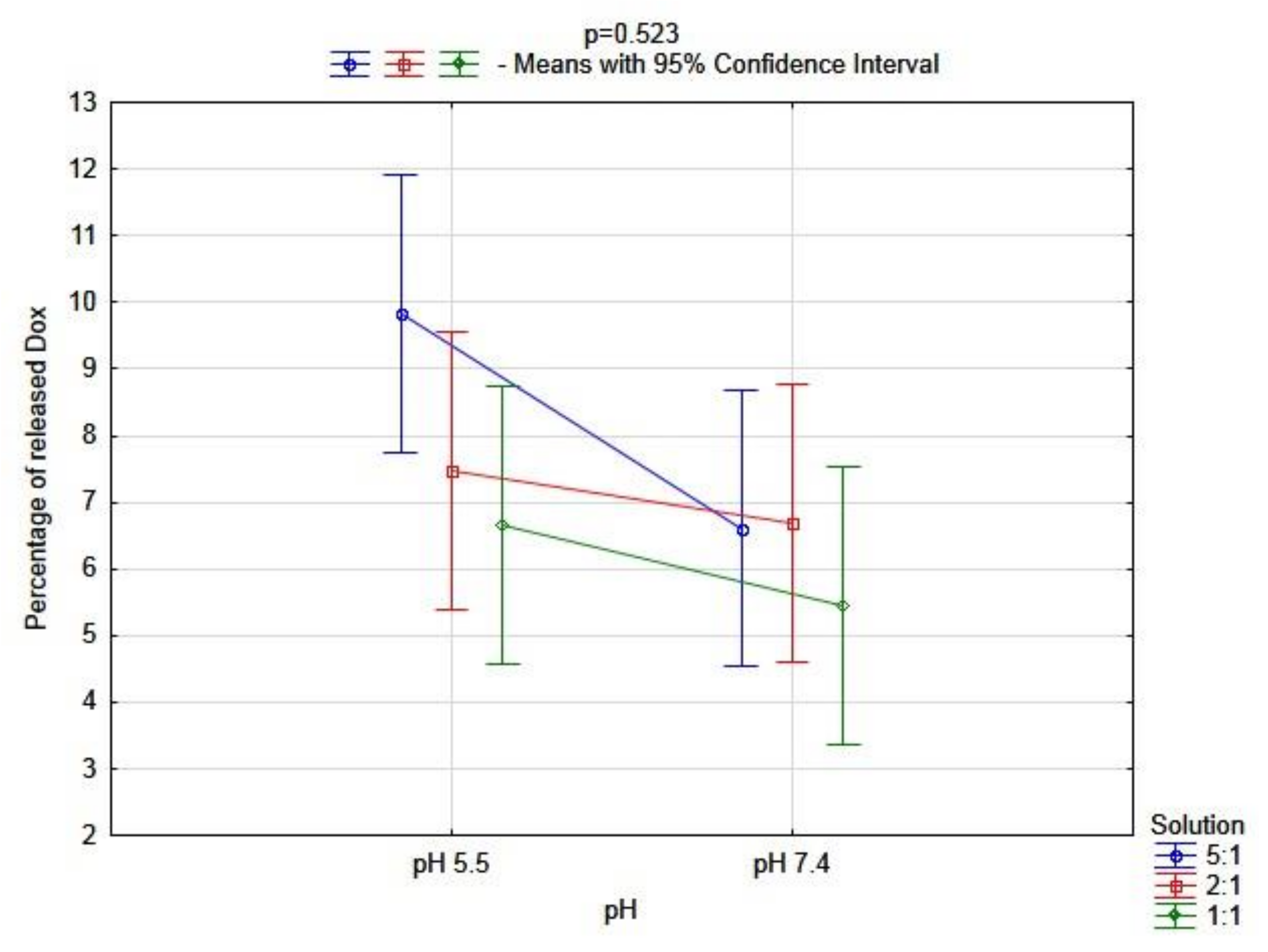
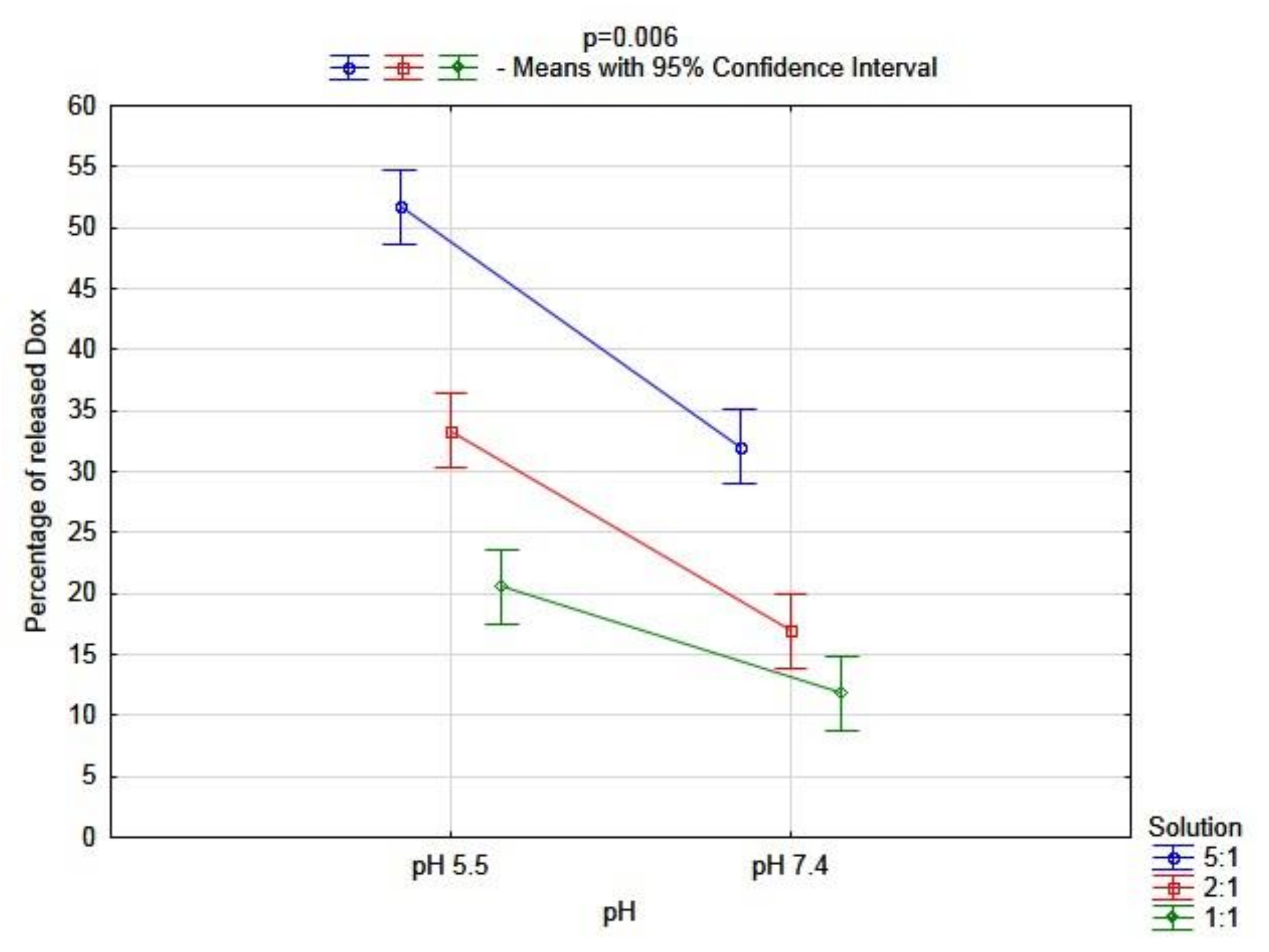
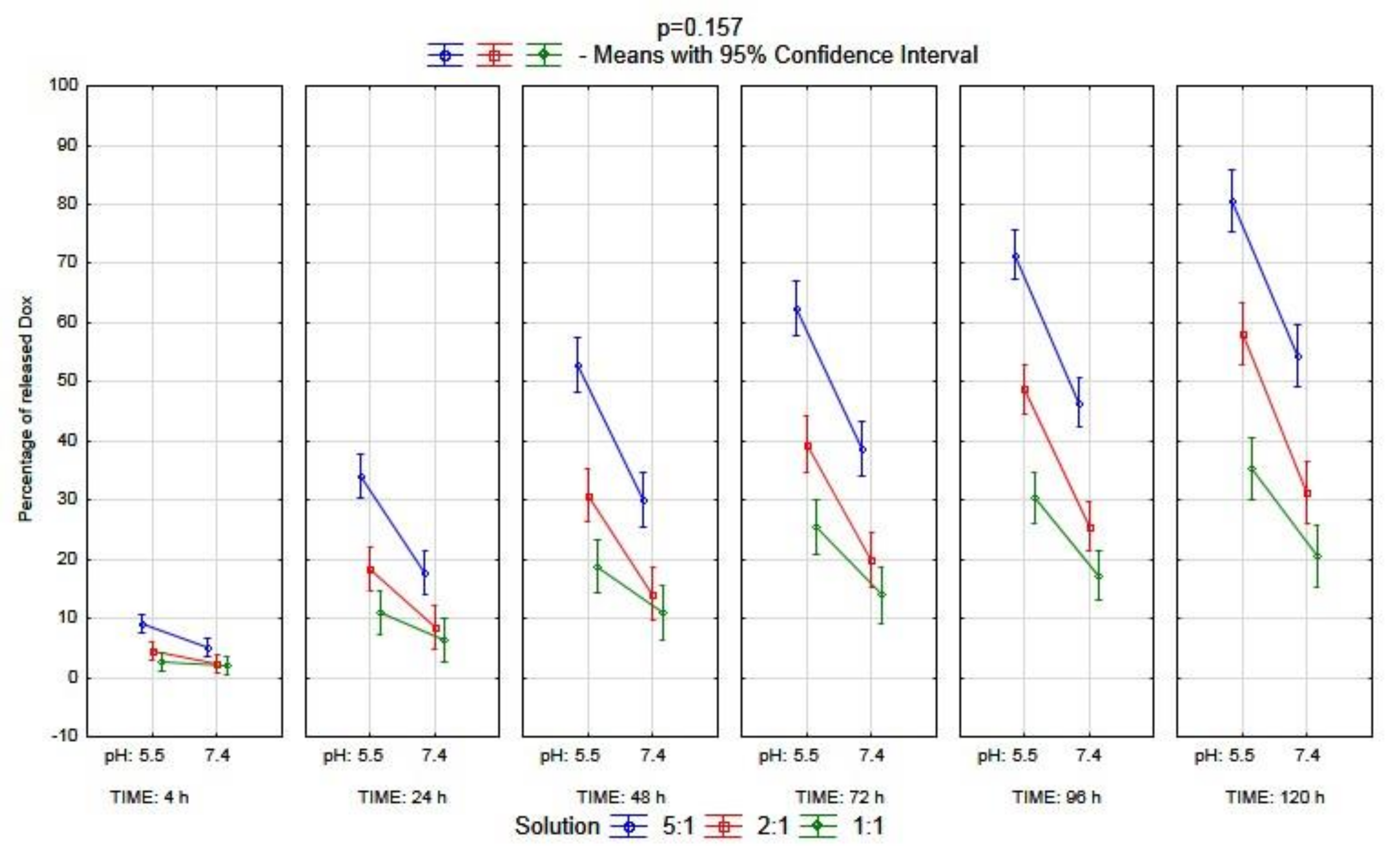
2.4. Dox Is Most Efficiently Released from the BSA–CR–Dox Complex (CR–Dox = 2:1) at pH = 5.5. Dialysis
Statistical Analysis
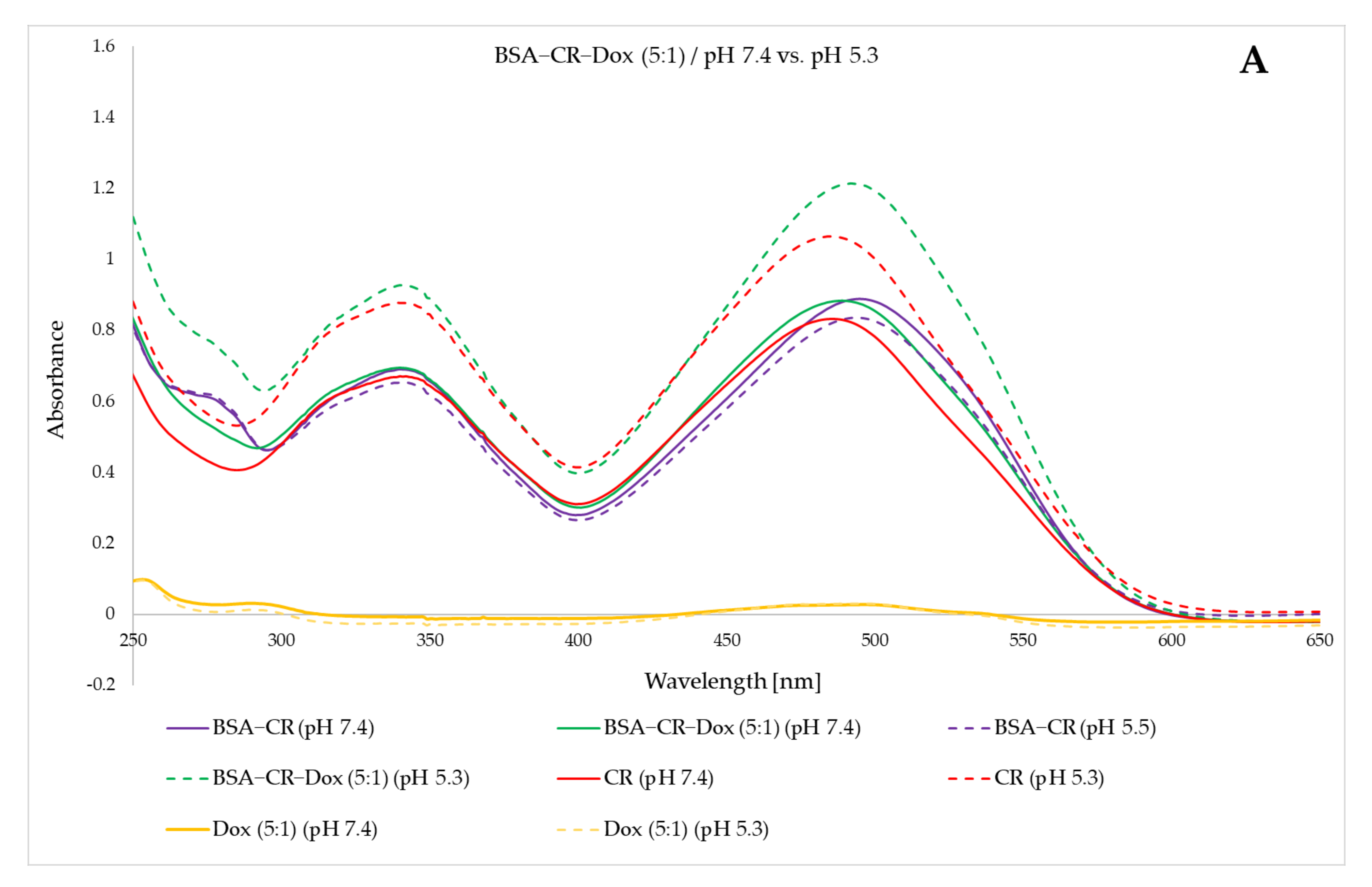
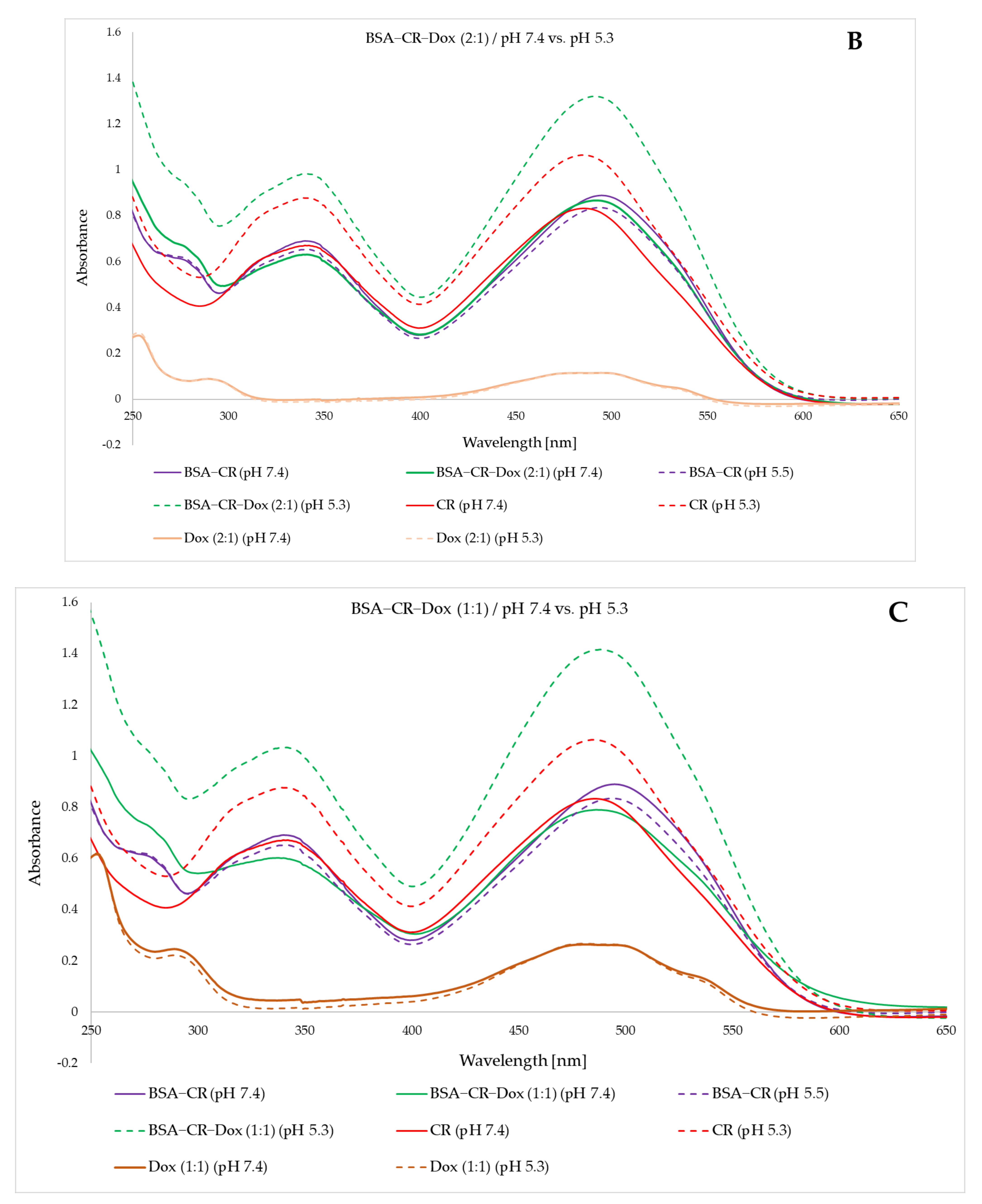
2.5. Changes in the UV/Vis Spectrum as a Result of Lowering the pH Indicate the Decomposition of the Complex (Three Different Molar Ratios)
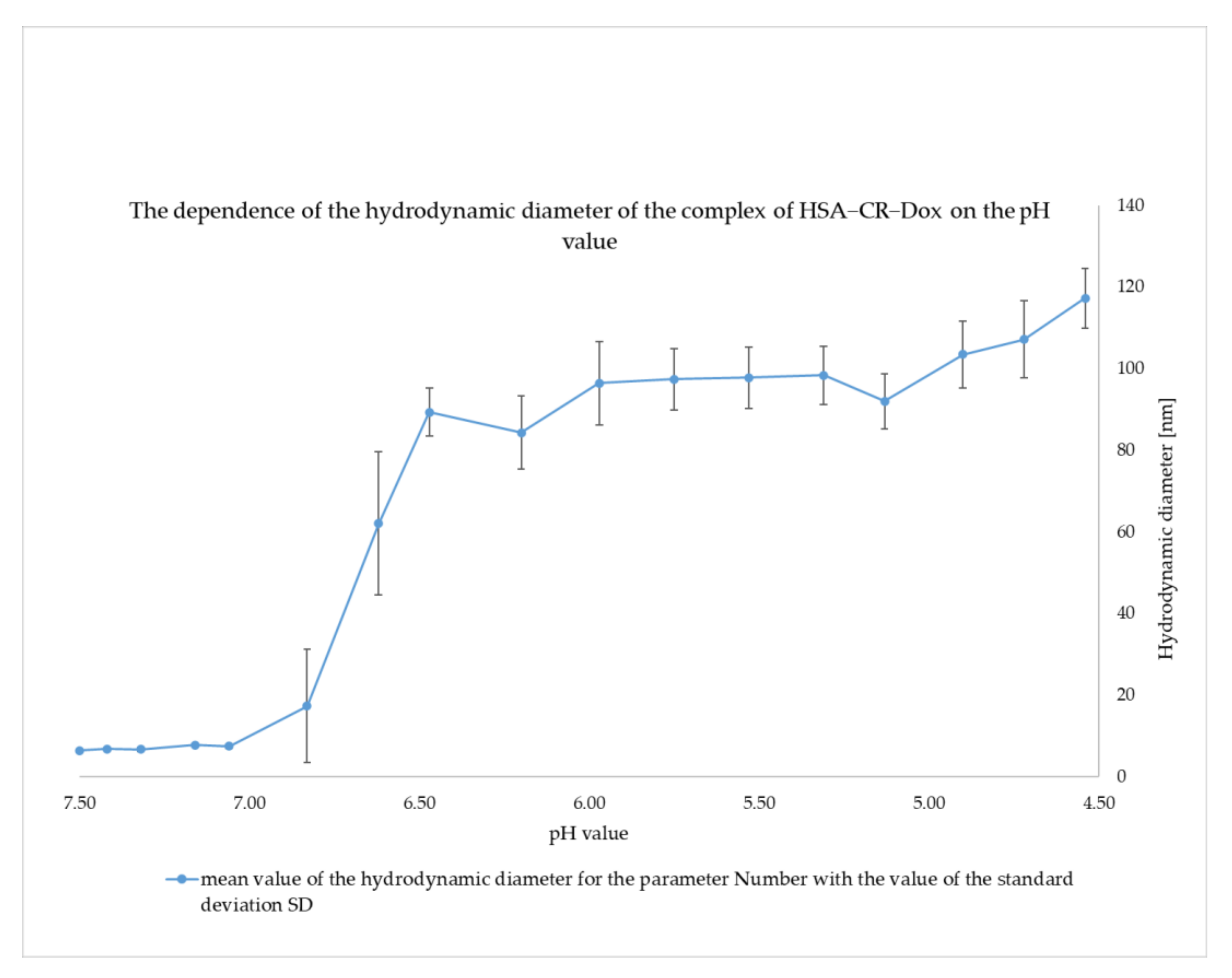
2.6. Change in Size of the BSA–CR–Dox System during a Smooth pH Change (pH Range 7.4 to 4.2). DLS
3. Discussion
4. Materials and Methods
4.1. Materials
4.2. Methods
4.2.1. Preparation of BSA–CR, CR–Dox, and BSA–CR–Dox Complexes
4.2.2. Characterization of CR–Dox or BSA–CR–Dox Complexes
- Assessment of differences between the complexes with different molar ratios after electrophoretic separation;
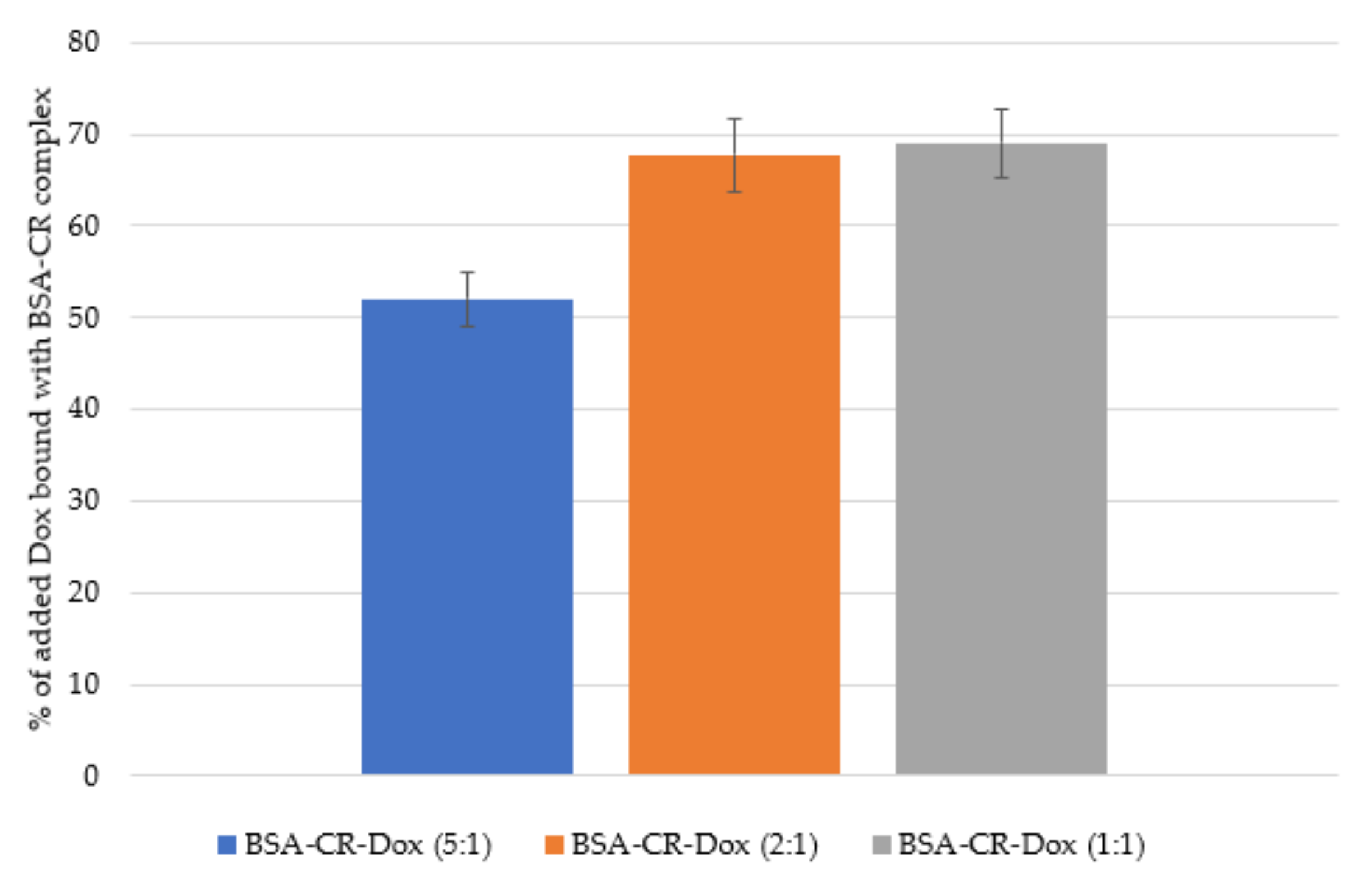
- Chromatographic and fluorimetric evaluation of the amount of Dox bound in the complexes;
- Assessment of Dox binding by BSA–CR complexes—gel filtration;
- Assessment of how CR-Dox binds to albumin—changes in the size of the BSA–CR–Dox systems after adding an additional portion of BSA (DLS);
4.2.3. Assessment of the Release of Dox after Lowering the pH
- Assessment of Dox release depending on the pH—dialysis;
- Assessment of Dox release depending on the pH—UV/VIS spectrum;
- Assessment of the stability of the tested complexes depending on the pH—Dynamic light scattering (DLS);
4.2.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Patra, J.K.; Das, G.; Fraceto, L.F.; Campos, E.V.R.; Rodriguez–Torres, M.D.P.; Acosta–Torres, L.S.; Diaz–Torres, L.A.; Grillo, R.; Swamy, M.K.; Sharma, S.; et al. Nano based drug delivery systems: Recent developments and future prospects. J. Nanobiotechnol. 2018, 16, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tiwari, G.; Tiwari, R.; Sriwastawa, B.; Bhati, L.; Pandey, S.; Pandey, P.; Bannerjee, S.K. Drug delivery systems: An updated review. Int. J. Pharm. Investig. 2012, 2, 2–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karimi, M.; Bahrami, S.; Ravari, S.B.; Zangabad, P.S.; Mirshekari, H.; Bozorgomid, M.; Shahreza, S.; Sori, M.; Hamblin, M.R. Albumin nano structures as advanced drug delivery systems. Expert Opin. Drug Deliv. 2016, 13, 1609–1623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zorzi, A.; Linciano, S.; Angelini, A. Non–covalent albumin–binding ligands for extending the circulating half–life of small biotherapeutics. MedChemComm 2019, 10, 1068–1081. [Google Scholar] [CrossRef]
- Rehman, M.T.; Khan, A.U. Understanding the interaction between human serum albumin and anti–bacterial/ anti–cancer compounds. Curr. Pharm. Des. 2015, 21, 1785–1799. [Google Scholar] [CrossRef]
- Riley, R.S.; June, C.H.; Langer, R.; Mitchell, M.J. Delivery Technologies For Cancer Immunotherapy. Nat. Rev. Drug Discov. 2019, 18, 175–196. [Google Scholar] [CrossRef]
- Milling, L.; Zhang, Y.; Irvine, D.J. Delivering safer immunotherapies for cancer. Adv. Drug Deliv. Rev. 2017, 114, 79–101. [Google Scholar] [CrossRef]
- Tripathi, J.; Thapa, P.; Maharjan, R.; Jeong, S.H. Current State and Future Perspectives on Gastroretentive Drug Delivery Systems. Pharmaceutics 2019, 11, 193. [Google Scholar] [CrossRef] [Green Version]
- Tambosi, G.; Felippi Coelo, P.; Luciano, S.; Schmücker Lenschow, I.C.; Zétola, M.; Stulzer, H.K.; Ramos Pezzini, B. Challenges to improve the biopharmaceutical properties of poorly water–soluble drugs and the application of the solid dispersion technology. Matéria (Rio De Jan.) 2018, 23, e-12224. [Google Scholar] [CrossRef]
- Baudino, T.A. Targeted Cancer Therapy: The Next Generation of Cancer Treatment. Curr. Drug Discov. Technol. 2015, 12, 3–20. [Google Scholar] [CrossRef]
- Lohcharoenkal, W.; Wang, L.; Chen, Y.C.; Rojanasakul, Y. Protein nanoparticles as drug delivery carriers for cancer therapy. BioMed Res. Int. 2014, 2014, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J. The Enhanced Permeability and Retention (EPR) Effect: The Significance of the Concept and Methods to Enhance Its Application. J. Pers. Med. 2021, 11, 771. [Google Scholar] [CrossRef] [PubMed]
- Desai, N.; Trieu, V.; Damascelli, B.; Soon–Shiong, P. SPARC expression correlates with tumor response to albumin–bound paclitaxel in head and neck cancer patients. Transl. Oncol. 2009, 2, 59–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, L.; Yuvienco, C.; Montclare, J.K. Protein Based Therapeutic Delivery Agents: Contemporary Developments and Challenges. Biomaterials 2017, 134, 91–116. [Google Scholar] [CrossRef]
- Sriraman, S.K.; Aryasomayajula, B.; Torchilin, V.P. Barriers to drug delivery in solid tumors. Tissue Barriers 2014, 2, e29528. [Google Scholar] [CrossRef] [Green Version]
- Fanali, G.; di Masi, A.; Trezza, V.; Marino, M.; Fasano, M.; Ascenzi, P. Human serum albumin: From bench to bedside. Mol. Asp. Med. 2012, 33, 209–290. [Google Scholar] [CrossRef]
- Hirose, M.; Tachibana, A.; Tanabe, T. Recombinant human serum albumin hydrogel as a novel drug delivery vehicle. Mater. Sci. Eng. C 2010, 30, 664–669. [Google Scholar] [CrossRef]
- Kratz, F. Albumin as a drug carrier: Design of prodrugs, drug conjugates and nanoparticles. J. Control. Release 2008, 132, 171–183. [Google Scholar] [CrossRef]
- Vallner, J.J. Binding of Drugs by Albumin Plasma Protein. J. Pharm. Sci. 1977, 66, 447–465. [Google Scholar] [CrossRef]
- Koch–Weser, J.; Sellers, E.M. Binding of Drugs to Serum Albumin. N. Engl. J. Med. 1976, 294, 311–316. [Google Scholar] [CrossRef]
- Chuanbo, L.; Zuojia, L.; Jin, W. Uncovering the molecular and physiological processes of anticancer leads binding human serum albumin: A physical insight into drug efficacy. PLoS ONE 2017, 12, e0178660. [Google Scholar] [CrossRef] [Green Version]
- Ulldemolins, M.; Roberts, J.A.; Rello, J.; Paterson, D.L.; Lipman, J. The Effects of Hypoalbuminaemia on Optimizing Antibacterial Dosing in Critically Ill Patients. Clin. Pharmacokinet. 2011, 50, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Moman, R.N.; Gupta, N.; Varacallo, M. Physiology, Albumin. In StatPearls Treasure Island (FL); StatPearls Publishing: Treasure Island, FL, USA, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK459198/ (accessed on 25 July 2021).
- Lee, P.; Wu, X. Review: Modifications of human serum albumin and their binding effect. Curr. Pharm. Des. 2015, 21, 1862–1865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goncharov, N.V.; Belinskaia, D.A.; Shmurak, V.I.; Terpilowski, M.A.; Jenkins, R.O.; Avdonin, P.V. Serum Albumin Binding and Esterase Activity: Mechanistic Interactions with Organophosphates. Molecules 2017, 22, 1201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karami, E.; Behdani, M.; Kazemi–Lomedasht, F. Albumin nanoparticles as nanocarriers for drug delivery: Focusing on antibody and nanobody delivery and albumin–based drugs. J. Drug Deliv. Sci. Technol. 2020, 55, 101471. [Google Scholar] [CrossRef]
- Stopa, B.; Rybarska, J.; Drozd, A.; Konieczny, L.; Król, M.; Lisowski, M.; Piekarska, B.; Roterman, I.; Spólnik, P.; Zemanek, G. Albumin binds self–assembling dyes as specific polymolecular ligands. Int. J. Biol. Macromol. 2006, 40, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Magdalena, P.-K.; Klaudia, K.; Jacek, K.; Katarzyna, C.; Mateusz, B.; Irena, R.; Anna, J. Structure and Location of Protein Sites Binding Self–Associated Congo Red Molecules with Intercalated Drugs as Compact Ligands—Theoretical Studies. Biomolecules 2021, 11, 501. [Google Scholar] [CrossRef]
- Jagusiak, A.; Chłopaś, K.; Zemanek, G.; Kościk, I.; Roterman, I. Interaction of Supramolecular Congo Red and Congo Red–Doxorubicin Complexes with Proteins for Drug Carrier Design. Pharmaceutics 2021, 13, 2027. [Google Scholar] [CrossRef]
- Wei, S.; Li, J.; He, H.; Shu, C.; Dardik, A.; Bai, H. A three–layered hydrogel patch with hierarchy releasing of PLGA nanoparticle drugs decrease neointimal hyperplasia. Smart Mater. Med. 2022, 3, 139–147. [Google Scholar] [CrossRef]
- Tong, P.; Sheng, Y.; Hou, R.; Iqbal, M.; Chen, L.; Li, J. Recent progress on coatings of biomedical magnesium alloy. Smart Mater. Med. 2022, 3, 104–116. [Google Scholar] [CrossRef]
- Amighi, F.; Emam–Djomeh, Z.; Labbafi–Mazraeh–Shahi, M. Effect of different cross–linking agents on the preparation of bovine serum albumin nanoparticles. J. Iran Chem. Soc. 2020, 17, 1223–1235. [Google Scholar] [CrossRef]
- Yue Gao, Y.; Nai, J.; Yang, Z.; Zhang, J.; Ma, S.; Zhao, Y.; Li, H.; Li, J.; Yang, Y.; Yang, M.; et al. A novel preparative method for nanoparticle albumin–bound paclitaxel with high drug loading and its evaluation both in vitro and in vivo. PLoS ONE 2021, 16, e0250670. [Google Scholar] [CrossRef]
- Aroulmoji, V.; Bergamin, M.; Erminio Murano, M.R. NMR Diffusion Studies on the Binding of Hyaluronate –Methotrexate Conjugates with Bovine Serum Albumin in Aqueous Solution. Int. J. Adv. Sci. Eng. 2015, 1, 12–17. [Google Scholar]
- Bolling, C.; Graefe, T.; Lübbing, C.; Jankevicius, F.; Uktveris, S.; Cesas, A.; Meyer–Moldenhauer, W.-H.; Starkmann, H.; Weigel, M.; Burk, K. Phase II study of MTX–HSA in combination with cisplatin as first line treatment in patients with advanced or metastatic transitional cell carcinoma. Investig. New Drugs 2006, 24, 521–527. [Google Scholar] [CrossRef]
- Wunder, A.; Müller–Ladner, U.; Stelzer, E.H.K.; Funk, J.; Neumann, E.; Stehle, G.; Pap, T.; Sinn, H.; Gay, S.; Fiehn, C. Albumin–Based Drug Delivery as Novel Therapeutic Approach for Rheumatoid Arthritis. J. Immunol. 2003, 170, 4793–4801. [Google Scholar] [CrossRef] [Green Version]
- Iglesias, J. nab–Paclitaxel (Abraxane®): An albumin–bound cytotoxic exploiting natural delivery mechanisms into tumors. Breast Cancer Res. 2009, 11 (Suppl. 1), 1. [Google Scholar] [CrossRef]
- Conlin, A.K.; Seidman, A.D.; Bach, A.; Lake, D.; Dickler, M.; D’Andrea, G.; Traina, T.; Danso, M.; Brufsky, A.M.; Saleh, M. Phase II trial of weekly nanoparticle albumin–bound paclitaxel with carboplatin and trastuzumab as first–line therapy for women with HER2–overexpressing metastatic breast cancer. Clin. Breast Cancer 2010, 10, 281–287. [Google Scholar] [CrossRef] [Green Version]
- Brown, M.A.; Mitar, D.A.; Whitworth, J.A. Measurement of Plasma Volume in Pregnancy. Clin. Sci. 1992, 83, 29–34. [Google Scholar] [CrossRef]
- Alves, N.G.; Motawe, Z.Y.; Yuan, S.Y.; Breslin, J.W. Chapter Four—Endothelial Protrusions in Junctional Integrity and Barrier Function. In Current Topics in Membranes; Belvitch, P., Dudek, S., Eds.; Academic Press: Cambridge, MA, USA, 2018; Volume 82, pp. 93–140. [Google Scholar] [CrossRef]
- Michael, E.G. Chapter 9—Clinical Evaluation of Adults. In Dysphagia, 3rd ed.; Michael, E., Groher, M., Crary, A., Eds.; Mosby: Maryland Heights, MO, USA, 2021; pp. 149–178. [Google Scholar] [CrossRef]
- Jiang, S.; Gong, X.; Zhao, X.; Zu, Y. Preparation, characterization, and antitumor activities of folate–decorated docetaxel–loaded human serum albumin nanoparticles. Drug Deliv. 2015, 22, 206–213. [Google Scholar] [CrossRef] [Green Version]
- Abu–Khalaf, M.M.; Baumgart, M.A.; Gettinger, S.N.; Doddamane, I.; Tuck, D.P.; Hou, S.; Chen, N.; Sullivan, C.; Lezon–Geyda, K.; Zelterman, D.; et al. Phase 1b study of the mammalian target of rapamycin inhibitor sirolimus in combination with nanoparticle albumin–bound paclitaxel in patients with advanced solid tumors. Cancer 2015, 121, 1817–1826. [Google Scholar] [CrossRef]
- LoRusso, P.M.; Sarantopoulos, J. A Phase 1 Trial of ABI–011 in Patients with Advanced Solid Tumors or Lymphomas. Available online: https://clinicaltrials.gov/ct2/show/study/NCT01163071 (accessed on 14 November 2019).
- Wan, X.; Zheng, X.; Pang, X.; Pang, Z.; Zhao, J.; Zhang, Z.; Jiang, T.; Xu, W.; Zhang, Q.; Jiang, X. Lapatinib–loaded human serum albumin nanoparticles for the prevention and treatment of triple–negative breast cancer metastasis to the brain. Oncotarget 2016, 7, 34038–34051. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.-R.; Suntharalingam, K.; Johnstone, T.C.; Yoo, H.; Lin, W.; Brooks, J.G.; Lippard, S.J. Pt(IV) Prodrugs Designed to Bind Non–Covalently to Human Serum Albumin for Drug Delivery. J. Am. Chem. Soc. 2014, 136, 8790–8798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qi, W.W.; Yu, H.Y.; Guo, H.; Lou, J.; Wang, Z.M.; Liu, P.; Sapin–Minet, A.; Maincent, P.; Hong, X.C.; Hu, X.M.; et al. Doxorubicin–loaded glycyrrhetinic acid modified recombinant human serum albumin nanoparticles for targeting liver tumor chemotherapy. Mol. Pharm. 2015, 12, 675–683. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Jeong, K.; Lee, Y.; Guo, T.; Lee, D.; Park, J.; Kwon, N.; Na, J.H.; Hong, S.K.; Cha, S.S.; et al. Water–Soluble Phthalocyanines Selectively Bind to Albumin Dimers: A Green Approach Toward Enhancing Tumor–Targeted Photodynamic Therapy. Theranostics 2019, 9, 6412–6423. [Google Scholar] [CrossRef]
- Tacar, O.; Sriamornsak, P.; Dass, C.R. Doxorubicin: An update on anticancer molecular action, toxicity and novel drug delivery systems. J. Pharm. Pharmacol. 2013, 65, 157–170. [Google Scholar] [CrossRef]
- Arcamone, F. Doxorubicin: Anticancer Antibiotics; Elsevier: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Yokoi, K.; Chan, D.; Kojic, M.; Milosevic, M.; Engler, D.; Matsunami, R.; Tanei, T.; Saito, Y.; Ferrari, M.; Ziemys, A. Liposomal doxorubicin extravasation controlled by phenotype–specific transport properties of tumor microenvironment and vascular barrier. J. Control. Release 2015, 217, 293–299. [Google Scholar] [CrossRef] [Green Version]
- Contreras, L.; Villarroel, I.; Torres, C.; Rozas, R. Doxorubicin Encapsulation in Carbon Nanotubes Having Haeckelite or Stone–Wales Defects as Drug Carriers: A Molecular Dynamics Approach. Molecules 2021, 26, 1586. [Google Scholar] [CrossRef]
- Matyszewska, D. Drug delivery systems in the transport of doxorubicin. Surf. Innov. 2014, 2, 201–210. [Google Scholar] [CrossRef]
- Quan, Q.; Xie, J.; Gao, H.; Yang, M.; Zhang, F.; Liu, G.; Lin, X.; Wang, A.; Eden, H.S.; Lee, S.; et al. HSA coated iron oxide nanoparticles as drug delivery vehicles for cancer therapy. Mol. Pharm. 2011, 8, 1669–1676. [Google Scholar] [CrossRef] [Green Version]
- Bae, S.; Ma, K.; Kim, T.H.; Lee, E.S.; Oh, K.T.; Park, E.-S.; Lee, K.C.; Youn, Y.S. Doxorubicin–loaded human serum albumin nanoparticles surface–modified with TNF–related apoptosis–inducing ligand and transferrin for targeting multiple tumor types. Biomaterials 2012, 33, 1536–1546. [Google Scholar] [CrossRef]
- Lee, H.; Park, S.; Kim, J.B.; Kim, J.; Kim, H. Entrapped doxorubicin nanoparticles for the treatment of metastatic anoikis–resistant cancer cells. Cancer Lett. 2013, 332, 110–119. [Google Scholar] [CrossRef] [PubMed]
- Agudelo, D.; Bourassa, P.; Bruneau, J.; Bérubé, G.; Asselin, E.; Tajmir–Riahi, H. Probing the binding sites of antibiotic drugs doxorubicin and N–(trifluoroacetyl) doxorubicin with human and bovine serum albumins. PLoS ONE 2012, 7, e43814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kratz, F. A clinical update of using albumin as a drug vehicle—A commentary. J. Control. Release 2014, 190, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Peters, T., Jr. All about Albumin: Biochemistry, Genetics, and Medical Applications; Academic Press: Cambridge, MA, USA, 1995. [Google Scholar]
- Jagusiak, A.; Chlopas, K.; Zemanek, G.; Wolski, P.; Panczyk, T. Controlled Release of Doxorubicin from the Drug Delivery Formulation Composed of Single–Walled Carbon Nanotubes and Congo Red: A Molecular Dynamics Study and Dynamic Light Scattering Analysis. Pharmaceutics 2020, 12, 622. [Google Scholar] [CrossRef]
- Deb, P.K.; Al–Attraqchi, O.; Prasad, M.R.; Tekade, R.K. Chapter 11 Protein and Tissue Binding: Implication on Pharmacokinetic Parameters. In Advances in Pharmaceutical Product Development and Research, Dosage Form Design Considerations; Tekade, R., Ed.; Academic Press: Cambridge, MA, USA, 2018; pp. 371–399. [Google Scholar] [CrossRef]
- Chubarov, A.; Spitsyna, A.; Krumkacheva, O.; Mitin, D.; Suvorov, D.; Tormyshev, V.; Fedin, M.; Bowman, M.K.; Bagryanskaya, E. Reversible Dimerization of Human Serum Albumin. Molecules 2020, 26, 108. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Elution Volume (Ve) | BSA–CR–Dox (5:1) | BSA–CR–Dox (2:1) | CR–Dox (5:1) | CR–Dox (2:1) | BSA–CR | BSA |
|---|---|---|---|---|---|---|
| BSA [mL] | 0.6 | 0.3 | - | - | 0.6 | 0.7 |
| CR [mL] | 0.6 | 0.3 | 0.8 | 0.3 | 0.6 | - |
| Dox [mL] | 0.6 | 0.3 | 0.8 | 0.3 | - | - |
| Complex creation | YES | YES | YES | YES | YES | - |
| Elution Volume (Ve) | BSA–CR–Dox (2:1) pH 7.4 | BSA–CR–Dox (2:1) pH 5.5 |
|---|---|---|
| BSA [mL] | 0.6 | 0.4 |
| CR [mL] | 0.6 | 0.4 |
| Dox [mL] | 0.6 | 0.4 |
| Complex creation | YES | YES |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jagusiak, A.; Chłopaś, K.; Zemanek, G.; Kościk, I.; Skorek, P.; Stopa, B. Albumin Binds Doxorubicin via Self–Assembling Dyes as Specific Polymolecular Ligands. Int. J. Mol. Sci. 2022, 23, 5033. https://doi.org/10.3390/ijms23095033
Jagusiak A, Chłopaś K, Zemanek G, Kościk I, Skorek P, Stopa B. Albumin Binds Doxorubicin via Self–Assembling Dyes as Specific Polymolecular Ligands. International Journal of Molecular Sciences. 2022; 23(9):5033. https://doi.org/10.3390/ijms23095033
Chicago/Turabian StyleJagusiak, Anna, Katarzyna Chłopaś, Grzegorz Zemanek, Izabela Kościk, Paweł Skorek, and Barbara Stopa. 2022. "Albumin Binds Doxorubicin via Self–Assembling Dyes as Specific Polymolecular Ligands" International Journal of Molecular Sciences 23, no. 9: 5033. https://doi.org/10.3390/ijms23095033
APA StyleJagusiak, A., Chłopaś, K., Zemanek, G., Kościk, I., Skorek, P., & Stopa, B. (2022). Albumin Binds Doxorubicin via Self–Assembling Dyes as Specific Polymolecular Ligands. International Journal of Molecular Sciences, 23(9), 5033. https://doi.org/10.3390/ijms23095033