
The Potential Impact of Neuroimaging and Translational Research on the Clinical Management of Lacunar Stroke



Abstract
1. Introduction: Clinical Relevance and Aims of the Review
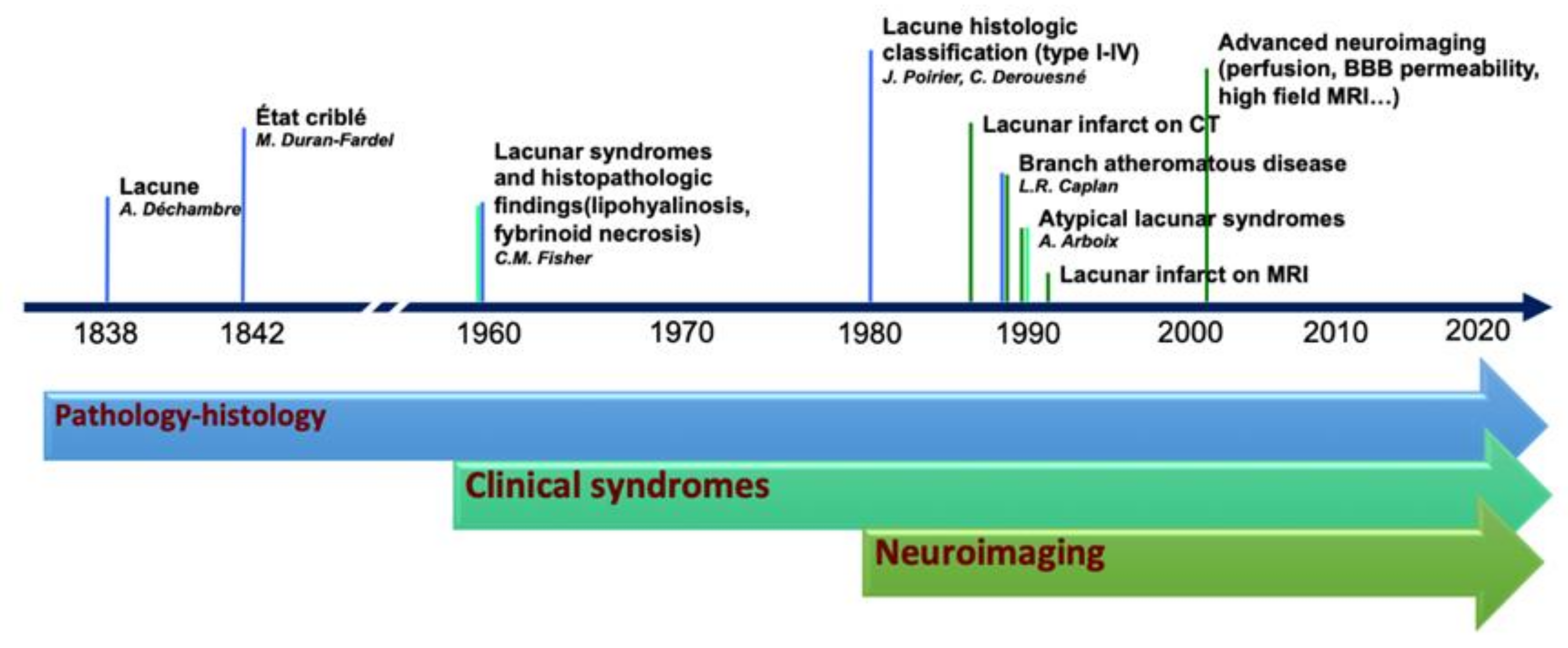
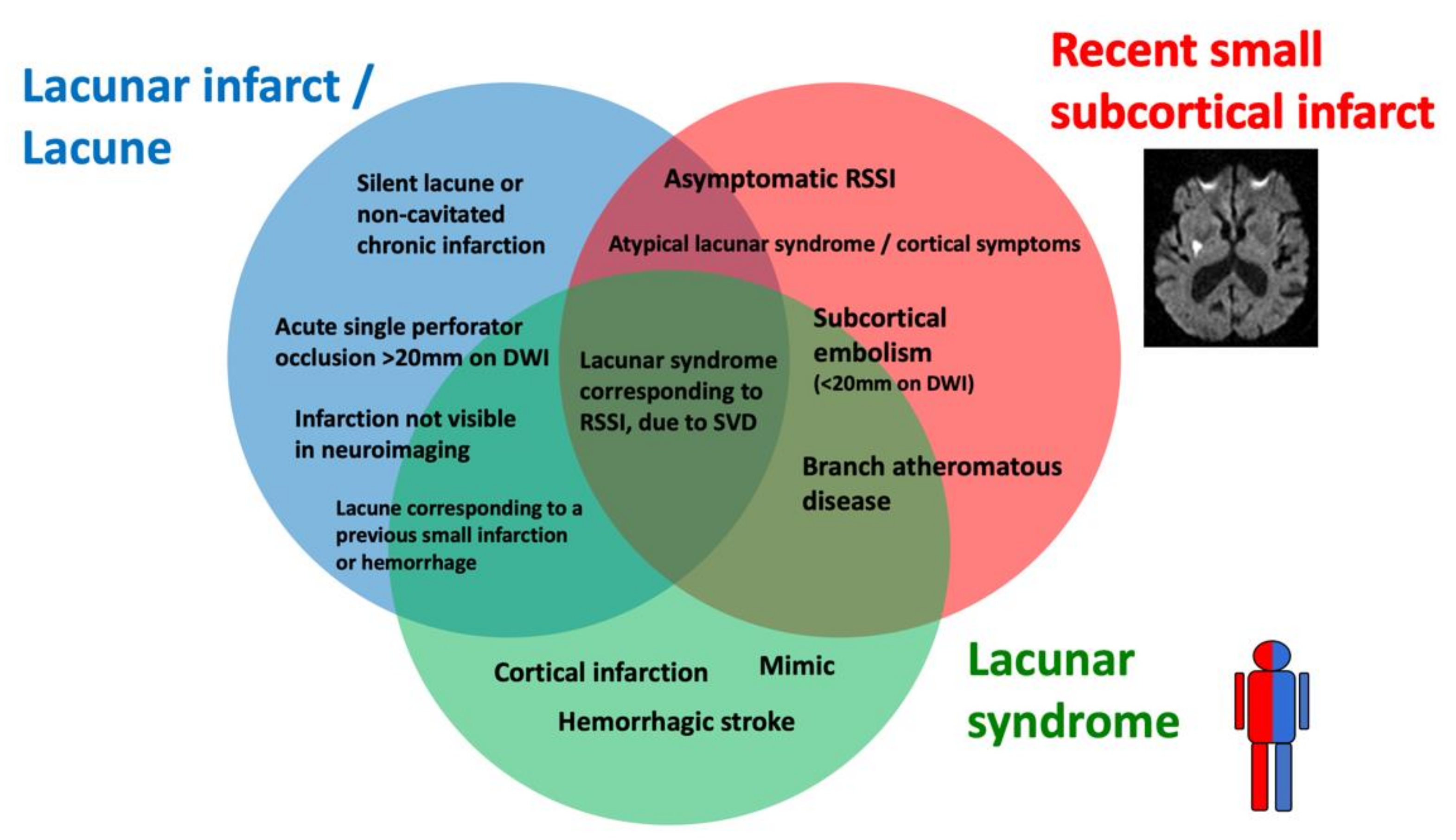
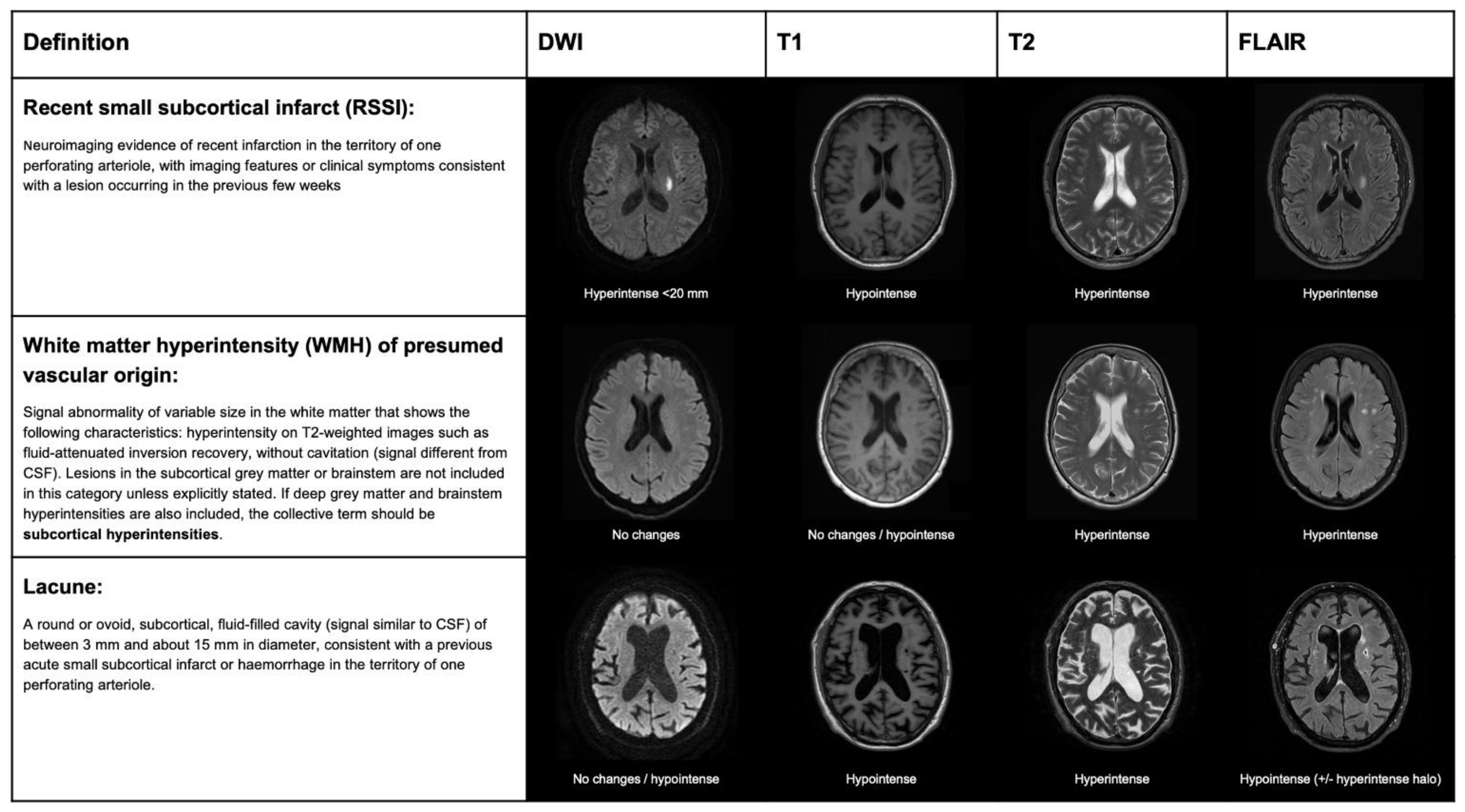
2. Terminology and Correlations between Histopathological, Clinical and Imaging Definitions
3. Mechanisms of Lacunar Strokes: From Pathology Studies to Advanced Neuroimaging
4. Plasmatic Biomarkers in Patients with Lacunar Strokes
5. Insights from Translational Research
6. Prevalence and Diagnostic/Topographic Accuracy of the Lacunar Syndromes
7. Neuroimaging in Patients with Suspected Lacunar Stroke
8. Lacunar Stroke Management
9. Intravenous Thrombolysis
10. Secondary Prevention
10.1. Antplatelets
10.2. Statins
10.3. Anti-Hypertensive Treatments
10.4. Lifestyle Interventions
11. New Molecular Targets in Lacunar Stroke
12. Future Directions
13. Limitations of the Review
14. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Arboix, A.; Martí-Vilalta, J.L. New Concepts in Lacunar Stroke Etiology: The Constellation of Small-Vessel Arterial Disease. Cerebrovasc. Dis. 2004, 17 (Suppl. 1), 58–62. [Google Scholar] [CrossRef] [PubMed]
- Norrving, B. Long-Term Prognosis after Lacunar Infarction. Lancet Neurol. 2003, 2, 238–245. [Google Scholar] [CrossRef]
- Blanco-Rojas, L.; Arboix, A.; Canovas, D.; Grau-Olivares, M.; Oliva Morera, J.C.; Parra, O. Cognitive Profile in Patients with a First-Ever Lacunar Infarct with and without Silent Lacunes: A Comparative Study. BMC Neurol. 2013, 13. [Google Scholar] [CrossRef] [PubMed]
- Wardlaw, J.M.; Smith, C.; Dichgans, M. Small Vessel Disease: Mechanisms and Clinical Implications. Lancet Neurol. 2019, 18, 684–696. [Google Scholar] [CrossRef]
- Wardlaw, J.M.; Smith, E.E.; Biessels, G.J.; Cordonnier, C.; Fazekas, F.; Frayne, R.; Lindley, R.I.; O’Brien, J.T.; Barkhof, F.; Benavente, O.R.; et al. Neuroimaging Standards for Research into Small Vessel Disease and Its Contribution to Ageing and Neurodegeneration. Lancet Neurol. 2013, 12, 822–838. [Google Scholar] [CrossRef]
- Bailey, E.L.; Mcculloch, J.; Sudlow, C.; Wardlaw, J.M. Potential Animal Models of Lacunar Stroke: A Systematic Review. Stroke 2009, 40, e451–e458. [Google Scholar] [CrossRef]
- Mustapha, M.; Nassir, C.M.N.C.M.; Aminuddin, N.; Safri, A.A.; Ghazali, M.M. Cerebral Small Vessel Disease (CSVD)—Lessons from the Animal Models. Front. Physiol. 2019, 10, 1317. [Google Scholar] [CrossRef]
- Fisher, C.M. Lacunar Strokes and Infarcts: A Review. Neurology 1982, 32, 871–876. [Google Scholar] [CrossRef]
- Poirier, J.; Derouesne, C. Cerebral Lacunae. A Proposed New Classification. Clin. Neuropathol. 1984, 3, 266. [Google Scholar]
- Lammie, G.A. Hypertensive Cerebral Small Vessel Disease and Stroke. Brain Pathol. 2002, 12, 358–370. [Google Scholar] [CrossRef]
- Bailey, E.L.; Smith, C.; Sudlow, C.L.M.; Wardlaw, J.M. Pathology of Lacunar Ischemic Stroke in Humans—A Systematic Review. Brain Pathol. 2012, 22, 583–591. [Google Scholar] [CrossRef]
- Adams, H.P., Jr.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E., 3rd. Classification of Subtype of Acute Ischemic Stroke. Definitions for Use in a Multicenter Clinical Trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef]
- Amarenco, P.; Bogousslavsky, J.; Caplan, L.R.; Donnan, G.A.; Wolf, M.E.; Hennerici, M.G. The ASCOD Phenotyping of Ischemic Stroke (Updated ASCO Phenotyping). Cerebrovasc. Dis. 2013, 36, 1–5. [Google Scholar] [CrossRef]
- Ay, H.; Furie, K.L.; Singhal, A.; Smith, W.S.; Sorensen, A.G.; Koroshetz, W.J. An Evidence-Based Causative Classification System for Acute Ischemic Stroke. Ann. Neurol. 2005, 58, 688–697. [Google Scholar] [CrossRef]
- Humphreys, C.A.; Smith, C.; Wardlaw, J.M. Correlations in Post-Mortem Imaging-Histopathology Studies of Sporadic Human Cerebral Small Vessel Disease: A Systematic Review. Neuropathol. Appl. Neurobiol. 2021. [Google Scholar] [CrossRef]
- Wardlaw, J.M.; Smith, C.; Dichgans, M. Mechanisms of Sporadic Cerebral Small Vessel Disease: Insights from Neuroimaging. Lancet Neurol. 2013, 12, 483–497. [Google Scholar] [CrossRef]
- Regenhardt, R.W.; Das, A.S.; Lo, E.H.; Caplan, L.R. Advances in Understanding the Pathophysiology of Lacunar Stroke: A Review. JAMA Neurol. 2018, 75, 1273–1281. [Google Scholar] [CrossRef]
- Caplan, L.R. Lacunar Infarction and Small Vessel Disease: Pathology and Pathophysiology. J. Stroke 2015, 17, 2–6. [Google Scholar] [CrossRef]
- Xie, W.; Wang, C.; Liu, S.; Tang, R.; Chai, S.; Guo, Y.; Qian, T.; Chang, B.; Yang, Q.; Fan, Z.; et al. Visualization of Lenticulostriate Artery by Intracranial Dark-Blood Vessel Wall Imaging and Its Relationships with Lacunar Infarction in Basal Ganglia: A Retrospective Study. Eur. Radiol. 2021, 31, 5629–5639. [Google Scholar] [CrossRef]
- Ling, C.; Fang, X.; Kong, Q.; Sun, Y.; Wang, B.; Zhuo, Y.; An, J.; Zhang, W.; Wang, Z.; Zhang, Z.; et al. Lenticulostriate Arteries and Basal Ganglia Changes in Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy, a High-Field Mri Study. Front. Neurol. 2019, 10, 1–9. [Google Scholar] [CrossRef]
- Arboix, A.; Altés, E.; García-Eroles, L.; Massons, J. Clinical Study of Lacunar Infarcts in Non-Hypertensive Patients. J. Stroke Cerebrovasc. Dis. 2003, 12, 232–236. [Google Scholar] [CrossRef] [PubMed]
- Zonneveld, T.P.; Richard, E.; Vergouwen, M.D.I.; Nederkoorn, P.J.; de Haan, R.; Roos, Y.B.; Kruyt, N.D. Blood Pressure-Lowering Treatment for Preventing Recurrent Stroke, Major Vascular Events, and Dementia in Patients with a History of Stroke or Transient Ischaemic Attack. Cochrane Database Syst. Rev. 2018, 7, CD007858. [Google Scholar] [CrossRef] [PubMed]
- Sps, T.; Group, S. Blood-Pressure Targets in Patients with Recent Lacunar Stroke: The SPS3 Randomised Trial. Lancet 2013, 382, 507–515. [Google Scholar] [CrossRef]
- Petrone, L.; Nannoni, S.; Del Bene, A.; Palumbo, V.; Inzitari, D. Branch Atheromatous Disease: A Clinically Meaningful, yet Unproven Concept. Cerebrovasc. Dis. 2016, 41, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Caplan, L.R. Intracranial Branch Atheromatous Disease: A Neglected, Understudied, and Underused Concept. Neurology 1989, 39, 1246–1250. [Google Scholar] [CrossRef]
- Amarenco, P.; Bogousslavsky, J.; Callahan, A.; Goldstein, L.B.; Hennerici, M.; Rudolph, A.E.; Sillesen, H.; Simunovic, L.; Szarek, M.; Welch, K.M.A.; et al. High-Dose Atorvastatin after Stroke or Transient Ischemic Attack. Curr. Atheroscler. Rep. 2007, 9, 96. [Google Scholar] [CrossRef]
- Suzuki, T.; Natori, T.; Sasaki, M.; Miyazawa, H.; Narumi, S.; Ito, K.; Kamada, A.; Yoshida, M.; Tsuda, K.; Yoshioka, K.; et al. Evaluating Recanalization of Relevant Lenticulostriate Arteries in Acute Ischemic Stroke Using High-Resolution MRA at 7T. Int. J. Stroke 2021, 16, 1039–1046. [Google Scholar] [CrossRef]
- Rudilosso, S.; Laredo, C.; Mancosu, M.; Moya-Planas, N.; Zhao, Y.; Chirife, O.; Chamorro, Á.; Urra, X. Cerebral Perfusion and Compensatory Blood Supply in Patients with Recent Small Subcortical Infarcts. J. Cereb. Blood Flow Metab. 2019, 39, 1326–1335. [Google Scholar] [CrossRef]
- Rydén, L.; Sacuiu, S.; Wetterberg, H.; Najar, J.; Guo, X.; Kern, S.; Zettergren, A.; Shams, S.; Pereira, J.B.; Wahlund, L.-O.; et al. Atrial Fibrillation, Stroke, and Silent Cerebrovascular Disease: A Population-Based MRI Study. Neurology 2021, 97, e1608–e1619. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, Y.J.; Moon, Y.; Cho, H.J.; Kim, H.Y. Acute Simultaneous Multiple Lacunar Infarcts: A Severe Disease Entity in Small Artery Disease. Eur. Neurol. 2012, 67, 303–311. [Google Scholar] [CrossRef]
- Stewart, C.R.; Stringer, M.S.; Shi, Y.; Thrippleton, M.J.; Wardlaw, J.M. Associations Between White Matter Hyperintensity Burden, Cerebral Blood Flow and Transit Time in Small Vessel Disease: An Updated Meta-Analysis. Front. Neurol. 2021, 12, 647848. [Google Scholar] [CrossRef]
- Wardlaw, J.; Bath, P.M.W.; Doubal, F.; Heye, A.; Sprigg, N.; Woodhouse, L.J.; Blair, G.; Appleton, J.; Cvoro, V.; England, T.; et al. Protocol: The Lacunar Intervention Trial 2 (LACI-2). A Trial of Two Repurposed Licenced Drugs to Prevent Progression of Cerebral Small Vessel Disease. Eur. Stroke J. 2020, 5. [Google Scholar] [CrossRef]
- Roseborough, A.D.; Rasheed, B.; Jung, Y.; Nishimura, K.; Pinsky, W.; Langdon, K.D.; Hammond, R.; Pasternak, S.H.; Khan, A.R.; Whitehead, S.N. Microvessel Stenosis, Enlarged Perivascular Spaces, and Fibrinogen Deposition Are Associated with Ischemic Periventricular White Matter Hyperintensities. Brain Pathol. 2021, 32, e13017. [Google Scholar] [CrossRef]
- Simpson, J.E.; Wharton, S.B.; Cooper, J.; Gelsthorpe, C.; Baxter, L.; Forster, G.; Shaw, P.J.; Savva, G.; Matthews, F.E.; Brayne, C.; et al. Alterations of the Blood-Brain Barrier in Cerebral White Matter Lesions in the Ageing Brain. Neurosci. Lett. 2010, 486, 246–251. [Google Scholar] [CrossRef]
- Low, A.; Mak, E.; Rowe, J.B.; Markus, H.S.; O’Brien, J.T. Inflammation and Cerebral Small Vessel Disease: A Systematic Review. Ageing Res. Rev. 2019, 53, 100916. [Google Scholar] [CrossRef]
- Wardlaw, J.M. Blood-Brain Barrier and Cerebral Small Vessel Disease. J. Neurol. Sci. 2010, 299, 66–71. [Google Scholar] [CrossRef]
- Hainsworth, A.H.; Minett, T.; Andoh, J.; Forster, G.; Bhide, I.; Barrick, T.R.; Elderfield, K.; Jeevahan, J.; Markus, H.S.; Bridges, L.R. Neuropathology of White Matter Lesions, Blood-Brain Barrier Dysfunction, and Dementia. Stroke 2017, 48, 2799–2804. [Google Scholar] [CrossRef]
- Wharton, S.B.; Simpson, J.E.; Brayne, C.; Ince, P.G. Age-Associated White Matter Lesions: The MRC Cognitive Function and Ageing Study. Brain Pathol. 2015, 25, 35–43. [Google Scholar] [CrossRef]
- Wiseman, S.; Marlborough, F.; Doubal, F.; Webb, D.J.; Wardlaw, J. Blood Markers of Coagulation, Fibrinolysis, Endothelial Dysfunction and Inflammation in Lacunar Stroke versus Non-Lacunar Stroke and Non-Stroke: Systematic Review and Meta-Analysis. Cerebrovasc. Dis. 2014, 37, 64–75. [Google Scholar] [CrossRef]
- Kelly, P.; Weimar, C.; Lemmens, R.; Murphy, S.; Purroy, F.; Arsovska, A.; Bornstein, N.M.; Czlonkowska, A.; Fischer, U.; Fonseca, A.C.; et al. Colchicine for Prevention of Vascular Inflammation in Non-CardioEmbolic Stroke (CONVINCE)—Study Protocol for a Randomised Controlled Trial. Eur. Stroke J. 2021, 6, 222–228. [Google Scholar] [CrossRef]
- Chamorro, Á.; Amaro, S.; Castellanos, M.; Segura, T.; Arenillas, J.; Martí-Fábregas, J.; Gállego, J.; Krupinski, J.; Gomis, M.; Cánovas, D.; et al. Safety and Efficacy of Uric Acid in Patients with Acute Stroke (URICO-ICTUS): A Randomised, Double-Blind Phase 2b/3 Trial. Lancet Neurol. 2014, 13, 453–460. [Google Scholar] [CrossRef]
- Ridker, P.M.; Thuren, T.; Zalewski, A.; Libby, P. Interleukin-1β Inhibition and the Prevention of Recurrent Cardiovascular Events: Rationale and Design of the Canakinumab Anti-Inflammatory Thrombosis Outcomes Study (CANTOS). Am. Heart J. 2011, 162, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Rudilosso, S.; Urra, X.; San Roman, L.; Laredo, C.; Lopez-Rueda, A.; Amaro, S.; Oleaga, L.; Chamorro, A. Perfusion Deficits and Mismatch in Patients with Acute Lacunar Infarcts Studied with Whole-Brain CT Perfusion. Am. J. Neuroradiol. 2015, 36, 1407–1412. [Google Scholar] [CrossRef] [PubMed]
- Förster, A.; Kerl, H.U.; Wenz, H.; Brockmann, M.A.; Nölte, I.; Groden, C. Diffusion- and Perfusion-Weighted Imaging in Acute Lacunar Infarction: Is There a Mismatch? PLoS ONE 2013, 8, e77428. [Google Scholar] [CrossRef]
- Förster, A.; Mürle, B.; Böhme, J.; Al-Zghloul, M.; Kerl, H.U.; Wenz, H.; Groden, C. Perfusion-Weighted Imaging and Dynamic 4D Angiograms for the Estimation of Collateral Blood Flow in Lacunar Infarction. J. Cereb. Blood Flow Metab. 2016, 36, 1744–1754. [Google Scholar] [CrossRef]
- Huang, Y.C.; Lee, J.D.; Pan, Y.T.; Weng, H.H.; Yang, J.T.; Lin, L.C.; Tsai, Y.H. Perfusion Defects and Collateral Flow Patterns in Acute Small Subcortical Infarction: A 4D Dynamic MRI Study. Transl. Stroke Res. 2021. [Google Scholar] [CrossRef]
- Smirnov, M.; Destrieux, C.; Maldonado, I.L. Cerebral White Matter Vasculature: Still Uncharted? Brain 2021, 144, 3561–3575. [Google Scholar] [CrossRef]
- Jouvent, E.; Duering, M.; Chabriat, H. Cerebral Autosomal Dominant Arteriopathy With Subcortical Infarcts and Leukoencephalopathy: Lessons from Neuroimaging. Stroke 2020, 51, 21–28. [Google Scholar] [CrossRef]
- Choi, J.C. Genetics of Cerebral Small Vessel Disease. J. Stroke 2015, 17, 7–16. [Google Scholar] [CrossRef]
- Muiño, E.; Fernández-Cadenas, I.; Arboix, A. Contribution of “Omic” Studies to the Understanding of CADASIL. A Systematic Review. Int. J. Mol. Sci. 2021, 22, 7357. [Google Scholar] [CrossRef]
- Mancuso, M.; Arnold, M.; Bersano, A.; Burlina, A.; Chabriat, H.; Debette, S.; Enzinger, C.; Federico, A.; Filla, A.; Finsterer, J.; et al. Monogenic Cerebral Small-Vessel Diseases: Diagnosis and Therapy. Consensus Recommendations of the European Academy of Neurology. Eur. J. Neurol. 2020, 27, 909–927. [Google Scholar] [CrossRef]
- Smith, E.E.; Biessels, G.J.; De Guio, F.; de Leeuw, F.E.; Duchesne, S.; Düring, M.; Frayne, R.; Ikram, M.A.; Jouvent, E.; MacIntosh, B.J.; et al. Harmonizing Brain Magnetic Resonance Imaging Methods for Vascular Contributions to Neurodegeneration. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2019, 11, 191–204. [Google Scholar] [CrossRef]
- Lee, J.M.; Grabb, M.C.; Zipfel, G.J.; Choi, D.W. Brain Tissue Responses to Ischemia. J. Clin. Investig. 2000, 106, 723–731. [Google Scholar] [CrossRef]
- Kim, J.G.; Choi, H.; Sohn, S.Y.; Kim, D.H.; Lee, S.J. Transient Ischemic Attacks Preceding Acute Lacunar Infarction. Eur. Neurol. 2016, 76, 278–283. [Google Scholar] [CrossRef]
- Rudilosso, S.; Urra, X.; Chirife, O.; Chamorro, Á. Altered Brain Computed Tomography Perfusion in Patients with Fluctuating Lacunar Syndrome and Normal Magnetic Resonance Imaging. JAMA Neurol. 2016, 73, 348–349. [Google Scholar] [CrossRef]
- Donnan, G.A.; O’Malley, H.M.; Quang, L.; Hurley, S.; Bladin, P.F. The Capsular Warning Syndrome: Pathogenesis and Clinical Features. Neurology 1993, 43, 957–962. [Google Scholar] [CrossRef]
- Camps-Renom, P.; Delgado-Mederos, R.; Martínez-Domeño, A.; Prats-Sánchez, L.; Cortés-Vicente, E.; Simón-Talero, M.; Arboix, A.; Ois, Á.; Purroy, F.; Martí-Fàbregas, J. Clinical Characteristics and Outcome of the Capsular Warning Syndrome: A Multicenter Study. Int. J. Stroke 2015, 10, 571–575. [Google Scholar] [CrossRef]
- Saposnik, G.; De Tilly, L.N.; Caplan, L.R. Pontine Warning Syndrome. Arch. Neurol. 2008, 65, 1375–1377. [Google Scholar] [CrossRef]
- Muengtaweepongsa, S.; Singh, N.N.; Cruz-Flores, S. Pontine Warning Syndrome: Case Series and Review of Literature. J. Stroke Cerebrovasc. Dis. 2010, 19, 353–356. [Google Scholar] [CrossRef]
- He, L.; Xu, R.; Wang, J.; Zhang, L.; Zhang, L.; Zhou, F.; Dong, W. Capsular Warning Syndrome: Clinical Analysis and Treatment. BMC Neurol. 2019, 19, 1–7. [Google Scholar] [CrossRef]
- Rudilosso, S.; Olivera, M.; Esteller, D.; Laredo, C.; Amaro, S.; Llull, L.; Renú, A.; Obach, V.; Vera, V.; Rodríguez, A.; et al. Susceptibility Vessel Sign in Deep Perforating Arteries in Patients with Recent Small Subcortical Infarcts. J. Stroke Cerebrovasc. Dis. 2021, 30, 1–7. [Google Scholar] [CrossRef]
- Jiang, S.; Yan, Y.; Yang, T.; Zhu, Q.; Wang, C.; Bai, X.; Hao, Z.; Zhang, S.; Yang, Q.; Fan, Z.; et al. Plaque Distribution Correlates with Morphology of Lenticulostriate Arteries in Single Subcortical Infarctions. Stroke 2020, 51, 2801–2809. [Google Scholar] [CrossRef]
- Zhang, Z.; Fan, Z.; Kong, Q.; Xiao, J.; Wu, F.; An, J.; Yang, Q.; Li, D.; Zhuo, Y. Visualization of the Lenticulostriate Arteries at 3T Using Black-Blood T1-Weighted Intracranial Vessel Wall Imaging: Comparison with 7T TOF-MRA. Eur. Radiol. 2019, 29, 1452–1459. [Google Scholar] [CrossRef]
- Wardlaw, J.M.; Doubal, F.; Armitage, P.; Chappell, F.; Carpenter, T.; Muñoz Maniega, S.; Farrall, A.; Sudlow, C.; Dennis, M.; Dhillon, B. Lacunar Stroke Is Associated with Diffuse Blood-Brain Barrier Dysfunction. Ann. Neurol. 2009, 65, 194–202. [Google Scholar] [CrossRef]
- Blair, G.W.; Thrippleton, M.J.; Shi, Y.; Hamilton, I.; Stringer, M.; Chappell, F.; Dickie, D.A.; Andrews, P.; Marshall, I.; Doubal, F.N.; et al. Intracranial Hemodynamic Relationships in Patients with Cerebral Small Vessel Disease. Neurology 2020, 94, e2258–e2269. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, S.F.; Doubal, F.N.; Shuler, K.; Wardlaw, J.M. A Systematic Review of Dynamic Cerebral and Peripheral Endothelial Function in Lacunar Stroke versus Controls. Stroke 2010, 41, 434–442. [Google Scholar] [CrossRef]
- Moreau, F.; Patel, S.; Lauzon, M.L.; McCreary, C.R.; Goyal, M.; Frayne, R.; Demchuk, A.M.; Coutts, S.B.; Smith, E.E. Cavitation after Acute Symptomatic Lacunar Stroke Depends on Time, Location, and MRI Sequence. Stroke 2012, 43, 1837–1842. [Google Scholar] [CrossRef]
- Lee, K.J.; Jung, H.; Oh, Y.S.; Lim, E.Y.; Cho, A.H. The Fate of Acute Lacunar Lesions in Terms of Shape and Size. J. Stroke Cerebrovasc. Dis. 2017, 26, 1254–1257. [Google Scholar] [CrossRef]
- Gattringer, T.; Valdes Hernandez, M.; Heye, A.; Armitage, P.A.; Makin, S.; Chappell, F.; Pinter, D.; Doubal, F.; Enzinger, C.; Fazekas, F.; et al. Predictors of Lesion Cavitation After Recent Small Subcortical Stroke. Transl. Stroke Res. 2020, 11, 402–411. [Google Scholar] [CrossRef]
- Benjamin, P.; Trippier, S.; Lawrence, A.J.; Lambert, C.; Zeestraten, E.; Williams, O.A.; Patel, B.; Morris, R.G.; Barrick, T.R.; MacKinnon, A.D.; et al. Lacunar Infarcts, but Not Perivascular Spaces, Are Predictors of Cognitive Decline in Cerebral Small-Vessel Disease. Stroke 2018, 49, 586–593. [Google Scholar] [CrossRef]
- del C. Valdés Hernández, M.; Maconick, L.C.; Muñoz Maniega, S.; Wang, X.; Wiseman, S.; Armitage, P.A.; Doubal, F.N.; Makin, S.; Sudlow, C.L.; Dennis, M.S.; et al. A Comparison of Location of Acute Symptomatic vs. “silent” Small Vessel Lesions. Int. J. Stroke 2015, 10, 1044–1050. [Google Scholar] [CrossRef] [PubMed]
- Duering, M.; Csanadi, E.; Gesierich, B.; Jouvent, E.; Hervé, D.; Seiler, S.; Belaroussi, B.; Ropele, S.; Schmidt, R.; Chabriat, H.; et al. Incident Lacunes Preferentially Localize to the Edge of White Matter Hyperintensities: Insights into the Pathophysiology of Cerebral Small Vessel Disease. Brain 2013, 136, 2717–2726. [Google Scholar] [CrossRef]
- Keith, J.; Gao, F.Q.; Noor, R.; Kiss, A.; Balasubramaniam, G.; Au, K.; Rogaeva, E.; Masellis, M.; Black, S.E. Collagenosis of the Deep Medullary Veins: An Underrecognized Pathologic Correlate of White Matter Hyperintensities and Periventricular Infarction? J. Neuropathol. Exp. Neurol. 2017, 76, 299–312. [Google Scholar] [CrossRef] [PubMed]
- Tuttolomondo, A.; Di Sciacca, R.; Di Raimondo, D.; Renda, C.; Pinto, A.; Licata, G. Inflammation as a Therapeutic Target in Acute Ischemic Stroke Treatment. Curr. Top. Med. Chem. 2009, 9, 1240–1260. [Google Scholar] [CrossRef]
- Shoamanesh, A.; Preis, S.R.; Beiser, A.S.; Kase, C.S.; Wolf, P.A.; Vasan, R.S.; Benjamin, E.J.; Seshadri, S.; Romero, J.R. Circulating Biomarkers and Incident Ischemic Stroke in the Framingham Offspring Study. Neurology 2016, 87, 1206–1211. [Google Scholar] [CrossRef]
- Mengozzi, M.; Kirkham, F.A.; Girdwood, E.E.R.; Bunting, E.; Drazich, E.; Timeyin, J.; Ghezzi, P.; Rajkumar, C. C-Reactive Protein Predicts Further Ischemic Events in Patients With Transient Ischemic Attack or Lacunar Stroke. Front. Immunol. 2020, 11, 1–7. [Google Scholar] [CrossRef]
- Elkind, M.S.V.; Luna, J.M.; McClure, L.A.; Zhang, Y.; Coffey, C.S.; Roldan, A.; Del Brutto, O.H.; Pretell, E.J.; Pettigrew, L.C.; Meyer, B.C.; et al. C-Reactive Protein as a Prognostic Marker after Lacunar Stroke Levels of Inflammatory Markers in the Treatment of Stroke Study. Stroke 2014, 45, 707–716. [Google Scholar] [CrossRef]
- Boehme, A.K.; McClure, L.A.; Zhang, Y.; Luna, J.M.; Del Brutto, O.H.; Benavente, O.R.; Elkind, M.S.V. Inflammatory Markers and Outcomes after Lacunar Stroke: Levels of Inflammatory Markers in Treatment of Stroke Study. Stroke 2016, 47, 659–667. [Google Scholar] [CrossRef]
- Lindgren, A.; Lindoff, C.; Norrving, B.; Åstedt, B.; Johansson, B.B. Tissue Plasminogen Activator and Plasminogen Activator Inhibitor-1 in Stroke Patients. Stroke 1996, 27, 1066–1071. [Google Scholar] [CrossRef]
- Salobir, B.; Šabovič, M.; Peternel, P.; Stegnar, M. Vascular Bed Specific Alterations in Coagulation and Fibrinolytic Parameters in Young Women Following Myocardial Infarction, Lacunar Cerebral Infarction and Deep Vein Thrombosis. Pathophysiol. Haemost. Thromb. 2003, 33, 96–101. [Google Scholar] [CrossRef]
- Jood, K.; Ladenvall, P.; Tjärnlund-Wolf, A.; Ladenvall, C.; Andersson, M.; Nilsson, S.; Blomstrand, C.; Jern, C. Fibrinolytic Gene Polymorphism and Ischemic Stroke. Stroke 2005, 36, 2077–2081. [Google Scholar] [CrossRef] [PubMed]
- Yokokawa, H.; Goto, A.; Terui, K.; Funami, Y.; Watanabe, K.; Yasumura, S. Prevalence of Metabolic Syndrome and Serum Marker Levels in Patients with Four Subtypes of Cerebral Infarction in Japan. J. Clin. Neurosci. 2008, 15, 769–773. [Google Scholar] [CrossRef]
- Ilhan, D.; Özbabalik, D.; Gulcan, E.; Özdemir, Ö.; Gülbaçs, Z. Evaluation of Platelet Activation, Coagulation, and Fibrinolytic Activation in Patients with Symptomatic Lacunar Stroke. Neurologist 2010, 16, 188–191. [Google Scholar] [CrossRef]
- Kilpatrick, T.J.; Matkovic, Z.; Davis, S.M.; McGrath, C.M.; Dauer, R.J. Hematologic Abnormalities Occur in Both Cortical and Lacunar Infarction. Stroke 1993, 24, 1945–1950. [Google Scholar] [CrossRef]
- Beamer, N.B.; Coull, B.M.; Clark, W.M.; Hazel, J.S.; Silberger, J.R. Interleukin-6 and Interleukin-1 Receptor Antagonist in Acute Stroke. Ann. Neurol. 1995, 37, 800–805. [Google Scholar] [CrossRef]
- Bath, P.M.W.; Blann, A.; Smith, N.; Butterworth, R.J. Von Willebrand Factor, P-Selectin and Fibrinogen Levels in Patients with Acute Ischaemic and Haemorrhagic Stroke, and Their Relationship with Stroke Sub-Type and Functional Outcome. Platelets 1998, 9, 155–159. [Google Scholar] [CrossRef]
- Kataoka, S.; Hirose, G.; Hori, A.; Shirakawa, T.; Saigan, T. Activation of Thrombosis and Fibrinolysis Following Brain Infarction. J. Neurol. Sci. 2000, 181, 82–88. [Google Scholar] [CrossRef]
- Alvarez-Perez, F.J.; Castelo-Branco, M.; Alvarez-Sabin, J. Usefulness of Measurement of Fibrinogen, D-Dimer, D-Dimer/Fibrinogen Ratio, C Reactive Protein and Erythrocyte Sedimentation Rate to Assess the Pathophysiology and Mechanism of Ischaemic Stroke. J. Neurol. Neurosurg. Psychiatry 2011, 82, 986–992. [Google Scholar] [CrossRef]
- Beer, C.; Blacker, D.; Hankey, G.J.; Puddey, I.B. Association of Clinical and Aetiologic Subtype of Acute Ischaemic Stroke with Inflammation, Oxidative Stress and Vascular Function: A Cross-Sectional Observational Study. Med. Sci. Monit. 2011, 17, CR467. [Google Scholar] [CrossRef]
- Zhang, B.; Zhang, W.Z.; Li, X.; Pu, S.X.; Yin, J.R.; Yang, N.; Yi, Y.H.; Gao, Q.C.; Gao, C. Admission Markers Predict Lacunar and Non-Lacunar Stroke in Young Patients. Thromb. Res. 2011, 128, 14–17. [Google Scholar] [CrossRef]
- Datta, A.; Chen, C.P.; Sze, S.K. Discovery of Prognostic Biomarker Candidates of Lacunar Infarction by Quantitative Proteomics of Microvesicles Enriched Plasma. PLoS ONE 2014, 9, e94663. [Google Scholar] [CrossRef] [PubMed]
- Takano, K.; Yamaguchi, T.; Uchida, K. Markers of a Hypercoagulable State Following Acute Ischemic Stroke. Stroke 1992, 23, 194–198. [Google Scholar] [CrossRef] [PubMed]
- Ageno, W.; Finazzi, S.; Steidl, L.; Biotti, M.G.; Mera, V.; D’Eril, G.V.M.; Venco, A. Plasma Measurement of D-Dimer Levels for the Early Diagnosis of Ischemic Stroke Subtypes. Arch. Intern. Med. 2002, 162, 2589–2593. [Google Scholar] [CrossRef]
- Montaner, J.; Perea-Gainza, M.; Delgado, P.; Ribó, M.; Chacón, P.; Rosell, A.; Quintana, M.; Palacios, M.E.; Molina, C.A.; Alvarez-Sabín, J. Etiologic Diagnosis of Ischemic Stroke Subtypes with Plasma Biomarkers. Stroke 2008, 39, 2280–2287. [Google Scholar] [CrossRef]
- Brouns, R.; Van Den Bossche, J.; De Surgeloose, D.; Sheorajpanday, R.; De Deyn, P.P. Clinical and Biochemical Diagnosis of Small-Vessel Disease in Acute Ischemic Stroke. J. Neurol. Sci. 2009, 285, 185–190. [Google Scholar] [CrossRef]
- Isenegger, J.; Meier, N.; Lämmle, B.; Alberio, L.; Fischer, U.; Nedeltchev, K.; Gralla, J.; Kohler, H.P.; Mattle, H.P.; Arnold, M. D-Dimers Predict Stroke Subtype When Assessed Early. Cerebrovasc. Dis. 2009, 29, 82–86. [Google Scholar] [CrossRef]
- Eikelboom, J.W.; Hankey, G.J.; Anand, S.S.; Lofthouse, E.; Staples, N.; Baker, R.I. Association between High Homocyst(e)Ine and Ischemic Stroke Due to Large- and Small-Artery Disease but Not Other Etiologic Subtypes of Ischemic Stroke. Stroke 2000, 31, 1069–1075. [Google Scholar] [CrossRef]
- Hassan, A.; Gormley, K.; O’Sullivan, M.; Knight, J.; Sham, P.; Vallance, P.; Bamford, J.; Markus, H. Endothelial Nitric Oxide Gene Haplotypes and Risk of Cerebral Small-Vessel Disease. Stroke 2004, 35, 654–659. [Google Scholar] [CrossRef]
- Parnetti, L.; Caso, V.; Santucci, A.; Corea, F.; Lanari, A.; Floridi, A.; Conte, C.; Bottiglieri, T. Mild Hyperhomocysteinemia Is a Risk-Factor in All Etiological Subtypes of Stroke. Neurol. Sci. 2004, 25, 13–17. [Google Scholar] [CrossRef]
- Khan, U.; Hassan, A.; Vallance, P.; Markus, H.S. Asymmetric Dimethylarginine in Cerebral Small Vessel Disease. Stroke 2007, 38, 411–413. [Google Scholar] [CrossRef]
- Khan, U.; Crossley, C.; Kalra, L.; Rudd, A.; Wolfe, C.D.A.; Collinson, P.; Markus, H.S. Homocysteine and Its Relationship to Stroke Subtypes in a UK Black Population: The South London Ethnicity and Stroke Study. Stroke 2008, 39, 2943–2949. [Google Scholar] [CrossRef]
- Jeong, S.K.; Kim, D.H.; Cho, Y.I. Homocysteine and Pulsatility Index in Lacunar Infarction. Clin. Neurol. Neurosurg. 2011, 113, 459–463. [Google Scholar] [CrossRef]
- Pavlovic, A.M.; Pekmezovic, T.; Obrenovic, R.; Novakovic, I.; Tomic, G.; Mijajlovic, M.; Sternic, N. Increased Total Homocysteine Level Is Associated with Clinical Status and Severity of White Matter Changes in Symptomatic Patients with Subcortical Small Vessel Disease. Clin. Neurol. Neurosurg. 2011, 113, 711–715. [Google Scholar] [CrossRef]
- Lavallée, P.C.; Labreuche, J.; Faille, D.; Huisse, M.G.; Nicaise-Roland, P.; Dehoux, M.; Gongora-Rivera, F.; Jaramillo, A.; Brenner, D.; Deplanque, D.; et al. Circulating Markers of Endothelial Dysfunction and Platelet Activation in Patients with Severe Symptomatic Cerebral Small Vessel Disease on Behalf of the Lacunar-B.I.C.H.A.T. Investigators. Cerebrovasc. Dis. 2013, 36, 131–138. [Google Scholar] [CrossRef]
- Hanson, E.; Jood, K.; Karlsson, S.; Nilsson, S.; Blomstrand, C.; Jern, C. Plasma Levels of von Willebrand Factor in the Etiologic Subtypes of Ischemic Stroke. J. Thromb. Haemost. 2011, 9, 275–281. [Google Scholar] [CrossRef]
- Kozuka, K.; Kohriyama, T.; Ikeda, J.; Nakamura, S.; Nomura, E.; Kajikawa, H. Endothelial Markers and Adhesion Molecules in Acute Ischemic Stroke-Sequential Change and Differences in Stroke Subtype. Atherosclerosis 2002, 161, 161–168. [Google Scholar] [CrossRef]
- Tsai, N.W.; Chang, W.N.; Shaw, C.F.; Jan, C.R.; Huang, C.R.; Chen, S.D.; Chuang, Y.C.; Lee, L.H.; Lu, C.H. The Value of Leukocyte Adhesion Molecules in Patients after Ischemic Stroke. J. Neurol. 2009, 256, 1296–1302. [Google Scholar] [CrossRef]
- Turgut, B.; Turgut, N.; Çelik, Y.; Tekgündüz, E.; Pamuk, G.E.; Demir, M. Differences in Platelet-Leukocyte Aggregates among Subtypes of Acute Cerebral Ischemia. J. Neurol. Sci. 2011, 305, 126–130. [Google Scholar] [CrossRef]
- Castellanos, M.; Castillo, J.; García, M.M.; Leira, R.; Serena, J.; Chamorro, A.; Dávalos, A. Inflammation-Mediated Damage in Progressing Lacunar Infarctions a Potential Therapeutic Target. Stroke 2002, 33, 982–987. [Google Scholar] [CrossRef]
- Supanc, V.; Biloglav, Z.; Kes, V.; Demarin, V. Role of Cell Adhesion Molecules in Acute Ischemic Stroke. Ann. Saudi Med. 2011, 31, 365–370. [Google Scholar] [CrossRef]
- Rouhl, R.P.W.; Damoiseaux, J.G.M.C.; Lodder, J.; Theunissen, R.O.M.F.I.H.; Knottnerus, I.L.H.; Staals, J.; Henskens, L.H.G.; Kroon, A.A.; de Leeuw, P.W.; Tervaert, J.W.C.; et al. Vascular Inflammation in Cerebral Small Vessel Disease. Neurobiol. Aging 2012, 33, 1800–1806. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.M.; Bushnell, C.D.; Samsa, G.P.; Goldstein, L.B.; Colton, C.A. Chronic Systemic Immune Dysfunction in African-Americans with Small Vessel-Type Ischemic Stroke. Transl. Stroke Res. 2015, 6, 430–436. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Nakase, T.; Yamazaki, T.; Ogura, N.; Suzuki, A.; Nagata, K. The Impact of Inflammation on the Pathogenesis and Prognosis of Ischemic Stroke. J. Neurol. Sci. 2008, 271, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Mitaki, S.; Nagai, A.; Oguro, H.; Yamaguchi, S. C-Reactive Protein Levels Are Associated with Cerebral Small Vessel-Related Lesions. Acta Neurol. Scand. 2016, 133, 68–74. [Google Scholar] [CrossRef]
- Intiso, D.; Zarrelli, M.M.; Lagioia, G.; Di Rienzo, F.; De Ambrosio, C.C.; Simone, P.; Tonali, P.; Cioffi, R.P. Tumor Necrosis Factor Alpha Serum Levels and Inflammatory Response in Acute Ischemic Stroke Patients. Neurol. Sci. 2004, 24, 390–396. [Google Scholar] [CrossRef]
- Vila, N.; Castillo, J.; Dávalos, A.; Chamorro, Á. Proinflammatory Cytokines and Early Neurological Worsening in Ischemic Stroke. Stroke 2000, 31, 2325–2329. [Google Scholar] [CrossRef]
- Salobir, B.; Šabovič, M. Possible Vascular-Bed-Specific Role of Interleukin-6 in Young Women with a History of Myocardial Infarction, Lacunar Cerebral Infarction and Deep Vein Thrombosis. Cytokine 2004, 25, 265–272. [Google Scholar] [CrossRef]
- Guldiken, B.; Guldiken, S.; Turgut, B.; Turgut, N.; Demir, M.; Celik, Y.; Arikan, E.; Tugrul, A. The Roles of Oxidized Low-Density Lipoprotein and Interleukin-6 Levels in Acute Atherothrombotic and Lacunar Ischemic Stroke. Angiology 2008, 59, 224–229. [Google Scholar] [CrossRef]
- Horie, N.; Maag, A.L.; Hamilton, S.A.; Shichinohe, H.; Bliss, T.M.; Steinberg, G.K. Mouse Model of Focal Cerebral Ischemia Using Endothelin-1. J. Neurosci. Methods 2008, 173, 286–290. [Google Scholar] [CrossRef]
- Capone, C.; Faraco, G.; Park, L.; Cao, X.; Davisson, R.L.; Iadecola, C. The Cerebrovascular Dysfunction Induced by Slow Pressor Doses of Angiotensin II Precedes the Development of Hypertension. Am. J. Physiol.-Hear. Circ. Physiol. 2011, 300, H397–H407. [Google Scholar] [CrossRef]
- Cipolla, M.J.; Sweet, J.G.; Gokina, N.I.; White, S.L.; Nelson, M.T. Mechanisms of Enhanced Basal Tone of Brain Parenchymal Arterioles during Early Postischemic Reperfusion: Role of ET-1-Induced Peroxynitrite Generation. J. Cereb. Blood Flow Metab. 2013, 33, 1486–1492. [Google Scholar] [CrossRef]
- Cui, X.; Chopp, M.; Zacharek, A.; Ning, R.; Ding, X.; Roberts, C.; Chen, J. Endothelial Nitric Oxide Synthase Regulates White Matter Changes via the BDNF/TrKB Pathway after Stroke in Mice. PLoS ONE 2013, 8, e80358. [Google Scholar] [CrossRef]
- Rapp, J.H.; Pan, X.M.; Yu, B.; Swanson, R.A.; Higashida, R.T.; Simpson, P.; Saloner, D. Cerebral Ischemia and Infarction from Atheroemboli <100 Μm in Size. Stroke 2003, 34, 1976–1980. [Google Scholar] [CrossRef]
- Wang, C.B.; Hu, H.S.; Liu, Y.M. Animal Study in Combining Targeted-Microbubbles with Low-Frequency Ultrasound for the Treatment of Ischemic Stroke. J. Sichuan Univ. Medical Sci. Ed. 2012, 43, 864–867. [Google Scholar]
- Silasi, G.; She, J.; Boyd, J.D.; Xue, S.; Murphy, T.H. A Mouse Model of Small-Vessel Disease That Produces Brain-Wide-Identified Microocclusions and Regionally Selective Neuronal Injury. J. Cereb. Blood Flow Metab. 2015, 35, 734–738. [Google Scholar] [CrossRef]
- Walz, W.; Cayabyab, F.S. Neutrophil Infiltration and Matrix Metalloproteinase-9 in Lacunar Infarction. Neurochem. Res. 2017, 42, 2560–2565. [Google Scholar] [CrossRef]
- Wen, Z.; Jiang, Y.; Zhang, L.; Xu, X.; Zhao, N.; Xu, X.; Wang, F.; Gao, J.; Yang, G.Y.; Liu, X. The Effect of Anterior Communicating Artery Flow on Neurovascular Injury and Neurobehavioral Outcomes in Mice with Recurrent Stroke. Brain Res. 2019, 1724. [Google Scholar] [CrossRef]
- Choi, J.I.; Ha, S.K.; Lim, D.J.; Kim, S.D.; Kim, S.H. S100ß, Matrix Metalloproteinase-9, D-Dimer, and Heat Shock Protein 70 Are Serologic Biomarkers of Acute Cerebral Infarction in a Mouse Model of Transient MCA Occlusion. J. Korean Neurosurg. Soc. 2018, 61, 548–558. [Google Scholar] [CrossRef]
- Kwon, S.K.; Ahn, M.; Song, H.J.; Kang, S.K.; Jung, S.B.; Harsha, N.; Jee, S.; Moon, J.Y.; Suh, K.S.; Lee, S.D.; et al. Nafamostat Mesilate Attenuates Transient Focal Ischemia/Reperfusion-Induced Brain Injury via the Inhibition of Endoplasmic Reticulum Stress. Brain Res. 2015, 1627, 12–20. [Google Scholar] [CrossRef]
- Hainsworth, A.H.; Markus, H.S. Do in Vivo Experimental Models Reflect Human Cerebral Small Vessel Disease? A Systematic Review. J. Cereb. Blood Flow Metab. 2008, 28, 1877–1891. [Google Scholar] [CrossRef]
- Mencl, S.; Garz, C.; Niklass, S.; Braun, H.; Göb, E.; Homola, G.; Heinze, H.J.; Reymann, K.G.; Kleinschnitz, C.; Schreiber, S. Early Microvascular Dysfunction in Cerebral Small Vessel Disease Is Not Detectable on 3.0 Tesla Magnetic Resonance Imaging: A Longitudinal Study in Spontaneously Hypertensive Stroke-Prone Rats. Exp. Transl. Stroke Med. 2013, 5, 8. [Google Scholar] [CrossRef]
- Ayata, C. CADASIL: Experimental Insights from Animal Models. Stroke 2010, 41, S129–S134. [Google Scholar] [CrossRef]
- Joutel, A. Pathogenesis of CADASIL: Transgenic and Knock-out Mice to Probe Function and Dysfunction of the Mutated Gene, Notch3, in the Cerebrovasculature. BioEssays 2011, 33, 73–80. [Google Scholar] [CrossRef]
- Ruchoux, M.M.; Domenga, V.; Brulin, P.; Maciazek, J.; Limol, S.; Tournier-Lasserve, E.; Joutel, A. Transgenic Mice Expressing Mutant Notch3 Develop Vascular Alterations Characteristic of Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy. Am. J. Pathol. 2003, 162, 329–342. [Google Scholar] [CrossRef]
- Cipolla, L.; Consonni, A.; Guidetti, G.; Canobbio, I.; Okigaki, M.; Falasca, M.; Ciraolo, E.; Hirsch, E.; Balduini, C.; Torti, M. The Proline-Rich Tyrosine Kinase Pyk2 Regulates Platelet Integrin AIIbβ3 Outside-in Signaling. J. Thromb. Haemost. 2013, 11, 345–356. [Google Scholar] [CrossRef]
- Fisher, C.M. Lacunes: Small, Deep Cerebral Infarcts. Neurology 1965, 15, 774–784. [Google Scholar] [CrossRef]
- Fisher, C.M. Pure Sensory Stroke Involving Face, Arm, and Leg. Neurology 1965, 15, 78–80. [Google Scholar] [CrossRef]
- Mohr, J.P.; Kase, C.S.; Meckler, R.J.; Fisher, C.M. Sensorimotor Stroke Due to Thalamocapsular Ischemia. Arch. Neurol. 1977, 34, 739–741. [Google Scholar] [CrossRef]
- Chamorro, A.; Sacco, R.L.; Mohr, J.P.; Foulkes, M.A.; Kase, C.S.; Tatemichi, T.K.; Wolf, P.A.; Price, T.R.; Hier, D.B. Clinical-Computed Tomographic Correlations of Lacunar Infarction in the Stroke Data Bank. Stroke 1991, 22, 175–181. [Google Scholar] [CrossRef]
- Arboix, A.; García-Plata, C.; García-Eroles, L.; Massons, J.; Comes, E.; Oliveres, M.; Targa, C. Clinical Study of 99 Patients with Pure Sensory Stroke. J. Neurol. 2005, 252, 156–162. [Google Scholar] [CrossRef]
- Arboix, A.; Bell, Y.; García-Eroles, L.; Massons, J.; Comes, E.; Balcells, M.; Targa, C. Clinical Study of 35 Patients with Dysarthria-Clumsy Hand Syndrome. J. Neurol. Neurosurg. Psychiatry 2004, 75, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.Y.; Lui, F.S. Ataxic-Hemiparesis, Localization and Clinical Features. Stroke 1984, 15, 363–366. [Google Scholar] [CrossRef] [PubMed]
- Arboix, A. Hemiparesia Atáxica: Estudio de 23 Pacientes. Med. Clin. (Barc) 2004, 122, 342–344. [Google Scholar] [CrossRef]
- Fisher, C.M. Ataxic Hemiparesis: A Pathologic Study. Arch. Neurol. 1978, 35, 126–128. [Google Scholar] [CrossRef] [PubMed]
- Arboix, A.; Martí-Vilaita, J.L. Lacunar Stroke. Expert Rev. Neurother. 2009, 9, 179–196. [Google Scholar] [CrossRef] [PubMed]
- Arboix, A.; López-Grau, M.; Casasnovas, C.; García-Eroles, L.; Massons, J.; Balcells, M. Clinical Study of 39 Patients with Atypical Lacunar Syndrome. J. Neurol. Neurosurg. Psychiatry 2006, 77, 381–384. [Google Scholar] [CrossRef]
- Potter, G.; Doubal, F.; Jackson, C.; Sudlow, C.; Dennis, M.; Wardlaw, J. Associations of Clinical Stroke Misclassification (‘Clinical-Imaging Dissociation’) in Acute Ischemic Stroke. Cerebrovasc. Dis. 2010, 29, 395–402. [Google Scholar] [CrossRef]
- Ay, H.; Oliveira-Filho, J.; Buonanno, F.S.; Ezzeddine, M.; Schaefer, P.W.; Rordorf, G.; Schwamm, L.H.; Gonzalez, R.G.; Koroshetz, W.J. Diffusion-Weighted Imaging Identifies a Subset of Lacunar Infarction Associated with Embolic Source. Stroke 1999, 30, 2644–2650. [Google Scholar] [CrossRef]
- Hofmeister, C.; Hartmann, A.; Marx, P.; Mast, H.; Stapf, C. Predictive Value of Clinical Syndromes for Lacunar Infarcts on Magnetic Resonance Brain Imaging. Acta Neurol. Scand. 2000, 101, 13–18. [Google Scholar] [CrossRef]
- Lindgren, A.; Staaf, G.; Geijer, B.; Brockstedt, S.; Ståhlberg, F.; Holtås, S.; Norrving, B. Clinical Lacunar Syndromes as Predictors of Lacunar Infarcts: A Comparison of Acute Clinical Lacunar Syndromes and Findings on Diffusion- Weighted MRI. Acta Neurol. Scand. 2000, 101, 128–134. [Google Scholar] [CrossRef]
- Seifert, T.; Enzinger, C.; Storch, M.K.; Pichler, G.; Niederkorn, K.; Fazekas, F. Acute Small Subcortical Infarctions on Diffusion Weighted MRI: Clinical Presentation and Aetiology. J. Neurol. Neurosurg. Psychiatry 2005, 76, 1520–1524. [Google Scholar] [CrossRef]
- Wessels, T.; Röttger, C.; Jauss, M.; Kaps, M.; Traupe, H.; Stol, E. Identification of Embolic Stroke Patterns by Diffusion-Weighted MRI in Clinically Defined Lacunar Stroke Syndromes. Stroke 2005, 36, 757–761. [Google Scholar] [CrossRef]
- Arboix, A.; Massons, J.; García-Eroles, L.; Targa, C.; Comes, E.; Parra, O. Clinical Predictors of Lacunar Syndrome Not Due to Lacunar Infarction. BMC Neurol. 2010, 10, 31. [Google Scholar] [CrossRef]
- Altmann, M.; Thommessen, B.; Rønning, O.M.; Reichenbach, A.S.; Fure, B. Diagnostic Accuracy and Risk Factors of the Different Lacunar Syndromes. J. Stroke Cerebrovasc. Dis. 2014, 23, 2085–2090. [Google Scholar] [CrossRef]
- Giacomozzi, S.; Caso, V.; Agnelli, G.; Acciarresi, M.; Alberti, A.; Venti, M.; Mosconi, M.G.; Paciaroni, M. Lacunar Stroke Syndromes as Predictors of Lacunar and Non-Lacunar Infarcts on Neuroimaging: A Hospital-Based Study. Intern. Emerg. Med. 2020, 15, 429–436. [Google Scholar] [CrossRef]
- Arba, F.; Mair, G.; Phillips, S.; Sandercock, P.; Wardlaw, J.M. Improving Clinical Detection of Acute Lacunar Stroke: Analysis from the IST-3. Stroke 2020, 51, 1411–1418. [Google Scholar] [CrossRef]
- Nelson, R.F.; Pullicino, P.; Kendall, B.E.; Marshall, J. Computed Tomography in Patients Presenting with Lacunar Syndromes. Stroke 1980, 11, 256–261. [Google Scholar] [CrossRef]
- Rothrock, J.F.; Lyden, P.D.; Hesselink, J.R.; Brown, J.J.; Healy, M.E. Brain Magnetic Resonance Imaging in the Evaluation of Lacunar Stroke. Stroke 1987, 18, 781–786. [Google Scholar] [CrossRef]
- Noguchi, K.; Nagayoshi, T.; Watanabe, N.; Kanazawa, T.; Toyoshima, S.; Morijiri, M.; Shojaku, H.; Shimizu, M.; Seto, H. Diffusion-Weighted Echo-Planar MRI of Lacunar Infarcts. Neuroradiology 1998, 40, 448–451. [Google Scholar] [CrossRef]
- Schonewille, W.J.; Tuhrim, S.; Singer, M.B.; Atlas, S.W. Diffusion-Weighted MRI in Acute Lacunar Syndromes: A Clinical- Radiological Correlation Study. Stroke 1999, 30, 2066–2069. [Google Scholar] [CrossRef]
- Tan, M.Y.Q.; Singhal, S.; Ma, H.; Chandra, R.V.; Cheong, J.; Clissold, B.B.; Ly, J.; Srikanth, V.; Phan, T.G. Examining Subcortical Infarcts in the Era of Acute Multimodality CT Imaging. Front. Neurol. 2016, 7, 220. [Google Scholar] [CrossRef]
- Arsava, E.M.; Ballabio, E.; Benner, T.; Cole, J.W.; Delgado-Martinez, M.P.; Dichgans, M.; Fazekas, F.; Furie, K.L.; Illoh, K.; Jood, K.; et al. The Causative Classification of Stroke System: An International Reliability and Optimization Study. Neurology 2010, 75, 1277–1284. [Google Scholar] [CrossRef]
- Das, T.; Settecase, F.; Boulos, M.; Huynh, T.; D’Esterre, C.D.; Symons, S.P.; Zhang, L.; Aviv, R.I. Multimodal CT Provides Improved Performance for Lacunar Infarct Detection. Am. J. Neuroradiol. 2015, 36, 1069–1075. [Google Scholar] [CrossRef]
- Benson, J.C.; Payabvash, S.; Mortazavi, S.; Zhang, L.; Salazar, P.; Hoffman, B.; Oswood, M.; McKinney, A.M. CT Perfusion in Acute Lacunar Stroke: Detection Capabilities Based on Infarct Location. Am. J. Neuroradiol. 2016, 37, 2239–2244. [Google Scholar] [CrossRef]
- Cao, W.; Yassi, N.; Sharma, G.; Yan, B.; Desmond, P.M.; Davis, S.M.; Campbell, B.C.V. Diagnosing Acute Lacunar Infarction Using CT Perfusion. J. Clin. Neurosci. 2016, 29, 70–72. [Google Scholar] [CrossRef]
- Garcia-Esperon, C.; Visser, M.; Churilov, L.; Miteff, F.; Bivard, A.; Lillicrap, T.; Levi, C.R.; Spratt, N.J.; Parsons, M.W. Role of Computed Tomography Perfusion in Identification of Acute Lacunar Stroke Syndromes. Stroke 2020, 339–343. [Google Scholar] [CrossRef]
- Chapman, K.M.; Woolfenden, A.R.; Graeb, D.; Johnston, D.C.C.; Beckman, J.; Schulzer, M.; Teal, P.A. Intravenous Tissue Plasminogen Activator for Acute Ischemic Stroke. Stroke 2000, 31, 2920–2924. [Google Scholar] [CrossRef][Green Version]
- Pantoni, L.; Fierini, F.; Poggesi, A. Thrombolysis in Acute Stroke Patients with Cerebral Small Vessel Disease. Cerebrovasc. Dis. 2014, 37, 5–13. [Google Scholar] [CrossRef]
- Matusevicius, M.; Paciaroni, M.; Caso, V.; Bottai, M.; Khurana, D.; de Bastos, M.; Martins, S.C.; Krespi, Y.; Cooray, C.; Toni, D.; et al. Outcome after Intravenous Thrombolysis in Patients with Acute Lacunar Stroke: An Observational Study Based on SITS International Registry and a Meta-Analysis. Int. J. Stroke 2019, 14, 878–886. [Google Scholar] [CrossRef]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. 2018 Guidelines for the Early Management of Patients with Acute Ischemic Stroke: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2018, 49, e46–e99. [Google Scholar] [CrossRef]
- Thomalla, G.; Boutitie, F.; Ma, H.; Koga, M.; Ringleb, P.; Schwamm, L.H.; Wu, O.; Bendszus, M.; Bladin, C.F.; Campbell, B.C.V.; et al. Intravenous Alteplase for Stroke with Unknown Time of Onset Guided by Advanced Imaging: Systematic Review and Meta-Analysis of Individual Patient Data. Lancet 2020, 396, 1574–1584. [Google Scholar] [CrossRef]
- Barow, E.; Boutitie, F.; Cheng, B.; Cho, T.H.; Ebinger, M.; Endres, M.; Fiebach, J.B.; Fiehler, J.; Ford, I.; Galinovic, I.; et al. Functional Outcome of Intravenous Thrombolysis in Patients with Lacunar Infarcts in the Wake-up Trial. JAMA Neurol. 2019, 76, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Campbell, B.C.V.; Ma, H.; Ringleb, P.A.; Parsons, M.W.; Churilov, L.; Bendszus, M.; Levi, C.R.; Hsu, C.; Kleinig, T.J.; Fatar, M.; et al. Extending Thrombolysis to 4·5–9 h and Wake-up Stroke Using Perfusion Imaging: A Systematic Review and Meta-Analysis of Individual Patient Data. Lancet 2019, 394, 139–147. [Google Scholar] [CrossRef]
- Vynckier, J.; Maamari, B.; Grunder, L.; Goeldlin, M.B.; Meinel, T.R.; Kaesmacher, J.; Hakim, A.; Arnold, M.; Gralla, J.; Seiffge, D.J.; et al. Early Neurologic Deterioration in Lacunar Stroke. Neurology 2021, 97, e1437–e1446. [Google Scholar] [CrossRef] [PubMed]
- Kwok, C.S.; Shoamanesh, A.; Copley, H.C.; Myint, P.K.; Loke, Y.K.; Benavente, O.R. Efficacy of Antiplatelet Therapy in Secondary Prevention Following Lacunar Stroke: Pooled Analysis of Randomized Trials. Stroke 2015, 46, 1014–1023. [Google Scholar] [CrossRef] [PubMed]
- Fergus, I.V. Effects of Clopidogrel Added to Aspirin in Patients with Recent Lacunar Stroke. N. Engl. J. Med. 2012, 367, 817–825. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, Y.; Zhao, X.; Liu, L.; Wang, D.; Wang, C.; Wang, C.; Li, H.; Meng, X.; Cui, L.; et al. Clopidogrel with Aspirin in Acute Minor Stroke or Transient Ischemic Attack. N. Engl. J. Med. 2013, 369, 11–19. [Google Scholar] [CrossRef]
- Johnston, S.C.; Easton, J.D.; Farrant, M.; Barsan, W.; Conwit, R.A.; Elm, J.J.; Kim, A.S.; Lindblad, A.S.; Palesch, Y.Y. Clopidogrel and Aspirin in Acute Ischemic Stroke and High-Risk TIA. N. Engl. J. Med. 2018, 379, 215–225. [Google Scholar] [CrossRef]
- Johnston, S.C.; Amarenco, P.; Denison, H.; Evans, S.R.; Himmelmann, A.; James, S.; Knutsson, M.; Ladenvall, P.; Molina, C.A.; Wang, Y. Ticagrelor and Aspirin or Aspirin Alone in Acute Ischemic Stroke or TIA. N. Engl. J. Med. 2020, 383, 207–217. [Google Scholar] [CrossRef]
- Jing, J.; Meng, X.; Zhao, X.; Liu, L.; Wang, A.; Pan, Y.; Li, H.; Wang, D.; Johnston, S.C.; Wang, Y.; et al. Dual Antiplatelet Therapy in Transient Ischemic Attack and Minor Stroke with Different Infarction Patterns Subgroup Analysis of the CHANCE Randomized Clinical Trial. JAMA Neurol. 2018, 75, 711–719. [Google Scholar] [CrossRef]
- Berberich, A.; Schneider, C.; Reiff, T.; Gumbinger, C.; Ringleb, P.A. Dual Antiplatelet Therapy Improves Functional Outcome in Patients With Progressive Lacunar Strokes. Stroke 2019, 50, 1007–1009. [Google Scholar] [CrossRef]
- Takeuchi, M.; Miyashita, K.; Nakagawara, J.; Toyoda, K.; Todo, K.; Metoki, N.; Suzuki, R.; Manabe, Y.; Akaiwa, Y.; Yamamoto, Y.; et al. Analysis of Factors Associated with Progression and Long-Term Outcomes of Penetrating Artery Territory Infarction: A Retrospective Study. J. Stroke Cerebrovasc. Dis. 2016, 25, 1952–1959. [Google Scholar] [CrossRef]
- Dawson, J.; Merwick, Á.; Webb, A.; Dennis, M.; Ferrari, J.; Fonseca, A.C. European Stroke Organisation Expedited Recommendation for the Use of Short-Term Dual Antiplatelet Therapy Early after Minor Stroke and High-Risk TIA. Eur. Stroke J. 2021, 6, CLXXXVII–CXCI. [Google Scholar] [CrossRef]
- Wiśniewski, A.; Filipska, K. The Phenomenon of Clopidogrel High On-Treatment Platelet Reactivity in Ischemic Stroke Subjects: A Comprehensive Review. Int. J. Mol. Sci. 2020, 21, 6408. [Google Scholar] [CrossRef]
- Wiśniewski, A.; Sikora, J.; Karczmarska-Wódzka, A.; Sobczak, P. A Combination of Aspirin and Clopidogrel Predict More Favorable Dynamics of Platelet Reactivity versus Clopidogrel Alone in the Acute Phase of Minor Stroke. Healthcare 2021, 9, 628. [Google Scholar] [CrossRef]
- McHutchison, C.; Blair, G.W.; Appleton, J.P.; Chappell, F.M.; Doubal, F.; Bath, P.M.; Wardlaw, J.M. Cilostazol for Secondary Prevention of Stroke and Cognitive Decline: Systematic Review and Meta-Analysis. Stroke 2020, 51, 2374–2385. [Google Scholar] [CrossRef]
- Amarenco, P.; Benavente, O.; Goldstein, L.B.; Callahan, A.; Sillesen, H.; Hennerici, M.G.; Gilbert, S.; Rudolph, A.E.; Simunovic, L.; Zivin, J.A.; et al. Results of the Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) Trial by Stroke Subtypes. Stroke 2009, 40, 1405–1409. [Google Scholar] [CrossRef]
- Ungvari, Z.; Toth, P.; Tarantini, S.; Prodan, C.I.; Sorond, F.; Merkely, B.; Csiszar, A. Hypertension-Induced Cognitive Impairment: From Pathophysiology to Public Health. Nat. Rev. Nephrol. 2021, 17, 639–654. [Google Scholar] [CrossRef]
- Spence, J.D. Blood Pressure Gradients in the Brain: Their Importance to Understanding Pathogenesis of Cerebral Small Vessel Disease. Brain Sci. 2019, 9, 21. [Google Scholar] [CrossRef]
- Liu, L.; Wang, Z.; Gong, L.; Zhang, Y.; Thijs, L.; Staessen, J.A.; Wang, J. Blood Pressure Reduction for the Secondary Prevention of Stroke: A Chinese Trial and a Systematic Review of the Literature. Hypertens. Res. 2009, 32, 1032–1040. [Google Scholar] [CrossRef]
- Zhou, Z.; Xia, C.; Carcel, C.; Yoshimura, S.; Wang, X.; Delcourt, C.; Malavera, A.; Chen, X.; Mair, G.; Woodward, M.; et al. Intensive versus Guideline-Recommended Blood Pressure Reduction in Acute Lacunar Stroke with Intravenous Thrombolysis Therapy: The ENCHANTED Trial. Eur. J. Neurol. 2021, 28, 783–793. [Google Scholar] [CrossRef]
- Deijle, I.A.; Van Schaik, S.M.; Van Wegen, E.E.H.; Weinstein, H.C.; Kwakkel, G.; Van Den Berg-Vos, R.M. Lifestyle Interventions to Prevent Cardiovascular Events after Stroke and Transient Ischemic Attack. Stroke 2017, 48, 174–179. [Google Scholar] [CrossRef]
- Autenrieth, C.S.; Evenson, K.R.; Yatsuya, H.; Shahar, E.; Baggett, C.; Rosamond, W.D. Association between Physical Activity and Risk of Stroke Subtypes: The Atherosclerosis Risk in Communities Study. Neuroepidemiology 2013, 40, 109–116. [Google Scholar] [CrossRef]
- Krawcyk, R.S.; Vinther, A.; Petersen, N.C.; Faber, J.; Hansen, R.H.; Rostrup, E.; Kruuse, C. Home-Based Aerobic Exercise in Patients with Lacunar Stroke: Design of the HITPALS Randomized Controlled Trial. Contemp. Clin. Trials Commun. 2019, 14, 100332. [Google Scholar] [CrossRef]
- Han, S.W.; Lee, S.S.; Kim, S.H.; Lee, J.H.; Kim, G.S.; Kim, O.J.; Koh, I.S.; Lee, J.Y.; Suk, S.H.; Lee, S.I.; et al. Effect of Cilostazol in Acute Lacunar Infarction Based on Pulsatility Index of Transcranial Doppler (ECLIPse): A Multicenter, Randomized, Double-Blind, Placebo-Controlled Trial. Eur. Neurol. 2013, 69, 33–40. [Google Scholar] [CrossRef]
- Stack, J.; Ryan, J.; McCarthy, G. Colchicine: New Insights to an Old Drug. Am. J. Ther. 2015, 22, e151–e157. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Mechanism | Description | Evidence | Unsolved Issues | Possible Intervention Target |
|---|---|---|---|---|
| Hypertensive arteriosclerosis | Progressive hypertensive-related arteriosclerotic injury. Superposed microthrombosis may lead to complete arteriolar occlusion. | Typical histopathological findings in perforating arteries. Indirect evidence from high field MRI techniques [19,20]. | Non hypertensive patients may also present with lacunar stroke [21]. In vivo radiological confirmation of small artery wall alterations are not available. | Hypertension is the most modifiable risk factor for stroke secondary prevention [22]. In patients with lacunar strokes, intensive vs. standard blood pressure reduction did not reduce the risk of all stroke recurrency, although it reduced the risk of intracranial hemorrhage (SPS3) [23]. |
| Atherosclerosis (branch atheromatous disease) | Atherosclerotic plaques in the main cerebral vessel may occlude the orifice of perforating arterioles [24,25]. | Anatomopathological studies [18]. Small plaques are also visible using high field MRI techniques for vessel wall assessment [24]. | Atherosclerosis in large vessel arteries may represent an epiphenomenon. | Lipid lowering is effective for reducing stroke recurrence in non-cardioembolic strokes (SPARCL trial) [26]. Other new drugs aimed to stabilize the inflammatory process in atherosclerosis, which might represent a promising therapeutic target. |
| Microembolisms | Small emboli, either from proximal atherosclerotic plaques or cardiac source, may produce single or multiple small subcortical infarcts. | Perforating arteries in lacunar strokes may be patent in pathology studies [8] and advanced 7T MRI techniques [27]. Increased blood flow on CT perfusion suggests recanalization of an embolic occlusion of a perforating artery [28]. Subcortical infarcts in animal models produced by microembolism [6]. | There is an association between atrial fibrillation, load of subcortical infarcts, and WMH [29], but direct evidence of embolism is lacking. Multiple RSSIs do not exclude mechanisms related to SVD (about 20% of RSSI present multiple infarcts, especially in patients with severe SVD [30]). | Treatments aimed to stabilize active plaques or anticoagulant treatment, in case of mayor embolic source. Prothrombotic state (i.e., acute cancer), marantic, or infectious endocarditis should be ruled out in patients with multiple subcortical strokes. |
| Chronic global cerebral hypoperfusion | Chronic hypoperfusion of distal vascular territories may lead to progressive ischemia in the white matter. Small infarctions may occur in the edges of WMH and contribute to SVD progression. | In animal models, small subcortical infarcts may be produced by bilateral carotid occlusions [6]. | The causal relationship between hypoperfusion and SVD progression in longitudinal studies is controversial [31], as hypoperfusion might also be also secondary to reduced metabolism in WMH. | Vasodilatory drugs to increase brain perfusion: mononitrate isosorbide, nitric oxide. (LACI-2) [32]. |
| Inflammation, endothelial dysfunction, and BBB disruption | Endothelial dysfunction may trigger the pro-inflammatory mechanisms promoting pro-thrombotic agents, microglial activation, altered neurovascular homeostasis, and impaired coupling between metabolic demand and nutrient supply. | Markers of BBB leakage in pathology studies [33,34]. Association between the number of lacunes and inflammatory blood markers [35]. BBB permeability on dynamic contrast enhanced MRI is increased in lacunar strokes, compared to cortical strokes [36]. | Some studies on post-mortem brain samples did not confirm the association of markers of endothelial dysfunction or BBB leakage and SVD [37,38]. A causal relationship with focal BBB leakage prior lacunar strokes is to be determined. BBB permeability variations are mild and difficult to measure in SVD. Blood markers of endothelial dysfunction and inflammation are are not specific of lacunar stroke subtype [39]. | Anti-inflammatory drugs: colchicine in non-cardioembolic strokes (CONVINCE) [40], uric acid (URICO-ICTUS) [41], and canakinumab [42]. |
| Focal hypoperfusion and compensatory blood flow in acute perforating artery occlusion | Abrupt reduction in blood flow after perforating artery occlusion, regardless the causing mechanisms (either intrinsic SVD or atheroembolic). The extent and the time to establish infarction may depend on factors such as compensatory blood flow through capillary network and cerebrovascular reserve. | Perfusion studies show persistence of residual blood flow, in the territory of perforating arteries corresponding to RSSI [43,44]. Sequential imaging from row perfusion sequences may show retrograde flow, suggesting collateral circulation involvement in RSSI [28,45,46] Microscopic studies showed a dense capillary network, linking contiguous perforating arteries and few arteriolar anastomoses [47]. | Lack of direct evidence of perforating artery occlusion and recruiting collateral circulation in RSSI | Thrombolysis in lacunar stroke would not be effective without compensatory mechanisms maintaining the tissue viable until recanalization. Perfusion imaging-based thrombolysis, outside of the conventional time window, may also be effective in patients with RSSI. Vasodilatory agents may improve collateral recruitment. Neuroprotective agents may reach the ischemic area through retrograde in the territory supplied by an occluded perforating artery. |
| Mechanism | Molecule | Findings | References |
|---|---|---|---|
| Coagulation and fibrinolysis | Tissue plasminogen activator (TPA) |
| Lindgren, 1996 [79] Salobir, 2003 [80] Jood, 2005 [81] |
| Plasminogen activator inhibitor (PAI) |
| Lindgren, 1996 [79] Salobir, 2002 [80] Jood, 2005 [81] Yokokawa, 2008 [82] Ilhan, 2010 [83] | |
| Fibrinogen |
| Kilpatrick, 1993 [84] Beamer, 1995 [85] Bath, 1998 [86] Kataoka, 2000 [87] Salobir, 2003 [80] Jood, 2008 [81] Álvarez-Pérez, 2011 [88] Beer, 2011 [89] Zhang, 2011 [90] Datta, 2014 [91] | |
| D-dimer |
| Takano, 1992 [92] Kataoka, 2000 [87] Ajeno, 2002 [93] Salobir, 2003 [80] Ilhan, 2010 [83] Montaner, 2008 [94] Brouns, 2009 [95] Isenegger, 2010 [96] Álvarez-Pérez, 2011 [88] | |
| Endothelial dysfunction | Homocysteine |
| Eikelboom, 2000 [97] Hassan, 2004 [98] Parnetti, 2004 [99] Khan, 2007 [100] Khan, 2008 [101] Yokokawa, 2008 [82] Beer, 2011 [89] Jeong, 2011 [102] Pavlovic, 2011 [103] Lavallée, 2013 [104] |
| Von Willebrand factor (vWF) |
| Beer, 2011 [89] Hanson, 2011 [105] Lavallée, 2013 [104] | |
| E-selectin |
| Kozuka, 2002 [106] Beer, 2011 [89] | |
| P-selectin |
| Bath, 1998 [86] Kozuka, 2002 [106] Tsai, 2009 [107] Ilhan, 2010 [83] Turgut, 2011 [108] Lavallée, 2013 [104] | |
| Intercellular adhesion molecule 1 (ICAM-1) |
| Castellanos, 2002 [109] Hassan, 2003 [98] Supanc, 2011 [110] Rouhl, 2012 [111] | |
| Vascular cellular adhesion molecule 1 (VCAM-1) |
| Supanc, 2011 [110] Rouhl, 2012 [111] Brwon, 2015 [112] | |
| Inflammation | C-reactive protein (CRP) |
| Ladenvall, 2006 [81] Yokokawa, 2008 [82] Montaner, 2008 [94] Nakase, 2008 [113] Álvarez-Pérez, 2011 [88] Beer, 2011 [89] Turgut, 2011 [108] Mitaki, 2016 [114] |
| Tumor necrosis factor α (TNFα) |
| Castellanos, 2002 [109] Domac, 2007 [115] Boehme, 2016 [78] | |
| Interleukin 6 (IL-6) |
| Beamer, 1995 [85] Vila, 2000 [116] Castellanos, 2002 [109] Salobir, 2004 [117] Domac, 2007 [115] Guldiken, 2008 [118] Boehme, 2016 [78] |
| Mechanism | Techniques | Description | Advantages | Disadvantages | References |
|---|---|---|---|---|---|
| Vasoconstriction of perforating arteries | Endothelin-1, nitric oxide synthase inhibitor, and L-NAME | Strong vasoconstrictive action that affects several microvessels | Small subcortical infarcts | Multiple vessels affected at once | Horie, 2008 [119] Capone, 2011 [120] Cipolla, 2013 [135] Cui, 2013 [122] |
| Embolism | Microspheres, microthrombi injection, atheroemboli, black beads, preformed clots, and silicone rubber cylinders | Injection of different materials in the carotid to produce micro-occlusions by lodging in brain vessels | Multiple subcortical infarcts | Mostly cortical infarcts, mechanism not related to SVD | Rapp, 2003 [123] Wang, 2012 [124] Silasi, 2015 [125] |
| Spontaneous lesions | High salt, spontaneous in SHRSP, surgical narrowing of the aorta, and genetic mutations in the renin-angiotensin system | Mice breeds with an increased risk of stroke, genetically or surgically induced | Mechanism consistent with hypertensive SVD | Difficult to track lesion location and timing | Hainsworth, 2008 [130] Bailey, 2009 [6] Mencl, 2013 [131] |
| Perforating artery occlusion | Surgery (pial vessel disruption model), sodium laurate thrombosis, and photothrombosis | Endothelium damage and thrombosis, using toxic substances or surgical models | Accurate localization of the lesions | Strokes larger than lacunar infarcts | Walz, 2017 [126] Wen, 2019 [127] |
| Transient large vessel occlusion | Bilateral common carotid artery occlusion | Repeated transient large vessel occlusion, followed by reperfusion | Mechanism reflects the hypoperfusion in SVD | Lesions are not related to small vessel pathology | Choi, 2018 [128] Kwon, 2015 [129] |
| Genetic models | CADASIL mouse models, COL4A1/2 mouse models | Studies in mice with rare genetic disorders which make them prone to SVD | Mechanism related to genetic SVD etiology | Not enough brain affection | Ayata, 2010 [132] Joutel, 2011 [133] Ruchoux, 2003 [134] |
| Reference | Cohort | Lacunar Syndrome, n (%) | Cortical Syndrome, n (%) | RSSI/NonLacunar Syndrome, n (%) | Non-RSSI/Lacunar Syndrome, n (%) | Lacunar Syndrome/DWI Negative, n (%) | Cortical Syndrome/DWI Negative, (%) | Lacunar Syndrome Positive Predictive Value |
|---|---|---|---|---|---|---|---|---|
| Potter, 2010 [147] | 313 | 79 (25) | 136 (43) | 21/93 (23) | 7/44 (16) | 35/79 (44) | 43/136 (32) | 46% ° 84% °° |
| Ay, 1999 [148] | 62 | 62 (100) | - | - | 10/62 (16) | 9/62 (14) | - | 68% |
| Stapf, 2000 [149] | 54 | 54 (100) | - | - | 3/54 (6) | 0/54 (0) | - | 94% |
| Lindgren, 2000 [150] | 23 | 23 (100) | - | - | 2/23 (8) | 1/23 (4) | - | 86% |
| Seifert, 2005 [151] | 93 | 41 (44) | POCS (39) PACS (15) TACS (1) | 15/93 (16) | - | - | - | 44% ^ 83% ^^ |
| Wessels, 2005 [152] | 73 | 73 (100) | - | - | 30/73 (38) | 0/73 (0) | - | 58% |
| Arboix, 2010 * [153] | 879 | 879 (100) | - | - | 146/879 (17) | - | - | 83% |
| Altmann, 2014 [154] | 119 | 119 (100) | - | - | 16/119 (13) | 17/86 (20) | - | 60% · 65% ·· |
| Giacomozzi, 2019 [155] | 1796 | 478 (26) | 1313 (74) | 346/1313 (26) | 104/478 (21) | - | - | 78% |
| Arba, 2020 ** [156] | 568 | 330 (58) | 238 (42) | 59/238 (25) | 102/330 (31) | - | - | 25% *** 75% **** |
| Reference | Population | Perfusion Maps | Main Findings |
|---|---|---|---|
| Rudilosso, 2015 [43] | A total of 33 patients with lacunar syndrome (16 lacunar strokes, 13 non-lacunar strokes, and 4 no ischemic lesions). Lacunar stroke defined as infarct volume <1.767 cm3 (the volume of a sphere with a diameter 1.5 cm) on DWI. | Postprocessing software: CT Neuro Perfusion Syngo.via (Siemens Healthcare GmbH) for visual assessment. MIStar (Apollo Medical Imaging Technology, Melbourne, Australia) for core/penumbra threshold analysis. Perfusion maps: CBF, CBV, MTT, Tmax, TTP, TTD, and MIP. | SE and PPV for lacunar stroke higher than non-contrast CT (63% vs. 19%). CTP was more sensitive for supratentorial lesions, compared with infratentorial lesions (65% versus 16%). SP was low (20%) and influenced by low lacunar stroke prevalence. TTD was the most informative map for the identification of ischemic lesions. |
| Das, 2015 [163] | A total of 88 patients with lacunar syndrome (after excluding stroke mimics). RSSI: 59/88 (67%). | Postprocessing software: GE Healthcare Perfusion maps: CBV, CBF, and MTT. | SE56%, SP 83%. CTP increased the diagnostic performance 5-fold over non-contrast CT. MTT were the most informative maps to identify RSSI. |
| Benson, 2016 [164] | A total of 113 patients: 37 with ischemic lesions on DWI < 20 mm in maximum diameter (either cortical or subcortical) and 76 without ischemic lesions. Ischemic lesions > 20 mm, and patients treated with iv tPA were excluded from the analysis. | Postprocessing software: Vitrea workstation (Vital Imaged, Minnetonka, Minnesota) Perfusion maps: TTP, MTT, CBV, and CBF. | TTP were the maps with highest SE (49%), and lowest for non-contrast CT (3%). SP was high regardless the map evaluated (all >97%). The perfusion lesions on CTP appeared larger than the lesion on DWI. |
| Tan, 2016 [161] | A total of 182 patients with ischemic strokes (31 single subcortical, 9 multiple subcortical, 34 cortical only, 33 non-confluent cortical-subcortical, and 75 confluent cortical-subcortical). | Postprocessing software: Advantage Windows (GE Medical Systems) and Extended Brilliance Workspace (Philips Healthcare, Best, Netherlands) Perfusion maps: MTT. | 39% of the RSSI (single subcortical) on DWI had a perfusion deficit. However, for 67% of them, the perfusion deficit was larger than the DWI lesion and were associated with a large vessel occlusion on CT angiography. |
| Cao, 2016 [165] | A total of 62 patients: 32 with RSSI and 30 without lesions on DWI. | Postprocessing software: RAPID iSchemicView (Menlo Park, CA, US) Perfusion maps: CBF, CBV, MTT, and Tmax. | MTT showed 56% SE. No false positive perfusion images were rated. |
| García-Esperón, 2021 [166] | A total of 106 patients with lacunar syndrome: RSSI, 33 cortical and 14 posterior fossa strokes. Patients without lesions on DWI were excluded. | Postprocessing software: MIStar (Apollo Medical Imaging Technology, Melbourne, Australia) Perfusion maps: CBF, CBV, MTT, and DT. | 42% SE, 80% SP for RSSI. Visual inspection of CTP maps had higher SE than the automated method (42% vs. 6%). Sensitivity on non-contrast CT was very low (<4%). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rudilosso, S.; Rodríguez-Vázquez, A.; Urra, X.; Arboix, A. The Potential Impact of Neuroimaging and Translational Research on the Clinical Management of Lacunar Stroke. Int. J. Mol. Sci. 2022, 23, 1497. https://doi.org/10.3390/ijms23031497
Rudilosso S, Rodríguez-Vázquez A, Urra X, Arboix A. The Potential Impact of Neuroimaging and Translational Research on the Clinical Management of Lacunar Stroke. International Journal of Molecular Sciences. 2022; 23(3):1497. https://doi.org/10.3390/ijms23031497
Chicago/Turabian StyleRudilosso, Salvatore, Alejandro Rodríguez-Vázquez, Xabier Urra, and Adrià Arboix. 2022. "The Potential Impact of Neuroimaging and Translational Research on the Clinical Management of Lacunar Stroke" International Journal of Molecular Sciences 23, no. 3: 1497. https://doi.org/10.3390/ijms23031497
APA StyleRudilosso, S., Rodríguez-Vázquez, A., Urra, X., & Arboix, A. (2022). The Potential Impact of Neuroimaging and Translational Research on the Clinical Management of Lacunar Stroke. International Journal of Molecular Sciences, 23(3), 1497. https://doi.org/10.3390/ijms23031497