
Potential Biomarkers for Post-Stroke Cognitive Impairment: A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Results
2.1. Characteristics of the Included Studies Reporting Potential Biomarkers for PSCI
2.2. Classification of Potential Blood Biomarkers for PSCI
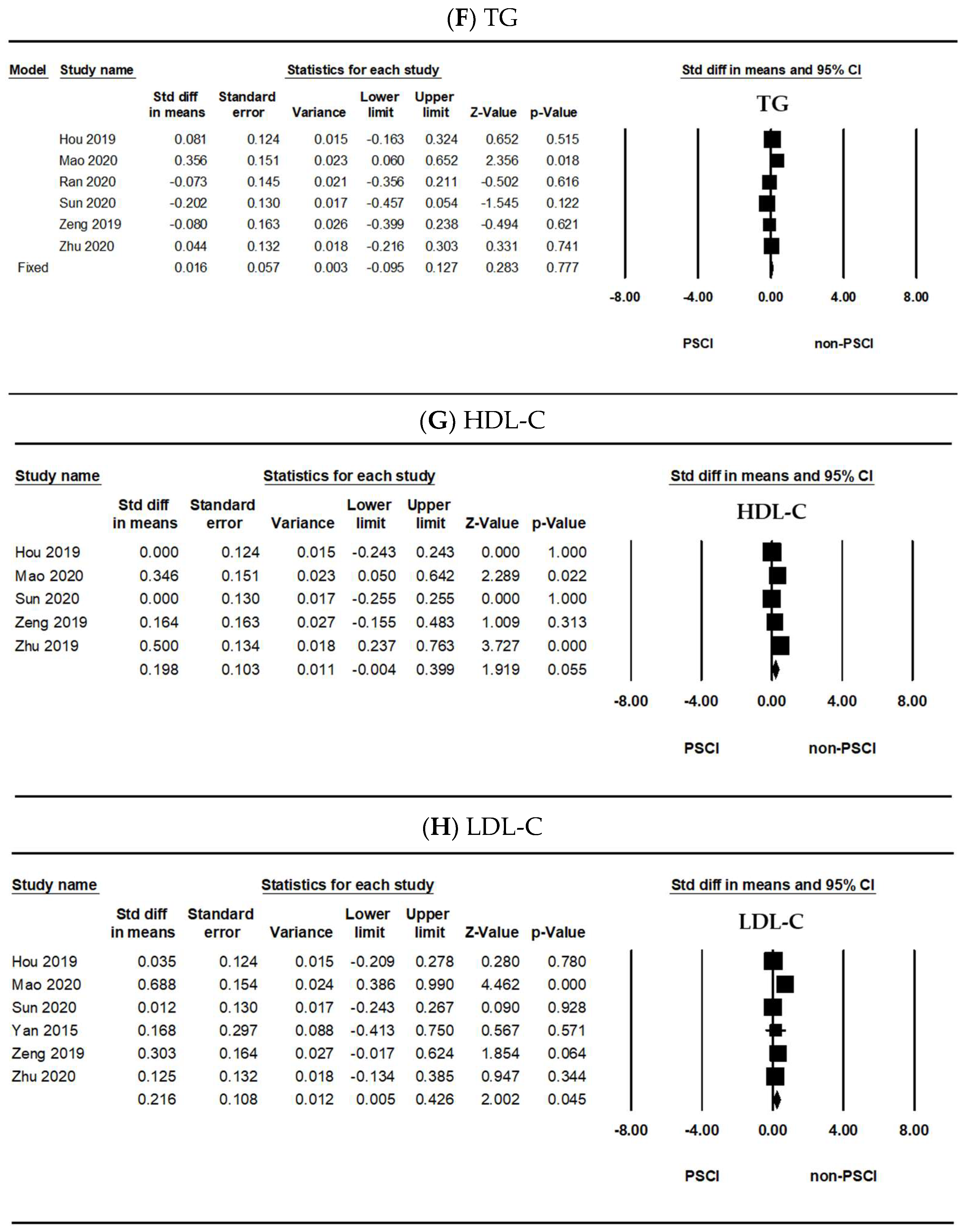
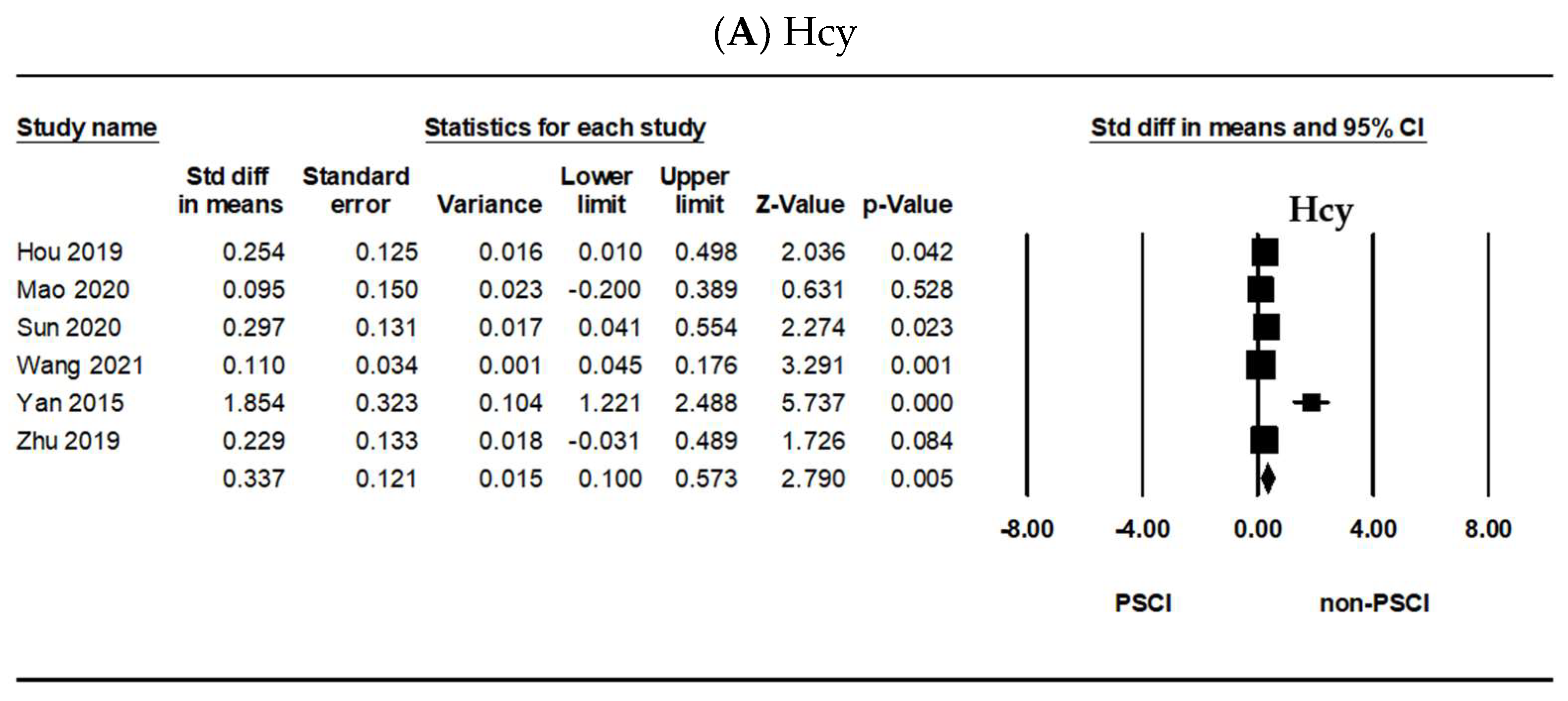
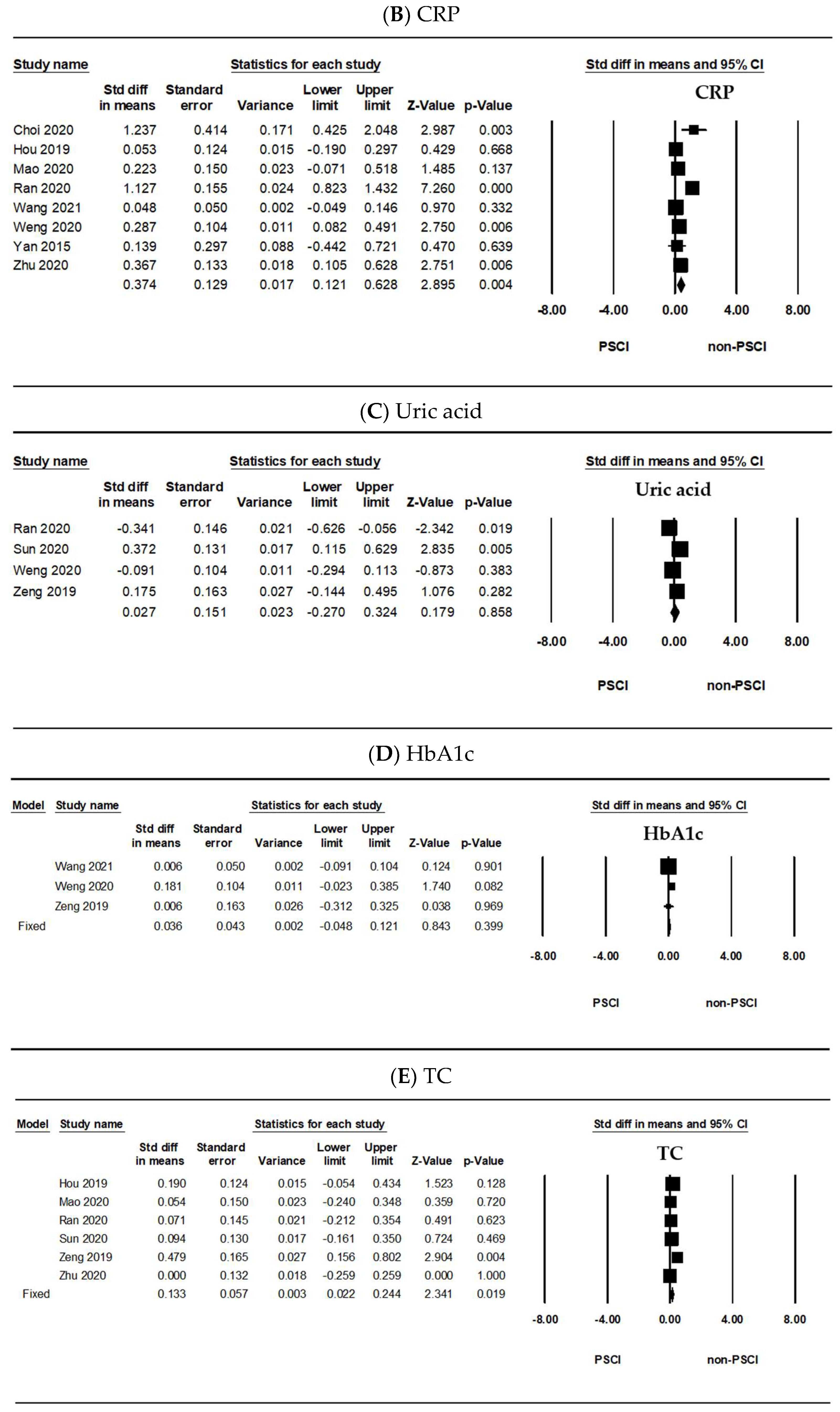
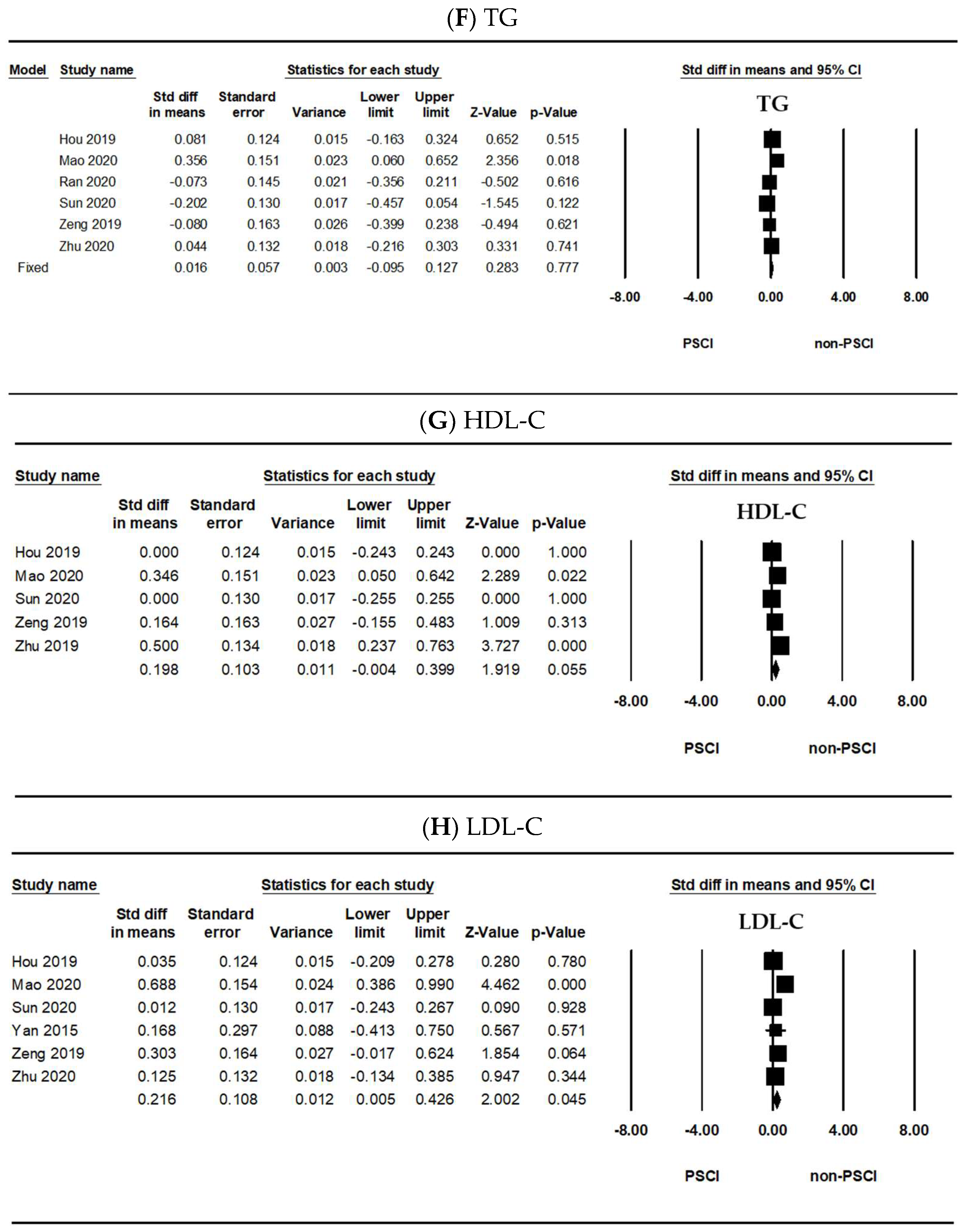
2.3. Meta-Analysis Results of the Hcy, hs-CRP, Uric Acid, HbA1c, TC, TG, HDL-C, and LDL-C Levels
3. Discussion
4. Materials and Methods
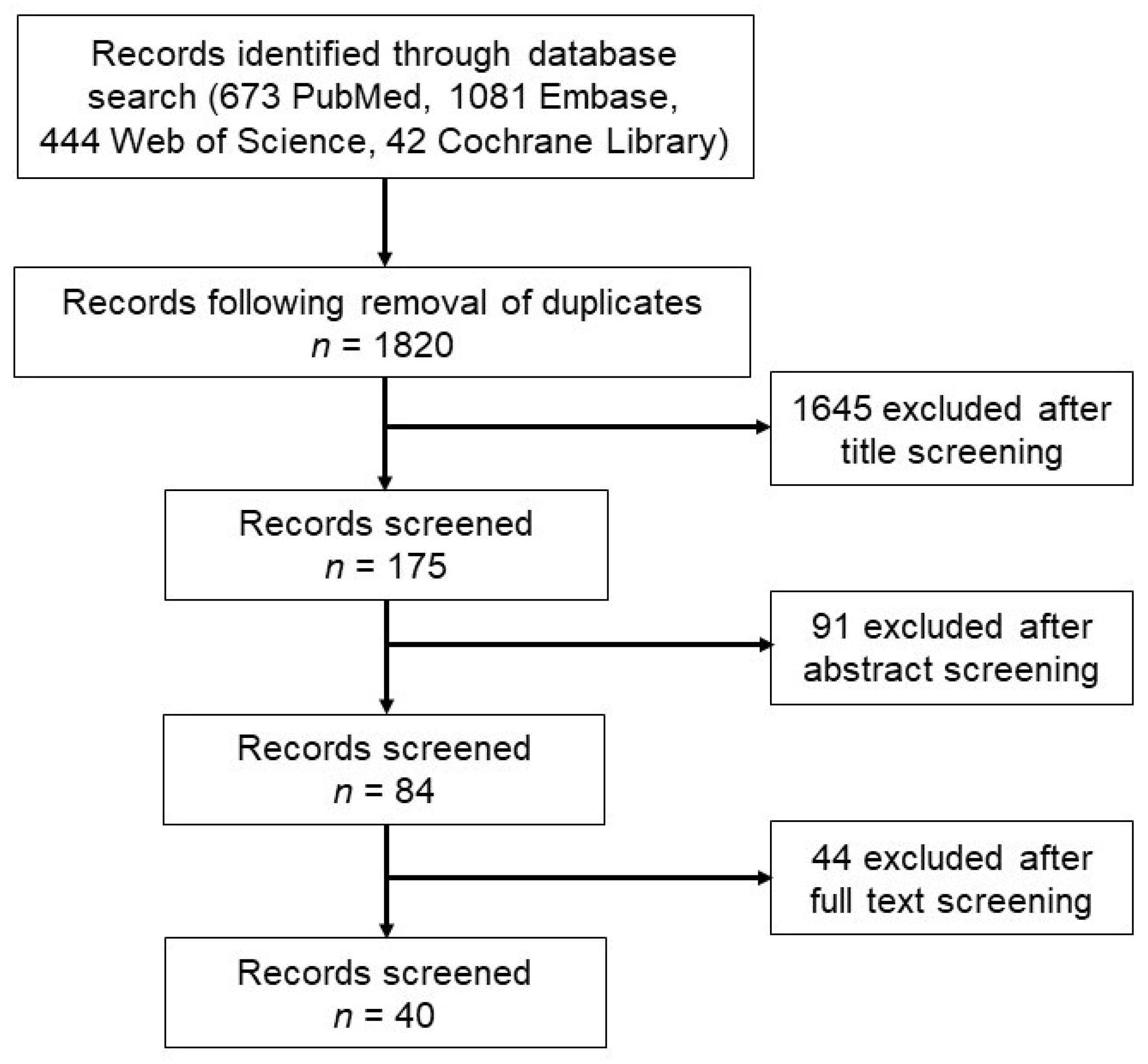
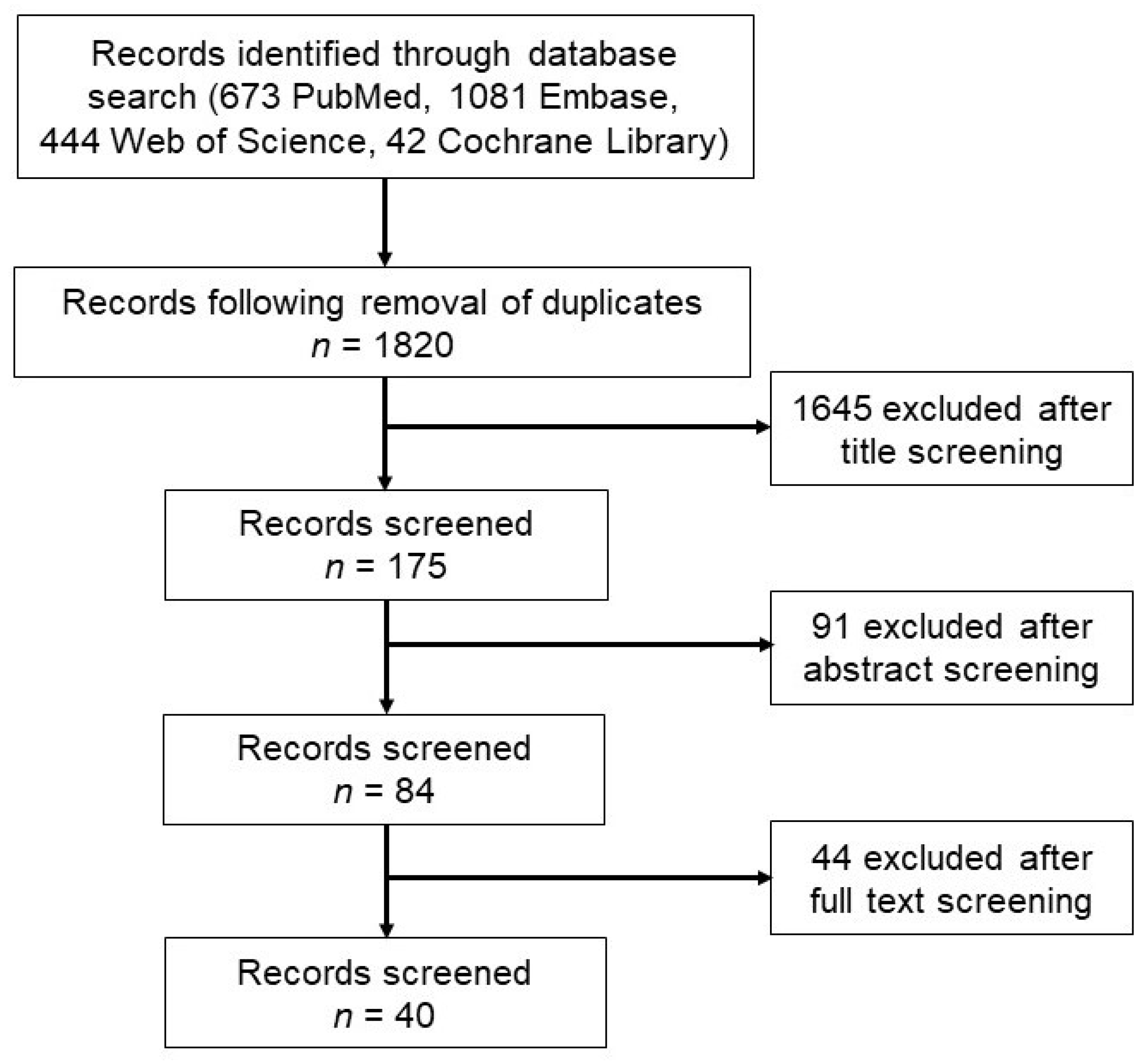
4.1. Literature Search and Selection Criteria
4.2. Data Extraction and Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Krishnamurthi, R.V.; Ikeda, T.; Feigin, V.L. Global, regional and country-specific burden of ischaemic stroke, intracerebral haemorrhage and subarachnoid haemorrhage: A systematic analysis of the global burden of disease study 2017. Neuroepidemiology 2020, 54, 171–179. [Google Scholar] [CrossRef]
- Jia, J.; Zhang, H.; Liang, X.; Dai, Y.; Liu, L.; Tan, K.; Ma, R.; Luo, J.; Ding, Y.; Ke, C. Application of metabolomics to the discovery of biomarkers for ischemic stroke in the murine model: A comparison with the clinical results. Mol. Neurobiol. 2021. [Google Scholar] [CrossRef]
- Campbell, B.C.V.; Khatri, P. Stroke. Lancet 2020, 396, 129–142. [Google Scholar] [CrossRef]
- Zhang, L.F.; Yang, J.; Hong, Z.; Yuan, G.G.; Zhou, B.F.; Zhao, L.C.; Huang, Y.N.; Chen, J.; Wu, Y.F.; Collaborative Group of China Multicenter Study of Cardiovascular, E. Proportion of different subtypes of stroke in China. Stroke 2003, 34, 2091–2096. [Google Scholar] [CrossRef] [PubMed]
- Woodruff, T.M.; Thundyil, J.; Tang, S.C.; Sobey, C.G.; Taylor, S.M.; Arumugam, T.V. Pathophysiology, treatment, and animal and cellular models of human ischemic stroke. Mol. Neurodegener. 2011, 6, 11. [Google Scholar] [CrossRef] [Green Version]
- Zhang, P.; Wang, C.; Wu, J.; Zhang, S. A systematic review of the predictive value of plasma D-dimer levels for Predicting stroke outcome. Front. Neurol. 2021, 12, 693524. [Google Scholar] [CrossRef]
- Grotta, J.C.; Albers, G.W.; Broderick, J.P.; Day, A.L.; Kasner, S.E.; Lo, E.H.; Sacco, R.L.; Wong, L.K.S. Stroke: Pathophysiology, Diagnosis, and Management, 7th. ed.; Elsevier, Inc.: Philadelphia, PA, USA, 2021. [Google Scholar]
- Fride, Y.; Adamit, T.; Maeir, A.; Ben Assayag, E.; Bornstein, N.M.; Korczyn, A.D.; Katz, N. What are the correlates of cognition and participation to return to work after first ever mild stroke? Top Stroke Rehabil 2015, 22, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Mijajlovic, M.D.; Pavlovic, A.; Brainin, M.; Heiss, W.D.; Quinn, T.J.; Ihle-Hansen, H.B.; Hermann, D.M.; Assayag, E.B.; Richard, E.; Thiel, A.; et al. Post-stroke dementia—A comprehensive review. BMC Med. 2017, 15, 11. [Google Scholar] [CrossRef] [Green Version]
- Onyike, C.U. Cerebrovascular disease and dementia. Int. Rev. Psychiatry. 2006, 18, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Kalaria, R.N.; Akinyemi, R.; Ihara, M. Stroke injury, cognitive impairment and vascular dementia. Biochim. Biophys. Acta. 2016, 1862, 915–925. [Google Scholar] [CrossRef] [Green Version]
- Vataja, R.; Pohjasvaara, T.; Mantyla, R.; Ylikoski, R.; Leppavuori, A.; Leskela, M.; Kalska, H.; Hietanen, M.; Aronen, H.J.; Salonen, O.; et al. MRI correlates of executive dysfunction in patients with ischaemic stroke. Eur. J. Neurol. 2003, 10, 625–631. [Google Scholar] [CrossRef]
- Kandiah, N.; Wiryasaputra, L.; Narasimhalu, K.; Karandikar, A.; Marmin, M.; Chua, E.V.; Sitoh, Y.Y. Frontal subcortical ischemia is crucial for post stroke cognitive impairment. J. Neurol. Sci. 2011, 309, 92–95. [Google Scholar] [CrossRef] [PubMed]
- Stephens, S.; Kenny, R.A.; Rowan, E.; Allan, L.; Kalaria, R.N.; Bradbury, M.; Ballard, C.G. Neuropsychological characteristics of mild vascular cognitive impairment and dementia after stroke. Int. J. Geriatr. Psychiatry 2004, 19, 1053–1057. [Google Scholar] [CrossRef] [PubMed]
- Roman, G.C.; Tatemichi, T.K.; Erkinjuntti, T.; Cummings, J.L.; Masdeu, J.C.; Garcia, J.H.; Amaducci, L.; Orgogozo, J.M.; Brun, A.; Hofman, A.; et al. Vascular dementia—Diagnostic-criteria for research studies—Report of the Ninds-Airen international workshop. Neurology 1993, 43, 250–260. [Google Scholar] [CrossRef] [PubMed]
- Schnider, A.; Regard, M.; Landis, T. Anterograde and retrograde amnesia following bitemporal infarction. Behav. Neurol. 1994, 7, 87–92. [Google Scholar] [CrossRef] [Green Version]
- Baez, S.D.; del Barco, D.G.; Hardy-Sosa, A.; Nieto, G.G.; Bringas-Vega, M.L.; Llibre-Guerra, J.J.; Valdes-Sosa, P. Scalable Bio marker combinations for early stroke diagnosis: A systematic review. Front. Neurol. 2021, 12. [Google Scholar] [CrossRef]
- Maas, M.B.; Furie, K.L. Molecular biomarkers in stroke diagnosis and prognosis. Biomark. Med. 2009, 3, 363–383. [Google Scholar] [CrossRef] [Green Version]
- Alex Matos Ribeiro, J.; Fernanda Garcia-Salazar, L.; Regina Saade-Pacheco, C.; Shirley Moreira Silva, E.; Garcia Oliveira, S.; Flavia Silveira, A.; Sanches Garcia-Araujo, A.; Luiz Russo, T. Prognostic molecular markers for motor recovery in acute hemorrhagic stroke: A systematic review. Clin. Chim. Acta 2021, 522, 45–60. [Google Scholar] [CrossRef]
- Biomarkers Definitions Working, Group. Biomarkers and surrogate endpoints: Preferred definitions and conceptual framework. Clin. Pharmacol. Ther. 2001, 69, 89–95. [Google Scholar] [CrossRef]
- Andone, S.; Bajko, Z.; Motataianu, A.; Mosora, O.; Balasa, R. The role of biomarkers in atherothrombotic stroke—A systematic review. Int. J. Mol. Sci. 2021, 22. [Google Scholar] [CrossRef]
- Boyd, L.A.; Hayward, K.S.; Ward, N.S.; Stinear, C.M.; Rosso, C.; Fisher, R.J.; Carter, A.R.; Leff, A.P.; Copland, D.A.; Carey, L.M.; et al. Biomarkers of stroke Recovery: Consensus-based core recommendations from the stroke recovery and rehabilitation roundtable. Neurorehabil. Neural Repair 2017, 31, 864–876. [Google Scholar] [CrossRef] [PubMed]
- Troiani, Z.; Ascanio, L.; Rossitto, C.P.; Ali, M.; Mohammadi, N.; Majidi, S.; Mocco, J.; Kellner, C.P. Prognostic utility of serum biomarkers in intracerebral hemorrhage: A systematic review. Neurorehabil. Neural Repair 2021, 15459683211041314. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Bi, X. Post-stroke cognitive impairment: A review focusing on molecular biomarkers. J. Mol. Neurosci. 2020, 70, 1244–1254. [Google Scholar] [CrossRef] [PubMed]
- Verdelho, A.; Wardlaw, J.; Pavlovic, A.; Pantoni, L.; Godefroy, O.; Duering, M.; Charidimou, A.; Chabriat, H.; Biessels, G.J. Cognitive impairment in patients with cerebrovascular disease: A white paper from the ESO Dementia Committee. Eur. Stroke J. 2021, 6, 5–17. [Google Scholar] [CrossRef]
- Kulesh, A.; Drobakha, V.; Kuklina, E.; Nekrasova, I.; Shestakov, V. Cytokine response, tract-specific fractional anisotropy, and brain morphometry in post-stroke cognitive impairment. J. Stroke Cerebrovasc. Dis. 2018, 27, 1752–1759. [Google Scholar] [CrossRef]
- Ball, E.L.; Sutherland, R.; Squires, C.; Mead, G.E.; Religa, D.; Lundstrom, E.; Cheyne, J.; Wardlaw, J.M.; Quinn, T.J.; Shenkin, S.D. Predicting post-stroke cognitive impairment using acute CT neuroimaging: A systematic review and meta-analysis. Int. J. Stroke 2021, 17474930211045836. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.S.; Lee, J.J.; Woo, C.W. Post-stroke cognitive impairment: Pathophysiological insights into brain disconnectome from advanced neuroimaging analysis techniques. J. Stroke 2021, 23, 297–311. [Google Scholar] [CrossRef]
- Potter, T.; Lioutas, V.A.; Tano, M.; Pan, A.; Meeks, J.; Woo, D.; Seshadri, S.; Selim, M.; Vahidy, F. Cognitive impairment after intracerebral Hemorrhage: A systematic review of current evidence and knowledge gaps. Front. Neurol. 2021, 12, 716632. [Google Scholar] [CrossRef]
- Kalra, L.P.; Khatter, H.; Ramanathan, S.; Sapehia, S.; Devi, K.; Kaliyaperumal, A.; Bal, D.; Sebastian, I.; Kakarla, R.; Singhania, A.; et al. Serum GFAP for stroke diagnosis in regions with limited access to brain imaging (BE FAST India). Eur. Stroke J. 2021, 6, 176–184. [Google Scholar] [CrossRef]
- Bustamante, A.; Penalba, A.; Orset, C.; Azurmendi, L.; Llombart, V.; Simats, A.; Pecharroman, E.; Ventura, O.; Ribo, M.; Vivien, D.; et al. Blood biomarkers to differentiate Ischemic and hemorrhagic strokes. Neurology 2021, 96, e1928–e1939. [Google Scholar] [CrossRef]
- Dias, A.; Silva, I.; Pinto, I.M.; Maia, L.F. Timely and blood-based multiplex molecular profiling of acute stroke. Life 2021, 11, 816. [Google Scholar] [CrossRef]
- Park, D.; Joo, S.S.; Lee, H.J.; Choi, K.C.; Kim, S.U.; Kim, Y.B. Microtubule-associated protein 2, an early blood marker of ischemic brain injury. J. Neurosci. Res. 2012, 90, 461–467. [Google Scholar] [CrossRef]
- Misra, S.; Kumar, A.; Kumar, P.; Yadav, A.K.; Mohania, D.; Pandit, A.K.; Prasad, K.; Vibha, D. Blood-based protein biomarkers for stroke differentiation: A systematic review. Proteomics Clin. Appl. 2017, 11. [Google Scholar] [CrossRef]
- Wang, L.; Song, Q.; Wang, C.; Wu, S.; Deng, L.; Li, Y.; Zheng, L.; Liu, M. Neutrophil to lymphocyte ratio predicts poor outcomes after acute ischemic stroke: A cohort study and systematic review. J. Neurol. Sci. 2019, 406, 116445. [Google Scholar] [CrossRef]
- Pendlebury, S.T.; Rothwell, P.M. Prevalence, incidence, and factors associated with pre-stroke and post-stroke dementia: A systematic review and meta-analysis. Lancet Neurol. 2009, 8, 1006–1018. [Google Scholar] [CrossRef]
- Hachinski, V.; Iadecola, C.; Petersen, R.C.; Breteler, M.M.; Nyenhuis, D.L.; Black, S.E.; Powers, W.J.; DeCarli, C.; Merino, J.G.; Kalaria, R.N.; et al. National Institute of Neurological Disorders and Stroke-Canadian Stroke Network vascular cognitive impairment harmonization standards. Stroke 2006, 37, 2220–2241. [Google Scholar] [CrossRef]
- de Champlain, J.; Wu, R.; Girouard, H.; Karas, M.A.; El Midaoui, A.; Laplante, M.A.; Wu, L. Oxidative stress in hypertension. Clin. Exp. Hypertens. 2004, 26, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Verhaeghen, P.; Salthouse, T.A. Meta-analyses of age-cognition relations in adulthood: Estimates of linear and nonlinear age effects and structural models. Psychol. Bull. 1997, 122, 231–249. [Google Scholar] [CrossRef] [PubMed]
- Alzheimer’s, Association. 2016 Alzheimer’s disease facts and figures. Alzheimers Dement. 2016, 12, 459–509. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhong, X.; Shen, J.; Jiao, L.; Tong, J.; Zhao, W.; Du, K.; Gong, S.; Liu, M.; Wei, M. Elevated serum TC and LDL-C levels in Alzheimer’s disease and mild cognitive impairment: A meta-analysis study. Brain Res. 2020, 1727, 146554. [Google Scholar] [CrossRef]
- Fernandez, C.; Lobo, M.D.V.T.; Gomez-Coronado, D.; Lasuncion, M.A. Cholesterol is essential for mitosis progression and its deficiency induces polyploid cell formation. Exp. Cell Res. 2004, 300, 109–120. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, C.; Martin, M.; Gomez-Coronado, D.; Lasuncion, M.A. Effects of distal cholesterol biosynthesis inhibitors on cell proliferation and cell cycle progression. J. Lipid Res. 2005, 46, 920–929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hooper, N.M. Detergent-insoluble glycosphingolipid/cholesterol-rich membrane domains, lipid rafts and caveolae. Mol. Membr. Biol. 1999, 16, 145–156. [Google Scholar] [CrossRef]
- Nwokoro, N.A.; Wassif, C.A.; Porter, F.D. Genetic disorders of cholesterol biosynthesis in mice and humans. Mol. Genet. Metab. 2001, 74, 105–119. [Google Scholar] [CrossRef] [PubMed]
- Goedeke, L.; Fernandez-Hernando, C. Regulation of cholesterol homeostasis. Cell Mol. Life Sci. 2012, 69, 915–930. [Google Scholar] [CrossRef]
- Ohvo-Rekila, H.; Ramstedt, B.; Leppimaki, P.; Slotte, J.P. Cholesterol interactions with phospholipids in membranes. Prog. Lipid Res. 2002, 41, 66–97. [Google Scholar] [CrossRef]
- Laudanski, K. Persistence of lipoproteins and cholesterol alterations after sepsis: Implication for atherosclerosis progression. Int. J. Mol. Sci. 2021, 22, 517. [Google Scholar] [CrossRef]
- Barba, R.; Martinez-Espinosa, S.; Rodriguez-Garcia, E.; Pondal, M.; Vivancos, J.; Del Ser, T. Poststroke dementia: Clinical features and risk factors. Stroke 2000, 31, 1494–1501. [Google Scholar] [CrossRef] [Green Version]
- Rasquin, S.M.; Verhey, F.R.; van Oostenbrugge, R.J.; Lousberg, R.; Lodder, J. Demographic and CT scan features related to cognitive impairment in the first year after stroke. J. Neurol. Neurosurg. Psychiatry 2004, 75, 1562–1567. [Google Scholar] [CrossRef] [Green Version]
- Baum, L.; Chen, X.; Cheung, W.S.; Cheung, C.K.; Cheung, L.W.; Chiu, K.F.; Wen, H.M.; Poon, P.; Woo, K.S.; Ng, H.K.; et al. Polymorphisms and vascular cognitive impairment after ischemic stroke. J. Geriatr. Psychiatry Neurol. 2007, 20, 93–99. [Google Scholar] [CrossRef]
- Tamam, B.; Tasdemir, N.; Tamam, Y. The prevalence of dementia three months after stroke and its risk factors. Turk. Psikiyatri. Derg. 2008, 19, 46–56. [Google Scholar]
- Kumral, E.; Gulluoglu, H.; Alakbarova, N.; Deveci, E.E.; Colak, A.Y.; Caginda, A.D.; Evyapan, D.; Orman, M. Cognitive decline in patients with leukoaraiosis within 5 years after initial stroke. J. Stroke Cerebrovasc. Dis. 2015, 24, 2338–2347. [Google Scholar] [CrossRef] [PubMed]
- Casolla, B.; Caparros, F.; Cordonnier, C.; Bombois, S.; Henon, H.; Bordet, R.; Orzi, F.; Leys, D. Biological and imaging predictors of cognitive impairment after stroke: A systematic review. J. Neurology 2019, 266, 2593–2604. [Google Scholar] [CrossRef] [PubMed]
- Ikonen, E. Mechanisms for cellular cholesterol transport: Defects and human disease. Physiol. Rev. 2006, 86, 1237–1261. [Google Scholar] [CrossRef] [PubMed]
- Maxfield, F.R.; Tabas, I. Role of cholesterol and lipid organization in disease. Nature 2005, 438, 612–621. [Google Scholar] [CrossRef]
- Gliozzi, M.; Musolino, V.; Bosco, F.; Scicchitano, M.; Scarano, F.; Nucera, S.; Zito, M.C.; Ruga, S.; Carresi, C.; Macri, R.; et al. Cholesterol homeostasis: Researching a dialogue between the brain and peripheral tissues. Pharmacol. Res. 2021, 163. [Google Scholar] [CrossRef]
- Quan, G.; Xie, C.; Dietschy, J.M.; Turley, S.D. Ontogenesis and regulation of cholesterol metabolism in the central nervous system of the mouse. Brain Res. Dev. Brain Res. 2003, 146, 87–98. [Google Scholar] [CrossRef]
- Saher, G.; Brugger, B.; Lappe-Siefke, C.; Mobius, W.; Tozawa, R.; Wehr, M.C.; Wieland, F.; Ishibashi, S.; Nave, K.A. High cholesterol level is essential for myelin membrane growth. Nat. Neurosci. 2005, 8, 468–475. [Google Scholar] [CrossRef]
- Morell, P.; Jurevics, H. Origin of cholesterol in myelin. Neurochem. Res. 1996, 21, 463–470. [Google Scholar] [CrossRef]
- Maiuolo, J.; Maretta, A.; Gliozzi, M.; Musolino, V.; Carresi, C.; Bosco, F.; Mollace, R.; Scarano, F.; Palma, E.; Scicchitano, M.; et al. Ethanol-induced cardiomyocyte toxicity implicit autophagy and NFkB transcription factor. Pharmacol. Res. 2018, 133, 141–150. [Google Scholar] [CrossRef]
- Dietschy, J.M.; Turley, S.D. Thematic review series: Brain lipids. Cholesterol metabolism in the central nervous system during early development and in the mature animal. J. Lipid Res. 2004, 45, 1375–1397. [Google Scholar] [CrossRef] [Green Version]
- Selhub, J. Homocysteine metabolism. Annu. Rev. Nutr. 1999, 19, 217–246. [Google Scholar] [CrossRef] [Green Version]
- Smith, A.D.; Refsum, H. Homocysteine—From disease biomarker to disease prevention. J. Intern. Med. 2021, 290, 826–854. [Google Scholar] [CrossRef]
- McCaddon, A.; Miller, J.W. Assessing the association between homocysteine and cognition: Reflections on Bradford Hill, meta-analyses, and causality. Nutr. Rev. 2015, 73, 723–735. [Google Scholar] [CrossRef] [PubMed]
- Sachdev, P.S.; Brodaty, H.; Valenzuela, M.J.; Lorentz, L.; Looi, J.C.; Berman, K.; Ross, A.; Wen, W.; Zagami, A.S. Clinical determinants of dementia and mild cognitive impairment following ischaemic stroke: The Sydney stroke study. Dement. Geriatr. Cogn. Disord. 2006, 21, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Hassan, A.; Hunt, B.J.; O’Sullivan, M.; Bell, R.; D’Souza, R.; Jeffery, S.; Bamford, J.M.; Markus, H.S. Homocysteine is a risk factor for cerebral small vessel disease, acting via endothelial dysfunction. Brain 2004, 127, 212–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ostrakhovitch, E.A.; Tabibzadeh, S. Homocysteine and age-associated disorders. Ageing Res. Rev. 2019, 49, 144–164. [Google Scholar] [CrossRef]
- Garcia, A.; Zanibbi, K. Homocysteine and cognitive function in elderly people. Can. Med. Assoc. J. 2004, 171, 897–904. [Google Scholar] [CrossRef] [Green Version]
- Price, B.R.; Wilcock, D.M.; Weekman, E.M. Hyperhomocysteinemia as a risk factor for vascular contributions to cognitive impairment and dementia. Front. Aging Neurosci. 2018, 10. [Google Scholar] [CrossRef] [Green Version]
- Sala, I.; Sanchez-Saudinos, M.B.; Molina-Porcel, L.; Lazaro, E.; Gich, I.; Clarimon, J.; Blanco-Vaca, F.; Blesa, R.; Gomez-Isla, T.; Lleo, A. Homocysteine and cognitive impairment relation with diagnosis and neuropsychological performance. Dement. Geriatr. Cogn. Disord. 2008, 26, 506–512. [Google Scholar] [CrossRef]
- Zhou, S.; Chen, J.; Cheng, L.; Fan, K.; Xu, M.; Ren, W.; Chen, Y.; Geng, D.; Cheng, H.; Luan, X.; et al. Age-dependent association between elevated homocysteine and cognitive impairment in a post-stroke population: A prospective study. Front. Nutr. 2021, 8, 691837. [Google Scholar] [CrossRef]
- Den Heijer, T.; Vermeer, S.E.; Clarke, R.; Oudkerk, M.; Koudstaal, P.J.; Hofman, A.; Breteler, M.M. Homocysteine and brain atrophy on MRI of non-demented elderly. Brain 2003, 126, 170–175. [Google Scholar] [CrossRef] [Green Version]
- Hsuchou, H.; Kastin, A.J.; Mishra, P.K.; Pan, W. C-reactive protein increases BBB permeability: Implications for obesity and neuroinflammation. Cell Physiol. Biochem. 2012, 30, 1109–1119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeon, M.T.; Kim, K.S.; Kim, E.S.; Lee, S.; Kim, J.; Hoe, H.S.; Kim, D.G. Emerging pathogenic role of peripheral blood factors following BBB disruption in neurodegenerative disease. Ageing Res. Rev. 2021, 68, 101333. [Google Scholar] [CrossRef] [PubMed]
- Di Napoli, M.; Godoy, D.A.; Campi, V.; Masotti, L.; Smith, C.J.; Parry Jones, A.R.; Hopkins, S.J.; Slevin, M.; Papa, F.; Mogoanta, L.; et al. C-reactive protein in intracerebral hemorrhage: Time course, tissue localization, and prognosis. Neurology 2012, 79, 690–699. [Google Scholar] [CrossRef]
- Di Napoli, M.; Parry-Jones, A.R.; Smith, C.J.; Hopkins, S.J.; Slevin, M.; Masotti, L.; Campi, V.; Singh, P.; Papa, F.; Popa-Wagner, A.; et al. C-reactive protein predicts hematoma growth in intracerebral hemorrhage. Stroke 2014, 45, 59–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Napoli, M.; Slevin, M.; Popa-Wagner, A.; Singh, P.; Lattanzi, S.; Divani, A.A. Monomeric C-reactive protein and cerebral Hemorrhage: From bench to bedside. Front. Immunol. 2018, 9, 1921. [Google Scholar] [CrossRef]
- Slevin, M.; Matou, S.; Zeinolabediny, Y.; Corpas, R.; Weston, R.; Liu, D.; Boras, E.; Di Napoli, M.; Petcu, E.; Sarroca, S.; et al. Monomeric C-reactive protein—A key molecule driving development of Alzheimer’s disease associated with brain ischaemia? Sci. Rep. 2015, 5, 13281. [Google Scholar] [CrossRef] [Green Version]
- Komulainen, P.; Lakka, T.A.; Kivipelto, M.; Hassinen, M.; Penttila, I.M.; Helkala, E.L.; Gylling, H.; Nissinen, A.; Rauramaa, R. Serum high sensitivity C-reactive protein and cognitive function in elderly women. Age Ageing 2007, 36, 443–448. [Google Scholar] [CrossRef] [Green Version]
- Bettcher, B.M.; Wilheim, R.; Rigby, T.; Green, R.; Miller, J.W.; Racine, C.A.; Yaffe, K.; Miller, B.L.; Kramer, J.H. C-reactive protein is related to memory and medial temporal brain volume in older adults. Brain Behav. Immun. 2012, 26, 103–108. [Google Scholar] [CrossRef] [Green Version]
- Hoth, K.F.; Haley, A.P.; Gunstad, J.; Paul, R.H.; Poppas, A.; Jefferson, A.L.; Tate, D.F.; Ono, M.; Jerskey, B.A.; Cohen, R.A. Elevated C-reactive protein is related to cognitive decline in older adults with cardiovascular disease. J. Am. Geriatr. Soc. 2008, 56, 1898–1903. [Google Scholar] [CrossRef] [PubMed]
- Wersching, H.; Duning, T.; Lohmann, H.; Mohammadi, S.; Stehling, C.; Fobker, M.; Conty, M.; Minnerup, J.; Ringelstein, E.B.; Berger, K.; et al. Serum C-reactive protein is linked to cerebral microstructural integrity and cognitive function. Neurology 2010, 74, 1022–1029. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Su, W.; Fang, J.H.; Chen, N.; Zhou, M.K.; Zhang, Y.; He, L. Elevated CRP at admission predicts post-stroke cognitive impairment in Han Chinese patients with intracranial arterial stenosis. Neurol. Res. 2018, 40, 292–296. [Google Scholar] [CrossRef]
- Tegeler, C.; O’Sullivan, J.L.; Bucholtz, N.; Goldeck, D.; Pawelec, G.; Steinhagen-Thiessen, E.; Demuth, I. The inflammatory markers CRP, IL-6, and IL-10 are associated with cognitive function—data from the Berlin aging study II. Neurobiol. Aging 2016, 38, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Ben Assayag, E.; Eldor, R.; Korczyn, A.D.; Kliper, E.; Shenhar-Tsarfaty, S.; Tene, O.; Molad, J.; Shapira, I.; Berliner, S.; Volfson, V.; et al. Type 2 diabetes mellitus and impaired renal function are associated with brain alterations and poststroke cognitive decline. Stroke 2017, 48, 2368–2374. [Google Scholar] [CrossRef]
- Qiao, M.; Chen, C.; Liang, Y.; Luo, Y.; Wu, W. The influence of serum uric acid level on Alzheimer’s Disease: A narrative review. BioMed. Res. Int. 2021, 2021, 5525710. [Google Scholar] [CrossRef]
- Kueider, A.M.; An, Y.; Tanaka, T.; Kitner-Triolo, M.H.; Studenski, S.; Ferrucci, L.; Thambisetty, M. Sex-dependent associations of serum uric acid with brain function during aging. J. Alzheimers Dis. 2017, 60, 699–706. [Google Scholar] [CrossRef]
- Noble, J.H., Jr. Meta-analysis: Methods, strengths, weaknesses, and political uses. J. Lab. Clin. Med. 2006, 147, 7–20. [Google Scholar] [CrossRef]
- Esterhuizen, T.M.; Thabane, L. Con: Meta-analysis: Some key limitations and potential solutions. Nephrol. Dial. Transplant. 2016, 31, 882–885. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author and Year | Country | Study Groups | Sample Size (M/F) | Age (y) | Outcome Measurement Tool | Specimen | Potential Biomarkers |
|---|---|---|---|---|---|---|---|
| Bunevicius et al., 2015 | Lithuania | Acute ischemic stroke | 53/25 | 72 | MMSE | Serum | NT-proBNP, IL-6, hs-CRP |
| Hemorrhagic stroke | |||||||
| Casas et al., 2017 | Argentina | Control | 20/20 | 70 ± 3/77 ± 1 | MoCA | Plasma | BDNF, NO−2 |
| Acute ischemic stroke | 20/20 | 72 ± 4/83 ± 2 | |||||
| Chei et al., 2014 | Japan | Control | 88/104 | 62.2 ± 4.4 | The dementia status was classified into six ranks. | Serum | hs-CRP |
| Dementia with a history of stroke | 44/52 | 62.4 ± 4.3 | |||||
| Control | 98/260 | 62.8 ± 5.6 | |||||
| Dementia without a history of stroke | 49/130 | 63.1 ± 5.6 | |||||
| Chen et al., 2019a | Taiwan | Post-stroke without dementia | 56/31 | 62.98 ± 9.23 | CDR | Plasma | BChE |
| Post-stroke dementia | 18/12 | 73.20 ± 8.68 | |||||
| Chen et al., 2019b | Taiwan | Post-stroke without dementia | 41/12 | 61.7 ± 8.95 | MMSE | Plasma | D-amino acid oxidase |
| Post-stroke dementia | 11/9 | 69.35 ± 7.24 | |||||
| Choi et al., 2020 | USA | Acute ischemic stroke alone | 27/8 | 64.5 ± 14.1 | Serum | IL-6, CRP, complement component 3, S100B | |
| Acute ischemic stroke and underlying dementia | 5/3 | 85.8 ± 9.6 | |||||
| Cogo et al., 2021 | France | Post-stroke cognitive decline | 6/4 | 64.7 ± 13.3 | MMSE | Serum | Quinolinic acid, quinolinic acid/kynurenic acid ratio, tryptophan, kynurenine, kynurenic acid, kynurenine/tryptophan ratio, indoleamine 2,3-dioxygenase |
| Post-stroke cognitive decline | 8/5 | 69.4 ± 17.8 | |||||
| El Hussini et al., 2020 | USA | Small-vessel-type stroke | 9/13 | 56.5 (49.5–62.0) | A standardized battery of neuropsychological tests | Plasma | VCAM-1, IFN-γ, IL-1 RA, IL-6, IL-8, IL-10, thrombin-antithrombin |
| Feng et al., 2020 | China | Stroke rhGH group | 18/8 | 61.3 ± 10 | MoCA | Plasma | TC, LDL-C, HDL-C, TG, FBG, HbA1c, IGF-1, VEGF |
| Stroke placebo group | 17/9 | 60.8 ± 11.3 | |||||
| Ge et al., 2020 | China | Acute ischemic stroke | 414/184 | 59.9 ± 10.5 | MMSE/MoCA | Serum | TIMP-1, MMP-9 |
| Gold et al., 2011 | Canada | Ischemic stroke | 22/19 | 72.3 ± 12.2 | MMSE | Plasma | Tryptophan, L-kynurenine, L-kynurenine/tryptophan |
| Hou et al., 2019 | China | Total stroke | 140/121 | 66.4 ± 9.3 | MoCA | Serum | TC, TG, LDL-C, HDL-C, hs-CRP, Hcy, retinoic acid |
| Stroke without PSCI | 65/55 | 67.7 ± 9.3 | |||||
| Stroke with PSCI | 75/66 | 67.7 ± 9.3 | |||||
| Kliper et al., 2013 | Israel | First-ever mild to moderate stroke | MoCA | Serum | CRP | ||
| Krzystanek et al., 2007 | Poland | Stroke | 15/17 | 74.13 ± 7.43 | MMSE | Platelet | Phospholipase A2 |
| Vascular dementia | 13/19 | 75.25 ± 9.22 | |||||
| Alzheimer’s disease | 10/27 | 73 ± 6.45 | |||||
| Kulesh et al., 2018 | Russian Federation | Normal cognition | 8/7 | 59.5 ± 10.0 | MMSE/MoCA | Serum | IL-1β, IL-6, IL-10, TNFα |
| Dysexecutive cognitive impairment | 13/8 | 66.4 ± 8.8 | |||||
| Mixed cognitive impairment | 16/5 | 67.8 ± 8.2 | |||||
| Liu et al., 2018 | China | Acute ischemic stroke | 71/37 | MMSE | Plasma | Uric acid, creatinine, urea N, glucose | |
| Better outcome (mRS score of ≤ 2) | 32/19 | 63.9 ± 14.9 | |||||
| Poor outcome (mRS score of >2) | 39/18 | 66.1 ± 16.2 | |||||
| Liu et al., 2017 | China | Non-PSCI | 65/27 | 60 (52.3–65.8) | MMSE | Serum | Malondialdehyde, 8-OHdG |
| PSCI | 56/45 | 66 (56–72) | |||||
| Lu et al., 2016 | China | Acute ischemic stroke | 192/61 | MMSE/MoCA | Non-HDL-C, TC, HDL-C, LDL-C, FBG, TG, Hcy, hs-CRP, HbA1c | ||
| Normal non-HDL-C | 63.1 ± 11.9 | ||||||
| High non-HDL-C | 62.2 ± 10.8 | ||||||
| Mao et al., 2020 | China | Non-PSCI | 79/37 | 65 (60–74) | MoCA | Serum | Aβ42, T3, T4, FT3, FT4, TSH, TC, TG, HDL-C, LDL-C, hs-CRP, Hcy |
| PSCI | 38/34 | 73 (66–80) | |||||
| Marklund et al., 2004 | Sweden | Acute ischemic stroke | 56/32 | 71 ± 11 | MMSE | Serum | Cortisol, DS, cortisol/DS ratio |
| Pedersen et al., 2018 | Sweden | Acute ischemic stroke | 169/99 | 18–69 | BNIS | Plasma/serum | Von Willebrand factor, tissue plasminogen activator, fibrinogen, hs-CRP |
| Stroke for <50 years | 32/35 | ||||||
| Qian et al., 2012 | China | Stroke | 44/20 | 62.1 ± 1.6 | MMSE/MoCA | Serum | sRAGE, BACE, neprilysin |
| Vascular cognitive impairment with no dementia | 19/18 | 65.5 ± 1.7 | |||||
| Vascular dementia | 18/18 | 73.8 ± 2.1 | |||||
| Mixed dementia | 6/9 | 74.6 ± 2.2 | |||||
| Qian et al., 2020 | China | Endostatin concentration group | 431/182 | 60.0 ± 10.5 | MoCA | Plasma | Endostatin |
| Ran et al., 2020 | China | Stroke | 41/74 | 57.72 ± 6.11 | MoCA | Serum | Uric acid, hs-CRP, fibrinogen, TG, cholesterol |
| PSCI | 43/39 | 59.99 ± 7.46 | |||||
| Stokowska et al., 2021 | Sweden | Intervention group | 64/51 | Letter number sequence test | Plasma | NfL | |
| Sun et al., 2020 | China | Non-PSCI | 60/26 | 64.66 ± 11.57 | MoCA | Serum | Uric acid, folic acid, VB12, Hcy, TG, cholesterol, HDL-C, LDL-C |
| PSCI | 110/78 | 71.3 ± 10.88 | |||||
| Tang et al., 2017 | Taiwan | Stroke without vascular dementia | 90/46 | 71.2 ± 6.9 | CDR/MMSE/MoCA | Plasma | sRAGE, esRAGE |
| Stroke with vascular dementia | 21/15 | 75.4 ± 8.8 | |||||
| Tong et al., 2017 | China | Stroke | 21/21 | 75.55 ± 2.39 | MMSE | Plasma | Semicarbazide-sensitive amino oxidase, formaldehyde |
| Post-stroke dementia | 21/21 | 76.14 ± 3.73 | |||||
| Wang et al., 2021 | China | Stable | 148/107 | 64.86 ± 9.37 | MMSE/MoCA | Serum | NfL |
| Progression | 26/23 | 65.18 ± 8.61 | |||||
| Wang et al., 2020 | China | Control | 14/16 | 66.1 ± 5.9 | MMSE/MoCA | Plasma/serum | Aβ40, Aβ42, Aβ42/Aβ40, CRP, TNF-α, IL-6 |
| Observation | 17/13 | 67.2 ± 7.1 | |||||
| Wang et al., 2021 | China | Non-PSCI | 355/200 | 62 ± 13 | MoCA | Plasma | pNfL, HbA1c, hs-CRP, Hcy |
| PSCI | 538/491 | 66 ± 18.5 | |||||
| Weng et al., 2020 | China | Non-PSCI | 130/67 | 64 | MoCA | Blood | CRP, TB, DBIL, IBIL, TC, Ca, uric acid, HbA1c, D-dimer |
| PSCI | 102/74 | 72 | |||||
| Yalbuzdag et al., 2015 | Turkey | Ischemic | 53/43 | 63.78 ± 12.3 | MMSE | Plasma | 25(OH)D |
| Hemorrhagic | 11/13 | 61.8 ± 10.0 | |||||
| Yan et al., 2015 | China | Non-vascular dementia | 56/48 | MMSE/MoCA | Serum | Hcy, hs-CRP, LDL-C | |
| Vascular dementia | |||||||
| Zeng et al., 2019 | China | Cognitive impairment no dementia | 61/20 | 71.40 ± 11.32 | MoCA | Serum | Cystatin C, HbA1c, creatinine, uric acid, TC, TG, HDL-C, LDL-C |
| Vascular cognitive impairment | 45/26 | 76.28 ± 15.16 | |||||
| Zhong et al., 2018 | China | MMP concentration group | 558 | MMSE/MoCA | Serum | MMP-9 | |
| Zhong et al., 2021 | China | Choline/betaine/TMAO | 433/184 | 60 ± 10.5 | MMSE/MoCA | Plasma | Choline, betaine, TMAO |
| Zhu et al., 2020 | China | Non-PSCI | 89/81 | 65 ± 10.8 | MMSE | Plasma | TMAO, TC, TG, LDL-C, HDL-C, hs-CRP, FBG, Hcy |
| PSCI | 50/36 | 71.1 ± 10.4 | |||||
| Zhu et al., 2019 | China | RF concentration group | 582 | MMSE/MoCA | Serum | RF | |
| Zhu et al., 2019 | China | MMSE/MoCA group | 448/190 | 60.7 ± 10.3 | MMSE/MoCA | Serum | aPS, GPS, aCL, GPL, β2-GPI, RF, NT-proBNP, Lp-PLA2 mass, MMP-9, tHcy, eGFR, uric acid, HGF |
| Category | Level | Potential Biomarkers |
|---|---|---|
| Blood and vascular functions | Increase | D-dimer, Hcy, endostatin, fibrinogen, VCAM-1 |
| No change | Direct bilirubin, fibrinogen, Hcy, indirect bilirubin, total bilirubin, tissue plasminogen activator, vitamin B12, VEGF, von Willebrand factor, thrombin-antithrombin | |
| Inflammatory and immune functions | Increase | esRAGE, hs-CRP (CRP), indoleamine 2,3-dioxygenase, IL-10, IL-1β, IL-6, kynurenine, MMP-9, phospholipase A2, quinolinic acid, RF, sRAGE, semicarbazide-sensitive amino oxidase, TIMP-1, TMAO, TNF-α, kynurenine/tryptophan ratio, quinolinic acid/kynurenic acid ratio |
| Decrease | BChE, hs-CRP (CRP), sRAGE | |
| No change | aCL GPL, aPS GPS, β2-GPI, complement component 3, hs-CPR (CRP), kynurenic acid, Lp-PLA2 mass, tryptophan, IFN-γ, IL-1 RA, IL-6, IL-8, IL-10 | |
| Metabolic function | Increase | FBG, HbA1c, HDL-C, LDL-C, non-HDL-C, TC, TG |
| Decrease | Betaine, TC levels | |
| No change | FBG, glucose, HbA1c, HDL-C, HGF, LDL-C, TC, TG, IGF-1 | |
| Neuronal function | Increase | BACE1, neprilysin, NfL |
| Decrease | BDNF, Aβ42, Aβ42/Aβ40, NfL | |
| No change | S100B, Aβ42, Aβ40, AChE, neprilysin | |
| Kidney function | Increase | Cystatin C, uric acid |
| Decrease | eGFR, uric acid | |
| No change | Creatinine, uric acid, urea N | |
| Oxidative stress | Increase | 8-OHdG, D-amino acid oxidase, malondialdehyde |
| Hormone | Increase | NT-proBNP, cortisol |
| Decrease | 25(OH)D, FT4, T3 | |
| No change | Cortisol/DS ratio, DS, FT3, NT-proBNP, T4, TSH | |
| Others | Decrease | Choline, formaldehyde, NO−2 |
| No change | Ca, folic acid, TMAO, retinoic acid |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, K.Y.; Shin, K.Y.; Chang, K.-A. Potential Biomarkers for Post-Stroke Cognitive Impairment: A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2022, 23, 602. https://doi.org/10.3390/ijms23020602
Kim KY, Shin KY, Chang K-A. Potential Biomarkers for Post-Stroke Cognitive Impairment: A Systematic Review and Meta-Analysis. International Journal of Molecular Sciences. 2022; 23(2):602. https://doi.org/10.3390/ijms23020602
Chicago/Turabian StyleKim, Ka Young, Ki Young Shin, and Keun-A Chang. 2022. "Potential Biomarkers for Post-Stroke Cognitive Impairment: A Systematic Review and Meta-Analysis" International Journal of Molecular Sciences 23, no. 2: 602. https://doi.org/10.3390/ijms23020602
APA StyleKim, K. Y., Shin, K. Y., & Chang, K.-A. (2022). Potential Biomarkers for Post-Stroke Cognitive Impairment: A Systematic Review and Meta-Analysis. International Journal of Molecular Sciences, 23(2), 602. https://doi.org/10.3390/ijms23020602