

Esketamine and Psilocybin—The Comparison of Two Mind-Altering Agents in Depression Treatment: Systematic Review

 ,
, 
Abstract
1. Introduction
1.1. Current Depression Treatments
1.2. The Potential of Mind-Altering Substances
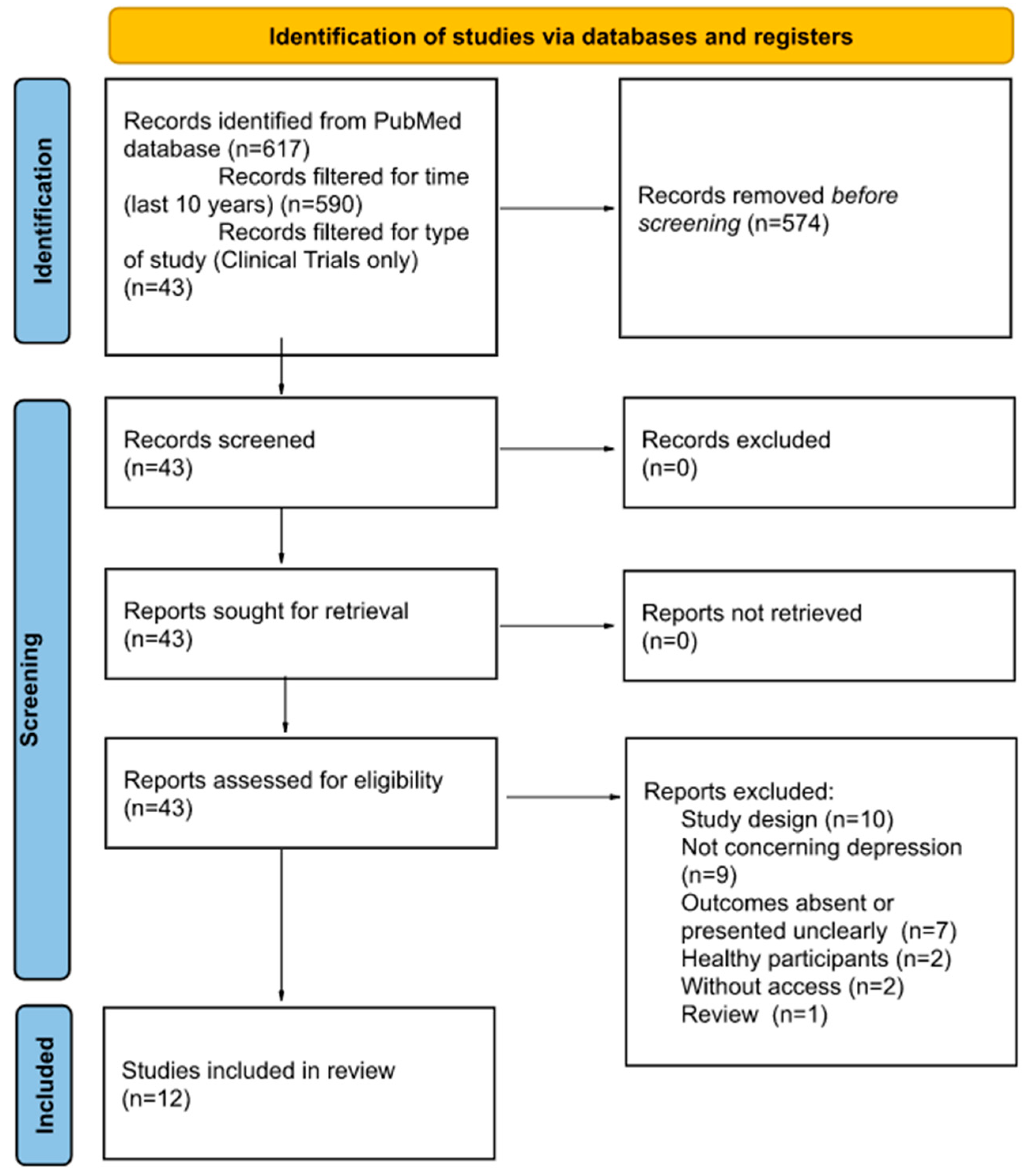
2. Methods
3. Results
3.1. Rapid Effects
3.2. Long-Term Outcomes
3.3. Suicidality
3.4. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/depression (accessed on 2 September 2022).
- Lima-Ojeda, J.M.; Rupprecht, R.; Baghai, T.C. Neurobiology of depression: A neurodevelopmental approach. World J. Biol. Psychiatry 2018, 19, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Dean, J.; Keshavan, M. The neurobiology of depression: An integrated view. Asian J. Psychiatr. 2017, 27, 101–111. [Google Scholar] [CrossRef]
- Gronemann, F.H.; Jorgensen, M.B.; Nordentoft, M.; Andersen, P.K.; Osler, M. Treatment-resistant depression and risk of all-cause mortality and suicidality in Danish patients with major depression. J. Psychiatr. Res. 2021, 135, 197–202. [Google Scholar] [CrossRef]
- Dome, P.; Rihmer, Z.; Gonda, X. Suicide Risk in Bipolar Disorder: A Brief Review. Medicina 2019, 55, 403. [Google Scholar] [CrossRef]
- Ribeiro, J.; Huang, X.; Fox, K.; Franklin, J. Depression and hopelessness as risk factors for suicide ideation, attempts and death: Meta-analysis of longitudinal studies. Br. J. Psychiatry 2018, 212, 279–286. [Google Scholar] [CrossRef]
- Wang, Z.; Ma, X.; Xiao, C. Standardized Treatment Strategy for Depressive Disorder. Adv. Exp. Med. Biol. 2019, 1180, 193–199. [Google Scholar]
- Kverno, K.S.; Mangano, E. Treatment-Resistant Depression: Approaches to Treatment. J. Psychosoc. Nurs. Ment. Health Serv. 2021, 59, 7–11. [Google Scholar] [CrossRef]
- Simon, G.E.; Savarino, J. Suicide attempts among patients starting depression treatment with medications or psychotherapy. Am. J. Psychiatry 2007, 164, 1029–1034. [Google Scholar] [CrossRef]
- Moncrieff, J.; Cooper, R.E.; Stockmann, T.; Amendola, S.; Hengartner, M.P.; Horowitz, M.A. The serotonin theory of depression: A systematic umbrella review of the evidence. Mol. Psychiatry 2022. [Google Scholar] [CrossRef]
- Nichols, D.E. Psychedelics. Pharmacol. Rev. 2016, 68, 264–355. [Google Scholar] [CrossRef]
- Psiuk, D.; Nowak, E.; Cholewa, K.; Łopuszańska, U.; Samardakiewicz, M. The Potential Role of Serotonergic Hallucinogens in Depression Treatment. Life 2021, 11, 765. [Google Scholar] [CrossRef] [PubMed]
- Carhart-Harris, R.L.; Goodwin, G.M. The Therapeutic Potential of Psychedelic Drugs: Past, Present, and Future. Neuropsychopharmacology 2017, 42, 2105–2113. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Amit, K. Comeback of ketamine: Resurfacing facts and dispelling myths. Korean J. Anesth. 2021, 74, 103–114. [Google Scholar] [CrossRef] [PubMed]
- Delray Center for Healing. Available online: https://www.delraycenter.com/a-brief-history-of-ketamine/ (accessed on 2 September 2022).
- FDA Approves New Nasal Spraw Medication for Treatment-Resistant Depression; Available Only at a Certified Doctor’s Office or Clinic. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-new-nasal-spray-medication-treatment-resistant-depression-available-only-certified (accessed on 2 September 2022).
- Byock, I. Taking Psychedelics Seriously. J. Palliat. Med. 2018, 21, 417–421. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.W.; Griffiths, R.R. Potential Therapeutic Effects of Psilocybin. Neurotherapeutics 2017, 14, 734–740. [Google Scholar] [CrossRef]
- Carhart-Harris, R.L.; Roseman, L.; Bolstridge, M.; Demetriou, L.; Pannekoek, J.N.; Wall, M.B.; Tanner, M.; Kaelen, M.; McGonigle, J.; Murphy, K.; et al. Psilocybin for treatment-resistant depression: fMRI-measured brain mechanisms. Sci. Rep. 2017, 7, 13187. [Google Scholar] [CrossRef]
- PubChem [Internet]. Bethesda (MD): National Library of Medicine (US), National Center for Biotechnology Information; PubChem Compound Summary for CID 10624, Psilocybine. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Psilocybine (accessed on 20 September 2022).
- Lowe, H.; Toyang, N.; Steele, B.; Valentine, H.; Grant, J.; Ali, A.; Ngwa, W.; Gordon, L. The Therapeutic Potential of Psilocybin. Molecules 2021, 26, 2948. [Google Scholar] [CrossRef] [PubMed]
- Kuypers, K. The therapeutic potential of microdosing psychedelics in depression. Ther. Adv. Psychopharmacol. 2020, 10. [Google Scholar] [CrossRef]
- Carhart-Harris, R.L. How do psychedelics work? Curr. Opin. Psychiatry 2019, 32, 16–21. [Google Scholar] [CrossRef]
- Nutt, D.J.; King, L.A.; Phillips, L.D. Independent Scientific Committee on Drugs. Drug harms in the UK: A multicriteria decision analysis. Lancet 2010, 376, 1558–1565. [Google Scholar] [CrossRef]
- Usdin, E.; Efron, D.; National Institute of Mental Health. Psychotropic Drugs and Related Compounds, 2nd ed.; National Institute of Mental Health: Bethesda, MD, USA, 1972; p. 138.
- Daly, E.J.; Singh, J.B.; Fedgchin, M.; Cooper, K.; Lim, P.; Shelton, R.C.; Thase, M.E.; Winokur, A.; Van Nueten, L.; Manji, H.; et al. Efficacy and Safety of Intranasal Esketamine Adjunctive to Oral Antidepressant Therapy in Treatment-Resistant Depression: A Randomized Clinical Trial. JAMA Psychiatry 2018, 75, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Smith-Apeldoorn, S.; Veraart, J.; Kamphuis, J.; van Asselt, A.; Touw, D.J.; Aan Het Rot, M.; Schoevers, R.A. Oral esketamine for treatment-resistant depression: Rationale and design of a randomized controlled trial. BMC Psychiatry 2019, 19, 375. [Google Scholar] [CrossRef] [PubMed]
- PubChem [Internet]. Bethesda (MD): National Library of Medicine (US), National Center for Biotechnology Information, PubChem Compound Summary for CID 182137, Esketamine. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Esketamine (accessed on 2 September 2022).
- Spravato. Product Information. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/spravato (accessed on 2 September 2022).
- McIntyre, R.S.; Rosenblat, J.D.; Nemeroff, C.B.; Sanacora, G.; Murrough, J.W.; Berk, M.; Brietzke, E.; Dodd, S.; Gorwood, P.; Ho, R.; et al. Synthesizing the Evidence for Ketamine and Esketamine in Treatment-Resistant Depression: An International Expert Opinion on the Available Evidence and Implementation. Am. J. Psychiatry 2021, 178, 383–399. [Google Scholar] [CrossRef] [PubMed]
- ICD-10. Available online: https://icd.who.int/browse10/2019/en/F44 (accessed on 2 September 2022).
- Molero, P.; Ramos-Quiroga, J.A.; Martin-Santos, R.; Calvo-Sánchez, E.; Gutiérrez-Rojas, L.; Meana, J.J. Antidepressant Efficacy and Tolerability of Ketamine and Esketamine: A Critical Review. CNS Drugs 2018, 32, 411–420. [Google Scholar] [CrossRef]
- Canuso, C.M.; Singh, J.B.; Fedgchin, M.; Alphs, L.; Lane, R.; Lim, P.; Pinter, C.; Hough, D.; Sanacora, G.; Manji, H.; et al. Efficacy and Safety of Intranasal Esketamine for the Rapid Reduction of Symptoms of Depression and Suicidality in Patients at Imminent Risk for Suicide: Results of a Double-Blind, Randomized, Placebo-Controlled Study. Am. J. Psychiatry 2018, 175, 620–630. [Google Scholar] [CrossRef]
- Fedgchin, M.; Trivedi, M.; Daly, E.J.; Melkote, R.; Lane, R.; Lim, P.; Vitagliano, D.; Blier, P.; Fava, M.; Liebowitz, M.; et al. Efficacy and Safety of Fixed-Dose Esketamine Nasal Spray CombinedWith a New Oral Antidepressant in Treatment-Resistant Depression: Results of a Randomized, Double-Blind, Active-Controlled Study (TRANSFORM-1). Int. J. Neuropsychopharmacol. 2019, 22, 616–630. [Google Scholar] [CrossRef]
- Popova, V.; Daly, E.J.; Trivedi, M.; Cooper, K.; Lane, R.; Lim, P.; Mazzucco, C.; Hough, D.; Thase, M.E.; Shelton, R.C.; et al. Efficacy and Safety of Flexibly Dosed Esketamine Nasal Spray Combined with a Newly Initiated Oral Antidepressant in Treatment-Resistant Depression: A Randomized Double-Blind Active-Controlled Study [correction]. Am. J. Psychiatry 2019, 176, 428–438. [Google Scholar] [CrossRef] [PubMed]
- Daly, E.J.; Trivedi, M.H.; Janik, A.; Li, H.; Zhang, Y.; Li, X.; Lane, R.; Lim, P.; Duca, A.R.; Hough, D.; et al. Efficacy of Esketamine Nasal Spray Plus Oral Antidepressant Treatment for Relapse Prevention in Patients with Treatment-Resistant Depression: A Randomized Clinical Trial. JAMA Psychiatry 2019, 76, 893–903. [Google Scholar] [CrossRef] [PubMed]
- Fu, D.J.; Ionescu, D.F.; Li, X.; Lane, R.; Lim, P.; Sanacora, G.; Hough, D.; Manji, H.; Drevets, W.C.; Canuso, C.M. Esketamine Nasal Spray for Rapid Reduction of Major Depressive Disorder Symptoms in Patients Who Have Active Suicidal Ideation with Intent: Double-Blind, Randomized Study (ASPIRE I). J. Clin. Psychiatry 2020, 81, 19m13191. [Google Scholar] [CrossRef] [PubMed]
- Ochs-Ross, R.; Daly, E.J.; Zhang, Y.; Lane, R.; Lim, P.; Morrison, R.L.; Hough, D.; Manji, H.; Drevets, W.C.; Sanacora, G.; et al. Efficacy and Safety of Esketamine Nasal Spray Plus an Oral Antidepressant in Elderly Patients with Treatment-Resistant Depression-TRANSFORM-3. Am. J. Geriatr. Psychiatry 2020, 28, 121–141. [Google Scholar] [CrossRef]
- Takahashi, N.; Yamada, A.; Shiraishi, A.; Shimizu, H.; Goto, R.; Tominaga, Y. Efficacy and safety of fixed doses of intranasal Esketamine as an add-on therapy to Oral antidepressants in Japanese patients with treatment-resistant depression: A phase 2b randomized clinical study. BMC Psychiatry 2020, 21, 526. [Google Scholar] [CrossRef] [PubMed]
- Ionescu, D.F.; Fu, D.J.; Qiu, X.; Lane, R.; Lim, P.; Kasper, S.; Hough, D.; Drevets, W.C.; Manji, H.; Canuso, C.M. Esketamine Nasal Spray for Rapid Reduction of Depressive Symptoms in Patients with Major Depressive Disorder Who Have Active Suicide Ideation with Intent: Results of a Phase 3, Double-Blind, Randomized Study (ASPIRE II). Int. J. Neuropsychopharmacol. 2021, 24, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, R.R.; Johnson, M.W.; Carducci, M.A.; Umbricht, A.; Richards, W.A.; Richards, B.D.; Cosimano, M.P.; Klinedinst, M.A. Psilocybin produces substantial and sustained decreases in depression and anxiety in patients with life-threatening cancer: A randomized double-blind trial. J. Psychopharmacol. 2016, 30, 1181–1197. [Google Scholar] [CrossRef]
- Ross, S.; Bossis, A.; Guss, J.; Agin-Liebes, G.; Malone, T.; Cohen, B.; Mennenga, S.E.; Belser, A.; Kalliontzi, K.; Babb, J. Rapid and sustained symptom reduction following psilocybin treatment for anxiety and depression in patients with life-threatening cancer: A randomized controlled trial. J. Psychopharmacol. 2016, 30, 1165–1180. [Google Scholar] [CrossRef]
- Carhart-Harris, R.; Giribaldi, B.; Watts, R.; Baker-Jones, M.; Murphy-Beiner, A.; Murphy, R.; Martell, J.; Blemings, A.; Erritzoe, D.; Nutt, D.J. Trial of Psilocybin versus Escitalopram for Depression. N. Engl. J. Med. 2021, 384, 1402–1411. [Google Scholar] [CrossRef] [PubMed]
- Malhi, G.S.; Mann, J.J. Depression. Lancet 2018, 392, 2299–2312. [Google Scholar] [CrossRef]
- Dos Santos, R.G.; Hallak, J.E.; Baker, G.; Dursun, S. Hallucinogenic/psychedelic 5HT2A receptor agonists as rapid antidepressant therapeutics: Evidence and mechanisms of action. J. Psychopharmacol. 2021, 35, 453–458. [Google Scholar] [CrossRef]
- Carhart-Harris, R.L.; Erritzoe, D.; Williams, T.; Stone, J.M.; Reed, L.J.; Colasanti, A.; Tyacke, R.J.; Leech, R.; Malizia, A.L.; Murphy, K.; et al. Neural correlates of the psychedelic state as determined by fMRI studies with psilocybin. Proc. Natl. Acad. Sci. USA 2012, 109, 2138–2143. [Google Scholar] [CrossRef]
- Liu, W.; Ge, T.; Leng, Y.; Pan, Z.; Fan, J.; Yang, W.; Cui, R. The Role of Neural Plasticity in Depression: From Hippocampus to Prefrontal Cortex. Neural Plast. 2017, 2017, 6871089. [Google Scholar] [CrossRef] [PubMed]
- Smigielski, L.; Scheidegger, M.; Kometer, M.; Vollenweider, F.X. Psilocybin-assisted mindfulness training modulates self-consciousness and brain default mode network connectivity with lasting effects. NeuroImage 2019, 196, 207–215. [Google Scholar] [CrossRef]
- Duman, R.S.; Aghajanian, G.K.; Sanacora, G.; Krystal, J.H. Synaptic Plasticity and Depression: New Insights from Stress and Rapid-Acting Antidepressants. Nat. Med. 2016, 22, 238–249. [Google Scholar] [CrossRef] [PubMed]
- Wojtas, A.; Bysiek, A.; Wawrzczak-Bargiela, A.; Szych, Z.; Majcher-Maślanka, I.; Herian, M.; Maćkowiak, M.; Gołembiowska, K. Effect of Psilocybin and Ketamine on Brain Neurotransmitters, Glutamate Receptors, DNA and Rat Behavior. Int. J. Mol. Sci. 2022, 23, 6713. [Google Scholar] [CrossRef]
- Spravato.com. Available online: https://www.spravato.com/ (accessed on 2 September 2022).
- Pereira, S.; Brennan, E.; Patel, A.; Moran, M.; Wallier, J.; Liebowitz, M.R. Managing dissociative symptoms following the use of esketamine nasal spray: A case report. Int. Clin. Psychopharmacol. 2021, 36, 54–57. [Google Scholar] [CrossRef]
- Hirschfeld, T.; Schmidt, T.T. Dose-response relationships of psilocybin-induced subjective experiences in humans. J. Psychopharmacol. 2021, 35, 384–397. [Google Scholar] [CrossRef]
- Ballard, E.D.; Zarate, C.A. The role of dissociation in ketamine’s antidepressant effects. Nat. Commun. 2020, 11, 6431. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Chen, L.; Zhang, Y.; Li, X.; Lane, R.; Lim, P.; Daly, E.J.; Furey, M.L.; Fedgchin, M.; Popova, V.; et al. Relationship Between Dissociation and Antidepressant Effects of Esketamine Nasal Spray in Patients With Treatment-Resistant Depression. Int. J. Neuropsychopharmacol. 2022, 25, 269–279. [Google Scholar] [CrossRef]
- Griffiths, R.R.; Johnson, M.W.; Richards, W.A.; Richards, B.D.; Jesse, R.; MacLean, K.A.; Barrett, F.S.; Cosimano, M.P.; Klinedinst, M.A. Psilocybin-occasioned mystical-type experience in combination with meditation and other spiritual practices produces enduring positive changes in psychological functioning and in trait measures of prosocial attitudes and behaviors. J. Psychopharmacol. 2018, 32, 49–69. [Google Scholar] [CrossRef]
- Lodge, D.; Mercier, M.S. Ketamine and phencyclidine: The good, the bad and the unexpected. Br. J. Pharm. 2015, 172, 4254–4276. [Google Scholar] [CrossRef] [PubMed]
- Sassano-Higgins, S.; Baron, D.; Juarez, G.; Esmaili, N.; Gold, M. A review of ketamine abuse and diversion. Depress. Anxiety 2016, 33, 718–727. [Google Scholar] [CrossRef] [PubMed]
- Spravato(esketamine) Nasal Spray: WHAT Are the Risks? A Guide for Patients. Available online: https://www.medicines.org.uk/emc/rm446m/1720/ (accessed on 2 September 2022).
- Nutt, D. Drugs without the Hot Air: Making Sense of Legal and Illegal Drugs; UIT Cambridge Ltd.: Cambridge, UK, 2012; pp. 254–448. [Google Scholar]
- Johnson, M.W.; Hendricks, P.S.; Barrett, F.; Griffiths, R.R. Classic psychedelics: An integrative review of epidemiology, therapeutics, mystical experience, and brain network function. Pharmacol. Ther. 2019, 197, 83–102. [Google Scholar] [CrossRef]


{kind=link}
| Author, Year | Substance | Phase | No. Part. | Condition |
|---|---|---|---|---|
| Griffiths, R. 2016 [41] | Psilocybin | Phase 2 | 51 | Depression and/or anxiety |
| Ross, S. 2016 [42] | Psilocybin | Early Phase 1 | 29 | Depression and/or anxiety |
| Carhart-Harris, R. 2021 [43] | Psilocybin | Phase 2 | 59 | Moderate-to-severe Major Depressive Disorder |
| Daly, E.J. 2018 [26] | Esketamine | Phase 2 | 57 | Treatment Resistant depression |
| Canuso, C.M. 2018 [33] | Esketamine | Phase 2 | 68 | Treatment Resistant Depression with Suicide Ideation |
| Fedgchin, M. 2019 [34] | Esketamine | Phase 3 | 346 | Treatment Resistant Depression |
| Popova, V. 2019 [35] | Esketamine | Phase 3 | 227 | Treatment Resistant depression |
| Daly, E.J. 2019 [36] | Esketamine | Phase 3 | 297 | Treatment Resistant depression |
| Fu, D-J. 2020 [37] | Esketamine | Phase 3 | 226 | Treatment Resistant Depression with Suicide Ideation |
| Ochs-Ross, R. 2020 [38] | Esketamine | Phase 3 | 51 | Treatment Resistant Depression |
| Takahashi, N. 2021 [39] | Esketamine | Phase 3b | 202 | Treatment Resistant Depression |
| Ionescu, D.F. 2021 [40] | Esketamine | Phase 3 | 230 | Treatment Resistant Depression with Suicide Ideation |
| Change in MADRS after: | LS and MD from Baseline and AD + Placebo | Author, Year | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Daly, E.J. 2018 [26] [a] | Canuso, C.M. 2018 [33] [b] | Fedgchin, M. 2019 [34] [a] | Popova, V. 2019 [35] [c] | Fu, D.-J. 2020 [37] [b] | Ionescu, D.F. 2021 [40] [b] | ||||
| 2–4 h postdose | MD from baseline | −14.3 [a1] | −17.6 * [a2] | −13.4 * | - | - | - | - | - |
| LS MD from AD + placebo | −4.6 [a1] | −7.9 * [a2] | −5.3 * | - | - | - | - | −4.2 * | |
| 24 h postdose | MD from baseline | −15.7 * [a1] | −16.4 * [a2] | - | - | - | - | −16.4 * | −15.7 * |
| LS MD from AD + placebo | −10.0 * [a1] | −10.7 * [a2] | −7.2 * | −3.0 ** [a1] | −2.2 ** [a2] | −3.3 | −3.8 * | −3.9 * | |
| Author, Year | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Canuso, C.M. 2018 [33] [a] | Fedgchin, M. 2019 [34] [b] | Popova, V. 2019 [35] [c] | Ochs-Ross, R. 2020 [38] [c] | Takahashi, N. 2021 [39] [b] | Ionescu, D.F. 2021 [40] [a] | ||||
| Day 25.–28. | MD from baseline | - | −19.0 ** | −18.8 ** | −21.4 * | −10.0 | −14.5 [b1] | −15.1 [b2] | - |
| LS mean difference from AD + placebo | −4.5 | −4.1 ** [b1] | −3.2 ** [b2] | −4.0 * | −3.6 | 0.6 [b1] | −0.9 [b2] | −3.7* | |
| Author, Year | Substance | Scale | Response Rate (vs. Control) | Remission Rate (vs. Control) |
|---|---|---|---|---|
| Griffiths, R. 2016 [41] | Psilocybin | GRID-HAMD-17 | 92% (vs. 32%) | 60% (vs. 16%) |
| Ross, S. 2016 [42] | Psilocybin | BDI | ~80% (vs. ~15%) | ~80% (vs. ~15%) |
| HADS Depression | ~70% (vs. ~40%) | ~70% (vs. ~40%) | ||
| Carhart-Harris, R. 2021 [43] | Psilocybin | QIDS-SR-16 | 70% (vs. 48%) [a] | 57% (vs. 28%) [a] |
| Daly, E.J. 2018 [26] | Esketamine | MADRS | 56% [b] | 42% [b] |
| Fedgchin, M. 2019 [34] | Esketamine | MADRS | 54.1% and 53.1% (vs. 38.9%) [c] | 36.0% and 38.8% (vs. 30.6%) [c] |
| Popova, V. 2019 [35] | Esketamine | MADRS | 69.3% (vs. 52.0%) | 52.5% (vs. 31.0%) |
| Ochs-Ross, R. 2020 [38] | Esketamine | MADRS | 27.0% (vs. 13.3%) | 17.5% (vs. 6.7%) |
| Ionescu, D.F. 2021 [40] | Esketamine | MADRS | 59% (vs. 48.0%) | 43.0% (vs. 27.0%) |
| Author, Year | Dose | Time Frame | Primary Outcome Measure | Results | Secondary Outcome Measure | Results |
|---|---|---|---|---|---|---|
| Griffiths, R. 2016 [41] | 22 or 30 mg/70 kg | 5 weeks after the 1st session | GRID-HAMD-17 | Significant difference between the Psilocybin-1st(Placebo-2nd) and Placebo-1st(Psilocybin-2nd) groups | BDI, HADS | Decrease, significant difference between the Psilocybin-1st(Placebo-2nd) and Placebo-1st(Psilocybin-2nd) groups |
| 5 weeks after the 2nd session = crossover | No significant difference between the Psilocybin-1st(Placebo-2nd) and Placebo-1st(Psilocybin-2nd) groups * | Decrease, no significant difference between the Psilocybin-1st(Placebo-2nd) and Placebo-1st(Psilocybin-2nd) groups * | ||||
| 6-months’ follow-up | Significant difference from baseline | Decrease, significant difference between baseline and 6-months’ follow-up | ||||
| Ross, S. 2016 [42] | 0.3 mg/kg | 6 weeks after the 1st session | HADS D, BDI | Significant difference from baseline in the Psilocybin-1st(Placebo-2nd) group. Significant difference between the Psilocybin-1st(Placebo-2nd) and Placebo-1st(Psilocybin-2nd) groups. | - | - |
| 6 weeks after the 2nd session = crossover | Significant difference from baseline in the Psilocybin-1st(Placebo-2nd) group. Significant difference from baseline in the Placebo-1st(Psilocybin-2nd) group in BDI, but not in HADS; No significant difference between groups in BDI, but not HADS * | |||||
| 26-week follow-up | Significant difference from baseline in both Psilocybin-1st(Placebo-2nd) and Placebo-1st(Psilocybin-2nd) groups; No significant difference between groups * | |||||
| Carhart-Harris, R. 2021 [43] | 25 mg | 6 weeks | QIDS-SR-16 | No significant difference between the psilocybin and escitalopram groups | HAMD-D-17, MADRS, BDI | As the primary endpoint was not met, the secondary outcomes’ significance was not adjusted, but in general the differences between groups favored psilocybin over escitalopram |
| Author, Year | No. of Assessed Patients | Dissociation [%] | Headaches [%] | Dizziness [%] | Vertigo [%] | Nausea [%] | Dysgeusia [%] | Elevation in BP [%] |
|---|---|---|---|---|---|---|---|---|
| Canuso, C.M. 2018 [33] | 35 (DB), 27 (FU) | 31.4 (DB), 0 (FU) | 31.4 (DB), 7.4 (FU) | 34.3 (DB), 3.7 (FU) | 11.4 (DB), 0 (FU) | 37.1 (DB), 0 (FU) | 31.4 (DB), 3.7 (FU) | N/A |
| Daly, E.J. 2018 [26] | 56 (DB), 57 (OL) | 20 (DB) | 21 (DB), 14 (OL) | 36 (DB), 39 (OL) | 7 (DB) | 18 (DB), 16 (OL) | 18 (DB), 23 (OL) | Hypertension-5 (DB) |
| Fedgchin, M. 2019 [34] | 231 | 26.8 | 20.3 | 25.1 | 20.8 | 29.4 | 16.0 | 8.2 |
| Popova, V. 2019 [35] | 116 | 26.1 | 20.0 | 20.9 | 26.1 | 26.1 | 24.3 | 9.6 |
| Daly, E.J. 2019 [36] | 152 | 23.0 | 17.8 | 20.4 | 25.0 | 16.4 | 27.0 | 6.6 |
| Fu, D-J. 2020 [37] | 113 | 29.2 | 18.6 | 35.4 | 6.2 | 20.4 | 14.2 | 16.8 |
| Ochs-Ross, R. 2020 [38] | 72 | 12.5 | 12.5 | 20.8 | 11.1 | 18.1 | 5.6 | 12.5 |
| Takahashi, N. 2021 [39] | 122 | 37.7 | 12.3 | 36.1 | 15.6 | 18.0 | N/A | 41.0 |
| Ionescu, D.F. 2021 [40] | 114 | 38.6 | 21.9 | 41.2 | 6.1 | 33.3 | 25.4 | 6.1 |
| Author, Year | Number of Assessed Patients | Dose | Psychiatric | Neurological | Cardiovascular | Gastroenterological | General |
|---|---|---|---|---|---|---|---|
| Griffiths, R. 2016 [41] | 50 cross-over | (high dose 22 or 30 mg/70 kg), (low dose 1 or 3 mg/70 kg) | psychological discomfort: 32 (high dose), 12 (low dose); transient anxiety: 26 (high dose), 15 (low dose) | - | elevation in SBP: 34 (high dose), 17 (low dose); DBP: 12 (high dose), 2 (low dose) | nausea/vomiting: 15 (high dose session), 0 (low dose) | physical discomfort: 21 (high dose session), 8 (low dose session) |
| Ross, S. 2016 [42] | 28 cross-over | 0.3 mg/kg | transient anxiety: 17; transient psychotic-like symptoms: 7 | headaches/migraine: 28 | elevation in BP and HR: 76 | nausea: 14 | - |
| Carhart-Harris, R. 2021 [43] | 30 (6-week trial period), 30 (dosing-day 1) | 25 mg | feeling jittery: 7 (6-week trial), 0 (dosing-day 1) | headaches: 67 (6-week trial), 43 (dosing-day 1); migraine: 10 (6-week trial), 0 (dosing-day 1); dizziness: 7 (6-week trial) | - | nausea: 27 (6-week trial), 13 (dosing-day 1); vomiting: 7 (6-week trial), 0 (dosing-day 1 | fatigue: 7 (6-week trial), 0 (dosing-day 1) |
| Substance | Psilocybin | Esketamine |
|---|---|---|
| Mechanisms of action | Activates the 5-HT2A receptors | Blocks subsets of NMDA receptors on GABA interneurons |
| Conjunction | In conjunction with psychotherapy | In conjunction with SSRI, SNRI |
| Depression tupe | Under research in Major Depressive Disorder and Depression Related to Life-Threatening Diseases | Treatment-Resistant Depression, Major Depressive Disorder with Suicidal Thoughts or Behaviors |
| Influence on cognitive functions | Mind-altering effects, “hallucinations” | Dissociation |
| Influence on suicidal thoughts | Likely reducing | Reducing |
| Advantages | Neither addictive nor hepatotoxic, and not toxic to tissues; Route of administration: oral; Rapid onset and long-term effects (up to 6 months) Seems to produce no serious adverse events Probably no or little abuse potential | Route of administration: nasal; Rapid onset and long-term effects (up to 7 weeks) |
| Limitations | Mind-altering side-effects, misuse potential (must be administered under monitored conditions) Caution: may increase the risk of mania in patients with bipolar disorder, and may increase the risk of cardiac arrest and death in patients with cardiovascular diseases | Mind-altering side effects (administration must take place in a clinic and be closely monitored) Not recommended for use during pregnancy or in women of age, not applicable to children under 7 years of age Reproductive Contraindications: hypersensitivity (also to ketamine), aneurysm, intracerebral hemorrhage, recent heart attack Can have abuse potential |
| Adverse Events | Minor side effects: transient increase in blood pressure, body tremors, fear and sadness, mild to moderate transient headache | Can produce serious adverse events (e.g., suicidal ideation, suicidal attempt, lacunar stroke, seizures) Other: sedation, transient increase in blood pressure |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Psiuk, D.; Nowak, E.M.; Dycha, N.; Łopuszańska, U.; Kurzepa, J.; Samardakiewicz, M. Esketamine and Psilocybin—The Comparison of Two Mind-Altering Agents in Depression Treatment: Systematic Review. Int. J. Mol. Sci. 2022, 23, 11450. https://doi.org/10.3390/ijms231911450
Psiuk D, Nowak EM, Dycha N, Łopuszańska U, Kurzepa J, Samardakiewicz M. Esketamine and Psilocybin—The Comparison of Two Mind-Altering Agents in Depression Treatment: Systematic Review. International Journal of Molecular Sciences. 2022; 23(19):11450. https://doi.org/10.3390/ijms231911450
Chicago/Turabian StylePsiuk, Dominika, Emilia Magdalena Nowak, Natalia Dycha, Urszula Łopuszańska, Jacek Kurzepa, and Marzena Samardakiewicz. 2022. "Esketamine and Psilocybin—The Comparison of Two Mind-Altering Agents in Depression Treatment: Systematic Review" International Journal of Molecular Sciences 23, no. 19: 11450. https://doi.org/10.3390/ijms231911450
APA StylePsiuk, D., Nowak, E. M., Dycha, N., Łopuszańska, U., Kurzepa, J., & Samardakiewicz, M. (2022). Esketamine and Psilocybin—The Comparison of Two Mind-Altering Agents in Depression Treatment: Systematic Review. International Journal of Molecular Sciences, 23(19), 11450. https://doi.org/10.3390/ijms231911450