
Proteomic Analysis of Human Sputum for the Diagnosis of Lung Disorders: Where Are We Today?



Abstract
1. Introduction
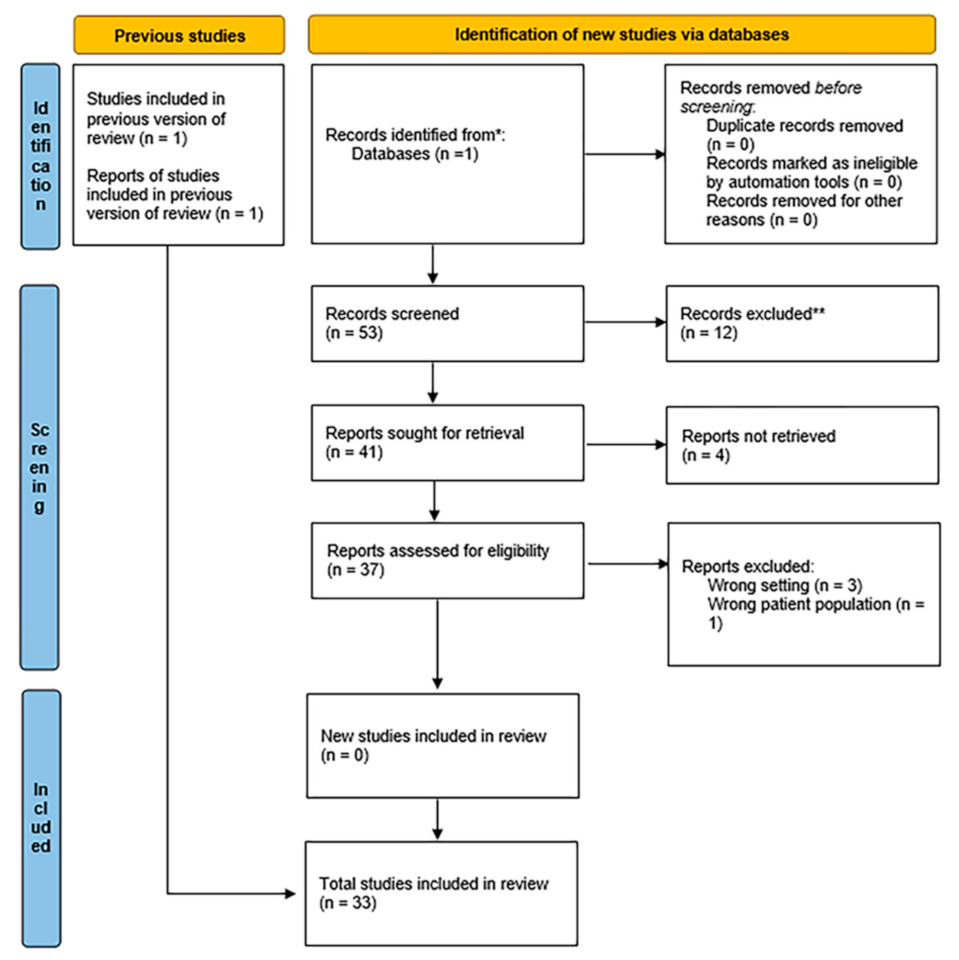
2. Methodology Followed for the Preparation of the Current Article
3. Sputum Collection and Manipulation
4. Sputum Proteomics to Investigate SARS-CoV2
5. Proteomics of Sputum in Chronic Obstructive Pulmonary Disease (COPD)
5.1. Stable COPD
5.2. Exacerbation of COPD
5.3. Overlap of COPD and Asthma and their Differentiation
6. Sputum Proteomics in Asthma
6.1. Asthma
6.2. Asthma and Gastro-Esophageal Reflux
7. Sputum Proteomics to Investigate Cystic Fibrosis
8. Sputum Proteomics and Lung Cancer
9. Proteomics of Extracellular Vesicles in Lung Disorders
10. Exploring the Role of Biomarkers
11. Methodological Considerations in Sputum Proteomics
12. Potential New Modalities of Sputum Analysis with Clinical Relevance
13. Concluding Remarks
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| Chronic obstructive pulmonary disease | COPD |
| Cystic fibrosis | CF |
| Parallel reaction monitoring | PRM |
| Reactive oxygen species | ROS |
| Neutrophil extracellular traps | NETs |
| Idiopathic pulmonary fibrosis | IPF |
| Alpha1-antitrypssin deficiency | AATD |
| Controlled asthma | CA |
| Severe uncontrolled asthma | SUA |
| Ex-smokers | ESA |
| Current smokers | CA |
| Gastro-oesophageal reflux | GORD |
| Forced expiratory volume in 1 sec | FEV1 |
References
- Iadarola, P.; Viglio, S. Spit it out! How could the sputum proteome aid clinical research into pulmonary diseases? Expert Rev. Proteom. 2017, 14, 391–393. [Google Scholar] [CrossRef] [PubMed]
- Nicholas, B.; Djukanović, R. Induced sputum: A window to lung pathology. Biochem. Soc. Trans. 2009, 37, 868–872. [Google Scholar] [CrossRef] [PubMed]
- Pitchenik, A.E.; Ganjei, P.; Torres, A.; Evans, D.A.; Rubin, E.; Baier, H. Sputum examination for the diagnosis of Pneumocystis carinii pneumonia in the acquired immunodeficiency syndrome. Am. Rev. Respir. Dis. 1986, 133, 226–229. [Google Scholar] [PubMed]
- Brightling, C.E. Clinical applications of induced sputum. Chest 2006, 129, 1344–1348. [Google Scholar] [CrossRef]
- Stacy, K.M. Pulmonary therapeutic management. In Critical Care Nursing: Diagnosis and Management, 8th ed.; Urden, L.D., Stacy, K.M., Lough., M.E., Eds.; Elsevier: Maryland Heights, MO, USA, 2018; pp. 487–519. [Google Scholar]
- Nicholas, B.; Skipp, P.; Mould, R.; Rennard, S.; Davies, D.E.; O’Connor, C.D.; Djukanović, R. Shotgun proteomic analysis of human-induced sputum. Proteomics 2006, 6, 4390–4401. [Google Scholar] [CrossRef]
- Casado, B.; Iadarola, P.; Pannell, L.K.; Luisetti, M.; Corsico, A.; Ansaldo, E.; Ferrarotti, I.; Boschetto, P.; Baraniuk, J.N. Protein expression in sputum of smokers and chronic obstructive pulmonary disease patients: A pilot study by CapLC-ESI-Q-TOF. J. Proteome Res. 2007, 6, 4615–4623. [Google Scholar] [CrossRef]
- Chen, H.; Wang, D.; Bai, C.; Wang, X. Proteomics-based biomarkers in chronic obstructive pulmonary disease. J. Proteome Res. 2010, 9, 2798–2808. [Google Scholar] [CrossRef]
- Terracciano, R.; Preianò, M.; Palladino, G.P.; Carpagnano, G.E.; Barbaro, M.P.; Pelaia, G.; Savino, R.; Maselli, R. Peptidome profiling of induced sputum by mesoporous silica beads and MALDI-TOF MS for non-invasive biomarker discovery of chronic inflammatory lung diseases. Proteomics 2011, 11, 3402–3414. [Google Scholar] [CrossRef]
- Paone, G.; Leone, V.; Conti, V.; De Marchis, L.; Ialleni, E.; Graziani, C.; Salducci, M.; Ramaccia, M.; Munafò, G. Blood and sputum biomarkers in COPD and asthma: A review. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 698–708. [Google Scholar]
- Pelaia, G.; Terracciano, R.; Vatrella, A.; Gallelli, L.; Busceti, M.T.; Calabrese, C.; Stellato, C.; Savino, R.; Maselli, R. Application of proteomics and peptidomics to COPD. Biomed. Res. Int. 2014, 2014, 764581. [Google Scholar] [CrossRef]
- Terracciano, R.; Pelaia, G.; Preianò, M.; Savino, R. Asthma and COPD proteomics: Current approaches and future directions. Proteom. Clin. Appl. 2015, 9, 203–220. [Google Scholar] [CrossRef] [PubMed]
- Guiot, J.; Demarche, S.; Henket, M.; Paulus, V.; Graff, S.; Schleich, F.; Corhay, J.L.; Louis, R.; Moermans, C. Methodology for Sputum Induction and Laboratory Processing. J. Vis. Exp. 2017, 130, 56612. [Google Scholar] [CrossRef] [PubMed]
- Delvaux, M.; Henket, M.; Lau, L.; Kange, P.; Bartsch, P.; Djukanovic, R.; Louis, R. Nebulised salbutamol administered during sputum induction improves bronchoprotection in patients with asthma. Thorax 2004, 59, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Haas, P.; Muralidharan, M.; Krogan, N.J.; Kaake, R.M.; Hüttenhain, R. Proteomic Approaches to Study SARS-CoV-2 Biology and COVID-19 Pathology. J. Proteome Res. 2021, 20, 1133–1152. [Google Scholar] [CrossRef]
- Griffin, J.H.; Downard, K.M. Mass spectrometry analytical responses to the SARS-CoV2 coronavirus in review. Trends Analyt. Chem. 2021, 142, 116328. [Google Scholar] [CrossRef]
- Amiri-Dashatan, N.; Koushki, M.; Rezaei-Tavirani, M. Mass Spectrometry-Based Proteomics Research to Fight COVID-19: An Expert Review on Hopes and Challenges. OMICS 2022, 26, 19–34. [Google Scholar] [CrossRef]
- Dollman, N.L.; Griffin, J.H.; Downard, K.M. Detection, Mapping, and Proteotyping of SARS-CoV-2 Coronavirus with High Resolution Mass Spectrometry. ACS Infect. Dis. 2020, 6, 3269–3276. [Google Scholar] [CrossRef]
- Nikolaev, E.N.; Indeykina, M.I.; Brzhozovskiy, A.G.; Bugrova, A.E.; Kononikhin, A.S.; Starodubtseva, N.L.; Petrotchenko, E.V.; Kovalev, G.I.; Borchers, C.H.; Sukhikh, G.T. Mass-Spectrometric Detection of SARS-CoV-2 Virus in Scrapings of the Epithelium of the Nasopharynx of Infected Patients via Nucleocapsid N Protein. J. Proteome Res. 2020, 19, 4393–4397. [Google Scholar] [CrossRef]
- Mann, C.; Griffin, J.H.; Downard, K.M. Detection and evolution of SARS-CoV-2 coronavirus variants of concern with mass spectrometry. Anal. Bioanal. Chem. 2021, 413, 7241–7249. [Google Scholar] [CrossRef]
- Bezstarosti, K.; Lamers, M.M.; Doff, W.A.S.; Wever, P.C.; Thai, K.T.D.; van Kampen, J.J.A.; Haagmans, B.L.; Demmers, J.A.A. Targeted proteomics as a tool to detect SARS-CoV-2 proteins in clinical specimens. PLoS ONE 2021, 16, e0259165. [Google Scholar] [CrossRef]
- Fisher, J.; Mohanty, T.; Karlsson, C.A.Q.; Khademi, S.M.H.; Malmström, E.; Frigyesi, A.; Nordenfelt, P.; Malmstrom, J.; Linder, A. Proteome Profiling of Recombinant DNase Therapy in Reducing NETs and Aiding Recovery in COVID-19 Patients. Mol. Cell. Proteom. 2021, 20, 100113. [Google Scholar] [CrossRef] [PubMed]
- Baraniuk, J.N.; Casado, B.; Pannell, L.K.; McGarvey, P.B.; Boschetto, P.; Luisetti, M.; Iadarola, P. Protein neworks in induced sputum from smokers and COPD patients. Int. J. Chron. Obstruct. Pulmon. Dis. 2015, 10, 1957–1975. [Google Scholar] [CrossRef] [PubMed]
- Reidel, B.; Radicioni, G.; Clapp, P.W.; Ford, A.A.; Abdelwahab, S.; Rebuli, M.E.; Haridass, P.; Alexis, N.E.; Jaspers, I.; Kesimer, M. E-Cigarette Use Causes a Unique Innate Immune Response in the Lung, Involving Increased Neutrophilic Activation and Altered Mucin Secretion. Am. J. Respir. Crit. Care Med. 2018, 197, 492–501. [Google Scholar] [CrossRef] [PubMed]
- Titz, B.; Sewer, A.; Schneider, T.; Elamin, A.; Martin, F.; Dijon, S.; Luettich, K.; Guedj, E.; Vuillaume, G.; Ivanov, N.V.; et al. Alterations in the sputum proteome and transcriptome in smokers and early-stage COPD subjects. J. Proteom. 2015, 128, 306–320. [Google Scholar] [CrossRef]
- Gao, J.; Ohlmeier, S.; Nieminen, P.; Toljamo, T.; Tiitinen, S.; Kanerva, T.; Bingle, L.; Araujo, B.; Rönty, M.; Höyhtyä, M.; et al. Elevated sputum BPIFB1 levels in smokers with chronic obstructive pulmonary disease: A longitudinal study. Am. J. Physiol. Lung Cell Mol. Physiol. 2015, 309, 17–26. [Google Scholar] [CrossRef]
- Ohlmeier, S.; Mazur, W.; Linja-Aho, A.; Louhelainen, N.; Rönty, M.; Toljamo, T.; Bergmann, U.; Kinnula, V.L. Sputum proteomics identifies elevated PIGR levels in smokers and mild-to-moderate COPD. J. Proteome Res. 2012, 11, 599–608. [Google Scholar] [CrossRef]
- Ohlmeier, S.; Nieminen, P.; Gao, J.; Kanerva, T.; Rönty, M.; Toljamo, T.; Bergmann, U.; Mazur, W.; Pulkkinen, V. Lung tissue proteomics identifies elevated transglutaminase 2 levels in stable chronic obstructive pulmonary disease. Am. J. Physiol. Lung Cell Mol. Physiol. 2016, 310, 1155–1165. [Google Scholar] [CrossRef]
- Moon, J.Y.; Leitao Filho, F.S.; Shahangian, K.; Takiguchi, H.; Sin, D.D. Blood and sputum protein biomarkers for chronic obstructive pulmonary disease (COPD). Expert Rev. Proteomics 2018, 15, 923–935. [Google Scholar] [CrossRef]
- Dong, T.; Santos, S.; Yang, Z.; Yang, S.; Kirkhus, N.E. Sputum and salivary protein biomarkers and point-of-care biosensors for the management of COPD. Analyst 2020, 145, 1583–1604. [Google Scholar] [CrossRef]
- Vogelmeier, C.F.; Criner, G.J.; Martinez, F.J.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Chen, R.; Decramer, M.; Fabbri, L.M.; et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am. J. Respir. Crit. Care Med. 2017, 195, 557–582. [Google Scholar] [CrossRef]
- Damera, G.; Pham, T.H.; Zhang, J.; Ward, C.K.; Newbold, P.; Ranade, K.; Sethi, S. A Sputum Proteomic Signature That Associates with Increased IL-1β Levels and Bacterial Exacerbations of COPD. Lung 2016, 194, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Mallia-Milanes, B.; Dufour, A.; Philp, C.; Solis, N.; Klein, T.; Fischer, M.; Bolton, C.E.; Shapiro, S.; Overall, C.M.; Johnson, S.R. TAILS proteomics reveals dynamic changes in airway proteolysis controlling protease activity and innate immunity during COPD. Am. J. Physiol. Lung Cell Mol. Physiol. 2018, 315, L1003–L1014. [Google Scholar] [CrossRef] [PubMed]
- O’Neil, S.E.; Lundbäck, B.; Lötvall, J. Proteomics in asthma and COPD phenotypes and endotypes for biomarker discovery and improved understanding of disease entities. J. Proteom. 2011, 75, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Terracciano, R.; Preianò, M.; Maggisano, G.; Pelaia, C.; Savino, R. Hexagonal Mesoporous Silica as a Rapid, Efficient and Versatile Tool for MALDI-TOF MS Sample Preparation in Clinical Peptidomics Analysis: A Pilot Study. Molecules 2019, 24, 2311. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Lin, F.; Liu, F.; Li, Q.; Li, Y.; Zhu, Z.; Guo, H.; Liu, L.; Liu, X.; Liu, W.; et al. Proteomic profiling reveals a distinctive molecular signature for critically ill COVID-19 patients compared with asthma and COPD: A distinctive molecular signature for critically ill COVID-19 patients. Int. J. Infect. Dis. 2022, 116, 258–267. [Google Scholar] [CrossRef]
- Dasgupta, A.; Chakraborty, R.; Saha, B.; Suri, H.; Singh, P.; Raj, A.; Taneja, B.; Dash, D.; Sengupta, S.; Agrawal, A. Sputum Protein Biomarkers in Airway Diseases: A Pilot Study. Int. J. Chron. Obstruct. Pulmon. Dis. 2021, 16, 2203–2215. [Google Scholar] [CrossRef]
- Lee, T.H.; Jang, A.S.; Park, J.S.; Kim, T.H.; Choi, Y.S.; Shin, H.R.; Park, S.W.; Uh, S.T.; Choi, J.S.; Kim, Y.H.; et al. Elevation of S100 calcium binding protein A9 in sputum of neutrophilic inflammation in severe uncontrolled asthma. Ann. Allergy Asthma Immunol. 2013, 111, 268–275. [Google Scholar] [CrossRef]
- Takahashi, K.; Pavlidis, S.; Ng Kee Kwong, F.; Hoda, U.; Rossios, C.; Sun, K.; Loza, M.; Baribaud, F.; Chanez, P.; Fowler, S.J.; et al. Sputum proteomics and airway cell transcripts of current and ex-smokers with severe asthma in U-BIOPRED: An exploratory analysis. Eur. Respir. J. 2018, 51, 1702173. [Google Scholar] [CrossRef]
- Lefaudeux, D.; De Meulder, B.; Loza, M.J.; Peffer, N.; Rowe, A.; Baribaud, F.; Bansal, A.T.; Lutter, R.; Sousa, A.R.; Corfield, J.; et al. U-BIOPRED clinical adult asthma clusters linked to a subset of sputum omics. J. Allergy Clin. Immunol. 2017, 139, 1797–1807. [Google Scholar] [CrossRef]
- Schofield, J.P.R.; Burg, D.; Nicholas, B.; Strazzeri, F.; Brandsma, J.; Staykova, D.; Folisi, C.; Bansal, A.T.; Xian, Y.; Guo, Y.; et al. Stratification of asthma phenotypes by airway proteomic signatures. J. Allergy Clin. Immunol. 2019, 144, 70–82. [Google Scholar] [CrossRef]
- Tariq, K.; Schofield, J.P.R.; Nicholas, B.L.; Burg, D.; Brandsma, J.; Bansal, A.T.; Wilson, S.J.; Lutter, R.; Fowler, S.J.; Bakke; et al. Sputum proteomic signature of gastro-oesophageal reflux in patients with severe asthma. Respir. Med. 2019, 150, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Sloane, A.J.; Lindner, R.A.; Prasad, S.S.; Sebastian, L.T.; Pedersen, S.K.; Robinson, M.; Bye, P.T.; Nielson, D.W.; Harry, J.L. Proteomic analysis of sputum from adults and children with cystic fibrosis and from control subjects. Am. J. Respir. Crit. Care Med. 2005, 172, 1416–1426. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, S.K.; Sloane, A.J.; Prasad, S.S.; Sebastian, L.T.; Lindner, R.A.; Hsu, M.; Robinson, M.; Bye, P.T.; Weinberger, R.P.; Harry, J.L. An immunoproteomic approach for identification of clinical biomarkers for monitoring disease: Application to cystic fibrosis. Mol. Cell. Proteom. 2005, 4, 1052–1060. [Google Scholar] [CrossRef] [PubMed]
- Gray, R.D.; MacGregor, G.; Noble, D.; Imrie, M.; Dewar, M.; Boyd, A.C.; Innes, J.A.; Porteous, D.J.; Greening, A.P. Sputum proteomics in inflammatory and suppurative respiratory diseases. Am. J. Respir. Crit. Care Med. 2008, 178, 444–452. [Google Scholar] [CrossRef]
- Graf, A.C.; Striesow, J.; Pané-Farré, J.; Sura, T.; Wurster, M.; Lalk, M.; Pieper, D.H.; Becher, D.; Kahl, B.C.; Riedel, K. An Innovative Protocol for Metaproteomic Analyses of Microbial Pathogens in Cystic Fibrosis Sputum. Front. Cell Infect. Microbiol. 2021, 11, 724569. [Google Scholar] [CrossRef]
- Pattison, S.H.; Gibson, D.S.; Johnston, E.; Peacock, S.; Rivera, K.; Tunney, M.M.; Pappin, D.J.; Elborn, J.S. Proteomic profile of cystic fibrosis sputum cells in adults chronically infected with Pseudomonas aeruginosa. Eur. Respir. J. 2017, 50, 1601569. [Google Scholar] [CrossRef]
- Wu, X.; Siehnel, R.J.; Garudathri, J.; Staudinger, B.J.; Hisert, K.B.; Ozer, E.A.; Hauser, A.R.; Eng, J.K.; Manoil, C.; Singh, P.K.; et al. In Vivo Proteome of Pseudomonas aeruginosa in Airways of Cystic Fibrosis Patients. J. Proteome Res. 2019, 18, 2601–2612. [Google Scholar] [CrossRef]
- Penesyan, A.; Kumar, S.S.; Kamath, K.; Shathili, A.M.; Venkatakrishnan, V.; Krisp, C.; Packer, N.H.; Molloy, M.P.; Paulsen, I.T. Genetically and Phenotypically Distinct Pseudomonas Aeruginosa Cystic Fibrosis Isolates Share a Core Proteomic Signature. PLoS ONE 2015, 10, e0138527. [Google Scholar] [CrossRef]
- Yu, L.; Shen, J.; Mannoor, K.; Guarnera, M.; Jiang, F. Identification of ENO1 as a potential sputum biomarker for early-stage lung cancer by shotgun proteomics. Clin. Lung Cancer 2014, 15, 372–378. [Google Scholar] [CrossRef]
- Ali-Labib, R.; Louka, M.L.; Galal, I.H.; Tarek, M. Evaluation of matrix metalloproteinase-2 in lung cancer. Proteom. Clin. Appl. 2014, 8, 251–257. [Google Scholar] [CrossRef]
- Rostila, A.M.; Anttila, S.L.; Lalowski, M.M.; Vuopala, K.S.; Toljamo, T.I.; Lindström, I.; Baumann, M.H.; Puustinen, A.M. Reactive oxygen species-regulating proteins peroxiredoxin 2 and thioredoxin, and glyceraldehyde-3-phosphate dehydrogenase are differentially abundant in induced sputum from smokers with lung cancer or asbestos exposure. Eur. J. Cancer Prev. 2020, 29, 238–247. [Google Scholar] [CrossRef] [PubMed]
- Böttger, F.; Schaaij-Visser, T.B.; de Reus, I.; Piersma, S.R.; Pham, T.V.; Nagel, R.; Brakenhoff, R.H.; Thunnissen, E.; Smit, E.F.; Jimenez, C.R. Proteome analysis of non-small cell lung cancer cell line secretomes and patient sputum reveals biofluid biomarker candidates for cisplatin response prediction. J. Proteom. 2019, 196, 106–119. [Google Scholar] [CrossRef] [PubMed]
- Gaspar Marques, J.; Lobato, M.; Leiria-Pinto, P.; Neuparth, N.; Carreiro Martins, P. Asthma and COPD “overlap”: A treatable trait or common several treatable-traits? Eur. Ann. Allergy Clin. Immunol. 2020, 52, 148–159. [Google Scholar] [CrossRef] [PubMed]
- Havemann, B.D.; Henderson, C.A.; El-Serag, H.B. The association between gastro-oesophageal reflux disease and asthma: A systematic review. Gut 2007, 56, 1654–1664. [Google Scholar] [CrossRef] [PubMed]
- Han, Z.; Kautto, L.; Nevalainen, H. Secretion of Proteases by an Opportunistic Fungal Pathogen Scedosporium aurantiacum. PLoS ONE 2017, 12, e0169403. [Google Scholar] [CrossRef] [PubMed]
- Hoseok, I.; Je-Yoel, C. Lung cancer biomarkers. Adv. Clin. Chem. 2015, 72, 107–170. [Google Scholar]
- Molina, J.R.; Yang, P.; Cassivi, S.D.; Schild, S.E.; Adjei, A.A. Non-small cell lung cancer: Epidemiology, risk factors, treatment, and survivorship. Mayo Clin. Proc. 2008, 83, 584–594. [Google Scholar] [CrossRef]
- Hassanein, M.; Callison, J.C.; Callaway-Lane, C.; Aldrich, M.C.; Grogan, E.L.; Massion, P.P. The state of molecular biomarkers for the early detection of lung cancer. Cancer Prev. Res. 2012, 5, 992–1006. [Google Scholar] [CrossRef]
- Basset, P.; Okada, A.; Cenard, M.P.; Kannan, R.; Stoll, I.; Anglard, P.; Bellocq, J.P.; Rio, M.C. Matrix metalloproteinases as stromal effectors of human carcinoma progression: Therapeutical implications. Matrix Biol. 1997, 15, 535–541. [Google Scholar] [CrossRef]
- Johnsen, M.; Lund, L.R.; Romer, J.; Almholt, K.; Danø, K. Cancer invasion and tissue remodelling: Common themes in proteoglytic matrix. Curr. Opin. Cell Biol. 1998, 10, 667–671. [Google Scholar] [CrossRef]
- Leeman, M.F.; Curran, S.; Murray, G.I. New insights into the roles of matrix metalloproteinases in colorectal cancer development and progression. J. Pathol. 2003, 201, 528–534. [Google Scholar] [CrossRef] [PubMed]
- Menegon, S.; Columbano, A.; Giordano, S. The dual roles of NRF2 in cancer. Trends Mol. Med. 2016, 22, 578–593. [Google Scholar] [CrossRef] [PubMed]
- Lehtonen, S.T.; Svensk, A.M.; Soini, Y.; Pääkkö, P.; Hirvikoski, P.; Kang, S.W.; Säily, M.; Kinnula, V.L. Peroxiredoxins, a novel protein family in lung cancer. Int. J. Cancer 2004, 111, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Jung, A.L.; Møller Jørgensen, M.; Bæk, R.; Griss, K.; Han, M.; Auf Dem Brinke, K.; Timmesfeld, N.; Bertrams, W.; Greulich, T.; Koczulla, R.; et al. Surface Proteome of Plasma Extracellular Vesicles as Biomarkers for Pneumonia and Acute Exacerbation of Chronic Obstructive Pulmonary Disease. J. Infect. Dis. 2020, 221, 325–335. [Google Scholar] [CrossRef] [PubMed]
- Useckaite, Z.; Ward, M.P.; Trappe, A.; Reilly, R.; Lennon, J.; Davage, H.; Matallanas, D.; Cassidy, H.; Dillon, E.T.; Brennan, K.; et al. Increased extracellular vesicles mediate inflammatory signalling in cystic fibrosis. Thorax 2020, 75, 449–458. [Google Scholar] [CrossRef]
- Vykoukal, J.; Sun, N.; Aguilar-Bonavides, C.; Katayama, H.; Tanaka, I.; Fahrmann, J.F.; Capello, M.; Fujimoto, J.; Aguilar, M.; Wistuba, I.I.; et al. Plasma-derived extracellular vesicle proteins as a source of biomarkers for lung adenocarcinoma. Oncotarget 2017, 8, 95466–95480. [Google Scholar] [CrossRef]
- Lässer, C.; O’Neil, S.E.; Shelke, G.V.; Sihlbom, C.; Hansson, S.F.; Gho, Y.S.; Lundbäck, B.; Lötvall, J. Exosomes in the nose induce immune cell trafficking and harbour an altered protein cargo in chronic airway inflammation. J. Transl. Med. 2016, 14, 181. [Google Scholar] [CrossRef]
- Trappe, A.; Donnelly, S.C.; McNally, P.; Coppinger, J.A. Role of extracellular vesicles in chronic lung disease. Thorax 2021, 76, 1047–1056. [Google Scholar] [CrossRef]
- Dobler, C.C. Biomarkers in respiratory diseases. Breathe 2019, 15, 265–266. [Google Scholar] [CrossRef]
- Bene, Z.; Fejes, Z.; Macek, M., Jr.; Amaral, M.D.; Balogh, I.; Nagy, B., Jr. Laboratory biomarkers for lung disease severity and progression in cystic fibrosis. Clin. Chim. Acta 2020, 508, 277–286. [Google Scholar] [CrossRef]
- Maghsoudloo, M.; Azimzadeh Jamalkandi, S.; Najafi, A.; Masoudi-Nejad, A. Identification of biomarkers in common chronic lung diseases by co-expression networks and drug-target interactions analysis. Mol. Med. 2020, 26, 9. [Google Scholar] [CrossRef] [PubMed]
- Group, B.D.W. Biomarkers and surrogate endpoints: Preferred definitions and conceptual framework. Clin. Pharmacol. Ther. 2001, 69, 89–95. [Google Scholar]
- Miyah, Y.; Benjelloun, M.; Lairini, S.; Lahrichi, A. COVID-19 Impact on Public Health, Environment, Human Psychology, Global Socioeconomy, and Education. Sci. World J. 2022, 2022, 5578284. [Google Scholar] [CrossRef] [PubMed]
- Rocha-Filho, C.R.; Martins, J.W.L.; Lucchetta, R.C.; Ramalho, G.S.; Trevisani, G.F.M.; da Rocha, A.P.; Pinto, A.C.P.N.; Reis, F.S.A.; Ferla, L.J.; Mastroianni, P.C.; et al. Hospitalization costs of coronaviruses diseases in upper-middle-income countries: A systematic review. PLoS ONE 2022, 17, e0265003. [Google Scholar] [CrossRef] [PubMed]
- He, G.; Dong, T.; Yang, Z.; Branstad, A.; Huang, L.; Jiang, Z. Point-of-care COPD diagnostics: Biomarkers, sampling, paper-based analytical devices, and perspectives. Analyst 2022, 147, 1273–1293. [Google Scholar] [CrossRef] [PubMed]
- Miravitlles, M.; Herepath, M.; Priyendu, A.; Sharma, S.; Vilchez, T.; Vit, O.; Haensel, M.; Lepage, V.; Gens, H.; Greulich, T. Disease burden associated with alpha-1 antitrypsin deficiency: Systematic and structured literature reviews. Eur. Respir. Rev. 2022, 31, 210262. [Google Scholar] [CrossRef]
- Morel, D. Special Needs Insurance: More Stability for a Growing Family’s Budget. J. Insur. Med. 2021, 49 (Suppl. 1), 1–31. [Google Scholar] [CrossRef]
- Poste, G. Bring on the biomarkers. Nature 2011, 469, 156–157. [Google Scholar] [CrossRef]
- Rosenberg, S.R.; Kalhan, R. Biomarkers in chronic obstructive pulmonary disease. Transl. Res. 2012, 159, 228–237. [Google Scholar] [CrossRef]
- Chen, Y.W.; Leung, J.M.; Sin, D.D. A Systematic Review of Diagnostic Biomarkers of COPD Exacerbation. PLoS ONE 2016, 11, e0158843. [Google Scholar] [CrossRef]
- He, L.X.; Tang, Z.H.; Huang, Q.S.; Li, W.H. DNA Methylation: A Potential Biomarker of Chronic Obstructive Pulmonary Disease. Front. Cell Dev. Biol. 2020, 8, 585. [Google Scholar] [CrossRef] [PubMed]
- Stockley, R.A.; Halpin, D.M.G.; Celli, B.R.; Singh, D. Chronic Obstructive Pulmonary Disease Biomarkers and Their Interpretation. Am. J. Respir. Crit. Care Med. 2019, 199, 1195–1204. [Google Scholar] [CrossRef]
- Tiotiu, A. Biomarkers in asthma: State of the art. Asthma Res. Pract. 2018, 4, 10. [Google Scholar] [CrossRef] [PubMed]
- Alving, K.; Diamant, Z.; Lucas, S.; Magnussen, H.; Pavord, I.D.; Piacentini, G.; Price, D.; Roche, N.; Sastre, J.; Thomas, M.; et al. Point-of-care biomarkers in asthma management: Time to move forward. Allergy 2020, 75, 995–997. [Google Scholar] [CrossRef] [PubMed]
- Leru, P.M. Biomarkers in Asthma-Interpretation, and Utility in Current Asthma Management. Curr. Respir. Med. Rev. 2021, 17, 62–68. [Google Scholar] [CrossRef]
- Rabilloud, T. Paleoproteomics explained to youngsters: How did the wedding of two-dimensional electrophoresis and protein sequencing spark proteomics on: Let there be light. J. Proteom. 2014, 107, 5–12. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Rogowska-Wrzesinska, A.; Le Bihan, M.C.; Thaysen-Andersen, M.; Roepstorff, P. 2D gels still have a niche in proteomics. J. Proteomics 2013, 88, 4–13. [Google Scholar] [CrossRef]
- Oliveira, B.M.; Coorssen, J.R.; Martins-de-Souza, D. 2DE: The phoenix of proteomics. J. Proteom. 2014, 104, 140–150. [Google Scholar] [CrossRef]
- Zhan, X.; Li, B.; Zhan, X.; Schlüter, H.; Jungblut, P.R.; Coorssen, J.R. Innovating the Concept and Practice of Two-Dimensional Gel Electrophoresis in the Analysis of Proteomes at the Proteoform Level. Proteomes 2019, 7, 36. [Google Scholar] [CrossRef]
- Marcus, K.; Lelong, C.; Rabilloud, T. What Room for Two-Dimensional Gel-Based Proteomics in a Shotgun Proteomics World? Proteomes 2020, 8, 17. [Google Scholar] [CrossRef]
- Greco, V.; Piras, C.; Pieroni, L.; Ronci, M.; Putignani, L.; Roncada, P.; Urbani, A. Applications of MALDI-TOF mass spectrometry in clinical proteomics. Exp. Rev. Proteom. 2018, 15, 683–696. [Google Scholar] [CrossRef] [PubMed]
- Liotta, L.A.; Petricoin, E.F. Mass spectrometry-based protein biomarker discovery: Solving the remaining challenges to reach the promise of clinical benefit. Clin. Chem. 2010, 56, 1641–1642. [Google Scholar] [CrossRef] [PubMed]
- Saude, E.J.; Lacy, P.; Musat-Marcu, S.; Mayes, D.C.; Bagu, J.; Man, S.F.; Sykes, B.D.; Moqbel, R. NMR analysis of neutrophil activation in sputum samples from patients with cystic fibrosis. Magn. Reason. Med. 2004, 52, 807–814. [Google Scholar] [CrossRef] [PubMed]
- Abrami, M.; Ascenzioni, F.; Di Domenico, E.G.; Maschio, M.; Ventura, A.; Confalonieri, M.; Di Gioia, S.; Conese, M.; Dapas, B.; Grassi, G.; et al. A novel approach based on low-field NMR for the detection of the pathological components of sputum in cystic fibrosis patients. Magn. Reason. Med. 2018, 79, 2323–2331. [Google Scholar] [CrossRef] [PubMed]
- Emwas, A.H.; Roy, R.; McKay, R.T.; Tenori, L.; Saccenti, E.; Gowda, G.A.N.; Raftery, D.; Alahmari, F.; Jaremko, L.; Jaremko, M.; et al. NMR Spectroscopy for Metabolomics Research. Metabolites 2019, 9, 123. [Google Scholar] [CrossRef] [PubMed]
- Hogan, D.A.; Willger, S.D.; Dolben, E.L.; Hampton, T.H.; Stanton, B.A.; Morrison, H.G.; Sogin, M.L.; Czum, J.; Ashare, A. Analysis of Lung Microbiota in Bronchoalveolar Lavage, Protected Brush and Sputum Samples from Subjects with Mild-To-Moderate Cystic Fibrosis Lung Disease. PLoS ONE 2016, 11, e0149998. [Google Scholar] [CrossRef]
- Hauptmann, M.; Schaible, U.E. Linking microbiota and respiratory disease. FEBS Lett. 2016, 590, 3721–3738. [Google Scholar] [CrossRef]
- Wang, Z.; Singh, R.; Miller, B.E.; Tal-Singer, R.; Van Horn, S.; Tomsho, L.; Mackay, A.; Allinson, J.P.; Webb, A.J.; Brookes, A.J.; et al. Sputum microbiome temporal variability and dysbiosis in chronic obstructive pulmonary disease exacerbations: An analysis of the COPDMAP study. Thorax 2018, 73, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Maschera, B.; Lea, S.; Kolsum, U.; Michalovich, D.; Van Horn, S.; Traini, C.; Brown, J.R.; Hessel, E.M.; Singh, D. Airway host-microbiome interactions in chronic obstructive pulmonary disease. Respir. Res. 2019, 20, 113. [Google Scholar] [CrossRef]
- Haldar, K.; George, L.; Wang, Z.; Mistry, V.; Ramsheh, M.Y.; Free, R.C.; John, C.; Reeve, N.F.; Miller, B.E.; Tal-Singer, R.; et al. The sputum microbiome is distinct between COPD and health, independent of smoking history. Respir. Res. 2020, 21, 183. [Google Scholar] [CrossRef]
- Tsay, J.J.; Segal, L.N. Could the Sputum Microbiota Be a Biomarker That Predicts Mortality after Acute Exacerbations of Chronic Obstructive Pulmonary Disease? Am. J. Respir. Crit. Care Med. 2019, 199, 1175–1176. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Subjects Investigated | Method of Sputum Collection and Processing | Proteomic Technique Applied | Target of the Research | Finding | Reference # |
|---|---|---|---|---|---|
| COVID-19 patients | Spontaneous. Sputum was diluted in medium and a few droplets pipetted on glass slides, dried and fixed in 80% acetone. | Parallel reaction monitoring MS Proteomics | Determining the LOD of viral proteins in sputum and nasopharyngeal swabs of patients | The method is suitable for the successful detection of viral infection in clinical specimens and can be used in clinical and diagnostics labs | [21] |
| COVID-19 patients | Spontaneous. Sputum was treated with or without 10 units of rhDNase Samples were cytocentrifuged and then prepared for immunostaining. | Data-independent acquisition MS | Identification of neutrophil extracellular traps (NETS) in sputum and blood plasma of patients | Several NET-derived proteins were identified | [22] |
| Subjects Investigated | Method of Sputum Collection and Processing | Proteomic Technique Applied | Target of the Rersearch | Finding | Reference # |
|---|---|---|---|---|---|
| Nonsmokers/Smokers, COPD Patients with or without emphysema | Induced *. Sputum was treated with DTT, and cellular and aggregated material removed. Proteins in the supernatant were alkylated and digested with trypsin. | Capillary LC-MS/MS | Finding biomarkers of emphysema | Mucins, long palate lung nasal clone 1 and other proteins were identified as potential biomarkers | [7,23] |
| Nonsmokers/Smokers, e-cigarette users | Induced. Sputum was diluted 1:1 in GuHC and proteins alkylated and digested with trypsin. | Nano LC /MS | Potential adverse health effects of e-cigarettes on human airways | The use of e-cigarette altered the profile of innate defense proteins in airway secretions | [24] |
| Never smokers, former smokers, current asymptomatic smokers, and smokers with early-stage COPD | Induced. Sputum was centrifuged and supernatant containing the proteins treated as indicated above (see ref. [7]). | Nano LC-MS/MS | Relationship between cigarette smoking and onset of COPD | Alterations in mucin/trefoil proteins and a prominent xenobiotic/oxidative stress response in smokers | [25] |
| Nonsmokers/Smokers with and without COPD | Induced. Sputum was centrifuged and treated as indicated above (see ref. [24]). | 2-DE and MS | Longitudinal changes of lung function in smokers with COPD | Secreted BPIFB1 was significantly elevated in sputum of COPD patients compared with that of smokers and non-smokers | [26] |
| Non-smokers, smokers without and with moderate COPD | Induced. Sputum was centrifuged and treated as indicated above (see ref. [24]). | 2D-DIGE coupled to MS | Identification of proteins involved in COPD pathogenesis | Altered proteins, COPD-, AATD-, and IPF-specific were identified | [27,28] |
| Patients with stable-COPD and acute exacerbation | Induced. Sputum was centrifuged and supernatant used for experiments. | Luminex-based multiplex equipment | Explore the percent of patients in which COPD is principally driven by activation of the interleukin-1β signalling pathway | A 2-fold increase of five IL-1β-mediated proteins was observed in sputum of acute exacerbation patients relative to stable COPD | [32] |
| Stable COPD patients and during exacerbations | Induced. Sputum was treated with DTT, and cellular and aggregated material removed. Proteins in the supernatant were alkylated and digested with trypsin. | Nano HPLC coupled to MS | Identify the substrates of proteases and determine their activity in airways of COPD patients | Differences in activity of airway elastase and processing of specific elastase substrates during stable disease and in the phase of exacerbation. | [33] |
| Patients with COPD and asthma | Induced. Sputum was centrifuged and petides contained in the supernatant identified by MS. | MALDI-TOF MS platform | Elucidate the mechanisms underlying the pathobiology of COPD and asthma | Peptide profiles allowed to differentiate COPD from asthma | [9,11,12,35] |
| Healthy controls, COPD, asthma, and COVID-19 patients | Spontaneous/induced. Sputum was diluted in PBS, centrifuged and proteins reduced with DTT followed by alkylation and digestion with trypsin. | UPLC-MS/MS | Finding of differentially expressed proteins specific to each group of patients | Proteomic changes specific for COVID-19 patients and different from those related to COPD and asthma | [36,37] |
| Subjects Investigated | Method of Sputum Collection and Processing | Proteomic Technique Applied | Target of the Rersearch | Finding | Reference # |
|---|---|---|---|---|---|
| Patients with controlled asthma and severe uncontrolled asthma | Induced. Sputum was centrifuged and loaded on 2-DE. | 2 DE coupled to MALDI-TOF | Identifying biomarkers to differentiate the two conditions | S100 calcium binding protein A9 was considered a potential biomarker of neutrophilic inflammation in severe UA | [38] |
| Non-smokers; healthy non-smokers; ex-smokers and current smokers | Induced. Sputum plugs were separated into cells and supernatant. This latter was submitted to MS analysis. | LC-MS | Define severe asthma molecular phenotypes | The differentially expressed proteins identified allowed to distinguish current smokers from ex-smokers | [39] |
| Patients with moderate-to-severe asthma | Induced. Sputum plugs were selected and liquefied with DTT.Transcriptomic analysis was performed on extracted RNA from sputum cells derived from cell pellets | Affymetrix HT HG-U133 + PM GeneChip | Stratify patients into clusters | Four clusters were identified that showed significant differences in sputum proteomics and transcriptomics | [40] |
| Asthmatic patients | Induced. Sputum was treated with DTT, and cellular and aggregated material removed by centrifugation. Proteins in the supernatant were alkylated and digested with trypsin. | LC-MS | Patient stratification | Patients were stratified in 10 clusters representing 3 sub phenotypes of asthma: highly eosinophilic, highly neutrophilic, and highly atopic with relatively low granulocytic inflammation | [41] |
| Mild/moderate asthmatics, healthy controls and of a subset of severe asthmatics | Induced sputum was acquired and processed DTE as a mucolytic to obtain supernatant for mass spectrometric analysis. | LC-MS | Identify proteins associated with Gastro-oesophageal reflux disease (GORD) in asthmatic patients | GORD was three- and ten-fold more prevalent in severe asthmatics compared to mild/moderate asthmatics and healthy controls | [42] |
| Subjects Investigated | Method of Sputum Collection and processing | Proteomic Technique Applied | Target of the Rersearch | Finding | Reference # |
|---|---|---|---|---|---|
| Exacerbated CF subjects, clinically stable CF children, and control subjects | Induced sputum was solubilized in the presence of a protease inhibitor cocktail to prevent proteolytic degradation and submtted to 2-DE. | 2-DE coupled to MALDI-TOF MS | Comparison of sputum proteins among groups and capture of antigens from complex proteomes of sputum | Changes in protein profiles and expression were observed as markers of disease progression | [43,44] |
| Healthy subjects and patients with asthma, COPD, CF, and bronchiectasis | Induced. Sputum plugs were selected and processed with DTE after which PBS was added. Samples were filtered and centrifuged to remove the cells. Supernatants were submitted to MS analysis. | SELDI-TOF MS | Identification of potential biomarkers of suppurative and inflammatory lung disease | Potential biomarkers that differentiated each of the disease groups from healthy controls were identified | [45] |
| CF patients | Spontaneous.Sputum was homogenized in PBS with the addition of EDTA and of a protease inhibitor cocktail and split in aliquots for analysis. | 2-DE coupled to MS/MS | Insight into the pathophysiology of the microbial community in lungs of CF patients | An important basis for future investigations on the physiology of microbial pathogens in CF in vivo | [46] |
| Healthy subjects and CF adults chronically infected with P. aeruginosa | Induced. The cell population was harvested from mucus plugs, washed and proteins extracted and treated as above indicated (see ref. [41]). | MudPIT platform | Identification of sputum cellular proteins | The CF proteome was largely distinct from that of healthy subjects | [47] |
| CF patients | Spontaneously expectorated sputum was homogenized by mixing with PBS containing DTE. The homogenate was digested with trypsin and submitted to analysis. | LC-MS/MS | Study of the P. aeruginosa physiology | Development of future treatment strategies aimed at altering PA physiology in vivo | [48] |
| CF patients | Spontaneous. Sputum plugs were washed and soluble proteins isolated. | 1-DE and MS | Comparison of Several PA isolates from CF patients’ sputum | In a conventional medium, PAO1 expressed numerous proteins that were absent in the CF isolates | [49] |
| Subjects Investigated | Method of Sputum Collection and Processing | Proteomic Technique Applied | Target of the Rersearch | Finding | Reference # |
|---|---|---|---|---|---|
| Lung cancer patients and healthy controls | Induced. Sputum was centrifuged and supernatant diluted with PBS and filtered. Supernatant was submitted to 1-DE. | 1-DE coupled to MS | Identification of proteins involved in lung cancer | The expression level of five proteins was higher in sputum of cancer patients compared to controls | [50] |
| Lung cancer patients and healthy controls | Spontaneous/induced. Diluted with normal saline and centrifuged to separate pellet from supernatant. This latter was collected and separate aliquots were saved for measurements. | ELISA assay | Establish a new diagnostic and prognostic biomarker for lung cancer | A significant increase in the level of MMP-2 was observed in the sputum of metastatic compared to the non-metastatic group | [51] |
| Smokers, subjects exposed to asbestos, and lung cancer patients | Induced sputum was centrifuged and potential cancer biomarkers identified in supernatant. | 2D-DIGE coupled to LC-MS/MS | Detect protein abundance differences in the proteome of induced sputum obtained from different groups | Five proteins, four of which associated to lung cancer (PRDX2, TXN, GAPDH and S100A8), have been validated | [52] |
| Lung cancer patients | Spontaneous. DTT was added and pellet and supernatant were separated by centrifugation. Supernatant was filtered, concentrated and submitted to electrophoresis. | 1-DE followed by nano LC-MS/MS | Identification of patients who are most likely to respond to platinum-based lung cancer chemotherapies | UDP-glucose glycoprotein glucosyltransferase 1 and collagen chain alpha-1 (VI) were best biomarker candidates for sensitivity to cisplatin | [53] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Amato, M.; Iadarola, P.; Viglio, S. Proteomic Analysis of Human Sputum for the Diagnosis of Lung Disorders: Where Are We Today? Int. J. Mol. Sci. 2022, 23, 5692. https://doi.org/10.3390/ijms23105692
D’Amato M, Iadarola P, Viglio S. Proteomic Analysis of Human Sputum for the Diagnosis of Lung Disorders: Where Are We Today? International Journal of Molecular Sciences. 2022; 23(10):5692. https://doi.org/10.3390/ijms23105692
Chicago/Turabian StyleD’Amato, Maura, Paolo Iadarola, and Simona Viglio. 2022. "Proteomic Analysis of Human Sputum for the Diagnosis of Lung Disorders: Where Are We Today?" International Journal of Molecular Sciences 23, no. 10: 5692. https://doi.org/10.3390/ijms23105692
APA StyleD’Amato, M., Iadarola, P., & Viglio, S. (2022). Proteomic Analysis of Human Sputum for the Diagnosis of Lung Disorders: Where Are We Today? International Journal of Molecular Sciences, 23(10), 5692. https://doi.org/10.3390/ijms23105692