
Evaluation of the Usability of a Low-Cost 3D Printer in a Tissue Engineering Approach for External Ear Reconstruction

 ,
,
Abstract
:1. Introduction
2. Results
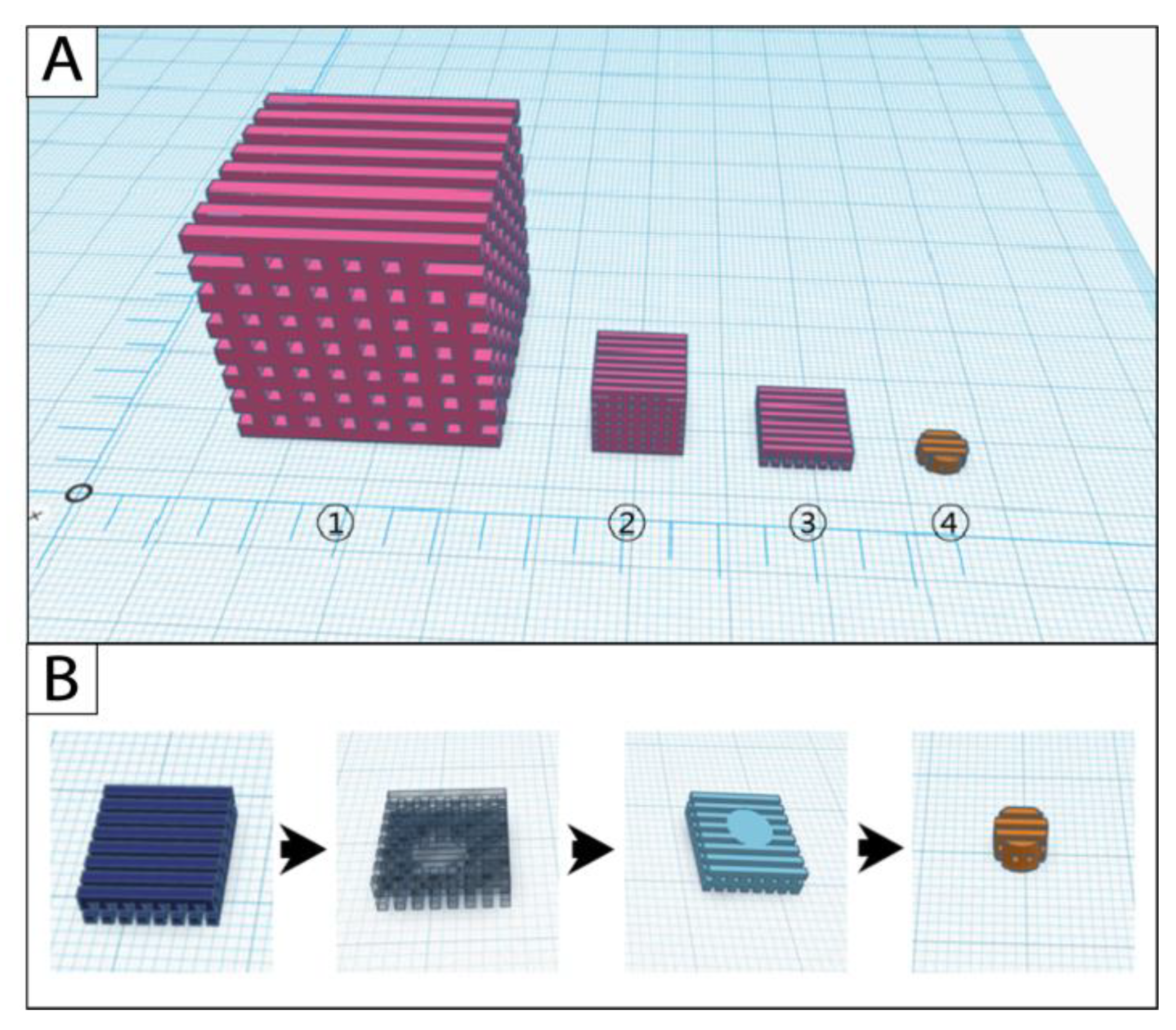
2.1. Scaffold Modifications during the CAD-CAM Process
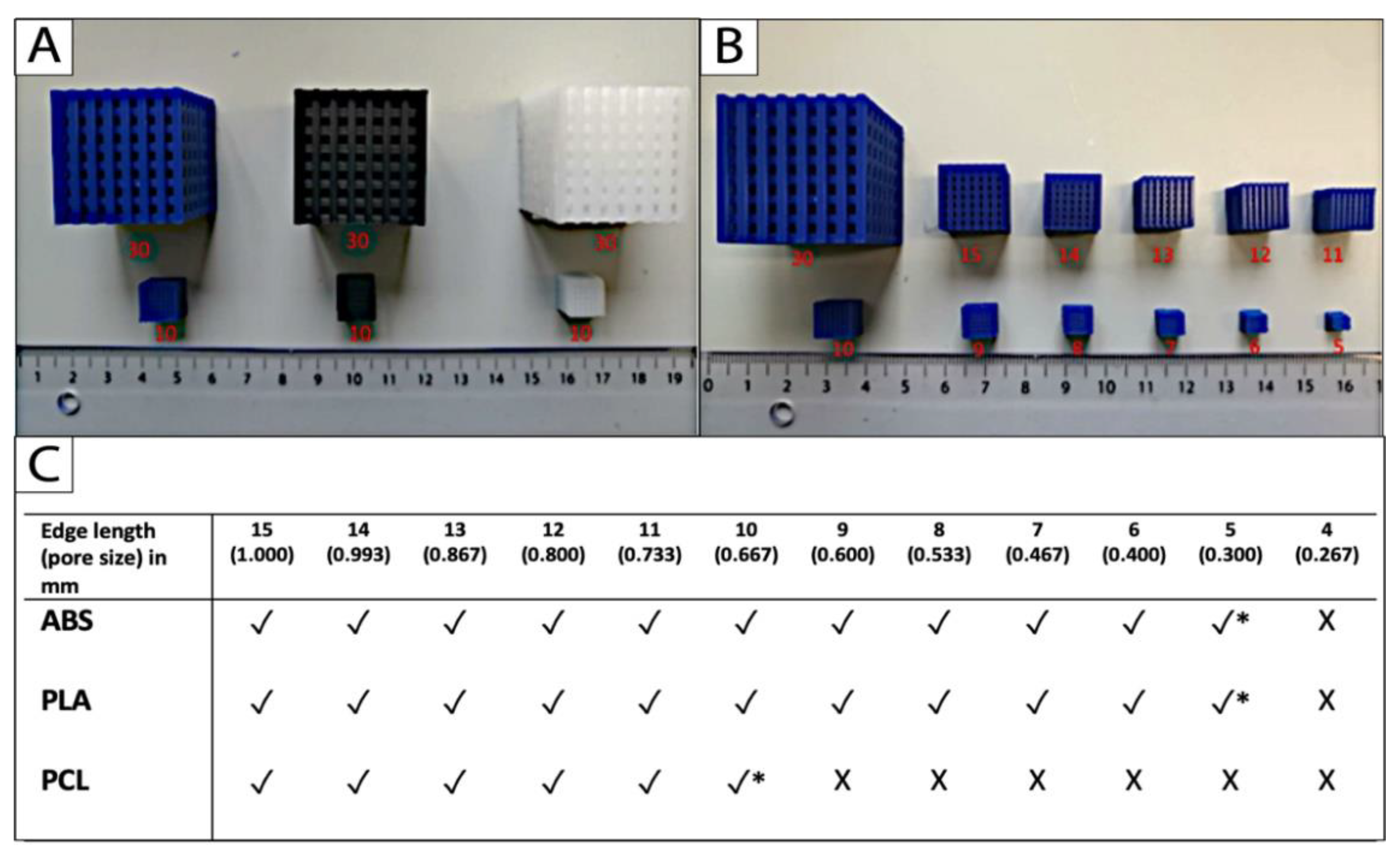
2.2. Limit Test
2.3. Micro- and Macrodimensions of the Porous Scaffolds
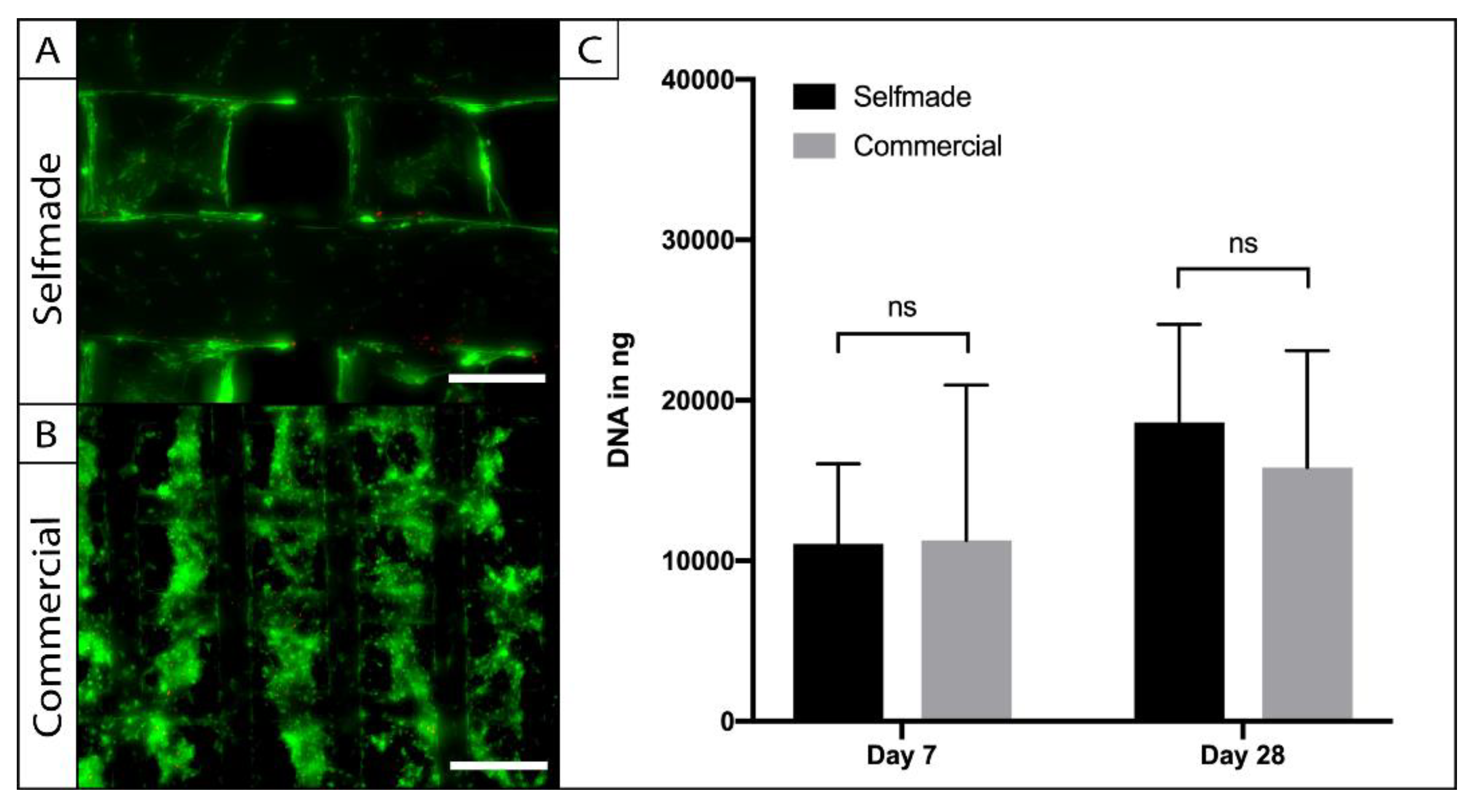
2.4. Biocompatibility of the Self-Made in Comparison to the Commercially Available Scaffold
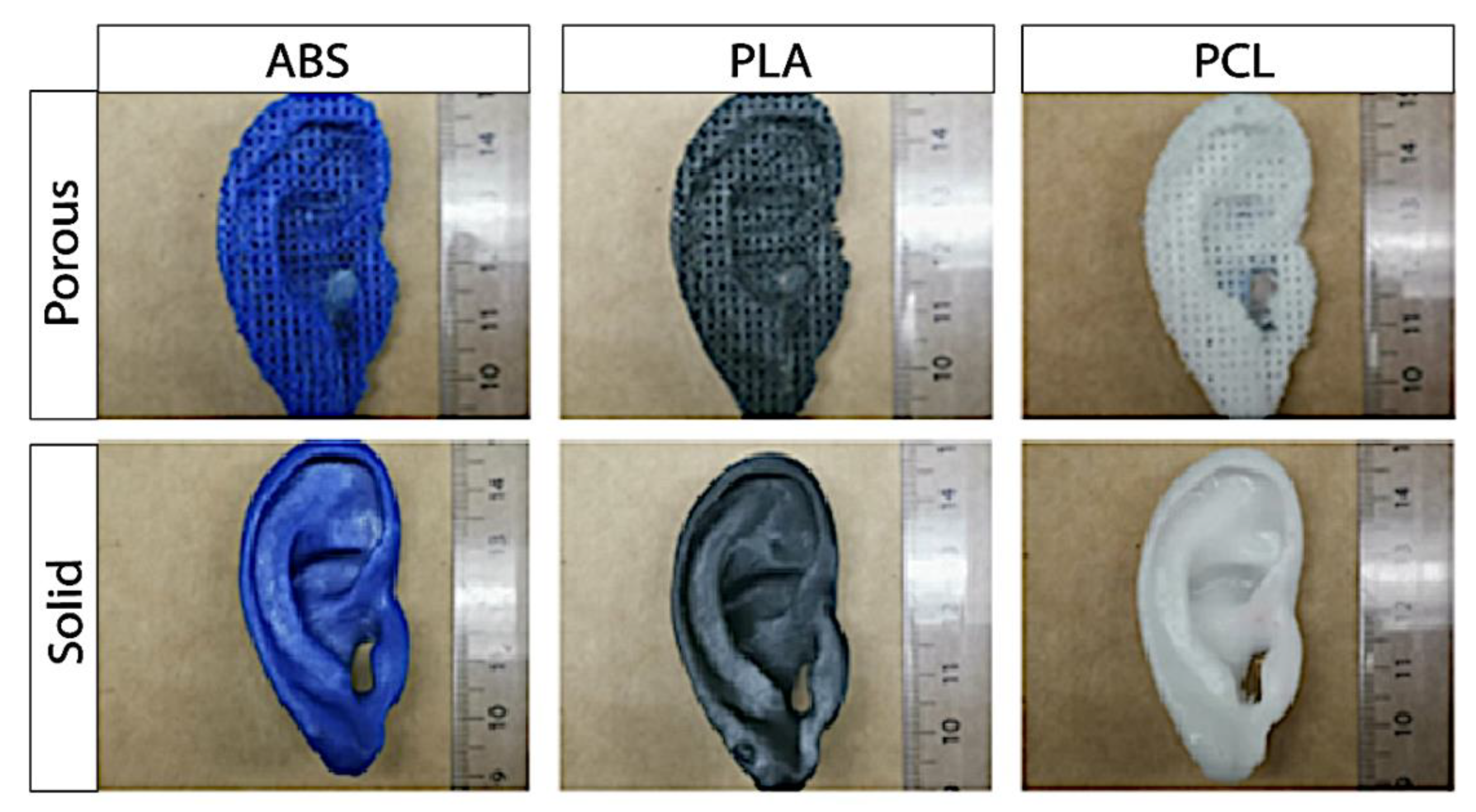
2.5. Porous Auricular Constructs
2.6. Solid Auricular Constructs
3. Discussion
4. Materials and Methods
4.1. Computer-Assisted Design (CAD) of the Scaffold
4.2. Computer-Assisted Manufacturing (CAM) of the Scaffold
4.3. Uniform Scaling and Limit Test
4.4. Evaluation of The Macro- and Microdimensions of the Cube Scaffolds
4.5. In Vitro Cultivation with Human Adipose-Tissue Derived Stem Cells (ASCs)
4.6. Testing for Biocompatibility
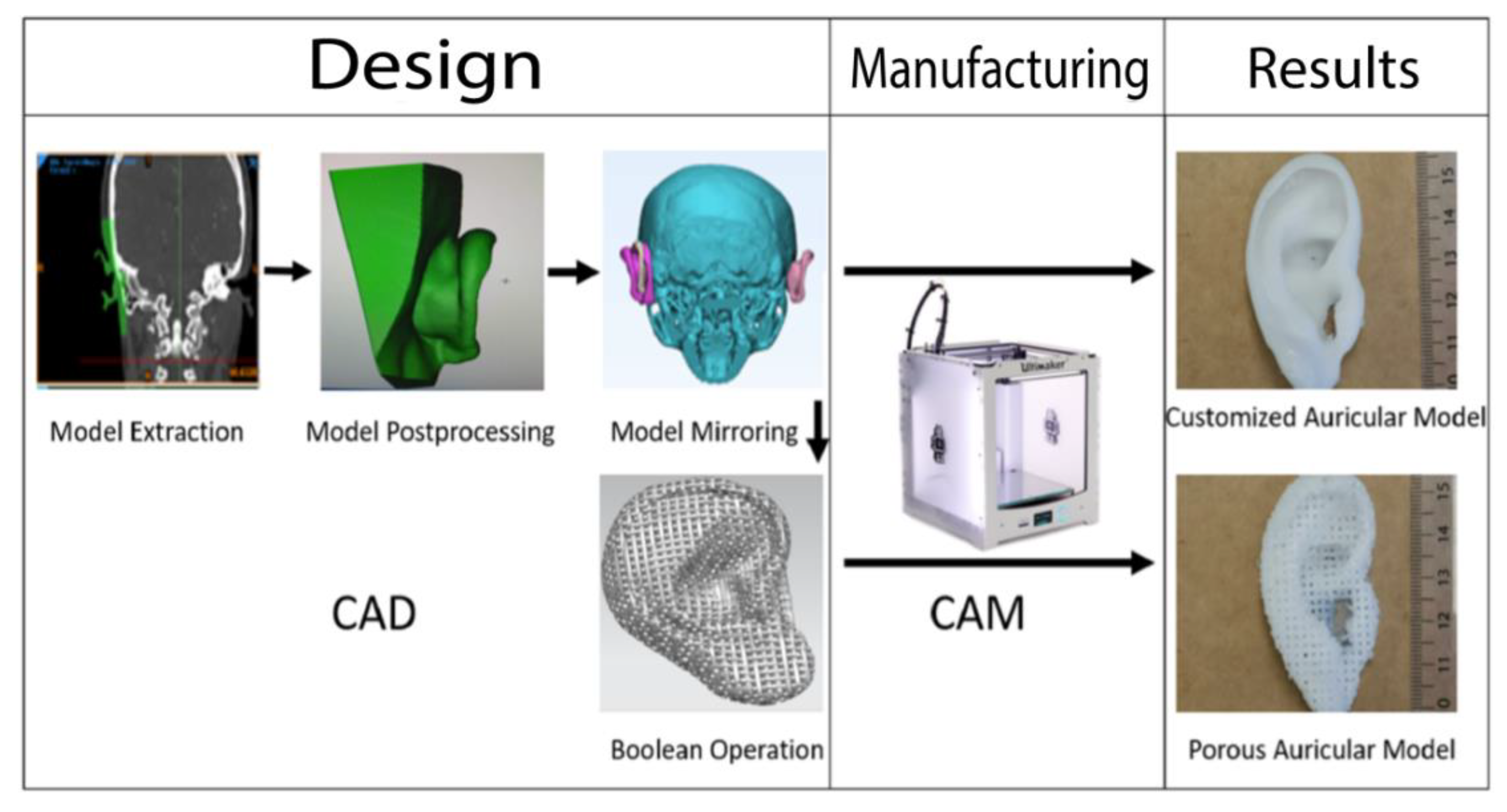
4.7. Computer-Assisted Design (CAD) of Customized Porous and Solid Auricular Constructs
4.8. Evaluation of the Macro- and Microdimensions of the Auricular Constructs
4.9. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Denadai, R.; Raposo-Amaral, C.E.; Zanco, G.L.; Raposo-Amaral, C.A. Autologous Ear Reconstruction for Microtia Does Not Result in Loss of Cutaneous Sensitivity. Plast. Reconstr. Surg. 2019, 143, 808e–819e. [Google Scholar] [CrossRef]
- Firmin, F.; Sänger, C.; O‘Toole, G. Ear reconstruction following severe complications of otoplasty. J. Plast. Reconstr. Aesthetic Surg. 2008, 61, S13–S20. [Google Scholar] [CrossRef] [PubMed]
- Nagata, S. A New Method of Total Reconstruction of the Auricle for Microtia. Plast. Reconstr. Surg. 1993, 92, 187–201. [Google Scholar] [CrossRef] [PubMed]
- Kasrai, L.; Snyder-Warwick, A.K.; Fisher, D.M. Single-Stage Autologous Ear Reconstruction for Microtia. Plast. Reconstr. Surg. 2014, 133, 652–662. [Google Scholar] [CrossRef] [PubMed]
- Ohara, K.; Nakamura, K.; Ohta, E. Chest Wall Deformities and Thoracic Scoliosis after Costal Cartilage Graft Harvesting. Plast. Reconstr. Surg. 1997, 99, 1030–1036. [Google Scholar] [CrossRef] [PubMed]
- Wiggenhauser, P.S.; Schantz, J.T.; Rotter, N. Cartilage engineering in reconstructive surgery: Auricular, nasal and tracheal engineering from a surgical perspective. Regen. Med. 2017, 12, 303–314. [Google Scholar] [CrossRef]
- Long, X.; Yu, N.; Huang, J.; Wang, X. Complication Rate of Autologous Cartilage Microtia Reconstruction: A systematic review. Plast. Reconstr. Surg.—Glob. Open 2013, 1, e57. [Google Scholar] [CrossRef]
- Ladani, P.S.; Valand, R.; Sailer, H. Ear Reconstruction Using Autologus Costal Cartilage: A Steep Learning Curve. J. Maxillofac. Oral Surg. 2018, 18, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Chin, W.; Zhang, R.; Zhang, Q.; Xu, Z.; Li, D.; Wu, J. Modifications of Three-Dimensional Costal Cartilage Framework Grafting in Auricular Reconstruction for Microtia. Plast. Reconstr. Surg. 2009, 124, 1940–1946. [Google Scholar] [CrossRef]
- Mussi, E.; Furferi, R.; Volpe, Y.; Facchini, F.; McGreevy, K.S.; Uccheddu, F. Ear Reconstruction Simulation: From Handcrafting to 3D Printing. Bioengineering 2019, 6, 14. [Google Scholar] [CrossRef] [Green Version]
- Nayyer, L.; Patel, K.H.; Esmaeili, A.; Rippel, R.A.; Birchall, M.; O‘toole, G.; Butler, P.E.; Seifalian, A.M. Tissue Engineering: Revolution and challenge in auricular cartilage reconstruction. Plast. Reconstr. Surg. 2012, 129, 1123–1137. [Google Scholar] [CrossRef] [PubMed]
- Ha, J.F.; Morrison, R.J.; Green, G.E.; Zopf, D.A. Computer-Aided Design and 3-Dimensional Printing for Costal Cartilage Simulation of Airway Graft Carving. Otolaryngol.—Head Neck Surg. (USA) 2017, 156, 1044–1047. [Google Scholar] [CrossRef] [PubMed]
- Melchels, F.; Wiggenhauser, P.S.; Warne, D.; Barry, M.; Ong, F.R.; Chong, W.S.; Hutmacher, D.W.; Schantz, J.-T. CAD/CAM-assisted breast reconstruction. Biofabrication 2011, 3, 034114. [Google Scholar] [CrossRef] [Green Version]
- Hutmacher, D.W.; Schantz, T.; Zein, I.; Ng, K.W.; Teoh, S.H.; Tan, K.C. Mechanical properties and cell cultural response of polycaprolactone scaffolds designed and fabricated via fused deposition modeling. J. Biomed. Mater. Res. 2001, 55, 203–216. [Google Scholar] [CrossRef]
- Zein, I.; Hutmacher, D.W.; Tan, K.C.; Teoh, S.H. Fused deposition modeling of novel scaffold architectures for tissue engineering applications. Biomaterials 2001, 23, 1169–1185. [Google Scholar] [CrossRef]
- Rosenzweig, D.H.; Carelli, E.; Steffen, T.; Jarzem, P.; Haglund, L. 3D-Printed ABS and PLA Scaffolds for Cartilage and Nucleus Pulposus Tissue Regeneration. Int. J. Mol. Sci. 2015, 16, 15118–15135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siddiqui, N.; Asawa, S.; Birru, B.; Baadhe, R.; Rao, S. PCL-Based Composite Scaffold Matrices for Tissue Engineering Applications. Mol. Biotechnol. 2018, 60, 506–532. [Google Scholar] [CrossRef]
- Labet, M.; Thielemans, W. Synthesis of polycaprolactone: A review. Chem. Soc. Rev. 2009, 38, 3484–3504. [Google Scholar] [CrossRef]
- Wiggenhauser, P.S.; Schwarz, S.; Koerber, L.; Hoffmann, T.K.; Rotter, N. Addition of decellularized extracellular matrix of porcine nasal cartilage improves cartilage regenerative capacities of PCL-based scaffolds in vitro. J. Mater. Sci. Mater. Med. 2019, 30, 121. [Google Scholar] [CrossRef]
- Wiggenhauser, P.S.; Balmayor, E.R.; Rotter, N.; Schantz, J.T. In vivo evaluation of a regenerative approach to nasal dorsum augmentation with a polycaprolactone-based implant. Eur. J. Med. Res. 2019, 24, 6. [Google Scholar] [CrossRef]
- Olubamiji, A.D.; Izadifar, Z.; Si, J.L.; Cooper, D.M.L.; Eames, B.F.; Chen, X. Modulating mechanical behaviour of 3D-printed cartilage-mimetic PCL scaffolds: Influence of molecular weight and pore geometry. Biofabrication 2016, 8, 025020. [Google Scholar] [CrossRef]
- Theodoridis, K.; Aggelidou, E.; Vavilis, T.; Manthou, M.E.; Tsimponis, A.; Demiri, E.C.; Boukla, A.; Salpistis, C.; Bakopoulou, A.; Mihailidis, A.; et al. Hyaline cartilage next generation implants from adipose-tissue-derived mesenchymal stem cells: Comparative study on 3D-printed polycaprolactone scaffold patterns. J. Tissue Eng. Regen. Med. 2019, 13, 342–355. [Google Scholar] [CrossRef] [PubMed]
- Kuhlmann, C.; Schenck, T.L.; Tluczynski, K.; Aszodi, A.; Metzger, P.; Giunta, R.; Paul, I.; Wiggenhauser, P.S. Experimental approach to nasal septal cartilage regeneration with adipose tissue-derived stem cells and decellularized porcine septal cartilage. Xenotransplantation 2020, 28, e12660. [Google Scholar] [CrossRef]
- Bekisz, J.M.; Liss, H.A.; Maliha, S.G.; Witek, L.; Coelho, P.G.; Flores, R.L. In-House Manufacture of Sterilizable, Scaled, Patient-Specific 3D-Printed Models for Rhinoplasty. Aesthetic Surg. J. 2018, 39, 254–263. [Google Scholar] [CrossRef] [PubMed]
- Patrício, T.; Domingos, M.; Gloria, A.; D’Amora, U.; Coelho, J.; Bartolo, P. Fabrication and characterisation of PCL and PCL/PLA scaffolds for tissue engineering. Rapid Prototyp. J. 2014, 20, 145–156. [Google Scholar] [CrossRef]
- Zuniga, J.; Katsavelis, D.; Peck, J.; Stollberg, J.; Petrykowski, M.; Carson, A.; Fernandez, C. Cyborg beast: A low-cost 3d-printed prosthetic hand for children with upper-limb differences. BMC Res. Notes 2015, 8, 10. [Google Scholar] [CrossRef] [Green Version]
- Lim, D.; Georgiou, T.; Bhardwaj, A.; O’Connell, G.D.; Agogino, A.M. Customization of a 3D Printed Prosthetic Finger Using Parametric Modeling. In International Design Engineering Technical Conferences and Computers and Information in Engineering Conference; ASME: New York, NY, USA, 2018. [Google Scholar] [CrossRef]
- Blum, J.C.; Schenck, T.L.; Birt, A.; Giunta, R.E.; Wiggenhauser, P.S. Artificial decellularized extracellular matrix improves the regenerative capacity of adipose tissue derived stem cells on 3D printed polycaprolactone scaffolds. J. Tissue Eng. 2021, 12. [Google Scholar] [CrossRef]
- Aigner, T.; Stöve, J. Collagens—Major component of the physiological cartilage matrix, major target of cartilage degeneration, major tool in cartilage repair. Adv. Drug Deliv. Rev. 2003, 55, 1569–1593. [Google Scholar] [CrossRef] [PubMed]
- Nehrer, S.; Breinan, H.A.; Ramappa, A.; Young, G.; Shortkroff, S.; Louie, L.K.; Sledge, C.B.; Yannas, I.V.; Spector, M. Matrix collagen type and pore size influence behaviour of seeded canine chondrocytes. Biomaterials 1997, 18, 769–776. [Google Scholar] [CrossRef]
- Schwarz, S.; Elsaesser, A.F.; Koerber, L.; Goldberg-Bockhorn, E.; Seitz, A.M.; Bermueller, C.; Dürselen, L.; Ignatius, A.; Breiter, R.; Rotter, N. Processed xenogenic cartilage as innovative biomatrix for cartilage tissue engineering: Effects on chondrocyte differentiation and function. J. Tissue Eng. Regen. Med. 2015, 9, E239–E251. [Google Scholar] [CrossRef] [PubMed]
- Kemppainen, J.M.; Hollister, S.J. Differential effects of designed scaffold permeability on chondrogenesis by chondrocytes and bone marrow stromal cells. Biomaterials 2010, 31, 279–287. [Google Scholar] [CrossRef]
- Kuhlmann, C.; Schenck, T.L.; Aszodi, A.; Giunta, R.E.; Wiggenhauser, P.S. Zone-Dependent Architecture and Biochemical Composition of Decellularized Porcine Nasal Cartilage Modulate the Activity of Adipose Tissue-Derived Stem Cells in Cartilage Regeneration. Int. J. Mol. Sci. 2021, 22, 9917. [Google Scholar] [CrossRef] [PubMed]
- Im, G.-I.; Ko, J.-Y.; Lee, J.H. Chondrogenesis of Adipose Stem Cells in a Porous Polymer Scaffold: Influence of the Pore Size. Cell Transplant. 2012, 21, 2397–2405. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.H.; Kim, T.H.; Im, G.I.; Lee, J.H. Investigation of Pore Size Effect on Chondrogenic Differentiation of Adipose Stem Cells Using a Pore Size Gradient Scaffold–Biomacromolecules (ACS Publications). Biomacromolecules 2010, 11, 1948–1955. [Google Scholar] [CrossRef] [PubMed]
- Hatz, C.R.; Msallem, B.; Aghlmandi, S.; Brantner, P.; Thieringer, F.M. Can an entry-level 3D printer create high-quality anatomical models? Accuracy assessment of mandibular models printed by a desktop 3D printer and a professional device. Int. J. Oral Maxillofac. Surg. 2020, 49, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Wise, J.K.; Yarin, A.L.; Megaridis, C.M.; Cho, M. Chondrogenic Differentiation of Human Mesenchymal Stem Cells on Oriented Nanofibrous Scaffolds: Engineering the Superficial Zone of Articular Cartilage. Tissue Eng. Part A 2009, 15, 913–921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassan, W.N.W.; Yusoff, Y.; Mardi, N.A. Comparison of reconstructed rapid prototyping models produced by 3-dimensional printing and conventional stone models with different degrees of crowding. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 209–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.-Y.; Ng, L.-S.; Chang, C.-S.; Lu, T.-C.; Chen, N.-H.; Chen, Z.-C. Pursuing Mirror Image Reconstruction in Unilateral Microtia: Customizing Auricular Framework by Application of Three-Dimensional Imaging and Three-Dimensional Printing. Plast. Reconstr. Surg. 2017, 139, 1433–1443. [Google Scholar] [CrossRef] [PubMed]
- Otto, I.A.; Melchels, F.P.W.; Zhao, X.; Randolph, M.A.; Kon, M.; Breugem, C.C.; Malda, J. Auricular reconstruction using biofabrication-based tissue engineering strategies. Biofabrication 2015, 7, 032001. [Google Scholar] [CrossRef]
- Zhou, G.; Jiang, H.; Yin, Z.; Liu, Y.; Zhang, Q.; Zhang, C.; Pan, B.; Zhou, J.; Zhou, X.; Sun, H.; et al. In Vitro Regeneration of Patient-specific Ear-shaped Cartilage and Its First Clinical Application for Auricular Reconstruction. EBioMedicine 2018, 28, 287–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farkas, L.G.; Posnick, J.C.; Hreczko, T.M. Anthropometric Growth Study of the Ear. Cleft Palate-Craniofacial J. 1992, 29, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Modabber, A.; Galster, H.; Peters, F.; Möhlhenrich, S.C.; Kniha, K.; Knobe, M.; Hölzle, F.; Ghassemi, A. Three-Dimensional Analysis of the Ear Morphology. Aesthetic Plast. Surg. 2018, 42, 766–773. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.Y.; Jung, S.Y.; Lee, S.J.; Lee, H.J.; Truong, M.-D.; Kim, H.S. Fabrication and characterization of 3D-printed elastic auricular scaffolds: A pilot study. Laryngoscope 2019, 129, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Demoor, M.; Ollitrault, D.; Gomez-Leduc, T.; Bouyoucef, M.; Hervieu, M.; Fabre, H.; Lafont, J.; Denoix, J.-M.; Audigié, F.; Mallein-Gerin, F.; et al. Cartilage tissue engineering: Molecular control of chondrocyte differentiation for proper cartilage matrix reconstruction. Biochim. Biophys. Acta—Gen. Subj. 2014, 1840, 2414–2440. [Google Scholar] [CrossRef]
- Adachi, T.; Osako, Y.; Tanaka, M.; Hojo, M.; Hollister, S.J. Framework for optimal design of porous scaffold microstructure by computational simulation of bone regeneration. Biomaterials 2006, 27, 3964–3972. [Google Scholar] [CrossRef]
- Lee, D.J.; Kwon, J.; Kim, Y.-I.; Kwon, Y.H.; Min, S.; Shin, H.W. Coating Medpor® Implant with Tissue-Engineered Elastic Cartilage. J. Funct. Biomater. 2020, 11, 34. [Google Scholar] [CrossRef]
- Park, Y.J.; Cha, J.H.; Bang, S.I.; Kim, S.Y. Clinical Application of Three-Dimensionally Printed Biomaterial Polycaprolactone (PCL) in Augmentation Rhinoplasty. Aesthetic Plast. Surg. 2018, 43, 437–446. [Google Scholar] [CrossRef]
- Park, S.H.; Yun, B.G.; Won, J.Y.; Yun, W.S.; Shim, J.H.; Lim, M.H.; Kim, D.H.; Baek, S.A.; AlAhmari, Y.D.; Jeun, J.H.; et al. New application of three-dimensional printing biomaterial in nasal reconstruction. Laryngoscope 2016, 127, 1036–1043. [Google Scholar] [CrossRef] [PubMed]
- Schantz, J.-T.; Teoh, S.H.; Lim, T.C.; Endres, M.; Lam, C.X.F.; Hutmacher, D.W. Repair of Calvarial Defects with Customized Tissue-Engineered Bone Grafts, I. Evaluation of Osteogenesis in a Three-Dimensional Culture System. Tissue Eng. 2003, 9 (Suppl. 1), S113–S126. [Google Scholar] [CrossRef] [PubMed]
- De Moraes Ferreira, A.C.R.; Muñoz, X.M.J.P.; Okamoto, R.; Pellizer, E.P.; Garcia, I.R. Postoperative Complications in Craniomaxillofacial Reconstruction with Medpor. J. Craniofacial Surg. 2016, 27, 425–428. [Google Scholar] [CrossRef]
- Zammit, D.; Safran, T.; Ponnudurai, N.; Jaberi, M.; Chen, L.; Noel, G.; Gilardino, M.S. Step-Specific Simulation: The Utility of 3D Printing for the Fabrication of a Low-Cost, Learning Needs-Based Rhinoplasty Simulator. Aesthetic Surg. J. 2020, 40, NP340–NP345. [Google Scholar] [CrossRef] [PubMed]
- Ganguli, A.; Pagan-Diaz, G.J.; Grant, L.; Cvetkovic, C.; Bramlet, M.; Vozenilek, J.; Kesavadas, T.; Bashir, R. 3D printing for preoperative planning and surgical training: A review. Biomed. Microdevices 2018, 20, 65. [Google Scholar] [CrossRef] [PubMed]
- Brouwers, L.; Teutelink, A.; Van Tilborg, F.A.J.B.; De Jongh, M.A.C.; Lansink, K.W.W.; Bemelman, M. Validation study of 3D-printed anatomical models using 2 PLA printers for preoperative planning in trauma surgery, a human cadaver study. Eur. J. Trauma Emerg. Surg. 2019, 45, 1013–1020. [Google Scholar] [CrossRef]
- Alhazmi, B.; Alshomer, F.; Alawirdhi, B. Multiscale sterilizable 3D printed auricular templates to guide cartilaginous framework sizing and sculpture during autologous microtia reconstruction. JPRAS Open 2021, 28, 121–125. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Xue, G.-H.; Fu, J.-Z. Fabrication of low cost soft tissue prostheses with the desktop 3D printer. Sci. Rep. 2014, 4, 6973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jovic, T.H.; Combellack, E.J.; Jessop, Z.M.; Whitaker, I.S. Using 3D Printing Technology to Teach Cartilage Framework Carving for Ear Reconstruction. Front. Surg. 2020, 7, 44. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Jiang, M.; Coles-Black, J.; Mansour, K.; Chuen, J.; Amott, D. Three-dimensional printing as a tool in otolaryngology training: A systematic review. J. Laryngol. Otol. 2020, 134, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Coward, T.J.; Watson, R.M.; Scott, B.J.J. Laser scanning for the identification of repeatable landmarks of the ears and face. Br. J. Plast. Surg. 1997, 50, 308–314. [Google Scholar] [CrossRef]
- Coward, T.J.; Scott, B.J.J.; Watson, R.M.; Richards, R. Laser scanning of the ear identifying the shape and position in subjects with normal facial symmetry. Int. J. Oral Maxillofac. Surg. 2000, 29, 18–23. [Google Scholar] [CrossRef]
- Witek, L.; Khouri, K.S.; Coelho, P.G.; Flores, R.L. Patient-specific 3D Models for Autogenous Ear Reconstruction. Plast. Reconstr. Surg.—Glob. Open 2016, 4, e1093. [Google Scholar] [CrossRef]
- Wiggenhauser, P.S.; Kuhlmann, C.; Blum, J.; Giunta, R.E.; Schenck, T. Influence of software parameters on measurements in automatized image-based analysis of fat tissue histology. Acta Histochem. 2020, 122, 151537. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnosis (Code) | Microtia (Q17.2) | ||
|---|---|---|---|
| Procedure | Ear reconstruction with autologous cartilage | Ear reconstruction with a self-made porous PCL implant | Ear reconstruction with a commercially available alloplastic implant |
| Surgical complexity of the procedure | High | Medium | Medium |
| CAD-CAM-assisted patient-customization | No | Yes | No |
| Donor site morbidity | Yes | No | No |
| G-DRG Procedural Code | 5–187.2 | 5–187.4 | 5–187.4 |
| Revenue (€) * | 5695.2 | 3645.3 | 3645.3 |
| Material costs/ implant (€) | 0 | 0.56 | 1161.44 (incl. VAT) ** |
| Equipment costs (€) | 0 | 2309 | 0 |
| Difference (€) | 5695.2 | 1335.7 | 2483.87 |
| Difference without equipment costs (€) | 5695.2 | 3644.74 | 2483.87 |
| Material | ABS | PLA | PCL | ANOVA | |||
|---|---|---|---|---|---|---|---|
| Dimension (mm) | Mean | SD | Mean | SD | Mean | SD | |
| Edge Length | 10.03 | 0.05 | 10.00 | 0.06 | 10.01 | 0.05 | ns |
| Height | 2.670 | 0.02 | 2.67 | 0.02 | 2.67 | 0.03 | ns |
| WRU | 0.661 | 0.01 | 0.66 | 0.01 | 0.67 | 0.01 | ns |
| Pore Size | 0.669 | 0.01 | 0.66 | 0.01 | 0.67 | 0.01 | ns |
| Material | ABS | PLA | PCL | ANOVA | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Dimension (mm) | Mean | SD | t-test | Mean | SD | t-test | Mean | SD | t-test | |
| PEL | 51.74 | 0.12 | 0.97 | 51.75 | 0.11 | 0.84 | 51.73 | 0.15 | 0.91 | ns |
| MEL | 25.46 | 0.10 | 0.86 | 25.48 | 0.11 | 0.61 | 25.43 | 0.09 | 0.64 | ns |
| PEW | 28.39 | 0.13 | 0.89 | 28.37 | 0.11 | 0.84 | 28.39 | 0.12 | 0.89 | ns |
| MEW | 31.41 | 0.11 | 0.51 | 31.39 | 0.12 | 0.89 | 31.36 | 0.12 | 0.75 | ns |
| Ear height | 12.51 | 0.12 | 0.72 | 12.49 | 0.09 | 0.93 | 12.5 | 0.08 | 0.32 | ns |
| Material | ABS | PLA | PCL | ANOVA | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Dimension (mm) | Mean | SD | t-test | Mean | SD | t-test | Mean | SD | t-test | |
| PEL | 51.73 | 0.10 | 0.84 | 51.75 | 0.11 | 0.88 | 51.72 | 0.15 | 0.77 | ns |
| MEL | 25.47 | 0.11 | 0.71 | 25.47 | 0.11 | 0.76 | 25.43 | 0.08 | 0.62 | ns |
| PEW | 28.41 | 0.12 | 0.80 | 28.37 | 0.13 | 0.58 | 28.38 | 0.11 | 0.70 | ns |
| MEW | 31.42 | 0.10 | 0.68 | 31.42 | 0.11 | 0.70 | 31.36 | 0.14 | 0.55 | ns |
| Ear height | 12.51 | 0.09 | 0.69 | 12.5 | 0.08 | 0.40 | 12.56 | 0.13 | 0.64 | ns |
| Filament Material | ABS | PLA | PCL |
|---|---|---|---|
| Company | Formfutura, Nijmegen, The Netherlands | Formfutura, Nijmegen, The Netherlands | 3D4MAKERS, Haarlem, The Netherlands |
| Color | Blue | Black | White |
| Diameter | 2.85 mm (+/− 0.05 mm) | 2.85 mm (+/− 0.05 mm) | 2.85 mm (+/− 0.05 mm) |
| Roundness | 99% | 99% | 99% |
| Density | 1.05 g/cm3 | 1.24 g/cm3 | 1.1 g/cm3 |
| Properties | Strong and durable | Easy to print | Safe, nontoxic, and biodegradable |
| Application | End-use parts and casings | Prototypes | Medical implantation |
| Printing temp. | 230–250 °C | 180–210 °C | 80–160 °C |
| Strength | High | Medium | Low |
| Flexibility | Low | Medium | High |
| Ease of printing | Medium | High | Low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuhlmann, C.; Blum, J.C.; Schenck, T.L.; Giunta, R.E.; Wiggenhauser, P.S. Evaluation of the Usability of a Low-Cost 3D Printer in a Tissue Engineering Approach for External Ear Reconstruction. Int. J. Mol. Sci. 2021, 22, 11667. https://doi.org/10.3390/ijms222111667
Kuhlmann C, Blum JC, Schenck TL, Giunta RE, Wiggenhauser PS. Evaluation of the Usability of a Low-Cost 3D Printer in a Tissue Engineering Approach for External Ear Reconstruction. International Journal of Molecular Sciences. 2021; 22(21):11667. https://doi.org/10.3390/ijms222111667
Chicago/Turabian StyleKuhlmann, Constanze, Jana C. Blum, Thilo L. Schenck, Riccardo E. Giunta, and Paul Severin Wiggenhauser. 2021. "Evaluation of the Usability of a Low-Cost 3D Printer in a Tissue Engineering Approach for External Ear Reconstruction" International Journal of Molecular Sciences 22, no. 21: 11667. https://doi.org/10.3390/ijms222111667
APA StyleKuhlmann, C., Blum, J. C., Schenck, T. L., Giunta, R. E., & Wiggenhauser, P. S. (2021). Evaluation of the Usability of a Low-Cost 3D Printer in a Tissue Engineering Approach for External Ear Reconstruction. International Journal of Molecular Sciences, 22(21), 11667. https://doi.org/10.3390/ijms222111667