Combination Drug Therapy for the Management of Alzheimer’s Disease
 , , ,
, , ,  ,
, 

 ,
,  and
and 
Abstract
1. Introduction
2. Widely Studied Combination Therapies for Alzheimer’s Disease
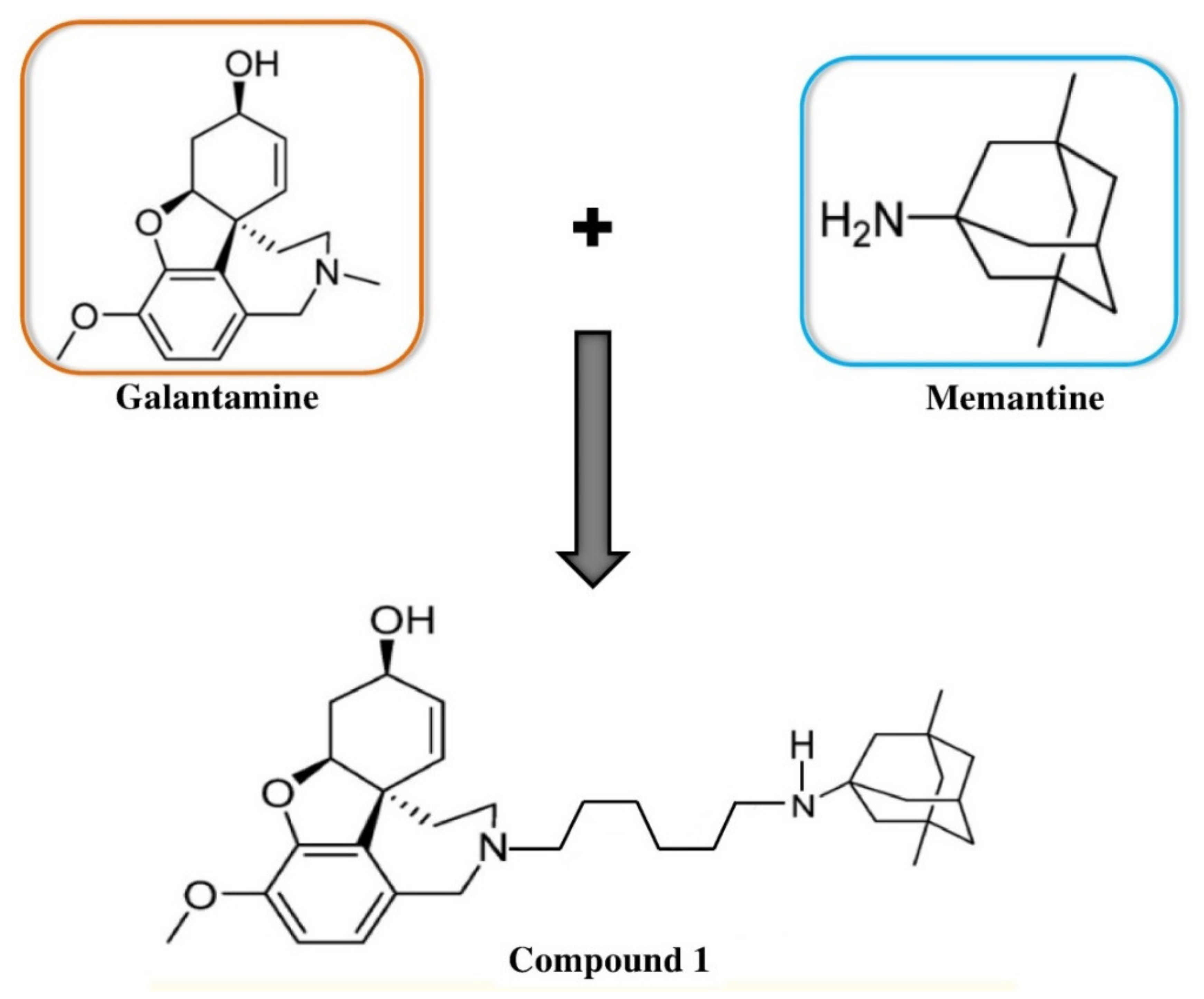
2.1. Combination of Galantamine and Memantine
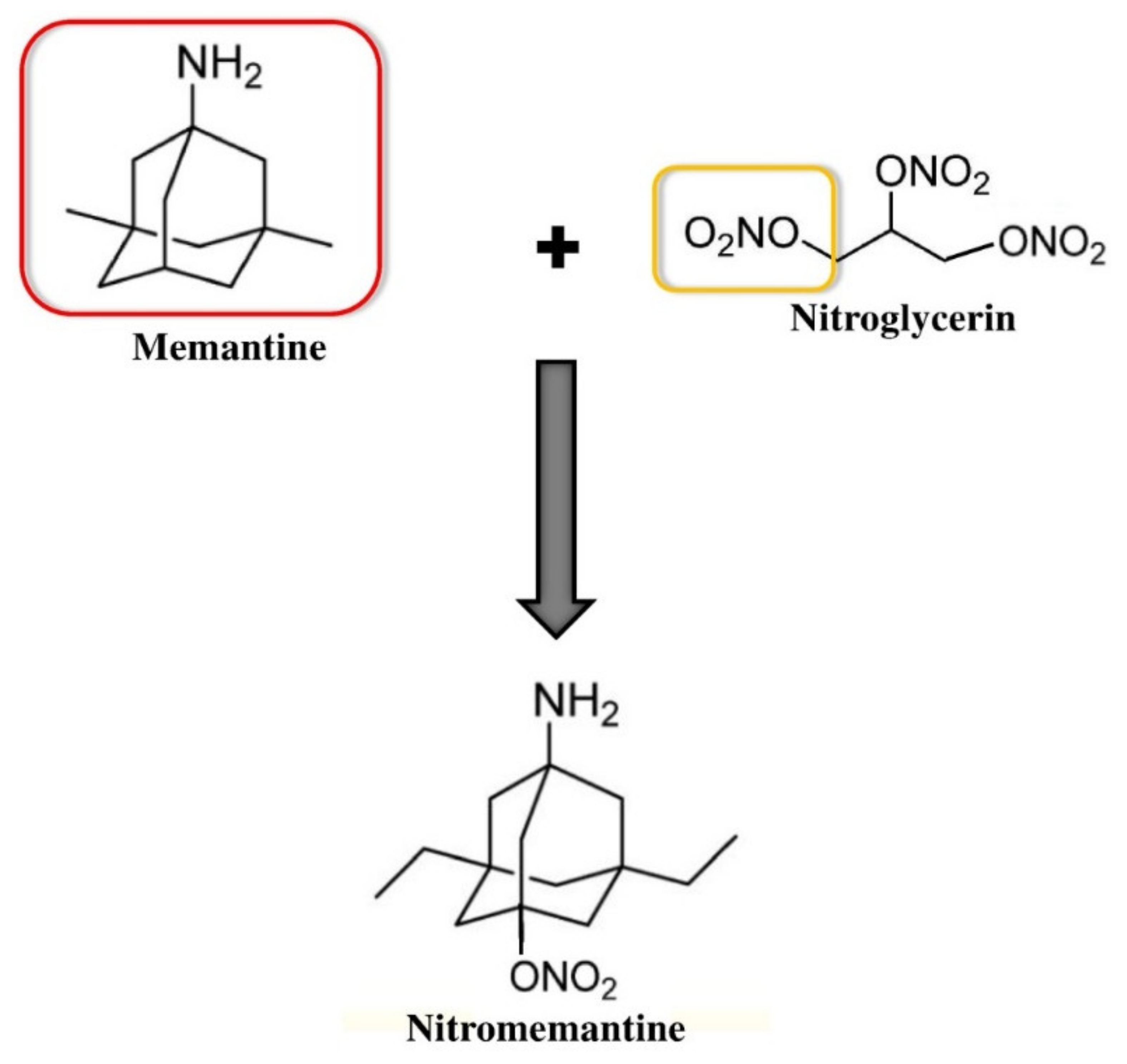
2.2. Combination of Memantine and Nitroglycerin
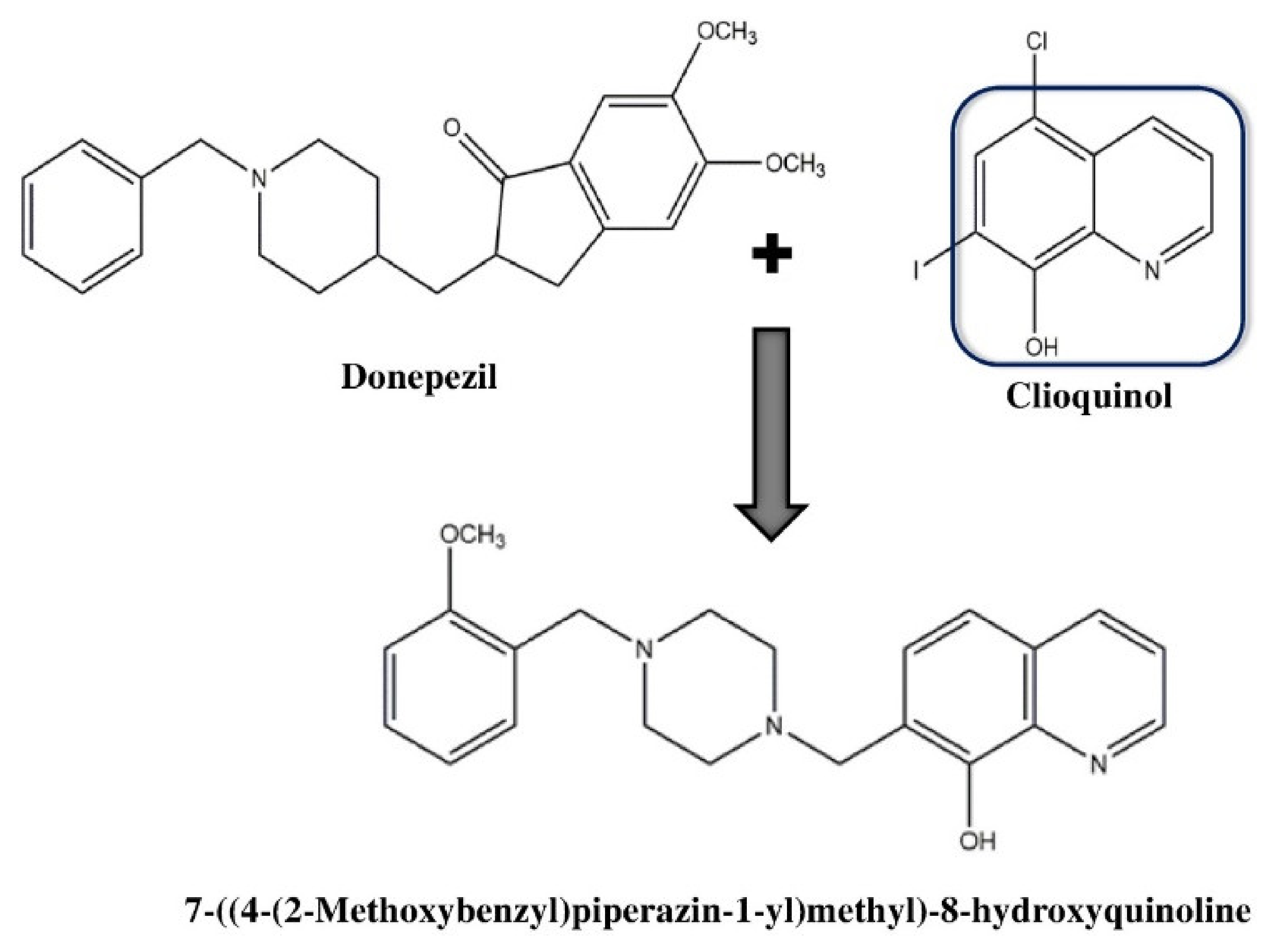
2.3. Combination of Donepezil and Clioquinol
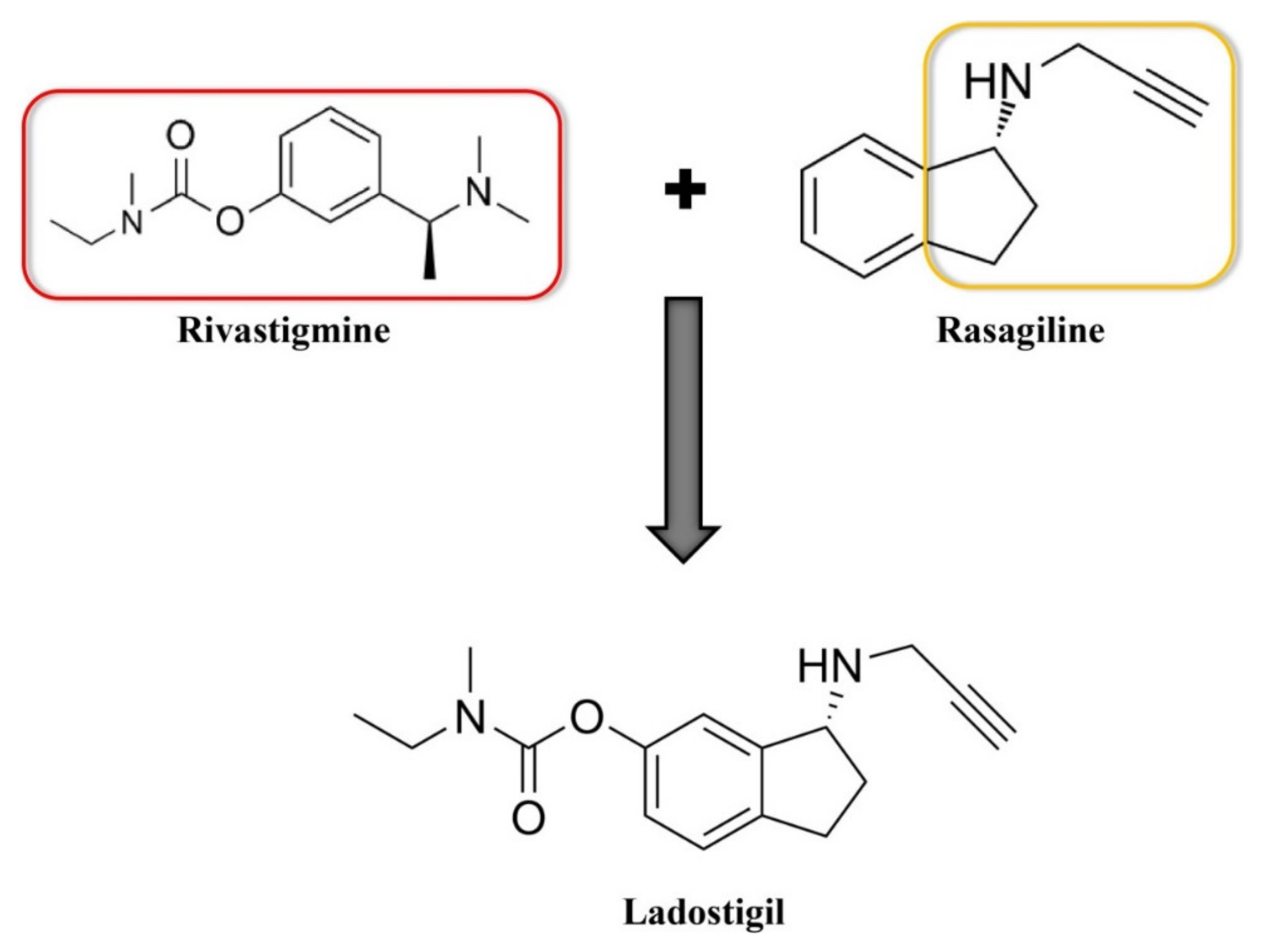
2.4. Combination of Rivastigmine and Rasagiline
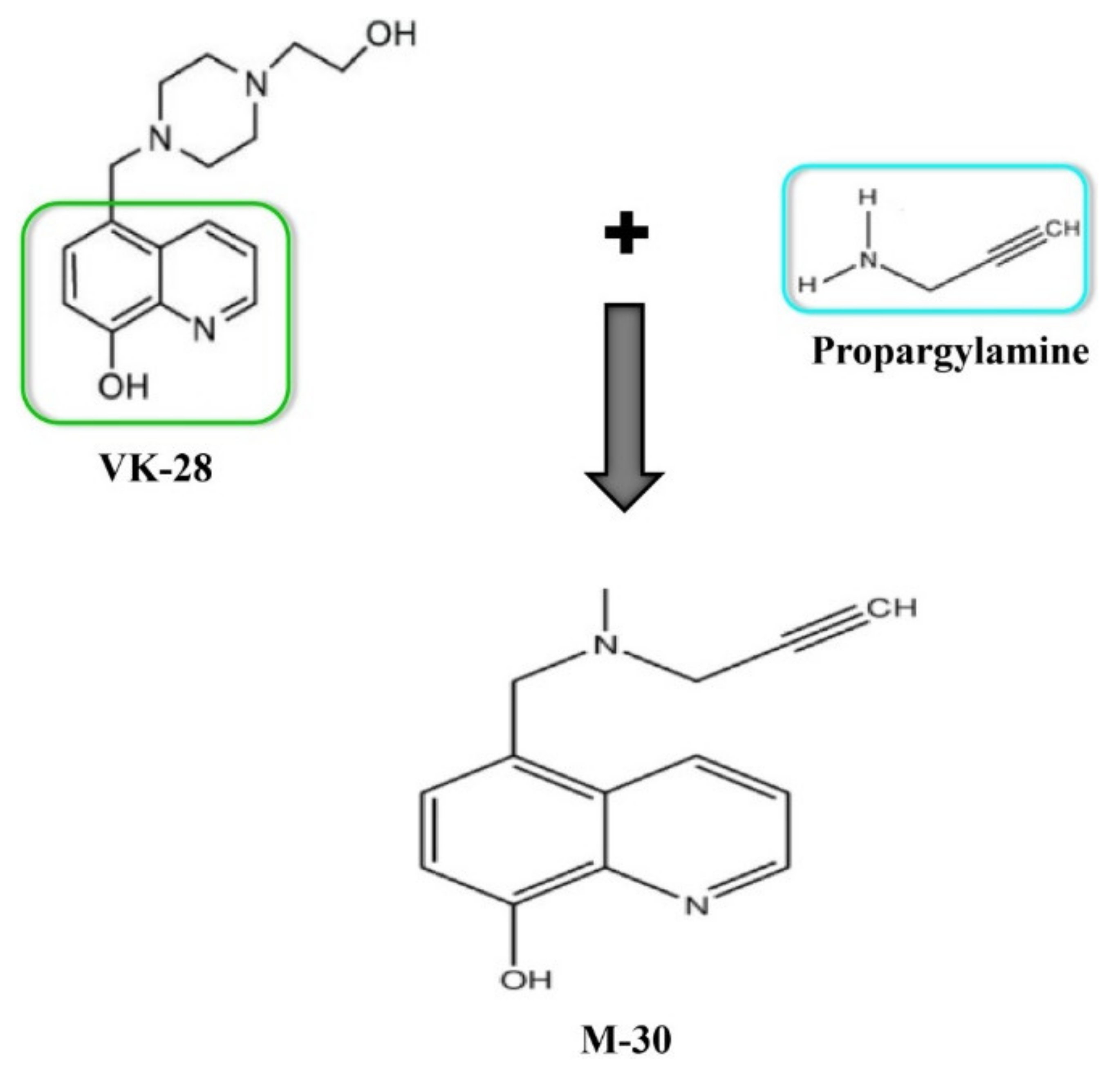
2.5. Combination of VK-28 and Propargylamine
3. Other Combination Approaches for Alzheimer’s Disease
3.1. Combination of PBT2 and ChEIs
3.2. Combination of Noradrenaline Reuptake Inhibitors and ChEIs/NMDAR Antagonists
3.3. Combination of Anti-Tau Agents
3.4. Combination of Neurotrophic Agents
3.5. Combination of Antioxidative Factors
3.6. Combination of Anti-inflammatory Drugs
3.7. Combination of Antidiabetic Drugs
4. Potential Benefits of Combination Therapies
4.1. Clinical Efficacy
4.2. Cognitive Effects
4.3. Behavioral Effects
5. Safety and Tolerability of Combination Therapies
6. Challenges of Combination Therapies in Alzheimer’s Disease
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Uddin, M.S.; Al Mamun, A.; Jakaria, M.; Thangapandiyan, S.; Ahmad, J.; Rahman, M.A.; Mathew, B.; Abdel-Daim, M.M.; Aleya, L. Emerging promise of sulforaphane-mediated Nrf2 signaling cascade against neurological disorders. Sci. Total Environ. 2019, 135624. [Google Scholar] [CrossRef] [PubMed]
- Al Mamun, A.; Uddin, M.S. KDS2010: A Potent Highly Selective and Reversible MAO-B Inhibitor to Abate Alzheimer’s Disease. Comb. Chem. High Throughput Screen. 2020, 23. [Google Scholar] [CrossRef] [PubMed]
- Alzheimer’s Association. 2016 Alzheimer’s disease facts and figures. Alzheimer’s Dement. 2016, 12, 459–509. [Google Scholar] [CrossRef] [PubMed]
- Uddin, M.S.; Kabir, M.T. Emerging Signal Regulating Potential of Genistein Against Alzheimer’s Disease: A Promising Molecule of Interest. Front. Cell Dev. Biol. 2019, 7, 1–12. [Google Scholar] [CrossRef]
- Ringman, J.M.; Goate, A.; Masters, C.L.; Cairns, N.J.; Danek, A.; Graff-Radford, N.; Ghetti, B.; Morris, J.C. Dominantly Inherited Alzheimer Network Genetic Heterogeneity in Alzheimer Disease and Implications for Treatment Strategies. Curr. Neurol. Neurosci. Rep. 2014, 14, 499. [Google Scholar] [CrossRef]
- Uddin, M.S.; Kabir, M.T.; Al Mamun, A.; Abdel-Daim, M.M.; Barreto, G.E.; Ashraf, G.M. APOE and Alzheimer’s Disease: Evidence Mounts that Targeting APOE4 may Combat Alzheimer’s Pathogenesis. Mol. Neurobiol. 2019, 56, 2450–2465. [Google Scholar] [CrossRef]
- Bateman, R.J.; Aisen, P.S.; De Strooper, B.; Fox, N.C.; Lemere, C.A.; Ringman, J.M.; Salloway, S.; Sperling, R.A.; Windisch, M.; Xiong, C. Autosomal-dominant Alzheimer’s disease: A review and proposal for the prevention of Alzheimer’s disease. Alzheimer’s Res. Ther. 2011, 2, 1. [Google Scholar] [CrossRef]
- Uddin, M.S.; Kabir, M.T.; Niaz, K.; Jeandet, P.; Clément, C.; Mathew, B.; Rauf, A.; Rengasamy, K.R.R.; Sobarzo-Sánchez, E.; Ashraf, G.M.; et al. Molecular insight into the therapeutic promise of flavonoids against Alzheimer’s disease. Molecules 2020, 25, 1267. [Google Scholar] [CrossRef]
- Rahman, M.A.; Rahman, M.R.; Zaman, T.; Uddin, M.S.; Islam, R.; Abdel-Daim, M.M.; Rhim, H. Emerging Potential of Naturally Occurring Autophagy Modulator against Neurodegeneration. Curr. Pharm. Des. 2020, 26, 772–779. [Google Scholar] [CrossRef]
- Uddin, M.S.; Tewari, D.; Mamun, A.A.; Kabir, M.T.; Niaz, K.; Wahed, M.I.I.; Barreto, G.E.; Ashraf, G.M. Circadian and sleep dysfunction in Alzheimer’s disease. Ageing Res. Rev. 2020, 60, 101046. [Google Scholar] [CrossRef]
- Mamun, A.A.; Uddin, M.S.; Mathew, B.; Ashraf, G.M. Toxic tau: Structural origins of tau aggregation in Alzheimer’s disease. Neural Regen. Res. 2020, 15, 1417–1420. [Google Scholar] [CrossRef] [PubMed]
- Uddin, M.S.; Kabir, M.T.; Rahman, M.M.; Mathew, B.; Shah, M.A.; Ashraf, G.M. TV 3326 for Alzheimer’s dementia: A novel multimodal ChE and MAO inhibitors to mitigate Alzheimer’s-like neuropathology. J. Pharm. Pharmacol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Nichols, E.; Szoeke, C.E.I.; Vollset, S.E.; Abbasi, N.; Abd-Allah, F.; Abdela, J.; Aichour, M.T.E.; Akinyemi, R.O.; Alahdab, F.; Asgedom, S.W.; et al. Global, regional, and national burden of Alzheimer’s disease and other dementias, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 88–106. [Google Scholar] [CrossRef]
- Uddin, M.S.; Al Mamun, A.; Asaduzzaman, M.; Hosn, F.; Abu Sufian, M.; Takeda, S.; Herrera-Calderon, O.; Abdel-Daim, M.M.; Uddin, G.M.S.; Noor, M.A.A.; et al. Spectrum of Disease and Prescription Pattern for Outpatients with Neurological Disorders: An Empirical Pilot Study in Bangladesh. Ann. Neurosci. 2018, 25, 25–37. [Google Scholar] [CrossRef] [PubMed]
- Cummings, J.; Aisen, P.S.; Dubois, B.; Frölich, L.; Jack, C.R.; Jones, R.W.; Morris, J.C.; Raskin, J.; Dowsett, S.A.; Scheltens, P. Drug development in Alzheimer’s disease: The path to 2025. Alzheimer’s Res. Ther. 2016, 8, 39. [Google Scholar] [CrossRef] [PubMed]
- Cummings, J.L.; Morstorf, T.; Zhong, K. Alzheimer’s disease drug-development pipeline: Few candidates, frequent failures. Alzheimers. Res. Ther. 2014, 6, 37. [Google Scholar] [CrossRef]
- Kabir, M.T.; Abu Sufian, M.; Uddin, M.S.; Begum, M.M.; Akhter, S.; Islam, A.; Mathew, B.; Islam, M.S.; Amran, M.S.; Md Ashraf, G. NMDA Receptor Antagonists: Repositioning of Memantine as Multitargeting Agent for Alzheimer’s Therapy. Curr. Pharm. Des. 2019, 25, 3506–3518. [Google Scholar] [CrossRef]
- Uddin, M.S.; Kabir, M.T.; Tewari, D.; Mathew, B.; Aleya, L. Emerging signal regulating potential of small molecule biflavonoids to combat neuropathological insults of Alzheimer’s disease. Sci. Total Environ. 2020, 700, 1–11. [Google Scholar] [CrossRef]
- Kabir, M.T.; Uddin, M.S.; Begum, M.M.; Thangapandiyan, S.; Rahman, M.S.; Aleya, L.; Mathew, B.; Ahmed, M.; Ashraf, G.M.; Barreto, G.E. Cholinesterase Inhibitors for Alzheimer’s Disease: Multitargeting Strategy based on Anti-Alzheimer’s Drugs Repositioning. Curr. Pharm. Des. 2019, 25, 3519–3535. [Google Scholar] [CrossRef]
- Deardorff, W.J.; Grossberg, G.T. A fixed-dose combination of memantine extended-release and donepezil in the treatment of moderate-to-severe Alzheimer’s disease. Drug Des. Devel. Ther. 2016, 10, 3267–3279. [Google Scholar] [CrossRef]
- Agatonovic-Kustrin, S.; Kettle, C.; Morton, D.W. A molecular approach in drug development for Alzheimer’s disease. Biomed. Pharmacother. 2018, 106, 553–565. [Google Scholar] [CrossRef] [PubMed]
- Capurro, V.; Busquet, P.; Lopes, J.P.; Bertorelli, R.; Tarozzo, G.; Bolognesi, M.L.; Piomelli, D.; Reggiani, A.; Cavalli, A. Pharmacological Characterization of Memoquin, a Multi-Target Compound for the Treatment of Alzheimer’s Disease. PLoS ONE 2013, 8, e56870. [Google Scholar] [CrossRef] [PubMed]
- Patel, L.; Grossberg, G.T. Combination Therapy for Alzheimerʼs Disease. Drugs Aging 2011, 28, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, B.; Bernhardt, T.; Moeller, H.-J.; Heuser, I.; Frolich, L. Combination therapy in Alzheimer’s disease: A review of current evidence. CNS Drugs 2004, 18, 827–844. [Google Scholar] [CrossRef] [PubMed]
- Atri, A.; Shaughnessy, L.W.; Locascio, J.J.; Growdon, J.H. Long-term Course and Effectiveness of Combination Therapy in Alzheimer Disease. Alzheimer Dis. Assoc. Disord. 2008, 22, 209–221. [Google Scholar] [CrossRef]
- Choi, S.H.; Park, K.W.; Na, D.L.; Han, H.J.; Kim, E.-J.; Shim, Y.S.; Lee, J.-H.; EXPECT Study Group. Tolerability and efficacy of memantine add-on therapy to rivastigmine transdermal patches in mild to moderate Alzheimer’s disease: A multicenter, randomized, open-label, parallel-group study. Curr. Med. Res. Opin. 2011, 27, 1375–1383. [Google Scholar] [CrossRef]
- Cummings, J.L.; Schneider, E.; Tariot, P.N.; Graham, S.M.; Memantine MEM-MD-02 Study Group. Behavioral effects of memantine in Alzheimer disease patients receiving donepezil treatment. Neurology 2006, 67, 57–63. [Google Scholar] [CrossRef]
- Farlow, M.R.; Alva, G.; Meng, X.; Olin, J.T. A 25-week, open-label trial investigating rivastigmine transdermal patches with concomitant memantine in mild-to-moderate Alzheimer’s disease: A post hoc analysis. Curr. Med. Res. Opin. 2010, 26, 263–269. [Google Scholar] [CrossRef]
- Dantoine, T.; Auriacombe, S.; Sarazin, M.; Becker, H.; Pere, J.-J.; Bourdeix, I. Rivastigmine monotherapy and combination therapy with memantine in patients with moderately severe Alzheimer’s disease who failed to benefit from previous cholinesterase inhibitor treatment. Int. J. Clin. Pract. 2005, 60, 110–118. [Google Scholar] [CrossRef]
- Feldman, H.H.; Schmitt, F.A.; Olin, J.T.; Memantine MEM-MD-02 Study Group. Activities of Daily Living in Moderate-to-Severe Alzheimer Disease: An Analysis of the Treatment Effects of Memantine in Patients Receiving Stable Donepezil Treatment. Alzheimer Dis. Assoc. Disord. 2006, 20, 263–268. [Google Scholar] [CrossRef][Green Version]
- Lopez, O.L.; Becker, J.T.; Wahed, A.S.; Saxton, J.; Sweet, R.A.; Wolk, D.A.; Klunk, W.; DeKosky, S.T. Long-term effects of the concomitant use of memantine with cholinesterase inhibition in Alzheimer disease. J. Neurol. Neurosurg. Psychiatry 2009, 80, 600–607. [Google Scholar] [CrossRef] [PubMed]
- Porsteinsson, A.; Grossberg, G.; Mintzer, J.; Olin, J.; Memantine MEM-MD-12 Study Group. Memantine Treatment in Patients with Mild to Moderate Alzheimers Disease Already Receiving a Cholinesterase Inhibitor: A Randomized, Double-Blind, Placebo-Controlled Trial. Curr. Alzheimer Res. 2008, 5, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, F.A.; van Dyck, C.H.; Wichems, C.H.; Olin, J.T.; Memantine MEM-MD-02 Study Group. Cognitive response to memantine in moderate to severe Alzheimer disease patients already receiving donepezil: An exploratory reanalysis. Alzheimer Dis. Assoc. Disord. 2006, 20, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Riepe, M.W.; Adler, G.; Ibach, B.; Weinkauf, B.; Tracik, F.; Gunay, I. Domain-Specific Improvement of Cognition on Memantine in Patients with Alzheimer’s Disease Treated with Rivastigmine. Dement. Geriatr. Cogn. Disord. 2007, 23, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Tariot, P.N.; Farlow, M.R.; Grossberg, G.T.; Graham, S.M.; McDonald, S.; Gergel, I.; Memantine Study Group. Memantine treatment in patients with moderate to severe Alzheimer disease already receiving donepezil: A randomized controlled trial. JAMA 2004, 291, 317. [Google Scholar] [CrossRef]
- Weiner, M.W.; Sadowsky, C.; Saxton, J.; Hofbauer, R.K.; Graham, S.M.; Yu, S.Y.; Li, S.; Hsu, H.-A.; Suhy, J.; Fridman, M.; et al. Magnetic resonance imaging and neuropsychological results from a trial of memantine in Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 425–435. [Google Scholar] [CrossRef]
- Wilkinson, D. A review of the effects of memantine on clinical progression in Alzheimer’s disease. Int. J. Geriatr. Psychiatry 2012, 27, 769–776. [Google Scholar] [CrossRef]
- Grossberg, G.; Manes, F.; Allegri, R.; Gutierrez Robledo, L.M.; Gloger, S.; Xie, L.; Jia, X.D.; Perhach, J.; Graham, S.M. P4-405: A multinational, randomized, double-blind, placebo-controlled, parallel-group trial of memantine extended-release capsule (28 mg, once daily) in patients with moderate to severe Alzheimer’s disease. Alzheimer’s Dement. 2008, 4, T793. [Google Scholar] [CrossRef]
- Thomas, S.J.; Grossberg, G.T. Memantine: A review of studies into its safety and efficacy in treating Alzheimer’s disease and other dementias. Clin. Interv. Aging 2009, 4, 367–377. [Google Scholar]
- Parsons, C.G.; Danysz, W.; Dekundy, A.; Pulte, I. Memantine and Cholinesterase Inhibitors: Complementary Mechanisms in the Treatment of Alzheimer’s Disease. Neurotox. Res. 2013, 24, 358–369. [Google Scholar] [CrossRef]
- Posadas, I.; Lopez-Hernandez, B.; Cena, V. Nicotinic Receptors in Neurodegeneration. Curr. Neuropharmacol. 2013, 11, 298–314. [Google Scholar] [CrossRef] [PubMed]
- Jun Kawamata, J.; Syuuichirou Suzuki, S.; Shun Shimohama, S. α7 nicotinic acetylcholine receptor mediated neuroprotection in Parkinson’s disease. Curr. Drug Targets 2012, 13, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Takada-Takatori, Y.; Kume, T.; Sugimoto, M.; Katsuki, H.; Sugimoto, H.; Akaike, A. Acetylcholinesterase inhibitors used in treatment of Alzheimer’s disease prevent glutamate neurotoxicity via nicotinic acetylcholine receptors and phosphatidylinositol 3-kinase cascade. Neuropharmacology 2006, 51, 474–486. [Google Scholar] [CrossRef] [PubMed]
- Lopes, J.P.; Tarozzo, G.; Reggiani, A.; Piomelli, D.; Cavalli, A. Galantamine potentiates the neuroprotective effect of memantine against NMDA-induced excitotoxicity. Brain Behav. 2013, 3, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Rosini, M.; Simoni, E.; Bartolini, M.; Cavalli, A.; Ceccarini, L.; Pascu, N.; McClymont, D.W.; Tarozzi, A.; Bolognesi, M.L.; Minarini, A.; et al. Inhibition of Acetylcholinesterase, β-Amyloid Aggregation, and NMDA Receptors in Alzheimer’s Disease: A Promising Direction for the Multi-target-Directed Ligands Gold Rush. J. Med. Chem. 2008, 51, 4381–4384. [Google Scholar] [CrossRef]
- Simoni, E.; Daniele, S.; Bottegoni, G.; Pizzirani, D.; Trincavelli, M.L.; Goldoni, L.; Tarozzo, G.; Reggiani, A.; Martini, C.; Piomelli, D.; et al. Combining Galantamine and Memantine in Multitargeted, New Chemical Entities Potentially Useful in Alzheimer’s Disease. J. Med. Chem. 2012, 55, 9708–9721. [Google Scholar] [CrossRef]
- Lipton, S.A. Paradigm shift in neuroprotection by NMDA receptor blockade: Memantine and beyond. Nat. Rev. Drug Discov. 2006, 5, 160–170. [Google Scholar] [CrossRef]
- Lipton, S.A.; Choi, Y.B.; Pan, Z.H.; Lei, S.Z.; Chen, H.S.V.; Sucher, N.J.; Loscalzo, J.; Singel, D.J.; Stamler, J.S. A redox-based mechanism for the neuroprotective and neurodestructive effects of nitric oxide and related nitroso-compounds. Nature 1993, 364, 626–632. [Google Scholar] [CrossRef]
- Zheng, H.; Fridkin, M.; Youdim, M. From single target to multitarget/network therapeutics in Alzheimer’s therapy. Pharmaceuticals 2014, 7, 113–135. [Google Scholar] [CrossRef]
- Serrano-Pozo, A.; William, C.M.; Ferrer, I.; Uro-Coste, E.; Delisle, M.B.; Maurage, C.A.; Hock, C.; Nitsch, R.M.; Masliah, E.; Growdon, J.H.; et al. Beneficial effect of human anti-amyloid-β active immunization on neurite morphology and tau pathology. Brain 2010, 133, 1312–1327. [Google Scholar] [CrossRef]
- Dodel, R.; Rominger, A.; Bartenstein, P.; Barkhof, F.; Blennow, K.; Förster, S.; Winter, Y.; Bach, J.P.; Popp, J.; Alferink, J.; et al. Intravenous immunoglobulin for treatment of mild-to-moderate Alzheimer’s disease: A phase 2, randomised, double-blind, placebo-controlled, dose-finding trial. Lancet Neurol. 2013, 12, 233–243. [Google Scholar] [CrossRef]
- Talantova, M.; Sanz-Blasco, S.; Zhang, X.; Xia, P.; Akhtar, M.W.; Okamoto, S.I.; Dziewczapolski, G.; Nakamura, T.; Cao, G.; Pratt, A.E.; et al. Aβ induces astrocytic glutamate release, extrasynaptic NMDA receptor activation, and synaptic loss. Proc. Natl. Acad. Sci. USA 2013, 110, E2518-27. [Google Scholar] [CrossRef] [PubMed]
- Prati, F.; Bergamini, C.; Fato, R.; Soukup, O.; Korabecny, J.; Andrisano, V.; Bartolini, M.; Bolognesi, M.L. Novel 8-Hydroxyquinoline Derivatives as Multitarget Compounds for the Treatment of Alzheimer′s Disease. ChemMedChem 2016, 11, 1284–1295. [Google Scholar] [CrossRef] [PubMed]
- Suh, S.W.; Jensen, K.B.; Jensen, M.S.; Silva, D.S.; Kesslak, P.J.; Danscher, G.; Frederickson, C.J. Histochemically-reactive zinc in amyloid plaques, angiopathy, and degenerating neurons of Alzheimer’s diseased brains. Brain Res. 2000, 852, 274–278. [Google Scholar] [CrossRef]
- Curtain, C.C.; Ali, F.; Volitakis, I.; Cherny, R.A.; Norton, R.S.; Beyreuther, K.; Barrow, C.J.; Masters, C.L.; Bush, A.I.; Barnham, K.J. Alzheimer’s Disease Amyloid-β Binds Copper and Zinc to Generate an Allosterically Ordered Membrane-penetrating Structure Containing Superoxide Dismutase-like Subunits. J. Biol. Chem. 2001, 276, 20466–20473. [Google Scholar] [CrossRef]
- Fernández-Bachiller, M.I.; Peérez, C.; González-Munñoz, G.C.; Conde, S.; Loópez, M.G.; Villarroya, M.; Garciía, A.G.; Rodriíguez-Franco, M.I. Novel Tacrine−8-Hydroxyquinoline Hybrids as Multifunctional Agents for the Treatment of Alzheimer’s Disease, with Neuroprotective, Cholinergic, Antioxidant, and Copper-Complexing Properties. J. Med. Chem. 2010, 53, 4927–4937. [Google Scholar] [CrossRef]
- Peña-Altamira, E.; Prati, F.; Massenzio, F.; Virgili, M.; Contestabile, A.; Bolognesi, M.L.; Monti, B. Changing paradigm to target microglia in neurodegenerative diseases: From anti-inflammatory strategy to active immunomodulation. Expert Opin. Ther. Targets 2016, 20, 627–640. [Google Scholar] [CrossRef]
- Weinstock, M.; Bejar, C.; Wang, R.-H.; Poltyrev, T.; Gross, A.; Finberg, J.P.M.; Youdim, M.B.H. TV3326, a novel neuroprotective drug with cholinesterase and monoamine oxidase inhibitory activities for the treatment of Alzheimer’s disease. In Advances in Research on Neurodegeneration; Springer: Vienna, Austria, 2000; pp. 157–169. [Google Scholar]
- Bar-Am, O.; Weinreb, O.; Amit, T.; Youdim, M.B.H. The novel cholinesterase-monoamine oxidase inhibitor and antioxidant, ladostigil, confers neuroprotection in neuroblastoma cells and aged rats. J. Mol. Neurosci. 2009, 37, 135–145. [Google Scholar] [CrossRef]
- Bar-Am, O.; Yogev-Falach, M.; Amit, T.; Sagi, Y.; Youdim, M.B.H. Regulation of protein kinase C by the anti-Parkinson drug, MAO-B inhibitor, rasagiline and its derivatives, in vivo. J. Neurochem. 2004, 89, 1119–1125. [Google Scholar] [CrossRef]
- Weinreb, O.; Amit, T.; Bar-Am, O.; Youdim, M.B.H. Rasagiline: A novel anti-Parkinsonian monoamine oxidase-B inhibitor with neuroprotective activity. Prog. Neurobiol. 2010, 92, 330–344. [Google Scholar] [CrossRef]
- Faux, N.G.; Ritchie, C.W.; Gunn, A.; Rembach, A.; Tsatsanis, A.; Bedo, J.; Harrison, J.; Lannfelt, L.; Blennow, K.; Zetterberg, H.; et al. PBT2 rapidly improves cognition in alzheimer’s disease: Additional phase II analyses. J. Alzheimer’s Dis. 2010, 20, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Savelieff, M.G.; Detoma, A.S.; Derrick, J.S.; Lim, M.H. The ongoing search for small molecules to study metal-Associated amyloid-β species in alzheimers disease. Acc. Chem. Res. 2014, 47, 2475–2482. [Google Scholar] [CrossRef] [PubMed]
- Gal, S.; Zheng, H.; Fridkin, M.; Youdim, M.B.H. Novel multifunctional neuroprotective iron chelator-monoamine oxidase inhibitor drugs for neurodegenerative diseases. In vivo selective brain monoamine oxidase inhibition and prevention of MPTP-induced striatal dopamine depletion. J. Neurochem. 2005, 95, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.; Gal, S.; Weiner, L.M.; Bar-Am, O.; Warshawsky, A.; Fridkin, M.; Youdim, M.B.H. Novel multifunctional neuroprotective iron chelator-monoamine oxidase inhibitor drugs for neurodegenerative diseases: In vitro studies on antioxidant activity, prevention of lipid peroxide formation and monoamine oxidase inhibition. J. Neurochem. 2005, 95, 68–78. [Google Scholar] [CrossRef]
- Kupershmidt, L.; Amit, T.; Bar-Am, O.; Weinreb, O.; Youdim, M.B.H. Multi-target, neuroprotective and neurorestorative M30 improves cognitive impairment and reduces Alzheimer’s-like neuropathology and age-related alterations in mice. Mol. Neurobiol. 2012, 46, 217–220. [Google Scholar] [CrossRef]
- Kupershmidt, L.; Amit, T.; Bar-Am, O.; Youdim, M.B.H.; Weinreb, O. Neuroprotection by the multitarget iron chelator M30 on age-related alterations in mice. Mech. Ageing Dev. 2012, 133, 267–274. [Google Scholar] [CrossRef]
- Salloway, S.; Sperling, R.; Gilman, S.; Fox, N.C.; Blennow, K.; Raskind, M.; Sabbagh, M.; Honig, L.S.; Doody, R.; van Dyck, C.H.; et al. A phase 2 multiple ascending dose trial of bapineuzumab in mild to moderate Alzheimer disease. Neurology 2009, 73, 2061–2070. [Google Scholar] [CrossRef]
- Rinne, J.O.; Brooks, D.J.; Rossor, M.N.; Fox, N.C.; Bullock, R.; Klunk, W.E.; Mathis, C.A.; Blennow, K.; Barakos, J.; Okello, A.A.; et al. 1C-PiB PET assessment of change in fi brillar amyloid-β load in patients with Alzheimer’s disease treated with bapineuzumab: A phase 2, double-blind, placebo-controlled, ascending-dose study. Lancet Neurol. 2010, 9, 363–372. [Google Scholar] [CrossRef]
- Sperling, R.; Salloway, S.; Brooks, D.J.; Tampieri, D.; Barakos, J.; Fox, N.C.; Raskind, M.; Sabbagh, M.; Honig, L.S.; Porsteinsson, A.P.; et al. Amyloid-related imaging abnormalities in patients with Alzheimer’s disease treated with bapineuzumab: A retrospective analysis. Lancet Neurol. 2012, 11, 241–249. [Google Scholar] [CrossRef]
- Fettelschoss, A.; Zabel, F.; Bachmann, M.F. Vaccination against Alzheimer disease: An update on future strategies. Hum. Vaccin. Immunother. 2014, 10, 847–851. [Google Scholar] [CrossRef]
- Holmes, C.; Boche, D.; Wilkinson, D.; Yadegarfar, G.; Hopkins, V.; Bayer, A.; Jones, R.W.; Bullock, R.; Love, S.; Neal, J.W.; et al. Long-term effects of Aβ42 immunisation in Alzheimer’s disease: Follow-up of a randomised, placebo-controlled phase I trial. Lancet 2008, 372, 216–223. [Google Scholar] [CrossRef]
- Vellas, B.; Black, R.; Thal, L.; Fox, N.; Daniels, M.; McLennan, G.; Tompkins, C.; Leibman, C.; Pomfret, M.; Grundman, M. Long-Term Follow-Up of Patients Immunized with AN1792: Reduced Functional Decline in Antibody Responders. Curr. Alzheimer Res. 2009, 6, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Klaver, A.C.; Finke, J.M.; Digambaranath, J.; Balasubramaniam, M.; Loeffler, D.A. Antibody concentrations to Aβ1-42 monomer and soluble oligomers in untreated and antibody-antigen-dissociated intravenous immunoglobulin preparations. Int. Immunopharmacol. 2010, 10, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Relkin, N.R.; Szabo, P.; Adamiak, B.; Burgut, T.; Monthe, C.; Lent, R.W.; Younkin, S.; Younkin, L.; Schiff, R.; Weksler, M.E. 18-Month study of intravenous immunoglobulin for treatment of mild Alzheimer disease. Neurobiol. Aging 2009, 30, 1728–1736. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. A Study of Semagacestat for Alzheimer’s Patients (Identity XT). Available online: https://clinicaltrials.gov/ct2/show/NCT01035138 (accessed on 19 March 2020).
- Fleisher, A.S.; Raman, R.; Siemers, E.R.; Becerra, L.; Clark, C.M.; Dean, R.A.; Farlow, M.R.; Galvin, J.E.; Peskind, E.R.; Quinn, J.F.; et al. Phase 2 safety trial targeting amyloid β production with a γ-secretase inhibitor in Alzheimer disease. Arch. Neurol. 2008, 65, 1031–1038. [Google Scholar] [CrossRef] [PubMed]
- Henley, D.B.; May, P.C.; Dean, R.A.; Siemers, E.R. Development of semagacestat (LY450139), a functional γ-secretase inhibitor, for the treatment of Alzheimer’s disease. Expert Opin. Pharmacother. 2009, 10, 1657–1664. [Google Scholar] [CrossRef] [PubMed]
- Aisen, P.S.; Gauthier, S.; Ferris, S.H.; Saumier, D.; Haine, D.; Garceau, D.; Duong, A.; Suhy, J.; Oh, J.; Lau, W.C.; et al. Tramiprosate in mild-to-moderate Alzheimer’s disease - A randomized, double-blind, placebo-controlled, multi-centre study (the alphase study). Arch. Med. Sci. 2011, 7, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Gauthier, S.; Aisen, P.S.; Ferris, S.H.; Saumier, D.; Duong, A.; Haine, D.; Garceau, D.; Suhy, J.; Oh, J.; Lau, W.; et al. Effect of tramiprosate in patients with mild-to-moderate Alzheimer’s disease: Exploratory analyses of the MRI sub-group of the Alphase study. J. Nutr. Health Aging 2009, 13, 550–557. [Google Scholar] [CrossRef]
- Vellas, B.; Sol, O.; Snyder, P.J.; Ousset, P.-J.; Haddad, R.; Maurin, M.; Lemarie, J.-C.; Desire, L.; Pando, M.P. EHT0202 in Alzheimers Disease: A 3-Month, Randomized, Placebo- Controlled, Double-Blind Study. Curr. Alzheimer Res. 2012, 8, 203–212. [Google Scholar] [CrossRef]
- Salloway, S.; Sperling, R.; Keren, R.; Porsteinsson, A.P.; Van Dyck, C.H.; Tariot, P.N.; Gilman, S.; Arnold, D.; Abushakra, S.; Hernandez, C.; et al. A phase 2 randomized trial of ELND005, scyllo-inositol, in mild to moderate Alzheimer disease. Neurology 2011, 77, 1253–1262. [Google Scholar] [CrossRef]
- Green, R.C.; Schneider, L.S.; Amato, D.A.; Beelen, A.P.; Wilcock, G.; Swabb, E.A.; Zavitz, K.H. Effect of tarenflurbil on cognitive decline and activities of daily living in patients with mild Alzheimer disease: A randomized controlled trial. JAMA J. Am. Med. Assoc. 2009, 302, 2557–2564. [Google Scholar] [CrossRef] [PubMed]
- Wilcock, G.K.; Black, S.E.; Hendrix, S.B.; Zavitz, K.H.; Swabb, E.A.; Laughlin, M.A. Efficacy and safety of tarenflurbil in mild to moderate Alzheimer’s disease: A randomised phase II trial. Lancet Neurol. 2008, 7, 483–493. [Google Scholar] [CrossRef]
- Harrington, C.; Sawchak, S.; Chiang, C.; Davies, J.; Donovan, C.; Saunders, A.M.; Irizarry, M.; Jeter, B.; Zvartau-Hind, M.; van Dyck, C.H.; et al. Rosiglitazone Does Not Improve Cognition or Global Function when Used as Adjunctive Therapy to AChE Inhibitors in Mild-to-Moderate Alzheimers Disease: Two Phase 3 Studies. Curr. Alzheimer Res. 2011, 8, 592–606. [Google Scholar] [CrossRef]
- Feldman, H.H.; Doody, R.S.; Kivipelto, M.; Sparks, D.L.; Waters, D.D.; Jones, R.W.; Schwam, E.; Schindler, R.; Hey-Hadavi, J.; Demicco, D.A.; et al. Randomized controlled trial of atorvastatin in mild to moderate Alzheimer disease: LEADe. Neurology 2010, 74, 956–964. [Google Scholar] [CrossRef] [PubMed]
- Sano, M.; Bell, K.L.; Galasko, D.; Galvin, J.E.; Thomas, R.G.; Van Dyck, C.H.; Aisen, P.S. A randomized, double-blind, placebo-controlled trial of simvastatin to treat Alzheimer disease. Neurology 2011, 77, 556–563. [Google Scholar] [CrossRef]
- Fleisher, A.S.; Truran, D.; Mai, J.T.; Langbaum, J.B.S.; Aisen, P.S.; Cummings, J.L.; Jack, C.R.; Weiner, M.W.; Thomas, R.G.; Schneider, L.S.; et al. Chronic divalproex sodium use and brain atrophy in Alzheimer disease. Neurology 2011, 77, 1263–1271. [Google Scholar] [CrossRef]
- Tariot, P.N.; Schneider, L.S.; Cummings, J.; Thomas, R.G.; Raman, R.; Jakimovich, L.J.; Loy, R.; Bartocci, B.; Fleisher, A.; Ismail, M.S.; et al. Chronic divalproex sodium to attenuate agitation and clinical progression of Alzheimer disease. Arch. Gen. Psychiatry 2011, 68, 853–861. [Google Scholar] [CrossRef]
- Martel, J.C.; Assié, M.B.; Bardin, L.; Depoortère, R.; Cussac, D.; Newman-Tancredi, A. 5-HT 1A receptors are involved in the effects of xaliproden on G-protein activation, neurotransmitter release and nociception. Br. J. Pharmacol. 2009, 158, 232–242. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. Study of Xaliproden (SR57746A) in Patients With Mild-to-Moderate Dementia of the Alzheimer’s Type. Available online: https://clinicaltrials.gov/ct2/show/NCT00104013 (accessed on 19 March 2020).
- Sevigny, J.J.; Ryan, J.M.; Van Dyck, C.H.; Peng, Y.; Lines, C.R.; Nessly, M.L. Growth hormone secretagogue MK-677: No clinical effect on AD progression in a randomized trial. Neurology 2008, 71, 1702–1708. [Google Scholar] [CrossRef]
- Alvarez, X.; Cacabelos, R.; Sampedro, C.; Couceiro, V.; Aleixandre, M.; Vargas, M.; Linares, C.; Granizo, E.; Garcia-Fantini, M.; Baurecht, W.; et al. Combination Treatment in Alzheimers Disease: Results of a Randomized, Controlled Trial with Cerebrolysin and Donepezil. Curr. Alzheimer Res. 2011, 8, 583–591. [Google Scholar] [CrossRef]
- Mohs, R.C.; Shiovitz, T.M.; Tariot, P.N.; Porsteinsson, A.P.; Baker, K.D.; Feldman, P.D. Atomoxetine augmentation of cholinesterase inhibitor therapy in patients with alzheimer disease: 6-month, randomized, double-blind, placebo-controlled, parallel-trial study. Am. J. Geriatr. Psychiatry 2009, 17, 752–759. [Google Scholar] [CrossRef] [PubMed]
- Lannfelt, L.; Blennow, K.; Zetterberg, H.; Batsman, S.; Ames, D.; Harrison, J.; Masters, C.L.; Targum, S.; Bush, A.I.; Murdoch, R.; et al. Safety, efficacy, and biomarker findings of PBT2 in targeting Aβ as a modifying therapy for Alzheimer’s disease: A phase IIa, double-blind, randomised, placebo-controlled trial. Lancet Neurol. 2008, 7, 779–786. [Google Scholar] [CrossRef]
- Plastino, M.; Fava, A.; Pirritano, D.; Cotronei, P.; Sacco, N.; Sperlì, T.; Spanò, A.; Gallo, D.; Mungari, P.; Consoli, D.; et al. Effects of insulinic therapy on cognitive impairment in patients with Alzheimer disease and diabetes mellitus type-2. J. Neurol. Sci. 2010, 288, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Rigaud, A.S.; André, G.; Vellas, B.; Touchon, J.; Pere, J.J. No additional benefit of HRT on response to rivastigmine in menopausal women with AD. Neurology 2003, 60, 148–150. [Google Scholar] [CrossRef] [PubMed]
- Sano, M.; Ernesto, C.; Thomas, R.G.; Klauber, M.R.; Schafer, K.; Grundman, M.; Woodbury, P.; Growdon, J.; Cotman, C.W.; Pfeiffer, E.; et al. A Controlled Trial of Selegiline, Alpha-Tocopherol, or Both as Treatment for Alzheimer’s Disease. N. Engl. J. Med. 1997, 336, 1216–1222. [Google Scholar] [CrossRef] [PubMed]
- Aisen, P.S.; Schneider, L.S.; Sano, M.; Diaz-Arrastia, R.; Van Dyck, C.H.; Weiner, M.F.; Bottiglieri, T.; Jin, S.; Stokes, K.T.; Thomas, R.G.; et al. High-dose B vitamin supplementation and cognitive decline in Alzheimer disease: A randomized controlled trial. JAMA J. Am. Med. Assoc. 2008, 300, 1774–1783. [Google Scholar] [CrossRef] [PubMed]
- Quinn, J.F.; Raman, R.; Thomas, R.G.; Yurko-Mauro, K.; Nelson, E.B.; Van Dyck, C.; Galvin, J.E.; Emond, J.; Jack, C.R.; Weiner, M.; et al. Docosahexaenoic acid supplementation and cognitive decline in Alzheimer disease: A randomized trial. JAMA J. Am. Med. Assoc. 2010, 304, 1903–1911. [Google Scholar] [CrossRef]
- Freund-Levi, Y.; Eriksdotter-Jönhagen, M.; Cederholm, T.; Basun, H.; Faxén-Irving, G.; Garlind, A.; Vedin, I.; Vessby, B.; Wahlund, L.O.; Palmblad, J. ω-3 fatty acid treatment in 174 patients with mild to moderate Alzheimer disease: OmegAD study - A randomized double-blind trial. Arch. Neurol. 2006, 63, 1402–1408. [Google Scholar] [CrossRef]
- Pasqualetti, P.; Bonomini, C.; Dal Forno, G.; Paulon, L.; Sinforiani, E.; Marra, C.; Zanetti, O.; Rossini, P.M. A randomized controlled study on effects of ibuprofen on cognitive progression of Alzheimer’s disease. Aging Clin. Exp. Res. 2009, 21, 102–110. [Google Scholar] [CrossRef]
- Soininen, H.; West, C.; Robbins, J.; Niculescu, L. Long-term efficacy and safety of celecoxib in Alzheimer’s disease. Dement. Geriatr. Cogn. Disord. 2006, 23, 8–21. [Google Scholar] [CrossRef]
- Aisen, P.S.; Schafer, K.A.; Grundman, M.; Pfeiffer, E.; Sano, M.; Davis, K.L.; Farlow, M.R.; Jin, S.; Thomas, R.G.; Thal, L.J. Effects of Rofecoxib or Naproxen vs Placebo on Alzheimer Disease Progression: A Randomized Controlled Trial. J. Am. Med. Assoc. 2003, 289, 2819–2826. [Google Scholar] [CrossRef] [PubMed]
- Huat, T.J.; Camats-Perna, J.; Newcombe, E.A.; Valmas, N.; Kitazawa, M.; Medeiros, R. Metal Toxicity Links to Alzheimer’s Disease and Neuroinflammation. J. Mol. Biol. 2019, 431, 1843–1868. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Park, M.K.; Seo, Y.R. Pathogenic mechanisms of heavy metal induced-Alzheimer’s disease. Toxicol. Environ. Health Sci. 2018, 10, 1–10. [Google Scholar] [CrossRef]
- Gannon, M.; Wang, Q. Complex noradrenergic dysfunction in Alzheimer’s disease: Low norepinephrine input is not always to blame. Brain Res. 2019, 1702, 12–16. [Google Scholar] [CrossRef]
- Gannon, M.; Che, P.; Chen, Y.; Jiao, K.; Roberson, E.D.; Wang, Q. Noradrenergic dysfunction in Alzheimer’s disease. Front. Neurosci. 2015, 9, 220. [Google Scholar] [CrossRef]
- Congdon, E.E.; Sigurdsson, E.M. Tau-targeting therapies for Alzheimer disease. Nat. Rev. Neurol. 2018, 14, 399–415. [Google Scholar] [CrossRef]
- Álvarez, A.; Cacabelos, R.; Sanpedro, C.; García-Fantini, M.; Aleixandre, M. Serum TNF-alpha levels are increased and correlate negatively with free IGF-I in Alzheimer disease. Neurobiol. Aging 2007, 28, 533–536. [Google Scholar] [CrossRef]
- Mufson, E.; Counts, S.; Fahnestock, M.; Ginsberg, S. Cholinotrophic Molecular Substrates of Mild Cognitive Impairment in the Elderly. Curr. Alzheimer Res. 2007, 4, 340–350. [Google Scholar] [CrossRef]
- Schindowski, K.; Belarbi, K.; Buée, L. Neurotrophic factors in Alzheimer’s disease: Role of axonal transport. In Proceedings of the Genes, Brain and Behavior; Blackwell Publishing Ltd.: Newark, NJ, USA, 2008; Volume 7, pp. 43–56. [Google Scholar]
- Uddin, M.S.; Uddin, G.M.S.; Begum, M.M.; Begum, Y.; Herrera-Calderon, O.; Islam, M.M.; Abdel-Daim, M.M. Inspection of phytochemical content and in vitro antioxidant profile of Gnaphalium luteoalbum L.: An unexplored phytomedicine. J. Pharm. Nutr. Sci. 2017, 7, 136–146. [Google Scholar] [CrossRef]
- Hossain, S.; Uddin, M.S.; Kabir, T.; Begum, M.; Koushal, P.; Herrera-Calderon, O.; Akter, R.; Asaduzzaman, M.D.; Abdel-Daim, M.M. In vitro screening for phytochemicals and antioxidant activities of Syngonium podophyllum l.: An incredible therapeutic plant. Biomed. Pharmacol. J. 2017, 10, 1267–1277. [Google Scholar] [CrossRef]
- Uddin, M.S.; Hossain, M.S.; Mamun, A.A.; Tewari, D.; Asaduzzaman, M.; Islam, M.S.; Abdel-Daim, M.M. Phytochemical analysis and antioxidant profile of methanolic extract of seed, pulp and peel of Baccaurea ramiflora Lour. Asian Pac. J. Trop. Med. 2018, 11, 443. [Google Scholar]
- Uddin, M.S.; Hossain, M.S.; Kabir, M.T.; Rahman, I.; Tewari, D.; Jamiruddin, M.R.; Al Mamun, A. Phytochemical screening and antioxidant profile of Syngonium podophyllum schott stems: A fecund phytopharmakon. J. Pharm. Nutr. Sci. 2018, 8, 120–128. [Google Scholar] [CrossRef]
- Uddin, M.S.; Kabir, M.T. Oxidative Stress in Alzheimer’s Disease: Molecular Hallmarks of Underlying Vulnerability. In Biological, Diagnostic and Therapeutic Advances in Alzheimer’s Disease; Springer Singapore: New York, NY, USA, 2019; pp. 91–115. [Google Scholar]
- Uddin, M.S.; Upaganlawar, A.B. Oxidative Stress and Antioxidant Defense: Biomedical Value in Health and Diseases; Nova Science Publishers: New York, NY, USA, 2019; ISBN 9781536156874. [Google Scholar]
- Rahman, A.; Haque, A.; Uddin, M.S.; Mian, M.M.; Sufian, M.A.; Rahman, M.M.; Ali, Y.; Rafe, M.R.; Abdel-Daim, M.M.; Uddin, M.J.; et al. In vitro screening for antioxidant and anticholinesterase effects of Uvaria littoralis Blume.: A nootropic phytotherapeutic remedy. J. Intellect. Disabil. Diagnosis Treat. 2017, 5, 50–60. [Google Scholar] [CrossRef]
- Hossain, M.S.; Uddin, M.S.; Kabir, M.T.; Akhter, S.; Goswami, S.; Mamun, A.A.; Herrera-Calderon, O.; Asaduzzaman, M.; Abdel-Daim, M.M. In vivo screening for analgesic and anti-inflammatory activities of Syngonium podophyllum L.: A remarkable herbal medicine. Annu. Res. Rev. Biol. 2017, 16, 1–12. [Google Scholar] [CrossRef]
- Begum, M.M.; Islam, A.; Begum, R.; Uddin, M.S.; Rahman, M.S.; Alam, S.; Akter, W.; Das, M.; Rahman, M.S.; Imon, A.H.M.R. Ethnopharmacological Inspections of Organic Extract of Oroxylum indicum in Rat Models: A Promising Natural Gift. Evidence-Based Complement. Altern. Med. 2019, 2019, 1–13. [Google Scholar] [CrossRef]
- Moore, A.H.; Bigbee, M.J.; Boynton, G.E.; Wakeham, C.M.; Rosenheim, H.M.; Staral, C.J.; Morrissey, J.L.; Hund, A.K. Non-steroidal anti-inflammatory drugs in alzheimer’s disease and parkinson’s disease: Reconsidering the role of neuroinflammation. Pharmaceuticals 2010, 3, 1812–1841. [Google Scholar] [CrossRef]
- Akter, K.; Lanza, E.A.; Martin, S.A.; Myronyuk, N.; Rua, M.; Raffa, R.B. Diabetes mellitus and Alzheimer’s disease: Shared pathology and treatment? Br. J. Clin. Pharmacol. 2011, 71, 365–376. [Google Scholar] [CrossRef]
- Zhong, K.L.; Chen, F.; Hong, H.; Ke, X.; Lv, Y.G.; Tang, S.S.; Zhu, Y.B. New views and possibilities of antidiabetic drugs in treating and/or preventing mild cognitive impairment and Alzheimer’s Disease. Metab. Brain Dis. 2018, 33, 1009–1018. [Google Scholar] [CrossRef]
- Chow, V.W.; Savonenko, A.V.; Melnikova, T.; Kim, H.; Price, D.L.; Li, T.; Wong, P.C. Modeling an anti-amyloid combination therapy for Alzheimer’s disease. Sci. Transl. Med. 2010, 2. [Google Scholar] [CrossRef]
- Ihl, R.; Frölich, L.; Winblad, B.; Schneider, L.; Burns, A.; Möller, H.-J. WFSBP Task Force on Treatment Guidelines for Alzheimer’s Disease and other Dementias World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines for the Biological Treatment of Alzheimer’s disease and other dementias. World J. Biol. Psychiatry 2011, 12, 2–32. [Google Scholar] [CrossRef]
- Cummings, J.L. Treatment of Alzheimer’s disease: The role of symptomatic agents in an era of disease-modifying therapies. Rev. Neurol. Dis. 2007, 4, 57–62. [Google Scholar] [PubMed]
- Farlow, M.R.; Miller, M.L.; Pejovic, V. Treatment options in Alzheimer’s disease: Maximizing benefit, managing expectations. Dement. Geriatr. Cogn. Disord. 2008, 25, 408–422. [Google Scholar] [CrossRef] [PubMed]
- Deiana, S.; Harrington, C.R.; Wischik, C.M.; Riedel, G. Methylthioninium chloride reverses cognitive deficits induced by scopolamine: Comparison with rivastigmine. Psychopharmacology 2009, 202, 53–65. [Google Scholar] [CrossRef] [PubMed]
- Gauthier, S.; Loft, H.; Cummings, J. Improvement in behavioural symptoms in patients with moderate to severe Alzheimer’s disease by memantine: A pooled data analysis. Int. J. Geriatr. Psychiatry 2008, 23, 537–545. [Google Scholar] [CrossRef]
- Grossberg, G.T.; Pejović, V.; Miller, M.L.; Graham, S.M. Memantine Therapy of Behavioral Symptoms in Community-Dwelling Patients with Moderate to Severe Alzheimer’s Disease. Dement. Geriatr. Cogn. Disord. 2009, 27, 164–172. [Google Scholar] [CrossRef]
- Wilcock, G.K.; Ballard, C.G.; Cooper, J.A.; Loft, H. Memantine for agitation/aggression and psychosis in moderately severe to severe Alzheimer’s disease: A pooled analysis of 3 studies. J. Clin. Psychiatry 2008, 69, 341–348. [Google Scholar] [CrossRef]
- Jones, R.W. A review comparing the safety and tolerability of memantine with the acetylcholinesterase inhibitors. Int. J. Geriatr. Psychiatry 2009, 25, 547–553. [Google Scholar] [CrossRef]
- Ãlvarez, X.A.; Linares, C.; Masliah, E. Combination drug therapy for the treatment of alzheimer’s disease. Eur. Neurol. Rev. 2012, 7, 92–101. [Google Scholar] [CrossRef]
- Rountree, S.D.; Chan, W.; Pavlik, V.N.; Darby, E.J.; Siddiqui, S.; Doody, R.S. Persistent treatment with cholinesterase inhibitors and/or memantine slows clinical progression of Alzheimer disease. Alzheimers. Res. Ther. 2009, 1, 7. [Google Scholar] [CrossRef]
- Gillette-Guyonnet, S.; Andrieu, S.; Nourhashemi, F.; Gardette, V.; Coley, N.; Cantet, C.; Gauthier, S.; Ousset, P.J.; Vellas, B. Long-term progression of Alzheimer’s disease in patients under antidementia drugs. Alzheimer’s Dement. 2011, 7, 579–592. [Google Scholar] [CrossRef]
- Cummings, J.L.; Tong, G.; Ballard, C. Treatment Combinations for Alzheimer’s Disease: Current and Future Pharmacotherapy Options. J. Alzheimer’s Dis. 2019, 67, 779–794. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Combination Therapy | Participants | Disease State | Duration | Study Design | Effects | References |
|---|---|---|---|---|---|---|
| ChEIs + memantine | 47 | Alzheimer’s disease (AD) | 48 weeks | Single-arm, delayed-start exploratory study | No significant difference in the rates of total brain volume change between the two study periods. Treatment with memantine was also linked with superior performances on the executive functioning and reduction of right hippocampal atrophy. | [36] |
| Rivastigmine + memantine | 172 | Mild to moderate AD | 24 weeks | Multicenter, randomized, open-label study | No significant differences in efficacy. No noticeable differences in safety and tolerability between the treatment groups. | [26] |
| Memantine + rivastigmine | 176 | Mild-to-moderate AD | 25 weeks | Open-label, prospective, parallel-group study | No noticeable differences in tolerability between the treatment groups. No noticeable differences in cognition or global functioning. | [28] |
| ChEI + memantine | 943 | Probable AD | At least a 1-year follow-up | Real-world observational study on a long-term basis | Significantly extending time to nursing home admission. | [31] |
| Rivastigmine + memantine | 90 | Mild-to-moderate and moderate-to-severe AD | 12 weeks | Open-label, pilot study | Enhancement of attention/executive function with secondary memory progress | [34] |
| ChEI + memantine | 677 | Moderate to severe AD | 24 weeks | Multinational, randomized, double-blind, placebo-controlled, parallel-group trial | Significant improvements in severe impairment battery (SIB), clinician’s interview-based impression of change plus (CIBIC+) data, safe, and well-tolerated therapy. | [38,39] |
| ChEI + memantine | 433 | Mild to moderate AD | 24 weeks | Randomized, double-blind, placebo-controlled trial | No statistically significant differences between the memantine- and placebo group on outcome measures. | [32] |
| Donepezil + memantine | 404 | Moderate to severe AD | 24 weeks | Randomized, double-blind, placebo-controlled trial | As compared with monotherapy, combination showed significantly enhancement in SIB, less decline in AD Cooperative Study-Activities of Daily Living Inventory (ADCS-ADL) and improvement in CIBIC+ data. | [27,30,33,35] |
| ChEI + memantine | 382 | AD | 4 years | Long-term real-world observational study | CT slows cognitive and functional impairment as compared to ChEI and no treatment. | [25] |
| Rivastigmine + memantine | 202 | Moderately severe AD | 28 weeks | Open-label, multicentre study | Switching from donepezil or galantamine to rivastigmine may progress cognition and behavior. The addition of memantine may be useful. | [29] |
| Therapeutic Agent | Target | Participants | Disease State | Duration | Combination Therapy Type | Study Design | Effects | References |
|---|---|---|---|---|---|---|---|---|
| Bapineuzumab | Amyloid pathology | 234; 28; 210 | Mild-to-moderate Alzheimer’s disease (AD) | 78 weeks | Add-on | Phase II | No efficacy; Reduces cortical (11)C-PiB retention compared with both baseline and placebo | [68,69,70] |
| AN1792 | Amyloid pathology | 80; 159 | Mild-to-moderate AD | 4.6 years | Add-on | Phase IIA | Reduces neurite abnormality in the hippocampus; Decreases significantly functional decline | [50,71,72,73] |
| Intravenous immunoglobulins (Gammagard, Octagam, Flebogamma) | Amyloid pathology | 58 | Mild-to-moderate AD; Mild AD; AD | 24 weeks; 6+9 months; 24 months | Add-on | Phase II; Open label dose-ranging study | Stabilized cognitive functions, reduced levels of Aβ in cerebrospinal fluid (CSF) | [51,74,75] |
| Semagacestat (LY450139) | Amyloid pathology | 180; 51 | AD; Mild-to-moderate AD | 24 months; 14 weeks | Add-on | Phase III; Phase II | No efficacy; Decreases in plasma Aβ concentrations | [76,77,78] |
| Tramiprosate | Amyloid pathology | 1052 | Mild-to-moderate AD | 78 weeks | Add-on | Randomized, double-blind, placebo-controlled, multi-centre trial | No clinical efficacy and reduced hippocampal atrophy | [79,80] |
| Etazolate (EHT0202) | Amyloid pathology | 159 | Mild-to-moderate AD | 12 weeks | ChEIs | Phase IIA | Improves AD Cooperative Study-Activities of Daily Living Inventory (ADCS-ADL) data | [81] |
| Scyllo-inositol (ELND005) | Amyloid pathology | 353 | Mild-to-moderate AD | 78 weeks | Add-on | Phase II | No significant primary clinical efficacy, and reduces CSF Aβ42 levels | [82] |
| Tarenflurbil | Amyloid pathology | 1649; 210 | Mild AD; Mild to moderate AD | 18 months; 12+12 months | Add-on | Randomized controlled trial; Phase II | No clinical efficacy; Exerts a dose-related effect on measures of daily activities and global function | [83,84] |
| Rosiglitazone | Amyloid pathology | 1496 + 1485 | Mild-to-moderate AD | 48 weeks | Two phase III studies | No clinical efficacy | [85] | |
| Atorvastatin | Amyloid pathology | 640 | Mild-to-moderate AD | 72 weeks | Add-on | Phase III | No clinical efficacy | [86] |
| Simvastatin | Amyloid pathology | 406 | Mild-to-moderate AD | 18 months | Add-on | Phase III | No clinical efficacy | [87] |
| Divalproex sodium | Tau pathology | 313 | Moderate AD | 24 months | Add-on | Phase III | No clinical efficacy | [88,89] |
| Xaliproden | Neurotrophic deficits | 1455 | Mild-to-moderate AD | 18 months | Add-on | Phase III | No clinical efficacy | [90,91] |
| MK-677 | Neurotrophic deficits | 563 | Mild-to-moderate AD | 12 months | Add-on | Phase II | No clinical efficacy | [92] |
| Cerebrolysin | Neurotrophic deficits | 197 | Mild-to-moderate probable AD | 28 weeks | Donepezil | Randomized, double-blind trial | Improves cognitive and global functions | [93] |
| Atomoxetine | Neurotransmitter Deficits | 92 | Mild-to-moderate AD | 6 months | ChEIs | Phase II-III | No clinical efficacy | [94] |
| PBT2 | Excitotoxicity | 78 | AD | 12 weeks | ChEIs | Phase IIA | Improves cognition; Significant improvements in executive functions, and marked decrease in the CSF Aβ42 levels | [62,95] |
| Insulin | Metabolic alterations | 104 | Patients with mild-to-moderate AD and diabetes mellitus type-2 | 12 months | Add-on | Open-label | Reduces considerably cognitive decline | [96] |
| Hormone replacement therapy | Metabolic alterations | 117 | Menopausal women with AD | 28 weeks | Rivastigmine | Randomized controlled trial | No significant effect | [97] |
| Vitamin E, Selegiline | Oxidative stress | 341 | Moderately severe AD | 2 years | Combined versus monotherapy | Double-blind, placebo-controlled, randomized, multicenter trial | No superiority of combination to monotherapy | [98] |
| Folate/Vitamin B6/ Vitamin B12 | Oxidative stress | 409 | Mild to moderate AD | 18 months | Add-on | Multicenter, randomized, double-blind controlled trial | No effects on the primary cognitive measure | [99] |
| Docosahexaenoic acid | Oxidative stress | 402 | AD | 18 months | Add-on | Randomized, double-blind, placebo-controlled trial | No clinical efficacy | [100] |
| Docosahexaenoic acid/Eicosapentaenoic acid | Oxidative stress | 174 | Mild to moderate AD | 12 months | ChEIs | Randomized, double-blind, placebo-controlled trial | No clinical efficacy | [101] |
| Ibuprofen | Neuroinflammation | 132 | Mild to moderate AD | 12 months | Add-on | Multicenter, randomized, double-blind, placebo-controlled, parallel group trial | No clinical efficacy | [102] |
| Celecoxib | Neuroinflammation | Conducted in 8 countries at 30 sites | Established mild-to-moderate AD | 52 weeks | Add-on | Multicenter, randomized, double-blind, placebo-controlled, parallel-group trial | No clinical efficacy | [103] |
| Naproxen/Rofecoxib | Neuroinflammation | 351 | Mild-to-moderate AD | 52 weeks | ChEIs | Multicenter, randomized, double-blind, placebo-controlled, parallel group trial | No clinical efficacy | [104] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kabir, M.T.; Uddin, M.S.; Mamun, A.A.; Jeandet, P.; Aleya, L.; Mansouri, R.A.; Ashraf, G.M.; Mathew, B.; Bin-Jumah, M.N.; Abdel-Daim, M.M. Combination Drug Therapy for the Management of Alzheimer’s Disease. Int. J. Mol. Sci. 2020, 21, 3272. https://doi.org/10.3390/ijms21093272
Kabir MT, Uddin MS, Mamun AA, Jeandet P, Aleya L, Mansouri RA, Ashraf GM, Mathew B, Bin-Jumah MN, Abdel-Daim MM. Combination Drug Therapy for the Management of Alzheimer’s Disease. International Journal of Molecular Sciences. 2020; 21(9):3272. https://doi.org/10.3390/ijms21093272
Chicago/Turabian StyleKabir, Md. Tanvir, Md. Sahab Uddin, Abdullah Al Mamun, Philippe Jeandet, Lotfi Aleya, Rasha A. Mansouri, Ghulam Md Ashraf, Bijo Mathew, May N. Bin-Jumah, and Mohamed M. Abdel-Daim. 2020. "Combination Drug Therapy for the Management of Alzheimer’s Disease" International Journal of Molecular Sciences 21, no. 9: 3272. https://doi.org/10.3390/ijms21093272
APA StyleKabir, M. T., Uddin, M. S., Mamun, A. A., Jeandet, P., Aleya, L., Mansouri, R. A., Ashraf, G. M., Mathew, B., Bin-Jumah, M. N., & Abdel-Daim, M. M. (2020). Combination Drug Therapy for the Management of Alzheimer’s Disease. International Journal of Molecular Sciences, 21(9), 3272. https://doi.org/10.3390/ijms21093272