Uromodulin and microRNAs in Kidney Transplantation—Association with Kidney Graft Function


 , ,
, ,
Abstract
1. Introduction
2. Results
2.1. Characteristics of the Study Population
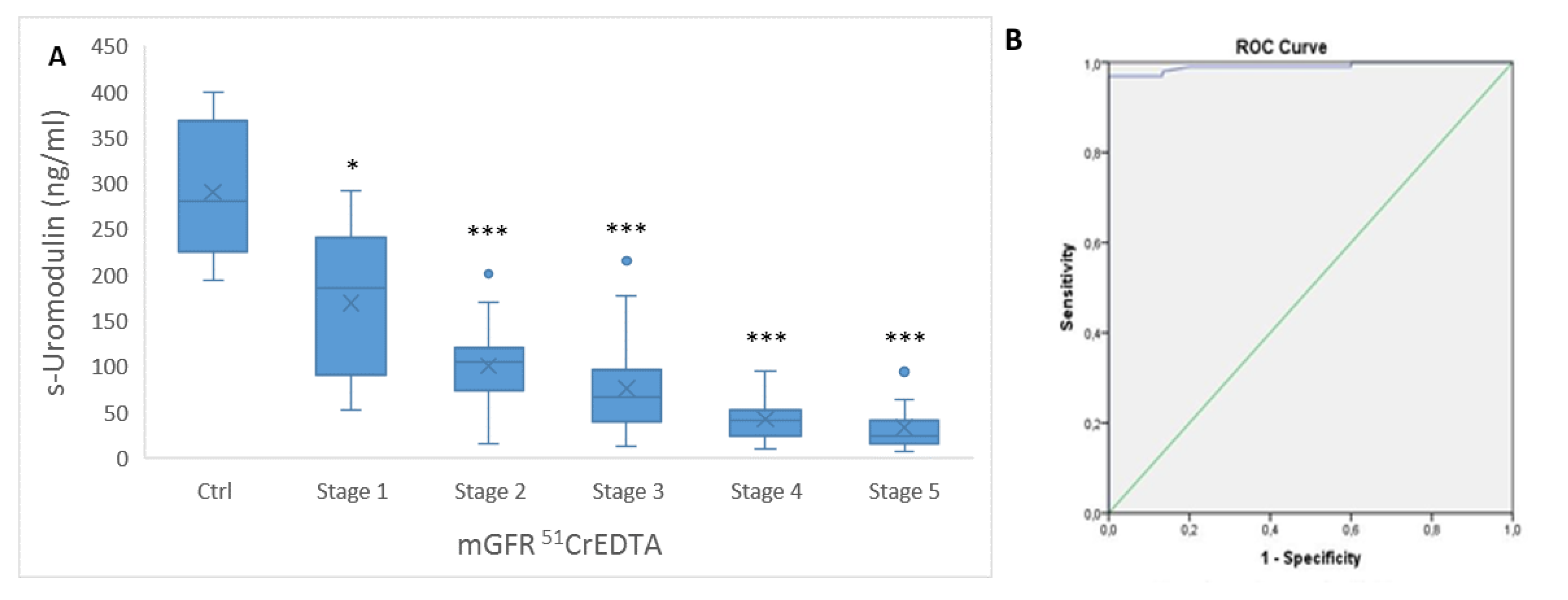
2.2. Relation between Kidney Function Parameters and s-Uromodulin
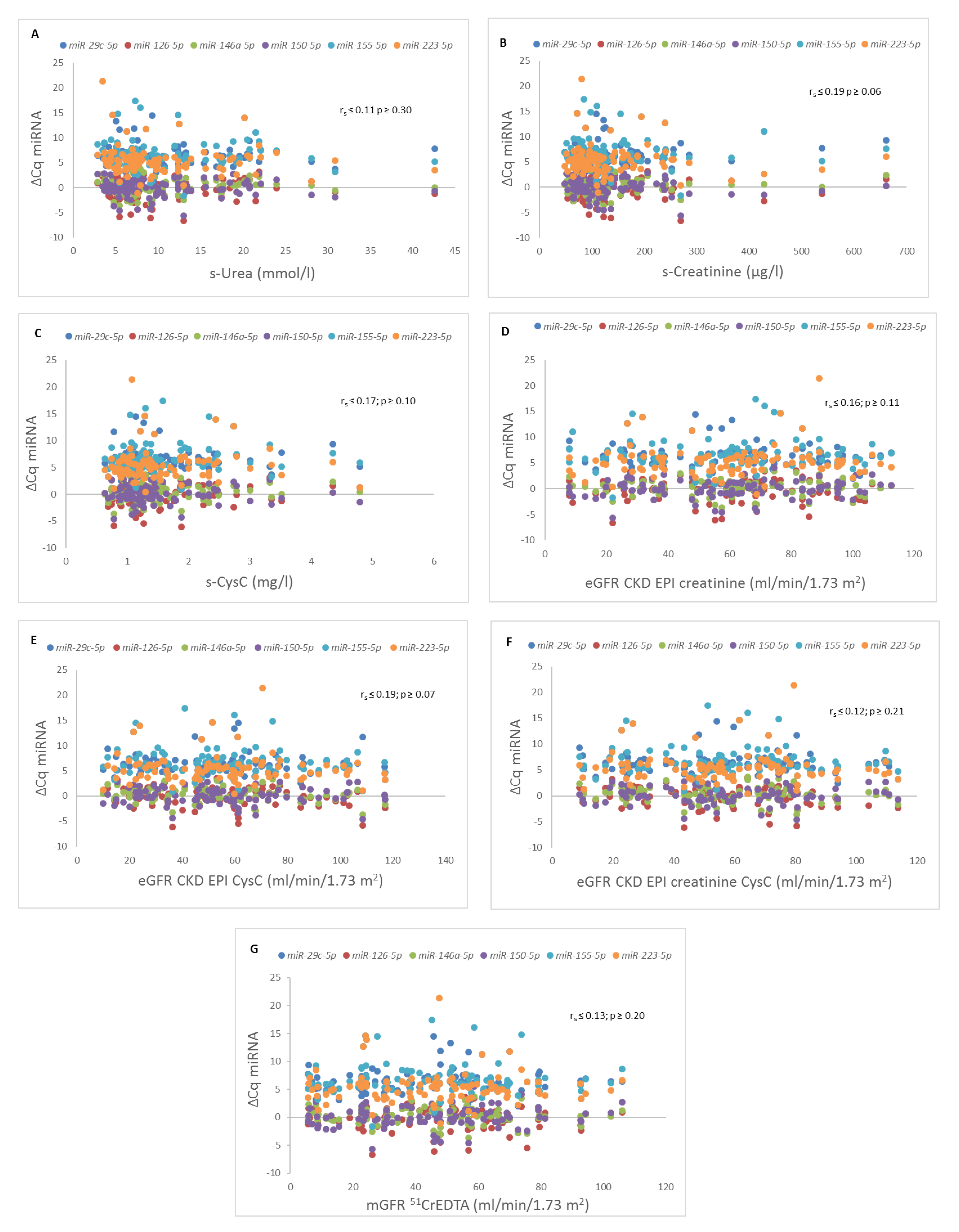
2.3. Relation between Kidney Function Parameters and Expression of Selected miRNAs
3. Discussion
4. Materials and Methods
4.1. Study Population Inclusion and Exclusion Criteria
4.2. Measurement of Serum Creatinine, Serum Urea, and Cystatin C Concentration
4.3. eGFR
4.4. Measurement of 51CrEDTA Clearance
4.5. Measurement of s-Uromodulin
4.6. miRNA Quantification
4.7. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| CKD | chronic kidney disease |
| CKD-T | chronic kidney disease of transplanted kidney |
| 51CrEDTA | chromium-51-ethylenediaminetetraacetic acid |
| GFR | glomerular filtration rate |
| eGFR | estimated GFR |
| eGFR CKD EPI creatinine | eGFR with Chronic Kidney Disease Epidemiology Collaboration study formula with s-Creatinine |
| eGFR CKD EPI CysC | eGFR with Chronic Kidney Disease Epidemiology Collaboration study formula with s-CysC |
| eGFR CKD EPI creatinine CysC | eGFR with Chronic Kidney Disease Epidemiology Collaboration study formula with s-Creatinine and s-CysC |
| mGFR 51CrEDTA | measured GFR with 51CrEDTA |
| IF/TA | interstitial fibrosis/tubular atrophy |
| KTRs | kidney transplant recipients |
| miRNA | microRNA |
| RNA | ribonucleic acid |
| s-Creatinine | serum creatinine concentration |
| s-CysC | serum cystatin C concentration |
| s-Urea | serum urea concentration |
| s-Uromodulin | serum uromodulin concentration |
References
- Tamm, I.; Horsfall, F.L., Jr. Characterization and separation of an inhibitor of viral hemagglutination present in urine. Proc. Soc. Exp. Biol. Med. 1950, 74, 106–108. [Google Scholar] [CrossRef] [PubMed]
- Vyletal, P.; Bleyer, A.J.; Kmoch, S. Uromodulin biology and pathophysiology—An update. Kidney Blood Press. Res. 2010, 33, 456–475. [Google Scholar] [CrossRef] [PubMed]
- Prajczer, S.; Heidenreich, U.; Pfaller, W.; Kotanko, P.; Lhotta, K.; Jennings, P. Evidence for a role of uromodulin in chronic kidney disease progression. Nephrol. Dial. Transplant. 2010, 25, 1896–1903. [Google Scholar] [CrossRef]
- Scherberich, J.E.; Gruber, R.; Nockher, W.A.; Christensen, E.I.; Schmitt, H.; Herbst, V.; Block, M.; Kaden, J.; Schlumberger, W. Serum uromodulin-a marker of kidney function and renal parenchymal integrity. Nephrol. Dial. Transplant. 2018, 33, 284–295. [Google Scholar] [CrossRef] [PubMed]
- Steubl, D.; Block, M.; Herbst, V.; Nockher, W.A.; Schlumberger, W.; Satanovskij, R.; Angermann, S.; Hasenau, A.L.; Stecher, L.; Heemann, U.; et al. Plasma Uromodulin Correlates With Kidney Function and Identifies Early Stages in Chronic Kidney Disease Patients. Medicine 2016, 95, e3011. [Google Scholar] [CrossRef] [PubMed]
- Bostom, A.; Steubl, D.; Garimella, P.S.; Franceschini, N.; Roberts, M.B.; Pasch, A.; Ix, J.H.; Tuttle, K.R.; Ivanova, A.; Shireman, T.; et al. Serum Uromodulin: A Biomarker of Long-Term Kidney Allograft Failure. Am. J. Nephrol 2018, 47, 275–282. [Google Scholar] [CrossRef]
- Steubl, D.; Block, M.; Herbst, V.; Schlumberger, W.; Nockher, A.; Angermann, S.; Schmaderer, C.; Heemann, U.; Renders, L.; Scherberich, J. Serum uromodulin predicts graft failure in renal transplant recipients. Biomarkers 2017, 22, 171–177. [Google Scholar] [CrossRef]
- Reznichenko, A.; van Dijk, M.C.; van der Heide, J.H.; Bakker, S.J.; Seelen, M.; Navis, G. Uromodulin in renal transplant recipients: Elevated urinary levels and bimodal association with graft failure. Am. J. Nephrol. 2011, 34, 445–451. [Google Scholar] [CrossRef]
- Khan, Z.; Suthanthiran, M.; Muthukumar, T. MicroRNAs and Transplantation. Clin. Lab. Med. 2019, 39, 125–143. [Google Scholar] [CrossRef]
- Wilflingseder, J.; Reindl-Schwaighofer, R.; Sunzenauer, J.; Kainz, A.; Heinzel, A.; Mayer, B.; Oberbauer, R. MicroRNAs in kidney transplantation. Nephrol. Dial. Transplant. 2015, 30, 910–917. [Google Scholar] [CrossRef]
- Janszky, N.; Susal, C. Circulating and urinary microRNAs as possible biomarkers in kidney transplantation. Transplant. Rev. 2018, 32, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Kriegel, A.J.; Liu, Y.; Fang, Y.; Ding, X.; Liang, M. The miR-29 family: Genomics, cell biology, and relevance to renal and cardiovascular injury. Physiol. Genomics 2012, 44, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Taibi, F.; Metzinger-Le Meuth, V.; M’Baya-Moutoula, E.; Djelouat, M.; Louvet, L.; Bugnicourt, J.M.; Poirot, S.; Bengrine, A.; Chillon, J.M.; Massy, Z.A.; et al. Possible involvement of microRNAs in vascular damage in experimental chronic kidney disease. Biochim. Biophys. Acta 2014, 1842, 88–98. [Google Scholar] [CrossRef]
- Metzinger-Le Meuth, V.; Burtey, S.; Maitrias, P.; Massy, Z.A.; Metzinger, L. microRNAs in the pathophysiology of CKD-MBD: Biomarkers and innovative drugs. Biochim. Biophys. Acta Mol. Basis Dis. 2017, 1863, 337–345. [Google Scholar] [CrossRef]
- Fourdinier, O.; Schepers, E.; Metzinger-Le Meuth, V.; Glorieux, G.; Liabeuf, S.; Verbeke, F.; Vanholder, R.; Brigant, B.; Pletinck, A.; Diouf, M.; et al. Serum levels of miR-126 and miR-223 and outcomes in chronic kidney disease patients. Sci. Rep. 2019, 9, 4477. [Google Scholar] [CrossRef] [PubMed]
- Testa, U.; Pelosi, E.; Castelli, G.; Labbaye, C. miR-146 and miR-155: Two Key Modulators of Immune Response and Tumor Development. Non-Coding RNA 2017, 3, 22. [Google Scholar] [CrossRef]
- Milhoransa, P.; Montanari, C.C.; Montenegro, R.; Manfro, R.C. Micro RNA 146a-5p expression in Kidney transplant recipients with delayed graft function. J. Bras. Nefrol. 2019, 41, 242–251. [Google Scholar] [CrossRef]
- Huang, X.L.; Zhang, L.; Li, J.P.; Wang, Y.J.; Duan, Y.; Wang, J. MicroRNA-150: A potential regulator in pathogens infection and autoimmune diseases. Autoimmunity 2015, 48, 503–510. [Google Scholar] [CrossRef]
- De Candia, P.; Torri, A.; Pagani, M.; Abrignani, S. Serum microRNAs as Biomarkers of Human Lymphocyte Activation in Health and Disease. Front. Immunol. 2014, 5, 43. [Google Scholar] [CrossRef]
- Yuan, X.; Berg, N.; Lee, J.W.; Le, T.T.; Neudecker, V.; Jing, N.; Eltzschig, H. MicroRNA miR-223 as regulator of innate immunity. J. Leukoc. Biol. 2018, 104, 515–524. [Google Scholar] [CrossRef]
- Metzinger-Le Meuth, V.; Metzinger, L. miR-223 and other miRNA’s evaluation in chronic kidney disease: Innovative biomarkers and therapeutic tools. Non-Coding RNA Res. 2019, 4, 30–35. [Google Scholar] [CrossRef]
- Li, S.; Chen, H.; Ren, J.; Geng, Q.; Song, J.; Lee, C.; Cao, C.; Zhang, J.; Xu, N. MicroRNA-223 inhibits tissue factor expression in vascular endothelial cells. Atherosclerosis 2014, 237, 514–520. [Google Scholar] [CrossRef] [PubMed]
- O’Callaghan, J.M.; Knight, S.R. Noninvasive biomarkers in monitoring kidney allograft health. Curr. Opin. Organ. Transplant. 2019, 24, 411–415. [Google Scholar] [CrossRef] [PubMed]
- Naesens, M.; Anglicheau, D. Precision Transplant Medicine: Biomarkers to the Rescue. J. Am. Soc. Nephrol. 2018, 29, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Buron, F.; Hadj-Aissa, A.; Dubourg, L.; Morelon, E.; Steghens, J.P.; Ducher, M.; Fauvel, J.P. Estimating glomerular filtration rate in kidney transplant recipients: Performance over time of four creatinine-based formulas. Transplantation 2011, 92, 1005–1011. [Google Scholar] [CrossRef] [PubMed]
- Fedak, D.; Kuzniewski, M.; Fugiel, A.; Wieczorek-Surdacka, E.; Przepiorkowska-Hoyer, B.; Jasik, P.; Miarka, P.; Dumnicka, P.; Kapusta, M.; Solnica, B.; et al. Serum uromodulin concentrations correlate with glomerular filtration rate in patients with chronic kidney disease. Pol. Arch. Med. Wewn. 2016, 126, 995–1004. [Google Scholar] [CrossRef]
- Gibson, T. Hyperuricemia, gout and the kidney. Curr. Opin. Rheumatol. 2012, 24, 127–131. [Google Scholar] [CrossRef]
- Millan, O.; Budde, K.; Sommerer, C.; Aliart, I.; Rissling, O.; Bardaji, B.; Matz, M.; Zeier, M.; Silva, I.; Guirado, L.; et al. Urinary miR-155-5p and CXCL10 as prognostic and predictive biomarkers of rejection, graft outcome and treatment response in kidney transplantation. Br. J. Clin. Pharmacol. 2017, 83, 2636–2650. [Google Scholar] [CrossRef]
- Delanaye, P.; Mariat, C. The applicability of eGFR equations to different populations. Nat. Rev. Nephrol. 2013, 9, 513–522. [Google Scholar] [CrossRef]
- Inker, L.A.; Eckfeldt, J.; Levey, A.S.; Leiendecker-Foster, C.; Rynders, G.; Manzi, J.; Waheed, S.; Coresh, J. Expressing the CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) cystatin C equations for estimating GFR with standardized serum cystatin C values. Am. J. Kidney Dis. 2011, 58, 682–684. [Google Scholar] [CrossRef]
- Levin, A.; Stevens, P.E.; Bilous, R.W.; Coresh, J.; De Francisco, A.L.M.; De Jong, P.E.; Griffith, K.E.; Hemmelgarn, B.R.; Iseki, K.; Lamb, E.J.; et al. Kidney disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar]
- Blaufox, M.D.; Aurell, M.; Bubeck, B.; Fommei, E.; Piepsz, A.; Russell, C.; Taylor, A.; Thomsen, H.S.; Volterrani, D. Report of the Radionuclides in Nephrourology Committee on renal clearance. J. Nucl. Med. 1996, 37, 1883–1890. [Google Scholar] [PubMed]
- Latham, G.J. Normalization of microRNA quantitative RT-PCR data in reduced scale experimental designs. Methods Mol. Biol. 2010, 667, 19–31. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameters of Kidney Graft Function | Spearman Correlation to s-Uromodulin | p |
|---|---|---|
| s-Creatinine | −0.698 | <0.001 |
| s-CysC | −0.720 | <0.001 |
| s-Urea | −0.740 | <0.001 |
| eGFR CKD EPI creatinine | 0.736 | <0.001 |
| eGFR CKD EPI CysC | 0.718 | <0.001 |
| eGFR CKD EPI creatinine CysC | 0.758 | <0.001 |
| mGFR 51CrEDTA | 0.669 | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borštnar, Š.; Večerić-Haler, Ž.; Boštjančič, E.; Pipan Tkalec, Ž.; Kovač, D.; Lindič, J.; Kojc, N. Uromodulin and microRNAs in Kidney Transplantation—Association with Kidney Graft Function. Int. J. Mol. Sci. 2020, 21, 5592. https://doi.org/10.3390/ijms21165592
Borštnar Š, Večerić-Haler Ž, Boštjančič E, Pipan Tkalec Ž, Kovač D, Lindič J, Kojc N. Uromodulin and microRNAs in Kidney Transplantation—Association with Kidney Graft Function. International Journal of Molecular Sciences. 2020; 21(16):5592. https://doi.org/10.3390/ijms21165592
Chicago/Turabian StyleBorštnar, Špela, Željka Večerić-Haler, Emanuela Boštjančič, Živa Pipan Tkalec, Damjan Kovač, Jelka Lindič, and Nika Kojc. 2020. "Uromodulin and microRNAs in Kidney Transplantation—Association with Kidney Graft Function" International Journal of Molecular Sciences 21, no. 16: 5592. https://doi.org/10.3390/ijms21165592
APA StyleBorštnar, Š., Večerić-Haler, Ž., Boštjančič, E., Pipan Tkalec, Ž., Kovač, D., Lindič, J., & Kojc, N. (2020). Uromodulin and microRNAs in Kidney Transplantation—Association with Kidney Graft Function. International Journal of Molecular Sciences, 21(16), 5592. https://doi.org/10.3390/ijms21165592