FIB-4 Index and Diabetes Mellitus Are Associated with Chronic Kidney Disease in Japanese Patients with Non-Alcoholic Fatty Liver Disease

 and
and
Abstract
1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Prevalence of Chronic Kidney Disease (CKD) and Associated Factors
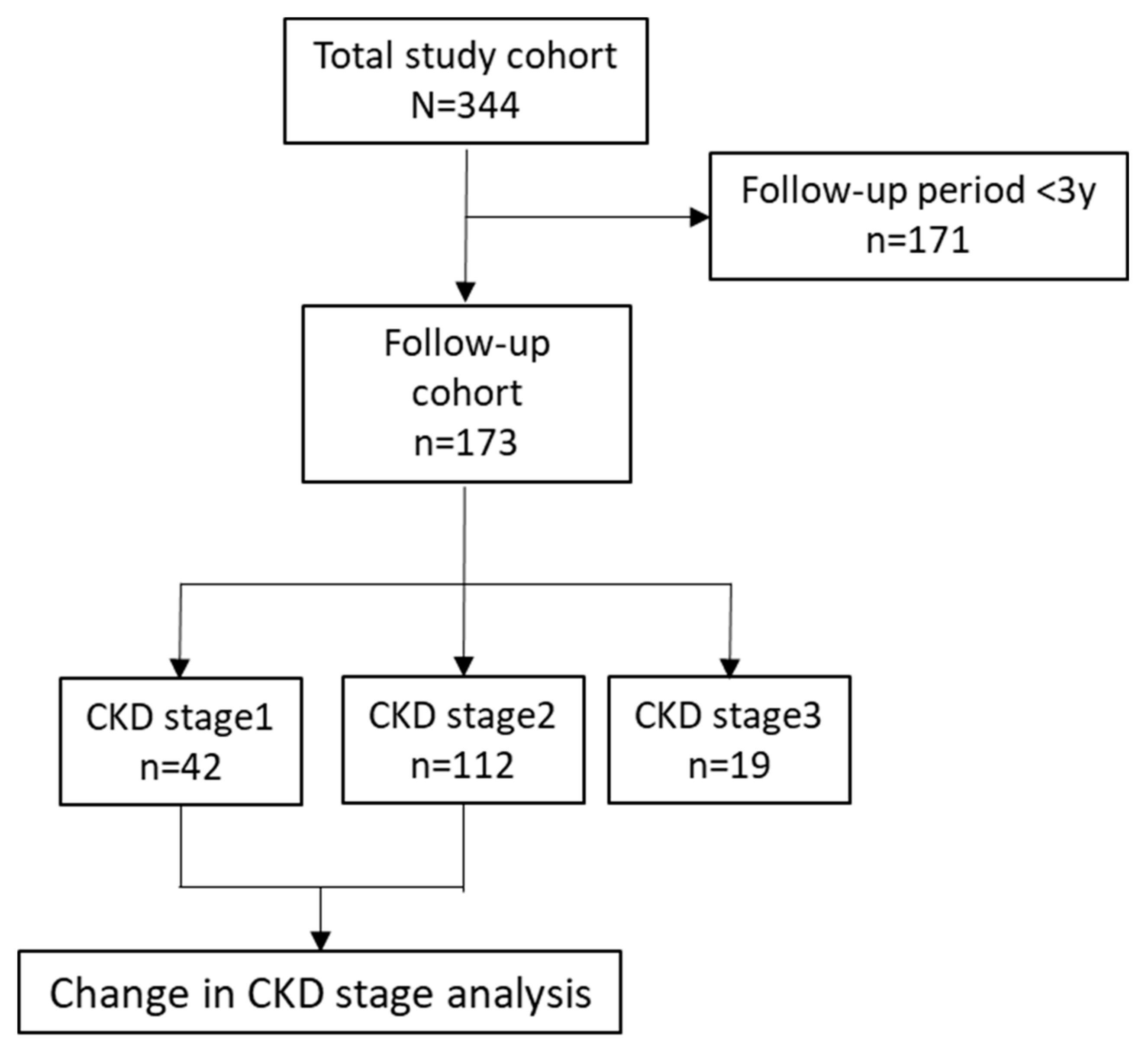
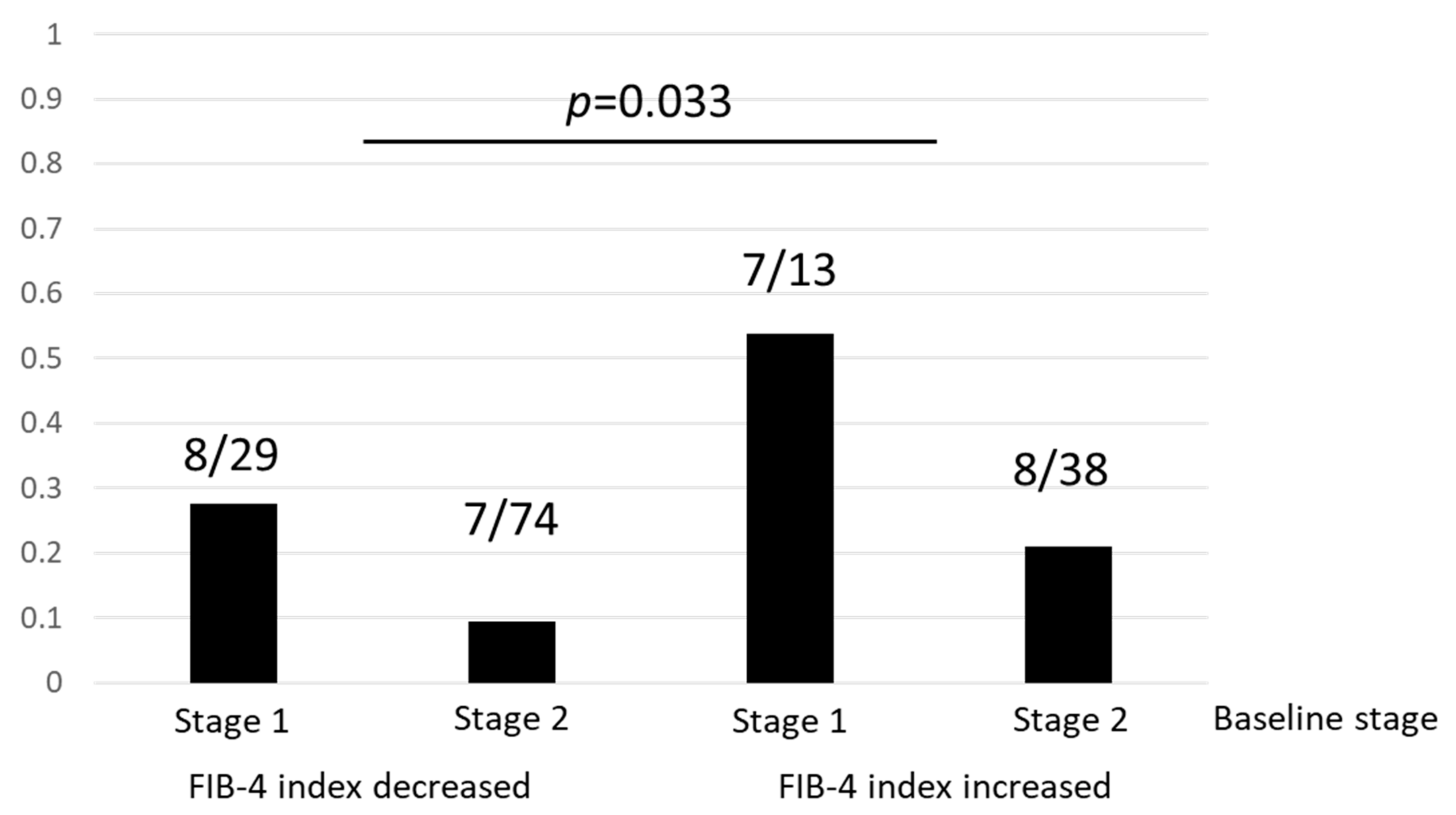
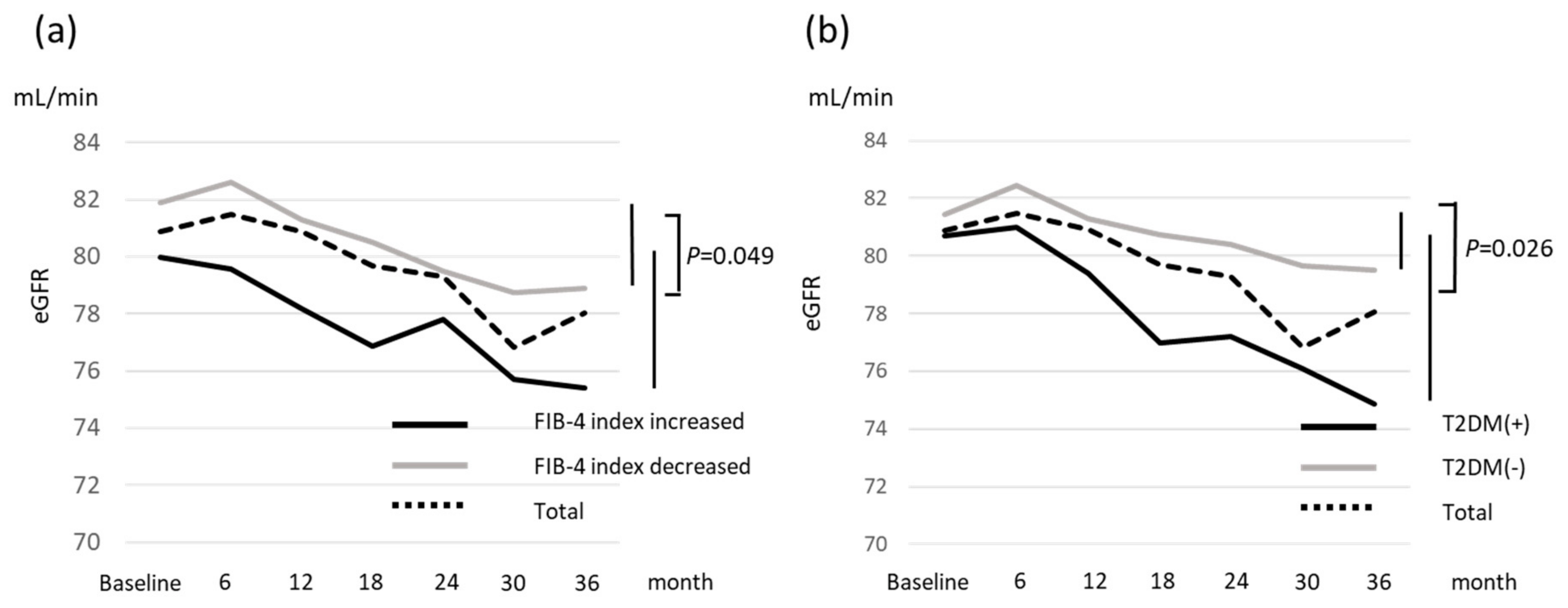
2.3. Change in Renal Function and Risk Factors for Incident CKD
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Laboratory and Clinical Parameters
4.3. DNA Preparation and Single Nucleotide Polymorphism (SNP) Genotyping
4.4. Liver Histology
4.5. Statistical Analysis
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ALT | alanine aminotransferase |
| AST | aspartate aminotransferase |
| BMI | body mass index |
| CI | confidence interval |
| CKD | chronic kidney disease |
| eGFR | estimated glomerular filtration rate |
| FPG | fasting plasma glucose |
| GGT | γ glutamyl transpeptidase |
| HbA1c | hemoglobin A1c |
| HDL-C | high-density lipoprotein cholesterol |
| LDL-C | low-density lipoprotein cholesterol |
| NAFLD | nonalcoholic fatty liver disease |
| NASH | nonalcoholic steatohepatitis |
| OR | odds ratio |
| T2DM | type 2 diabetes mellitus |
| PNPLA3 | patatin-like phospholipase domain containing 3 |
References
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, S.; Hashimoto, E.; Ikejima, K.; Uto, H.; Ono, M.; Sumida, Y.; Nakajima, A. Japanese Society of Gastroenterology; Japan Society of Hepatology. Evidence-based clinical practice guidelines for nonalcoholic fatty liver disease/nonalcoholic steatohepatitis. J. Gastroenterol. 2015, 50, 364–377. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Sanyal, A.J. The diagnosis and management of non-alcoholic fatty liver disease: Practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology 2012, 55, 2005–2023. [Google Scholar] [CrossRef] [PubMed]
- Byrne, C.D.; Targher, G. NAFLD: A multisystem disease. J. Hepatol. 2015, 62, S47–S64. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Byrne, C.D. Non-alcoholic fatty liver disease: An emerging driving force in chronic kidney disease. Nat. Rev. Nephrol. 2017, 13, 297–310. [Google Scholar] [CrossRef] [PubMed]
- Ozturk, K.; Demirci, H.; Kurt, O.; Kantarcioglu, M. Is nonalcoholic fatty liver disease a risk factor for chronic kidney disease? Eur. J. Gastroenterol. Hepatol. 2016, 28, 608–609. [Google Scholar] [CrossRef]
- Marcuccilli, M.; Chonchol, M. NAFLD and chronic kidney disease. Int. J. Mol. Sci. 2016, 17, 562. [Google Scholar] [CrossRef]
- Francque, S.M.; van der Graaff, D.; Kwanten, W.J. Non-alcoholic fatty liver disease and cardiovascular risk: Pathophysiological mechanisms and implications. J. Hepatol. 2016, 65, 425–443. [Google Scholar] [CrossRef]
- Mantovani, A.; Zaza, G.; Byrne, C.D.; Lonardo, A.; Zoppini, G.; Bonora, E.; Targher, G. Nonalcoholic fatty liver disease increases risk of incident chronic kidney disease: A systematic review and meta-analysis. Metabolism 2018, 79, 64–76. [Google Scholar] [CrossRef]
- Arase, Y.; Suzuki, F.; Kobayashi, M.; Suzuki, Y.; Kawamura, Y.; Matsumoto, N.; Hosaka, T. The development of chronic kidney disease in Japanese patients with non-alcoholic fatty liver disease. Intern. Med. 2011, 50, 1081–1087. [Google Scholar] [CrossRef]
- Targher, G.; Chonchol, M.; Bertolini, L.; Rodella, S.; Zenari, L.; Lippi, G.; Muggeo, M. Increased risk of CKD among type 2 diabetics with nonalcoholic fatty liver disease. J. Am. Soc. Nephrol. 2008, 19, 1564–1570. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Mantovani, A.; Pichiri, I.; Mingolla, L.; Cavalieri, V.; Mantovani, W.; Byrne, C.D. Nonalcoholic fatty liver disease is independently associated with an increased incidence of chronic kidney disease in patients with type 1 diabetes. Diabetes Care 2014, 37, 1729–1736. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Ryu, S.; Sung, E.; Woo, H.Y.; Oh, E.; Cha, K.; Kim, W.S. Nonalcoholic fatty liver disease predicts chronic kidney disease in nonhypertensive and nondiabetic Korean men. Metabolism 2008, 57, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Sinn, D.H.; Kang, D.; Jang, H.R.; Gu, S.; Cho, S.J.; Paik, S.W.; Cho, J. Development of chronic kidney disease in patients with non-alcoholic fatty liver disease: A cohort study. J. Hepatol. 2017, 67, 1274–1280. [Google Scholar] [CrossRef] [PubMed]
- Yasui, K.; Sumida, Y.; Mori, Y.; Mitsuyoshi, H.; Minami, M.; Itoh, Y.; Yoshikawa, T. Nonalcoholic steatohepatitis and increased risk of chronic kidney disease. Metabolism 2011, 60, 735–739. [Google Scholar] [CrossRef] [PubMed]
- Yun, H.R.; Kim, H.; Park, J.T.; Chang, T.I.; Yoo, T.H.; Kang, S.W.; Oh, K.H. Obesity, Metabolic Abnormality, and Progression of CKD. Am. J. Kidney Dis. 2018, 72, 400–410. [Google Scholar] [CrossRef]
- Kittiskulnam, P.; Thokanit, N.S.; Katavetin, P.; Susanthitaphong, P.; Srisawat, N.; Praditpornsilpa, K.; Eiam-Ong, S. The magnitude of obesity and metabolic syndrome among diabetic chronic kidney disease population: A nationwide study. PLoS ONE 2018, 13, e0196332. [Google Scholar] [CrossRef]
- Hashimoto, Y.; Tanaka, M.; Okada, H.; Senmaru, T.; Hamaguchi, M.; Asano, M.; Nakamura, N. Metabolically healthy obesity and risk of incident CKD. Clin. J. Am. Soc. Nephrol. 2015, 10, 578–583. [Google Scholar] [CrossRef]
- Yamagata, K.; Ishida, K.; Sairenchi, T.; Takahashi, H.; Ohba, S.; Shiigai, T.; Koyama, A. Risk factors for chronic kidney disease in a community-based population: A 10-year follow-up study. Kidney Int. 2007, 71, 159–166. [Google Scholar] [CrossRef]
- Targher, G.; Bertolini, L.; Rodella, S.; Lippi, G.; Zoppini, G.; Chonchol, M. Relationship between kidney function and liver histology in subjects with nonalcoholic steatohepatitis. Clin. J. Am. Soc. Nephrol. 2010, 5, 2166–2171. [Google Scholar] [CrossRef]
- Yilmaz, Y.; Alahdab, Y.O.; Yonal, O.; Kurt, R.; Kedrah, A.E.; Celikel, C.A.; Kalayci, C. Microalbuminuria in nondiabetic patients with nonalcoholic fatty liver disease: Association with liver fibrosis. Metabolism 2010, 59, 1327–1330. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.C.; Kao, W.Y.; Cheng, Y.L.; Wang, Y.J.; Hou, M.C.; Wu, J.C.; Su, C.W. The correlation between fatty liver disease and chronic kidney disease. J. Formos. Med. Assoc. 2019. [Google Scholar] [CrossRef] [PubMed]
- Imai, E.; Horio, M.; Yamagata, K.; Iseki, K.; Hara, S.; Ura, N.; Matsuo, S. Slower decline of glomerular filtration rate in the Japanese general population: A longitudinal 10-year follow-up study. Hypertens. Res. 2008, 31, 433–441. [Google Scholar] [CrossRef]
- Guebre-Egziabher, F.; Alix, P.M.; Koppe, L.; Pelletier, C.C.; Kalbacher, E.; Fouque, D.; Soulage, C.O. Ectopic lipid accumulation: A potential cause for metabolic disturbances and a contributor to the alteration of kidney function. Biochimie 2013, 95, 1971–1979. [Google Scholar] [CrossRef] [PubMed]
- Ix, J.H.; Sharma, K. Mechanisms linking obesity, chronic kidney disease, and fatty liver disease: The roles of fetuin-A, adiponectin, and AMPK. J. Am. Soc. Nephrol. 2010, 21, 406–412. [Google Scholar] [CrossRef]
- Foster, M.C.; Hwang, S.J.; Porter, S.A.; Massaro, J.M.; Hoffmann, U.; Fox, C.S. Fatty kidney, hypertension, and chronic kidney disease: The Framingham Heart Study. Hypertension 2011, 58, 784–790. [Google Scholar] [CrossRef]
- Lim, S. Ectopic fat assessment focusing on cardiometabolic and renal risk. Endocrinol. Metab. 2014, 29, 1–4. [Google Scholar] [CrossRef]
- Sun, D.Q.; Zheng, K.I.; Xu, G.; Ma, H.L.; Zhang, H.Y.; Pan, X.Y.; Chen, Y.P. PNPLA3 rs738409 is associated with renal glomerular and tubular injury in NAFLD patients with persistently normal ALT levels. Liver Int. 2019, 13. [Google Scholar] [CrossRef]
- Stevens, L.A.; Coresh, J.; Greene, T.; Levey, A.S. Assessing kidney function–measured and estimated glomerular filtration rate. N. Engl. J. Med. 2006, 354, 2473–2483. [Google Scholar] [CrossRef]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Hishida, A. Collaborators developing the Japanese equation for estimated GFR. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. Kidney Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef]
- Matteoni, C.A.; Younossi, Z.M.; Gramlich, T.; Boparai, N.; Liu, Y.C.; McCullough, A.J. Nonalcoholic fatty liver diseases: A spectrum of clinical and pathological severity. Gastroenterology 1999, 116, 1413–1419. [Google Scholar] [CrossRef]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Yeh, M. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef] [PubMed]
- Brunt, E.M.; Janney, C.G.; Di Bisceglie, A.M.; Neuschwander-Tetri, B.A.; Bacon, B.R. Nonalcoholic steatohepatitis: A proposal for grading and staging the histological lesions. Am. J. Gastroenterol. 1999, 94, 2467–2474. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total Cohort (n = 344) | Follow-Up Cohort (n = 173) | ||
|---|---|---|---|---|
| Baseline | 3 Years Later | p | ||
| NASH | 255 (74.1%) | 129 (74.6%) | ||
| Hypertension | 145 (42.2%) | 79 (45.7%) | ||
| T2DM | 143 (41.6%) | 73 (42.2%) | ||
| Hyperlipidemia | 209 (60.8%) | 126 (72.8%) | ||
| Sex, female | 179 (52.0%) | 88 (50.9%) | ||
| Age, year | 57 (22–84) | 57 (25–79) | 59 (28–82) | |
| BMI, kg/m2 | 27.0 (17.7–45.4) | 26.8 (17.7–40.3) | 26.7 (17.1–44.6) | 0.003 |
| Albumin, g/dL | 4.5 (3.4–7.2) | 4.5 (3.4–5.6) | 4.4 (2.8–5.1) | <0.001 |
| AST, IU/L | 43 (13–650) | 42 (12–208) | 31 (12–212) | <0.001 |
| ALT, IU/L | 57 (10–615) | 58 (10–263) | 36 (11–248) | <0.001 |
| GGT, IU/L | 64 (13–716) | 66 (14–355) | 40 (12–565) | <0.001 |
| Platelet count, × 103/μL | 217 (75–457) | 210 (75–457) | 214 (44–507) | 0.004 |
| Total cholesterol, mg/dL | 199 (95–347) | 203 (123–304) | 194 (109–306) | 0.009 |
| Triglyceride, mg/dL | 141 (10–923) | 146 (10–739) | 133 (46–574) | 0.010 |
| LDL-C, mg/dL | 123 (36–435) | 125 (48–435) | 118 (54–213) | 0.012 |
| HDL-C, mg/dL | 52 (16–107) | 52 (25–107) | 51 (22–95) | 0.878 |
| FPG, mg/dL | 107 (61–374) | 105 (61–325) | 114 (72–349) | 0.167 |
| HbA1c, % | 6.1 (4.7–11.0) | 6.1 (5.0–11.0) | 6.1 (5.1–11.1) | 0.338 |
| FIB-4 index | 1.53 (0.26–11.06) | 1.49 (0.27–7.84) | 1.43 (0.30–13.64) | <0.001 |
| eGFR, mL/min/1.73 m2 | 78.7 (37.2–165.4) | 80.0 (40.9–154.9) | 75.5 (31.0–142.4) | <0.001 |
| CKD stage 1/2/3 | 84/225/35 | 42/112/19 | 37/107/29 | <0.001 |
| Type IV collagen 7s, ng/mL | 5.0 (2.4–12.0) | 4.9 (2.4–12.0) | 4.8 (2.5–11.0) | 0.002 |
| Fibrosis stage (0/1/2/3/4) | 120/109/61/38/16 | 65/50/34/13/11 | ||
| Steatosis (1/2/3) | 99/185/60 | 37/107/29 | ||
| Inflammation (0/1/2/3) | 14/200/110/20 | 5/99/55/14 | ||
| Ballooning (0/1/2) | 105/144/95 | 46/67/60 | ||
| PNPLA3, CC/CG/GG | 56/110/116 | 34/60/73 | ||
| Variable | Multivariate Analysis | |
|---|---|---|
| OR (95% CI) a | p Value | |
| Sex (male) | 5.46 (2.35–12.70) | <0.001 |
| Age (per 1 year) | 1.07 (1.02–1.12) | 0.003 |
| BMI (per 1 kg/m2) | 0.94 (0.85–1.05) | 0.272 |
| NAS steatosis (2, 3, 4) | 0.84 (0.37–1.89) | 0.665 |
| NAS inflammation (3) | 1.86 (0.52–6.68) | 0.344 |
| FIB-4 index (≥1.30) | 3.85 (1.09–13.54) | 0.036 |
| Variable | Deterioration of CKD Stage | Incident CKD | ||||
|---|---|---|---|---|---|---|
| Yes (n = 30) | No (n = 124) | p | Yes (n = 15) | No (n = 139) | p | |
| NASH | 20 (66.7%) | 94 (75.8%) | 0.355 | 11 (73.3%) | 103 (74.1%) | 1.000 |
| Hypertension | 17 (56.7%) | 51 (41.1%) | 0.153 | 11 (73.3%) | 57 (41.0%) | 0.026 |
| Diabetes mellitus | 19 (63.3%) | 50 (40.3%) | 0.026 | 14 (93.3%) | 55 (39.6%) | <0.01 |
| Hyperlipidemia | 24 (80.0%) | 88 (71.0%) | 0.369 | 12 (80.0%) | 100 (71.9%) | 0.761 |
| Sex, female | 15 (50.0%) | 69 (55.6%) | 0.684 | 7 (46.7%) | 77 (55.4%) | 0.591 |
| Age, year | 57 (25–78) | 55 (25–79) | 0.290 | 57 (45–78) | 55 (25–79) | 0.115 |
| BMI, kg/m2 | 27.4 (17.9–40.3) | 26.9 (17.7–39.0) | 0.804 | 26.2 (22.0–31.0) | 27.1 (17.7–40.3) | 0.715 |
| Albumin, g/dL | 4.5 (3.7–5.0) | 4.5 (3.4–5.6) | 0.790 | 4.5 (3.8–4.8) | 4.5 (3.4–5.6) | 0.648 |
| AST, IU/L | 42 (24–104) | 42 (12–208) | 0.786 | 45 (24–104) | 42 (12–208) | 0.853 |
| ALT, IU/L | 59.5 (31–150) | 61 (10–263) | 0.967 | 61 (31–138) | 61 (10–263) | 0.891 |
| GGT, IU/L | 66.5 (21–198) | 67.5 (14–349) | 0.814 | 80 (31–198) | 66 (14–349) | 0.304 |
| Platelet count, × 103/μL | 201.5 (117–323) | 221 (99–457) | 0.256 | 168 (117–322) | 221 (99–457) | 0.071 |
| Total cholesterol, mg/dL | 212.5 (128–267) | 202 (127–304) | 0.266 | 216 (133–267) | 202.5 (127–304) | 0.538 |
| Triglyceride, mg/dL | 154.5 (50–739) | 143.5 (10–584) | 0.403 | 151 (68–739) | 146 (10–584) | 0.391 |
| LDL-C, mg/dL | 137 (92–177) | 125 (66–435) | 0.217 | 126 (92–169) | 126 (66–435) | 0.993 |
| HDL-C, mg/dL | 48.5 (30–84) | 53.5 (25–107) | 0.137 | 45 (30–72) | 53 (25–107) | 0.007 |
| FPG, mg/dL | 102.5 (72–212) | 105.5 (61–325) | 0.971 | 145 (72–212) | 105 (61–325) | 0.043 |
| HbA1c, % | 6.1 (5.3–8.9) | 6.1 (5.0–11.0) | 0.675 | 6.5 (5.9–8.9) | 6.1 (5.0–11.0) | 0.058 |
| FIB-4 index | 1.50 (0.40–4.44) | 1.42 (0.27–7.84) | 0.635 | 2.00 (0.61–4.44) | 1.40 (0.27–7.84) | 0.115 |
| eGFR, mL/min/1.73 m2 | 88.7 (61.6–106.0) | 80.8 (61.1–154.9) | 0.967 | 66.6 (61.6–86.4) | 81.4 (61.1–154.9) | <0.01 |
| CKD stage 1/2 | 15/15 | 27/97 | 0.003 | 0/15 | 42/97 | 0.012 |
| Type IV collagen 7s, ng/mL | 4.5 (3.1–12.0) | 5.0 (2.4–12.0) | 0.792 | 4.5 (2.4–12.0) | 4.9 (2.4–12.0) | 0.601 |
| Fibrosis stage (0/1/2/3/4) | 13/6/5/5/1 | 46/37/28/5/8 | 0.099 | 6/4/3/1/1 | 55/39/30/9/8 | 1.000 |
| Steatosis (1/2/3) | 5/22/3 | 26/74/24 | 0.341 | 3/9/3 | 28/87/24 | 0.964 |
| Inflammation (0/1/2/3) | 0/18/10/2 | 5/71/41/7 | 0.733 | 0/9/4/2 | 5/80/47/7 | 0.502 |
| Ballooning (0/1/2) | 10/10/10 | 31/50/43 | 0.623 | 4/5/6 | 37/55/47 | 0.867 |
| ΔBMI | −0.2 (−3.6–4.3) | −0.3 (−9.6–5.2) | 0.841 | 0.1 (−3.6–1.3) | 0.3 (−9.6–5.2) | 0.528 |
| ΔAST | −8.5 (−58–27) | −8 (−172–125) | 0.575 | –13 (−58–27) | –8 (−172–125) | 0.798 |
| ΔALT | −17.5 (−118–64) | −16 (−216–109) | 0.743 | –20 (−61–64) | –15 (−216–109) | 0.961 |
| ΔHbA1c | 0.1 (−2.1–1.3) | 0.1 (−3.2–2.6) | 0.828 | –0.4 (−2.1–1.3) | 0.1 (−3.2–2.6) | 0.142 |
| ΔFIB-4 index | 0.01 (−1.94–2.44) | −0.10 (−4.92–1.25) | 0.106 | 0.10 (−1.94–2.44) | –0.10 (−4.92–1.25) | 0.151 |
| PNPLA3, CC/CG/GG | 4/12/12 | 24/44/52 | 0.712 | 1/6/6 | 27/50/58 | 0.166 |
| Variable | Deterioration of CKD Stage | Development of CKD | ||
|---|---|---|---|---|
| OR (95% CI) a | p Value | OR (95% CI) a | p Value | |
| Sex | 0.656 | 0.899 | ||
| Age, year | 0.464 | 0.535 | ||
| T2DM | 2.44 (1.01–5.91) | 0.047 | 21.54 (2.50–185.33) | 0.005 |
| Hypertension | 0.335 | 0.379 | ||
| FIB-4 index at baseline | 0.292 | 0.708 | ||
| eGFR at baseline, mL/min | 0.783 | 0.88 (0.81–0.95) | 0.001 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seko, Y.; Yano, K.; Takahashi, A.; Okishio, S.; Kataoka, S.; Okuda, K.; Mizuno, N.; Takemura, M.; Taketani, H.; Umemura, A.; et al. FIB-4 Index and Diabetes Mellitus Are Associated with Chronic Kidney Disease in Japanese Patients with Non-Alcoholic Fatty Liver Disease. Int. J. Mol. Sci. 2020, 21, 171. https://doi.org/10.3390/ijms21010171
Seko Y, Yano K, Takahashi A, Okishio S, Kataoka S, Okuda K, Mizuno N, Takemura M, Taketani H, Umemura A, et al. FIB-4 Index and Diabetes Mellitus Are Associated with Chronic Kidney Disease in Japanese Patients with Non-Alcoholic Fatty Liver Disease. International Journal of Molecular Sciences. 2020; 21(1):171. https://doi.org/10.3390/ijms21010171
Chicago/Turabian StyleSeko, Yuya, Kohta Yano, Aya Takahashi, Shinya Okishio, Seita Kataoka, Keiichiroh Okuda, Naoki Mizuno, Masashi Takemura, Hiroyoshi Taketani, Atsushi Umemura, and et al. 2020. "FIB-4 Index and Diabetes Mellitus Are Associated with Chronic Kidney Disease in Japanese Patients with Non-Alcoholic Fatty Liver Disease" International Journal of Molecular Sciences 21, no. 1: 171. https://doi.org/10.3390/ijms21010171
APA StyleSeko, Y., Yano, K., Takahashi, A., Okishio, S., Kataoka, S., Okuda, K., Mizuno, N., Takemura, M., Taketani, H., Umemura, A., Nishikawa, T., Yamaguchi, K., Moriguchi, M., Okanoue, T., & Itoh, Y. (2020). FIB-4 Index and Diabetes Mellitus Are Associated with Chronic Kidney Disease in Japanese Patients with Non-Alcoholic Fatty Liver Disease. International Journal of Molecular Sciences, 21(1), 171. https://doi.org/10.3390/ijms21010171