
Right- vs. Left-Sided Metastatic Colorectal Cancer: Differences in Tumor Biology and Bevacizumab Efficacy


 ,
,  ,
, 
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
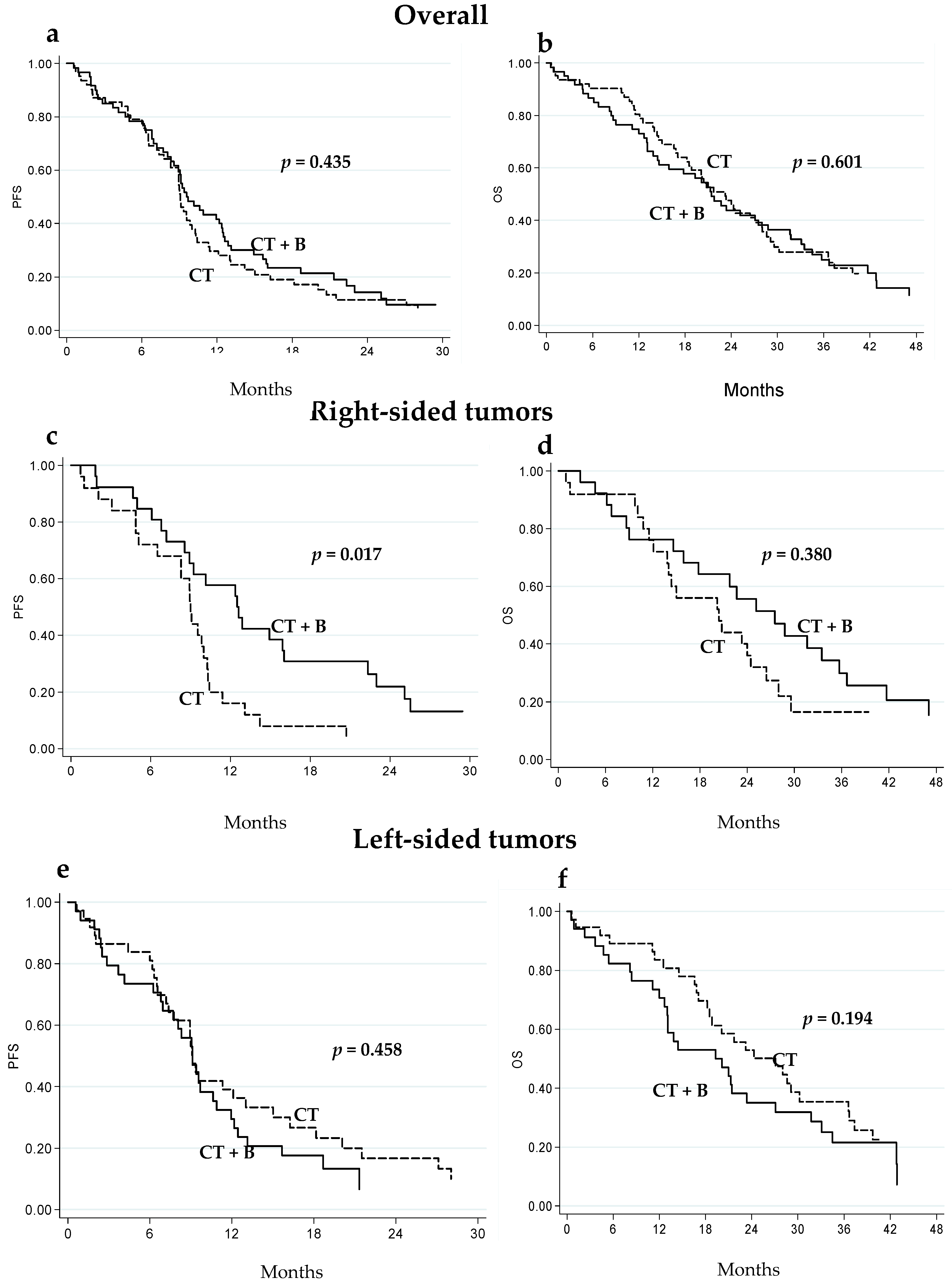
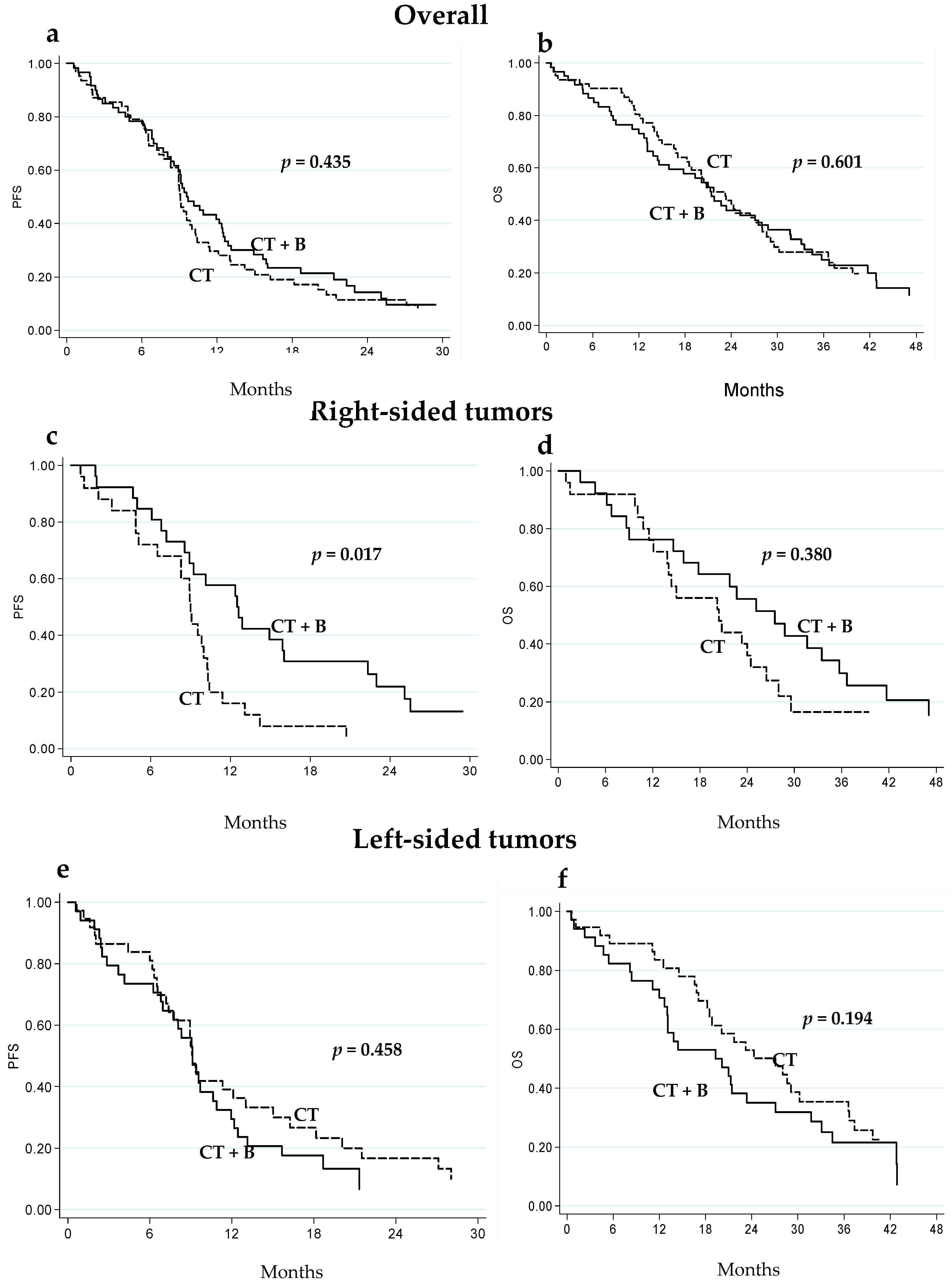
2.2. Clinical Outcome in Relation to Tumor Localization
2.3. Circulating Biomarkers in Right-Aided and Left-Sided Tumors
2.4. eNOS and VEGF Polymorphism Distribution in Relation to Tumor Localization
2.5. RAS and BRAF Mutation Profile
3. Discussion
4. Materials and Methods
4.1. Case Series
4.2. Biomarker Analysis
4.3. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| mCRC | Metastatic colorectal cancer |
| CT | Chemotherapy |
| B | Bevacizumab |
| VEGF | Vascular endothelial growth factor |
| eNOS | Endothelial nitric oxide synthase |
| COX2 | Cyclooxygenase-2 |
| EPHB4 | Ephrin type-B receptor 4 |
| HIF-1 | Hypoxia-inducible factor 1 |
| LDH | Lactate dehydrogenase |
| hs-CRP | High-sensitivity C-reactive protein |
| NLR | Neutrophil-lymphocyte ratio |
| PLR | Platelet-lymphocyte ratio |
| SII | Systemic immune-inflammation index |
| PFS | Progression-free survival |
| OS | Overall survival |
References
- Benedix, F.; Kube, R.; Meyer, F.; Schmidt, U.; Gastinger, I.; Lippert, H. Colon/rectum carcinomas (primary tumor) study group. Comparison of 17,641 patients with right- and left-sided colon cancer: differences in epidemiology, perioperative course, histology, and survival. Dis. Colon Rectum 2010, 53, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Missiaglia, E.; Jacobs, B.; D’Ario, G.; di Narzo, A.F.; Soneson, C.; Budinska, E.; Popovici, V.; Vecchione, L.; Gerster, S.; Yan, P.; et al. Distal and proximal colon cancers differ in terms of molecular, pathological, and clinical features. Ann. Oncol. 2014, 25, 1995–2001. [Google Scholar] [CrossRef] [PubMed]
- Tejpar, S.; Stintzing, S.; Ciardiello, F.; Tabernero, J.; van Cutsem, E.; Beier, F.; Esser, R.; Lenz, H.J.; Heinemann, V. Prognostic and predictive relevance of primary tumor location in patients with RAS wild-type metastatic colorectal cancer: Retrospective analyses of the CRYSTAL and FIRE-3 trials. JAMA Oncol. 2017, 3, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Guinney, J.; Dienstmann, R.; Wang, X.; de Reynies, A.; Schlicker, A.; Soneson, C.; Marisa, L.; Roepman, P.; Nyamundanda, G.; Angelino, P.; et al. The consensus molecular subtypes of colorectal cancer. Nat. Med. 2015, 21, 1350–1356. [Google Scholar] [CrossRef] [PubMed]
- Boisen, M.K.; Johansen, J.S.; Dehlendorff, C.; Larsen, J.S.; Osterlind, K.; Hansen, J.; Nielsen, S.E.; Pfeiffer, P.; Tarpgaard, L.S.; Hollander, N.H.; et al. Primary tumor location and bevacizumab effectiveness in patients with metastatic colorectal cancer. Ann. Oncol. 2013, 24, 2554–2559. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Bai, L.; Liu, T.S.; Yu, Y.Y.; He, M.M.; Liu, K.Y.; Luo, H.Y.; Zhang, D.S.; Jin, Y.; Wang, F.H.; et al. Right-sided colon cancer and left-sided colorectal cancers respond differently to cetuximab. Chin. J. Cancer 2015, 34, 384–393. [Google Scholar] [CrossRef] [PubMed]
- Brule, S.Y.; Jonker, D.J.; Karapetis, C.S.; O’Callaghan, C.J.; Moore, M.J.; Wong, R.; Tebbutt, N.C.; Underhill, C.; Yip, D.; Zalcberg, J.R.; et al. Location of colon cancer (right-sided versus left-sided) as a prognostic factor and a predictor of benefit from cetuximab in NCIC CO.17. Eur. J. Cancer 2015, 51, 1405–1414. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.H.; Shao, Y.Y.; Chen, H.M.; Lin, Y.L.; Lin, Z.Z.; Lai, M.S.; Cheng, A.L.; Yeh, K.H. Primary tumor site is a useful predictor of cetuximab efficacy in the third-line or salvage treatment of KRAS wild-type (exon 2 non-mutant) metastatic colorectal cancer: A nationwide cohort study. BMC Cancer 2016, 16, 327. [Google Scholar] [CrossRef] [PubMed]
- Moretto, R.; Cremolini, C.; Rossini, D.; Pietrantonio, F.; Battaglin, F.; Mennitto, A.; Bergamo, F.; Loupakis, F.; Marmorino, F.; Berenato, R.; et al. Location of primary tumor and benefit from anti-epidermal growth factor receptor monoclonal antibodies in patients with RAS and BRAF wild-type metastatic colorectal cancer. Oncologist 2016, 21, 988–994. [Google Scholar] [CrossRef] [PubMed]
- Holch, J.W.; Ricard, I.; Stintzing, S.; Modest, D.P.; Heinemann, V. The relevance of primary tumour location in patients with metastatic colorectal cancer: A meta-analysis of first-line clinical trials. Eur. J. Cancer 2017, 70, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Menter, D.G.; Kopetz, S. Right versus left colon cancer biology: Integrating the consensus molecular subtypes. J. Natl. Compr. Canc. Netw. 2017, 15, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Loupakis, F.; Yang, D.; Yau, L.; Feng, S.; Cremolini, C.; Zhang, W.; Maus, M.K.; Antoniotti, C.; Langer, C.; Scherer, S.J.; et al. primary tumor location as a prognostic factor in metastatic colorectal cancer. J. Natl. Cancer Inst. 2015, 107, dju427. [Google Scholar] [CrossRef] [PubMed]
- Venook, A.; Niedzwiecki, D.; Innocenti, F.; Fruth, B.; Greene, C.; O’Neil, B.; Shaw, J.; Atkins, J.; Horvath, L.; Polite, B.; et al. Impact of primary (1°) tumor location on overall survival (OS) and progression-free survival (PFS) in patients (pts) with metastatic colorectal cancer (mCRC): Analysis of CALGB/SWOG 80405 (Alliance). J. Clin. Oncol. 2016, 34, 3504. [Google Scholar]
- He, W.Z.; Liao, F.X.; Jiang, C.; Kong, P.F.; Yin, C.X.; Yang, Q.; Qiu, H.J.; Zhang, B.; Xia, L.P. Primary tumor location as a predictive factor for first-line bevacizumab effectiveness in metastatic colorectal cancer patients. J. Cancer 2017, 8, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Ulivi, P.; Scarpi, E.; Passardi, A.; Marisi, G.; Calistri, D.; Zoli, W.; del Re, M.; Frassineti, G.L.; Tassinari, D.; Tamberi, S.; et al. ENOS polymorphisms as predictors of efficacy of bevacizumab-based chemotherapy in metastatic colorectal cancer: Data from a randomized clinical trial. J. Transl. Med. 2015, 13, 258. [Google Scholar] [CrossRef] [PubMed]
- Passardi, A.; Scarpi, E.; Tamberi, S.; Cavanna, L.; Tassinari, D.; Fontana, A.; Pini, S.; Bernardini, I.; Accettura, C.; Ulivi, P.; et al. Impact of pre-treatment lactate dehydrogenase levels on prognosis and bevacizumab efficacy in patients with metastatic colorectal cancer. PLoS ONE 2015, 10, e0134732. [Google Scholar] [CrossRef] [PubMed]
- Casadei Gardini, A.; Carloni, S.; Scarpi, E.; Maltoni, P.; Dorizzi, R.M.; Passardi, A.; Frassineti, G.L.; Cortesi, P.; Giannini, M.B.; Marisi, G.; et al. Prognostic role of serum concentrations of high-sensitivity C-reactive protein in patients with metastatic colorectal cancer: results from the ITACa trial. Oncotarget 2016, 7, 10193–10202. [Google Scholar] [PubMed]
- Passardi, A.; Scarpi, E.; Cavanna, L.; Dall’Agata, M.; Tassinari, D.; Leo, S.; Bernardini, I.; Gelsomino, F.; Tamberi, S.; Brandes, A.A.; et al. Inflammatory indexes as predictors of prognosis and bevacizumab efficacy in patients with metastatic colorectal cancer. Oncotarget 2016, 7, 33210–33219. [Google Scholar] [CrossRef] [PubMed]
- Marisi, G.; Scarpi, E.; Passardi, A.; Nanni, O.; Ragazzini, A.; Valgiusti, M.; Frassineti, G.; Amadori, D.; Ulivi, P. Prognostic and predictive role of circulating eNOS and EPHB4 in metastatic colorectal cancer patients receiving bevacizumab. J. Clin. Oncol. 2016, 34, e23083. [Google Scholar]
- Marisi, G.; Scarpi, E.; Passardi, A.; Nanni, O.; Ragazzini, A.; Valgiusti, M.; Casadei Gardini, A.; Neri, L.; Frassineti, G.; Amadori, D.; et al. Circulating VEGF and eNOS variations as predictors of outcome in metastatic colorectal cancer patients receiving bevacizumab. Sci. Rep. 2017, 7, 1293. [Google Scholar] [CrossRef] [PubMed]
- Passardi, A.; Nanni, O.; Tassinari, D.; Turci, D.; Cavanna, L.; Fontana, A.; Ruscelli, S.; Mucciarini, C.; Lorusso, V.; Ragazzini, A.; et al. Effectiveness of bevacizumab added to standard chemotherapy in metastatic colorectal cancer: Final results for first-line treatment from the ITACa randomized clinical trial. Ann. Oncol. 2015, 26, 1201–1207. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; McGuffey, E.J.; Morris, J.S.; Manyam, G.; Baladandayuthapani, V.; Wei, W.; Morris, V.K.; Overman, M.J.; Maru, D.M.; Jiang, Z.Q.; et al. Association of CpG island methylator phenotype and EREG/AREG methylation and expression in colorectal cancer. Br. J. Cancer 2016, 114, 1352–1361. [Google Scholar] [CrossRef] [PubMed]
- De Smedt, L.; Lemahieu, J.; Palmans, S.; Govaere, O.; Tousseyn, T.; van Cutsem, E.; Prenen, H.; Tejpar, S.; Spaepen, M.; Matthijs, G.; et al. Microsatellite instable vs stable colon carcinomas: analysis of tumour heterogeneity, inflammation and angiogenesis. Br. J. Cancer 2015, 113, 500–509. [Google Scholar] [CrossRef] [PubMed]
- Mima, K.; Nowak, J.A.; Qian, Z.R.; Cao, Y.; Song, M.; Masugi, Y.; Shi, Y.; da Silva, A.; Gu, M.; Li, W.; et al. Tumor LINE-1 methylation level and colorectal cancer location in relation to patient survival. Oncotarget 2016, 7, 55098–55109. [Google Scholar] [CrossRef] [PubMed]
- Inamura, K.; Yamauchi, M.; Nishihara, R.; Lochhead, P.; Qian, Z.R.; Kuchiba, A.; Kim, S.A.; Mima, K.; Sukawa, Y.; Jung, S.; et al. Tumor LINE-1 methylation level and microsatellite instability in relation to colorectal cancer prognosis. J. Natl. Cancer Inst. 2014, 106. [Google Scholar] [CrossRef] [PubMed]
- Dejea, C.M.; Wick, E.C.; Hechenbleikner, E.M.; White, J.R.; Mark Welch, J.L.; Rossetti, B.J.; Peterson, S.N.; Snesrud, E.C.; Borisy, G.G.; Lazarev, M.; et al. Microbiota organization is a distinct feature of proximal colorectal cancers. Proc. Natl. Acad. Sci. USA 2014, 111, 18321–18326. [Google Scholar] [CrossRef] [PubMed]
- Casadei Gardini, A.; Capelli, L.; Ulivi, P.; Giannini, M.; Freier, E.; Tamberi, S.; Scarpi, E.; Passardi, A.; Zoli, W.; Ragazzini, A.; et al. KRAS, BRAF and PIK3CA status in squamous cell anal carcinoma (SCAC). PLoS ONE 2014, 9, e92071. [Google Scholar] [CrossRef] [PubMed]
- Capelli, L.; Casadei Gardini, A.; Scarpi, E.; Frassineti, G.L.; Saragoni, L.; Puccetti, M.; Scartozzi, M.; Giannini, M.; Tamberi, S.; Corbelli, J.; et al. No evidence of NRAS mutation in squamous cell anal carcinoma (SCAC). Sci. Rep. 2016, 6, 37621. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Total (n = 122) | ||
|---|---|---|
| Patient characteristics | Right-sided (n = 51) No. (%) | Left-sided (n = 71) No. (%) |
| Median age, years (range) | 68 (37–83) | 63 (34–82) |
| Gender | ||
| Male | 28 (54.9) | 42 (59.1) |
| Female | 23 (45.1) | 29 (40.9) |
| Performance Status (ECOG) | ||
| 0 | 43 (84.3) | 57 (80.3) |
| 1 + 2 | 8 (15.7) | 14 (19.7) |
| Stage at diagnosis | ||
| I–III | 8 (15.7) | 20 (28.2) |
| IV | 43 (84.3) | 51 (71.8) |
| Grading | ||
| 1 + 2 | 22 (48.9) | 43 (68.2) |
| 3 | 23 (51.1) | 20 (31.7) |
| Histological type | ||
| Adenocarcinoma NOS | 51 (100.0) | 68 (95.8) |
| Mucinous cancer | 0 | 3 (4.2) |
| CT regimen | ||
| FOLFOX4 | 31 (60.8) | 44 (62.0) |
| FOLFIRI | 20 (39.2) | 27 (38.0) |
| Prior cancer therapy | ||
| Surgery | 45 (88.2) | 50 (70.4) |
| Radiotherapy | 0 | 12 (16.9) |
| Adjuvant CT | 10 (19.6) | 8 (11.3) |
| Treatment group | ||
| CT + B | 26 (51.0) | 34 (47.9) |
| CT | 25 (49.0) | 37 (52.1) |
| PFS | OS | ||||||
|---|---|---|---|---|---|---|---|
| No. Patients | No. Events | Median PFS (months) (95% CI) | p | No. Events | Median OS (months) (95% CI) | p | |
| Overall | |||||||
| CT + B | 60 | 53 | 9.6 (8.3–12.4) | 49 | 21.4 (14.4–28.8) | ||
| CT | 62 | 56 | 9.1 (8.3–10.0) | 0.435 | 49 | 23.2 (18.2–28.0) | 0.601 |
| Right-sided | |||||||
| CT + B | 26 | 23 | 12.6 (8.6–16.0) | 21 | 27.5 (15.9–35.7) | ||
| CT | 25 | 24 | 9.0 (6.5–10.3) | 0.017 | 20 | 20.4 (13.8–26.4) | 0.380 |
| Left-sided | |||||||
| CT + B | 34 | 30 | 9.1 (6.8–10.9) | 28 | 19.7 (12.7–27.1) | ||
| CT | 37 | 32 | 9.1 (7.2–13.0) | 0.458 | 29 | 27.1 (18.2–36.6) | 0.194 |
| Biomarker | Right-Sided | Left-Sided | p |
|---|---|---|---|
| Median Value (Range) | Median Value (Range) | ||
| VEGF | 2.36 (0.68–37.69) | 2.22 (0.54–50.80) | 0.194 |
| COX | 1.37 (0.34–6.07) | 1.12 (0.37–4.78) | 0.067 |
| HIF1-α | 1.17 (0.28–4.23) | 1.07 (0.34–5.38) | 0.358 |
| EPHB4 | 3.57 (0.68–69.55) | 2.67 (0.21–129.51) | 0.027 |
| eNOS | 7.14 (0.59–123.16) | 5.09 (0.41–118.15) | 0.036 |
| Biomarker | Total (n = 122) | p | |
|---|---|---|---|
| Right-Sided (n = 51) No. (%) | Left-Sided (n = 71) No. (%) | ||
| NLR | |||
| <3 | 34 (66.7) | 31 (44.3) | |
| ≥3 | 17 (33.3) | 39 (55.7) | 0.015 |
| PLR | |||
| <169 | 27 (52.9) | 26 (37.1) | |
| ≥169 | 24 (47.1) | 44 (62.9) | 0.085 |
| SII | |||
| <730 | 30 (58.8) | 28 (40.0) | |
| ≥730 | 21 (41.2) | 42 (60.0) | 0.041 |
| hs-PCR | |||
| <13.1 | 29 (58.0) | 39 (60.0) | |
| ≥13.1 | 21 (42.0) | 26 (40.0) | 0.829 |
| LDH | |||
| ≤UNL | 16 (31.4) | 21 (29.6) | |
| >UNL | 35 (68.6) | 50 (70.4) | 0.832 |
| Gene | Total (n = 122) | p | |
|---|---|---|---|
| Patient Characteristics | Right-Sided (n = 51) No. (%) | Left-Sided (n = 71) No. (%) | |
| KRAS | |||
| Wild type | 29 (56.9) | 47 (66.2) | 0.296 |
| Mutated | 22 (43.1) | 24 (33.8) | |
| BRAF | |||
| Wild type | 43 (84.3) | 69 (97.2) | 0.017 |
| Mutated | 8 (15.7) | 2 (2.8) | |
| NRAS | |||
| Wild type | 48 (94.1) | 70 (98.6) | 0.307 |
| Mutated | 3 (5.9) | 1 (1.4) | |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ulivi, P.; Scarpi, E.; Chiadini, E.; Marisi, G.; Valgiusti, M.; Capelli, L.; Casadei Gardini, A.; Monti, M.; Ruscelli, S.; Frassineti, G.L.; et al. Right- vs. Left-Sided Metastatic Colorectal Cancer: Differences in Tumor Biology and Bevacizumab Efficacy. Int. J. Mol. Sci. 2017, 18, 1240. https://doi.org/10.3390/ijms18061240
Ulivi P, Scarpi E, Chiadini E, Marisi G, Valgiusti M, Capelli L, Casadei Gardini A, Monti M, Ruscelli S, Frassineti GL, et al. Right- vs. Left-Sided Metastatic Colorectal Cancer: Differences in Tumor Biology and Bevacizumab Efficacy. International Journal of Molecular Sciences. 2017; 18(6):1240. https://doi.org/10.3390/ijms18061240
Chicago/Turabian StyleUlivi, Paola, Emanuela Scarpi, Elisa Chiadini, Giorgia Marisi, Martina Valgiusti, Laura Capelli, Andrea Casadei Gardini, Manlio Monti, Silvia Ruscelli, Giovanni Luca Frassineti, and et al. 2017. "Right- vs. Left-Sided Metastatic Colorectal Cancer: Differences in Tumor Biology and Bevacizumab Efficacy" International Journal of Molecular Sciences 18, no. 6: 1240. https://doi.org/10.3390/ijms18061240
APA StyleUlivi, P., Scarpi, E., Chiadini, E., Marisi, G., Valgiusti, M., Capelli, L., Casadei Gardini, A., Monti, M., Ruscelli, S., Frassineti, G. L., Calistri, D., Amadori, D., & Passardi, A. (2017). Right- vs. Left-Sided Metastatic Colorectal Cancer: Differences in Tumor Biology and Bevacizumab Efficacy. International Journal of Molecular Sciences, 18(6), 1240. https://doi.org/10.3390/ijms18061240