
Potential Role of Methylation Marker in Glioma Supporting Clinical Decisions

 ,
, 
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Molecular Evaluation
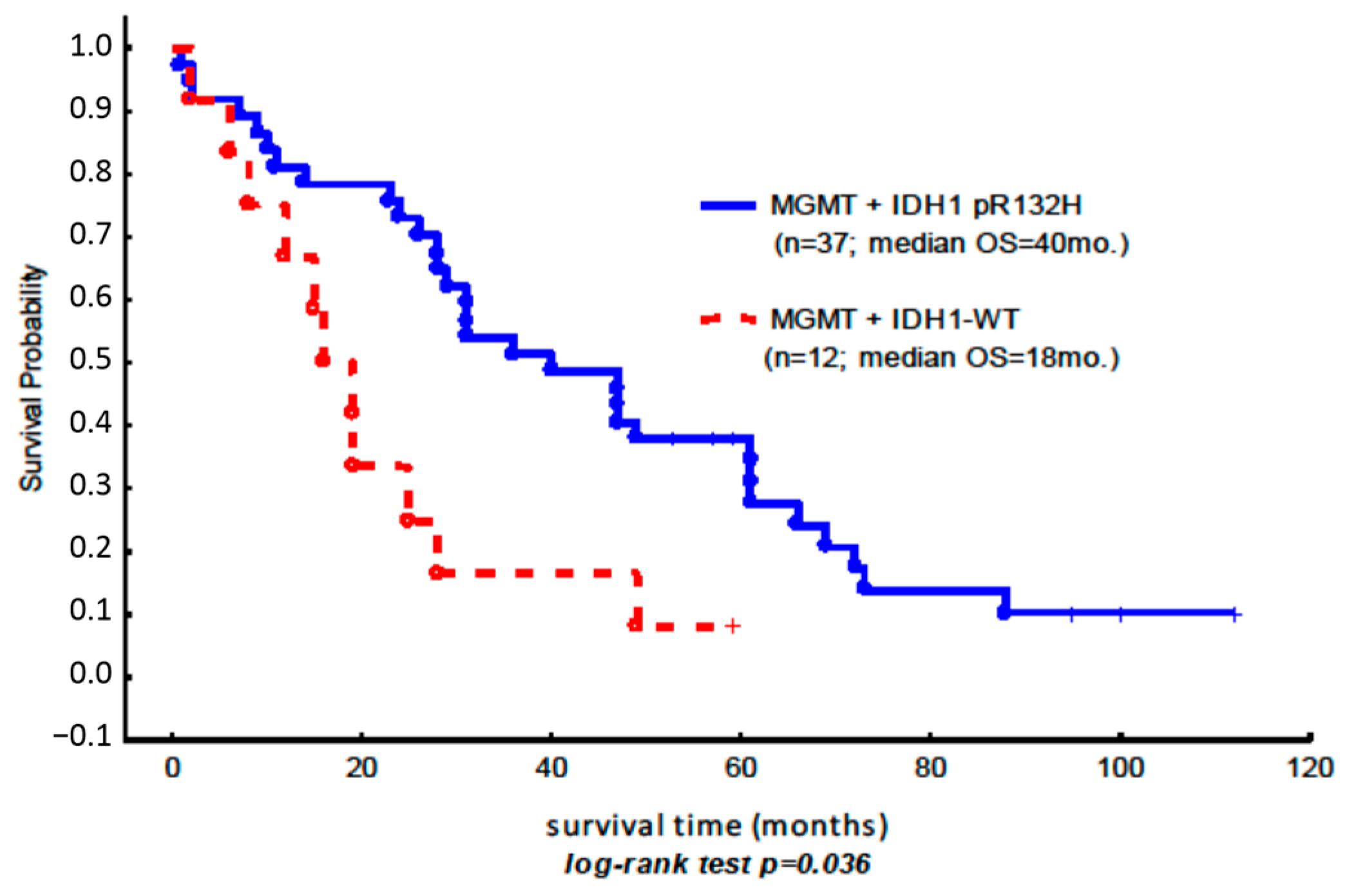
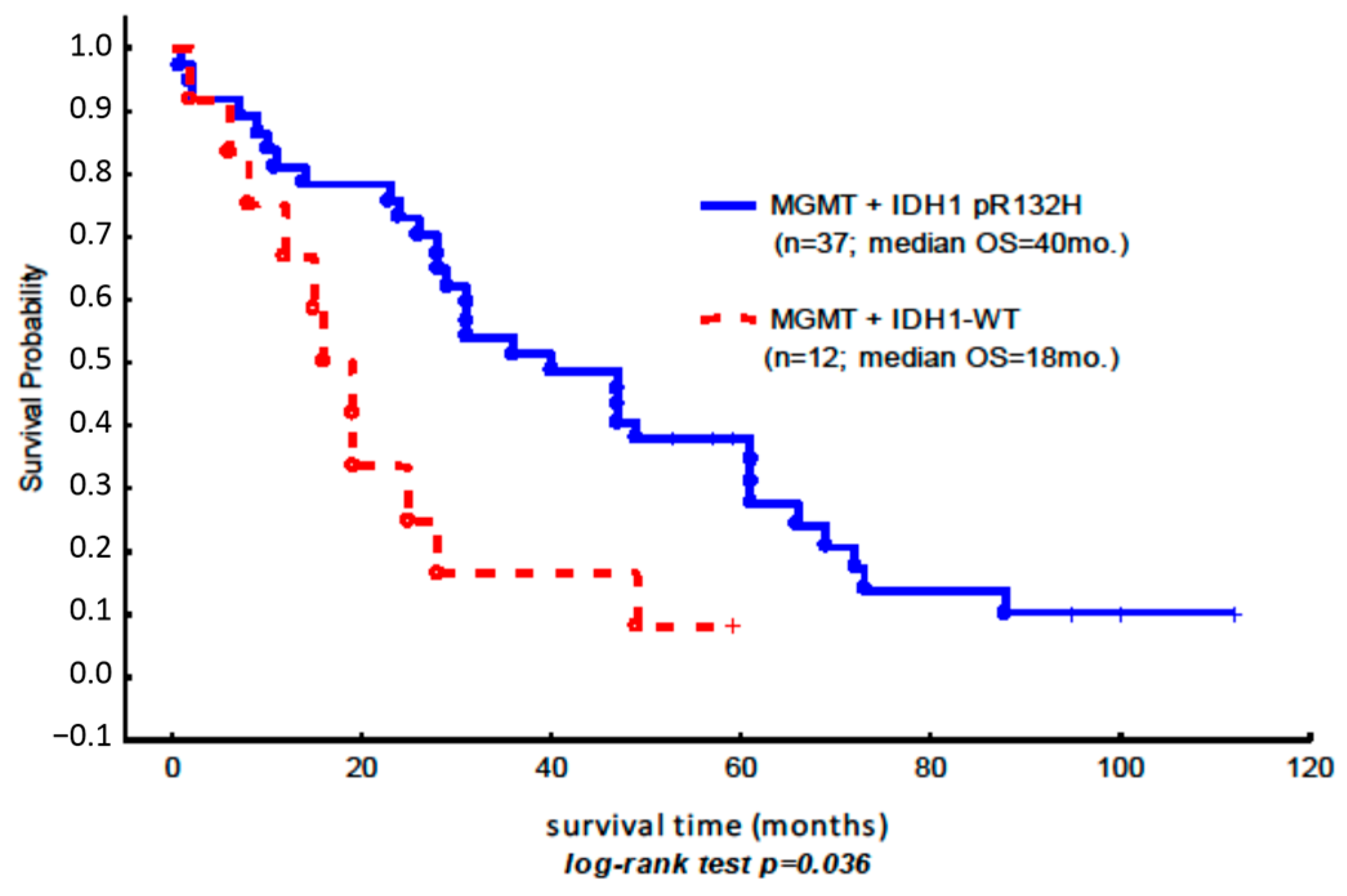
2.3. Overall Survival
3. Discussion
4. Materials and Methods
4.1. Patient Specimens
4.2. Methylation Analysis
4.3. Statistical Analysis
Author Contributions
Conflicts of Interest
References
- Lewandowska, M.A.; Costa, F.F.; Bischof, J.M.; Williams, S.H.; Soares, M.B.; Harris, A. Multiple mechanisms influence regulation of the cystic fibrosis transmembrane conductance regulator gene promoter. Am. J. Respir. Cell Mol. Biol. 2010, 43, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Boumil, R.M.; Ogawa, Y.; Sun, B.K.; Huynh, K.D.; Lee, J.T. Differential methylation of Xite and CTCF sites in Tsix mirrors the pattern of X-inactivation choice in mice. Mol. Cell. Biol. 2006, 26, 2109–2117. [Google Scholar] [CrossRef] [PubMed]
- Li, E.; Beard, C.; Jaenisch, R. Role for DNA methylation in genomic imprinting. Nature 1993, 366, 362–365. [Google Scholar] [CrossRef] [PubMed]
- Houshdaran, S.; Cortessis, V.K.; Siegmund, K.; Yang, A.; Laird, P.W.; Sokol, R.Z. Widespread epigenetic abnormalities suggest a broad DNA methylation erasure defect in abnormal human sperm. PLoS ONE 2007, 2, e1289. [Google Scholar] [CrossRef] [PubMed]
- Noushmehr, H.; Weisenberger, D.J.; Diefes, K.; Phillips, H.S.; Pujara, K.; Berman, B.P.; Pan, F.; Pelloski, C.E.; Sulman, E.P.; Bhat, K.P.; et al. Identification of a CpG island methylator phenotype that defines a distinct subgroup of glioma. Cancer Cell 2010, 17, 510–522. [Google Scholar] [CrossRef] [PubMed]
- Nalejska, E.; Maczynska, E.; Lewandowska, M.A. Prognostic and predictive biomarkers: Tools in personalized oncology. Mol. Diagn. Ther. 2014, 18, 273–284. [Google Scholar] [CrossRef] [PubMed]
- Das, P.M.; Singal, R. DNA methylation and cancer. J. Clin. Oncol. 2004, 22, 4632–4642. [Google Scholar] [CrossRef] [PubMed]
- Steemers, F.J.; Chang, W.; Lee, G.; Barker, D.L.; Shen, R.; Gunderson, K.L. Whole-genome genotyping with the single-base extension assay. Nat. Methods 2006, 3, 31–33. [Google Scholar] [CrossRef] [PubMed]
- Eckhardt, F.; Lewin, J.; Cortese, R.; Rakyan, V.K.; Attwood, J.; Burger, M.; Burton, J.; Cox, T.V.; Davies, R.; Down, T.A.; et al. DNA methylation profiling of human chromosomes 6, 20 and 22. Nat. Genet. 2006, 38, 1378–1385. [Google Scholar] [CrossRef] [PubMed]
- Feinberg, A.P.; Vogelstein, B. Hypomethylation of ras oncogenes in primary human cancers. Biochem. Biophys. Res. Commun. 1983, 111, 47–54. [Google Scholar] [CrossRef]
- Tuck-Muller, C.M.; Narayan, A.; Tsien, F.; Smeets, D.F.; Sawyer, J.; Fiala, E.S.; Sohn, O.S.; Ehrlich, M. DNA hypomethylation and unusual chromosome instability in cell lines from ICF syndrome patients. Cytogenet. Cell Genet. 2000, 89, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Lewandowska, M.A.; Furtak, J.; Szylberg, T.; Roszkowski, K.; Windorbska, W.; Rytlewska, J.; Jozwicki, W. An analysis of the prognostic value of IDH1 (isocitrate dehydrogenase 1) mutation in Polish glioma patients. Mol. Diagn. Ther. 2014, 18, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Reifenberger, J.; Reifenberger, G.; Liu, L.; James, C.D.; Wechsler, W.; Collins, V.P. Molecular genetic analysis of oligodendroglial tumors shows preferential allelic deletions on 19q and 1p. Am. J. Pathol. 1994, 145, 1175–1190. [Google Scholar] [PubMed]
- Buckner, J.C.; Shaw, E.G.; Pugh, S.L.; Chakravarti, A.; Gilbert, M.R.; Barger, G.R.; Coons, S.; Ricci, P.; Bullard, D.; Brown, P.D.; et al. Radiation plus Procarbazine, CCNU, and Vincristine in Low-Grade Glioma. N. Engl. J. Med. 2016, 374, 1344–1355. [Google Scholar] [CrossRef] [PubMed]
- Jiao, Y.; Killela, P.J.; Reitman, Z.J.; Rasheed, A.B.; Heaphy, C.M.; de Wilde, R.F.; Rodriguez, F.J.; Rosemberg, S.; Oba-Shinjo, S.M.; Nagahashi Marie, S.K.; et al. Frequent ATRX, CIC, FUBP1 and IDH1 mutations refine the classification of malignant gliomas. Oncotarget 2012, 3, 709–722. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Parsons, D.W.; Jin, G.; McLendon, R.; Rasheed, B.A.; Yuan, W.; Kos, I.; Batinic-Haberle, I.; Jones, S.; Riggins, G.J.; et al. IDH1 and IDH2 mutations in gliomas. N. Engl. J. Med. 2009, 360, 765–773. [Google Scholar] [CrossRef] [PubMed]
- Johnson, B.E.; Mazor, T.; Hong, C.; Barnes, M.; Aihara, K.; McLean, C.Y.; Fouse, S.D.; Yamamoto, S.; Ueda, H.; Tatsuno, K.; et al. Mutational analysis reveals the origin and therapy-driven evolution of recurrent glioma. Science 2014, 343, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.; Zhang, W.; Wang, Y.; Peng, X.; Chen, B.; Qiu, X.; Li, G.; Li, S.; Wu, C.; Yao, K.; et al. IDH mutation and MGMT promoter methylation in glioblastoma: Results of a prospective registry. Oncotarget 2015, 6, 40896–40906. [Google Scholar] [PubMed]
- Wick, W.; Meisner, C.; Hentschel, B.; Platten, M.; Schilling, A.; Wiestler, B.; Sabel, M.C.; Koeppen, S.; Ketter, R.; Weiler, M.; et al. Prognostic or predictive value of MGMT promoter methylation in gliomas depends on IDH1 mutation. Neurology 2013, 81, 1515–1522. [Google Scholar] [CrossRef] [PubMed]
- Li, M.Y.; Wang, Y.Y.; Cai, J.Q.; Zhang, C.B.; Wang, K.Y.; Cheng, W.; Liu, Y.W.; Zhang, W.; Jiang, T. Isocitrate dehydrogenase 1 Gene Mutation Is Associated with Prognosis in Clinical Low-Grade Gliomas. PLoS ONE 2015, 10, e0130872. [Google Scholar] [CrossRef] [PubMed]
- International Commission on Radiation Units and Measurements. Prescribing, Recording, and Reporting Photon Beam Therapy; Supplement to ICRU Report 50; ICRU: Bethesda, MD, USA, 1999; Volume 62. [Google Scholar]
- Herman, J.G.; Graff, J.R.; Myohanen, S.; Nelkin, B.D.; Baylin, S.B. Methylation-specific PCR: A novel PCR assay for methylation status of CpG islands. Proc. Natl. Acad. Sci. USA 1996, 93, 9821–9826. [Google Scholar] [CrossRef] [PubMed]
- Esteller, M.; Hamilton, S.R.; Burger, P.C.; Baylin, S.B.; Herman, J.G. Inactivation of the DNA repair gene O6-methylguanine-DNA methyltransferase by promoter hypermethylation is a common event in primary human neoplasia. Cancer Res. 1999, 59, 793–797. [Google Scholar] [PubMed]
- Esteller, M.; Garcia-Foncillas, J.; Andion, E.; Goodman, S.N.; Hidalgo, O.F.; Vanaclocha, V.; Baylin, S.B.; Herman, J.G. Inactivation of the DNA-repair gene MGMT and the clinical response of gliomas to alkylating agents. N. Engl. J. Med. 2000, 343, 1350–1354. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| No. of Patients | All Patients | 83 |
|---|---|---|
| Age | Median | 36 |
| ≤40 | 51 | |
| >40 | 32 | |
| Gender | Male | 48 |
| Female | 35 | |
| Histopathological diagnosis | Astrocytoma II | 57 |
| Astrocytoma III | 13 | |
| Glioblastoma | 13 | |
| Treatment | Radiotherapy | 83 |
| Chemotherapy | 7 | |
| ECOG performance status | I | 56 |
| II | 25 | |
| III | 2 | |
| IV | 0 |
| Astrocytoma II (n = 57) (Median OS, Month) | Astrocytoma III (n = 13) (Median OS, Month) | Glioblastoma (n = 13) (Median OS, Month) | ||||
|---|---|---|---|---|---|---|
| MGMT− | MGMT+ | MGMT− | MGMT+ | MGMT− | MGMT+ | |
| IDH1 pR132H | 33 (n = 11) | 47 (n = 24) | 28 (n = 5) | 47 (n = 7) | 22 (n = 2) | 22.5 (n = 6) |
| IDH1 WT | 21 (n = 11) | 19 (n = 11) | 14 (n = 1) | 0 | 7.5 (n = 4) | 2 (n = 1) |
| Methylation Ratio | M/U < 1 | M/U = 1 | M/U > 1 |
|---|---|---|---|
| IDH1 pR132H (n = 56) | n = 19 | n = 7 | n = 30 |
| IDH1 WT (n = 27) | n = 15 | n = 7 | n = 5 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roszkowski, K.; Furtak, J.; Zurawski, B.; Szylberg, T.; Lewandowska, M.A. Potential Role of Methylation Marker in Glioma Supporting Clinical Decisions. Int. J. Mol. Sci. 2016, 17, 1876. https://doi.org/10.3390/ijms17111876
Roszkowski K, Furtak J, Zurawski B, Szylberg T, Lewandowska MA. Potential Role of Methylation Marker in Glioma Supporting Clinical Decisions. International Journal of Molecular Sciences. 2016; 17(11):1876. https://doi.org/10.3390/ijms17111876
Chicago/Turabian StyleRoszkowski, Krzysztof, Jacek Furtak, Bogdan Zurawski, Tadeusz Szylberg, and Marzena A. Lewandowska. 2016. "Potential Role of Methylation Marker in Glioma Supporting Clinical Decisions" International Journal of Molecular Sciences 17, no. 11: 1876. https://doi.org/10.3390/ijms17111876
APA StyleRoszkowski, K., Furtak, J., Zurawski, B., Szylberg, T., & Lewandowska, M. A. (2016). Potential Role of Methylation Marker in Glioma Supporting Clinical Decisions. International Journal of Molecular Sciences, 17(11), 1876. https://doi.org/10.3390/ijms17111876