
Automated Spleen Injury Detection Using 3D Active Contours and Machine Learning


Abstract
1. Introduction
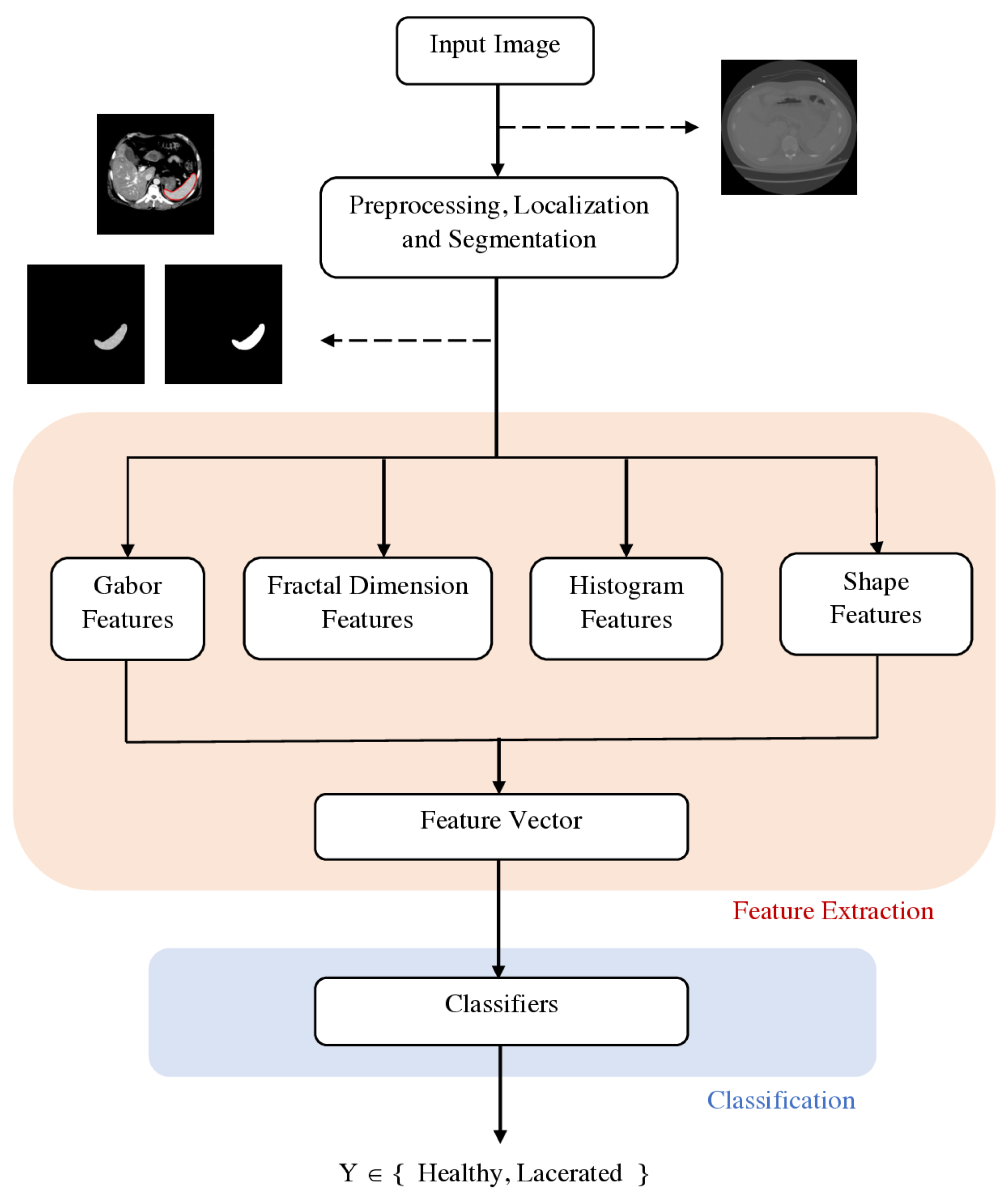
2. Materials and Methods
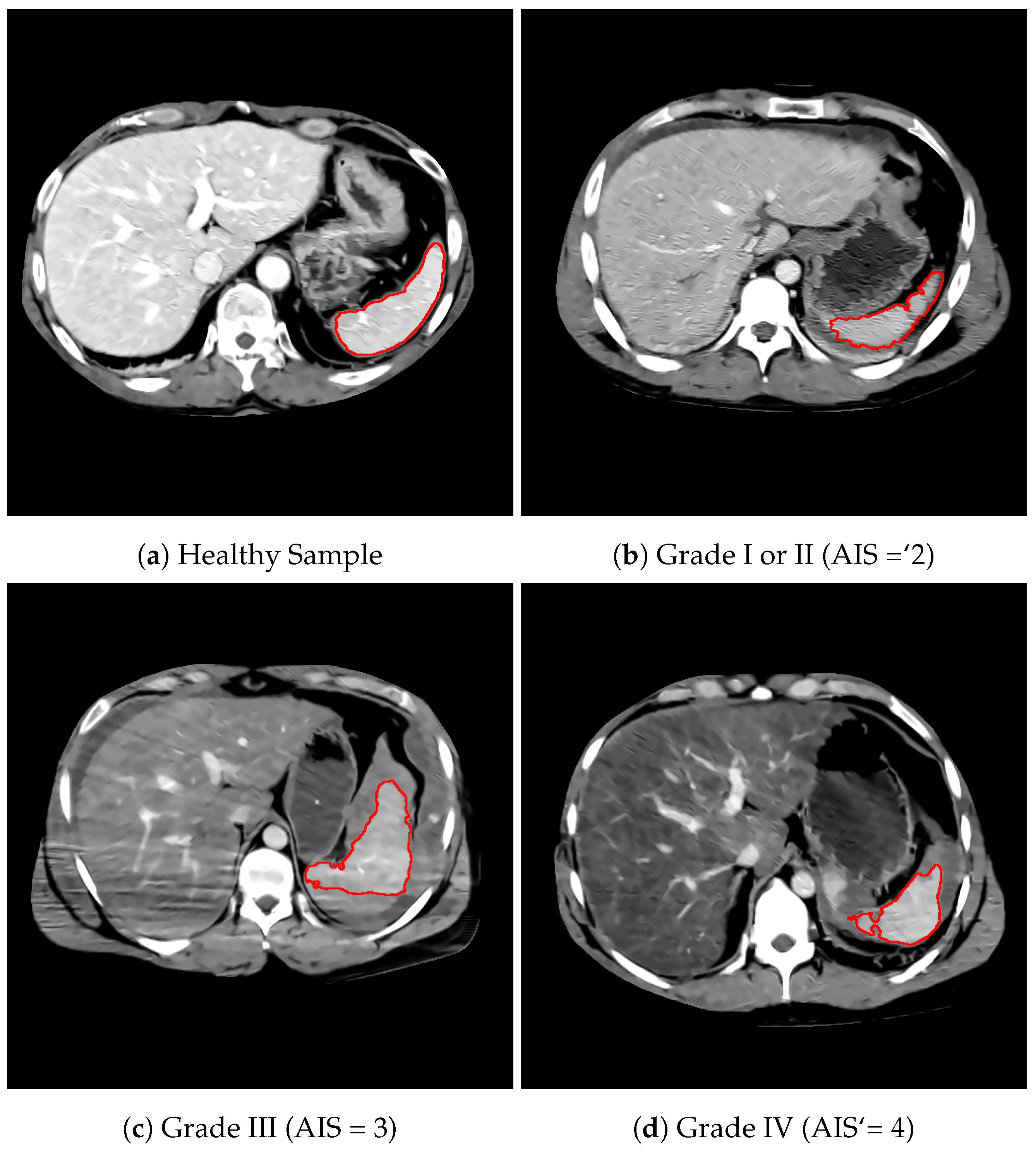
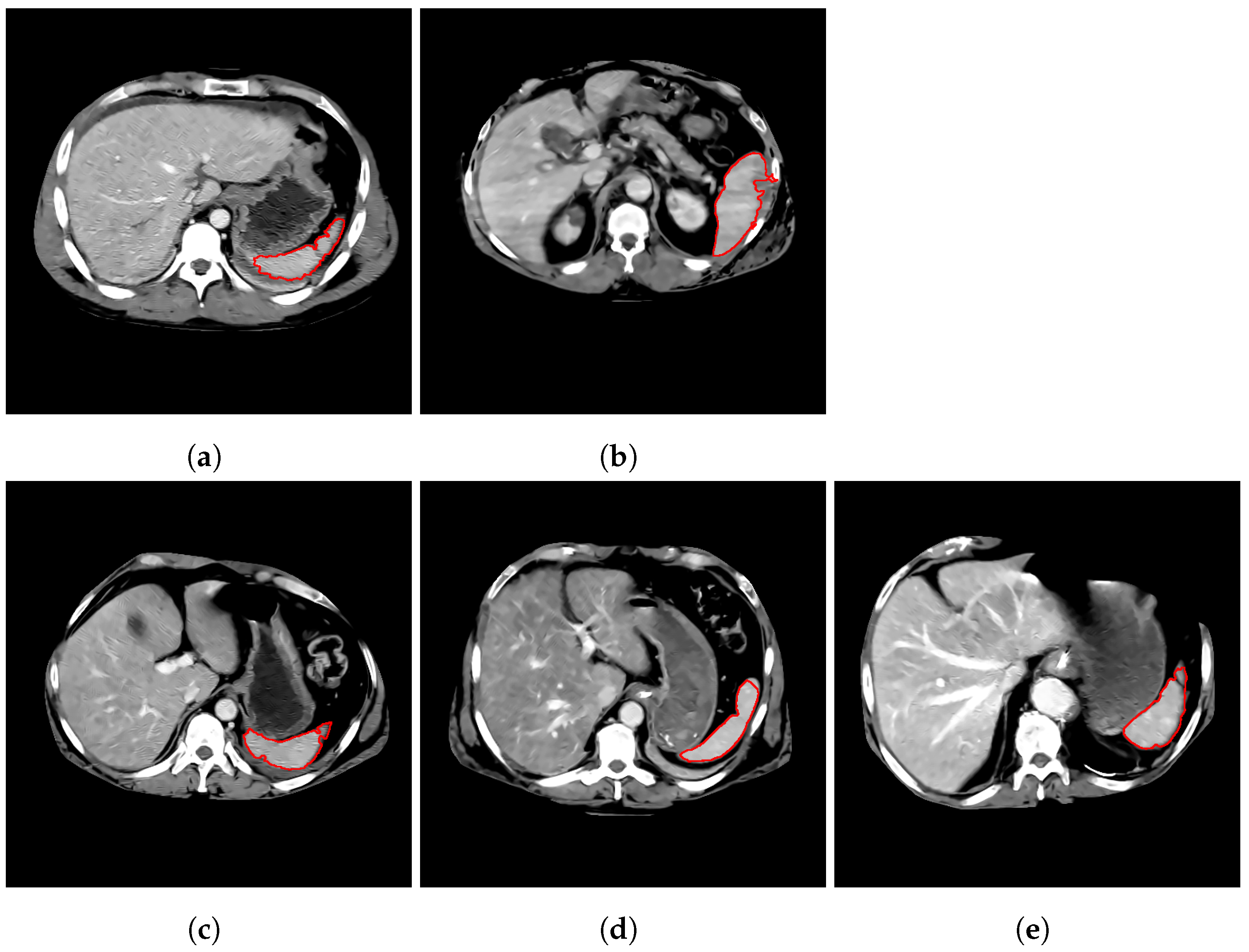
2.1. Dataset
2.2. Spleen Segmentation
2.3. Feature Extraction
2.3.1. Histogram Features
2.3.2. Fractal Dimension Analysis
2.3.3. Gabor Features
2.3.4. Shape Features
2.4. Classification
2.4.1. Training
2.4.2. Model Selection
3. Results
3.1. Classifier Performance
3.2. Comparison against Deep Learning
3.3. Leave-One-Site-Out Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shi, H.; Teoh, W.; Chin, F.; Tirukonda, P.; Cheong, S.; Yiin, R. CT of blunt splenic injuries: What the trauma team wants to know from the radiologist. Clin. Radiol. 2019, 74, 903–911. [Google Scholar] [CrossRef]
- Hassan, R.; Aziz, A.A.; Ralib, A.R.M.; Saat, A. Computed tomography of blunt spleen injury: A pictorial review. Malays. J. Med. Sci. MJMS 2011, 18, 60. [Google Scholar]
- Zhang, Z.; Sejdić, E. Radiological images and machine learning: Trends, perspectives, and prospects. Comput. Biol. Med. 2019, 108, 354–370. [Google Scholar] [CrossRef]
- Doi, K. Computer-aided diagnosis in medical imaging: Historical review, current status and future potential. Comput. Med Imaging Graph. 2007, 31, 198–211. [Google Scholar] [CrossRef]
- Syeda-Mahmood, T. Role of big data and machine learning in diagnostic decision support in radiology. J. Am. Coll. Radiol. 2018, 15, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Wood, A.; Soroushmehr, S.R.; Farzaneh, N.; Fessell, D.; Ward, K.R.; Gryak, J.; Kahrobaei, D.; Najarian, K. Fully Automated Spleen Localization In addition, Segmentation Using Machine Learning In addition, 3D Active Contours. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; pp. 53–56. [Google Scholar]
- Shi, X.; Cheng, H.D.; Hu, L.; Ju, W.; Tian, J. Detection and classification of masses in breast ultrasound images. Digit. Signal Process. 2010, 20, 824–836. [Google Scholar] [CrossRef]
- Dhanalakshmi, K.; Rajamani, V. An intelligent mining system for diagnosing medical images using combined texture-histogram features. Int. J. Imaging Syst. Technol. 2013, 23, 194–203. [Google Scholar] [CrossRef]
- Lee, W.L.; Chen, Y.C.; Hsieh, K.S. Ultrasonic liver tissues classification by fractal feature vector based on M-band wavelet transform. IEEE Trans. Med. Imaging 2003, 22, 382–392. [Google Scholar] [CrossRef]
- Xu, Y.; Lin, L.; Hu, H.; Yu, H.; Jin, C.; Wang, J.; Han, X.; Chen, Y.W. Combined density, texture and shape features of multi-phase contrast-enhanced CT images for CBIR of focal liver lesions: A preliminary study. In Innovation in Medicine and Healthcare 2015; Springer: Cham, Switzerland, 2016; pp. 215–224. [Google Scholar]
- Dhara, A.K.; Mukhopadhyay, S.; Dutta, A.; Garg, M.; Khandelwal, N. A combination of shape and texture features for classification of pulmonary nodules in lung CT images. J. Digit. Imaging 2016, 29, 466–475. [Google Scholar] [CrossRef]
- Zhu, X.; He, X.; Wang, P.; He, Q.; Gao, D.; Cheng, J.; Wu, B. A method of localization and segmentation of intervertebral discs in spine MRI based on Gabor filter bank. Biomed. Eng. Online 2016, 15, 32. [Google Scholar] [CrossRef]
- Wu, C.C.; Lee, W.L.; Chen, Y.C.; Lai, C.H.; Hsieh, K.S. Ultrasonic liver tissue characterization by feature fusion. Expert Syst. Appl. 2012, 39, 9389–9397. [Google Scholar] [CrossRef]
- Lee, W.L. An ensemble-based data fusion approach for characterizing ultrasonic liver tissue. Appl. Soft Comput. 2013, 13, 3683–3692. [Google Scholar] [CrossRef]
- Alkhawlani, M.; Elmogy, M.; Elbakry, H. Content-based image retrieval using local features descriptors and bag-of-visual words. Int. J. Adv. Comput. Sci. Appl. 2015, 6, 212–219. [Google Scholar] [CrossRef]
- U.S. Department of Transportation, National Highway Traffic Safety Administration (NHTSA). Crash Injury Research Engineering Network. 2017. Available online: https://www.nhtsa.gov/research-data/crash-injury-research (accessed on 1 February 2021).
- Keller, J.M.; Crownover, R.M.; Chen, R.Y. Characteristics of natural scenes related to the fractal dimension. IEEE Trans. Pattern Anal. Mach. Intell. 1987, 9, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Zmeskal, O.; Dzik, P.; Vesely, M. Entropy of fractal systems. Comput. Math. Appl. 2013, 66, 135–146. [Google Scholar] [CrossRef]
- Sergyan, S. Color histogram features based image classification in content-based image retrieval systems. In Proceedings of the 2008 6th International Symposium on Applied Machine Intelligence and Informatics, Herlany, Slovakia, 21–22 January 2008; pp. 221–224. [Google Scholar]
- Mandelbrot, B.B. The Fractal Geometry of Nature; WH freeman: New York, NY, USA, 1983; Volume 173. [Google Scholar]
- Chen, C.C.; DaPonte, J.S.; Fox, M.D. Fractal feature analysis and classification in medical imaging. IEEE Trans. Med. Imaging 1989, 8, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Zheng, D.; Zhao, Y.; Wang, J. Features extraction using a Gabor filter family. In Proceedings of the Sixth IASTED International Conference, Signal and Image Processing, Honolulu, HI, USA, 23–25 August 2004. [Google Scholar]
- Haghighat, M.; Zonouz, S.; Abdel-Mottaleb, M. CloudID: Trustworthy cloud-based and cross-enterprise biometric identification. Expert Syst. Appl. 2015, 42, 7905–7916. [Google Scholar] [CrossRef]
- Ashour, A.S.; Guo, Y.; Hawas, A.R.; Xu, G. Ensemble of subspace discriminant classifiers for schistosomal liver fibrosis staging in mice microscopic images. Health Inf. Sci. Syst. 2018, 6, 21. [Google Scholar] [CrossRef]
- Lee, J.G.; Jun, S.; Cho, Y.W.; Lee, H.; Kim, G.B.; Seo, J.B.; Kim, N. Deep learning in medical imaging: General overview. Korean J. Radiol. 2017, 18, 570. [Google Scholar] [CrossRef] [PubMed]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar] [CrossRef]
- Burduja, M.; Ionescu, R.T.; Verga, N. Accurate and Efficient Intracranial Hemorrhage Detection and Subtype Classification in 3D CT Scans with Convolutional and Long Short-Term Memory Neural Networks. Sensors 2020, 20, 5611. [Google Scholar] [CrossRef]
- Nguyen, N.T.; Tran, D.Q.; Nguyen, N.T.; Nguyen, H.Q. A CNN-LSTM Architecture for Detection of Intracranial Hemorrhage on CT scans. arXiv 2020, arXiv:2005.10992. [Google Scholar]
- Marentakis, P.; Karaiskos, P.; Kouloulias, V.; Kelekis, N.; Argentos, S.; Oikonomopoulos, N.; Loukas, C. Lung cancer histology classification from CT images based on radiomics and deep learning models. Med. Biol. Eng. Comput. 2021, 59, 215–226. [Google Scholar] [CrossRef]
- Kutlu, H.; Avcı, E. A novel method for classifying liver and brain tumors using convolutional neural networks, discrete wavelet transform and long short-term memory networks. Sensors 2019, 19, 1992. [Google Scholar] [CrossRef] [PubMed]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M.; et al. Imagenet large scale visual recognition challenge. Int. J. Comput. Vis. 2015, 115, 211–252. [Google Scholar] [CrossRef]
- Luo, C.; Li, X.; Wang, L.; He, J.; Li, D.; Zhou, J. How Does the Data set Affect CNN-based Image Classification Performance? In Proceedings of the 2018 5th International Conference on Systems and Informatics (ICSAI), Nanjing, China, 10–12 November 2018; pp. 361–366. [Google Scholar] [CrossRef]
- Tang, T.T.; Zawaski, J.A.; Francis, K.N.; Qutub, A.A.; Gaber, M.W. Image-based classification of tumor type and growth rate using machine learning: A preclinical study. Sci. Rep. 2019, 9, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Nedjar, I.; EL HABIB DAHO, M.; Settouti, N.; Mahmoudi, S.; Chikh, M.A. Random forest based classification of medical x-ray images using a genetic algorithm for feature selection. J. Mech. Med. Biol. 2015, 15, 1540025. [Google Scholar] [CrossRef]
- Geremia, E.; Clatz, O.; Menze, B.H.; Konukoglu, E.; Criminisi, A.; Ayache, N. Spatial decision forests for MS lesion segmentation in multi-channel magnetic resonance images. NeuroImage 2011, 57, 378–390. [Google Scholar] [CrossRef]
- Lebedev, A.; Westman, E.; Van Westen, G.; Kramberger, M.; Lundervold, A.; Aarsland, D.; Soininen, H.; Kłoszewska, I.; Mecocci, P.; Tsolaki, M.; et al. Random Forest ensembles for detection and prediction of Alzheimer’s disease with a good between-cohort robustness. Neuroimage Clin. 2014, 6, 115–125. [Google Scholar] [CrossRef]
- Alshipli, M.; Kabir, N.A. Effect of slice thickness on image noise and diagnostic content of single-source-dual energy computed tomography. J. Phys. Conf. Ser. IOP Publ. 2017, 851, 012005. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Metric | RF | Naive Bayes | SVM | k-NN | Subspace Discriminant |
|---|---|---|---|---|---|
| Accuracy | 0.83 (0.10) | 0.71 (0.11) | 0.73 (0.10) | 0.73 (0.10) | 0.67 (0.10) |
| Sensitivity | 0.77 (0.16) | 0.66 (0.17) | 0.61 (0.17) | 0.56 (0.18) | 0.44 (0.19) |
| Specificity | 0.89 (0.12) | 0.75 (0.15) | 0.84 (0.13) | 0.89 (0.11) | 0.87 (0.13) |
| F1 | 0.81 (0.12) | 0.68 (0.13) | 0.67 (0.14) | 0.65 (0.16) | 0.54 (0.18) |
| AUC | 0.91 (0.08) | 0.75 (0.12) | 0.81 ( 0.10) | 0.84 (0.10) | 0.77 (0.13) |
| Metric | RF | Naive Bayes | SVM | k-NN | Subspace Discriminant |
|---|---|---|---|---|---|
| Accuracy | 0.83 | 0.70 | 0.71 | 0.75 | 0.64 |
| Sensitivity | 0.76 | 0.63 | 0.56 | 0.59 | 0.40 |
| Specificity | 0.89 | 0.76 | 0.85 | 0.88 | 0.85 |
| F1 | 0.80 | 0.66 | 0.64 | 0.68 | 0.50 |
| AUC | 0.91 | 0.74 | 0.80 | 0.84 | 0.76 |
| Metric | RF (Hand-Crafted) | ResNet + LSTM (Deep Learning) |
|---|---|---|
| Accuracy | 0.83 | 0.79 |
| Sensitivity | 0.76 | 0.67 |
| Specificity | 0.89 | 0.90 |
| F1 | 0.80 | 0.75 |
| AUC | 0.91 | 0.72 |
| Metric | RF |
|---|---|
| Accuracy | 0.75 |
| Sensitivity | 0.59 |
| Specificity | 0.94 |
| F1 | 0.71 |
| AUC | 0.91 |
| Injury Grade | Training Accuracy | Testing Accuracy |
|---|---|---|
| Healthy | 0.89 (0.12) | 0.89 |
| AIS = 2 | 0.72 (0.30) | 0.70 |
| AIS = 3 | 0.74 (0.27) | 0.78 |
| AIS = 4, 5 | 0.88 (0.22) | 0.79 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.; Wood, A.; Gao, C.; Najarian, K.; Gryak, J. Automated Spleen Injury Detection Using 3D Active Contours and Machine Learning. Entropy 2021, 23, 382. https://doi.org/10.3390/e23040382
Wang J, Wood A, Gao C, Najarian K, Gryak J. Automated Spleen Injury Detection Using 3D Active Contours and Machine Learning. Entropy. 2021; 23(4):382. https://doi.org/10.3390/e23040382
Chicago/Turabian StyleWang, Julie, Alexander Wood, Chao Gao, Kayvan Najarian, and Jonathan Gryak. 2021. "Automated Spleen Injury Detection Using 3D Active Contours and Machine Learning" Entropy 23, no. 4: 382. https://doi.org/10.3390/e23040382
APA StyleWang, J., Wood, A., Gao, C., Najarian, K., & Gryak, J. (2021). Automated Spleen Injury Detection Using 3D Active Contours and Machine Learning. Entropy, 23(4), 382. https://doi.org/10.3390/e23040382