
Smart Devices and Wearable Technologies to Detect and Monitor Mental Health Conditions and Stress: A Systematic Review

 ,
, 
Abstract
1. Introduction
- What types of smart devices and wearable technologies are being used to detect or monitor depression, anxiety, and stress?
- What physiological or other process(es) do smart devices and wearable technologies utilise to detect depression, anxiety, and stress?
- Which of these devices have been manufactured and are available on the market as technology?
2. Materials and Methods
2.1. Selection Criteria for the Present Review
2.2. Literature Search Methods
2.3. Electronic Database Search
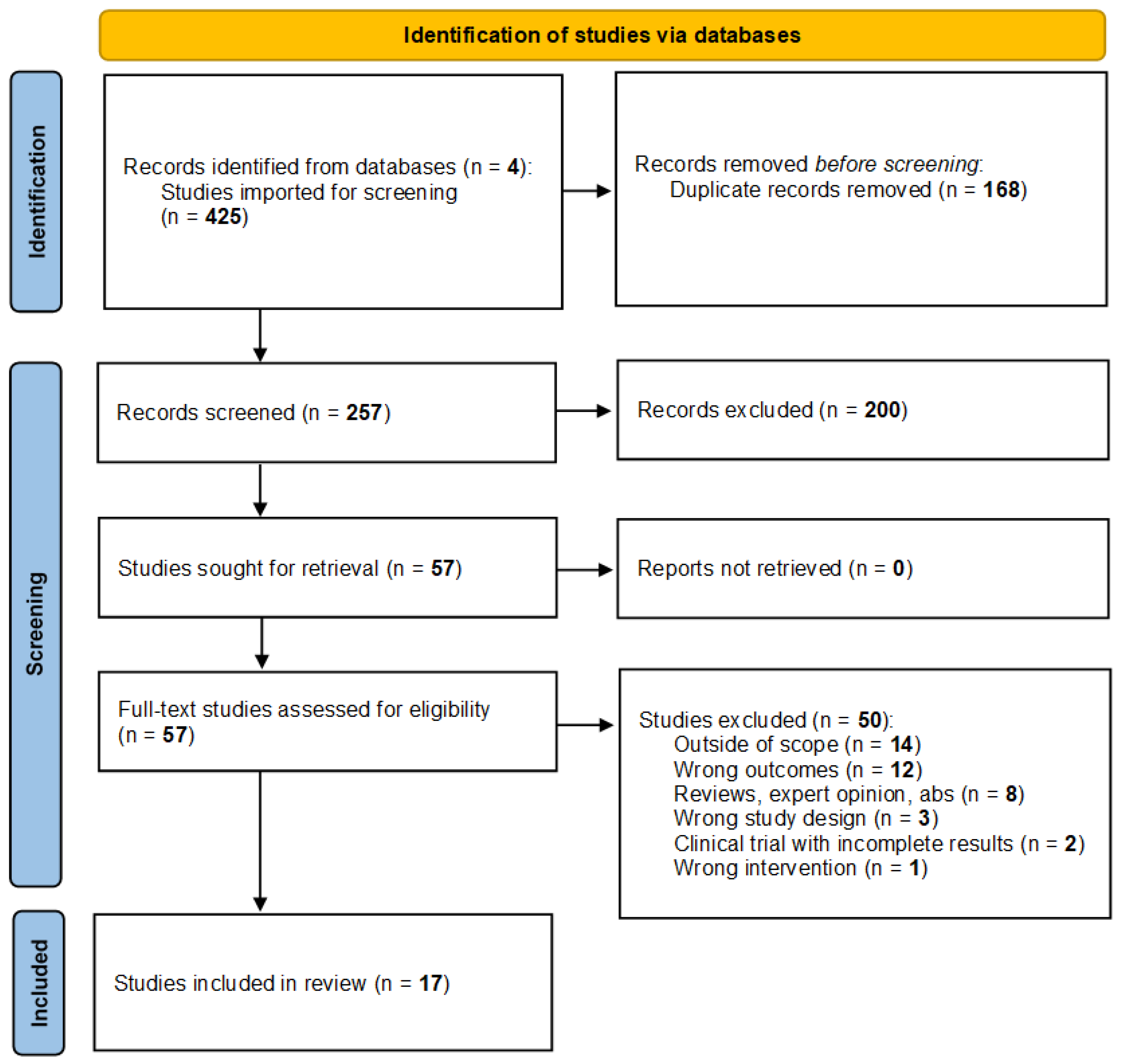
3. Results
4. Discussion
4.1. Anxiety
4.2. Findings of This Review
4.3. Stress
4.4. Findings of This Review
4.5. Depression
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Can, Y.S.; Chalabianloo, N.; Ekiz, D.; Ersoy, C. Continuous Stress Detection Using Wearable Sensors in Real Life: Algorithmic Programming Contest Case Study. Sensors 2019, 19, 1849. [Google Scholar] [CrossRef]
- Cho, D.; Ham, J.; Oh, J.; Park, J.; Kim, S.; Lee, N.-K.; Lee, B. Detection of Stress Levels from Biosignals Measured in Virtual Reality Environments Using a Kernel-Based Extreme Learning Machine. Sensors 2017, 17, 2435. [Google Scholar] [CrossRef] [PubMed]
- Vogel, J.; Auinger, A.; Riedl, R.; Kindermann, H.; Helfert, M.; Ocenasek, H. Digitally enhanced recovery: Investigating the use of digital self-tracking for monitoring leisure time physical activity of cardiovascular disease (CVD) patients undergoing cardiac rehabilitation. PLoS ONE 2017, 12, e0186261. [Google Scholar] [CrossRef] [PubMed]
- Elgendi, M.; Menon, C. Assessing Anxiety Disorders Using Wearable Devices: Challenges and Future Directions. Brain Sci. 2019, 9, 50. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Hu, B.; Shen, J.; Xu, T.; Retcliffe, M. Mild Depression Detection of College Students: An EEG-Based Solution with Free Viewing Tasks. J. Med Syst. 2015, 39, 187. [Google Scholar] [CrossRef]
- Peake, J.M.; Kerr, G.; Sullivan, J.P. A Critical Review of Consumer Wearables, Mobile Applications, and Equipment for Providing Biofeedback, Monitoring Stress, and Sleep in Physically Active Populations. Front. Physiol. 2018, 9, 743. [Google Scholar] [CrossRef]
- Weenk, M.; Bredie, S.J.H.; Koeneman, M.; Hesselink, G.J.; Goor, H.v.; Belt, T.H.v.d. Continuous Monitoring of Vital Signs in the General Ward Using Wearable Devices: Randomized Controlled Trial. J. Med. Internet Res. 2020, 22, e15471. [Google Scholar] [CrossRef]
- Chan, M.; Estève, D.; Fourniols, J.-Y.; Escriba, C.; Campo, E. Smart wearable systems: Current status and future challenges. Artif. Intell. Med. 2012, 56, 137–156. [Google Scholar] [CrossRef]
- Hernando, D.; Roca, S.; Sancho, J.; Alesanco, Á.; Bailón, R. Validation of the Apple Watch for Heart Rate Variability Measurements during Relax and Mental Stress in Healthy Subjects. Sensors 2018, 18, 2619. [Google Scholar] [CrossRef] [PubMed]
- Covidence Systematic Review Software, Veritas Health Innovation; Covidence: Melbourne, Australia. Available online: http://www.covidence.org (accessed on 27 December 2020).
- Lockwood, C.; Munn, Z.; Porritt, K. Qualitative research synthesis: Methodological guidance for systematic reviewers utilizing meta-aggregation. Int. J. Evid. Based Healthc. 2015, 13, 179–187. [Google Scholar] [CrossRef]
- Ahn, J.W.; Ku, Y.; Kim, H.C. A Novel Wearable EEG and ECG Recording System for Stress Assessment. Sensors 2019, 19, 1991. [Google Scholar] [CrossRef]
- Alberts, N.M.; Leisenring, W.M.; Flynn, J.S.; Whitton, J.; Gibson, T.M.; Jibb, L.; McDonald, A.; Ford, J.; Moraveji, N.; Dear, B.F.; et al. Wearable Respiratory Monitoring and Feedback for Chronic Pain in Adult Survivors of Childhood Cancer: A Feasibility Randomized Controlled Trial from the Childhood Cancer Survivor Study. JCO Clin. Cancer Inform. 2020, 4, 1014–1026. [Google Scholar] [CrossRef]
- Balconi, M.; Fronda, G.; Crivelli, D. Effects of technology-mediated mindfulness practice on stress: Psychophysiological and self-report measures. Stress 2019, 22, 200–209. [Google Scholar] [CrossRef] [PubMed]
- Cao, Z.; Lin, C.; Ding, W.; Chen, M.; Li, C.; Su, T. Identifying Ketamine Responses in Treatment-Resistant Depression Using a Wearable Forehead EEG. IEEE Trans. Biomed. Eng. 2018, 66, 1668–1679. [Google Scholar] [CrossRef]
- Engelniederhammer, A.; Papastefanou, G.; Xiang, L. Crowding density in urban environment and its effects on emotional responding of pedestrians: Using wearable device technology with sensors capturing proximity and psychophysiological emotion responses while walking in the street. J. Hum. Behav. Soc. Environ. 2019, 29, 630–646. [Google Scholar] [CrossRef]
- Hong, S.; Yang, Y.; Lee, J.; Yang, H.; Park, K.; Lee, S.; Lee, I.; Jang, Y. Ambulatory stress monitoring with a wearable bluetooth electrocardiographic device. Stud. Health Technol. Inform. 2010, 161, 66–76. [Google Scholar]
- Huang, C.J.; Chan, H.L.; Chang, Y.J.; Chen, S.M.; Hsu, M.J. Validity of the Polar V800 Monitor for Assessing Heart Rate Variability in Elderly Adults under Mental Stress and Dual Task Conditions. Int. J. Environ. Res. Public Health 2021, 18, 869. [Google Scholar] [CrossRef]
- Kim, J.; Park, J.; Park, J. Development of a statistical model to classify driving stress levels using galvanic skin responses. Hum. Factors Ergon. Manuf. Serv. Ind. 2020, 30, 321–328. [Google Scholar] [CrossRef]
- Lucas, B.; Grayson, S.; Hamidu, H.; Han, A.; No, S.; Varghese, A.; Campisi, J. Sex differences in heart rate responses to occupational stress. Stress: Int. J. Biol. Stress 2019, 23, 13–18. [Google Scholar]
- Narziev, N.; Goh, H.; Toshnazarov, K.; Lee, S.A.; Chung, K.-M.; Noh, Y. STDD: Short-Term Depression Detection with Passive Sensing. Sensors 2020, 20, 1396. [Google Scholar] [CrossRef] [PubMed]
- Pakhomov, S.V.S.; Thuras, P.D.; Finzel, R.; Eppel, J.; Kotlyar, M. Using consumer-wearable technology for remote assessment of physiological response to stress in the naturalistic environment. PLoS ONE 2020, 15, e0229942. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, S.; Paiva, J.S.; Dias, D.; Aleixo, M.; Filipe, R.M.; Cunha, J.P.S. Cognitive Impact and Psychophysiological Effects of Stress Using a Biomonitoring Platform. Int. J. Environ. Res. Public Health 2018, 15, 1080. [Google Scholar] [CrossRef]
- Sano, A.; Taylor, S.; McHill, A.W.; Phillips, A.J.; Barger, L.K.; Klerman, E.; Picard, R. Identifying Objective Physiological Markers and Modifiable Behaviors for Self-Reported Stress and Mental Health Status Using Wearable Sensors and Mobile Phones: Observational Study. J. Med. Internet Res. 2018, 20, e210. [Google Scholar] [CrossRef]
- Seoane, F.; Mohino-Herranz, I.; Ferreira, J.; Alvarez, L.; Buendia, R.; Ayllón, D.; Llerena, C.; Gil-Pita, R. Wearable biomedical measurement systems for assessment of mental stress of combatants in real time. Sensors 2014, 14, 7120–7141. [Google Scholar] [CrossRef]
- Silva, E.; Aguiar, J.; Reis, L.P.; E Sá, J.O.; Gonçalves, J.; Carvalho, V. Stress among Portuguese medical students: The eustress solution. J. Med. Syst. 2020, 44, 1–6. [Google Scholar] [CrossRef]
- Smith, E.N.; Santoro, E.; Moraveji, N.; Susi, M.; Crum, A.J. Integrating Wearables in Stress Management Interventions: Promising Evidence from a Randomized Trial. Int. J. Stress Manag. 2020, 27, 172–182. [Google Scholar] [CrossRef]
- van Kraaij, A.W.J.; Schiavone, G.; Lutin, E.; Claes, S.; Van Hoof, C. Relationship Between Chronic Stress and Heart Rate over Time Modulated by Gender in a Cohort of Office Workers: Cross-Sectional Study Using Wearable Technologies. J. Med. Internet Res. 2020, 22, e18253. [Google Scholar] [CrossRef] [PubMed]
- Zanella-Calzada, L.A.; Galván-Tejada, C.E.; Chávez-Lamas, N.M.; Gracia-Cortés, M.; Magallanes-Quintanar, R.; Celaya-Padilla, J.M.; Galván-Tejada, J.I.; Gamboa-Rosales, H. Feature Extraction in Motor Activity Signal: Towards a Depression Episodes Detection in Unipolar and Bipolar Patients. Diagnostics 2019, 9, 8. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Jayagopal, J.K.; Mehta, R.K.; Erraguntla, M.; Nuamah, J.; McDonald, A.D.; Taylor, H.; Chang, S.H. Classifying major depressive disorder using fNIRS during motor rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 961–969. [Google Scholar] [CrossRef]
- AIHW (Australian Institute of Health and Welfare). Australian Burden of Disease Study: Impact and Causes of Illness and Death in Australia 2015; Series no. 19. Cat. no. BOD 22; Australian Burden of Disease Study; Australian Institute of Health and Welfare: Canberra, Australia, 2019. [Google Scholar]
- Liu, H.; Wen, W.; Zhang, J.; Liu, G.; Yang, Z. Autonomic nervous pattern of motion interference in real-time anxiety detection. IEEE Access 2018, 6, 69763–69768. [Google Scholar] [CrossRef]
- Semple, D.; Smyth, R. Oxford Handbook of Psychiatry; Oxford University Press: Oxford, UK, 2013. [Google Scholar]
- Kreibig, S.D. Autonomic nervous system activity in emotion: A review. Biol. Psychol. 2010, 84, 394–421. [Google Scholar] [CrossRef]
- Adheena, M.; Sindhu, N.; Jerritta, S. Physiological Detection of Anxiety. In Proceedings of the 2018 International Conference on Circuits and Systems in Digital Enterprise Technology (ICCSDET), Pathamuttom, India, 21–22 December 2018. [Google Scholar]
- Wen, W.; Liu, G.; Mao, Z.H.; Huang, W.; Zhang, X.; Hu, H.; Yang, J.; Jia, W. Toward constructing a real-time social anxiety evaluation system: Exploring effective heart rate features. IEEE Trans. Affect. Comput. 2018, 11, 100–110. [Google Scholar] [CrossRef]
- Subhani, A.R.; Kamel, N.; Mohamad Saad, M.N.; Nandagopal, N.; Kang, K.; Malik, A.S. Mitigation of stress: New treatment alternatives. Cogn. Neurodyn. 2018, 12, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Thayer, J.F.; Åhs, F.; Fredrikson, M.; Sollers, J.J.; Wager, T.D. A meta-analysis of heart rate variability and neuroimaging studies: Implications for heart rate variability as a marker of stress and health. Neurosci. Biobehav. Rev. 2012, 36, 747–756. [Google Scholar] [CrossRef]
- Hovsepian, K.; al’Absi, M.; Ertin, E.; Kamarck, T.; Nakajima, M.; Kumar, S. cStress: Towards a Gold Standard for Continuous Stress Assessment in the Mobile Environment. In Proceedings of the 2015 ACM International Joint Conference on Pervasive and Ubiquitous Computing, Osaka, Japan, 9–11 September 2015. [Google Scholar]
- Vlemincx, E.; Taelman, J.; De Peuter, S.; Van Diest, I.; Van den Bergh, O. Sigh rate and respiratory variability during mental load and sustained attention. Psychophysiology 2011, 48, 117–120. [Google Scholar] [CrossRef]
- Boucsein, W. Electrodermal Activity; Springer Science & Business Media: Berlin, Germany, 2012. [Google Scholar]
- Boonnithi, S.; Phongsuphap, S. Comparison of heart rate variability measures for mental stress detection. In Proceedings of the Computing in Cardiology, Hangzhou, China, 18–21 September 2011. [Google Scholar]
- Castaldo, R.; Montesinos, L.; Melillo, P.; Massaro, S.; Pecchia, L. To What Extent Can We Shorten HRV Analysis in Wearable Sensing? A Case Study on Mental Stress Detection. In EMBEC & NBC 2017, Proceedings of the Conference of the European Medical and Biological Engineering Conference (EMBEC), Tampere, Finland, 11–15 June 2017; Eskola, H., Väisänen, O., Viik, J., Hyttinen, J., Eskola, H., Väisänen, O., Viik, J., Hyttinen, J., Eds.; Springer: Singapore, 2018; pp. 643–646. [Google Scholar]
- Seoane, F.; Ferreira, J.; Alvarez, L.; Buendia, R.; Ayllón, D.; Llerena, C.; Gil-Pita, R. Sensorized garments and textrode-enabled measurement instrumentation for ambulatory assessment of the autonomic nervous system response in the ATREC project. Sensors 2013, 13, 8997–9015. [Google Scholar] [CrossRef]
- Posada-Quintero, H.F.; Chon, K.H. Phasic Component of Electrodermal Activity is more Correlated to Brain Activity than Tonic Component. In Proceedings of the 2019 IEEE EMBS International Conference on Biomedical & Health Informatics (BHI), Chicago, IL, USA, 19–22 May 2019; pp. 1–4. [Google Scholar]
- Beauchaine, T.; Thayer, J. Heart rate variability as a transdiagnostic biomarker of psychopathology. Int. J. Psychophysiol. 2015, 98, 338–350. [Google Scholar] [CrossRef] [PubMed]
- Valenza, G.; Garcia, R.; Citi, L.; Scilingo, E.; Tomaz, C.; Barbieri, R. Nonlinear digital signal processing in mental health: Characterization of major depression using instantaneous entropy measures of heartbeat dynamics. Front. Physiol. 2015, 6, 74. [Google Scholar] [CrossRef]
- Castaldo, R.; Melillo, P.; Bracale, U.; Caserta, M.; Triassi, M.; Pecchia, L. Acute mental stress assessment via short term hrv analysis in healthy adults: A systematic review with meta-analysis. Biomed. Signal Process. Control 2015, 18, 370–377. [Google Scholar] [CrossRef]
- Mtui, E.; Gruener, G.; Dockery, P. Fitzgerald’s Clinical Neuroanatomy and Neuroscience; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-predicted maximal heart rate revisited. J. Am. Coll. Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef]
- Hou, X.; Liu, Y.; Sourina, O.; Tan, Y.R.E.; Wang, L.; Mueller-Wittig, W. EEG Based Stress Monitoring. In Proceedings of the 2015 IEEE International Conference on Systems, Man, and Cybernetics, Hong Kong, China, 9–12 October 2015; pp. 3110–3115. [Google Scholar]
- Chen, J.; Abbod, M.; Shieh, J.S. Pain and Stress Detection Using Wearable Sensors and Devices—A Review. Sensors 2021, 21, 1030. [Google Scholar] [CrossRef]
- Anusha, A.S.; Sukumaran, P.; Sarveswaran, V.; Shyam, A.; Akl, T.J.; Preejith, S.P.; Sivaprakasam, M. Electrodermal activity based pre-surgery stress detection using a wrist wearable. IEEE J. Biomed. Health Inform. 2019, 24, 92–100. [Google Scholar]
- Baskaran, A.; Milev, R.; McIntyre, R.S. The neurobiology of the EEG biomarker as a predictor of treatment response in depression. Neuropharmacology 2012, 63, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.C.; Yu, S.C.; McQuoid, D.R.; Messer, D.F.; Taylor, W.D.; Singh, K.; Boyd, B.D.; Krishnan, K.R.R.; MacFall, J.R.; Steffens, D.C.; et al. Reduction of dorsolateral prefrontal cortex gray matter in late-life depression. Psychiatry Res. Neuroimaging 2011, 193, 1–6. [Google Scholar] [CrossRef]
- Shiffman, S.; Stone, A.A.; Hufford, M.R. Ecological momentary assessment. Annu. Rev. Clin. Psychol. 2008, 4, 1–32. [Google Scholar] [CrossRef]
- Taj-Eldin, M.; Ryan, C.; O’Flynn, B.; Galvin, P. A Review of Wearable Solutions for Physiological and Emotional Monitoring for Use by People with Autism Spectrum Disorder and Their Caregivers. Sensors 2018, 18, 4271. [Google Scholar] [CrossRef] [PubMed]
- Warmerdam, L.; Riper, H.; Klein, M.C.; van de Ven, P.; Rocha, A.; Henriques, M.R.; Tousset, E.; Silva, H.; Andersson, G.; Cuijpers, P. Innovative ICT solutions to improve treatment outcomes for depression: The ICT4Depression project. Stud. Health Technol. Inform. 2012, 181, 339–343. [Google Scholar] [PubMed]
- Matcham, F.; di San Pietro, C.B.; Bulgari, V.; De Girolamo, G.; Dobson, R.; Eriksson, H.; Folarin, A.A.; Haro, J.M.; Kerz, M.; Lamers, F.; et al. Remote assessment of disease and relapse in major depressive disorder (RADAR-MDD): A multi-centre prospective cohort study protocol. BMC Psychiatry 2019, 19, 72. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Search Term | No. of Results |
|---|---|
| Step 1. Primary search term 1: Wearable device.ab,ti. | 1496 |
| Step 2. Primary search term 2: Wearable technology.ab,ti. | 892 |
| Step 3. Primary search term 3: Smart device.ab,ti. | 1265 |
| Step 4. Primary search term 4: Wireless device.ab,ti. | 1429 |
| Step 5. Combined primary search terms: Search term 1 or 2 or 3 or 4 | 2987 |
Step 6. Using only the secondary search terms below:
| 73,999 50,356 162,184 |
Step 7. Combined Step 5 and Step 6 (where Step 6 was):
| 34 24 113 |
| Search Term | No. of Results |
|---|---|
| Step 1. Primary search term 1: Wearable device.ab,ti. | 454 |
| Step 2. Primary search term 2: Wearable technology.ab,ti. | 463 |
| Step 3. Primary search term 3: Smart device.ab,ti. | 345 |
| Step 4. Primary search term 4: Wireless device.ab,ti. | 346 |
| Step 5. Combined primary search terms: Search term 1 or 2 or 3 or 4 | 1358 |
Step 6. Using only the secondary search terms below:
| 35,468 25,877 42,329 |
Step 7. Combined Step 5 and Step 6 (where Step 6 was):
| 18 17 45 |
| Search Term | No. of Results |
|---|---|
| Step 1. Primary search term 1: Wearable device.ab,ti. | 535 |
| Step 2. Primary search term 2: Wearable technology.ab,ti. | 300 |
| Step 3. Primary search term 3: Smart device.ab,ti. | 434 |
| Step 4. Primary search term 4: Wireless device.ab,ti. | 313 |
| Step 5. Combined primary search terms: Search term 1 or 2 or 3 or 4 | 1394 |
Step 6. Using only the secondary search terms below:
| 78,922 53,821 60,314 |
Step 7. Combined Step 5 and Step 6 (where Step 6 was):
| 93 93 85 |
| Search Term | No. of Results |
|---|---|
| Step 1. Primary search term 1: Wearable device.ab,ti. | 164 |
| Step 2. Primary search term 2: Wearable technology.ab,ti. | 121 |
| Step 3. Primary search term 3: Smart device.ab,ti. | 123 |
| Step 4. Primary search term 4: Wireless device.ab,ti. | 79 |
| Step 5. Combined primary search terms: Search term 1 or 2 or 3 | 435 |
Step 6. Using only the secondary search terms below:
| 76,926 62,904 72,329 |
Step 7. Combined Step 5 and Step 6 (where Step 6 was):
| 14 13 18 |
| Study | Wearable Technology | Population | Objective | Primary Results |
| Ahn et al., 2019 [12] | Novel, wearable EEG and ECG head band that hangs behind both ears. | 14 male subjects, young (mean age: 29.4 ± 3.3), healthy, with no reported comorbidities. | To develop a wearable device consisting of four sensors, with the capability of detecting stress using dual EEG and ECG. | Combined EEG and HRV were most accurate (87.5%) in detecting stress in healthy subjects, compared with EEG alone (77.9%) and HRV (75.0%). |
| Alberts et al., 2020 [13] | Spire Stone (Spire Health, San Francisco, CA, USA) and Spire Health Tag respiratory monitor (Spire Health, San Francisco, CA, USA) which monitor respiratory rate. | 65 subjects (30 male, 35 female), middle-aged (mean age: 44.1 ± 8.7), in adults with chronic pain. | To assess the feasibility, acceptability, and efficacy of wearable respiratory monitoring for chronic pain and associated stress, depression, and anxiety. | The device was acceptable to 90.3% of subjects. The use of wearable respiratory monitoring may be useful in monitoring anxiety and stress. |
| Balconi et al., 2019 [14] | Wearable brain-sensing device, either the Muse™ headband (InteraXon Inc.) or the Lowdown Focus glasses (SmithOptics Inc.). | 55 subjects (38 male, 17 female), young (mean age: 23.2 ± 1.8), with no known diagnosed psychiatric illness or cognitive impairment. | To use wearable devices in conjunction with mindfulness techniques to reduce overall stress and anxiety in a healthy population. | The use of wearable technology and mindfulness resulted in reduced perceived stress and anxiety. Further, HRV measures were reduced by the technology-mediated mindfulness exercise. |
| Cao et al., 2018 [15] | Wearable forehead EEG device the “Mindo-4S Jellyfish” (Eee Holter Technology Co.). | 55 subjects (10 male, 45 female), middle-aged (mean age: ~mean age: 48), with treatment-resistant depression (TRD). | To determine the response to ketamine in patients with TRD using a wearable forehead EEG and Hamilton depression rating score. | Post-ketamine treatment EEG signatures in the prefrontal cortex showed improvements in EEG depressive signatures when compared with baseline EEG (p < 0.05). |
| Engelniederhammer et al., 2019 [16] | Sensor smart wristband (Bodymonitor) which monitors electrodermal activity (EDA) and skin temperature. | 30 subjects (10 male, 20 female), young (mean age: 24.8 ± 0.7) with no known diagnosed psychiatric illness. | Using a wearable device to detect if invasion of individual personal space in crowded environments elicits an emotional response, including stress and aggression. | Aversive emotional responses (i.e., stress, anger, fear) detected by EDA-based emotion response type, were increased when personal space was encroached upon on busy streets. |
| Hernando et al., 2018 [9] | Apple Watch compared against the Polar H7 chest device (Polar Electro Oy) both of which detect HRV. | 20 subjects, young in age with no reported comorbidities (little demographic information provided). | To validate the Apple Watch in terms of HRV derived from the R–R interval series against the R–R interval provided by the Polar H7 chest device and validated in both a stressed and relaxed state. | HRV indices from the R–R interval series reflected changes brought on by mild stress compared with relaxed states. HRV from the Apple Watch was not significantly different to the Polar H7 chest device. |
| Hong et al., 2010 [17] | Dual electrode ECG device the Biopatch, worn on the precordium. | 29 (25 male, 4 female) healthy, young (mean age = 29.62 ± 5.28) participants, no known cardiovascular or neurological disease. | To verify the reliability of a wearable ECG device to detect stress, by correlating HRV to qualitative stress indices, cortisol, and catecholamine levels. | HRV parameters had high concordance correlations with stress. Catecholamines had the highest correlation with qualitative stress level. HRV had weak correlation with cortisol. |
| Huang et al., 2021 [18] | Heart rate variability measured using Polar V800 Heart Rate Monitor (Polar Electro OY, Kempele, Finland), | 40 (17 male, 23 female) elderly (aged 65–79 years old) participants, with no established cognitive impairment or neurological disease. | To investigate the validity of the Polar V800 heart rate monitor for assessing R–R intervals and to evaluate differences in HRV when under physical or cognitive stressors. | HRV parameters on the wearable device were highly correlated with ECG HRV, and were capable of adequately measuring HRV under different stressors. |
| Kim et al., 2020 [19] | Galvanic skin response (GSR) was recorded using Empatica wristband (E4, Empatica Inc.). | 9 subjects (no further demographics provided). | To develop a statistical model that accurately classifies driving stress by monitoring GSR. | Classification accuracy of the device to detect stress during driving was 85.3%. |
| Li et al., 2015 [5] | Single electrode EEG (no specifics provided). | 36 subjects (24 male, 12 female), 9 of which had mild depression. | To create a device which accurately and objectively detects depression and related risk factors. | 99.1% detection of mild depression using k-nearest neighbour kNN classifiers on EEG. |
| Lucas et al., 2019 [20] | Apple Watch (series 1) to track HR changes. | 23 subjects (16 male, mean age 30.1, 7 female, mean age 30.6), majority not physically active, with no chronic comorbidities. | To monitor changes in HR while exposed to occupational stress and to determine if gender or physical activity influences this change in HR. | Baseline HR significantly increased during a shift when compared to baseline, with females’ HR significantly higher than males (p < 0.001). Physical activity level had no significant impact. |
| Narziev et al., 2020 [21] | Android smartphone and smartwatch (Gear S3 Frontier) accelerometer, significant motion, and step count data, to assess physical activity. | 20 subjects (no demographic data) with either no, mild, moderate, or severe depression (PHQ-9). | To develop a Short-Term Depression Detector (STDD) framework that utilises a smartphone and smartwatch to continuously monitor self-reported symptoms and passive sensing data, respectively. Mood was ascertained by a combination of physical activity measures and mean HR. | Using a machine learning model, subjects’ passive sensing data (mood, physical activity, and sleep) was used to classify depression category and had high correlation to the self-reported depression score. The STDD had an accuracy of 96 ± 2.8% in depressive group classification. |
| Pakhomov et al., 2020 [22] | Fitbit® (equipped with photoplethysmography sensor). | 18 subjects (4 male, 14 female), young (mean age: 20.6 ± 2.0) that were non-smokers, not pregnant and with no comorbidities effecting HR. | To evaluate if wearable technology can detect physiological responses to stress when an individual is exposed to both stress-inducing scenarios and stress in everyday life. | Baseline HR was significantly lower than the HR recorded during a stressor (as identified by EMA surveys), up to ~9 beats higher. Concluded that Fitbit may be useful in identifying stressors in everyday life. |
| Rodrigues et al., 2018 [23] | Vital Jacket® (1-Lead, Biodevices S.A), a medical-grade wearable ECG device and actigraph. | 11 subjects (8 male, 3 female), mean age 46.7 ± 5.9, with no known cardiovascular diagnoses. | To assess the impact that stress has on cognitive performance in air traffic controllers and if this decreased performance was related to an autonomic stress response. | The TSST stress task resulted in significant changes in several HRV parameters and subjective stress level (STAI-six item) compared to baseline readings, as well as a decline in cognitive performance. |
| Sano et al., 2018 [24] | Two sensors on each wrist: Q-sensor (Affectiva) to measure skin conductance (SC), skin temperature (ST), three-axis acceleration (ACC), and Motion Logger to measure acceleration and ambient light data. | 201 college students (129 male, 72 female), young (aged 18–25) collected across 3 years (2013–2015). | To determine how accurately physiological and behavioural measures recorded off wearable devices could detect stress and poor mental health (anxiety/depressive symptoms), and to evaluate which of these physiological or behavioural measures were most accurate. | Wearable sensor features (SC, ST) were more accurate in classifying poor mental health (87%) and stress (78.3%) than mobile phone and modifiable behavioural modalities when using machine learning. |
| Seoane et al., 2014 [25] | Multiparametric sensorised garment, containing one: GSR, Temperature unit, ECG, Thoracic Impedance recording unit, Sensorised glove, upper-arm strap, chest strap system, and six textrodes and smart phone for voice recording. | 42 subjects (no demographic information provided). | The Assessment in Real Time of the Stress in Combatants (ATREC) project aimed to create a comprehensive wearable system to detect the real-time emotional, physical, and mental stress load of soldiers during military combat by monitoring various physiological parameters. | HR and respiratory rate, collected via ECG and electrical bioimpedance measurements from the thorax, respectively, were more useful in the assessment of stress than GSR, skin temperature, or speech. |
| Silva et al., 2020 [26] | Microsoft Smartband 2™, which measures skin conductance, body temperature, heart rate variability, calorie intake and expenditure, sleep patterns, and quality. | 82 Portuguese (63 male, 19 female) young (17–38 years old) medical students. | To assess the level of stress experienced by medical students during examination by monitoring of HRV parameters. | Multiple HRV parameters were significantly different during stressful condition than baseline. |
| Smith et al., 2020 [27] | Spire Stone (Spire Health) which tracks respiratory rate and variability. It identifies stress, which is relayed to a smartphone. | 169 subjects (76 male, 93 female), young (mean age: 33.2 ± 7.8). | To determine if mental health outcomes can be improved via a wearable stress management intervention and breathing biofeedback. | Of those that partook in the stress management intervention, 28.2% felt a reduction in stress and anxiety. The respiratory data was unavailable due to poor subject compliance in wearing the device. |
| vanKraaij et al., 2020 [28] | Chillband (wristband) to measure skin conductance and temperature, and ePATCH™ Extended Holter monitor. | 328 subjects (186 male, 142 female), mean age 38.9 ±10.2. | This study is part of the Stress in Work Environment (SWEET), with the aim to determine if chronic stress influences HR over time and to assess if gender or age modulates this effect. | There is a significant relationship between HR and the three-way interaction of chronic stress, gender, and the circadian harmonic. Female gender was found to be associated with higher heart rates. |
| Zanella-Calzada et al., 2019 [29] | Actiwatch (Cambridge Neurotechnology Ltd.) detects activity levels. | 5895 subjects from the “Depresjon Dataset” were used. No demographic data was given. | To use feature extraction of motor activity level data to detect depressed subjects accurately. | Subjects with depression were accurately detected in 86.7% of cases and those without depression were identified in 91.9% of cases. |
| Zhu et al., 2020 [30] | Brain oxy-hemodynamic (HbO) responses were recorded using a 16-channel wearable continuous-wave functional near-infrared spectroscopy (fNIRS) device model 1000, (United States). | 31 subjects, 14 with clinically diagnosed major depressive disorders (6 male, 8 female), and 17 healthy controls (6 male and 11 female), aged 20 to 80 years. | This study aimed to assess the feasibility of fNIRS to assess and classify depression using a motor rehabilitation task. | Subjects with depression were accurately classified in 92.6% of subjects. This study also identified mean HbO, full width half maximum and kurtosis, as specific neuromarkers, for predicting major depressive disorders across dorsolateral and ventrolateral prefrontal cortex. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hickey, B.A.; Chalmers, T.; Newton, P.; Lin, C.-T.; Sibbritt, D.; McLachlan, C.S.; Clifton-Bligh, R.; Morley, J.; Lal, S. Smart Devices and Wearable Technologies to Detect and Monitor Mental Health Conditions and Stress: A Systematic Review. Sensors 2021, 21, 3461. https://doi.org/10.3390/s21103461
Hickey BA, Chalmers T, Newton P, Lin C-T, Sibbritt D, McLachlan CS, Clifton-Bligh R, Morley J, Lal S. Smart Devices and Wearable Technologies to Detect and Monitor Mental Health Conditions and Stress: A Systematic Review. Sensors. 2021; 21(10):3461. https://doi.org/10.3390/s21103461
Chicago/Turabian StyleHickey, Blake Anthony, Taryn Chalmers, Phillip Newton, Chin-Teng Lin, David Sibbritt, Craig S. McLachlan, Roderick Clifton-Bligh, John Morley, and Sara Lal. 2021. "Smart Devices and Wearable Technologies to Detect and Monitor Mental Health Conditions and Stress: A Systematic Review" Sensors 21, no. 10: 3461. https://doi.org/10.3390/s21103461
APA StyleHickey, B. A., Chalmers, T., Newton, P., Lin, C.-T., Sibbritt, D., McLachlan, C. S., Clifton-Bligh, R., Morley, J., & Lal, S. (2021). Smart Devices and Wearable Technologies to Detect and Monitor Mental Health Conditions and Stress: A Systematic Review. Sensors, 21(10), 3461. https://doi.org/10.3390/s21103461