An sEMG-Controlled 3D Game for Rehabilitation Therapies: Real-Time Time Hand Gesture Recognition Using Deep Learning Techniques



Abstract
1. Introduction
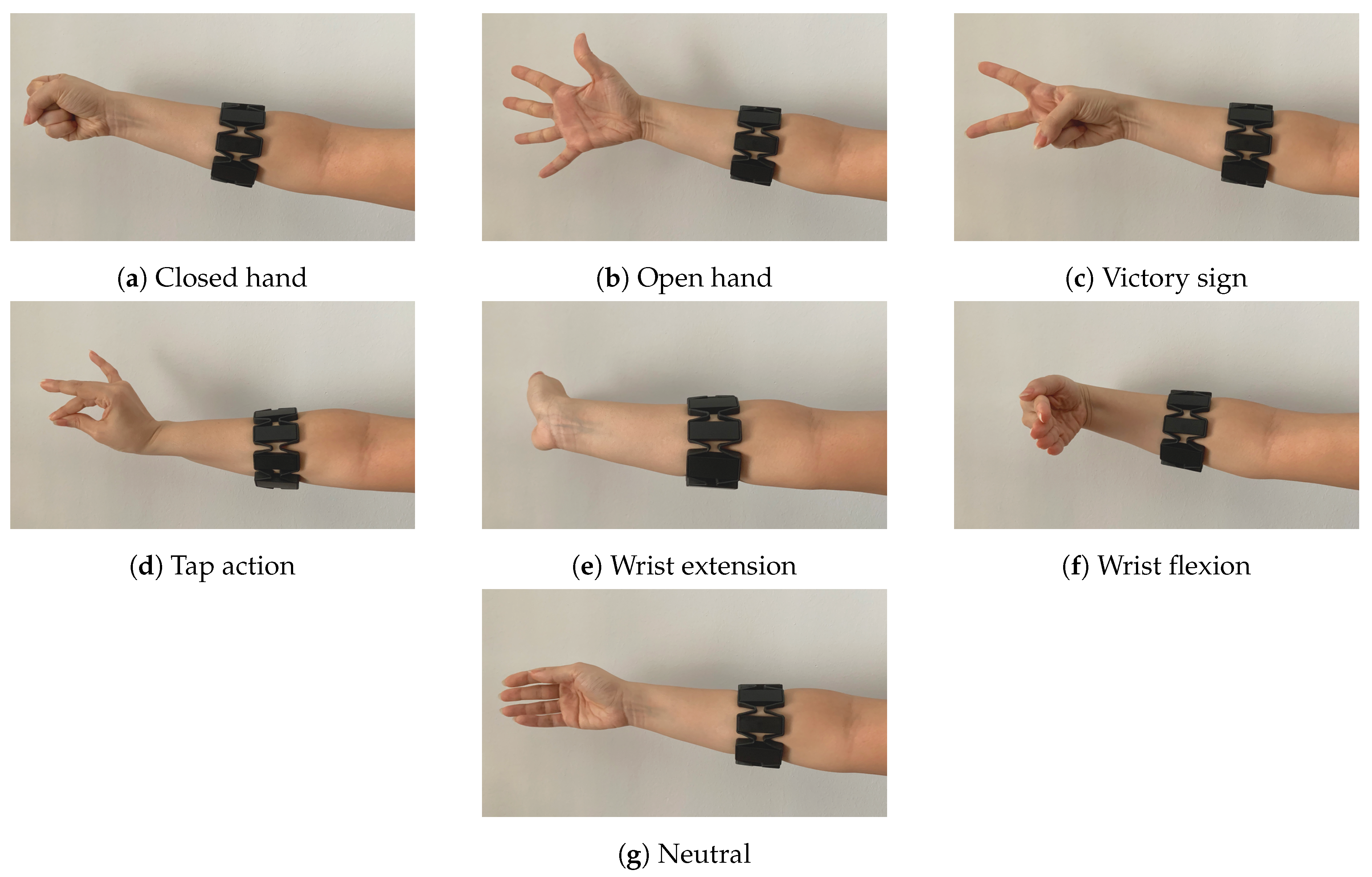
- A novel dataset acquired from 15 subjects with 7 dissimilar hand gestures.
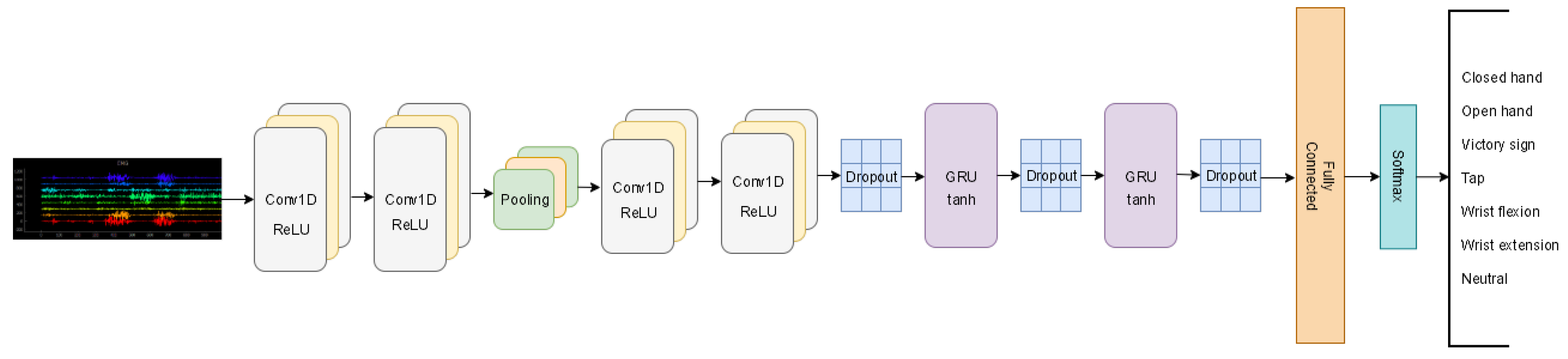
- A deep learning-based method for hand gesture recognition via sEMG signals.
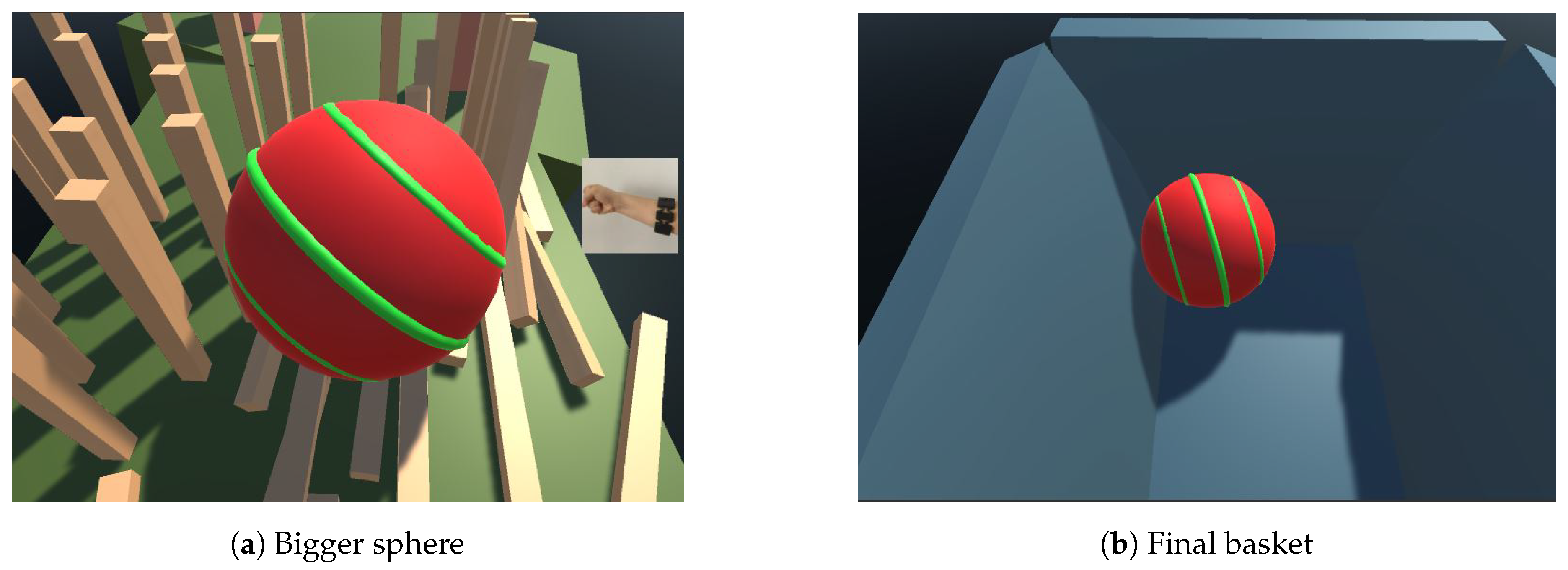
- A live 3D game for rehabilitation, that leverages AI (hand gesture recognition), to create a compelling experience for the user (rich visual stimuli).
2. Related Work
3. Sensor-Based Rehabilitation System
3.1. Database and Recording Hardware
3.2. Neural Network Architecture
3.3. 3D Game Experience
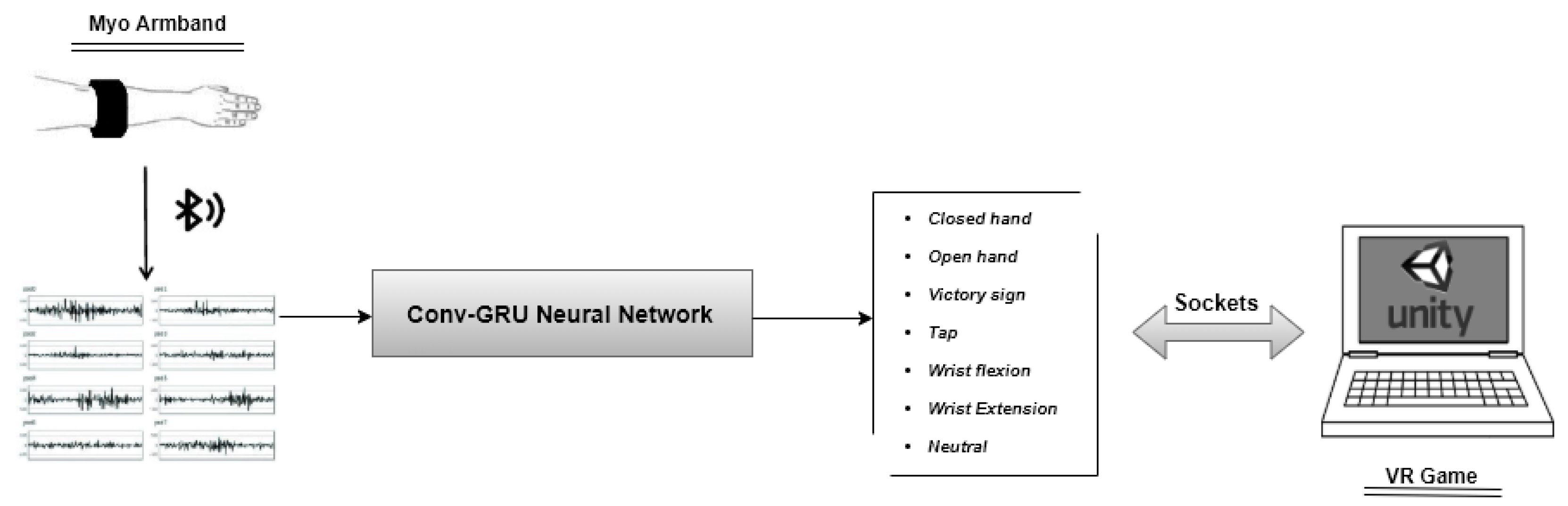
3.4. System Description
4. Experiments and Results
5. User Study
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Merians, A.S.; Poizner, H.; Boian, R.F.; Burdea, G.C.; Adamovich, S.V. Sensorimotor Training in a Virtual Reality Environment: Does It Improve Functional Recovery Poststroke? Neurorehabilit. Neural Repair 2006, 20, 252–267. [Google Scholar] [CrossRef]
- Ustinova, K.I.; Perkins, J.; Leonard, W.A.; Ingersoll, C.D.; Hausebeck, C. Virtual reality game-based therapy for persons with TBI: A pilot study. In Proceedings of the 2013 International Conference on Virtual Rehabilitation (ICVR), Philadelphia, PA, USA, 26–29 August 2013; pp. 87–93. [Google Scholar]
- Dukes, P.S.; Hayes, A.; Hodges, L.F.; Woodbury, M. Punching ducks for post-stroke neurorehabilitation: System design and initial exploratory feasibility study. In Proceedings of the 2013 IEEE Symposium on 3D User Interfaces (3DUI), Orlando, FL, USA, 16–17 March 2013; pp. 47–54. [Google Scholar]
- Barresi, G.; Mazzanti, D.; Caldwell, D.; Brogni, A. Distractive User Interface for Repetitive Motor Tasks: A Pilot Study. In Proceedings of the 2013 Seventh International Conference on Complex, Intelligent, and Software Intensive Systems, Taichung, Taiwan, 3–5 July 2013; pp. 588–593. [Google Scholar]
- Placidi, G.; Avola, D.; Iacoviello, D.; Cinque, L. Overall design and implementation of the virtual glove. Comput. Biol. Med. 2013, 43, 1927–1940. [Google Scholar] [CrossRef] [PubMed]
- Gama, A.D.; Chaves, T.M.; Figueiredo, L.S.; Baltar, A.; Ma, M.; Navab, N.; Teichrieb, V.; Fallavollita, P. MirrARbilitation: A clinically-related gesture recognition interactive tool for an AR rehabilitation system. Comput. Methods Programs Biomed. 2016, 135, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Brokaw, E.B.; Lum, P.S.; Cooper, R.A.; Brewer, B.R. Using the kinect to limit abnormal kinematics and compensation strategies during therapy with end effector robots. In Proceedings of the 2013 IEEE 13th International Conference on Rehabilitation Robotics (ICORR), Seattle, WA, USA, 24–26 June 2013; pp. 1–6. [Google Scholar]
- Rado, D.; Sankaran, A.; Plasek, J.M.; Nuckley, D.J.; Keefe, D.F. Poster: A Real-Time Physical Therapy Visualization Strategy to Improve Unsupervised Patient Rehabilitation. In Proceedings of the IEEE Visualization, Atlantic City, NJ, USA, 11–16 October 2009. [Google Scholar]
- Khademi, M.; Hondori, H.M.; Dodakian, L.; Cramer, S.; Lopes, C.V. Comparing “pick and place” task in spatial Augmented Reality versus non-immersive Virtual Reality for rehabilitation setting. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 4613–4616. [Google Scholar]
- Liao, Y.; Vakanski, A.; Xian, M. A deep learning framework for assessment of quality of rehabilitation exercises. arXiv 2019, arXiv:1901.10435. [Google Scholar]
- Liao, Y.; Vakanski, A.; Xian, M. A Deep Learning Framework for Assessing Physical Rehabilitation Exercises. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 468–477. [Google Scholar] [CrossRef]
- Cano Porras, D.; Siemonsma, P.; Inzelberg, R.; Zeilig, G.; Plotnik, M. Advantages of virtual reality in the rehabilitation of balance and gait. Neurology 2018, 90, 1017–1025. [Google Scholar] [CrossRef]
- Feng, H.; Li, C.; Liu, J.; Wang, L.; Ma, J.; Li, G.; Gan, L.; Shang, X.; Wu, Z. Virtual Reality Rehabilitation Versus Conventional Physical Therapy for Improving Balance and Gait in Parkinson’s Disease Patients: A Randomized Controlled Trial. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2019, 25, 4186–4192. [Google Scholar] [CrossRef]
- John, J.; Wild, J.; Franklin, T.D.; Woods, G.W. Patellar pain and quadriceps rehabilitation: An EMG study. Am. J. Sport. Med. 1982, 10, 12–15. [Google Scholar] [CrossRef]
- Mulas, M.; Folgheraiter, M.; Gini, G. An EMG-controlled exoskeleton for hand rehabilitation. In Proceedings of the 9th International Conference on Rehabilitation Robotics, Chicago, IL, USA, 28 June–1 July 2005; pp. 371–374. [Google Scholar]
- Sarasola-Sanz, A.; Irastorza-Landa, N.; López-Larraz, E.; Bibián, C.; Helmhold, F.; Broetz, D.; Birbaumer, N.; Ramos-Murguialday, A. A hybrid brain-machine interface based on EEG and EMG activity for the motor rehabilitation of stroke patients. In Proceedings of the 2017 International Conference on Rehabilitation Robotics (ICORR), London, UK, 17–20 July 2017; pp. 895–900. [Google Scholar]
- Liu, L.; Chen, X.; Lu, Z.; Cao, S.; Wu, D.; Zhang, X. Development of an EMG-ACC-Based Upper Limb Rehabilitation Training System. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 244–253. [Google Scholar] [CrossRef]
- Berg, A.; Palomäki, H.; Lehtihalmes, M.; Lönnqvist, J.; Kaste, M. Poststroke depression: An 18-month follow-up. Stroke 2003, 34, 138–143. [Google Scholar] [CrossRef]
- Paolucci, S.; Antonucci, G.A.; Grasso, M.G.; Morelli, D.; Troisi, E.M.; Coiro, P.; Angelis, D.D.; Rizzi, F.; Bragoni, M. Post-stroke depression, antidepressant treatment and rehabilitation results. A case-control study. Cerebrovasc. Dis. 2001, 12, 264–271. [Google Scholar] [CrossRef] [PubMed]
- Rincon, A.L.; Yamasaki, H.; Shimoda, S. Design of a video game for rehabilitation using motion capture, EMG analysis and virtual reality. In Proceedings of the 2016 International Conference on Electronics, Communications and Computers (CONIELECOMP), Cholula, Mexico, 24–26 February 2016; pp. 198–204. [Google Scholar]
- Vourvopoulos, A.; Badia, S.B. Motor priming in virtual reality can augment motor-imagery training efficacy in restorative brain-computer interaction: A within-subject analysis. J. Neuroeng. Rehabil. 2016, 13, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Perez-Marcos, D.; Chevalley, O.H.; Schmidlin, T.W.; Garipelli, G.; Serino, A.; Vuadens, P.; Tadi, T.; Blanke, O.; Millán, J.D.R. Increasing upper limb training intensity in chronic stroke using embodied virtual reality: A pilot study. J. Neuroeng. Rehabil. 2017, 14, 119. [Google Scholar] [CrossRef] [PubMed]
- Adamovich, S.V.; Fluet, G.G.; Tunik, E.; Merians, A.S. Sensorimotor training in virtual reality: A review. NeuroRehabilitation 2009, 25, 29–44. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.H.; Chen, P.C.; Liu, K.C.; Chan, C.T. Wearable Sensor-Based Rehabilitation Exercise Assessment for Knee Osteoarthritis. Sensors 2015, 15, 4193–4211. [Google Scholar] [CrossRef] [PubMed]
- Saito, H.; Watanabe, T.; Arifin, A. Ankle and Knee Joint Angle Measurements during Gait with Wearable Sensor System for Rehabilitation. In Proceedings of the World Congress on Medical Physics and Biomedical Engineering, Munich, Germany, 7–12 September 2009. [Google Scholar]
- Bonato, P. Advances in wearable technology and applications in physical medicine and rehabilitation. J. Neuroeng. Rehabil. 2005, 2, 2. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Park, H.J.; Bonato, P.; Chan, L.E.; Rodgers, M.M. A review of wearable sensors and systems with application in rehabilitation. J. Neuroeng. Rehabil. 2011, 9, 21. [Google Scholar] [CrossRef]
- Leonardis, D.D.; Barsotti, M.; Loconsole, C.; Solazzi, M.; Troncossi, M.; Mazzotti, C.; Parenti-Castelli, V.; Procopio, C.; Lamola, G.; Chisari, C.; et al. An EMG-Controlled Robotic Hand Exoskeleton for Bilateral Rehabilitation. IEEE Trans. Haptics 2015, 8, 140–151. [Google Scholar] [CrossRef]
- Ganesan, Y.; Gobee, S.; Durairajah, V. Development of an Upper Limb Exoskeleton for Rehabilitation with Feedback from EMG and IMU Sensor. Procedia Comput. Sci. 2015, 76, 53–59. [Google Scholar] [CrossRef]
- Abdallah, I.B.; Bouteraa, Y.; Rekik, C. Design and Development of 3D Printed Myoelectric Robotic Exoskeleton for Hand Rehabilitation. Int. J. Smart Sens. Intell. Syst. 2017, 10, 341–366. [Google Scholar] [CrossRef]
- Kim, J.; Bee, N.; Wagner, J.; André, E. Emote to Win: Affective Interactions with a Computer Game Agent; Gesellschaft fur Informatik e.V.: Bonn, Germany, 2004; pp. 159–164. [Google Scholar]
- Kim, J.; Mastnik, S.; André, E. EMG-based hand gesture recognition for realtime biosignal interfacing. In Proceedings of the 13th International Conference on Intelligent User Interfaces, Gran Canaria, Spain, 13–16 January 2008; pp. 30–39. [Google Scholar]
- Qi, J.; Jiang, G.; Li, G.; Sun, Y.; Tao, B. Surface EMG hand gesture recognition system based on PCA and GRNN. Neural Comput. Appl. 2019, 32, 6343–6351. [Google Scholar] [CrossRef]
- Shi, W.T.; Lyu, Z.J.; Tang, S.T.; Chia, T.L.; Yang, C.Y. A bionic hand controlled by hand gesture recognition based on surface EMG signals: A preliminary study. Biocybern. Biomed. Eng. 2018, 38, 126–135. [Google Scholar] [CrossRef]
- Su, H.; Ovur, S.E.; Zhou, X.; Qi, W.; Ferrigno, G.; Momi, E. Depth vision guided hand gesture recognition using electromyographic signals. Adv. Robot. 2020, 34, 985–997. [Google Scholar] [CrossRef]
- Geng, W.; Du, Y.M.; Jin, W.; Wei, W.; Hu, Y.H.; Li, J. Gesture recognition by instantaneous surface EMG images. Sci. Rep. 2016, 6, 36571. [Google Scholar] [CrossRef] [PubMed]
- Amma, C.; Krings, T.; Böer, J.; Schultz, T. Advancing Muscle-Computer Interfaces with High-Density Electromyography. In Proceedings of the 33rd Annual ACM Conference on Human Factors in Computing Systems, Seoul, Korea, 18–23 April 2015. [Google Scholar]
- Atzori, M.; Gijsberts, A.; Heynen, S.; Hager, A.G.M.; Deriaz, O.; van der Smagt, P.; Castellini, C.; Caputo, B.; Muller, H. Building the Ninapro database: A resource for the biorobotics community. In Proceedings of the 2012 4th IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics (BioRob), Rome, Italy, 24–27 June 2012; pp. 1258–1265. [Google Scholar]
- Pizzolato, S.; Tagliapietra, L.; Cognolato, M.; Reggiani, M.; Müller, H.; Atzori, M. Comparison of six electromyography acquisition setups on hand movement classification tasks. PLoS ONE 2017, 12, e0186132. [Google Scholar] [CrossRef]
- Nasri, N.; Orts, S.; Gomez-Donoso, F.; Cazorla, M. Inferring Static Hand Poses from a Low-Cost Non-Intrusive sEMG Sensor. Sensors 2019, 19, 371. [Google Scholar] [CrossRef]
- Nasri, N.; Gomez-Donoso, F.; Orts, S.; Cazorla, M. Using Inferred Gestures from sEMG Signal to Teleoperate a Domestic Robot for the Disabled. In Proceedings of the IWANN, Gran Canaria, Spain, 12–14 June 2019. [Google Scholar]
- Oskoei, M.A.; Hu, H. Myoelectric control systems—A survey. Biomed. Signal Process. Control 2007, 2, 275–294. [Google Scholar] [CrossRef]
- Allard, U.C.; Nougarou, F.; Fall, C.L.; Giguère, P.; Gosselin, C.; Laviolette, F.; Gosselin, B. A convolutional neural network for robotic arm guidance using sEMG based frequency-features. In Proceedings of the 2016 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS), Daejeon, Korea, 9–14 October 2016; pp. 2464–2470. [Google Scholar]
- Du, Y.; Wong, Y.; Jin, W.; Wei, W.; Hu, Y.; Kankanhalli, M.S.; Geng, W. Semi-Supervised Learning for Surface EMG-based Gesture Recognition. In Proceedings of the IJCAI, Melbourne, Australia, 19–25 August 2017. [Google Scholar]
- Liu, G.; Zhang, L.; Han, B.; Zhang, T.; Wang, Z.; Wei, P. sEMG-Based Continuous Estimation of Knee Joint Angle Using Deep Learning with Convolutional Neural Network. In Proceedings of the 2019 IEEE 15th International Conference on Automation Science and Engineering (CASE), Vancouver, BC, Canada, 22–26 August 2019; pp. 140–145. [Google Scholar]
- Zhang, J.; Dai, J.; Chen, S.; Xu, G.; Gao, X. Design of Finger Exoskeleton Rehabilitation Robot Using the Flexible Joint and the MYO Armband. In Proceedings of the ICIRA, Shenyang, China, 8–11 August 2019. [Google Scholar]
- Longo, B.; Sime, M.M.; Bastos-Filho, T. Serious Game Based on Myo Armband for Upper-Limb Rehabilitation Exercises. In Proceedings of the XXVI Brazilian Congress on Biomedical Engineering, Armacao de Buzios, Brazil, 21–25 October 2019. [Google Scholar]
- Widodo, M.S.; Zikky, M.; Nurindiyani, A.K. Guide Gesture Application of Hand Exercises for Post-Stroke Rehabilitation Using Myo Armband. In Proceedings of the 2018 International Electronics Symposium on Knowledge Creation and Intelligent Computing (IES-KCIC), Bali, Indonesia, 29–30 October 2018; pp. 120–124. [Google Scholar]
- Cho, K.; van Merrienboer, B.; Gülçehre, Ç.; Bahdanau, D.; Bougares, F.; Schwenk, H.; Bengio, Y. Learning Phrase Representations using RNN Encoder-Decoder for Statistical Machine Translation. In Proceedings of the EMNLP, Doha, Qatar, 25–29 October 2014. [Google Scholar]
- Bahdanau, D.; Cho, K.; Bengio, Y. Neural Machine Translation by Jointly Learning to Align and Translate. arXiv 2015, arXiv:1409.0473. [Google Scholar]
- Sutskever, I.; Vinyals, O.; Le, Q.V. Sequence to Sequence Learning with Neural Networks. arXiv 2014, arXiv:1409.3215. [Google Scholar]
- Chung, J.; Gülçehre, Ç.; Cho, K.; Bengio, Y. Empirical Evaluation of Gated Recurrent Neural Networks on Sequence Modeling. arXiv 2014, arXiv:1412.3555. [Google Scholar]
- Ballas, N.; Yao, L.; Pal, C.J.; Courville, A.C. Delving Deeper into Convolutional Networks for Learning Video Representations. arXiv 2016, arXiv:1511.06432. [Google Scholar]
- Jiang, R.; Zhao, L.; Wang, T.; Wang, J.; Zhang, X. Video Deblurring via Temporally and Spatially Variant Recurrent Neural Network. IEEE Access 2020, 8, 7587–7597. [Google Scholar] [CrossRef]
- Tian, L.; Li, X.; Ye, Y.; Xie, P.; Li, Y. A Generative Adversarial Gated Recurrent Unit Model for Precipitation Nowcasting. IEEE Geosci. Remote Sens. Lett. 2020, 17, 601–605. [Google Scholar] [CrossRef]
- Asadi-Aghbolaghi, M.; Clapes, A.; Bellantonio, M.; Escalante, H.J.; Ponce-López, V.; Baró, X.; Guyon, I.; Kasaei, S.; Escalera, S. A survey on deep learning based approaches for action and gesture recognition in image sequences. In Proceedings of the 2017 12th IEEE International Conference on Automatic Face & Gesture Recognition (FG 2017), Washington, DC, USA, 30 May–3 June 2017; pp. 476–483. [Google Scholar]
- Devineau, G.; Moutarde, F.; Xi, W.; Yang, J. Deep learning for hand gesture recognition on skeletal data. In Proceedings of the 2018 13th IEEE International Conference on Automatic Face & Gesture Recognition (FG 2018), Xi’an, China, 15–19 May 2018; pp. 106–113. [Google Scholar]
- Wei, W.; Dai, Q.; Wong, Y.; Hu, Y.; Kankanhalli, M.; Geng, W. Surface-Electromyography-Based Gesture Recognition by Multi-View Deep Learning. IEEE Trans. Biomed. Eng. 2019, 66, 2964–2973. [Google Scholar] [CrossRef] [PubMed]
- Atzori, M.; Cognolato, M.; Müller, H. Deep learning with convolutional neural networks applied to electromyography data: A resource for the classification of movements for prosthetic hands. Front. Neurorobotics 2016, 10, 9. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Song, Q.; Han, H.; Cheng, J. Sequentially supervised long short-term memory for gesture recognition. Cogn. Comput. 2016, 8, 982–991. [Google Scholar] [CrossRef]
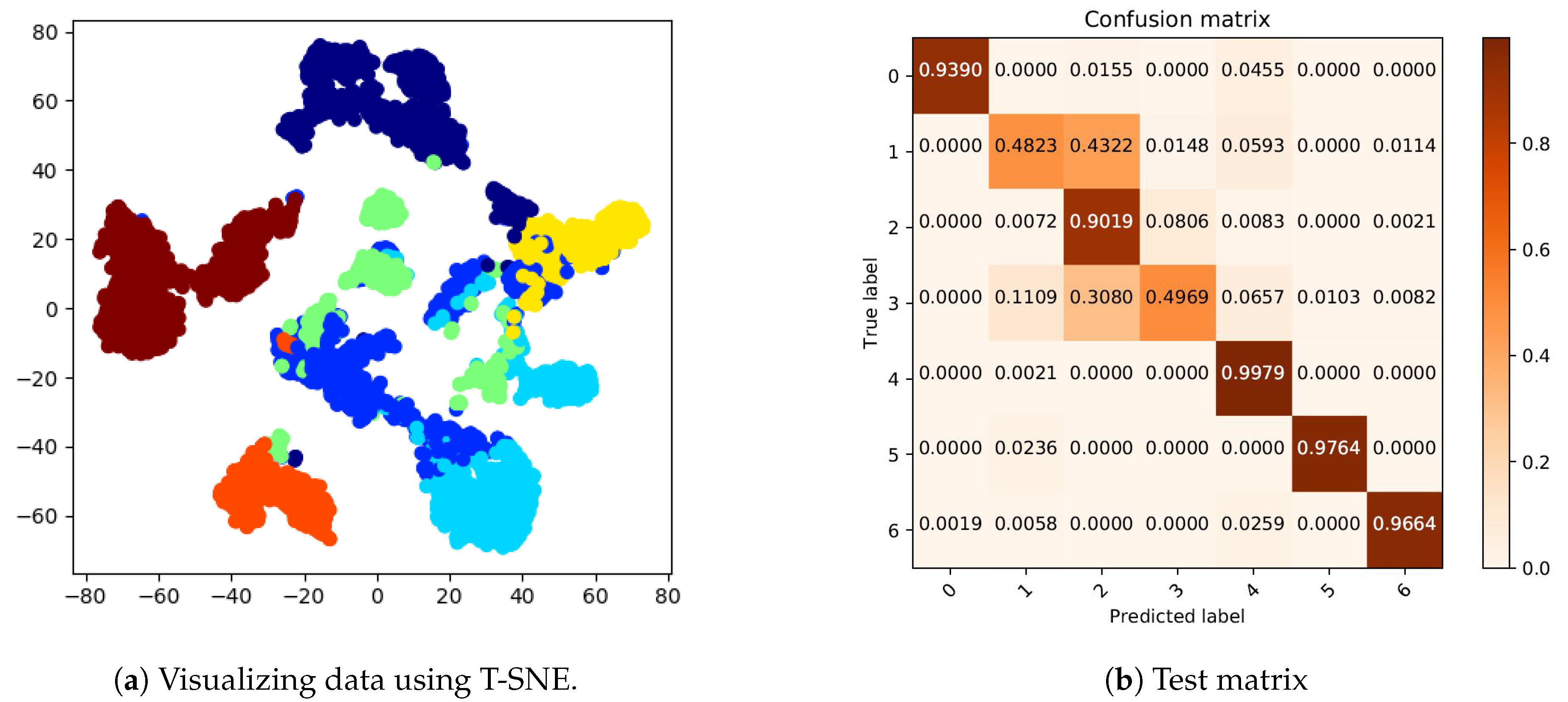
- Maaten, L.v.d.; Hinton, G. Visualizing data using t-SNE. J. Mach. Learn. Res. 2008, 9, 2579–2605. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Round1 | Round2 | Round3 | Round4 | Round5 | Player’s Opinion | |
| Subject 1 | Win | Win | Lose | Win | Lose | It is challenging and enjoyable |
| Subject 2 | Lose | Win | win | Lose | Lose | The sphere has too much speed |
| Subject 3 | Win | Lose | Win | Lose | Lose | The route should be extended |
| Subject 4 | Lose | Win | Lose | Lose | Lose | It is a difficult game to control with the armband |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nasri, N.; Orts-Escolano, S.; Cazorla, M. An sEMG-Controlled 3D Game for Rehabilitation Therapies: Real-Time Time Hand Gesture Recognition Using Deep Learning Techniques. Sensors 2020, 20, 6451. https://doi.org/10.3390/s20226451
Nasri N, Orts-Escolano S, Cazorla M. An sEMG-Controlled 3D Game for Rehabilitation Therapies: Real-Time Time Hand Gesture Recognition Using Deep Learning Techniques. Sensors. 2020; 20(22):6451. https://doi.org/10.3390/s20226451
Chicago/Turabian StyleNasri, Nadia, Sergio Orts-Escolano, and Miguel Cazorla. 2020. "An sEMG-Controlled 3D Game for Rehabilitation Therapies: Real-Time Time Hand Gesture Recognition Using Deep Learning Techniques" Sensors 20, no. 22: 6451. https://doi.org/10.3390/s20226451
APA StyleNasri, N., Orts-Escolano, S., & Cazorla, M. (2020). An sEMG-Controlled 3D Game for Rehabilitation Therapies: Real-Time Time Hand Gesture Recognition Using Deep Learning Techniques. Sensors, 20(22), 6451. https://doi.org/10.3390/s20226451