Timed Up and Go and Six-Minute Walking Tests with Wearable Inertial Sensor: One Step Further for the Prediction of the Risk of Fall in Elderly Nursing Home People


 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Population
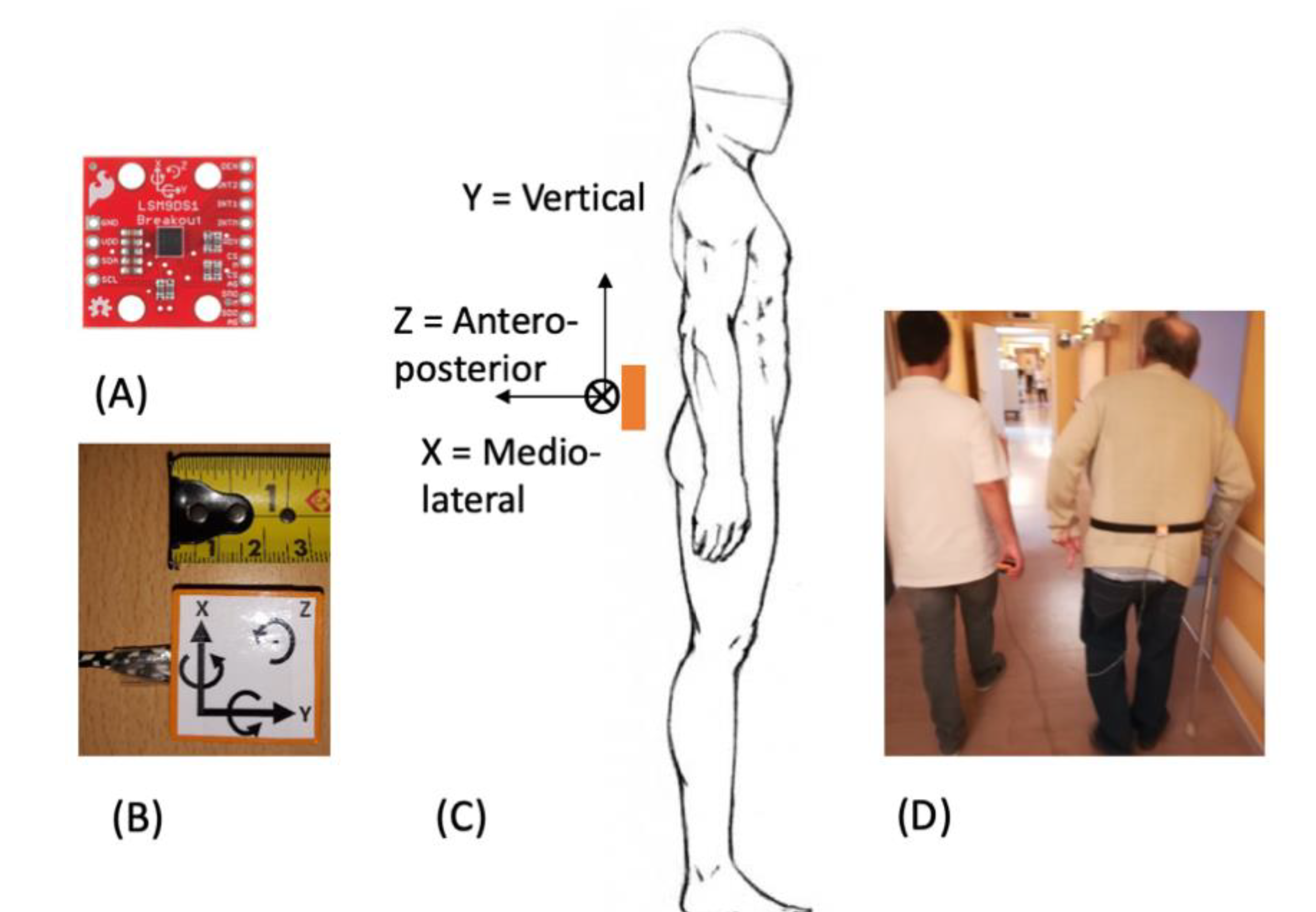
2.2. Protocol
2.3. Data Analysis
3. Results
3.1. Variability Indices
3.2. TUG and TUG+ Tests
3.3. AI Classification
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. TUG and TUG+ Tests with Logistic Regressions


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TUG (Logit) | TUG+ (Logit) | |
|---|---|---|
| Se | 0.837 | 0.898 |
| Sp | 0.250 | 0.333 |
| LR+ | 1.12 | 1.35 |
| LR− | 0.652 | 0.306 |
| PPV | 0.695 | 0.733 |
| NPV | 0.439 | 0.615 |
| Acc | 0.644 | 0.712 |
References
- Fatal Falls: WHO, Mortality Database 2010–2012. Available online: http://www.who.int/healthinfo/mortality_data/en/ (accessed on 12 February 2020).
- Hartholt, K. Falls and Drugs in Older Population: Medical and Societal Consequences; Erasmus University: Rotterdam, The Netherlands, 2011. [Google Scholar]
- Moreland, J.D.; Richardson, J.A.; Goldsmith, C.H.; Clase, C.M. Muscle weakness and falls in older adults: A systematic review and meta-analysis. J. Am. Geriatr. Soc. 2004, 52, 1121–1129. [Google Scholar] [CrossRef] [PubMed]
- Rossat, A.; Fantino, B.; Nitenberg, C.; Annweiler, C.; Poujol, L.; Herrmann, F.R.; Beauchet, O. Risk factors for falling in community-dwelling older adults: Which of them are associated with the recurrence of falls? J. Nutr. Health Aging 2010, 14, 787–791. [Google Scholar] [CrossRef] [PubMed]
- Ambrose, A.F.; Paul, G.; Hausdorff, J.M. Risk factors for falls among older adults: A review of the literature. Maturitas 2013, 75, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Posdiadlo, D.; Richardson, S. The time “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Herman, T.; Giladi, N.; Hausdorff, J.M. Properties of the ‘timed up and go’ test: More than meets the eye. Gerontology 2011, 57, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Panel on Prevention of Falls in Older Persons; American Geriatrics Society; British Geriatrics Society. Summary of the Updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons. J. Am. Geriatr. Soc. 2011, 14, 148–157. [Google Scholar]
- Hausdorff, J.M.; Rios, D.A.; Edelberg, H.K. Gait variability and fall risk in community-living older adults: A 1-year prospective study. Arch. Phys. Med. Rehabil. 2001, 82, 1050–1056. [Google Scholar] [CrossRef]
- Weiss, A.; Herman, T.; Plotnik, M.; Brozgol, M.; Giladi, N.; Hausdorff, J.M. An instrumented timed up and go: The added value of an accelerometer for identifying fall risk in idiopathic fallers. Physiol. Meas. 2011, 32, 2003–2018. [Google Scholar] [CrossRef] [PubMed]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar]
- Jehn, M.; Schmidt-Trucksäess, M.D.; Schuster, T.; Hanssen, H.; Weis, M.; Halle, M.; Koehler, F. Accelerometer-Based Quantification of 6-Minute Walk Test Performance in Patients with Chronic Heart Failure: Applicability in Telemedicine. J. Card. Fail. 2009, 15, 334–340. [Google Scholar] [CrossRef]
- Annegarn, J.; Spruit, M.A.; Savelberg, H.H.C.M.; Willems, P.J.B.; van de Bool, C.; Schols, A.M.W.J.; Wouters, E.F.M.; Meijer, K. Differences in Walking Pattern during 6-Min Walk Test between Patients with COPD and Healthy Subjects. PLoS ONE 2012, 7, e37329. [Google Scholar] [CrossRef]
- Hage, R.; Detrembleur, C.; Dierick, F.; Pitance, L.; Jojczyk, L.; Estievenart, W.; Buisseret, F. DYSKIMOT: An Ultra-Low-Cost Inertial Sensor to Assess Head’s Rotational Kinematics in Adults during the Didren-Laser Test. Sensors 2020, 20, 833. [Google Scholar] [CrossRef] [PubMed]
- Oks, A.; Katashev, A.; Zadinans, M.; Rancans, M.; Litvak, J. Development of Smart Sock System for Gate Analysis and Foot Pressure Control. In XIV Mediterranean Conference on Medical and Biological Engineering and Computing; Kyriacou, E., Christofides, S., Pattichis, C.S., Eds.; Springer International Publishing: Paphos, Cyprus, 2016; pp. 466–469. [Google Scholar]
- Esfahani, M.I.M.; Nussbaum, M.A.; Kong, Z. Using a smart textile system for classifying occupational manual material handling tasks: Evidence from lab-based simulations. Ergonomics 2019, 62, 823–833. [Google Scholar] [CrossRef] [PubMed]
- Rajagopalan, R.; Litvan, I.; Jung, T.-P. Fall Prediction and Prevention Systems: Recent Trends, Challenges, and Future Research Directions. Sensors 2017, 17, 2509. [Google Scholar] [CrossRef] [PubMed]
- Moulias, S.; Peigne, V.; Guérin, O.; Daire, R. Gériatrie, Cahier des EC, 3rd ed; Elsevier Masson: Paris, France, 2015; p. 95. [Google Scholar]
- Dierick, F.; Nivard, A.-L.; White, O.; Buisseret, F. Fractal analyses reveal independent complexity and predictability of gait. PLoS ONE 2017, 12, e0188711. [Google Scholar] [CrossRef]
- Kantz, H.; Schreiber, T. Nonlinear Time Series Analysis; Cambridge University Press: Cambridge, UK, 2004. [Google Scholar]
- Hausdorff, J.M.; Peng, C.K.; Ladin, Z.; Wei, J.Y.; Goldberger, A.L. Is walking a random walk? Evidence for long-range correlations in stride interval of human gait. J. Appl. Physiol. 1995, 78, 349–358. [Google Scholar] [CrossRef]
- Goodfellow, I.; Bengio, Y.; Courville, A. Deep Learning; MIT Press: Cambridge, MA, USA, 2016. [Google Scholar]
- Bergstra, J.; Bengio, Y. Random Search for Hyper-Parameter Optimization. J. Mach. Learn. Res. 2012, 13, 281. [Google Scholar]
- Shumway-Cook, A.; Brauer, S.; Woollacott, M. Predicting the Probability for Falls in Community-Dwelling Older Adults Using the Timed Up & Go Test. Phys. Ther. 2000, 80, 896–903. [Google Scholar]
- Schoene, D.; Wu, S.M.-S.; Mikolaizak, A.S.; Menant, J.C.; Smith, S.T.; Delbaere, K.; Lord, S.R. Discriminative ability and predictive validity of the timed up and go test in identifying older people who fall: Systematic review and meta-analysis. J. Am. Geriatr. Soc. 2013, 61, 202–208. [Google Scholar] [CrossRef]
- Viccaro, L.J.; Perera, S.; Studenski, S.A. Is timed up and go better than gait speed in predicting health, function, and falls in older adults? J. Am. Geriatr. Soc. 2001, 59, 887–892. [Google Scholar] [CrossRef]
- Preece, S.J.; Kenney, L.P.; Major, M.J.; Dias, T.; Lay, E.; Fernandes, B.T. Automatic identification of gait events using an instrumented sock. J. Neuroeng. Rehabil. 2011, 8, 32. [Google Scholar] [CrossRef]
- Tirosh, O.; Begg, R.; Passmore, E.; Knopp-Steinberg, N. Wearable textile sensor sock for gait analysis. In Proceedings of the Seventh International Conference on Sensing Technology, Wellington, New Zealand, 3–5 December 2013. [Google Scholar]
- Bergmann, J.H.M.; Chandaria, V.; McGregor, A. Wearable and implantable sensors: The patient’s perspective. Sensors 2012, 12, 16695–16709. [Google Scholar] [CrossRef]
- Kavanagh, J.J.; Barrett, R.S.; Morrison, S. Upper body accelerations during walking in healthy young and elderly men. Gait Posture 2004, 20, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Goldberger, A.L.; Amaral, L.A.N.; Hausdorff, J.M.; Ivanov, P.C.; Peng, C.-K.; Stanley, H.E. Fractal dynamics in physiology: Alterations with disease and aging. Proc. Natl. Acad. Sci. USA 2002, 99 (Suppl. 1), 2466–2472. [Google Scholar] [CrossRef] [PubMed]
- Kobsar, D.; Olson, C.; Paranjape, R.; Hadjistavropoulos, T.; Barden, J.M. Evaluation of age-related differences in the stride-to-stride fluctuations, regularity and symmetry of gait using a waist-mounted tri-axial accelerometer. Gait Posture 2014, 39, 553–557. [Google Scholar] [CrossRef]
- Sciurba, F.; Criner, G.J.; Lee, S.M.; Mohsenifar, Z.; Shade, D.; Slivka, W.; Wise, R.A. National Emphysema Treatment Trial Research Group. Six-minute Walk Distance in Chronic Obstructive Pulmonary Disease: Reproducibility and Effect of Walking Course Layout and Length. Am. J. Respir. Crit. Care Med. 2003, 167, 1522–1527. [Google Scholar] [CrossRef]
- Sun, R.; Sosnoff, J.J. Novel sensing technology in fall risk assessment in older adults: A systematic review. BMC Geriatr. 2014, 18, 14. [Google Scholar] [CrossRef] [PubMed]
- Howcroft, J.; Lemaire, E.D.; Kofman, J. Wearable-Sensor-Based Classification Models of Faller Status in Older Adults. PLoS ONE 2016, 11, e0153240. [Google Scholar] [CrossRef]
- Wall, J.C.; Bell, C.; Campbell, S.; Davis, J. The Timed Get-up-and-Go test revisited: Measurement of the component tasks. J. Rehabil. Res. Dev. 2000, 37, 109–113. [Google Scholar]
- Greene, B.R.; Doheny, E.P.; Kenny, R.A.; Caulfield, B. Classification of frailty and falls history using a combination of sensor-based mobility assessments. Physiol. Meas. 2014, 35, 2053–2066. [Google Scholar] [CrossRef]
- Greene, B.; Redmond, S.; Caulfield, B. Fall Risk Assessment through Automatic Combination of Clinical Fall Risk Factors and Body-Worn Sensor Data. IEEE J. Biomed. Health Inform. 2016, 21, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Luna-Perejón, F.; Domínguez-Morales, M.J.; Civit-Balcells, A. Wearable Fall Detector Using Recurrent Neural Networks. Sensors 2019, 19, 4885. [Google Scholar] [CrossRef] [PubMed]
- Santos, G.L.; Endo, P.T.; Monteiro, K.H.C.; Rocha, E.S.; Silva, I.; Lynn, T. Accelerometer-Based Human Fall Detection Using Convolutional Neural Networks. Sensors 2019, 19, 1644. [Google Scholar] [CrossRef]
- Zhang, J.; Wu, C.; Wang, Y. Human Fall Detection Based on Body Posture Spatio-Temporal Evolution. Sensors 2020, 20, 946. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, J.H.M.; McGregor, A.H. Body-worn sensor design: What do patients and clinicians want? Ann. Biomed. Eng. 2011, 39, 2299–2312. [Google Scholar] [CrossRef]
- Mokhlespour Esfahani, M.I.; Nussbaum, M.A. Classifying Diverse Physical Activities Using “Smart Garments”. Sensors 2019, 19, 3133. [Google Scholar] [CrossRef]








| t1 | t2 | |
|---|---|---|
| N | 80 | 73 |
| Age (years) | 83.2 ± 8.2 | 83.0 ± 8.3 |
| Male/Female | 28/52 | 28/45 |
| Walking aid required | 49 | 52 |
| Hypertension (%) | 44 | 42 |
| Number of medications | 4 [2–5] | 4 [2–5] |
| Cerebrovascular accident (%) | 10 | 10 |
| Dementia (%) | 14 | 16 |
| Previous heart surgery (%) | 21 | 23 |
| Diabetes (%) | 16 | 15 |
| Hip or knee replacement (%) | 16 | 16 |
| Fallers | 23 | |
| TUG (s) | 20 [17–27] | 17 [14–23] |
| Fallers | Nonfallers | p | |
|---|---|---|---|
| SDav (m/s2) | 0.0949 [0.0810–0.149] | 0.101 [0.0868–0.130] | 0.245 |
| SDaml (m/s2) | 0.0864 [0.0752–0.109] | 0.0950 [0.0747–0.109] | 0.891 |
| SDaap (m/s2) | 0.120 [0.0901–0.173] | 0.0900 [0.0753–0.120] | 0.010 |
| SDωv (°/s) | 17.4 [15.5–20.2] | 18.4 [15.0–21.9] | 0.957 |
| SDωml (°/s) | 15.8 [12.3–20.3] | 13.7 [11.1–19.2] | 0.480 |
| SDωap (°/s) | 8.29 [6.77–11.6] | 8.79 [7.44–12.6] | 0.487 |
| Dav | 1.78 [1.73–1.82] | 1.81 [1.77–1.85] | 0.044 |
| Daml | 1.78 [1.66–1.81] | 1.81 [1.77–1.83] | 0.088 |
| Daap | 1.73 [1.68–1.80] | 1.79 [1.73–1.83] | 0.072 |
| Dωv | 1.71 [1.67–1.76] | 1.74 [1.69–1.76] | 0.376 |
| Dωml | 1.74 [1.71–1.78] | 1.78 [1.72–1.82] | 0.098 |
| Dωap | 1.81 [1.75–1.83] | 1.82 [1.78–1.85] | 0.149 |
| TUG (s) | 23 [19–31] | 19 [16–25] | 0.035 |
| TUG | TUG+ | AI | |
|---|---|---|---|
| Se | 0.714 | 0.857 | 0.750 |
| Sp | 0.541 | 0.500 | 0.750 |
| LR+ | 1.56 | 1.71 | 3.00 |
| LR− | 0.529 | 0.286 | 0.333 |
| PPV | 0.481 | 0.778 | 0.750 |
| NPV | 0.761 | 0.632 | 0.750 |
| Acc | 0.657 | 0.739 | 0.750 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buisseret, F.; Catinus, L.; Grenard, R.; Jojczyk, L.; Fievez, D.; Barvaux, V.; Dierick, F. Timed Up and Go and Six-Minute Walking Tests with Wearable Inertial Sensor: One Step Further for the Prediction of the Risk of Fall in Elderly Nursing Home People. Sensors 2020, 20, 3207. https://doi.org/10.3390/s20113207
Buisseret F, Catinus L, Grenard R, Jojczyk L, Fievez D, Barvaux V, Dierick F. Timed Up and Go and Six-Minute Walking Tests with Wearable Inertial Sensor: One Step Further for the Prediction of the Risk of Fall in Elderly Nursing Home People. Sensors. 2020; 20(11):3207. https://doi.org/10.3390/s20113207
Chicago/Turabian StyleBuisseret, Fabien, Louis Catinus, Rémi Grenard, Laurent Jojczyk, Dylan Fievez, Vincent Barvaux, and Frédéric Dierick. 2020. "Timed Up and Go and Six-Minute Walking Tests with Wearable Inertial Sensor: One Step Further for the Prediction of the Risk of Fall in Elderly Nursing Home People" Sensors 20, no. 11: 3207. https://doi.org/10.3390/s20113207
APA StyleBuisseret, F., Catinus, L., Grenard, R., Jojczyk, L., Fievez, D., Barvaux, V., & Dierick, F. (2020). Timed Up and Go and Six-Minute Walking Tests with Wearable Inertial Sensor: One Step Further for the Prediction of the Risk of Fall in Elderly Nursing Home People. Sensors, 20(11), 3207. https://doi.org/10.3390/s20113207