
Eating Disorders and Diabetes: Facing the Dual Challenge



Abstract
:1. Introduction
2. Diabetes and Disordered Eating Behaviors/Eating Disorders
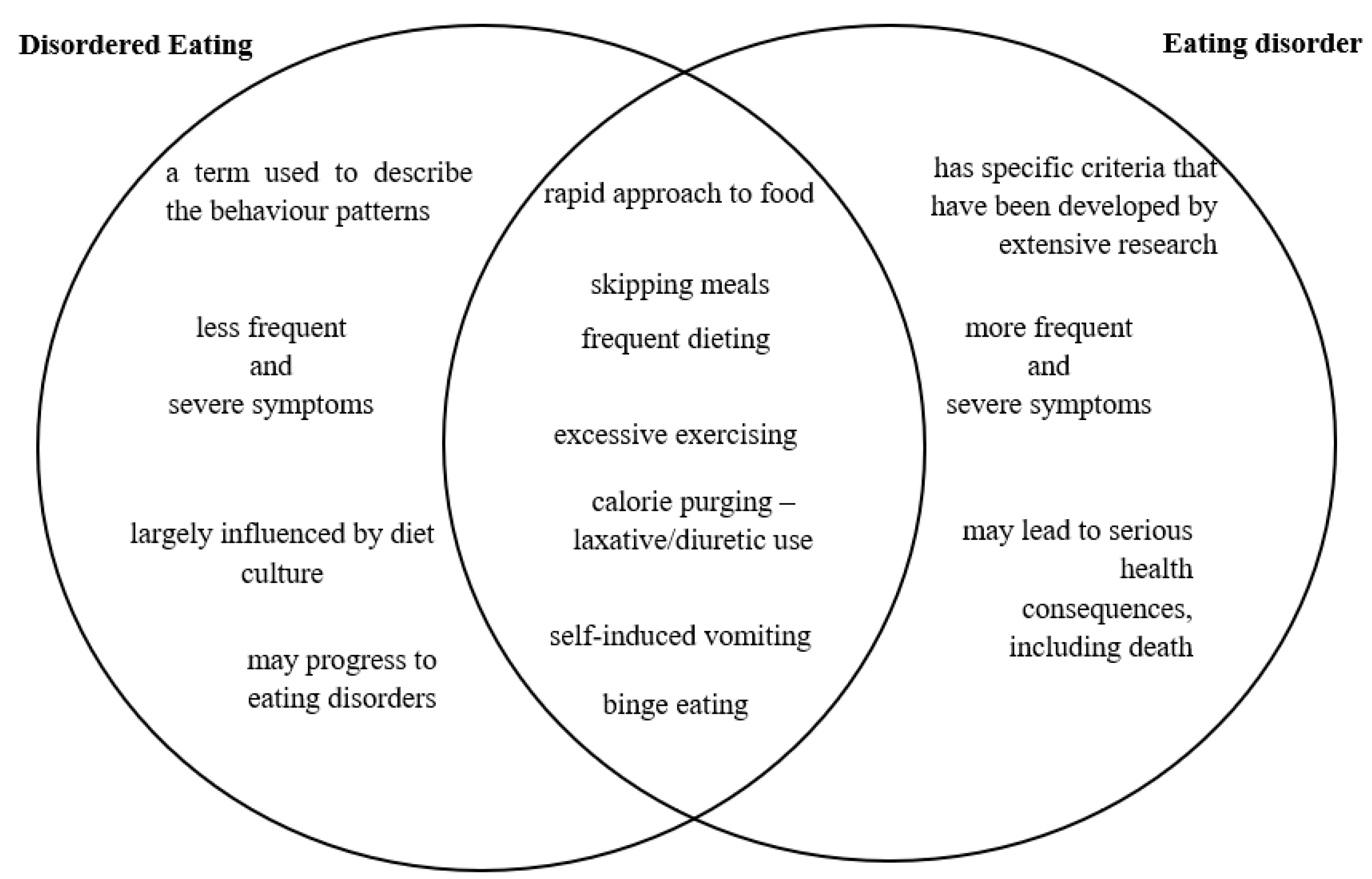
2.1. Disordered Eating vs. Eating Disorder
2.2. Eating Disorders in Type 1 Diabetes
2.2.1. Anorexia Nervosa
2.2.2. Avoidant/Restrictive Food Intake Disorder
2.2.3. Bulimia Nervosa
2.2.4. Diabulimia
2.3. Eating Disorders in Type 2 Diabetes
2.3.1. Binge Eating Disorder
2.3.2. Diarexia
2.3.3. Night Eating Syndrome
2.3.4. Orthorexia Nervosa
2.3.5. Pregorexia
3. Treating Eating Disorders and Diabetes—The Dual Challenge
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Weiselberg, E.C.; Gonzalez, M.; Fisher, M. Eating disorders in the twenty-first century. Minerva Ginecol. 2011, 63, 531–545. [Google Scholar] [PubMed]
- Arcelus, J.; Mitchell, A.J.; Wales, J.; Nielsen, S. Mortality rates in patients with anorexia nervosa and other eating disorders: A meta-analysis of 36 studies. Arch. Gen. Psychiatry 2011, 68, 724–731. [Google Scholar] [CrossRef] [PubMed]
- Santomauro, D.F.; Melen, S.; Mitchison, D.; Vos, T.; Whiteford, H.; Ferrari, A.J. The hidden burden of eating disorders: An extension of estimates from the Global Burden of Disease Study 2019. Lancet Psychiatry 2021, 8, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Hudson, J.I.; Hiripi, E.; Pope, H.G.; Kessler, R.C. The prevalence and correlates of eating disorders in the National Comorbidiy Survey Replication. Biol. Psychiatry 2007, 61, 348–358. [Google Scholar] [CrossRef]
- Galmiche, M.; Déchelotte, P.; Lambert, G.; Tavolacci, M.P. Prevalence of eating disorders over the 2000–2018 period: A systematic literature review. Am. J. Clin. Nutr. 2019, 109, 1402–1413. [Google Scholar] [CrossRef]
- Robinson, E.; Higgs, E. Liking food less: The impact of social influence on food liking evaluations in female students. PLoS ONE 2012, 7, e48858. [Google Scholar] [CrossRef]
- Medical News Today. Why Are Women More Vulnerable to Eating Disorders? Brain Study Sheds Light. 2016. Available online: https://www.medicalnewstoday.com/articles/313466#Using-virtual-reality-to-assess-the-brains-response-to-body-appearance (accessed on 20 March 2023).
- Engel, S.G.; Crosby, R.D.; Thomas, G.; Bond, D.; Lavender, J.M.; Mason, T.; Steffen, K.J.; Green, D.D.; Wonderlich, S.A. Ecological momentary assessment in eating disorder and obesity research: A review of the recent literature. Curr. Psychiatry Rep. 2016, 18, 37. [Google Scholar] [CrossRef]
- Crow, S.J.; Peterson, C.B.; Swanson, S.A.; Raymond, N.C.; Specker, S.; Eckert, E.D.; Mitchell, J.E. Increased mortality in bulimia nervosa and other eating disorders. Am. J. Psychiatry 2019, 166, 1342–1346. [Google Scholar] [CrossRef]
- Garber, A.K.; Cheng, J.; Accurso, E.C.; Adams, S.H.; Buckelew, S.M.; Kapphahn, C.J.; Kreiter, A.; Le Grange, D.; Machen, V.I.; Moscicki, A.-B.; et al. Weight loss and illness severity in adolescents with atypical anorexia nervosa. Pediatrics 2019, 144, e20192339. [Google Scholar] [CrossRef]
- Pisetsky, E.M.; Thornton, L.M.; Lichtenstein, P.; Pedersen, N.L.; Bulik, C.M. Suicide attempts in women with eating disorders. J. Abnorm. Psychol. 2013, 122, 1042–1056. [Google Scholar] [CrossRef]
- Halmi, A.K. Anorexia nervosa: An increasing problem in children and adolescents. Dialogues Clin. Neurosci. 2009, 11, 100–103. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, D.E.; Lynn, R.; Viner, R.M. Childhood eating disorders: British national surveillance study. Br. J. Psychiatry 2011, 198, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Wojtyła, A.; Biliński, P.; Bojar, I.; Wojtyła, C. Zaburzenia odżywiania u polskich gimnazjalistów. Prob. Hig. Epidemiol. 2011, 92, 343–350. [Google Scholar]
- Kołobo, H.; Woynarowska, B. Samoocena masy ciała i odchudzanie się młodzieży w okresie dojrzewania. Prz. Pediatryczny 2004, 34, 196–201. [Google Scholar]
- Hoek, H.W. Incidence, prevalence and mortality of anorexia nervosa and other eating disorders. Curr. Opin. Psychiatry 2006, 19, 389–394. [Google Scholar] [CrossRef]
- Ogden, C.L.; Carroll, M.D.; Curtin, L.R.; McDowell, M.A.; Tabak, C.J.; Flegal, K.M. Prevalence of overweight and obesity in the United States, 1999–2004. JAMA 2006, 295, 1549–1555. [Google Scholar] [CrossRef]
- Rabe-Jabłońska, J.; Pawełczyk, T.; Żechowski, C.; Jarema, M. Standardy leczenia zaburzeń odżywiania. Therapeutic standards in eating disorders. Psychiatr. I Psychol. Klin. 2008, 8, 20–40. [Google Scholar]
- Smink, R.R.E.; Van Hoeken, D.; Hoek, H.W. Epidemiology of eating disorders: Incidence, prevalence and mortality rates. Curr. Psychiatry Rep. 2012, 14, 406–414. [Google Scholar] [CrossRef]
- Gabbri-Goebel, A.; Copeland, P.; Touyz, S.; Hay, P. Editorial: Eating disorders in diabetes: Discussion on issues relevant to type 1 diabetes and an overview of the journal’s special issue. J. Eat. Disord. 2019, 7, 27. [Google Scholar] [CrossRef]
- Gagnon, C.; Aimé, A.; Bélanger, C.; Markowitz, J.T. Comorbid diabetes and eating disorders in adult patients. Diabetes Educ. 2012, 38, 537–542. [Google Scholar] [CrossRef]
- Goebel-Fabbri, A.E. Diabetes and eating disorders. J. Diabetes Sci. Technol. 2008, 2, 530–532. [Google Scholar] [CrossRef]
- Rydall, A.C.; Rodin, G.M.; Olmsted, M.P.; Devenyi, R.G.; Daneman, D. Disordered eating behavior and microvascular complications in young women with insulin-dependent diabetes mellitus. N. Engl. J. Med. 1997, 336, 1849–1854. [Google Scholar] [CrossRef]
- Steel, J.M.; Young, R.J.; Lloyd, G.G.; Clarke, B.F. Clinically apparent eating disorders in young diabetic women: Associations with painful neuropathy and other complications. Br. Med. J. 1987, 294, 859–862. [Google Scholar] [CrossRef]
- Affenito, S.; Lammi-Keefe, C.; Vogel, S.; Backstrand, J.; Welch, G.; Adams, C. Women with insulin-dependent diabetes mellitus (IDDM) complicated by eating disorders are at risk for exacerbated alterations in lipid metabolism. Eur. J. Clin. Nutr. 1997, 51, 462–466. [Google Scholar] [CrossRef] [PubMed]
- Custal, N.; Arcelus, J.; Agüera, Z.; I Bove, F.; Wales, J.; Granero, R.; Jiménez-Murcia, S.; Sánchez, I.; Riesco, N.; Alonso, P.; et al. Treatment outcome of patients with comorbid type 1 diabetes and eating disorders. BMC Psychiatry 2014, 14, 140. [Google Scholar] [CrossRef]
- Philpot, U. Eating disorders in young people with diabetes: Development, diagnosis and management. J. Diabetes Nurs. 2013, 17, 228–232. [Google Scholar]
- Winston, A.P. Eating Disorders and Diabetes. Curr. Diabetes Rep. 2020, 20, 32. [Google Scholar] [CrossRef] [PubMed]
- Hanlan, M.E.; Griffith, J.; Patel, N.; Jaser, S.S. Eating Disorders and Disordered Eating in Type 1 Diabetes: Prevalence, Screening, and Treatment Options. Curr. Diabetes Rep. 2013, 13, 909–916. [Google Scholar] [CrossRef] [PubMed]
- Toni, G.; Berioli, M.G.; Cerquiglini, L.; Ceccarini, G.; Grohmann, U.; Principi, N.; Esposito, S. Eating Disorders and Disordered Eating Symptoms in Adolescents with Type 1 Diabetes. Nutrients 2017, 9, 906. [Google Scholar] [CrossRef]
- Jones, J.M.; Lawson, M.L.; Daneman, D.; Olmsted, M.P.; Rodin, G. Eating disorders in adolescent females with and without type 1 diabetes: Cross sectional study. BMJ 2000, 320, 1563–1566. [Google Scholar] [CrossRef]
- Grylli, V.; Hafferl-Gattermayer, A.; Schober, E.; Karwautz, A. Prevalence and clinical manifestations of eating disorders in Austrian adolescents with type-1 diabetes. Wien Klin. Wochenschr. 2004, 116, 230–234. [Google Scholar] [CrossRef] [PubMed]
- Young, V.; Eiser, C.; Johnson, B.; Brierley, S.; Epton, T.; Elliott, J.; Heller, S. Eating problems in adolescents with Type 1 diabetes: A systematic review with meta-analysis. Diabet. Med. 2013, 30, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, L.J.; Banks, R.A.; Bennett Johnson, S.; Prine, J.M.; Desrosiers, P.M.; Silverstein, J.H. Disordered eating, body mass and glycemic control in adolescents with type 1 diabetes. Diabetes Care 2001, 24, 678–682. [Google Scholar] [CrossRef] [PubMed]
- Cass, K.; McGuire, C.; Bjork, I.; Sobotka, N.; Walsh, K.; Mehler, P.S. Medical Complications of Anorexia Nervosa. Psychosomatics 2020, 61, 625–631. [Google Scholar] [CrossRef]
- Lilenfeld, L.R.; Kaye, W.H.; Greeno, C.G.; Merikangas, K.R.; Plotnicov, K.; Pollice, C.; Rao, R.; Strober, M.; Bulik, C.M.; Nagy, L. A controlled family study of anorexia nervosa and bulimia nervosa: Psychiatric disorders in first-degree relatives and effects of proband comorbidity. Arch. Gen. Psychiatry 1998, 55, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Strober, M.; Freeman, R.; Lampert, C.; Diamond, J.; Kaye, W. Controlled family study of anorexia and bulimia nervosa: Evidence of shared liability and transmission of partial syndromes. Am. J. Psychiatry 2000, 157, 393–401. [Google Scholar] [CrossRef]
- Strober, M.; Freeman, R.; Lampert, C.; Diamond, J.; Kaye, W. Males with anorexia nervosa: A controlled study of eating disorders in first-degree relatives. Int. J. Eat. Disord. 2001, 29, 263–269. [Google Scholar] [CrossRef]
- Mitchell, J.E.; Crow, S. Medical complications of anorexia nervosa and bulimia nervosa. Curr. Opin. Psychiatry 2006, 19, 438–443. [Google Scholar] [CrossRef]
- Martínez-González, L.; Fernández-Villa, T.; Molina, A.J.; Delgado-Rodríguez, M.; Martín, V. Incidence of anorexia nervosa in women: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2020, 17, 3824. [Google Scholar] [CrossRef]
- Reas, D.L.; Ro, O. Time trends in healthcare-detected incidence of anorexia nervosa and bulimia nervosa in the Norwegian national patient register. Int. J. Eat. Disord. 2018, 51, 1144–1152. [Google Scholar] [CrossRef]
- Mannucci, E.; Rotella, F.; Ricca, V.; Moretti, S.; Placidi, G.F.; Rotella, C.M. Eating disorders in patients with type 1 diabetes: A meta-analysis. J. Endocrinol. Investig. 2005, 28, 417–419. [Google Scholar] [CrossRef] [PubMed]
- Bourne, L.; Bryant-Waugh, R.; Cook, J.; Mandy, W. Avoidant/restrictive food intake disorder: A systematic scoping review of the current literature. Psychiatry Res. 2020, 288, 112961. [Google Scholar] [CrossRef] [PubMed]
- Ornstein, R.M.; Essayli, J.H.; Nicely, T.A.; Masciulli, E.; Lane-Loney, S. Treatment of avoidant/restrictive food intake disorder in a cohort of young patients in a partial hospitalization program for eating disorders. Int. J. Eat. Disord. 2017, 50, 1067–1074. [Google Scholar] [CrossRef]
- Fisher, M.M.; Rosen, D.S.; Ornstein, R.M.; Mammel, K.A.; Katzman, D.K.; Rome, E.S.; Callahan, S.T.; Malizio, J.; Kearney, S.; Walsh, B.T. Characteristics of Avoidant/Restrictive Food Intake Disorder in Children and Adolescents: A “New Disorder” in DSM-5. J. Adolesc. Health 2014, 55, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Forman, S.F.; McKenzie, N.; Hehn, R.; Monge, M.C.; Kapphahn, C.J.; Mammel, K.A.; Callahan, S.T.; Sigel, E.J.; Bravender, T.; Romano, M.; et al. Predictors of outcome at 1 year in adolescents with DSM-5 restrictive eating disorders: Report of the national eating disorders quality improvement collaborative. J. Adolesc. Health 2014, 55, 750–756. [Google Scholar] [CrossRef]
- Nicely, T.A.; Lane-Loney, S.; Masciulli, E.; Hollenbeak, C.S.; Ornstein, R. Prevalence and characteristics of avoidant/restrictive food intake disorder in a cohort of young patients in day treatment for eating disorders. J. Eat. Disord. 2014, 2, 21. [Google Scholar] [CrossRef]
- Norris, M.L.; Robinson, A.; Obeid, N.; Harrison, M.; Spettigue, W.; Henderson, K. Exploring avoidant/restrictive food intake disorder in eating disordered patients: A descriptive study. Int. J. Eat. Disord. 2014, 47, 495–499. [Google Scholar] [CrossRef]
- Williams, K.E.; Hendy, H.M.; Field, D.G.; Belousov, Y.; Riegel, K.; Harclerode, W. Implications of avoidant/restrictive food intake disorder (ARFID) on children with feeding problems. Child. Health Care 2015, 44, 307–321. [Google Scholar] [CrossRef]
- Cooney, M.; Lieberman, M.; Guimond, T.; Katzman, D.K. Clinical and psychological features of children and adolescents diagnosed with avoidant/restrictive food intake disorder in a pediatric tertiary care eating disorder program: A descriptive study. J. Eat. Disord. 2018, 6, 7. [Google Scholar] [CrossRef]
- Krom, H.; van der Sluijs Veer, L.; van Zundert, S.; Otten, M.; Benninga, M.; Haverman, L.; Kindermann, A. Health related quality of life of infants and children with avoidant restrictive food intake disorder. Int. J. Eat. Disord. 2019, 52, 410–418. [Google Scholar] [CrossRef]
- Hay, P.; Mitchison, D.; Collado, A.E.L.; Gonzalez-Chica, D.A.; Stocks, N.; Touyz, S. Burden and health-related quality of life of eating disorders, including avoidant/restrictive food intake disorder (ARFID), in the Australian population. J. Eat. Disord. 2017, 5, 21. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, S.; Vieira, A.I.; Machado, B.C.; Costa, R.; Pinheiro, J.; Conceiçao, E. Avoidant/restrictive food intake disorder symptoms in children: Associations with child and family variables. Child. Health Care 2018, 48, 301–313. [Google Scholar] [CrossRef]
- Chen, Y.; Chen, W.J.; Lin, K.; Shen, L.; Gau, S.S. Prevalence of DSM-5 mental disorders in a nationally representative sample of children in Taiwan: Methodology and main findings. Epidemiol. Psychiatr. Sci. 2019, 30, E15. [Google Scholar] [CrossRef] [PubMed]
- Norris, M.L.; Spettigue, W.J.; Katzman, D.K. Update on eating disorders: Current perspectives on avoidant/restrictive food intake disorder in children and youth. Neuropsychiatr. Dis. Treat. 2016, 12, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Rzońca, E.; Bień, A.; Iwanowicz-Palus, G. Zaburzenia odżywiania-problem wciąż aktualny. J. Educ. Health Sport 2016, 6, 12. [Google Scholar]
- Osińska, A.; Mozol-Jursza, M.; Tyszkiewicz-Nwafor, M.; Słopień, A.; Paszyńska, E. Bulimia psychiczna–rozpowszechnienie, objawy i leczenie z uwzględnieniem aspektu stomatologicznego. Pediatr. I Med. Rodz. 2016, 3, 276–284. [Google Scholar] [CrossRef]
- Blake, K.; Davis, V. Medycyna okresu dorastania. In Nelson Pediatria; Marcdante, K.J., Kliegman, R.M., Jenson, H.B., Behrman, R.E., Eds.; Elsevier Urban & Partner: Wrocław, Poland, 2013; Volume 1, pp. 277–296. [Google Scholar]
- Zerwas, S.; Larsen, J.T.; Petersen, L.; Thornton, L.M.; Mortensen, P.B.; Bulik, C.M. The incidence of eating disorders in a Danish register study: Associations with suicide risk and mortality. J. Psychiatr. Res. 2015, 65, 16–22. [Google Scholar] [CrossRef]
- Hoek, H.W. Incidence, prevalence and mortality of anorexia nervosa and bulimia nervosa. Curr. Opin. Psychiatry 2021, 34, 515–524. [Google Scholar] [CrossRef]
- Himmerich, H.; Hotopf, M.; Shetty, H.; Schmidt, U.; Treasure, J.; Hayes, R.D.; Stewart, R.; Chang, C.-K. Psychiatric comorbidity as a risk factor for the mortality of people with bulimia nervosa. Soc. Psychiatry Psychiatr. Epidemiol. 2019, 54, 813–821. [Google Scholar] [CrossRef]
- Forcano, L.; Fernández-Aranda, F.; Álvarez-Moya, E.; Bulik, C.; Granero, R.; Gratacòs, M.; Jiménez-Murcia, S.; Krug, I.; Mercader, J.M.; Riesco, N.; et al. Suicide attempts in bulimia nervosa: Personality and psychopathological correlates. Eur. Psychiatry 2019, 24, 91–97. [Google Scholar] [CrossRef]
- Brown, C.A.; Mehler, P.S. Medical complications of self-induced vomiting. Eat. Disord. 2013, 21, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Herpertz, S.; Albus, C.; Lohff, S.; Michalski, K.; Masrour, M.; Lichtblau, K.; Köhle, K.; Mann, K.; Senf, W. Characteristics of diabetic patients with and without an eating disorder. Psychother. Psychosom. Med. Psychol. 2000, 50, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Vila, G.; Robert, J.-J.; Nollet-Clemencon, C.; Vera, L.; Crosnier, H.; Rault, G.; Jos, J.; Mouren-Simeoni, M.-C. Eating and emotional disorders in adolescent obese girls with insulin-dependent diabetes mellitus. Eur. Child Adolesc. Psychiatry 1995, 4, 270–279. [Google Scholar] [CrossRef] [PubMed]
- Ruth-Sahd, L.A.; Schneider, M.; Haagen, B. Diabulimia: What It Is and How to Recognize It in Critical Care. Dimens. Crit. Care Nurs. 2009, 28, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Colton, P.A.; Olmsted, M.P.; Daneman, D.; Farquhar, J.C.; Wong, H.; Muskat, S.; Rodin, G.M. Eating disorders in girls and women with type 1 diabetes: A longitudinal study of prevalence, onset, remission, and recurrence. Diabetes Care 2015, 38, 121–126. [Google Scholar] [CrossRef]
- Mather, A.A.; Cox, B.J.; Enns, M.W.; Sareen, J. Associations of obesity with psychiatric disorders and suicidal behaviors in a nationally representative sample. J. Psychosom. Res. 2009, 66, 277–285. [Google Scholar] [CrossRef]
- Bădescu, S.; Tătaru, C.; Kobylinska, L.; Georgescu, E.; Zahiu, D.; Zăgrean, A.; Zăgrean, L. The association between Diabetes mellitus and Depression. J. Med. Life 2016, 9, 120–125. [Google Scholar]
- Kessler, R.C.; Berglund, P.A.; Chiu, W.T.; Deitz, A.C.; Hudson, J.I.; Shahly, V.; Aguilar-Gaxiola, S.; Alonso, J.; Angermeyer, M.C.; Benjet, C.; et al. The Prevalence and Correlates of Binge Eating Disorder in the World Health Organization World Mental Health Surveys. Biol. Psychiatry 2013, 73, 904–914. [Google Scholar] [CrossRef]
- Giel, K.E.; Bulik, C.M.; Fernandez-Aranda, F.; Hay, P.; Keski-Rahkonen, A.; Schag, K.; Schmidt, U.; Zipfel, S. Binge eating disorder. Nat. Rev. Dis. Primers 2022, 8, 16. [Google Scholar] [CrossRef]
- Hilbert, A. Binge-eating disorder. Psychiatr. Clin. 2019, 42, 33–43. [Google Scholar] [CrossRef]
- García-Mayor, R.V.; García-Soidán, F.J. Eating disorders in type 2 diabetic people: Brief review. Diabetes Metab. Syndr. 2017, 11, 221–224. [Google Scholar] [CrossRef] [PubMed]
- Papelbaum, M.; Appolinário, J.C.; Moreira Rde, O.; Ellinger, V.C.; Kupfer, R.; Coutinho, W.F. Prevalence of eating disorders and psychiatric comorbidity in a clinical sample of type 2 diabetes mellitus patients. Braz. J. Psychiatry 2005, 27, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Herpertz, S.; Albus, C.; Wagener, R.; Kocnar, M.; Wagner, R.; Henning, A.; Best, F.; Foerster, H.; Schleppinghoff, B.S.; Thomas, W.; et al. Comorbidity of diabetes and eating disorders. Does diabetes control reflect disturbed eating behavior? Diabetes Care 1998, 21, 1110–1116. [Google Scholar] [CrossRef] [PubMed]
- Abbott, S.; Dindol, N.; Tahrani, A.A.; Piya, M.K. Binge eating disorder and night eating syndrome in adults with type 2 diabetes: A systematic review. J. Eat. Disord. 2018, 6, 36. [Google Scholar] [CrossRef] [PubMed]
- Raevuori, A.; Suokas, J.; Haukka, J.; Gissler, M.; Linna, M.; Grainger, M.; Suvisaari, J. Highly increased risk of type 2 diabetes in patients with binge eating disorder and bulimia nervosa. Int. J. Eat. Disord. 2015, 48, 555–562. [Google Scholar] [CrossRef]
- Dingemans, A.E.; Bruna, M.J.; van Furth, E.F. Binge eating disorder: A review. Int. J. Obes. 2002, 26, 299–307. [Google Scholar] [CrossRef]
- Winston, A.P. The clinical biochemistry of anorexia nervosa. Ann. Clin. Biochem. 2012, 49 Pt 2, 132–143. [Google Scholar] [CrossRef]
- Nielsen, S.; Emborg, C.; Mølbak, A.G. Mortality in Concurrent Type 1 Diabetes and Anorexia Nervosa. Diabetes Care 2002, 25, 309–312. [Google Scholar] [CrossRef]
- Stunkard, A.; Grace, W.; Wolff, H. The night-eating syndrome: A pattern of food intake among certain obese patients. Am. J. Med. 1955, 19, 78–86. [Google Scholar] [CrossRef]
- Gallant, A.R.; Lundgren, J.; Drapeau, V. The night-eating syndrome and obesity. Obes. Rev. 2012, 13, 528–536. [Google Scholar] [CrossRef]
- Night Eating Syndrome (NES). Available online: https://my.clevelandclinic.org/health/diseases/21731-night-eating-syndrome-nes (accessed on 6 August 2023).
- Varga, M.; Dukay-Szabó, S.; Túry, F.; van Furth Eric, F. Evidence and gaps in the literature on orthorexia nervosa. Eat. Weight Disord. -Stud. Anorex. Bulim. Obes. 2013, 18, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Hanganu-Bresch, C. Orthorexia: Eating right in the context of healthism. Med. Humanit. 2020, 46, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Uzdil, Z.; Kayacan, A.G.; Özyildirim, C.; Seda, K.; Kilinç, G.E.; Canan, A.; Kaya, P.S. Adölesanlarda Ortoreksiya Nervoza Varlığı ve Yeme Tutumunun İncelenmesi. Samsun Sağlık Bilim. Derg. 2019, 4, 8–13. [Google Scholar]
- Bratman, S.; Knight, D. Health Food Junkies: Orthorexia Nervosa: Overcoming the Obsession with Healthful Eating; Harmony: New York, NY, USA, 2004. [Google Scholar]
- Donini, L.M.; Marsili, D.; Graziani, M.P.; Imbriale, M.; Cannella, C. Orthorexia nervosa: A preliminary study with a proposal for diagnosis and an attempt to measure the dimension of the phenomenon. Eat. Weight Disord. -Stud. Anorex. Bulim. Obes. 2004, 9, 151–157. [Google Scholar] [CrossRef]
- Oberle, C.D.; Klare, D.L.; Patyk, K.C. Health beliefs, behaviors, and symptoms associated with orthorexia nervosa. Eat. Weight Disord. Stud. Anorexia. Bulim. Obes. 2019, 24, 495–506. [Google Scholar] [CrossRef]
- Koven, N.S.; Abry, A.W. The clinical basis of orthorexia nervosa: Emerging perspectives. Neuropsychiatr. Dis. Treat. 2015, 11, 385–394. [Google Scholar] [CrossRef]
- Altun, H.K.; Özyildirim, C.; Koç, Ş.; Aksoy, H.N.; Sağir, B.; Bozkurt, M.S.; Karasu, H. The factors associated with orthorexia nervosa in type 2 diabetes and their effect on diabetes self-management scores. Eat. Weight Disord. 2023, 28, 22. [Google Scholar] [CrossRef]
- Tunçere, E.; Bayindirgümüş, A. The Importance of Pregorexia Awareness. Clin. Exp. Health Sci. 2020, 10, 186–190. [Google Scholar]
- Wójciak, R.W.; Mojs, E.; Michalska, M.M.; Samulak, D. Podejmowanie odchudzania w okresie ciąży a poporodowe surowicze stężenia żelaza u kobiet–badanie wstępne. Probl. Hig. Epidemiol. 2013, 94, 893–896. [Google Scholar]
- Micali, N. Eating disorders and pregnancy. Psychiatry 2008, 7, 191–193. [Google Scholar] [CrossRef]
- Bee, H.; Boyd, D. The Developing Child, 10th ed.; Pearson Education Australia: Frenchs Forest, Australia, 2004. [Google Scholar]
- Eik-Nes, T.T.; Horn, J.; Strohmaier, S.; Holmen, T.L.; Micali, N.; Bjornelv, S. Impact of eating disorders on obstetric outcomes in a large clinical sample: A comparison with the HUNT study. Int. J. Eat. Disord. 2018, 51, 1134–1143. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association Professional Practice Committee. 3. Prevention or Delay of Type 2 Diabetes and Associated Comorbidities: Standards of Medical Care in Diabetes—2022. Diabetes Care 2022, 45, S39–S45. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association Professional Practice Committee. 8. Obesity and Weight Management for the Prevention and Treatment of Type 2 Diabetes: Standards of Medical Care in Diabetes–2022. Diabetes Care 2022, 45, S113–S124. [Google Scholar] [CrossRef] [PubMed]
- Wittert, G.; Bracken, K.; Robledo, K.P.; Grossmann, M.; Yeap, B.B.; Handelsman, D.J.; Stuckey, B.; Conway, A.; Inder, W.; McLachlan, R.; et al. Testosterone treatment to prevent or revert type 2 diabetes in men enrolled in a lifestyle programme (T4DM): A randomised, double-blind, placebo-controlled, 2-year, phase 3b trial. Lancet Diabetes Endocrinol. 2021, 9, 32–45. [Google Scholar] [CrossRef]
- Domecq, J.P.; Prutsky, G.; Leppin, A.; Sonbol, M.B.; Altayar, O.; Undavalli, C.; Wang, Z.; Elraiyah, T.; Brito, J.P.; Mauck, K.F.; et al. Clinical review: Drugs commonly associated with weight change: A systematic review and meta-analysis. J. Clin. Endocrinol. Metab. 2015, 100, 363–370. [Google Scholar] [CrossRef]
- Larrañaga, A.; Fluiters, E.; Docet, M.; Fernández Sastre, J.L.; García-Mayor, R.V. Comparative study of cognitive-behavioural psychotherapy and nutritional support in patients with different types of eating disorders. Med. Clin. 2014, 143, 196–200. [Google Scholar] [CrossRef]
- Coleman, S.E.; Caswell, N. Diabetes and eating disorders: An exploration of ‘Diabulimia’. BMC Psychol. 2020, 8, 101. [Google Scholar] [CrossRef]
- Kernardy, J.; Mensch, M.; Bowen, K.; Green, B.; Watson, J. Group therapy for binge eating in type 2 diabetes: A randomized trial. Diabet. Med. 2002, 19, 234–239. [Google Scholar] [CrossRef]
- Lehman, R.; Krumholz, H.M. Tight control of blood glucose in long standing type 2 diabetes. BMJ 2009, 338, 800–801. [Google Scholar] [CrossRef]
- Clery, P.; Stahl, D.; Ismail, K.; Treasure, J.; Kan, C. Systematic review and meta-analysis of the efficacy of interventions for people with Type 1 diabetes mellitus and disordered eating. Diabet. Med. 2017, 34, 1667–1675. [Google Scholar] [CrossRef]
- Nielsen, S. Eating disorders in females with type 1 diabetes: An update of a metaanalysis. Eur. Eat. Disord. Rev. 2002, 10, 241–254. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Signs of Disordered Eating in Diabetes |
|---|
| Preoccupation with Food —Constant thoughts about food, calories, and weight |
| Strict Meal Plans —Following excessively rigid eating patterns and meal plans |
| Fear of High Blood Sugar —Extreme anxiety or fear of elevated blood sugar levels and their consequences |
| Distorted Body Image —Negative perception of body shape or size, even when it may not align with reality |
| Unhealthy Weight Control Behaviors —Engaging in extreme weight control methods, such as skipping meals or purging |
| Withdrawing from social eating activities —Knowingly or intentionally removing oneself from social gatherings or events that involve eating |
| Insulin Manipulation —Intentional omission or underdosing of insulin to manipulate weight or blood sugar levels |
| Excessive Exercise —Compulsive or excessive exercise routines as a means of compensating for food intake or controlling weight |
| Mood Swings or Emotional Distress —Frequent mood changes, anxiety, depression, or irritability related to food, body image, or diabetes management |
| Types of Eating Disorders in Individuals with Diabetes |
|---|
| 1. Severe Dietary Restriction —Severe limitation of calories or essential macronutrients in the diet |
| 2. Objective Binge Eating —Consuming an unusually large amount of food in a short period while feeling out of control |
| 3. Subjective Binge Eating —Feeling a loss of control over eating without necessarily consuming large quantities of food |
| 4. Other Maladaptive Weight Control Strategies —Restricting life-saving insulin |
| Eating Disorders |
|---|
Anorexia Nervosa (AN)
|
Avoidant/Restrictive Food Intake Disorder (ARFID)
|
Bulimia Nervosa (BN)
|
Binge-Eating Disorder (BED)
|
Diabulimia
|
| Diagnosed Duration | Symptoms |
|---|---|
| Short term |
|
| Medium-term |
|
| Long term |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dziewa, M.; Bańka, B.; Herbet, M.; Piątkowska-Chmiel, I. Eating Disorders and Diabetes: Facing the Dual Challenge. Nutrients 2023, 15, 3955. https://doi.org/10.3390/nu15183955
Dziewa M, Bańka B, Herbet M, Piątkowska-Chmiel I. Eating Disorders and Diabetes: Facing the Dual Challenge. Nutrients. 2023; 15(18):3955. https://doi.org/10.3390/nu15183955
Chicago/Turabian StyleDziewa, Magdalena, Bartosz Bańka, Mariola Herbet, and Iwona Piątkowska-Chmiel. 2023. "Eating Disorders and Diabetes: Facing the Dual Challenge" Nutrients 15, no. 18: 3955. https://doi.org/10.3390/nu15183955
APA StyleDziewa, M., Bańka, B., Herbet, M., & Piątkowska-Chmiel, I. (2023). Eating Disorders and Diabetes: Facing the Dual Challenge. Nutrients, 15(18), 3955. https://doi.org/10.3390/nu15183955