
Follow-Up of Celiac Disease in Adults: “When, What, Who, and Where”
 ,
,  , , and
, , and
Abstract
1. Introduction
2. Follow-Up
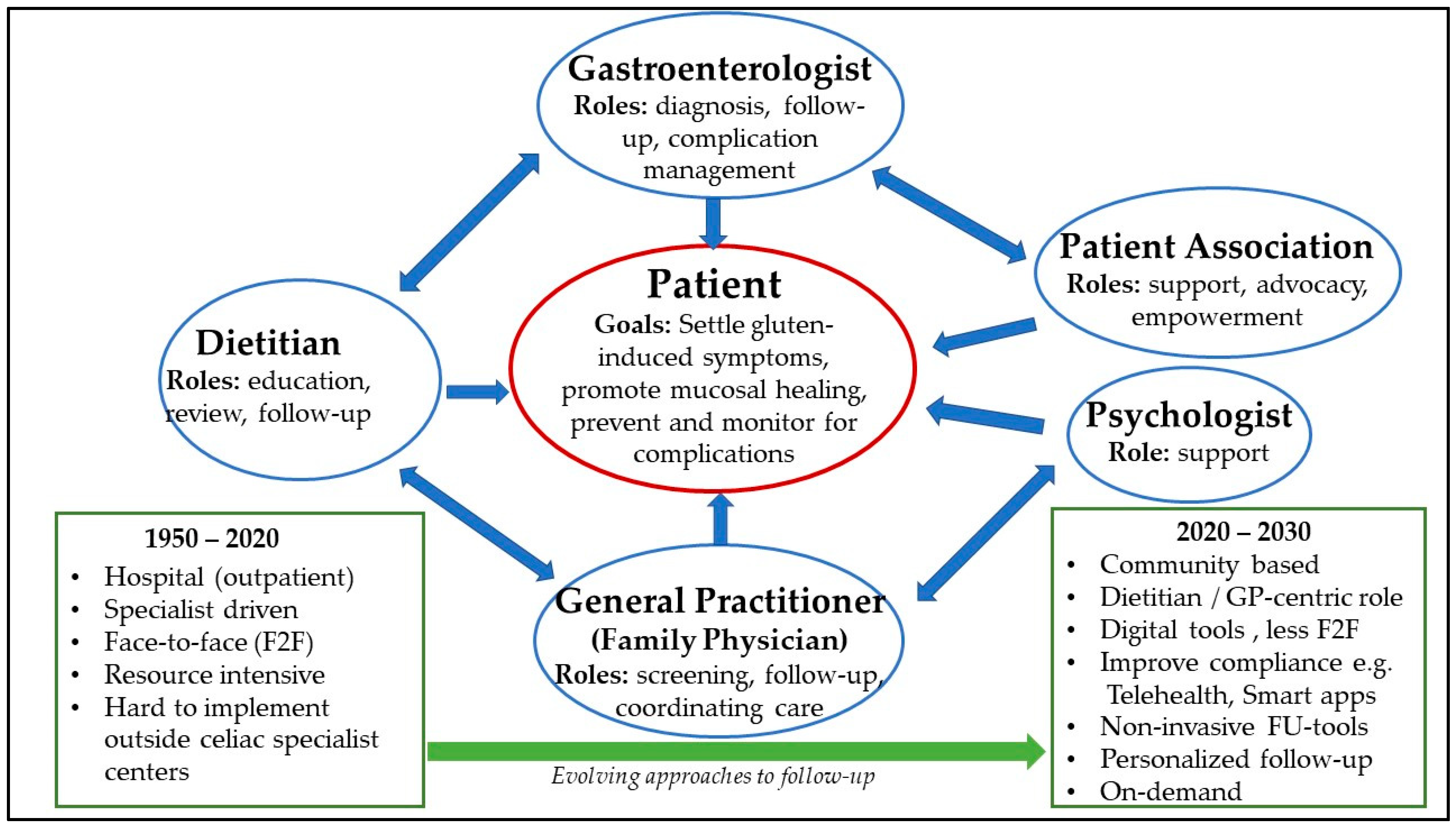
- a gastroenterologist for diagnosis and medical care;
- a registered celiac dietitian for a supervised gluten-free diet plan and for follow-ups;
- access to a social worker to help with the implementation of the diet at work, school, and in families;
- access to a clinical psychologist for support services.
2.1. Disease Monitoring (When, What, and Who?)
- Recognition of “slow responders”, which are CeD patients who still report symptoms six months to a year after initiation of a GFD. This is a common occurrence, and while some consider these patients to be “non-responsive‘’, a cause can usually be identified when a systematic approach to follow-up is undertaken. The most common cause is an ongoing gluten intake, albeit unintentional.
- Increased awareness of neurological symptoms that are related to gluten, including gluten ataxia, peripheral neuropathy, foggy mind, anxiety, and depression [32].
- Consultation is needed with a dermatologist when there is a suspicion of dermatitis herpetiformis (DH), the skin manifestation of CeD [33].
- Monitoring of people with CeD should include verification of the normalization of laboratory abnormalities detected during the initial laboratory investigation. Upper gastrointestinal (GI) endoscopy with duodenal biopsies is recommended for monitoring in cases with a lack of clinical response or relapse of symptoms despite a GFD [29,30,34].
- Metabolic syndrome and fatty liver disease should be monitored in CeD patients [35]. Abnormal liver function tests are a common finding in CeD, with the strongest association reported at presentation or diagnosis. CeD hepatitis is manifested by mild hypertransaminasemia (three to five times the upper limit of normal) and is due to a gluten-dependent liver injury that settles on a GFD [36,37]. Autoimmune liver diseases such as autoimmune hepatitis, primary biliary cholangitis, and primary sclerosing cholangitis are also more common in celiac disease. An increasingly reported complication is that of non-alcoholic fatty liver disease, which can occur as part of metabolic syndrome after starting the GFD. Long-term GFD has been associated with metabolic dysregulation and cardiovascular complications. Patients with metabolic dysfunction-associated fatty liver disease need strict counseling regarding increasing physical activity and optimizing their diet to reduce caloric intake, enrich unprocessed, naturally gluten-free foods, and minimize highly refined carbohydrates and saturated fat [38,39,40].
- The timing of bone density studies should follow a CeD-specific schedule with a defined age to start DXA screening [29]. It is important because osteopenia and, less frequently, osteoporosis are common in CeD. This applies for both females and males.
- Associated auto-immune conditions (in particular hypothyroidism) need to be checked regularly [28].
- Some CeD patients, especially young adults at diagnosis, have an increasing need for psychosocial counseling [41].
- CeD is associated with an increased risk of pneumococcal sepsis and mortality, and, therefore, pneumococcal vaccination is recommended, although practices differ widely. Some guidelines (ACG) recommend this vaccine for all adults with CeD [30], but, in some centers, it is given arbitrarily to all CeD patients with smaller spleens (125 cc) or beginning at the age of 70 years [42]. More generally, vaccination schedules for various infectious agents should be clarified for people with CeD.
- Tissue transglutaminase antibodies (IgA anti-TG2) have been shown in published studies to be insufficient for predicting relapse; other biomarkers are required, similar to the impact of fecal calprotectin measurement in the care of IBD patients [43].
- Proper data are still lacking on long-term outcomes in follow-up disease activity scores, such as the frequency of outpatient visits, histological follow-up, and cost effectiveness. CeD guidelines suggest that a full assessment of disease activity, such as antibodies and investigating for deficiency of essential elements, needs to be performed before starting GFD and after an adequate period, e.g., 12–24 months, to assess reversal or improvement in the manifestations of CeD [29,30].
- Specific attention to the possibility of refractory CeD (RCD); making the distinction between RCD type I and type II; and closely monitoring the nutritional status of both types. Clinicians require a “Red Flags” index for the diagnosis of refractory CeD, which carries a higher risk of developing lymphoproliferative malignancies [1,44]. A simple “Red Flags” index, using early signs and symptoms for family members and high-risk patients for developing CeD, might be useful. Specialist care of refractory CeD is important, and expediting review by an appropriate specialist may be aided by such a tool. It is recommended that patients with RCD II should be referred to secondary celiac centers with RCD-experienced gastroenterologists, immunologists, and hematologists [29].
2.2. Assessment of Dietary Adherence during the Follow-Up
2.3. Nutritional Education
2.4. Indications for Follow-Up Small Bowel Biopsy after GFD
2.5. Screening for Celiac Disease in Family Members
2.6. Interdisciplinary Team Membership
2.7. Celiac Disease Center and Coordinated Care Models
2.8. Celiac Disease Patient Registries
3. The Setting of Clinics
3.1. Face-to-Face
3.2. Virtual Clinics and Dietitians in the Lead
3.3. General Practitioners’ Key Roles in the Future
3.4. Patient Preferences
4. Gluten-Free Food in Outpatient Clinics and during Admission to Hospitals
5. Conclusions
Key Points
- ○
- Follow-ups of patients with CeD are important and include ensuring symptom resolution, optimization of nutrition and weight, normalization of serology, nutrient levels and bone density, preventive care, and minimization of long-term morbidity.
- ○
- Dieticians as well as psychosocial professionals should be an integral part of the multi-disciplinary follow-up team.
- ○
- CeD patient follow-ups are inconsistent and variable, and more studies are needed to inform on the best approach.
- ○
- An important surrogate endpoint of progress on a GFD is small bowel mucosal healing.
- ○
- There is a requirement for a “Red Flags” index for the diagnosis of refractory CeD, which carries a higher risk of developing lymphoproliferative malignancies.
- ○
- RCD II should be referred to secondary CeD centers with RCD-experienced gastroenterologists, immunologists, and hematologists.
- ○
- GPs will be a solution if the critical number of diagnosed celiacs in a local population is high enough.
- ○
- There is a need for models of care for CeD patients that facilitate effective follow-up and utilize health care resources in an efficient manner; the use of technologies such as video calls and smart phone apps carry a lot of appeal, but more research is needed.
- ○
- A CeD-Monitoring Index (consisting solely of patient-reported outcomes) might reduce time to recovery, increase GFD adherence, and reduce the number of F2F-outpatient visits.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mulder, C.J.; Wierdsma, N.J.; Berkenpas, M.; Jacobs, M.A.J.M.; Bouma, G. Preventing complications in celiac disease: Our experience with managing adult celiac disease. Best Pract. Res. Clin. Gastroenterol. 2015, 29, 459–468. [Google Scholar] [CrossRef]
- Dubé, C.; Rostom, A.; Sy, R.; Cranney, A.; Saloojee, N.; Garritty, C.; Sampson, M.; Zhang, L.; Yazdi, F.; Mamaladze, V.; et al. The prevalence of celiac disease in average-risk and at-risk Western European populations: A systematic review. Gastroenterology 2005, 128 (4 Suppl. S1), S57–S67. [Google Scholar] [CrossRef]
- Di Sabatino, A.; Corazza, G.R. Coeliac disease. Lancet 2009, 373, 1480–1493. [Google Scholar] [CrossRef]
- Herman, M.L.; Rubio-Tapia, A.; Lahr, B.D.; Larson, J.J.; Van Dyke, C.T.; Murray, J.A. Patients with celiac disease are not followed up adequately. Clin. Gastroenterol. Hepatol. 2012, 10, 893–899.e1. [Google Scholar] [CrossRef]
- Cohen, M.E.; Jaffe, A.; Strauch, C.B.; Lewis, S.K.; Lebwohl, B.; Green, P.H.R. Determinants of Follow-up Care for Patients With Celiac Disease. J. Clin. Gastroenterol. 2018, 52, 784–788. [Google Scholar] [CrossRef]
- Wessels, M.; Dolinsek, J.; Castillejo, G.; Donat, E.; Riznik, P.; Roca, M.; Valitutti, F.; Veenvliet, A.; Mearin, M.L. Follow-up practices for children and adolescents with celiac disease: Results of an international survey. Eur. J. Pediatr. 2022, 181, 1213–1220. [Google Scholar] [CrossRef]
- Hughey, J.J.; Ray, B.K.; Lee, A.R.; Voorhees, K.N.; Kelly, C.P.; Schuppan, D. Self-reported dietary adherence, disease-specific symptoms, and quality of life are associated with healthcare provider follow-up in celiac disease. BMC Gastroenterol. 2017, 17, 156. [Google Scholar] [CrossRef]
- Kivelä, L.; Hekkala, S.; Huhtala, H.; Kaukinen, K.; Kurppa, K. Lack of long-term follow-up after paediatric-adult transition in coeliac disease is not associated with complications, ongoing symptoms or dietary adherence. United Eur. Gastroenterol. J. 2020, 8, 157–166. [Google Scholar] [CrossRef]
- Raiteri, A.; Granito, A.; Giamperoli, A.; Catenaro, T.; Negrini, G.; Tovoli, F. Current guidelines for the management of celiac disease: A systematic review with comparative analysis. World J. Gastroenterol. 2022, 28, 154. [Google Scholar] [CrossRef]
- Khurana, A.; Leffler, D.A.; Gomez, K.; Thukral, C. Short and long-term follow-up and clinical outcomes in patients with celiac disease in a large private practice setting. BMC Gastroenterol. 2023, 23, 9. [Google Scholar] [CrossRef]
- Tye-Din, J.A. Review article: Follow-up of coeliac disease. Aliment. Pharmacol. Ther. 2022, 56 (Suppl. S1), S49–S63. [Google Scholar] [CrossRef]
- Pinto-Sanchez, M.I.; Bai, J.C. Toward New Paradigms in the Follow Up of Adult Patients With Celiac Disease on a Gluten-Free Diet. Front. Nutr. 2019, 6, 153. [Google Scholar] [CrossRef]
- van Megen, F.; Skodje, G.I.; Stendahl, M.; Veierød, M.B.; Lundin, K.E.A.; Henriksen, C. High disease burden in treated celiac patients—A web-based survey. Scand. J. Gastroenterol. 2021, 56, 882–888. [Google Scholar] [CrossRef]
- Pritchard, L.; Waters, C.; Murray, I.A.; Bebb, J.; Lewis, S. Comparing alternative follow-up strategies for patients with stable coeliac disease. Frontline Gastroenterol. 2019, 11, 93–97. [Google Scholar] [CrossRef]
- Lexner, J.; Hjortswang, H.; Ekesbo, R.; Sjöberg, K. Well-being and dietary adherence in patients with coeliac disease depending on follow-up. Scand. J. Gastroenterol. 2021, 56, 382–390. [Google Scholar] [CrossRef]
- Rubio-Tapia, A.; Rahim, M.W.; See, J.A.; Lahr, B.D.; Wu, T.-T.; Murray, J.A. Mucosal recovery and mortality in adults with celiac disease after treatment with a gluten-free diet. Am. J. Gastroenterol. 2010, 105, 1412–1420. [Google Scholar] [CrossRef]
- Viljamaa, M.; Kaukinen, K.; Pukkala, E.; Hervonen, K.; Reunala, T.; Collin, P. Malignancies and mortality in patients with coeliac disease and dermatitis herpetiformis: 30-year population-based study. Dig. Liver Dis. 2006, 38, 374–380. [Google Scholar] [CrossRef]
- Lebwohl, B.; Green, P.H.R.; Emilsson, L.; Mårild, K.; Söderling, J.; Roelstraete, B.; Ludvigsson, J.F. Cancer Risk in 47,241 Individuals with Celiac Disease: A Nationwide Cohort Study. Clin. Gastroenterol. Hepatol. 2022, 20, e111–e131. [Google Scholar] [CrossRef]
- Lebwohl, B.; Green, P.H.R.; Söderling, J.; Roelstraete, B.; Ludvigsson, J.F. Association between Celiac Disease and Mortality Risk in a Swedish Population. JAMA—J. Am. Med. Assoc. 2020, 323, 1277–1285. [Google Scholar] [CrossRef]
- Banti, T.; Fievet, L.; Fabre, A. Gluten: Is the information available on the Internet valid? Arch. Pediatr. 2017, 24, 977–985. [Google Scholar] [CrossRef]
- Rej, A.; Tai, F.W.D.; Green, P.H.R.; Lebwohl, B.; Sanders, D.S. The growing global interest in the gluten free diet as reflected by Google searches. Dig. Liver Dis. 2020, 52, 1061–1062. [Google Scholar] [CrossRef] [PubMed]
- Rostami, K.; Kerckhaert, J.; Tiemessen, R.; von Blomberg, B.M.; Meijer, J.W.; Mulder, C.J. Sensitivity of antiendomysium and antigliadin antibodies in untreated celiac disease: Disappointing in clinical practice. Am. J. Gastroenterol. 1999, 94, 888–894. [Google Scholar] [CrossRef] [PubMed]
- Marsh, M.N. Gluten, major histocompatibility complex, and the small intestine. A molecular and immunobiologic approach to the spectrum of gluten sensitivity (‘celiac sprue’). Gastroenterology 1992, 102, 330–354. Available online: http://www.ncbi.nlm.nih.gov/pubmed/1727768 (accessed on 1 March 2019). [CrossRef] [PubMed]
- Harder, G.; Schiepatti, A.; Biagi, F.; Borrelli de Andreis, F.; Agazzi, S.; Gabrielli, G.M.; Klersy, C. Optimising the follow-up of adult coeliac disease with a clinical-based score to identify patients in need of a histological reassessment: A retrospective single centre study. Br. J. Nutr. 2020, 123, 1159–1164. [Google Scholar] [CrossRef] [PubMed]
- Bebb, J.R.; Lawson, A.; Knight, T.; Long, R.G. Long-term follow-up of coeliac disease--what do coeliac patients want? Aliment. Pharmacol. Ther. 2006, 23, 827–831. [Google Scholar] [CrossRef] [PubMed]
- Siniscalchi, M.; Zingone, F.; Savarino, E.V.; D’Odorico, A.; Ciacci, C. COVID-19 pandemic perception in adults with celiac disease: An impulse to implement the use of telemedicine. Dig. Liver Dis. 2020, 52, 1071–1075. [Google Scholar] [CrossRef]
- Isaac, D.M.; Wu, J.; Mager, D.R.; Turner, J.M. Managing the pediatric patient with celiac disease: A multidisciplinary approach. J. Multidiscip. Healthc. 2016, 9, 529–536. [Google Scholar] [CrossRef]
- Meize-Grochowski, R. Celiac disease: A multisystem autoimmune disorder. Gastroenterol. Nurs. 2005, 28, 394–402. [Google Scholar] [CrossRef]
- Al-Toma, A.; Volta, U.; Auricchio, R.; Castillejo, G.; Sanders, D.S.; Cellier, C.; Mulder, C.J.; Lundin, K.E.A. European Society for the Study of Coeliac Disease (ESsCD) guideline for coeliac disease and other gluten-related disorders. United Eur. Gastroenterol. J. 2019, 7, 583–613. [Google Scholar] [CrossRef]
- Rubio-Tapia, A.; Hill, I.D.; Semrad, C.; Kelly, C.P.; Lebwohl, B. American College of Gastroenterology Guidelines Update: Diagnosis and Management of Celiac Disease. Am. J. Gastroenterol. 2023, 118, 59–76. [Google Scholar] [CrossRef]
- Bakker, S.F.; Tushuizen, M.E.; Von Blomberg, B.M.E.; Bontkes, H.J.; Mulder, C.J.; Simsek, S. Screening for coeliac disease in adult patients with type 1 diabetes mellitus: Myths, facts and controversy. Diabetol. Metab. Syndr. 2016, 8, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Mearns, E.S.; Taylor, A.; Thomas Craig, K.J.; Puglielli, S.; Leffler, D.A.; Sanders, D.S.; Lebwohl, B.; Hadjivassiliou, M. Neurological Manifestations of Neuropathy and Ataxia in Celiac Disease: A Systematic Review. Nutrients 2019, 11, 380. [Google Scholar] [CrossRef] [PubMed]
- Collin, P.; Salmi, T.T.; Hervonen, K.; Kaukinen, K.; Reunala, T. Dermatitis herpetiformis: A cutaneous manifestation of coeliac disease. Ann. Med. 2017, 49, 23–31. [Google Scholar] [CrossRef]
- Zingone, F.; Maimaris, S.; Auricchio, R.; Caio, G.P.I.; Carroccio, A.; Elli, L.; Galliani, E.; Montagnani, M.; Valiante, F.; Biagi, F. Guidelines of the Italian societies of gastroenterology on the diagnosis and management of coeliac disease and dermatitis herpetiformis. Dig. Liver Dis. 2022, 54, 1304–1319. [Google Scholar] [CrossRef] [PubMed]
- Sainsbury, A.; Sanders, D.S.; Ford, A.C. Meta-analysis: Coeliac disease and hypertransaminasaemia. Aliment. Pharmacol. Ther. 2011, 34, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Regev, A.; Ben-Tov, A.; Yerushalmy-Feler, A.; Weintraub, Y.; Moran-Lev, H.; Cohen, S.; Amir, A.Z. Elevated liver enzymes of newly diagnosed pediatric celiac patients—A prospective-observational study. Eur. J. Pediatr. 2022, 181, 753–762. [Google Scholar] [CrossRef]
- Garrido, I.; Liberal, R.; Peixoto, A.; Macedo, G. Long-term follow-up and prognosis of celiac hepatitis. Eur. J. Gastroenterol. Hepatol. 2022, 34, 1255–1260. [Google Scholar] [CrossRef] [PubMed]
- Tortora, R.; Capone, P.; De Stefano, G.; Imperatore, N.; Gerbino, N.; Donetto, S.; Monaco, V.; Caporaso, N.; Rispo, A. Metabolic Syndrome in Patients with Coeliac Disease on a Gluten-Free Diet. Aliment. Pharmacol. Ther. 2015, 41, 352–359. [Google Scholar] [CrossRef]
- Ciccone, A.; Gabrieli, D.; Cardinale, R.; Di Ruscio, M.; Vernia, F.; Stefanelli, G.; Necozione, S.; Melideo, D.; Viscido, A.; Frieri, G.; et al. Metabolic Alterations in Celiac Disease Occurring after Following a Gluten-Free Diet. Digestion 2019, 4, 262–268. [Google Scholar] [CrossRef]
- García-Manzanares, A.; Lucendo, A.J.; González-Castillo, S.; Moreno-Fernández, J.; García-Manzanares, Á. Resolution of metabolic syndrome after following a gluten free diet in an adult woman diagnosed with celiac disease. World J. Gastrointest. Pathophysiol. 2011, 2, 49–52. [Google Scholar] [CrossRef]
- Ho, W.H.J.; Atkinson, E.L.; David, A.L. Examining the Psychosocial Well-Being of Children and Adolescents with Coeliac Disease: A Systematic Review. J. Pediatr. Gastroenterol. Nutr. 2023, 76, E1–E14. [Google Scholar] [CrossRef]
- van Gils, T.; Nijeboer, P.; van Waesberghe, J.H.T.; Coupé, V.M.; Janssen, K.; Zegers, J.A.; Nurmohamed, S.A.; Kraal, G.; Jiskoot, S.C.; Bouma, G.; et al. Splenic volume differentiates complicated and non-complicated celiac disease. United Eur. Gastroenterol. J. 2017, 5, 374–379. [Google Scholar] [CrossRef] [PubMed]
- Lamb, C.A.; Kennedy, N.A.; Raine, T.; Hendy, P.A.; Smith, P.J.; Limdi, J.K.; Hayee, B.; Lomer, M.C.E.; Parkes, G.C.; Selinger, C.; et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut 2019, 68 (Suppl. S3), S1–S106. [Google Scholar] [CrossRef] [PubMed]
- Wierdsma, N.J.; Nijeboer, P.; de van der Schueren, M.A.E.; Berkenpas, M.; van Bodegraven, A.A.; Mulder, C.J.J. Refractory celiac disease and EATL patients show severe malnutrition and malabsorption at diagnosis. Clin. Nutr. 2016, 35, 685–691. [Google Scholar] [CrossRef] [PubMed]
- Rostami, K.; Bold, J.; Parr, A.; Johnson, M.W. Gluten-Free Diet Indications, Safety, Quality, Labels, and Challenges. Nutrients 2017, 9, 846. [Google Scholar] [CrossRef]
- Ciacci, C.; Cirillo, M.; Cavallaro, R.; Mazzacca, G. Long-term follow-up of celiac adults on gluten-free diet: Prevalence and correlates of intestinal damage. Digestion 2002, 66, 178–185. [Google Scholar] [CrossRef]
- Husby, S.; Murray, J.A.; Katzka, D.A. AGA Clinical Practice Update on Diagnosis and Monitoring of Celiac Disease-Changing Utility of Serology and Histologic Measures: Expert Review. Gastroenterology 2019, 156, 885–889. [Google Scholar] [CrossRef]
- Mehta, P.; Pan, Z.; Riley, M.D.; Liu, E. Adherence to a Gluten-free Diet: Assessment by Dietician Interview and Serology. J. Pediatr. Gastroenterol. Nutr. 2018, 66, e67–e70. [Google Scholar] [CrossRef]
- Silvester, J.A.; Kurada, S.; Szwajcer, A.; Kelly, C.P.; Leffler, D.A.; Duerksen, D.R. Tests for Serum Transglutaminase and Endomysial Antibodies Do Not Detect Most Patients with Celiac Disease and Persistent Villous Atrophy on Gluten-free Diets: A Meta-analysis. Gastroenterology 2017, 153, 689–701.e1. [Google Scholar] [CrossRef]
- Gerasimidis, K.; Zafeiropoulou, K.; Mackinder, M.; Ijaz, U.Z.; Duncan, H.; Buchanan, E.; Cardigan, T.; Edwards, C.A.; McGrogan, P.; Russell, R.K. Comparison of Clinical Methods With the Faecal Gluten Immunogenic Peptide to Assess Gluten Intake in Coeliac Disease. J. Pediatr. Gastroenterol. Nutr. 2018, 67, 356–360. [Google Scholar] [CrossRef]
- Adriaanse, M.P.; Tack, G.J.; Passos, V.L.; Damoiseaux, J.G.; Schreurs, M.W.; van Wijck, K.; Riedl, R.G.; Masclee, A.A.; Buurman, W.A.; Mulder, C.J.; et al. Serum I-FABP as marker for enterocyte damage in coeliac disease and its relation to villous atrophy and circulating autoantibodies. Aliment. Pharmacol. Ther. 2013, 37, 482–490. [Google Scholar] [CrossRef] [PubMed]
- Biagi, F.; Andrealli, A.; Bianchi, P.I.; Marchese, A.; Klersy, C.; Corazza, G.R. A gluten-free diet score to evaluate dietary compliance in patients with coeliac disease. Br. J. Nutr. 2009, 102, 882–887. [Google Scholar] [CrossRef] [PubMed]
- Leffler, D.A.; Edwards George, J.B.; Dennis, M.; Cook, E.F.; Schuppan, D.; Kelly, C.P. A prospective comparative study of five measures of gluten-free diet adherence in adults with coeliac disease. Aliment. Pharmacol. Ther. 2007, 26, 1227–1235. [Google Scholar] [CrossRef] [PubMed]
- Leffler, D.A.; Dennis, M.; Edwards George, J.B.; Jamma, S.; Magge, S.; Cook, E.F.; Schuppan, D.; Kelly, C.P. A simple validated gluten-free diet adherence survey for adults with celiac disease. Clin. Gastroenterol. Hepatol. 2009, 7, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Villafuerte-Galvez, J.; Vanga, R.R.; Dennis, M.; Hansen, J.; Leffler, D.A.; Kelly, C.P.; Mukherjee, R. Factors governing long-term adherence to a gluten-free diet in adult patients with coeliac disease. Aliment. Pharmacol. Ther. 2015, 42, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Hall, N.J.; Rubin, G.; Charnock, A. Systematic review: Adherence to a gluten-free diet in adult patients with coeliac disease. Aliment. Pharmacol. Ther. 2009, 30, 315–330. [Google Scholar] [CrossRef] [PubMed]
- Ford, S.; Howard, R.; Oyebode, J. Psychosocial aspects of coeliac disease: A cross-sectional survey of a UK population. Br. J. Health Psychol. 2012, 17, 743–757. [Google Scholar] [CrossRef]
- Sainsbury, K.; Mullan, B. Measuring beliefs about gluten free diet adherence in adult coeliac disease using the theory of planned behaviour. Appetite 2011, 56, 476–483. [Google Scholar] [CrossRef]
- Hall, N.J.; Rubin, G.P.; Charnock, A. Intentional and inadvertent non-adherence in adult coeliac disease. A cross-sectional survey. Appetite 2013, 68, 56–62. [Google Scholar] [CrossRef]
- DiMatteo, M.R. Social support and patient adherence to medical treatment: A meta-analysis. Health Psychol. 2004, 23, 207–218. [Google Scholar] [CrossRef]
- Kurppa, K.; Lauronen, O.; Collin, P.; Ukkola, A.; Laurila, K.; Huhtala, H.; Mäki, M.; Kaukinen, K. Factors associated with dietary adherence in celiac disease: A nationwide study. Digestion 2012, 86, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Paganizza, S.; Zanotti, R.; D’Odorico, A.; Scapolo, P.; Canova, C. Is Adherence to a Gluten-Free Diet by Adult Patients With Celiac Disease Influenced by Their Knowledge of the Gluten Content of Foods? Gastroenterol. Nurs. 2019, 42, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Sainsbury, K.; Mullan, B.; Sharpe, L. A randomized controlled trial of an online intervention to improve gluten-free diet adherence in celiac disease. Am. J. Gastroenterol. 2013, 108, 811–817. [Google Scholar] [CrossRef] [PubMed]
- Wahab, P.J.; Meijer, J.W.R.; Mulder, C.J.J. Histologic follow-up of people with celiac disease on a gluten-free diet: Slow and incomplete recovery. Am. J. Clin. Pathol. 2002, 118, 459–463. [Google Scholar] [CrossRef] [PubMed]
- Penny, H.A.; Raju, S.A.; Lau, M.S.; Marks, L.J.; Baggus, E.M.; Bai, J.C.; Bassotti, G.; Bontkes, H.J.; Carroccio, A.; Danciu, M.; et al. Accuracy of a no-biopsy approach for the diagnosis of coeliac disease across different adult cohorts. Gut 2021, 70, 876–883. [Google Scholar] [CrossRef]
- Sadeghi, A.; Rad, N.; Ashtari, S.; Rostami-Nejad, M.; Moradi, A.; Haghbin, M.; Rostami, K.; Volta, U.; Zali, M.R. The value of a biopsy in celiac disease follow up: Assessment of the small bowel after 6 and 24 months treatment with a gluten free diet. Rev. Esp. Enfermedades Dig. 2020, 112, 101–108. [Google Scholar] [CrossRef]
- Al-toma, A.; Verbeek, W.H.; Mulder, C.J. The management of complicated celiac disease. Dig. Dis. 2007, 25, 230–236. [Google Scholar] [CrossRef]
- Al-Toma, A.; Mulder, C. Chapter 13—Gluten-related disorders: Monitoring and follow-up. In Gluten-Related Disorders; Rostami-Nejad, M., Ed.; Academic Press: Cambridge, MA, USA, 2022; pp. 201–211. ISBN 9780128218464. [Google Scholar] [CrossRef]
- Singh, P.; Arora, S.; Lal, S.; Strand, T.A.; Makharia, G.K. Risk of Celiac Disease in the First- and Second-Degree Relatives of Patients With Celiac Disease: A Systematic Review and Meta-Analysis. Am. J. Gastroenterol. 2015, 110, 1539–1548. [Google Scholar] [CrossRef]
- Downey, L.; Houten, R.; Murch, S.; Longson, D.; Guideline Development Group. Recognition, assessment, and management of coeliac disease: Summary of updated NICE guidance. BMJ 2015, 351, h4513. [Google Scholar] [CrossRef]
- Karell, K.; Louka, A.S.; Moodie, S.J.; Ascher, H.; Clot, F.; Greco, L.; Ciclitira, P.J.; Sollid, L.M.; Partanen, J.; European Genetics Cluster on Celiac Disease. HLA types in celiac disease patients not carrying the DQA1 *05-DQB1 *02 (DQ2) heterodimer: Results from the European genetics cluster on celiac disease. Hum. Immunol. 2003, 64, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Paavola, S.; Kurppa, K.; Huhtala, H.; Saavalainen, P.; Lindfors, K.; Kaukinen, K. Coeliac disease re-screening among once seronegative at-risk relatives: A long-term follow-up study. United Eur. Gastroenterol. J. 2022, 10, 585–593. [Google Scholar] [CrossRef] [PubMed]
- King, J.A.; Jeong, J.; Underwood, F.E.; Quan, J.; Panaccione, N.; Windsor, J.W.; Coward, S.; deBruyn, J.; Ronksley, P.E.; Shaheen, A.A.; et al. Incidence of Celiac Disease Is Increasing Over Time: A Systematic Review and Meta-analysis. Am. J. Gastroenterol. 2020, 115, 507–525. [Google Scholar] [CrossRef] [PubMed]
- Provenzale, D.; Ofman, J.; Gralnek, I.; Rabeneck, L.; Koff, R.; McCrory, D. Gastroenterologist specialist care and care provided by generalists--an evaluation of effectiveness and efficiency. Am. J. Gastroenterol. 2003, 98, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F.; Lebwohl, B.; Chen, Q.; Bröms, G.; Wolf, R.L.; Green, P.H.R.; Emilsson, L. Anxiety after coeliac disease diagnosis predicts mucosal healing: A population-based study. Aliment. Pharmacol. Ther. 2018, 48, 1091–1098. [Google Scholar] [CrossRef] [PubMed]
- Halmos, E.P.; Deng, M.; Knowles, S.R.; Sainsbury, K.; Mullan, B.; Tye-Din, J.A. Food knowledge and psychological state predict adherence to a gluten-free diet in a survey of 5310 Australians and New Zealanders with coeliac disease. Aliment. Pharmacol. Ther. 2018, 48, 78–86. [Google Scholar] [CrossRef]
- Lomash, A.; Venkatakrishnan, A.; Bothra, M.; Dhingra, B.; Kumar, P.; Kapoor, S. Coeliac disease presenting atypically: A much wider spectrum. Trop Doct. 2021, 51, 309–314. [Google Scholar] [CrossRef]
- Scaldaferri, F.; Pugliese, D.; Privitera, G.; Onali, S.; Lopetuso, L.R.; Rizzatti, G.; Settanni, C.R.; Pizzoferrato, M.; Schiavoni, E.; Turchini, L.; et al. Impact of COVID-19 pandemic on the daily management of biotechnological therapy in inflammatory bowel disease patients: Reorganisational response in a high-volume Italian inflammatory bowel disease centre. United Eur. Gastroenterol. J. 2020, 8, 775–781. [Google Scholar] [CrossRef]
- Pekki, H.; Kaukinen, K.; Ilus, T.; Mäki, M.; Huhtala, H.; Laurila, K.; Kurppa, K. Long-term follow-up in adults with coeliac disease: Predictors and effect on health outcomes. Dig. Liver Dis. 2018, 50, 1189–1194. [Google Scholar] [CrossRef]
- Cohidon, C.; Wild, P.; Senn, N. Job stress among GPs: Associations with practice organisation in 11 high-income countries. Br. J. Gen. Pract. 2020, 70, E657–E667. [Google Scholar] [CrossRef]
- Franceschini, E.; Lionetti, M.E.; D’Adamo, G.; D’Angelo, E.; Gatti, S.; Naspi Catassi, G.; Malamisura, B.; Catassi, C. Misuse of serological screening tests for celiac disease in children: A prospective study in Italy. Dig. Liver Dis. 2019, 51, 1547–1550. [Google Scholar] [CrossRef]
- Mearin, M.L.; Agardh, D.; Antunes, H.; Al-Toma, A.; Auricchio, R.; Castillejo, G.; Catassi, C.; Ciacci, C.; Discepolo, V.; Dolinsek, J.; et al. ESPGHAN Position Paper on Management and Follow-up of Children and Adolescents With Celiac Disease. J. Pediatr. Gastroenterol. Nutr. 2022, 75, 369–386. [Google Scholar] [CrossRef] [PubMed]
- Celiac Disease Center at UCLA|Eat! Gluten-Free. Available online: https://celiac.org/eat-gluten-free/gf-services/celiac-disease-center-at-ucla/ (accessed on 26 February 2023).
- Homepage—Celiac Disease Center at Columbia University Medical Center Celiac Disease Center at Columbia University Medical Center. Available online: https://celiacdiseasecenter.columbia.edu/ (accessed on 26 February 2023).
- Celiac Disease Center at The University of Chicago|Eat! Gluten-Free. Available online: https://celiac.org/eat-gluten-free/gf-services/celiacdiseasecenterchicago/ (accessed on 26 February 2023).
- Celiac Disease Treatment in Spain: Cost, Reviews in Top 11 Clinics|MediGlobus. Available online: https://mediglobus.com/clinics/country-spain/diseases-celiac-disease/ (accessed on 9 April 2023).
- Cilleruelo, M.L.; Roman-Riechmann, E.; Sanchez-Valverde, F.; Donat, E.; Manuel-Ramos, J.; Martín-Orte, E.; López, M.J.; García-Novo, D.; García, S.; Pavón, P.; et al. Spanish National Registry of Celiac Disease: Incidence and clinical presentation. J. Pediatr. Gastroenterol. Nutr. 2014, 59, 522–526. [Google Scholar] [CrossRef]
- Weber, M.; Wolf, N.; Branchi, F.; Tangermann, P.; Itzlinger, A.; Poralla, L.; Preiß, J.C.; Grunert, P.; Daum, S.; Siegmund, B.; et al. Results from the German registry for refractory celiac disease. Z. Gastroenterol. 2021, 59, 944–953. [Google Scholar] [CrossRef]
- de Jong, M.J.; Boonen, A.; van der Meulen-de Jong, A.E.; Romberg-Camps, M.J.; van Bodegraven, A.A.; Mahmmod, N.; Markus, T.; Dijkstra, G.; Winkens, B.; van Tubergen, A.; et al. Cost-effectiveness of Telemedicine-directed Specialized vs Standard Care for Patients with Inflammatory Bowel Diseases in a Randomized Trial. Clin. Gastroenterol. Hepatol. 2020, 18, 1744–1752. [Google Scholar] [CrossRef] [PubMed]
- Nikniaz, Z.; Namvar, Z.A.; Shirmohammadi, M.; Maserat, E. Smartphone Application for Celiac Patients: Assessing Its Effect on Gastrointestinal Symptoms in a Randomized Controlled Clinical Trial. Int. J. Telemed. Appl. 2022, 2022, 8027532. [Google Scholar] [CrossRef] [PubMed]
- Perez-Junkera, G.; Vázquez-Polo, M.; Eizagirre, F.J.; Benjumea, L.; Tutau, C.; Esteban, B.; Miranda, J.; Larretxi, I.; Navarro, V.; Churruca, I.; et al. Application of a Platform for Gluten-Free Diet Evaluation and Dietary Advice: From Theory to Practice. Sensors 2022, 22, 732. [Google Scholar] [CrossRef]
- Muhammad, H.; Reeves, S.; Ishaq, S.; Mayberry, J.F.; Jeanes, Y.M. Telephone clinic improves gluten-free dietary adherence in adults with coeliac disease: Sustained at 6 months. Frontline Gastroenterol. 2020, 12, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Stuckey, C. Management of adult coeliac disease with a dietitian-led virtual clinic. Gastrointest. Nurs. 2015, 13, 38–43. [Google Scholar] [CrossRef]
- Zhou, F.; Mullen, T.; Kulai, T.; Rashid, M. Assessment of Knowledge of Gluten-Free Diet Amongst Food Handlers in Hospitals. Can. J. Diet. Pract. Res. 2022, 83, 1–6. [Google Scholar] [CrossRef]
- Accessing Gluten Free Food in Hospital—Coeliac UK. Available online: https://www.coeliac.org.uk/information-and-support/living-gluten-free/the-gluten-free-diet/hospital-visits/?&&type=rfst&set=true#cookie-widget (accessed on 9 April 2023).
- Catassi, C.; Fabiani, E.; Iacono, G.; D’Agate, C.; Francavilla, R.; Biagi, F.; Volta, U.; Accomando, S.; Picarelli, A.; De Vitis, I.; et al. A prospective, double-blind, placebo-controlled trial to establish a safe gluten threshold for patients with celiac disease. Am. J. Clin. Nutr. 2007, 85, 160–166. [Google Scholar] [CrossRef]
- Burger, J.P.W.; van Lochem, E.G.; Roovers, E.A.; Drenth, J.P.H.; Wahab, P.J. Dose-Escalating (50–500 mg) Gluten Administration Leads to Detectable Gluten-Immunogenic-Peptides in Urine of Patients with Coeliac Disease Which Is Unrelated to Symptoms, a Placebo Controlled Trial. Nutrients 2022, 14, 1771. [Google Scholar] [CrossRef]
- Al-Toma, A.; Herman, A.; Lems, W.F.; JMulder, C.J. The Dietary and Non-Dietary Management of Osteoporosis in Adult-Onset Celiac Disease: Current Status and Practical Guidance. Nutrients 2022, 14, 4554. [Google Scholar] [CrossRef] [PubMed]
- Clappison, E.; Hadjivassiliou, M.; Zis, P. Psychiatric Manifestations of Coeliac Disease, a Systematic Review and Meta-Analysis. Nutrients 2020, 12, 142. [Google Scholar] [CrossRef] [PubMed]
- Paarlahti, P.; Kurppa, K.; Ukkola, A.; Collin, P.; Huhtala, H.; Mäki, M.; Kaukinen, K. Predictors of persistent symptoms and reduced quality of life in treated coeliac disease patients: A large cross-sectional study. BMC Gastroenterol. 2013, 13, 75. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Time | What Is Needed | Who *? How? |
|---|---|---|
| At diagnosis | Physical Examination (BMI) | Physician and dietician. Face-to-face |
| Counselling by a “celiac” dietician | ||
| Discuss family screening | ||
| Recommend Celiac Society or Support group | ||
| Serology (IgA-anti TG2), lab, DXA (30–35 years start) or at diagnosis in special scenarios | ||
| Visit 3–4 months | Assess symptoms and compliance | Gastroenterologist and/or dietician; Face-to-face, telephone, or video call |
| Serology (IgA-anti TG2) | ||
| Routine tests (if previously abnormal) | ||
| At 12 months | Assess Weight, symptoms | Physician and/or dietitian Face-to-face, telephone, or video call |
| Diet review | ||
| Celiac serology, routine tests | ||
| Thyroid function tests | ||
| Metabolic status | ||
| Small bowel biopsy (not routinely) | ||
| At 24 months | Symptoms and dietary review | Physician and/or dietitian Face-to-face, telephone, or video call |
| Celiac serology | ||
| Other tests if clinically indicated | ||
| Thereafter every 1–2 years | Assess symptoms | Physician or dietitian Face-to-face, telephone, or video call |
| Consider dietary review | ||
| Celiac serology | ||
| Thyroid function tests | ||
| Other tests as clinically indicate | ||
| Bone densitometry (if abnormal) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mulder, C.J.J.; Elli, L.; Lebwohl, B.; Makharia, G.K.; Rostami, K.; Rubio-Tapia, A.; Schumann, M.; Tye-Din, J.; Zeitz, J.; Al-Toma, A. Follow-Up of Celiac Disease in Adults: “When, What, Who, and Where”. Nutrients 2023, 15, 2048. https://doi.org/10.3390/nu15092048
Mulder CJJ, Elli L, Lebwohl B, Makharia GK, Rostami K, Rubio-Tapia A, Schumann M, Tye-Din J, Zeitz J, Al-Toma A. Follow-Up of Celiac Disease in Adults: “When, What, Who, and Where”. Nutrients. 2023; 15(9):2048. https://doi.org/10.3390/nu15092048
Chicago/Turabian StyleMulder, Chris J. J., Luca Elli, Benjamin Lebwohl, Govind K. Makharia, Kamran Rostami, Alberto Rubio-Tapia, Michael Schumann, Jason Tye-Din, Jonas Zeitz, and Abdulbaqi Al-Toma. 2023. "Follow-Up of Celiac Disease in Adults: “When, What, Who, and Where”" Nutrients 15, no. 9: 2048. https://doi.org/10.3390/nu15092048
APA StyleMulder, C. J. J., Elli, L., Lebwohl, B., Makharia, G. K., Rostami, K., Rubio-Tapia, A., Schumann, M., Tye-Din, J., Zeitz, J., & Al-Toma, A. (2023). Follow-Up of Celiac Disease in Adults: “When, What, Who, and Where”. Nutrients, 15(9), 2048. https://doi.org/10.3390/nu15092048