

Yoghurt Intake and Gastric Cancer: A Pooled Analysis of 16 Studies of the StoP Consortium

 , , , , , ,
, , , , , ,  , , , , , ,
, , , , , ,  , , , , ,
, , , , ,  , , , ,
, , , ,  and add
Show full author list
and add
Show full author list
Abstract
1. Introduction
2. Methods
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Cancer Research Fund International. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective—The Third Expert Report; World Cancer Research Fund International: London, UK, 2018; Available online: https://www.wcrf.org/dietandcancer (accessed on 3 December 2022).
- Agudo, A.; Cayssials, V.; Bonet, C.; Tjønneland, A.; Overvad, K.; Boutron-Ruault, M.C.; Affret, A.; Fagherazzi, G.; Katzke, V.; Schübel, R.; et al. Inflammatory potential of the diet and risk of gastric cancer in the EuropeanProspective Investigation into Cancer and Nutrition (EPIC) study. Am. J. Clin. Nutr. 2018, 107, 607–616. [Google Scholar] [CrossRef] [PubMed]
- Aryana, K.J.; Olson, D.W. A 100-Year Review: Yogurt and other cultured dairy products. J. Dairy Sci. 2017, 100, 9987–10013. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Dai, H.; Liang, W.; Zhang, L.; Deng, Z. Fermented dairy foods intake and risk of cancer. Int. J. Cancer 2019, 144, 2099–2108. [Google Scholar] [CrossRef]
- Jeyaraman, M.M.; Abou-Setta, A.M.; Grant, L.; Farshidfar, F.; Copstein, L.; Lys, J.; Gottschalk, T.; Desautels, D.; Czaykowski, P.; Pitz, M.; et al. Dairy product consumption and development of cancer: An overview of reviews. BMJ Open 2019, 9, e023625. [Google Scholar] [CrossRef]
- Stiemsma, L.T.; Nakamura, R.E.; Nguyen, J.G.; Michels, K.B. Does Consumption of Fermented Foods Modify the Human Gut Microbiota? J. Nutr. 2020, 150, 1680–1692. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.J.; Sheu, B.S. Probiotics-containing yogurts suppress Helicobacter pylori load and modify immune response and intestinal microbiota in the Helicobacter pylori-infected children. Helicobacter 2012, 17, 297–304. [Google Scholar] [CrossRef]
- Uchida, M.; Shimizu, K.; Kurakazu, K. Yogurt containing Lactobacillus gasseri OLL 2716 (LG21 yogurt) accelerated the healing of acetic acid-induced gastric ulcer in rats. Biosci. Biotechnol. Biochem. 2010, 74, 1891–1894. [Google Scholar] [CrossRef]
- Koga, Y.; Ohtsu, T.; Kimura, K.; Asami, Y. Probiotic L. gasseri strain (LG21) for the upper gastrointestinal tract acting through improvement of indigenous microbiota. BMJ Open Gastroenterol. 2019, 6, e000314. [Google Scholar] [CrossRef]
- Nair, M.R.; Chouhan, D.; Sen Gupta, S.; Chattopadhyay, S. Fermented Foods: Are They Tasty Medicines for Helicobacter pylori Associated Peptic Ulcer and Gastric Cancer? Front. Microbiol. 2016, 7, 1148. [Google Scholar] [CrossRef]
- Maldonado Galdeano, C.; Novotny Nuñez, I.; Carmuega, E.; de Moreno de LeBlanc, A.; Perdigón, G. Role of probiotics and functional foods in health: Gut immune stimulation by two probiotic strains and a potential probiotic yoghurt. Endocr. Metab. Immune Disord. Drug Targets 2015, 15, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Poorolajal, J.; Moradi, L.; Mohammadi, Y.; Cheraghi, Z.; Gohari-Ensaf, F. Risk factors for stomach cancer: A systematic review and meta-analysis. Epidemiol Health 2020, 42, e2020004. [Google Scholar] [CrossRef]
- Thorning, T.K.; Raben, A.; Tholstrup, T.; Soedamah-Muthu, S.S.; Givens, I.; Astrup, A. Milk and dairy products: Good or bad for human health? An assessment of the totality of scientific evidence. Food Nutr. Res. 2016, 60, 32527. [Google Scholar] [CrossRef]
- Sun, Y.; Lin, L.J.; Sang, L.X.; Dai, C.; Jiang, M.; Zheng, C.Q. Dairy product consumption and gastric cancer risk: A meta-analysis. World J. Gastroenterol. 2014, 20, 15879–15898. [Google Scholar] [CrossRef]
- Tian, S.B.; Yu, J.C.; Kang, W.M.; Ma, Z.Q.; Ye, X.; Cao, Z.J. Association between dairy intake and gastric cancer: A meta-analysis of observational studies. PLoS ONE 2014, 9, e101728. [Google Scholar] [CrossRef]
- Available online: http://www.stop-project.org/ (accessed on 14 December 2022).
- Psaltopoulou, T.; Kyrozis, A.; Stathopoulos, P.; Trichopoulos, D.; Vassilopoulos, D.; Trichopoulou, A. Diet, physical activity and cognitive impairment among elders: The EPIC-Greece cohort (European Prospective Investigation into Cancer and Nutrition). Public Health Nutr. 2008, 11, 1054–1062. [Google Scholar] [CrossRef]
- The ATBC Cancer Prevention Study Group. The alpha-tocopherol, beta-carotene lung cancer prevention study: Design, methods, participant characteristics, and compliance. Ann. Epidemiol. 1994, 4, 1–10. [Google Scholar] [CrossRef]
- Pelucchi, C.; Lunet, N.; Boccia, S.; Zhang, Z.F.; Praud, D.; Boffetta, P.; Levi, F.; Matsuo, K.; Ito, H.; Hu, J.; et al. The stomach cancer pooling (StoP) project: Study design and presentation. Eur. J. Cancer Prev. 2015, 24, 16–23. [Google Scholar] [CrossRef]
- Lucenteforte, E.; Scita, V.; Bosetti, C.; Bertuccio, P.; Negri, E.; La Vecchia, C. Food groups and alcoholic beverages and the risk of stomach cancer: A case-control study in Italy. Nutr. Cancer 2008, 60, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Buiatti, E.; Palli, D.; Decarli, A.; Amadori, D.; Avellini, C.; Bianchi, S.; Biserni, R.; Cipriani, F.; Cocco, P.; Giacosa, A.; et al. A case-control study of gastric cancer and diet in Italy. Int. J. Cancer 1989, 44, 611–616. [Google Scholar] [CrossRef] [PubMed]
- Lunet, N.; Valbuena, C.; Vieira, A.L.; Lopes, C.; Lopes, C.; David, L.; Carneiro, F.; Barros, H. Fruit and vegetable consumption and gastric cancer by location and histological type: Case-control and meta-analysis. Eur. J. Cancer Prev. 2007, 16, 312–327. [Google Scholar] [CrossRef] [PubMed]
- Castaño-Vinyals, G.; Aragonés, N.; Pérez-Gómez, B.; Martín, V.; Llorca, J.; Moreno, V.; Altzibar, J.M.; Ardanaz, E.; de Sanjosé, S.; Jiménez-Moleón, J.J.; et al. Population-based multicase-control study in common tumors in Spain (MCC-Spain): Rationale and study design. Gac. Sanit. 2015, 29, 308–315. [Google Scholar] [CrossRef] [PubMed]
- Santibañez, M.; Alguacil, J.; de la Hera, M.G.; Navarrete-Muñoz, E.M.; Llorca, J.; Aragonés, N.; Kauppinen, T.; Vioque, J.; PANESOES Study Group. Occupational exposures and risk of stomach cancer by histological type. Occup. Environ. Med. 2012, 69, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Lagiou, P.; Samoli, E.; Lagiou, A.; Peterson, J.; Tzonou, A.; Dwyer, J.; Trichopoulos, D. Flavonoids, vitamin C and adenocarcinoma of the stomach. Cancer Causes Control 2004, 15, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Machida-Montani, A.; Sasazuki, S.; Inoue, M.; Natsukawa, S.; Shaura, K.; Koizumi, Y.; Kasuga, Y.; Hanaoka, T.; Tsugane, S. Association of Helicobacter pylori infection and environmental factors in non-cardia gastric cancer in Japan. Gastric. Cancer 2004, 7, 46–53. [Google Scholar] [CrossRef]
- Zaridze, D.; Borisova, E.; Maximovitch, D.; Chkhikvadze, V. Aspirin protects against gastric cancer: Results of a case-control study from Moscow, Russia. Int. J. Cancer 1999, 82, 473–476. [Google Scholar] [CrossRef]
- Hernández-Ramírez, R.U.; Galván-Portillo, M.V.; Ward, M.H.; Agudo, A.; González, C.A.; Oñate-Ocaña, L.F.; Herrera-Goepfert, R.; Palma-Coca, O.; López-Carrillo, L. Dietary intake of polyphenols, nitrate and nitrite and gastric cancer risk in Mexico City. Int. J. Cancer 2009, 125, 1424–1430. [Google Scholar] [CrossRef]
- López-Carrillo, L.; Hernández Avila, M.; Dubrow, R. Chili pepper consumption and gastric cancer in Mexico: A case-control study. Am. J. Epidemiol. 1994, 139, 263–271. [Google Scholar] [CrossRef]
- López-Carrillo, L.; López-Cervantes, M.; Robles-Díaz, G.; Ramírez-Espitia, A.; Mohar-Betancourt, A.; Meneses-García, A.; López-Vidal, Y.; Blair, A. Capsaicin consumption, Helicobacter pylori positivity and gastric cancer in Mexico. Int. J. Cancer 2003, 106, 277–282. [Google Scholar] [CrossRef]
- Zhang, Z.F.; Kurtz, R.C.; Klimstra, D.S.; Yu, G.P.; Sun, M.; Harlap, S.; Marshall, J.R. Helicobacter pylori infection on the risk of stomach cancer and chronic atrophic gastritis. Cancer Detect. Prev. 1999, 23, 357–367. [Google Scholar] [CrossRef]
- Schatzkin, A.; Subar, A.F.; Thompson, F.E.; Harlan, L.C.; Tangrea, J.; Hollenbeck, A.R.; Hurwitz, P.E.; Coyle, L.; Schussler, N.; Michaud, D.S.; et al. Design and serendipity in establishing a large cohort with wide dietary intake distributions: The National Institutes of Health-American Association of Retired Persons Diet and Health Study. Am. J. Epidemiol. 2001, 154, 1119–1125. [Google Scholar] [CrossRef]
- Peres, S.V.; Silva, D.R.M.; Coimbra, F.J.F.; Fagundes, M.A.; Auzier, J.J.N.; Pelosof, A.G.; Araujo, M.S.; Assumpção, P.P.; Curado, M.P. Consumption of processed and ultra-processed foods by patients with stomach adenocarcinoma: A multicentric case-control study in the Amazon and southeast regions of Brazil. Cancer Causes Control. 2022, 33, 889–898. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trial Control Clin Trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- StataCorp. Stata Statistical Software: Release 16; StataCorp LLC: College Station, TX, USA, 2019. [Google Scholar]
- Fisberg, M.; Machado, R. History of yogurt and current patterns of consumption. Nutr. Rev. 2015, 73 (Suppl. 1), 4–7. [Google Scholar] [CrossRef]
- Ritchie, M.L.; Romanuk, T.N. A meta-analysis of probiotic efficacy for gastrointestinal diseases. PLoS ONE 2012, 7, e34938. [Google Scholar] [CrossRef]
- Srinarong, C.; Siramolpiwat, S.; Wongcha-um, A.; Mahachai, V.; Vilaichone, R.K. Improved eradication rate of standard triple therapy by adding bismuth and probiotic supplement for Helicobacter pylori treatment in Thailand. Asian Pac. J. Cancer Prev. 2014, 15, 9909–9913. [Google Scholar] [CrossRef]
- Westerik, N.; Reid, G.; Sybesma, W.; Kort, R. The Probiotic Lactobacillus rhamnosus for Alleviation of Helicobacter pylori-Associated Gastric Pathology in East Africa. Front. Microbiol. 2018, 9, 1873. [Google Scholar] [CrossRef]
- Shi, X.; Zhang, J.; Mo, L.; Shi, J.; Qin, M.; Huang, X. Efficacy and safety of probiotics in eradicating Helicobacter pylori: A network meta-analysis. Medicine 2019, 98, e15180. [Google Scholar] [CrossRef]
- Wang, X.; Shu, X.; Li, Q.; Li, Y.; Chen, Z.; Wang, Y.; Pu, K.; Zheng, Y.; Ye, Y.; Liu, M.; et al. Prevalence and risk factors of Helicobacter pylori infection in Wuwei, a high-risk area for gastric cancer in northwest China: An all-ages population-based cross-sectional study. Helicobacter 2021, 26, e12810. [Google Scholar] [CrossRef]
- Scourboutakos, M.J.; Franco-Arellano, B.; Murphy, S.A.; Norsen, S.; Comelli, E.M.; L’Abbé, M.R. Mismatch between Probiotic Benefits in Trials versus Food Products. Nutrients 2017, 9, 400. [Google Scholar] [CrossRef] [PubMed]
- Soni, R.; Jain, N.K.; Shah, V.; Soni, J.; Suthar, D.; Gohel, P. Development of probiotic yogurt: Effect of strain combination on nutritional, rheological, organoleptic and probiotic properties. J. Food Sci. Technol. 2020, 57, 2038–2050. [Google Scholar] [CrossRef] [PubMed]
- Nagaoka, S. Yogurt Production. Methods Mol. Biol. 2019, 1887, 45–54. [Google Scholar]
- Ashraf, R.; Shah, N.P. Selective and differential enumerations of Lactobacillus delbrueckii subsp. bulgaricus, Streptococcus thermophilus, Lactobacillus acidophilus, Lactobacillus casei and Bifidobacterium spp. in yoghurt—A review. Int. J. Food Microbiol. 2011, 149, 194–208. [Google Scholar] [CrossRef]
- Thorning, T.K.; Bertram, H.C.; Bonjour, J.P.; de Groot, L.; Dupont, D.; Feeney, E.; Ipsen, R.; Lecerf, J.M.; Mackie, A.; McKinley, M.C.; et al. Whole dairy matrix or single nutrients in assessment of health effects: Current evidence and knowledge gaps. Am. J. Clin. Nutr. 2017, 105, 1033–1045. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Shan, Z.; Ren, H.; Chen, W. Dairy consumption and gastric cancer risk: A meta-analysis of epidemiological studies. Nutr. Cancer 2015, 67, 555–568. [Google Scholar] [CrossRef] [PubMed]
- Song, J.W.; Chung, K.C. Observational studies: Cohort and case-control studies. Plast Reconstr Surg. 2010, 126, 2234–2242. [Google Scholar] [CrossRef]
- Jacobs, D.R. Challenges in Research in Nutritional Epidemiology. In Nutritional Health. Nutrition and Health; Temple, N., Wilson, T., Jacobs, D., Jr., Eds.; Humana Press: Totowa, NJ, USA, 2012. [Google Scholar]
- Thornton, K.; Villamor, E. Nutritional Epidemiology. In Encyclopedia of Food and Health; Caballero, B., Finglas, P.M., Toldrá, F., Eds.; Academic Press: Oxford, UK, 2016; pp. 104–107. [Google Scholar]
- Honda, M.; Wong, S.L.; Healy, M.A.; Nakajima, T.; Watanabe, M.; Fukuma, S.; Fukuhara, S.; Ayanian, J.Z. Long-term Trends in Primary Sites of Gastric Adenocarcinoma in Japan and the United States. J. Cancer 2017, 8, 1935–1942. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Cases [N(%)] | Controls [N(%)] | |
|---|---|---|
| Total | 6278 (100.0) | 14,181 (100.0) |
| Sex | ||
| Male | 4099 (65.3) | 8389 (59.2) |
| Female | 2179 (34.7) | 5792 (40.8) |
| Age (years) | ||
| ≤55 | 1321 (21.1) | 3521 (24.8) |
| 56–59 | 528 (8.4) | 1165 (8.2) |
| 60–64 | 848 (13.5) | 1985 (14.0) |
| 65–69 | 1226 (19.5) | 2620 (18.5) |
| 70–74 | 1326 (21.1) | 2584 (18.2) |
| ≥75 | 1029 (16.4) | 2306 (16.3) |
| Tobacco smoking | ||
| Never | 2452 (40.3) | 6320 (45.7) |
| Former | 2214 (36.4) | 4706 (33.9) |
| Current | 1416 (23.3) | 2819 (20.4) |
| Alcohol drinking | ||
| Never | 1591 (26.1) | 3835 (28.8) |
| Low | 1721 (28.3) | 4725 (35.5) |
| Intermediate | 1899 (31.2) | 3441 (25.9) |
| High | 877 (14.4) | 1296 (9.8) |
| Socio-economic status | ||
| Low | 2870 (46.9) | 5159 (36.9) |
| Intermediate | 2155 (35.2) | 5290 (37.8) |
| High | 1100 (17.9) | 3530 (25.3) |
| Vegetables and fruit intake | ||
| Low | 1926 (32.0) | 3840 (29.7) |
| Intermediate | 1977 (33.9) | 4434 (34.3) |
| High | 1934 (33.1) | 4673 (36.1) |
| Gastric cancer subsite | ||
| Cardia | 1179 (18.8) | NA |
| Non-cardia | 3463 (55.2) | |
| Undefined | 1198 (19.0) | |
| Histological type | NA | |
| Intestinal | 1717 (27.3) | |
| Diffuse | 1191 (18.9) | |
| Undefined | 2249 (35.8) | |
| Mean number of portions of yoghurt per week | 0.16 (0.15–0.17) | 0.25 (0.24–0.26) |
| Exposure | Cases-Controls | Overall GC OR (95% CI) Adjusted Model | Overall GC OR (95% CI) Raw Model |
|---|---|---|---|
| Portions of yoghurt intake per week | |||
| 0 | 3103–5552 | Ref | Ref |
| >0–0.5 | 1259–2705 | 0.86 (0.78–0.95) | 0.79 (0.72–0.87) |
| >0.5–1.5 | 539–1417 | 0.96 (0.85–1.08) | 0.79 (0.70–0.88) |
| >1.5–4.5 | 470–1650 | 0.86 (0.76–0.98) | 0.71 (0.63–0.80) |
| >4.5 | 535–2020 | 1.08 (0.95–1.22) | 0.84 (0.75–0.95) |
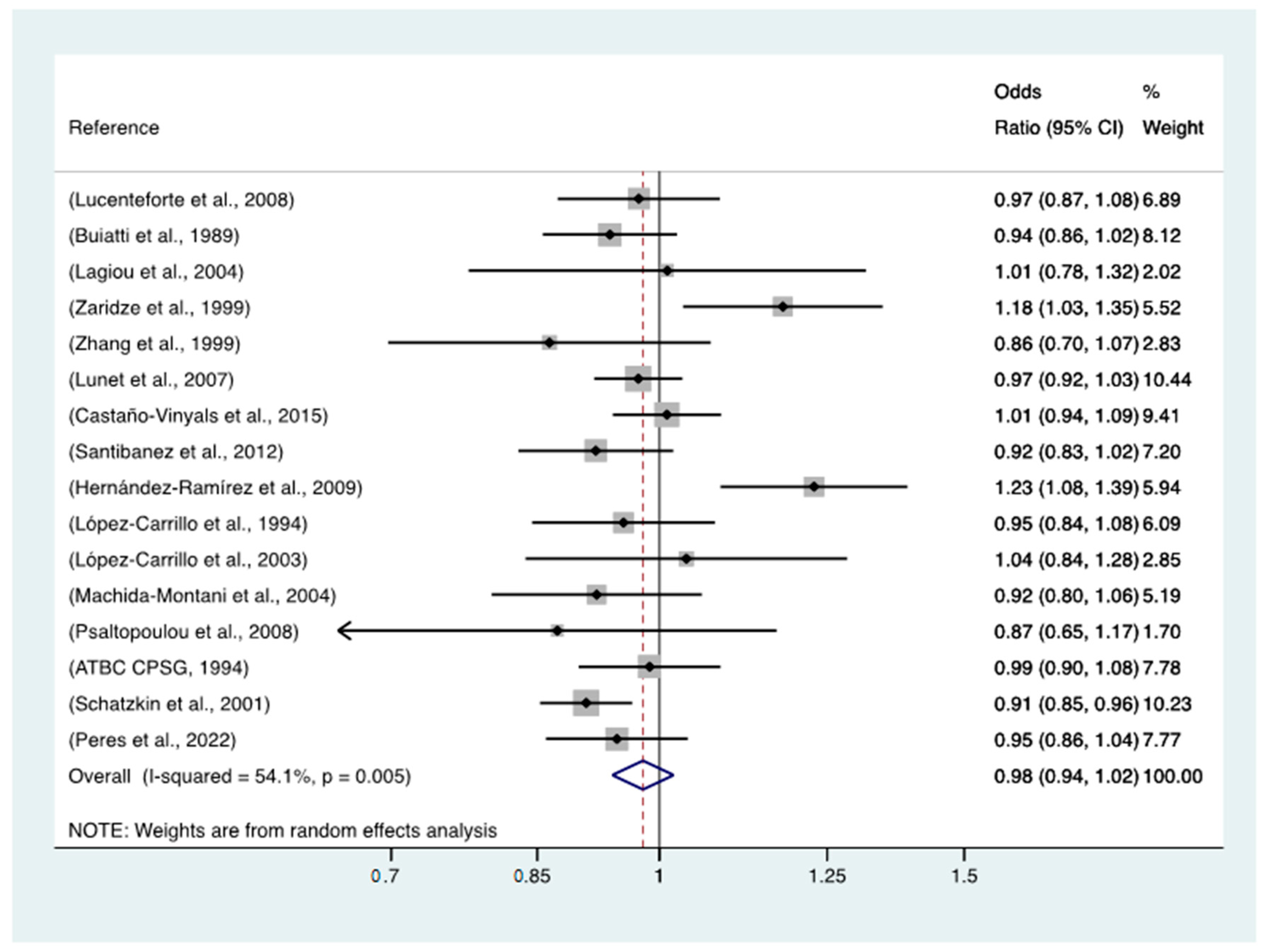
| Continuous (1 category per week increase) | 0.93 (0.97–1.03) | 0.93 (0.91–0.96) | |
| No/Any yoghurt intake | 0.92 (0.85–0.99) | 0.78 (0.73–0.84) |
| Exposure | Subsite of GC | Histology of GC | ||||
|---|---|---|---|---|---|---|
| Cardia (No = 1179) OR (95%CI) | Non-Cardia (No = 3463) OR (95%CI) | Undefined (No = 1198) OR (95% CI) | Diffuse (No = 1191) OR (95%CI) | Intestinal (No = 1717) OR (95%CI) | Undefined (No = 2249) OR (95% CI) | |
| Portions of yoghurt intake per week | ||||||
| 0 | Ref | Ref | Ref | Ref | Ref | Ref |
| >0–0.5 | 0.96 (0.81–1.13) | 0.95 (0.83–1.09) | 0.93 (0.78–1.11) | 1.05 (0.83–1.33) | 0.89 (0.72–1.11) | 0.87 (0.76–0.99) |
| >0.5–1.5 | 0.96 (0.74–1.24) | 1.01 (0.87–1.17) | 1.11 (0.89–1.40) | 1.34 (1.06–1.68) | 0.88 (0.71–1.09) | 0.92 (0.75–1.13) |
| >1.5–4.5 | 0.98 (0.75–1.29) | 0.93 (0.79–1.09) | 0.97 (0.76–1.25) | 1.15 (0.90–1.48) | 0.90 (0.71–1.13) | 0.88 (0.69–1.12) |
| >4.5 | 0.79 (0.58–1.06) | 1.23 (1.06–1.42) | 1.11 (0.85–1.45) | 1.73 (1.38–2.18) | 1.18 (0.96–1.45) | 0.83 (0.65–1.08) |
| Continuous (1 category increase) | 0.96 (0.90–1.02) | 1.03 (1.00–1.07) | 1.02 (0.96–1.08) | 1.12 (1.07–1.19) | 1.02 (0.97–1.06) | 0.95 (0.91–1.00) |
| p heterogeneity | p = 0.15 | p = <0.001 | ||||
| Exposure | Study Design | |
|---|---|---|
| Case-Control Hospital-Based OR (95%CI) | Case-Control Population-Based OR (95% CI) | |
| Yoghurt intake | ||
| 0 | Ref | Ref |
| >0–0.5 | 0.78 (0.64–0.95) | 0.86 (0.78–0.95) |
| >0.5–1.5 | 0.97 (0.79–1.21) | 0.96 (0.85–1.08) |
| >1.5–4.5 | 0.81 (0.65–1.02) | 0.86 (0.76–0.98) |
| >4.5 | 1.13 (0.89–1.44) | 1.08 (0.96–1.23) |
| Continuous (1 category increase) | 1.01 (0.96–1.06) | 1.00 (0.97–1.03) |
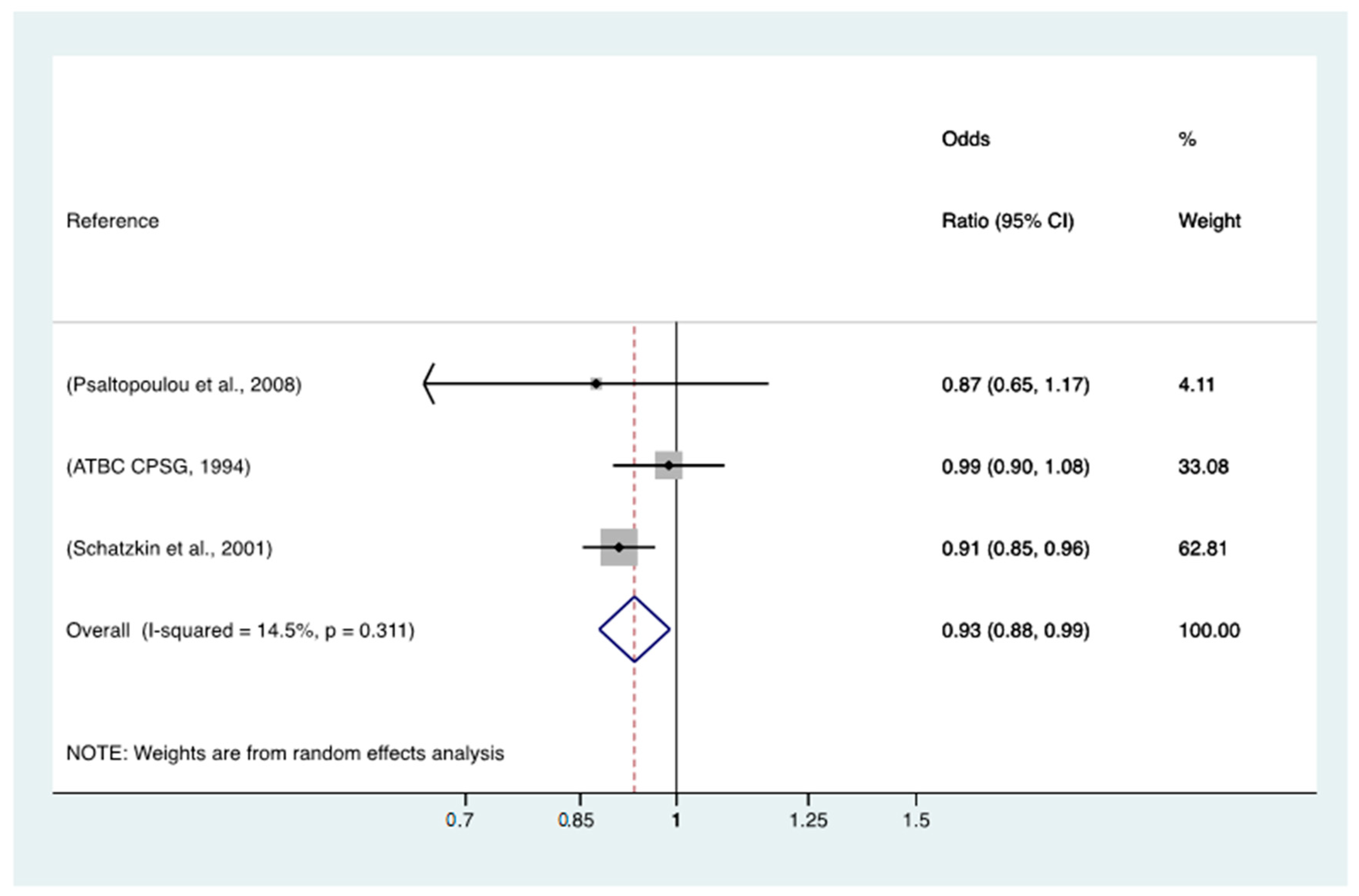
| p heterogeneity | 0.736 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Collatuzzo, G.; Negri, E.; Pelucchi, C.; Bonzi, R.; Turati, F.; Rabkin, C.S.; Liao, L.M.; Sinha, R.; Palli, D.; Ferraroni, M.; et al. Yoghurt Intake and Gastric Cancer: A Pooled Analysis of 16 Studies of the StoP Consortium. Nutrients 2023, 15, 1877. https://doi.org/10.3390/nu15081877
Collatuzzo G, Negri E, Pelucchi C, Bonzi R, Turati F, Rabkin CS, Liao LM, Sinha R, Palli D, Ferraroni M, et al. Yoghurt Intake and Gastric Cancer: A Pooled Analysis of 16 Studies of the StoP Consortium. Nutrients. 2023; 15(8):1877. https://doi.org/10.3390/nu15081877
Chicago/Turabian StyleCollatuzzo, Giulia, Eva Negri, Claudio Pelucchi, Rossella Bonzi, Federica Turati, Charles S. Rabkin, Linda M. Liao, Rashmi Sinha, Domenico Palli, Monica Ferraroni, and et al. 2023. "Yoghurt Intake and Gastric Cancer: A Pooled Analysis of 16 Studies of the StoP Consortium" Nutrients 15, no. 8: 1877. https://doi.org/10.3390/nu15081877
APA StyleCollatuzzo, G., Negri, E., Pelucchi, C., Bonzi, R., Turati, F., Rabkin, C. S., Liao, L. M., Sinha, R., Palli, D., Ferraroni, M., López-Carrillo, L., Lunet, N., Morais, S., Albanes, D., Weinstein, S. J., Parisi, D., Zaridze, D., Maximovitch, D., Dierssen-Sotos, T., ... Boffetta, P. (2023). Yoghurt Intake and Gastric Cancer: A Pooled Analysis of 16 Studies of the StoP Consortium. Nutrients, 15(8), 1877. https://doi.org/10.3390/nu15081877