
Randomized Clinical Trial to Evaluate the Morphological Changes in the Adventitial Vasa Vasorum Density and Biological Markers of Endothelial Dysfunction in Subjects with Moderate Obesity Undergoing a Very Low-Calorie Ketogenic Diet

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Approval
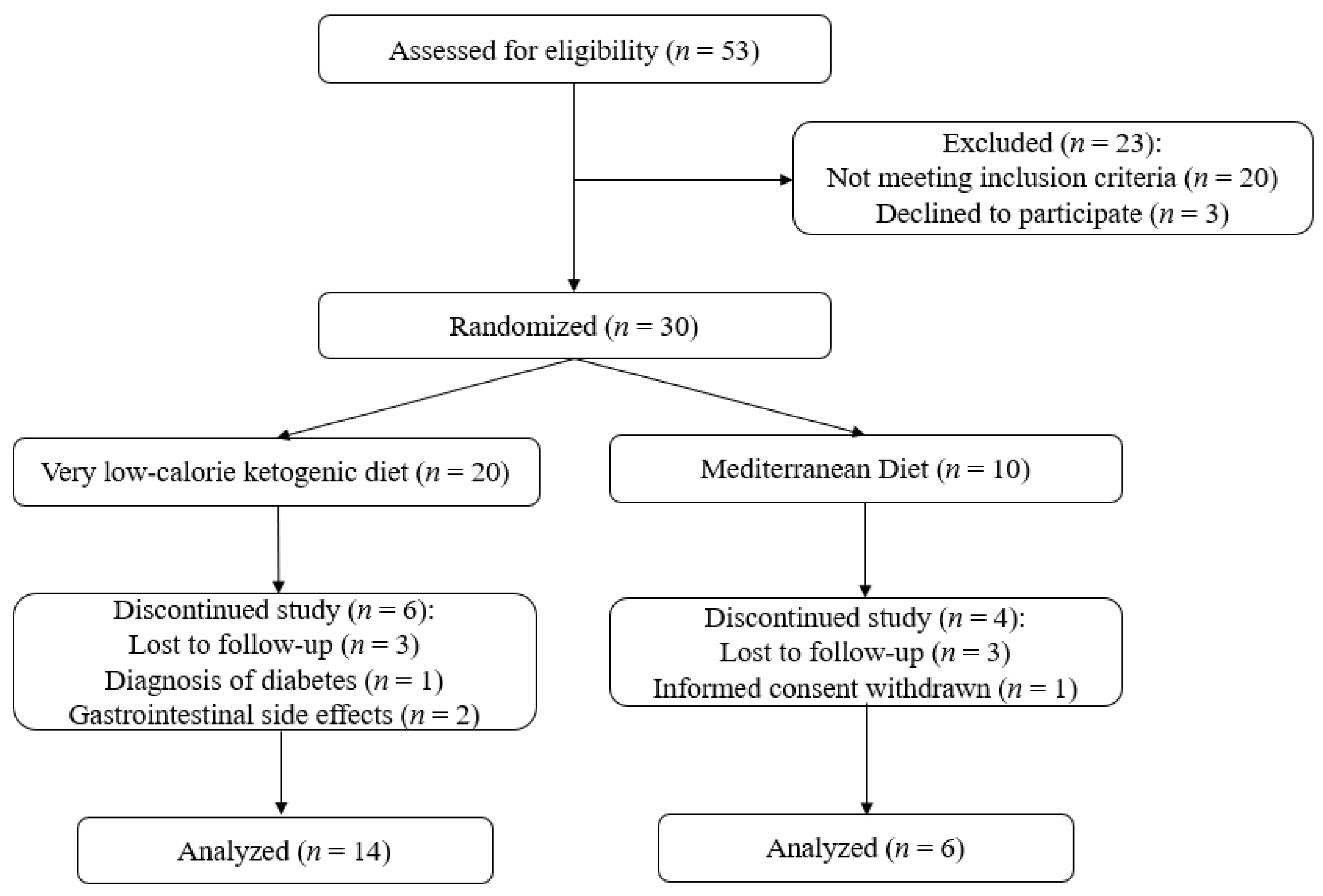
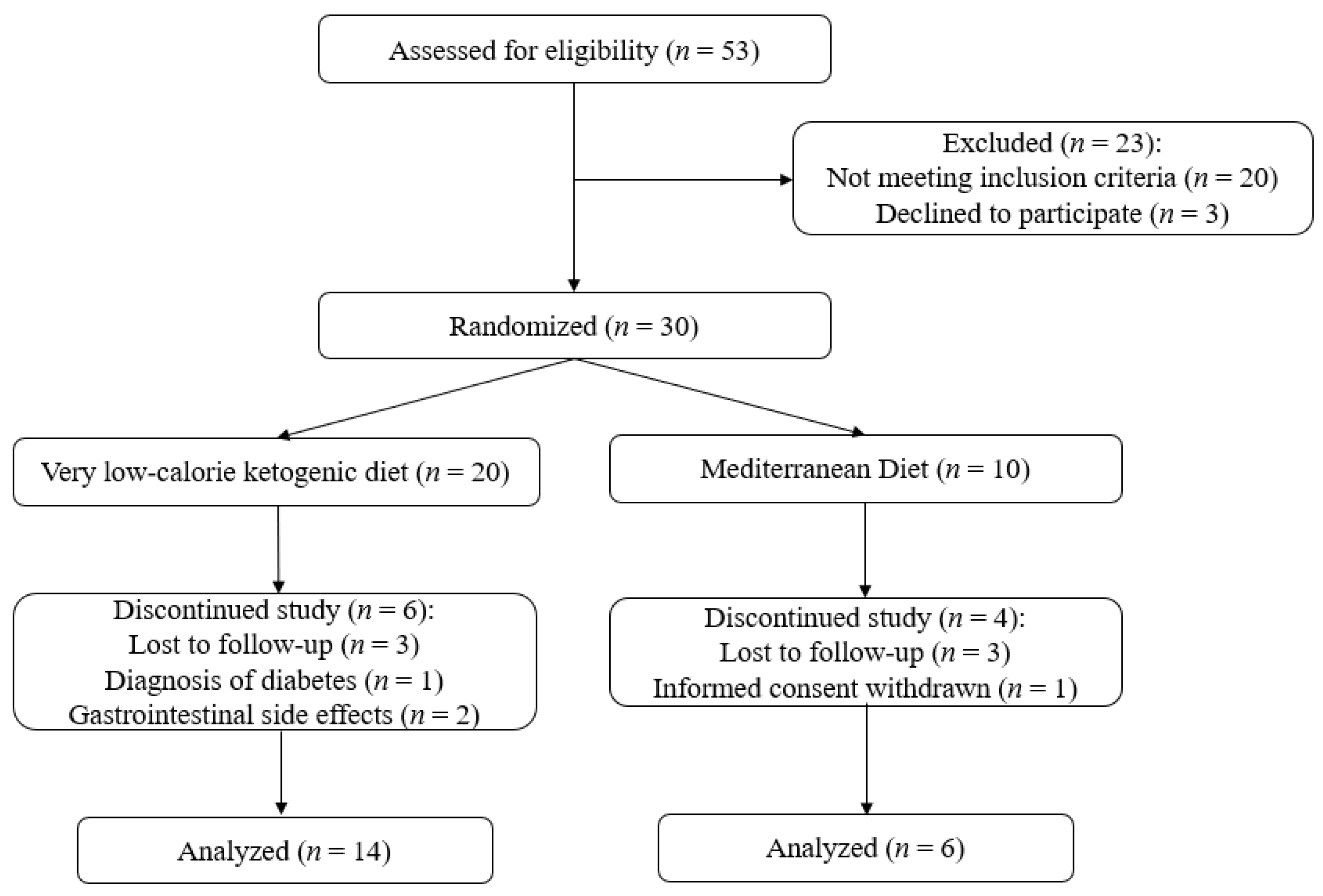
2.2. Study Design and Participants
2.3. Interventions
2.4. Contrast-Enhanced Carotid Ultrasound
2.5. Body Composition, Anthropometric Data, and Quality-of-Life Evaluation
2.6. Laboratory Assessment
2.7. Statistical Analysis
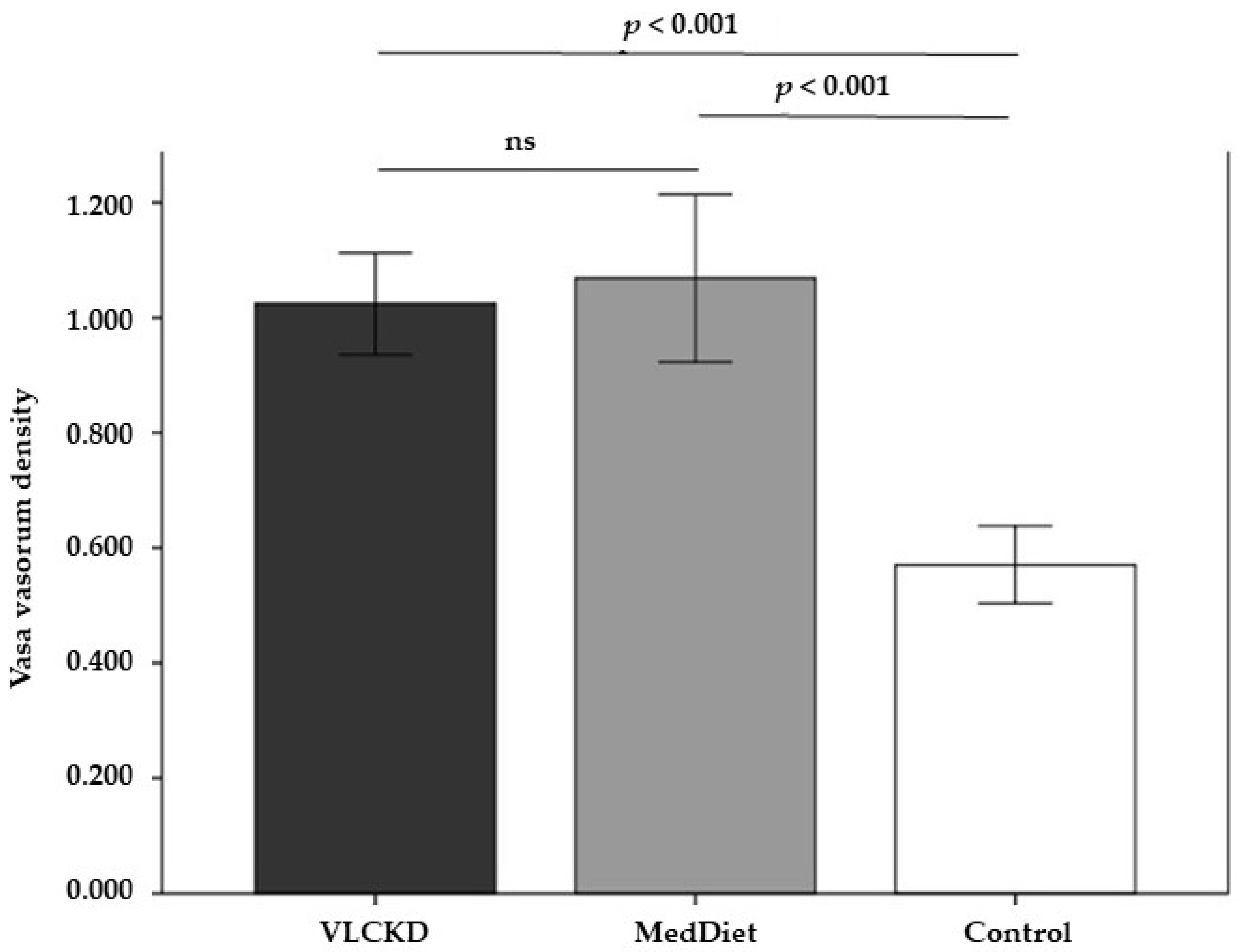
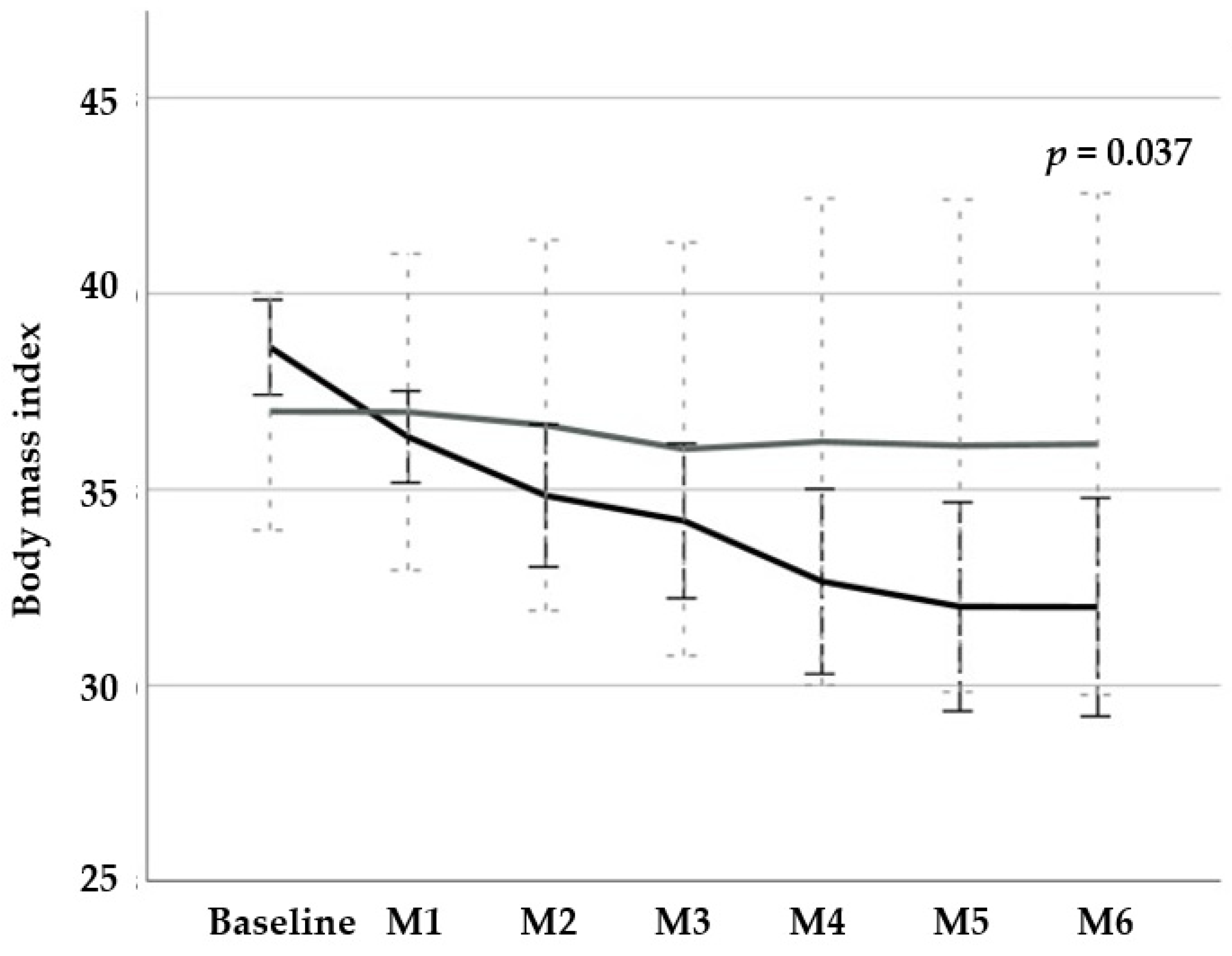
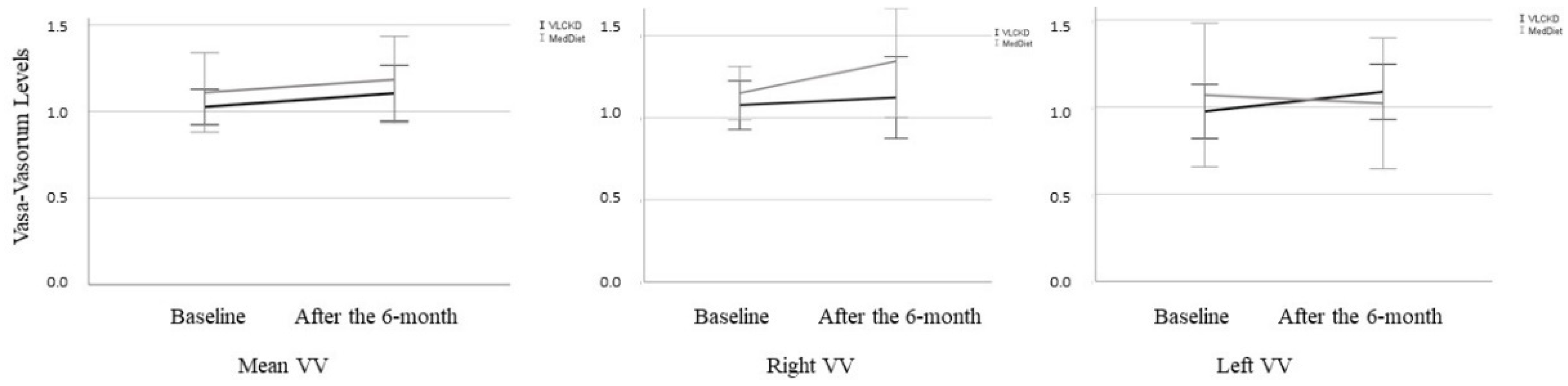
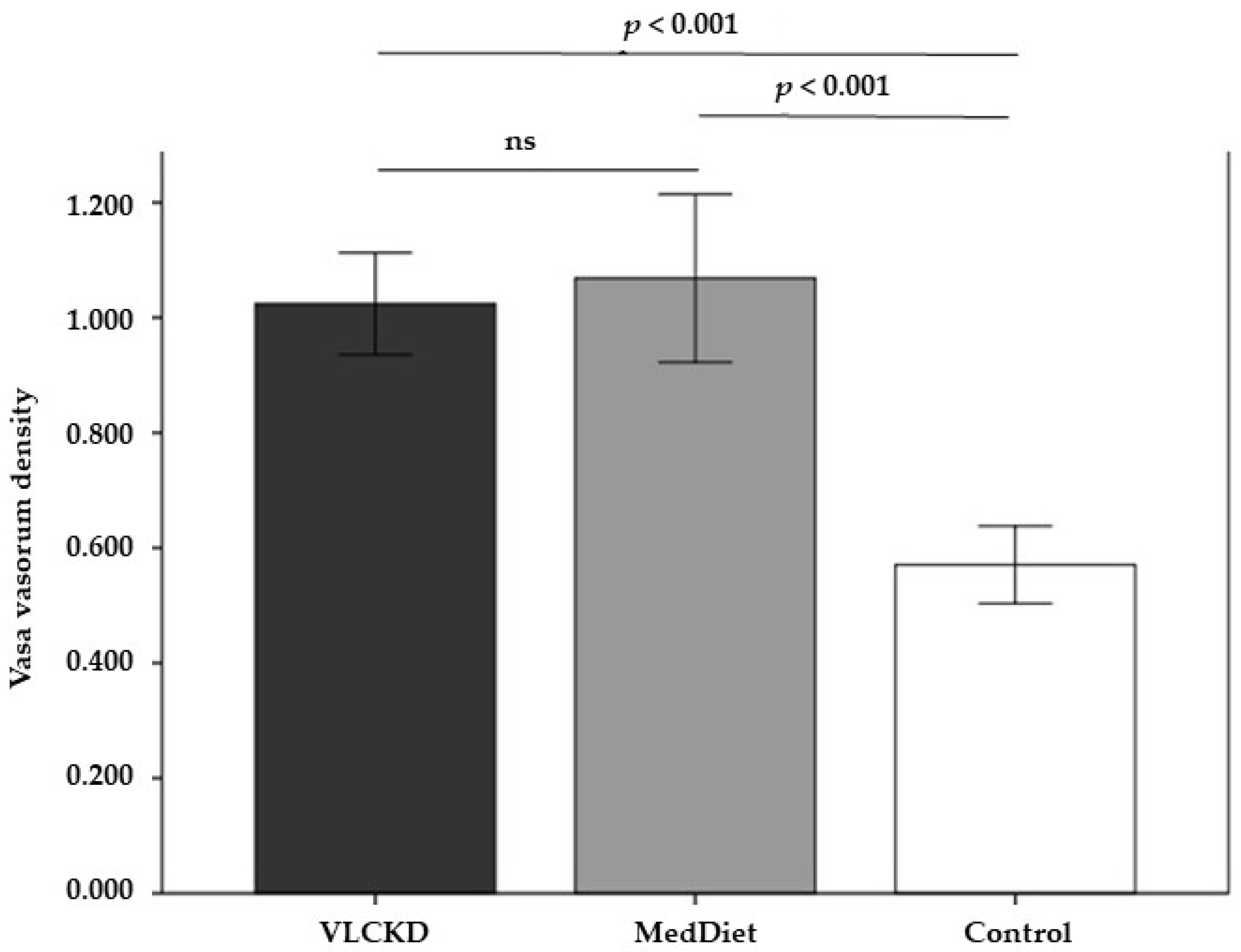
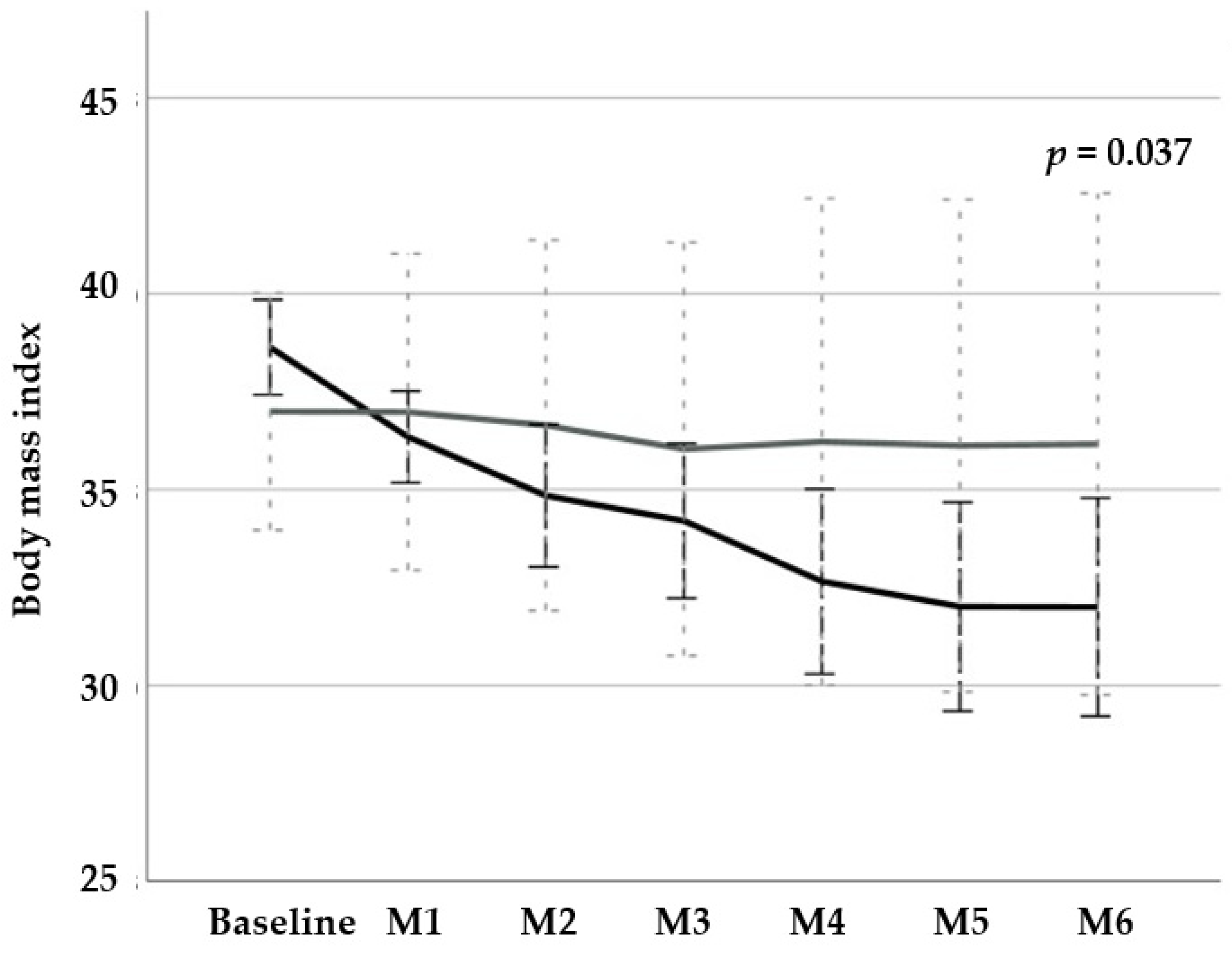
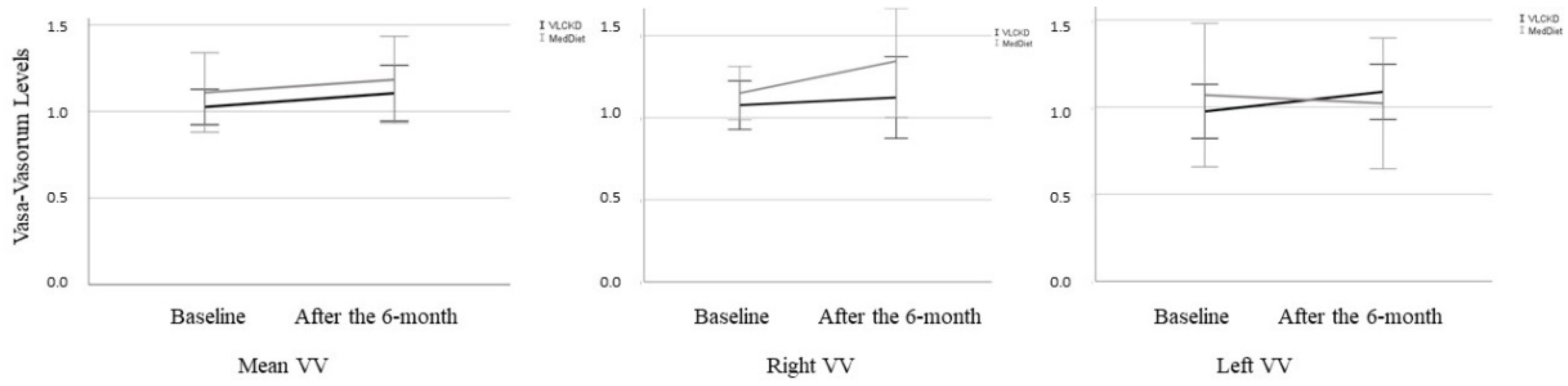
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Inoue, Y.; Qin, B.; Poti, J.; Sokol, R.; Gordon-Larsen, P. Epidemiology of Obesity in Adults: Latest Trends. Curr. Obes. Rep. 2018, 7, 276–288. [Google Scholar] [CrossRef]
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA 2014, 26, 806–814. [Google Scholar] [CrossRef] [Green Version]
- Aranceta-Bartrina, J.; Bartrina, J.A.; Alberdi-Aresti, G.; Ramos-Carrera, N.; Lázaro-Masedo, S. Prevalence of General Obesity and Abdominal Obesity in the Spanish Adult Population (Aged 25–64 Years) 2014–2015: The ENPE Study. Rev. Española Cardiol. 2016, 69, 579–587. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Global Health Observatory Data Repository. Available online: https://www.who.int/features/factfiles/obesity/en/ (accessed on 19 December 2021).
- Nyberg, S.T.; Batty, G.D.; Pentti, J.; Virtanen, M.; Alfredsson, L.; Fransson, E.I. Obesity and loss of disease-free years owing to major non-communicable diseases: A multicohort study. Lancet Public Health 2018, 3, e490–e497. [Google Scholar] [CrossRef] [Green Version]
- NCD Risk Factor Collaboration (NCD-RisC). Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19·2 million participants. Lancet 2016, 2, 1377–1396. [Google Scholar]
- Garcia-Labbé, D.; Ruka, E.; Bertrand, O.F.; Voisine, P.; Costerousse, O.; Poirier, P. Obesity and coronary artery disease: Evaluation and treatment. Can. J. Cardiol. 2015, 31, 184–194. [Google Scholar] [CrossRef] [PubMed]
- Kawabe, J.; Hasebe, N. Role of the vasa vasorum and vascular resident stem cells in atherosclerosis. Biomed. Res. Int. 2014, 2014, 701571. [Google Scholar] [CrossRef]
- Subbotin, V.M. Excessive intimal hyperplasia in human coronary arteries before intimal lipid depositions is the initiation of coronary atherosclerosis and constitutes a therapeutic target. Drug Discov. Today 2016, 21, 1578–1595. [Google Scholar] [CrossRef] [Green Version]
- Sedding, D.G.; Boyle, E.C.; Demandt, J.A.F.; Sluimer, J.C.; Dutzmann, J.; Haverich, A.; Bauersachs, J. Vasa Vasorum Angiogenesis: Key Player in the Initiation and Progression of Atherosclerosis and Potential Target for the Treatment of Cardiovascular Disease. Front. Immunol. 2018, 9, 706. [Google Scholar] [CrossRef] [Green Version]
- Ferns, G.A.A.; Heikal, L. Hypoxia in Atherogenesis. Angiology 2017, 68, 472–493. [Google Scholar] [CrossRef] [PubMed]
- Moreno, P.R.; Purushothaman, K.R.; Fuster, V.; Echeverri, D.; Truszczynska, H.; Sharma, S.K. Plaque neovascularization is increased in ruptured atherosclerotic lesions of human aorta: Implications for plaque vulnerability. Circulation 2004, 110, 2032–2038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rius, F.; Sánchez, E.; Betriu, À.; Baena-Fustegueras, J.A.; Yeramian, A.; Vidal, T.; Hernández, M.; López-Cano, C.; Bueno, M.; Gutiérrez-Carrasquilla, L.; et al. Influence of Morbid Obesity and Bariatric Surgery Impact on the Carotid Adventitial Vasa Vasorum Signal. Obes. Surg. 2018, 28, 3935–3942. [Google Scholar] [CrossRef]
- Trimboli, P.; Castellana, M.; Bellido, D.; Casanueva, F.F. Confusion in the nomenclature of ketogenic diets blurs evidence. Rev. Endocr. Metab. Disord. 2020, 21, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Arbelaez, D.; Bellido, D.; Castro, A.I.; Mayan, L.O.; Carreira, J.; Galban, C.; Olmos, M.; Ángel, M.; Crujeiras, A.B.; Sajoux, I.; et al. Body Composition Changes After Very-Low-Calorie Ketogenic Diet in Obesity Evaluated by 3 Standardized Methods. J. Clin. Endocrinol. Metab. 2017, 102, 488–498. [Google Scholar] [CrossRef] [PubMed]
- Muscogiuri, G.; El Ghoch, M.; Colao, A.; Hassapidou, M.; Yumuk, V.; Busetto, L.; Obesity Management Task Force (OMTF) of the European Association for the Study of Obesity (EASO). European Guidelines for Obesity Management in Adults with a Very Low-Calorie Ketogenic Diet: A Systematic Review and Meta-Analysis. Obes. Facts 2021, 14, 222–245. [Google Scholar] [CrossRef]
- Crosby, L.; Davis, B.; Joshi, S.; Jardine, M.; Paul, J.; Neola, M.; Barnard, N.D. Ketogenic Diets and Chronic Disease: Weighing the Benefits Against the Risks. Front. Nutr. 2021, 8, 702802. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMJ Med. 2010, 8, 18. [Google Scholar]
- Arcidiacono, M.V.; Rubinat, E.; Borràs, M.; Betriu, A.; Trujillano, J.; Vidal, T.; Mauricio, D.; Fernández, E. Left carotid adventitial vasa vasorum signal correlates directly with age and with left carotid intima-media thickness in individuals without atheromatous risk factors. Cardiovasc. Ultrasound 2015, 13, 20. [Google Scholar] [CrossRef] [Green Version]
- de Luis, D.; Domingo, J.C.; Izaola, O.; Casanueva, F.F.; Bellido, D.; Sajoux, I. Effect of DHA supplementation in a very low-calorie ketogenic diet in the treatment of obesity: A randomized clinical trial. Endocrine 2016, 54, 111–122. [Google Scholar] [CrossRef]
- SCOOP-VLCD TASK. Reports on Tasks for Scientific Cooperation. Collection of Data on Products Intendend for Use in Very-Low-Calorie-Diets. Report Brussels European Comission. 2002. Available online: http://www.foodedsoc.org/scoop.pdf (accessed on 18 December 2021).
- Carmona-Maurici, J.; Cuello, E.; Sánchez, E.; Miñarro, A.; Rius, F.; Bueno, M.; de la Fuente, M.C.; Kissler, J.J.O.; Vidal, T.; Maria, V.; et al. Impact of bariatric surgery on subclinical atherosclerosis in patients with morbid obesity. Surg. Obes. Relat. Dis. 2020, 16, 1419–1428. [Google Scholar] [CrossRef]
- Kolotkin, R.L.; Crosby, R.D. Psychometric evaluation of the impact of weight on quality of life-lite questionnaire (IWQOL-lite) in a community sample. Qual. Life Res. 2002, 11, 157–171. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Macías, J.C.; Ochoa-Martínez, A.C.; Varela-Silva, J.A.; Pérez-Maldonado, I.N. Atherogenic Index of Plasma: Novel Predictive Biomarker for Cardiovascular Illnesses. Arch. Med. Res. 2019, 50, 285–294. [Google Scholar] [CrossRef]
- Jin, J.-L.; Cao, Y.-X.; Wu, L.-G.; You, X.-D.; Guo, Y.-L.; Wu, N.-Q.; Zhu, C.-G.; Gao, Y.; Dong, Q.-T.; Zhang, H.-W.; et al. Triglyceride glucose index for predicting cardiovascular outcomes in patients with coronary artery disease. J. Thorac. Dis. 2018, 10, 6137–6146. [Google Scholar] [CrossRef] [PubMed]
- Casanueva, F.F.; Castellana, M.; Bellido, D.; Trimboli, P.; Castro, A.I.; Sajoux, I.; Carnero, M.G.R.; Gomez-Arbelaez, D.; Crujeiras, A.B.; Olmos, M.; et al. Ketogenic diets as treatment of obesity and type 2 diabetes mellitus. Rev. Endocr. Metab. Disord. 2020, 21, 381–397. [Google Scholar] [CrossRef]
- Caprio, M.; Infante, M.; Moriconi, E.; Armani, A.; Fabbri, A.; Mantovani, G.; Mariani, S.; Lubrano, C.; Poggiogalle, E.; Migliaccio, S.; et al. Very-low-calorie ketogenic diet (VLCKD) in the management of metabolic diseases: Systematic review and consensus statement from the Italian Society of Endocrinology (SIE). J. Endocrinol. Investig. 2019, 42, 1365–1386. [Google Scholar] [CrossRef]
- Heistad, D.D.; Marcus, M.L.; Larsen, G.E.; Armstrong, M.L. Role of vasa vasorum in nourishment of the aortic wall. Am. J. Physiol. 1981, 240, H781–H787. [Google Scholar] [CrossRef]
- Xu, J.; Lu, X.; Shi, G.P. Vasa vasorum in atherosclerosis and clinical significance. Int. J. Mol. Sci. 2015, 16, 11574–11608. [Google Scholar] [CrossRef] [Green Version]
- Chatterjee, T.K.; Aronow, B.J.; Tong, W.S.; Manka, D.; Tang, Y.; Bogdanov, V.; Unruh, D.; Blomkalns, A.L.; Piegore, M.G.; Weintraub, D.S.; et al. Human coronary artery perivascular adipocytes overexpress genes responsible for regulating vascular morphology, inflammation, and hemostasis. Physiol. Genom. 2013, 45, 697–709. [Google Scholar] [CrossRef] [Green Version]
- Manka, D.; Chatterjee, T.K.; Stoll, L.L.; Basford, J.E.; Konaniah, E.S.; Srinivasan, R.; Bogdanov, V.Y.; Tang, Y.; Blomkalns, A.L.; Hui, D.Y.; et al. Transplanted perivascular adipose tissue accelerates injury-induced neointimal hyperplasia: Role of monocyte chemoattractant protein-1. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1723–1730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.W.; Shi, H.; Winkler, M.A.; Lee, R.; Weintraub, N.L. Perivascular Adipose Tissue and Vascular Perturbation/Atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 2569–2576. [Google Scholar] [CrossRef]
- López-Cano, C.; Rius, F.; Sánchez, E.; Gaeta, A.M.; Betriu, À.; Fernández, E.; Yeramian, A.; Hernández, M.; Bueno, M.; Gutiérrez-Carrasquilla, L.; et al. The influence of sleep apnea syndrome and intermittent hypoxia in carotid adventitial vasa vasorum. PLoS ONE 2019, 14, e0211742. [Google Scholar] [CrossRef]
- Castellana, M.; Biacchi, E.; Procino, F.; Casanueva, F.F.; Trimboli, P. Very-low-calorie ketogenic diet for the management of obesity, overweight and related disorders. Minerva Endocrinol. 2020, 46, 161–167. [Google Scholar] [CrossRef]
- Castellana, M.; Conte, E.; Cignarelli, A.; Perrini, S.; Giustina, A.; Giovanella, L.; Giorgino, F.; Trimboli, P. Efficacy and safety of very low calorie ketogenic diet (VLCKD) in patients with overweight and obesity: A systematic review and meta-analysis. Rev. Endocr. Metab. Disord. 2020, 21, 5–16. [Google Scholar] [CrossRef]
- Sánchez, M.; Sánchez, E.; Hernández, M.; González, J.; Purroy, F.; Rius, F.; Pamplona, R.; Farràs-Sallés, C.; Gutiérrez-Carrasquilla, L.; Fernández, E.; et al. Dissimilar Impact of a Mediterranean Diet and Physical Activity on Anthropometric Indices: A Cross-Sectional Study from the ILERVAS Project. Nutrients 2019, 11, 1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cunha, G.M.; Guzman, G.; De Mello, L.L.C.; Trein, B.; Spina, L.; Bussade, I.; Prata, J.M.; Sajoux, I.; Countinho, W. Efficacy of a 2-Month Very Low-Calorie Ketogenic Diet (VLCKD) Compared to a Standard Low-Calorie Diet in Reducing Visceral and Liver Fat Accumulation in Patients with Obesity. Front. Endocrinol. 2020, 11, 607. [Google Scholar] [CrossRef]
- Arnold, N.; Lechner, K.; Waldeyer, C.; Shapiro, M.D.; Koenig, W. Inflammation and Cardiovascular Disease: The Future. Eur. Cardiol. 2021, 16, e20. [Google Scholar] [CrossRef] [PubMed]
- Bhanpuri, N.H.; Hallberg, S.J.; Williams, P.T.; McKenzie, A.L.; Ballard, K.D.; Campbell, W.W.; McCarter, J.P.; Phinney, S.D.; Volek, J.S. Cardiovascular disease risk factor responses to a type 2 diabetes care model including nutritional ketosis induced by sustained carbohydrate restriction at 1 year: An open label, non-randomized, controlled study. Cardiovasc. Diabetol. 2018, 17, 56. [Google Scholar] [CrossRef] [Green Version]
- Oppedisano, F.; Macrì, R.; Gliozzi, M.; Musolino, V.; Carresi, C.; Maiuolo, J.; Bosco, F.; Nucera, S.; Zito, M.C.; Guarnieri, L.; et al. The Anti-Inflammatory and Antioxidant Properties of n-3 PUFAs: Their Role in Cardiovascular Protection. Biomedicines 2020, 8, 306. [Google Scholar] [CrossRef]
- Volek, J.S.; Sharman, M.J. Cardiovascular and hormonal aspects of very-low-carbohydrate ketogenic diets. Obes. Res. 2004, 12 (Suppl. S2), 115S–123S. [Google Scholar] [CrossRef]
- Merra, G.; Miranda, R.; Barrucco, S.; Gualtieri, P.; Mazza, M.; Moriconi, E.; Marchetti, M.; Chang, T.F.M.; De Lorenzo, A.; Di Renzo, L. Very-low-calorie ketogenic diet with aminoacid supplement versus very low restricted-calorie diet for preserving muscle mass during weight loss: A pilot double-blind study. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 2613–2621. [Google Scholar] [PubMed]
- Muscaritoli, M.; Anker, S.D.; Argiles, J.; Aversa, Z.; Bauer, J.M.; Biolo, G.I.; Boirie, Y.; Bosaeus, I.; Cederholm, T.; Costelli, P.; et al. Consensus definition of sarcopenia, cachexia and pre-cachexia: Joint document elaborated by special interest groups (SIG) “cachexia-anorexia in chronic wasting diseases” and “nutrition in geriatrics”. Clin. Nutr. 2010, 29, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Santilli, V.; Bernetti, A.; Mangone, M.; Paoloni, M. Clinical definition of sarcopenia. Clin. Cases Miner. Bone Metab. 2014, 11, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Castro, A.I.; Gomez-Arbelaez, D.; Crujeiras, A.B.; Granero, R.; Aguera, Z.; Jimenez-Murcia, S.; Sajoux, I.; Lopez-Jaramillo, P.; Fernandez-Aranda, F.; Casanueva, F.F. Effect of A Very Low-Calorie Ketogenic Diet on Food and Alcohol Cravings, Physical and Sexual Activity, Sleep Disturbances, and Quality of Life in Obese Patients. Nutrients 2018, 10, 1348. [Google Scholar] [CrossRef] [Green Version]
- Forsythe, C.E.; Phinney, S.; Fernandez, M.L.; Quann, E.E.; Wood, R.J.; Bibus, D.M.; Kraemer, W.J.; Feinman, R.D.; Volek, J.S. Comparison of Low Fat and Low Carbohydrate Diets on Circulating Fatty Acid Composition and Markers of Inflammation. Lipids 2007, 43, 65–77. [Google Scholar] [CrossRef] [PubMed]
- Fu, Z.; Zhou, E.; Wang, X.; Tian, M.; Kong, J.; Lingyun, Z.; Jian, K.; Niu, C.; Shen, H.; Dong, S.; et al. Oxidized low-density lipoprotein-induced microparticles promote endothelial monocyte adhesion via intercellular adhesion molecule 1. Am. J. Physiol. Physiol. 2017, 313, C567–C574. [Google Scholar] [CrossRef] [PubMed]
- Tzoulaki, I.; Murray, G.D.; Lee, A.J.; Rumley, A.; Lowe, G.D.O.; Fowkes, F.G.R. C-reactive protein, interleukin- 6, and soluble adhesion molecules as predictors of progressive peripheral atherosclerosis in the general population: Edinburgh artery study. Circulation 2005, 112, 976–983. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, A.D.; Rifai, N.; Ridker, P.M. Soluble intercellular adhesion molecule-1, soluble vascular adhesion molecule-1, and the development of symptomatic peripheral arterial disease in men. Circulation 2002, 106, 820–825. [Google Scholar] [CrossRef] [Green Version]
- D’Abbondanza, M.; Ministrini, S.; Pucci, G.; Migliola, E.N.; Martorelli, E.-E.; Gandolfo, V.; Siepi, D.; Lupattelli, G.; Vaudo, G. Very Low-Carbohydrate Ketogenic Diet for the Treatment of Severe Obesity and Associated Non-Alcoholic Fatty Liver Disease: The Role of Sex Differences. Nutrients 2020, 12, 2748. [Google Scholar] [CrossRef] [PubMed]
- Fielding, R.A.; Vellas, B.; Evans, W.J.; Bhasin, S.; Morley, J.E.; Newman, A.B.; van Kan, G.A.; Andrieu, S.; Bauer, J.; Breuille, D.; et al. Sarcopenia: An undiagnosed condition in older adults—Current consensus definition: Prevalence, etiology, and consequences. International Working Group on Sarcopenia. J. Am. Med. Dir. Assoc. 2011, 12, 249–256. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 601. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| VLCKD (n = 20) | MedDiet (n = 10) | p Value | |
|---|---|---|---|
| Age (years) | 40.7 ± 9.6 | 39.7 ± 9.0 | 0.985 |
| Women, n (%) | 14 (70.0) | 8 (80.0) | 0.834 |
| BMI (kg/m2) | 38.1 ± 1.6 | 37.5 ± 2.5 | 0.284 |
| WC (cm) | 112.4 ± 7.2 | 111.3 ± 10.1 | 0.631 |
| TBF (%) | 42.4 ± 2.9 | 42.0 ± 4.1 | 0.790 |
| FFM (%) | 55.0 ± 5.6 | 56.1 ± 7.5 | 0.572 |
| SBP (mmHg) | 130.1 ± 15.9 | 134.8 ± 17.3 | 0.394 |
| FPG (mmol/L) | 107.0 ± 38.3 | 99.5 ± 14.3 | 0.579 |
| HbA1c (%) | 5.6 ± 1.2 | 5.3 ± 0.3 | 0.504 |
| Total cholesterol (mg/dL) | 192.1 ± 32.2 | 179.8 ± 30.5 | 0.356 |
| c-LDL (mg/dL) | 120.9 ± 30.6 | 110.5 ± 23.0 | 0.387 |
| c-HDL (mg/dL) | 47.5 ± 12.7 | 46.9 ± 14.6 | 0.922 |
| Triglycerides (mg/dL) | 138.7 ± 68.8 | 144.4 ± 72.4 | 0.839 |
| AIP | 0.5 ± 0.2 | 0.7 ± 0.2 | 0.667 |
| TyG index | 8.8 ± 0.4 | 9.1 ± 0.3 | 0.682 |
| Creatinine (mg/dL) | 0.67 ± 0.1 | 0.67 ± 0.2 | 0.964 |
| IWQOL-Lite | 79.0 ± 27.5 | 78.3 ± 35.9 | 0.539 |
| Baseline mean VV | 1.02 ± 0.2 | 1.06 ± 0.2 | 0.557 |
| Baseline right side VV | 1.07 ± 0.2 | 1.15 ± 0.2 | 0.770 |
| Baseline left side VV | 1.00 ± 0.3 | 1.06 ± 0.4 | 0.292 |
| sICAM-1 (ng/mL) | 416.4 ± 110.3 | 385.7 ± 159.3 | 0.527 |
| sVCAM-1 (ng/mL) | 1508.9 ± 201.3 | 1576.8 ± 321.4 | 0.499 |
| Baseline | 6 Months | Mean Difference (95% CI) | p Value | |
|---|---|---|---|---|
| BMI (kg/m2) VLCKD | 38.1 ± 1.6 | 32.8 ± 3.4 | −5.3 (−6.9 to −3.6) | <0.001 |
| BMI (kg/m2) MedDiet | 37.5 ± 2.5 | 37.3 ± 5.5 | −0.1 (−3.8 to 3.5) | 0.932 |
| ΔBMI (kg/m2) | - | - | −5.2 (−2.0 to −8.3) | 0.003 |
| WC (cm) VLCKD | 112.4 ± 7.2 | 93.4 ± 24.8 | −19.0 (−36.6 to −1.4) | 0.037 |
| WC (cm) MedDiet | 111.3 ± 10.1 | 112.2 ± 10.9 | 0.9 (−6.4 to 8.2) | 0.762 |
| ΔWC (cm) | - | - | −19.9 (−41.0 to 1.1) | 0.061 |
| TBF (%) VLCKD | 42.4 ± 2.9 | 35.4 ± 4.8 | −7.0 (−10.7 to −3.3) | 0.003 |
| TBF (%) MedDiet | 42.0 ± 4.1 | 40.7 ± 3.4 | −1.3 (−3.9 to 1.3) | 0.242 |
| ΔTBF (%) | - | - | −5.7 (−10.4 to 1.0) | 0.022 |
| FFM (%) VLCKD | 55.0 ± 5.6 | 51.9 ± 10.5 | −3.1 (−12.0 to 5.8) | 0.438 |
| FFM (%) MedDiet | 56.1 ± 7.5 | 58.2 ± 13.5 | 2.1 (−7.6 to 11.8) | 0.584 |
| ΔFFM (%) | - | - | 5.2 (−7.0 to 17.4) | 0.370 |
| SBP (mmHg) VLCKD | 130.1 ± 15.9 | 125.7 ± 19.9 | −4.4 (−14.1 to 5.2) | 0.304 |
| SBP (mmHg) MedDiet | 134.8 ± 17.3 | 127.5 ± 21.2 | −7.2 (−21.5 to 7.1) | 0.205 |
| ΔSBP (mmHg) | - | - | −2.8 (−11.3 to 16.9) | 0.662 |
| IWQOL-Lite total score VLCKD | 79.0 ± 27.5 | 37.6 ± 4.3 | −41.4 (−75.2 to −7.6) | 0.027 |
| IWQOL-Lite total score MedDiet | 78.3 ± 35.9 | 68.5 ± 29.9 | −9.8 (−29.3 to 9.8) | 0.210 |
| ΔIWQOL-Lite total score | - | - | −31.7 (−66.7 to 3.4) | 0.041 |
| Baseline | 6 Months | Mean Difference (95% CI) | p Value | |
|---|---|---|---|---|
| Mean VV VLCKD | 1.02 ± 0.2 | 1.10 ± 0.3 | 0.1 (−0.1 to 0.2) | 0.306 |
| Mean VV MedDiet | 1.06 ± 0.2 | 1.18 ± 0.2 | 0.1 (−0.1 to 0.2) | 0.204 |
| ΔMean VV | - | - | 0.0 (−0.3 to 0.2) | 0.963 |
| Right VV VLCKD | 1.07 ± 0.2 | 1.12 ± 0.4 | 0.1 (−0.2 to 0.3) | 0.691 |
| Right VV MedDiet | 1.15 ± 0.2 | 1.34 ± 0.3 | 0.2 (−0.2 to 0.5) | 0.207 |
| ΔRight VV | - | - | 0.1 (−0.5 to 0.2) | 0.461 |
| Left VV VLCKD | 1.00 ± 0.3 | 1.01 ± 0.3 | 0.1 (0.1 to −0.3) | 0.259 |
| Left VV MedDiet | 1.06 ± 0.4 | 1.02 ± 0.4 | −0.1 (−0.4 to 0.3) | 0.736 |
| ΔLeft VV | - | - | 0.2 (−0.5 to −0.2) | 0.359 |
| AIP VLCKD | 0.1 ± 0.2 | −0.0 ± 0.2 | 0.2 (−0.3 to −0.0) | 0.029 |
| AIP MedDiet | 0.7 ± 0.2 | 0.5 ± 0.3 | 0.2 (−0.4 to 0.7) | 0.375 |
| ΔAIP | - | - | 0.0 (−0.4 to 0.5) | 0.824 |
| TyG index VLCKD | 8.8 ± 0.4 | 8.4 ± 0.5 | 0.4 (−0.0 to 0.8) | 0.060 |
| TyG index MedDiet | 9.1 ± 0.3 | 8.8 ± 0.6 | 0.3 (−0.7 to 1.4) | 0.395 |
| ΔTyG index | - | - | 0.1 (−0.7 to 0.8) | 0.886 |
| sICAM-1 (ng/mL) VLCKD | 389.7 ± 117.9 | 315.3 ± 74.2 | −74.3 (−108.9 to −36.6) | <0.001 |
| sICAM-1 (ng/mL) MedDiet | 354.8 ± 146.4 | 341.4 ± 111.9 | −13.3 (−53.9 to 27.1) | 0.460 |
| ΔsICAM-1 (ng/mL) | - | - | −60.9 (−115.0 to −6.8) | 0.029 |
| sVCAM-1 (ng/mL) VLCKD | 1457.9 ± 190.7 | 1520.0 ± 178.2 | 62.1 (−41.2 to 165.5) | 0.213 |
| sVCAM-1 (ng/mL) MedDiet | 1651.0 ± 367.6 | 1625.0 ± 332.8 | −26 (−301.6 to 249.6) | 0.818 |
| ΔsVCAM-1 (ng/mL) | - | - | −88.2 (−123.1 to 299.5) | 0.390 |
| Baseline | 6 Months | Mean Difference (95% CI) | p Value | |
|---|---|---|---|---|
| CRI, VLCKD | 4.2 ± 1.0 | 3.6 ± 0.9 | −0.6 (−1.5 to 0.3) | 0.161 |
| CRI, MedDiet | 4.3 ± 0.4 | 4.0 ± 0.7 | −0.3 (−1.3 to 0.6) | 0.329 |
| ΔCRI | - | - | −0.2 (−1.5 to 1.0) | 0.437 |
| AI, VLCKD | 0.4 ± 0.2 | 0.2 ± 0.2 | −0.2 (−0.5 to 0.0) | 0.073 |
| AI, MedDiet | 0.7 ± 0.2 | 0.5 ± 0.3 | −0.2 (−0.7 to 0.3) | 0.375 |
| ΔAI | - | - | 0.0 (−0.4 to 0.3) | 0.824 |
| VLDL VLCKD | 29.3 ± 12.2 | 21.5 ± 7.6 | −7.8 (−14.6 to 0.9) | 0.028 |
| VLDL MedDiet | 39.5 ± 12.0 | 30.4 ± 18.7 | −9.1 (−50.7 to 32.0) | 0.537 |
| ΔVLDL | - | - | 1.2 (−17.4 to 20.0) | 0.887 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez, E.; Santos, M.-D.; Nuñez-Garcia, M.; Bueno, M.; Sajoux, I.; Yeramian, A.; Lecube, A. Randomized Clinical Trial to Evaluate the Morphological Changes in the Adventitial Vasa Vasorum Density and Biological Markers of Endothelial Dysfunction in Subjects with Moderate Obesity Undergoing a Very Low-Calorie Ketogenic Diet. Nutrients 2022, 14, 33. https://doi.org/10.3390/nu14010033
Sánchez E, Santos M-D, Nuñez-Garcia M, Bueno M, Sajoux I, Yeramian A, Lecube A. Randomized Clinical Trial to Evaluate the Morphological Changes in the Adventitial Vasa Vasorum Density and Biological Markers of Endothelial Dysfunction in Subjects with Moderate Obesity Undergoing a Very Low-Calorie Ketogenic Diet. Nutrients. 2022; 14(1):33. https://doi.org/10.3390/nu14010033
Chicago/Turabian StyleSánchez, Enric, Maria-Dolores Santos, Maitane Nuñez-Garcia, Marta Bueno, Ignacio Sajoux, Andree Yeramian, and Albert Lecube. 2022. "Randomized Clinical Trial to Evaluate the Morphological Changes in the Adventitial Vasa Vasorum Density and Biological Markers of Endothelial Dysfunction in Subjects with Moderate Obesity Undergoing a Very Low-Calorie Ketogenic Diet" Nutrients 14, no. 1: 33. https://doi.org/10.3390/nu14010033
APA StyleSánchez, E., Santos, M.-D., Nuñez-Garcia, M., Bueno, M., Sajoux, I., Yeramian, A., & Lecube, A. (2022). Randomized Clinical Trial to Evaluate the Morphological Changes in the Adventitial Vasa Vasorum Density and Biological Markers of Endothelial Dysfunction in Subjects with Moderate Obesity Undergoing a Very Low-Calorie Ketogenic Diet. Nutrients, 14(1), 33. https://doi.org/10.3390/nu14010033