
Effects of Acute Resistance Exercise with and without Whole-Body Electromyostimulation and Endurance Exercise on the Postprandial Glucose Regulation in Patients with Type 2 Diabetes Mellitus: A Randomized Crossover Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
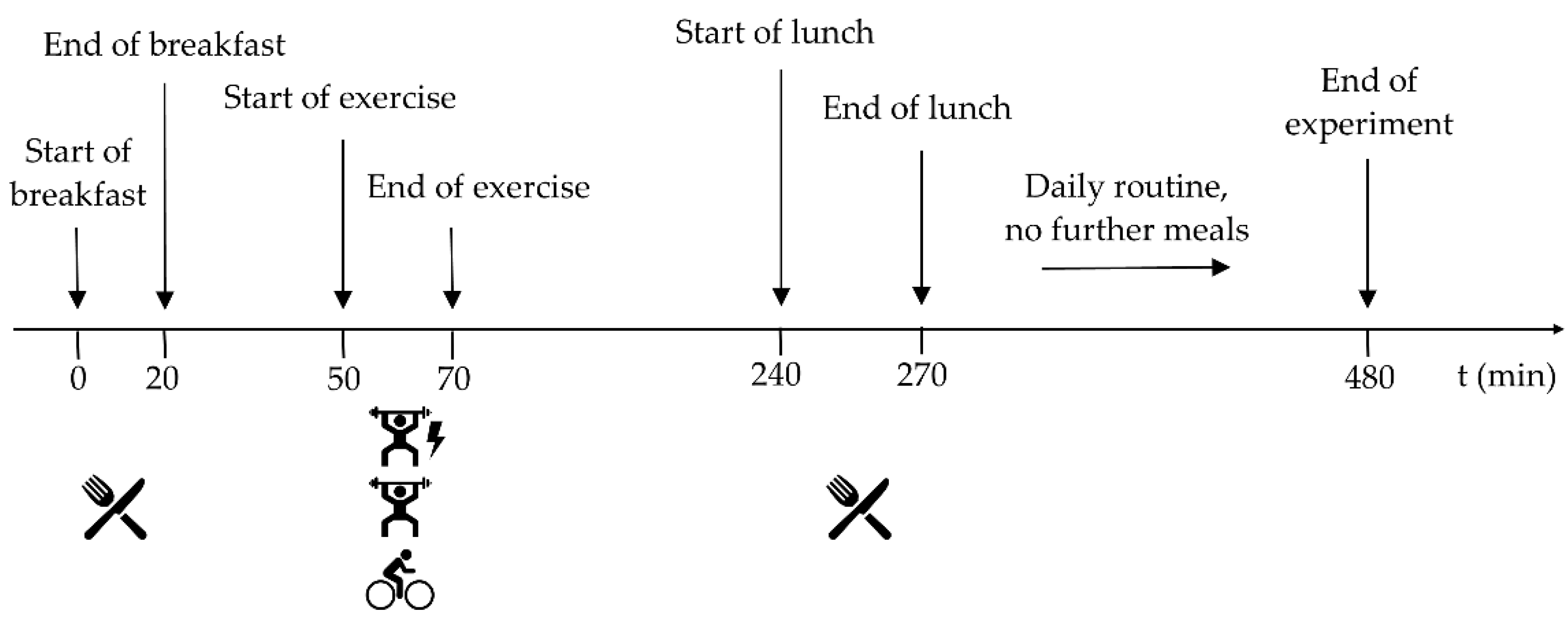
2.3. Experimental Procedure
2.4. Exercise Sessions
2.5. Continuous Glucose Monitoring
2.6. Questionnaire
2.7. Data Analysis
3. Results
3.1. Subjects’ Characteristics
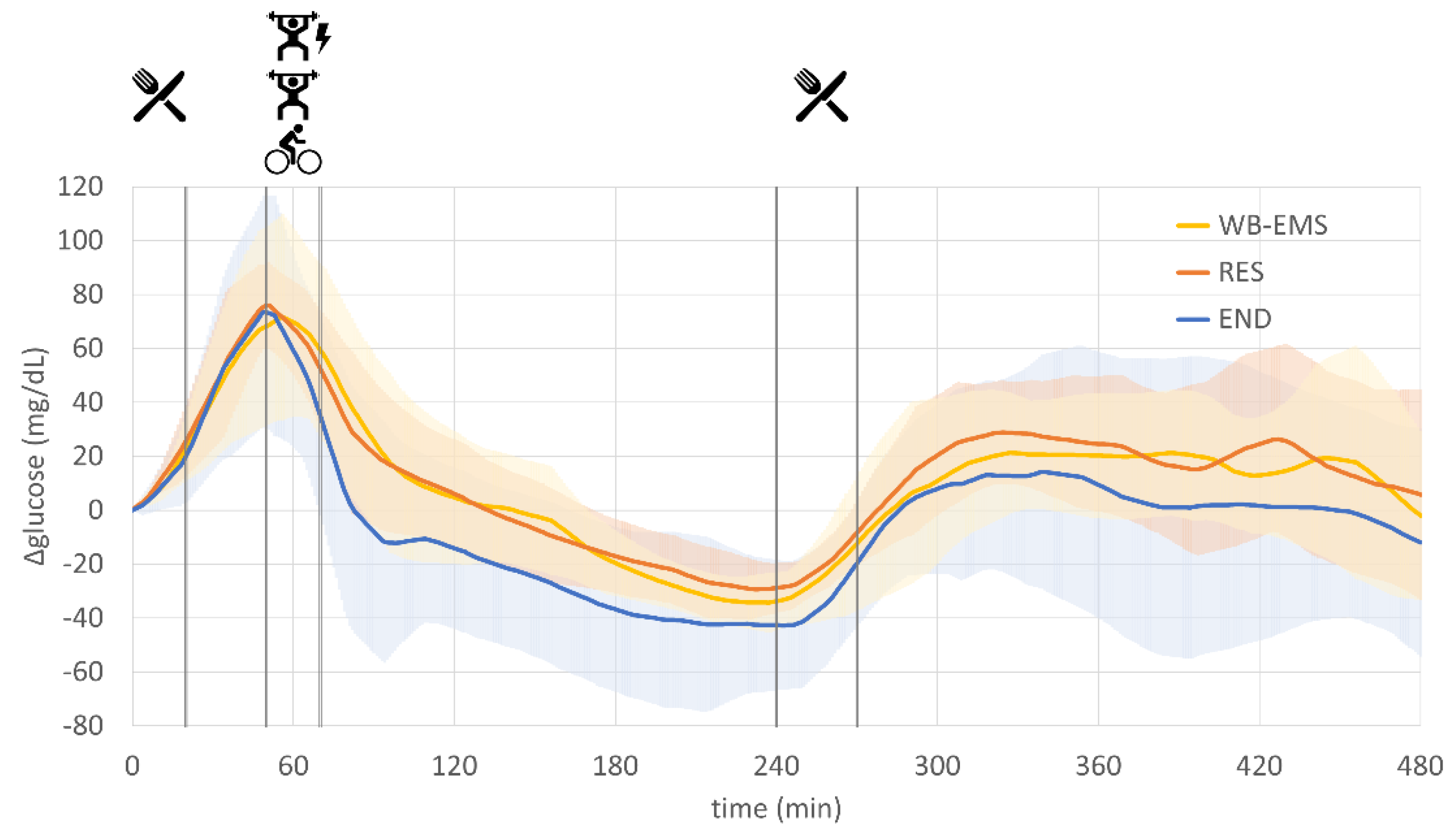
3.2. Glucose Profiles
3.3. Time to Baseline (TTB)
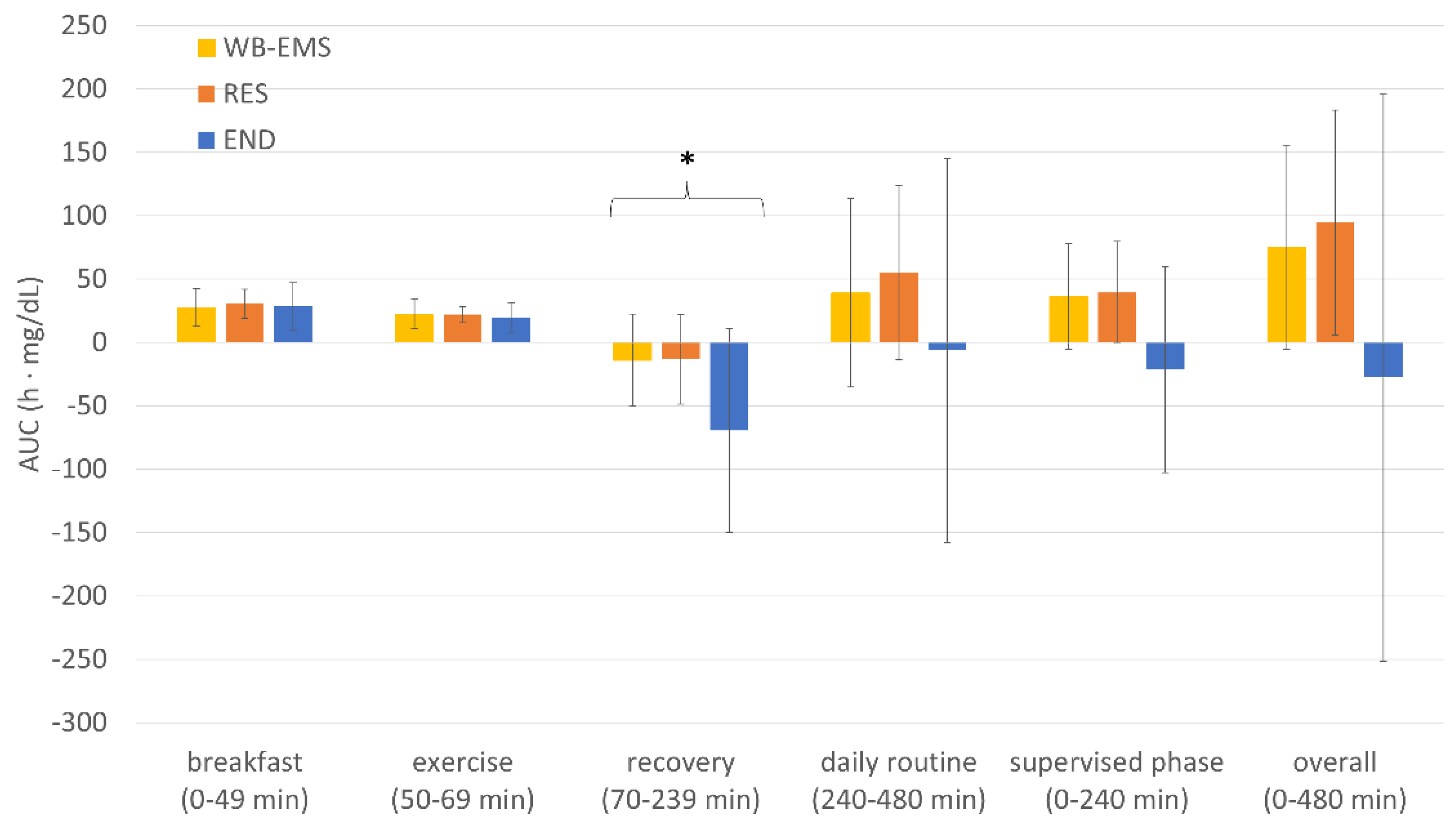
3.4. AUC Analyses
3.5. Time in/above/below Range (TIR, TAR, TBR)
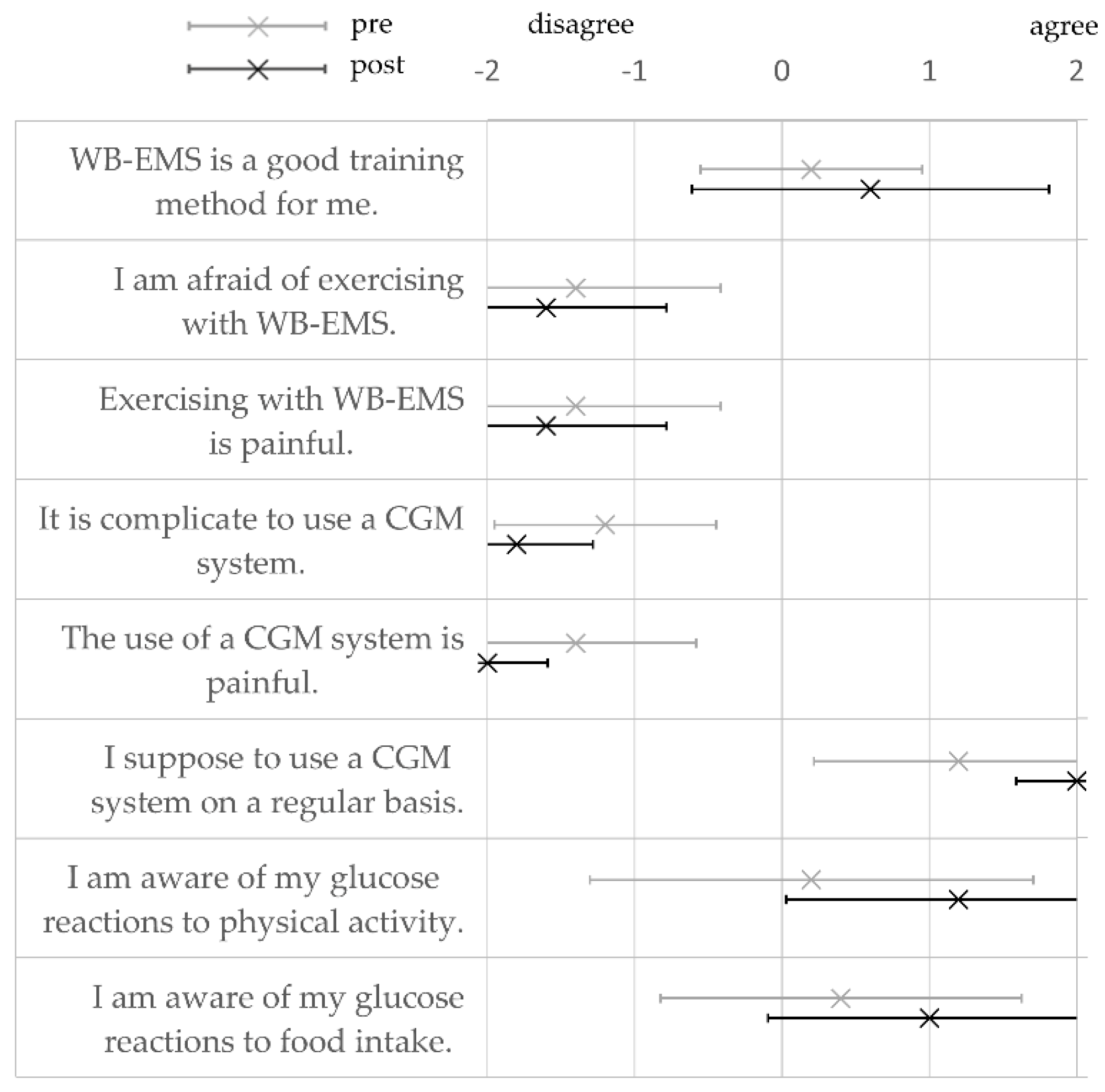
3.6. Questionnaire
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas, 8th ed.; International Diabetes Federation: Brussels, Belgium, 2017. [Google Scholar]
- Jaacks, L.M.; Siegel, K.R.; Gujral, U.P.; Narayan, K.V. Type 2 diabetes: A 21st century epidemic. Best Pract. Res. Clin. Endocrinol. Metab. 2016, 30, 331–343. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association 5. Lifestyle Management: Standards of Medical Care in Diabetes—2019. Diabetes Care 2018, 42, S46–S60. [Google Scholar] [CrossRef]
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical Activity/Exercise and Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef] [PubMed]
- Stanford, K.I.; Goodyear, L.J. Exercise and type 2 diabetes: Molecular mechanisms regulating glucose uptake in skeletal muscle. Adv. Physiol. Educ. 2014, 38, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, A.L.; Philp, A.; Harrison, M.; Bone, A.J.; Watt, P.W. Monitoring Exercise-Induced Changes in Glycemic Control in Type 2 Diabetes. Med. Sci. Sports Exerc. 2006, 38, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Korkiakangas, E.E.; Alahuhta, M.A.; Laitinen, J.H. Barriers to regular exercise among adults at high risk or diagnosed with type 2 diabetes: A systematic review. Health Promot. Int. 2009, 24, 416–427. [Google Scholar] [CrossRef]
- Lidegaard, L.P.; Schwennesen, N.; Willaing, I.; Faerch, K. Barriers to and motivators for physical activity among people with Type 2 diabetes: Patients’ perspectives. Diabet. Med. 2016, 33, 1677–1685. [Google Scholar] [CrossRef]
- Filipovic, A.; Kleinöder, H.; Dörmann, U.; Mester, J. Electromyostimulation—A Systematic Review of the Effects of Different Electromyostimulation Methods on Selected Strength Parameters in Trained and Elite Athletes. J. Strength Cond. Res. 2012, 26, 2600–2614. [Google Scholar] [CrossRef]
- Kemmler, W.; Weissenfels, A.; Willert, S.; Shojaa, M.; Von Stengel, S.; Filipovic, A.; Kleinöder, H.; Berger, J.; Fröhlich, M. Efficacy and Safety of Low Frequency Whole-Body Electromyostimulation (WB-EMS) to Improve Health-Related Outcomes in Non-athletic Adults. A Systematic Review. Front. Physiol. 2018, 9, 573. [Google Scholar] [CrossRef]
- Bax, L.; Staes, F.; Verhagen, A. Does Neuromuscular Electrical Stimulation Strengthen the Quadriceps Femoris? Sports Med. 2005, 35, 191–212. [Google Scholar] [CrossRef]
- Paillard, T. Combined Application of Neuromuscular Electrical Stimulation and Voluntary Muscular Contractions. Sports Med. 2008, 38, 161–177. [Google Scholar] [CrossRef]
- Kemmler, W.; Teschler, M.; Bebenek, M.; Von Stengel, S. Hohe Kreatinkinase-Werte nach exzessiver Ganzkörper-Elektromyostimulation: Gesundheitliche Relevanz und Entwicklung im Trainingsverlauf. Wien. Med. Wochenschr. 2015, 165, 427–435. [Google Scholar] [CrossRef]
- Stöllberger, C.; Finsterer, J. Side effects of whole-body electro-myo-stimulation. Wien. Med. Wochenschr. 2018, 169, 173–180. [Google Scholar] [CrossRef]
- Brancaccio, P.; Maffulli, N.; Limongelli, F.M. Creatine kinase monitoring in sport medicine. Br. Med. Bull. 2007, 81–82, 209–230. [Google Scholar] [CrossRef]
- Kemmler, W.; Froehlich, M.; Von Stengel, S.; Kleinöder, H. Whole-Body Electromyostimulation—The Need for Common Sense! Rationale and Guideline for a Safe and Effective Training. Dtsch. Z. Für Sportmed. /Ger. J. Sports Med. 2016, 2016, 218–221. [Google Scholar] [CrossRef]
- Kemmler, W.; Weissenfels, A.; Willert, S.; Fröhlich, M.; Ludwig, O.; Berger, J.; Zart, S.; Becker, S.; Backfisch, M.; Kleinöder, H.; et al. Recommended Contraindications for the Use of Non-Medical WB-Electromyostimulation. Dtsch. Z. Für Sportmed. /Ger. J. Sports Med. 2019, 70, 278–282. [Google Scholar] [CrossRef]
- Brinkmann, C.; Weh-Gray, O.; Brixius, K.; Bloch, W.; Predel, H.-G.; Kreutz, T. Effects of exercising before breakfast on the health of T2DM patients—A randomized controlled trial. Scand. J. Med. Sci. Sports 2019, 29, 1930–1936. [Google Scholar] [CrossRef]
- Ajjan, R.A.; Cummings, M.H.; Jennings, P.; Leelarathna, L.; Rayman, G.; Wilmot, E.G. Accuracy of flash glucose monitoring and continuous glucose monitoring technologies: Implications for clinical practice. Diabetes Vasc. Dis. Res. 2018, 15, 175–184. [Google Scholar] [CrossRef]
- Heinemann, L.; Schoemaker, M.; Schmelzeisen-Redecker, G.; Hinzmann, R.; Kassab, A.; Freckmann, G.; Reiterer, F.; Del Re, L. Benefits and Limitations of MARD as a Performance Parameter for Continuous Glucose Monitoring in the Interstitial Space. J. Diabetes Sci. Technol. 2019, 14, 135–150. [Google Scholar] [CrossRef]
- Filipovic, A.; Kleinöder, H.; Dörmann, U.; Mester, J. Electromyostimulation—A Systematic Review of the Influence of Training Regimens and Stimulation Parameters on Effectiveness in Electromyostimulation Training of Selected Strength Parameters. J. Strength Cond. Res. 2011, 25, 3218–3238. [Google Scholar] [CrossRef]
- De Nardi, A.T.; Tolves, T.; Lenzi, T.L.; Signori, L.U.; da Silva, A.M.V. High-intensity interval training versus continuous training on physiological and metabolic variables in prediabetes and type 2 diabetes: A meta-analysis. Diabetes Res. Clin. Pract. 2018, 137, 149–159. [Google Scholar] [CrossRef]
- Ramos, J.; Dalleck, L.C.; Tjonna, A.E.; Beetham, K.; Coombes, J.S. The Impact of High-Intensity Interval Training Versus Moderate-Intensity Continuous Training on Vascular Function: A Systematic Review and Meta-Analysis. Sports Med. 2015, 45, 679–692. [Google Scholar] [CrossRef]
- Hoss, U.; Budiman, E. Factory-Calibrated Continuous Glucose Sensors: The Science behind the Technology. Diabetes Technol. Ther. 2017, 19, S-44. [Google Scholar] [CrossRef]
- Le Floch, J.-P.; Escuyer, P.; Baudin, E.; Baudon, D.; Perlemuter, L. Blood Glucose Area Under the Curve: Methodological Aspects. Diabetes Care 1990, 13, 172–175. [Google Scholar] [CrossRef]
- Battelino, T.; Danne, T.; Bergenstal, R.M.; Amiel, S.A.; Beck, R.; Biester, T.; Bosi, E.; Buckingham, B.A.; Cefalu, W.T.; Close, K.L.; et al. Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Recommendations From the International Consensus on Time in Range. Diabetes Care 2019, 42, 1593–1603. [Google Scholar] [CrossRef]
- Beck, R.W.; Bergenstal, R.M.; Riddlesworth, T.D.; Kollman, C.; Li, Z.; Brown, A.S.; Close, K.L. Validation of Time in Range as an Outcome Measure for Diabetes Clinical Trials. Diabetes Care 2018, 42, 400–405. [Google Scholar] [CrossRef]
- Borror, A.; Zieff, G.; Battaglini, C.; Stoner, L. The Effects of Postprandial Exercise on Glucose Control in Individuals with Type 2 Diabetes: A Systematic Review. Sports Med. 2018, 48, 1479–1491. [Google Scholar] [CrossRef]
- van Dijk, J.-W.; Manders, R.J.F.; Tummers, K.; Bonomi, A.G.; Stehouwer, C.D.A.; Hartgens, F.; van Loon, L.J.C. Both resistance- and endurance-type exercise reduce the prevalence of hyperglycaemia in individuals with impaired glucose tolerance and in insulin-treated and non-insulin-treated type 2 diabetic patients. Diabetologia 2011, 55, 1273–1282. [Google Scholar] [CrossRef]
- Hamada, T.; Hayashi, T.; Kimura, T.; Nakao, K.; Moritani, T. Electrical stimulation of human lower extremities enhances energy consumption, carbohydrate oxidation, and whole body glucose uptake. J. Appl. Physiol. 2004, 96, 911–916. [Google Scholar] [CrossRef]
- Richter, E.A.; Hargreaves, M. Exercise, GLUT4, and Skeletal Muscle Glucose Uptake. Physiol. Rev. 2013, 93, 993–1017. [Google Scholar] [CrossRef]
- Jabbour, G.; Belliveau, L.; Probizanski, D.; Newhouse, I.; McAuliffe, J.; Jakobi, J.; Johnson, M. Effect of Low Frequency Neuromuscular Electrical Stimulation on Glucose Profile of Persons with Type 2 Diabetes: A Pilot Study. Diabetes Metab. J. 2015, 39, 264–267. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Miyamoto, T.; Fukuda, K.; Kimura, T.; Matsubara, Y.; Tsuda, K.; Moritani, T.; Miyamoto, T.; Fukuda, K.; Kimura, T.; Matsubara, Y.; et al. Effect of percutaneous electrical muscle stimulation on postprandial hyperglycemia in type 2 diabetes. Diabetes Res. Clin. Pract. 2012, 96, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Joubert, M.; Métayer, L.; Prévost, G.; Morera, J.; Rod, A.; Cailleux, A.; Parienti, J.-J.; Reznik, Y. Neuromuscular electrostimulation and insulin sensitivity in patients with type 2 diabetes: The ELECTRODIAB pilot study. Acta Diabetol. 2014, 52, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Crowe, L.; Caulfield, B. Aerobic neuromuscular electrical stimulation—an emerging technology to improve haemoglobin A1c in type 2 diabetes mellitus: Results of a pilot study. BMJ Open 2012, 2, e000219. [Google Scholar] [CrossRef]
- Giggins, O.M.; Crowe, L.; Coughlan, G.F.; Caulfield, B. Neuromuscular electrical stimulation exercise: A potential alternative to conventional exercise in the management of type 2 diabetes. Br. J. Diabetes Vasc. Dis. 2017, 17, 46–51. [Google Scholar] [CrossRef]
- Rose, B.; Lankisch, M.; Herder, C.; Röhrig, K.; Kempf, K.; Labrenz, S.; Hänsler, J.; Koenig, W.; Heinemann, L.; Martin, S. Beneficial Effects of External Muscle Stimulation on Glycaemic Control in Patients with Type 2 Diabetes. Exp. Clin. Endocrinol. Diabetes 2008, 116, 577–581. [Google Scholar] [CrossRef]
- Van Buuren, F.; Horstkotte, D.; Mellwig, K.P.; Fründ, A.; Vlachojannis, M.; Bogunovic, N.; Dimitriadis, Z.; Vortherms, J.; Humphrey, R.; Niebauer, J. Electrical Myostimulation (EMS) Improves Glucose Metabolism and Oxygen Uptake in Type 2 Diabetes Mellitus Patients—Results from the EMS Study. Diabetes Technol. Ther. 2015, 17, 413–419. [Google Scholar] [CrossRef]
- Wahl, P.; Hein, M.; Achtzehn, S.; Bloch, W.; Mester, J. Acute metabolic, hormonal and psychological responses to cycling with superimposed electromyostimulation. Graefe’s Arch. Clin. Exp. Ophthalmol. 2014, 114, 2331–2339. [Google Scholar] [CrossRef]
- Kuo, T.; McQueen, A.; Chen, T.-C.; Wang, J.-C. Regulation of Glucose Homeostasis by Glucocorticoids. In Advances in Experimental Medicine and Biology; Springer: Berlin/Heidelberg, Germany, 2015; Volume 872, pp. 99–126. [Google Scholar]
- Bellini, A.; Nicolò, A.; Bulzomì, R.; Bazzucchi, I.; Sacchetti, M. The Effect of Different Postprandial Exercise Types on Glucose Response to Breakfast in Individuals with Type 2 Diabetes. Nutrients 2021, 13, 1440. [Google Scholar] [CrossRef]
- Bacchi, E.; Negri, C.; Trombetta, M.; Zanolin, M.E.; Lanza, M.; Bonora, E.; Moghetti, P. Differences in the Acute Effects of Aerobic and Resistance Exercise in Subjects with Type 2 Diabetes: Results from the RAED2 Randomized Trial. PLoS ONE 2012, 7, e49937. [Google Scholar] [CrossRef]
- Asano, R.Y. Acute effects of physical exercise in type 2 diabetes: A review. World J. Diabetes 2014, 5, 659–665. [Google Scholar] [CrossRef]
- Jensen, T.E.; Richter, E.A. Regulation of glucose and glycogen metabolism during and after exercise. J. Physiol. 2012, 590, 1069–1076. [Google Scholar] [CrossRef]
- Maarbjerg, S.J.; Sylow, L.; Richter, E.A. Current understanding of increased insulin sensitivity after exercise—Emerging candidates. Acta Physiol. 2011, 202, 323–335. [Google Scholar] [CrossRef]
- Bweir, S.; Al-Jarrah, M.; Almalty, A.-M.; Maayah, M.; Smirnova, I.V.; Novikova, L.; Stehno-Bittel, L. Resistance exercise training lowers HbA1c more than aerobic training in adults with type 2 diabetes. Diabetol. Metab. Syndr. 2009, 1, 27. [Google Scholar] [CrossRef]
- Maiorino, M.I.; Signoriello, S.; Maio, A.; Chiodini, P.; Bellastella, G.; Scappaticcio, L.; Longo, M.; Giugliano, D.; Esposito, K. Effects of Continuous Glucose Monitoring on Metrics of Glycemic Control in Diabetes: A Systematic Review with Meta-analysis of Randomized Controlled Trials. Diabetes Care 2020, 43, 1146–1156. [Google Scholar] [CrossRef]
- Poole, R.B.; Harrold, C.P.; Burridge, J.H.; Byrne, C.D.; Holt, R.I.G. Electrical muscle stimulation acutely mimics exercise in neurologically intact individuals but has limited clinical benefits in patients with type 2 diabetes. Diabetes, Obes. Metab. 2004, 7, 344–351. [Google Scholar] [CrossRef]
- Manders, R.J.F.; van Dijk, J.-W.; van Loon, L.J. Low-Intensity Exercise Reduces the Prevalence of Hyperglycemia in Type 2 Diabetes. Med. Sci. Sports Exerc. 2010, 42, 219–225. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Phase | Interval | Start | End |
|---|---|---|---|
| breakfast | 0–49 min | beginning of experiment | start of exercise |
| exercise | 50–69 min | start of exercise | end of exercise |
| recovery | 70–239 min | end of exercise | start of lunch |
| daily routine | 240–480 min | start of lunch | end of experiment |
| supervised phase | 0–240 min | beginning of experiment | start of lunch |
| overall | 0–480 min | beginning of experiment | end of experiment |
| Anthropometric Data | Metabolic Variables | ||
|---|---|---|---|
| age (years) | 55.2 ± 7.5 | HbA1c (%) | 7.1 ± 0.5 |
| height (cm) | 175.4 ± 5.9 | fasting blood glucose (mg/dL) | 169.0 ± 49.3 |
| weight (kg) | 100.2 ± 21.6 | total cholesterol (mg/dL) | 202.5 ± 53.1 |
| BMI (kg/m2) | 32.7 ± 7.6 | LDL (mg/dL) | 117.8 ± 48.4 |
| HDL (mg/dL) | 48.5 ± 10.8 | ||
| triglycerides (mg/dL) | 208.7 ± 84.3 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holzer, R.; Schulte-Körne, B.; Seidler, J.; Predel, H.-G.; Brinkmann, C. Effects of Acute Resistance Exercise with and without Whole-Body Electromyostimulation and Endurance Exercise on the Postprandial Glucose Regulation in Patients with Type 2 Diabetes Mellitus: A Randomized Crossover Study. Nutrients 2021, 13, 4322. https://doi.org/10.3390/nu13124322
Holzer R, Schulte-Körne B, Seidler J, Predel H-G, Brinkmann C. Effects of Acute Resistance Exercise with and without Whole-Body Electromyostimulation and Endurance Exercise on the Postprandial Glucose Regulation in Patients with Type 2 Diabetes Mellitus: A Randomized Crossover Study. Nutrients. 2021; 13(12):4322. https://doi.org/10.3390/nu13124322
Chicago/Turabian StyleHolzer, Roman, Benedikt Schulte-Körne, Jan Seidler, Hans-Georg Predel, and Christian Brinkmann. 2021. "Effects of Acute Resistance Exercise with and without Whole-Body Electromyostimulation and Endurance Exercise on the Postprandial Glucose Regulation in Patients with Type 2 Diabetes Mellitus: A Randomized Crossover Study" Nutrients 13, no. 12: 4322. https://doi.org/10.3390/nu13124322
APA StyleHolzer, R., Schulte-Körne, B., Seidler, J., Predel, H.-G., & Brinkmann, C. (2021). Effects of Acute Resistance Exercise with and without Whole-Body Electromyostimulation and Endurance Exercise on the Postprandial Glucose Regulation in Patients with Type 2 Diabetes Mellitus: A Randomized Crossover Study. Nutrients, 13(12), 4322. https://doi.org/10.3390/nu13124322