
Effect of Polyphenol-Rich Foods, Juices, and Concentrates on Recovery from Exercise Induced Muscle Damage: A Systematic Review and Meta-Analysis

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Study Selection
2.4. Data Extraction
2.5. Risk of Bias in Individual Studies
2.6. Data Synthesis
2.7. Quality Assessment
3. Results
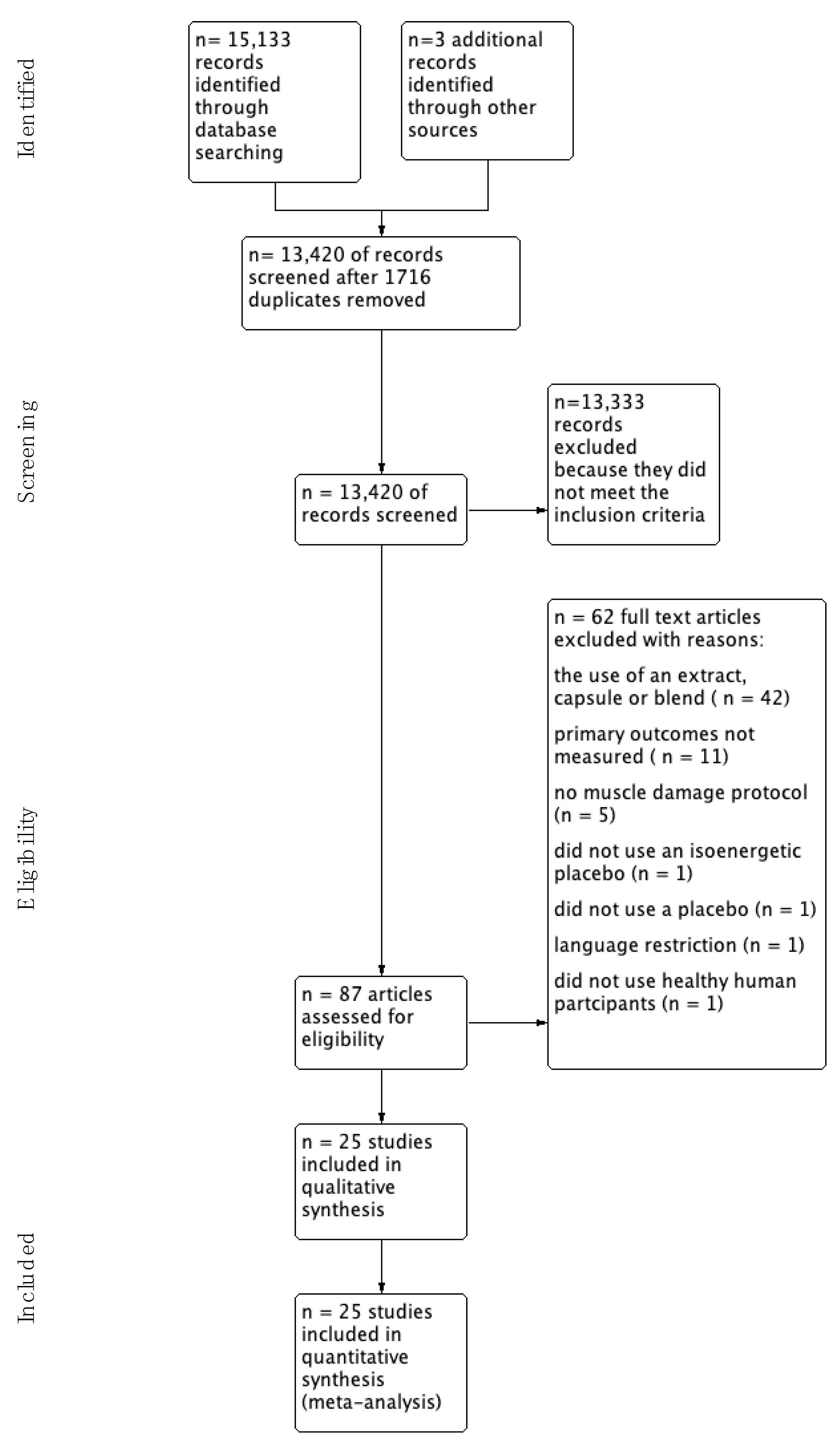
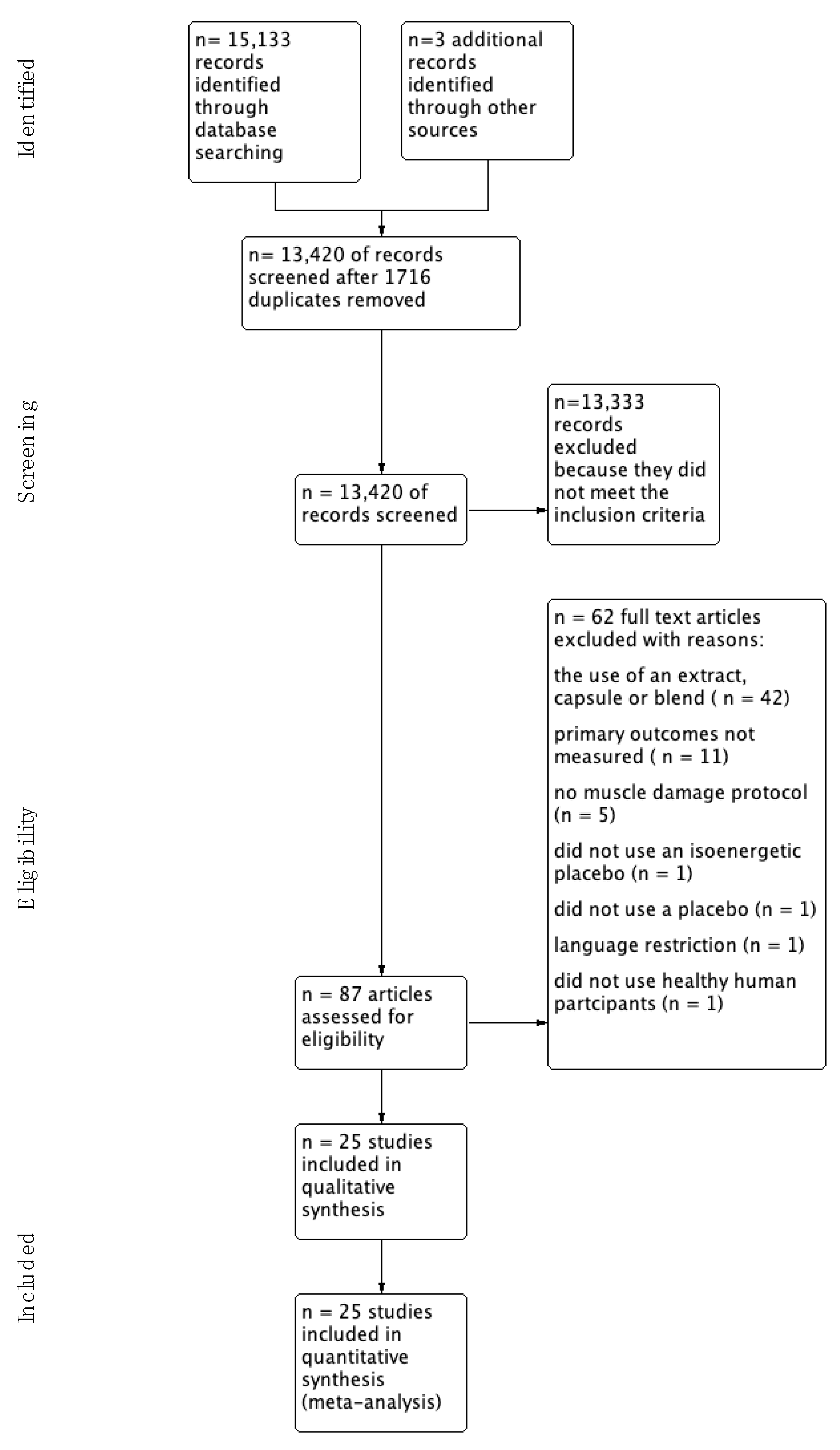
3.1. Study Selection
3.2. Study Characteristics
3.2.1. Methods
3.2.2. Participants
3.2.3. Intervention
3.2.4. Adverse Events
3.3. Outcomes
3.3.1. Primary
3.3.2. Secondary
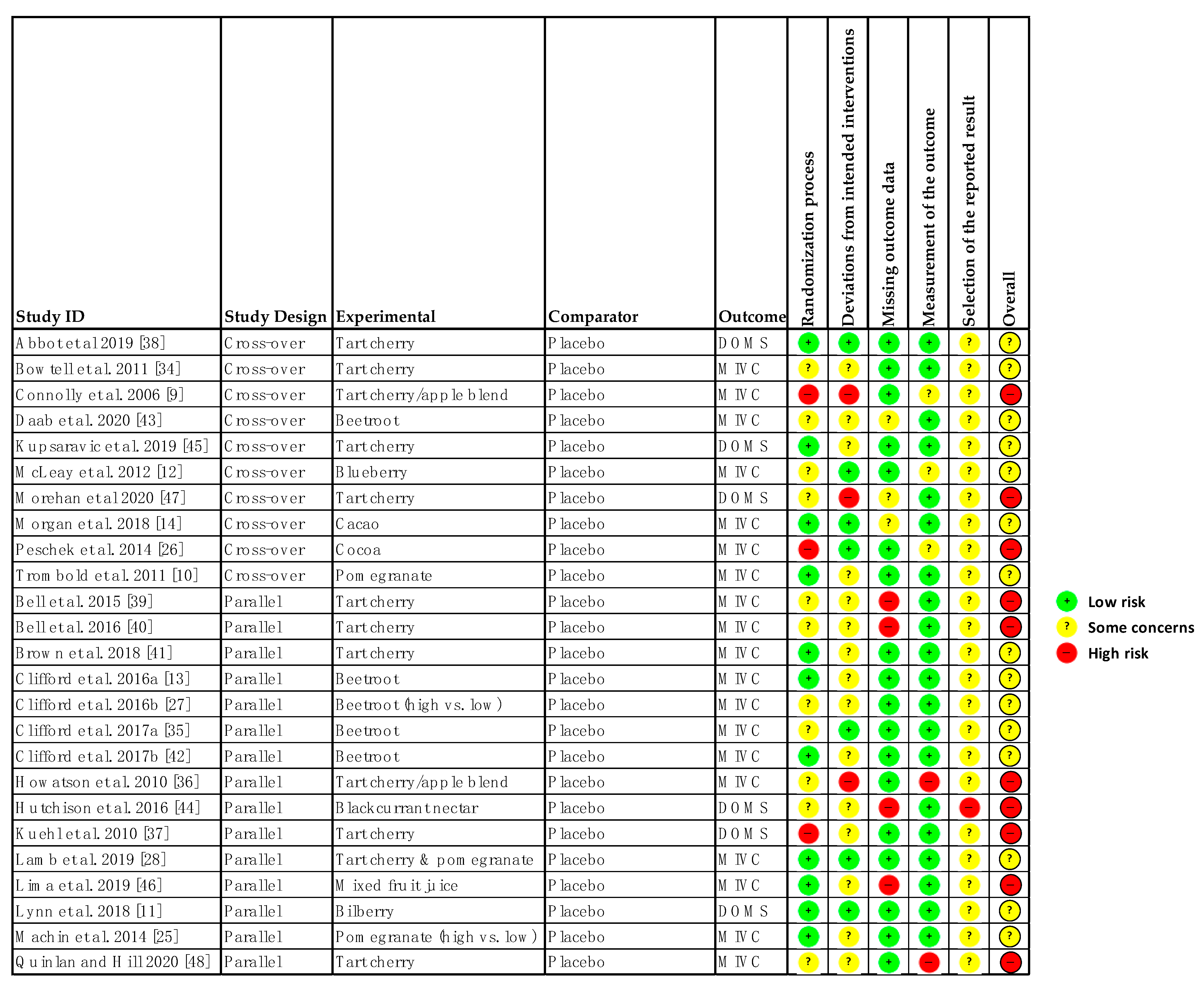
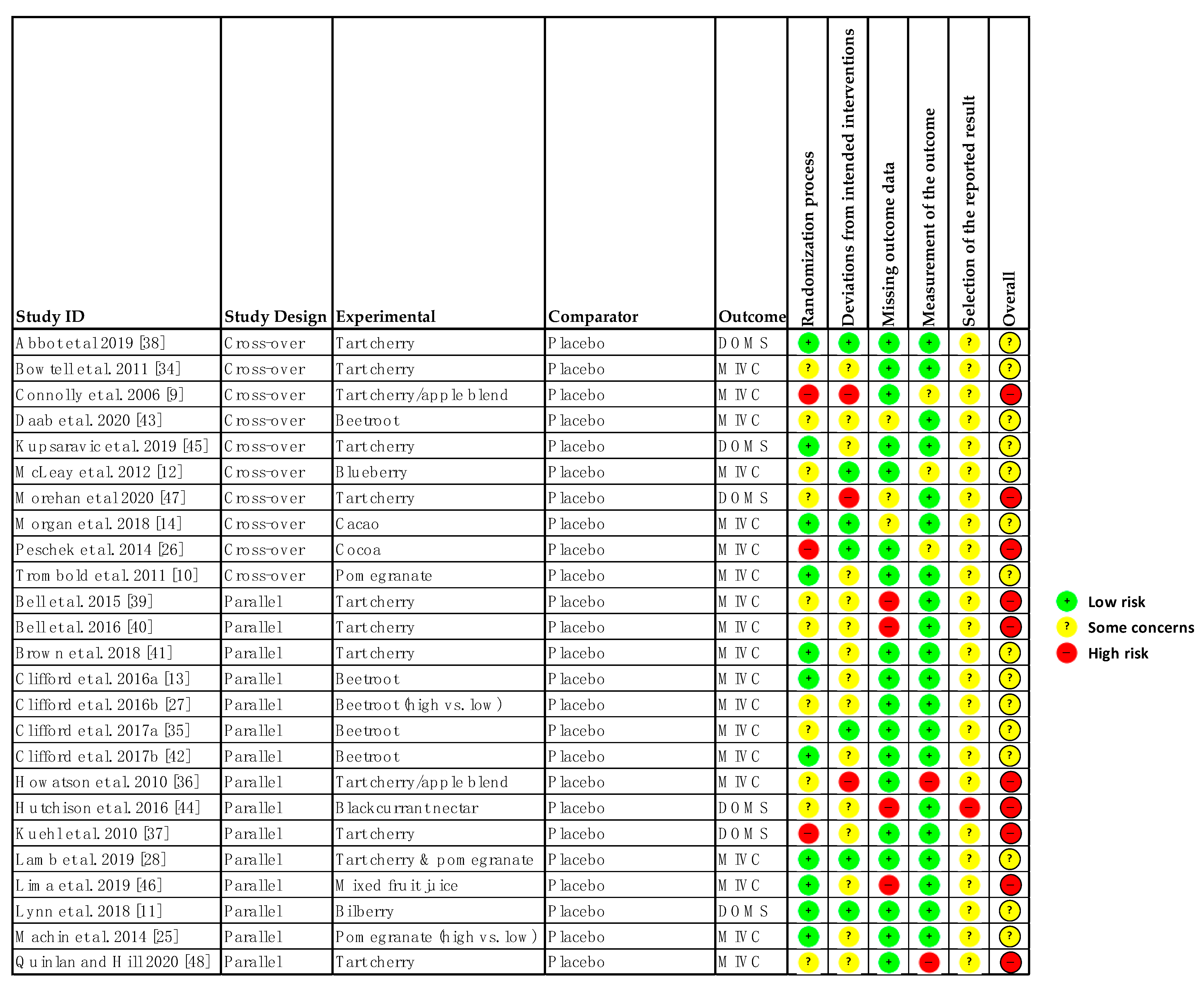
3.4. Risk of Bias within Studies
3.5. Syntheses of Results
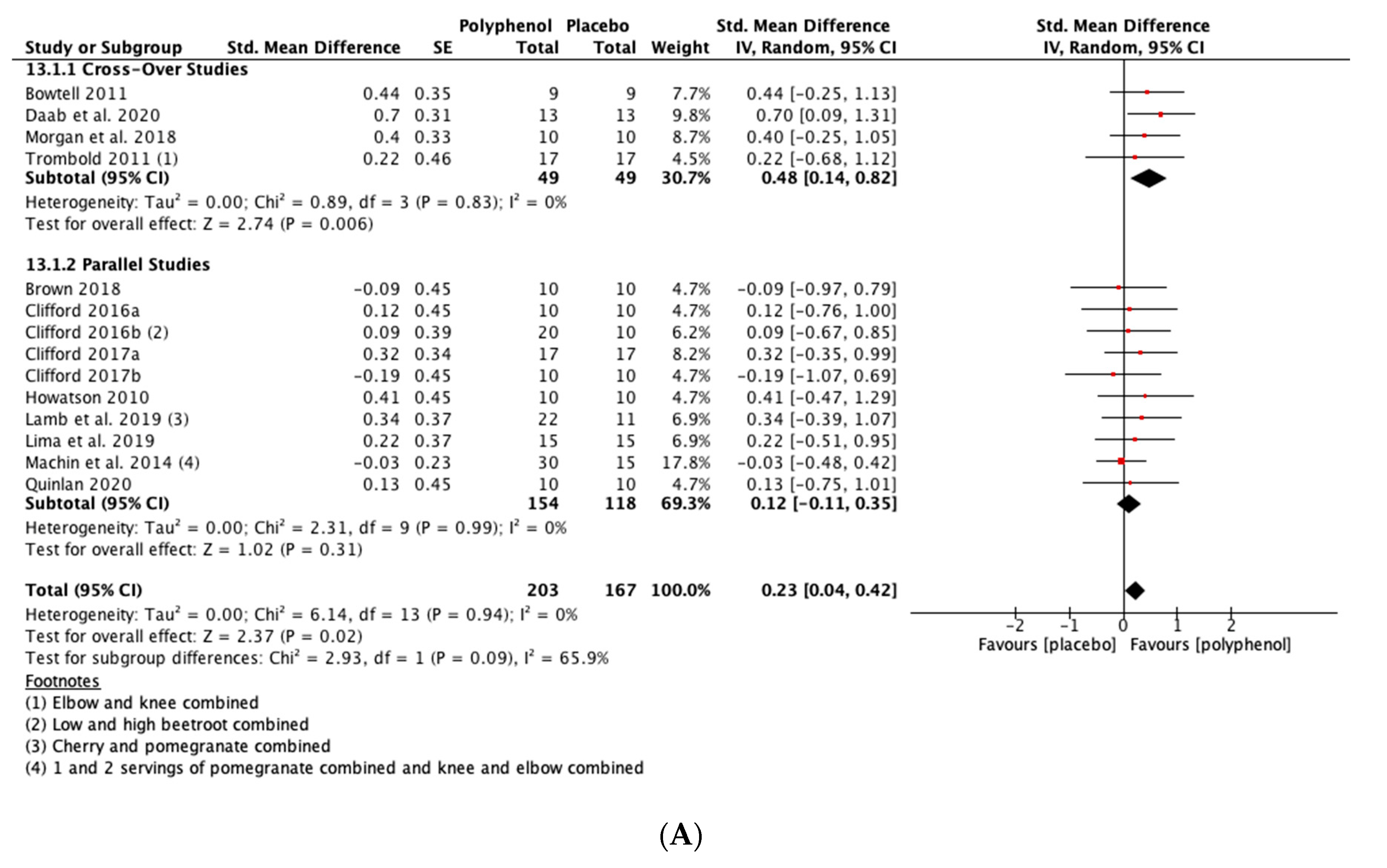
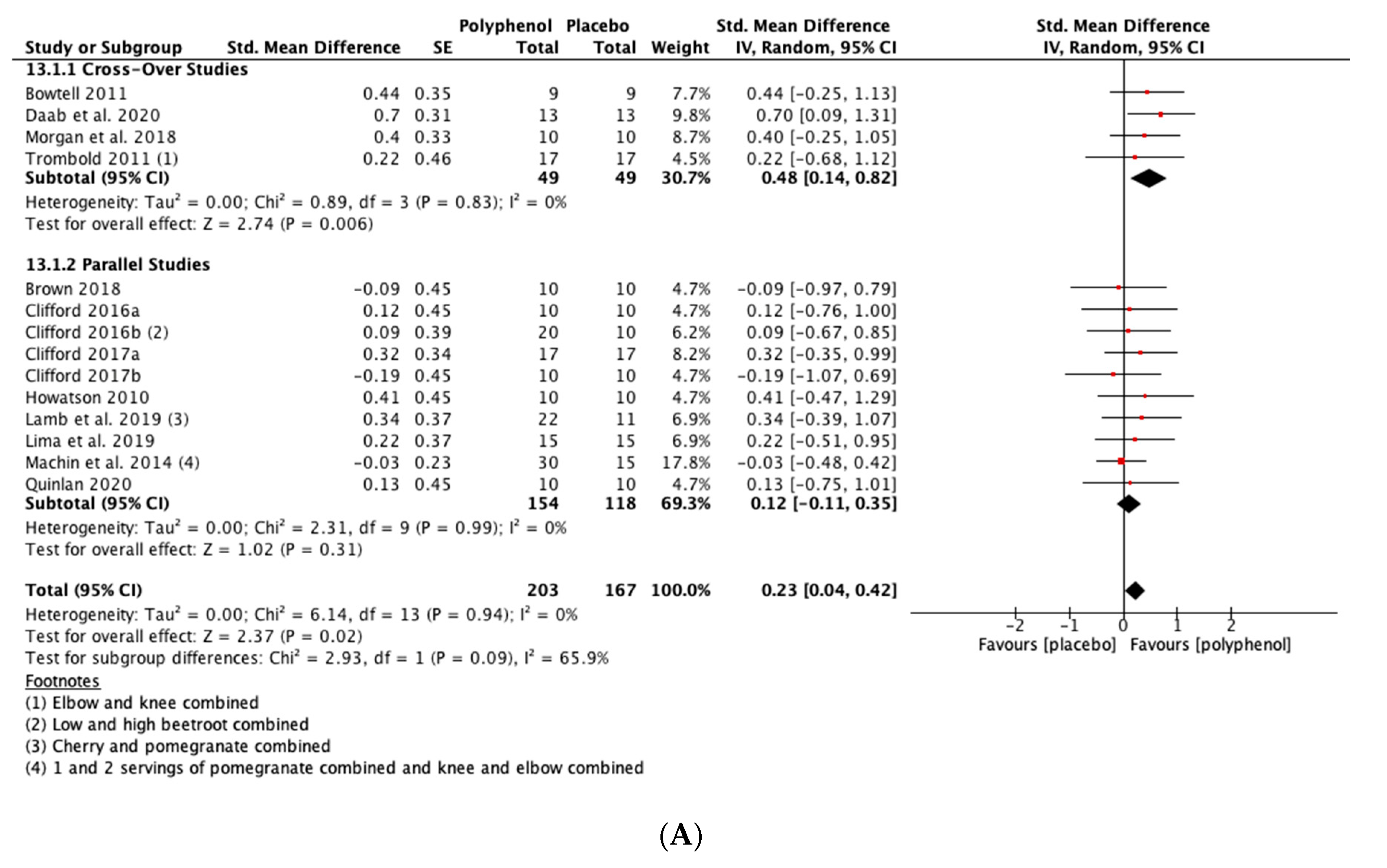
3.5.1. Primary Outcomes
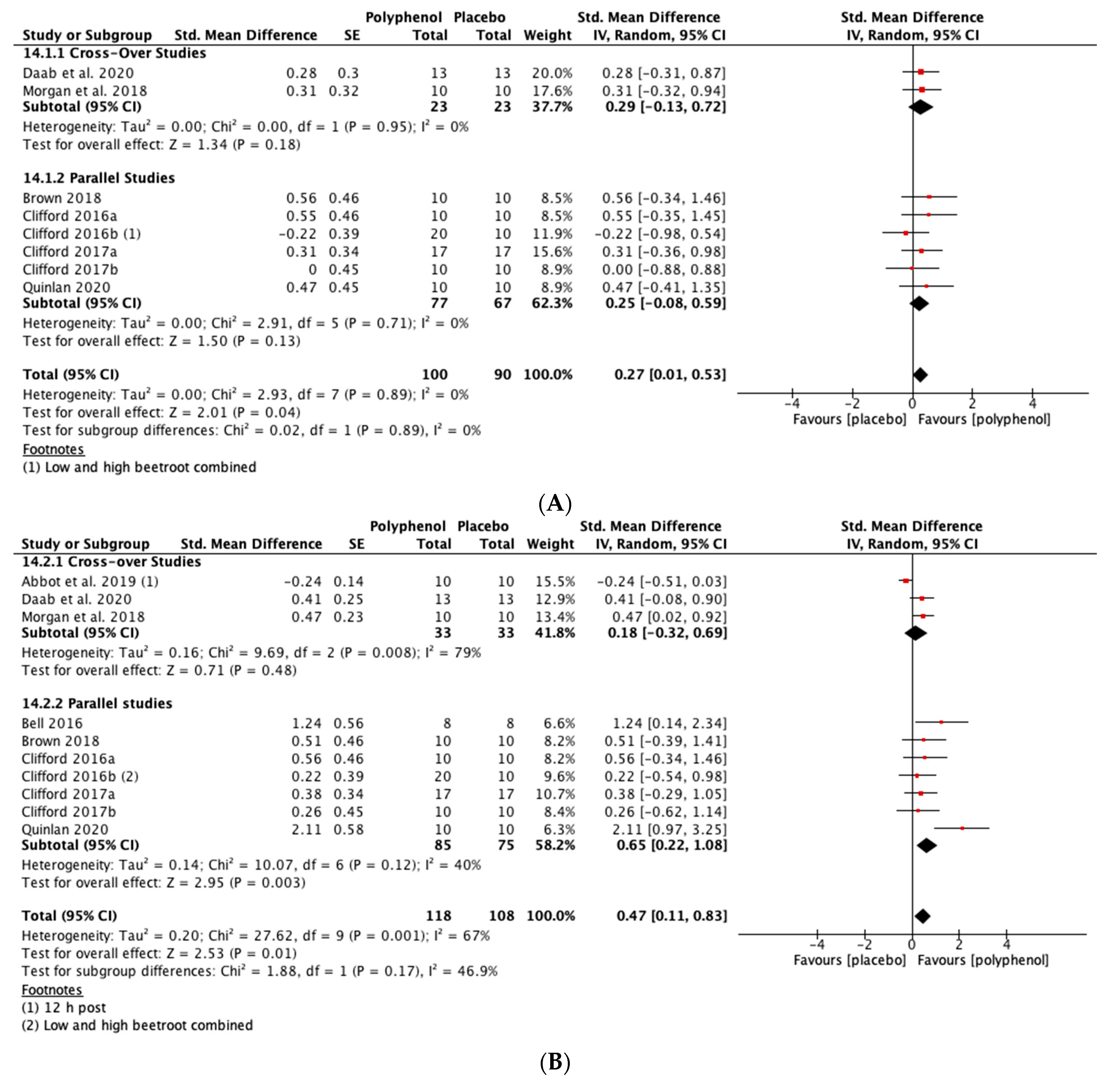
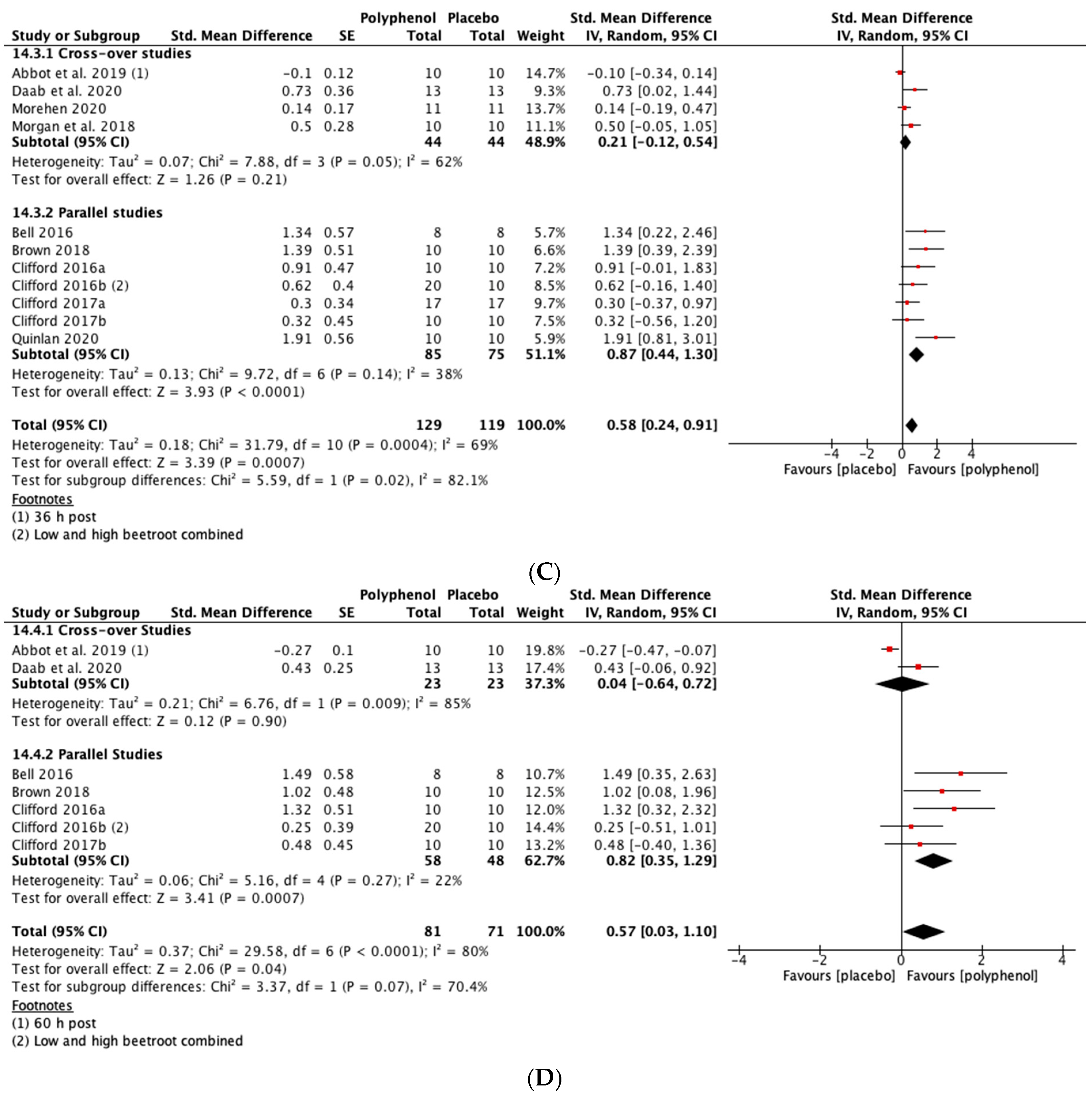
MIVC
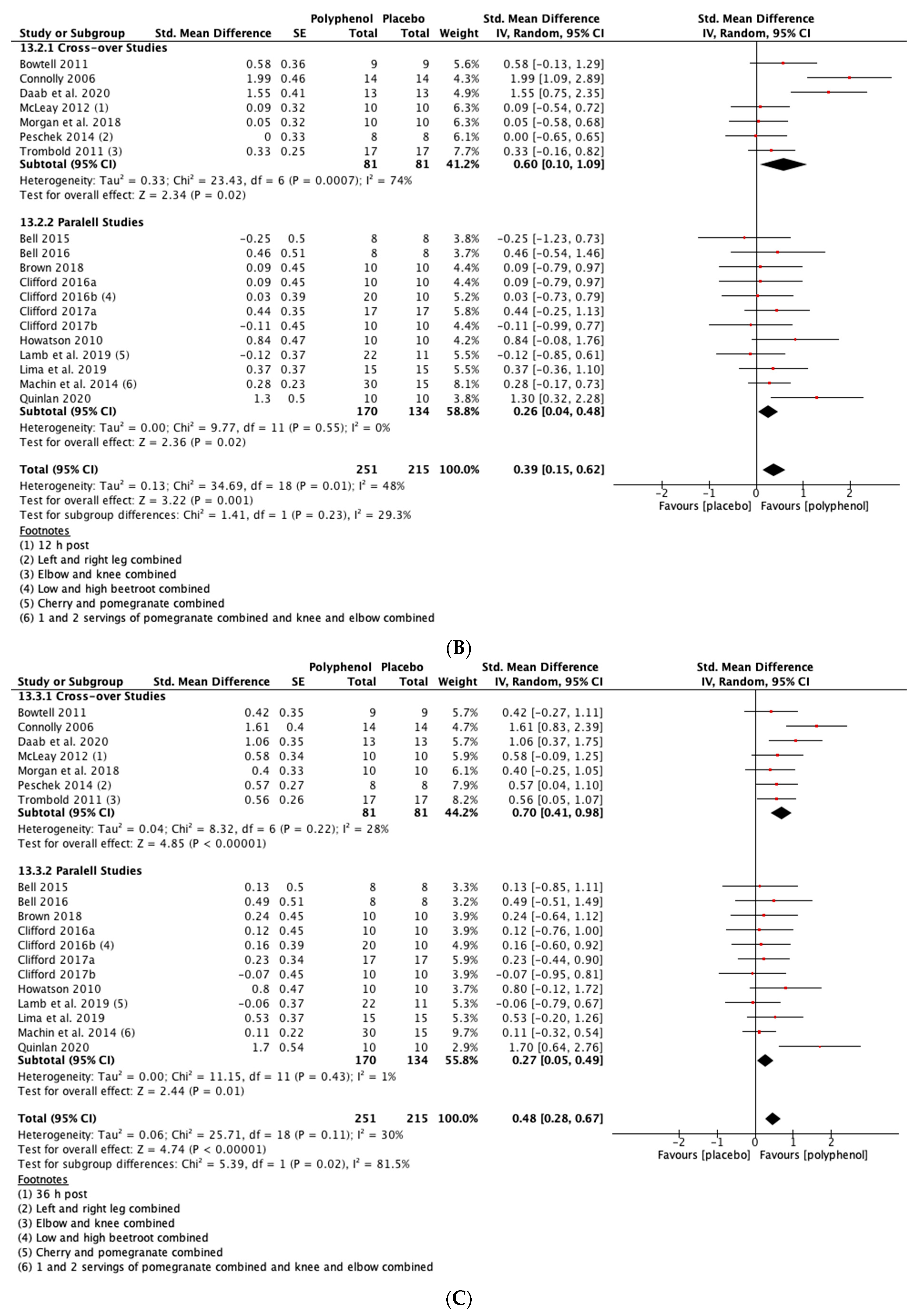
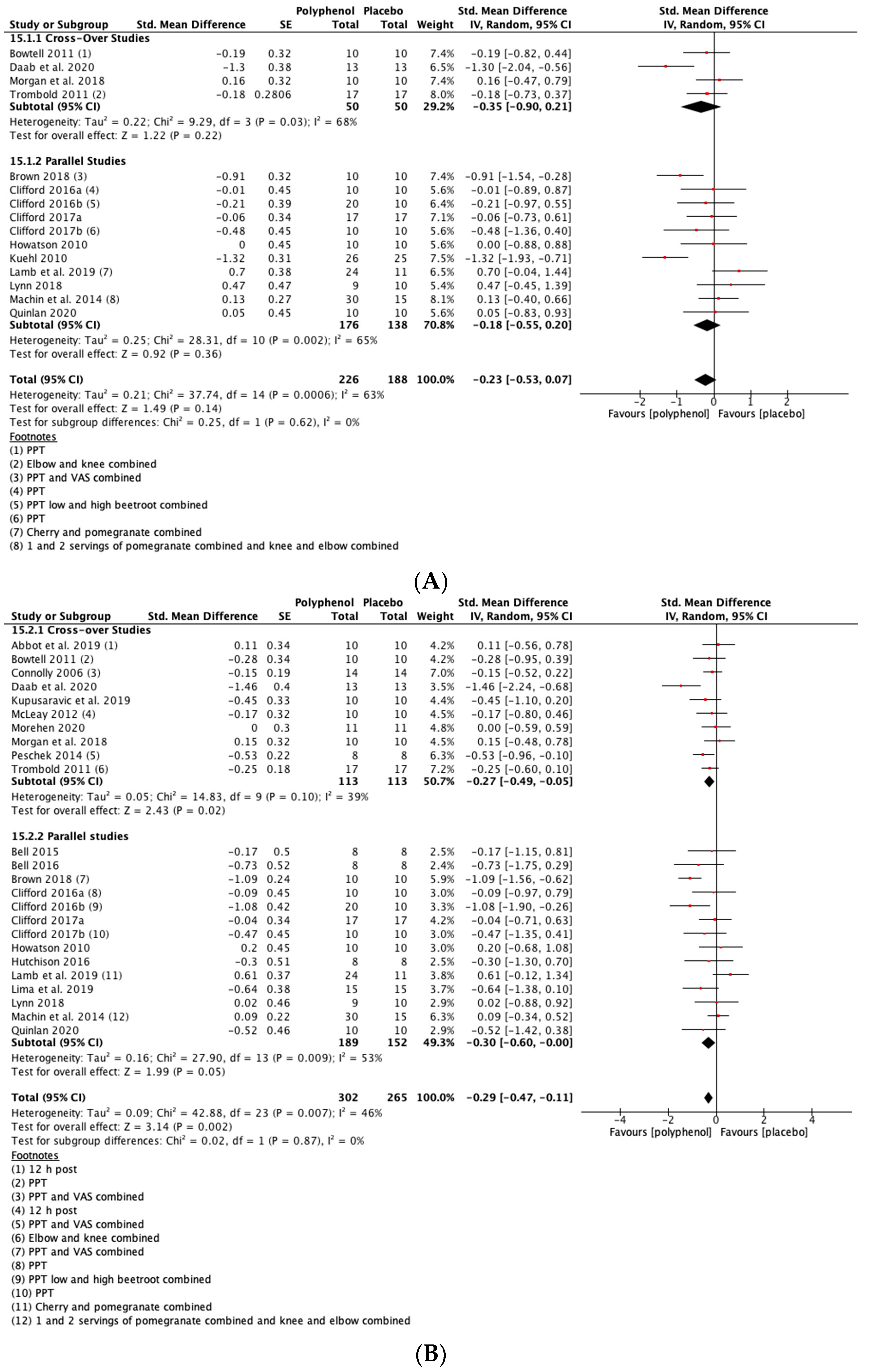
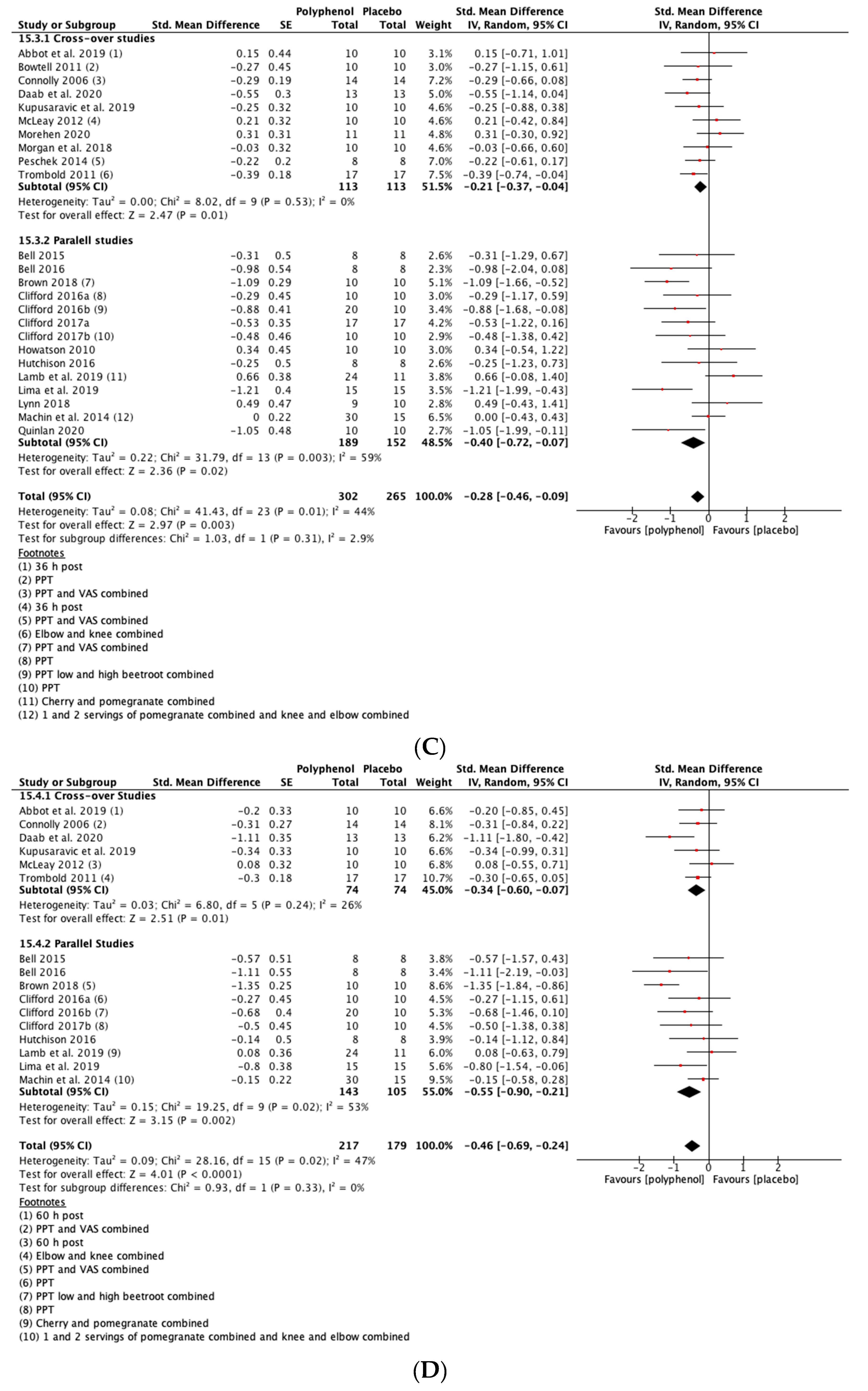
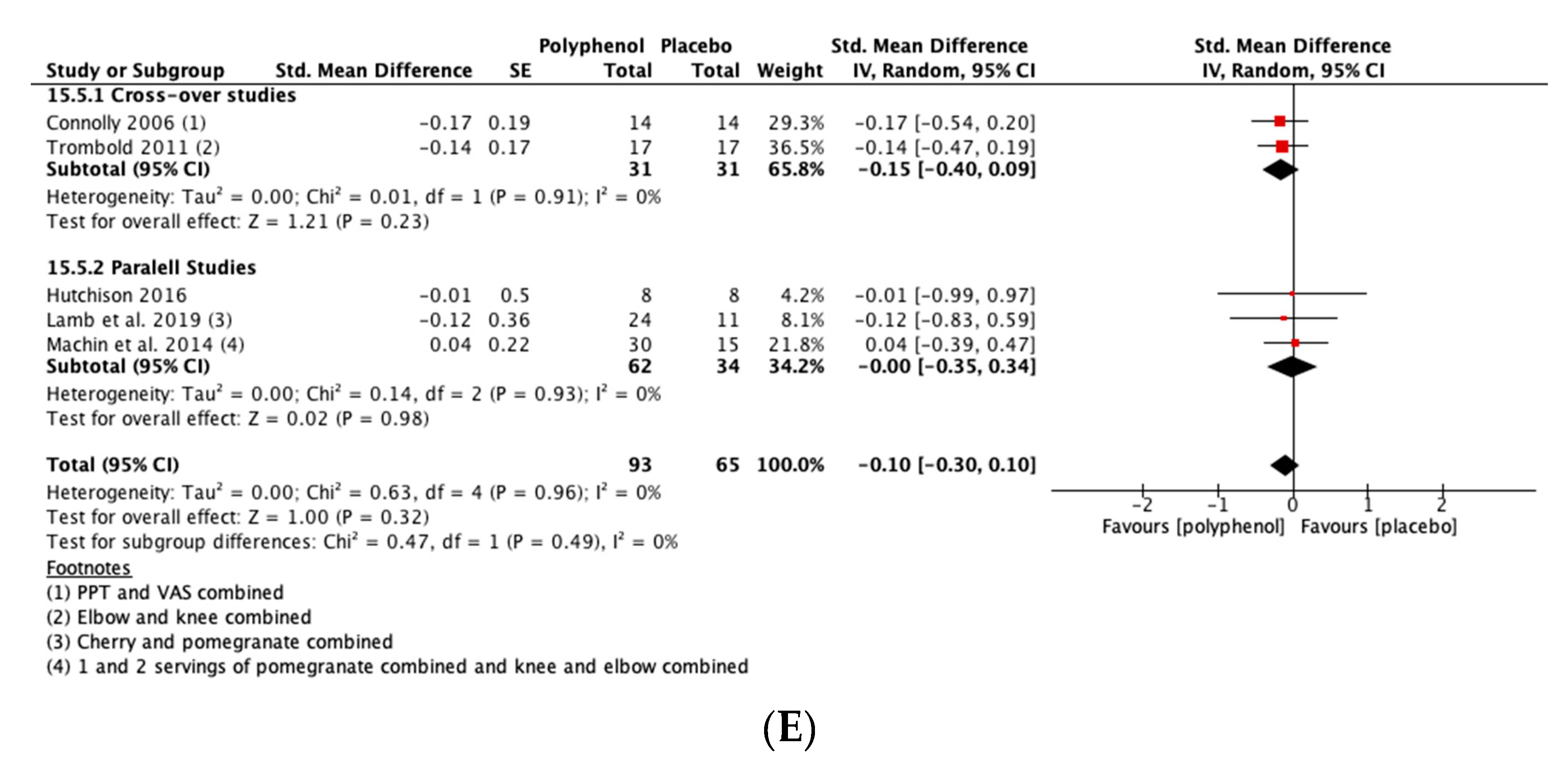
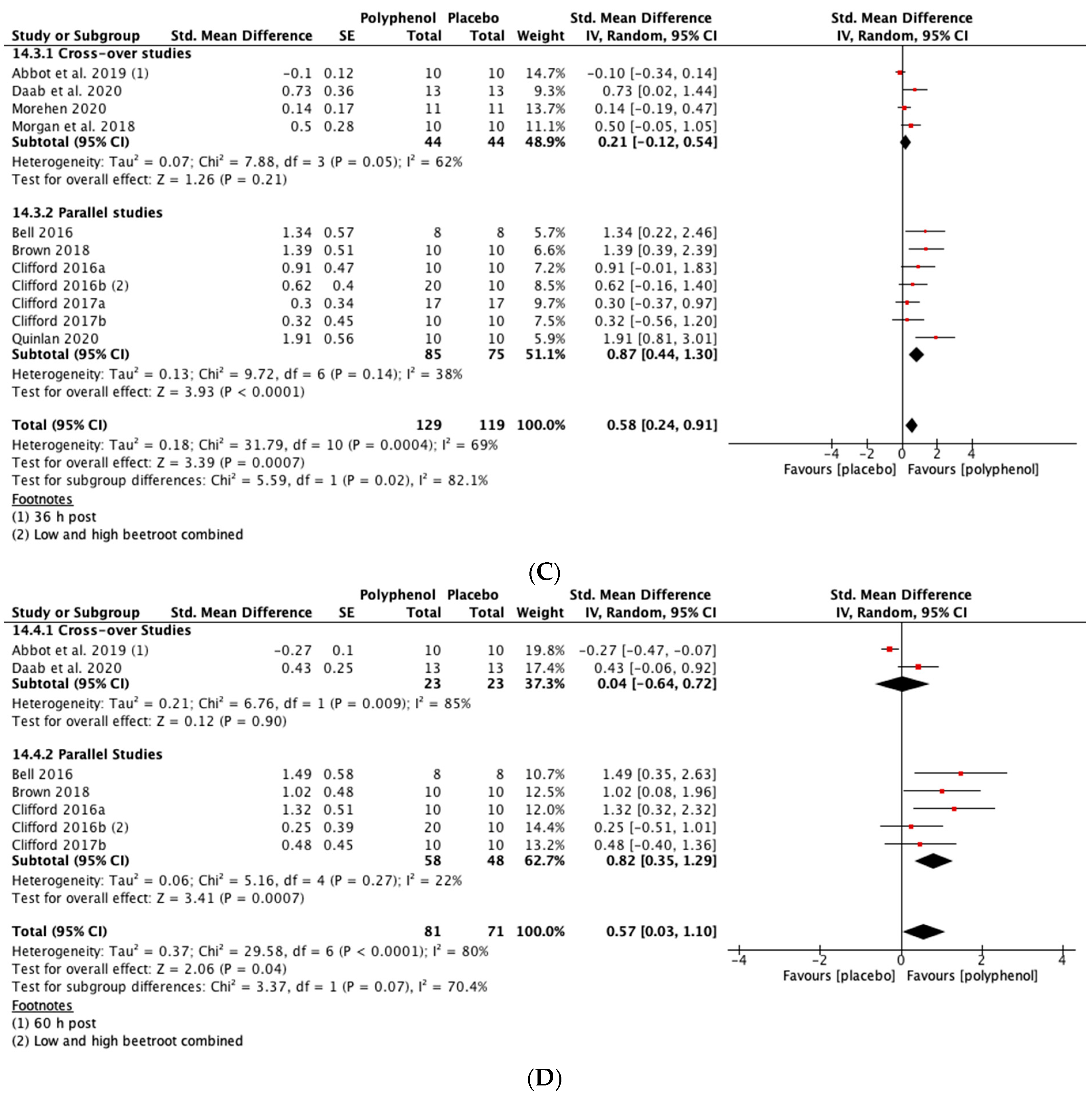
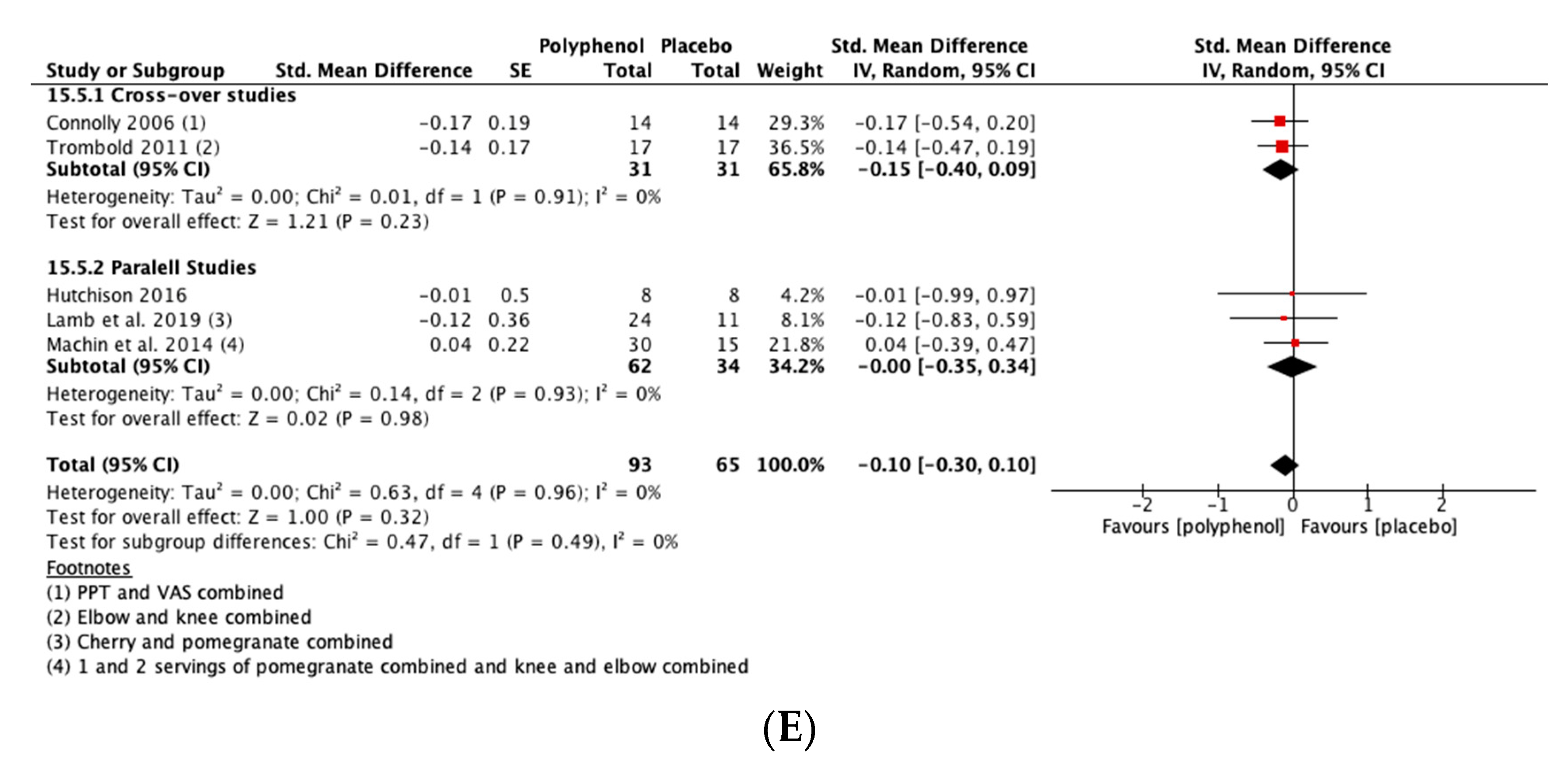
DOMS
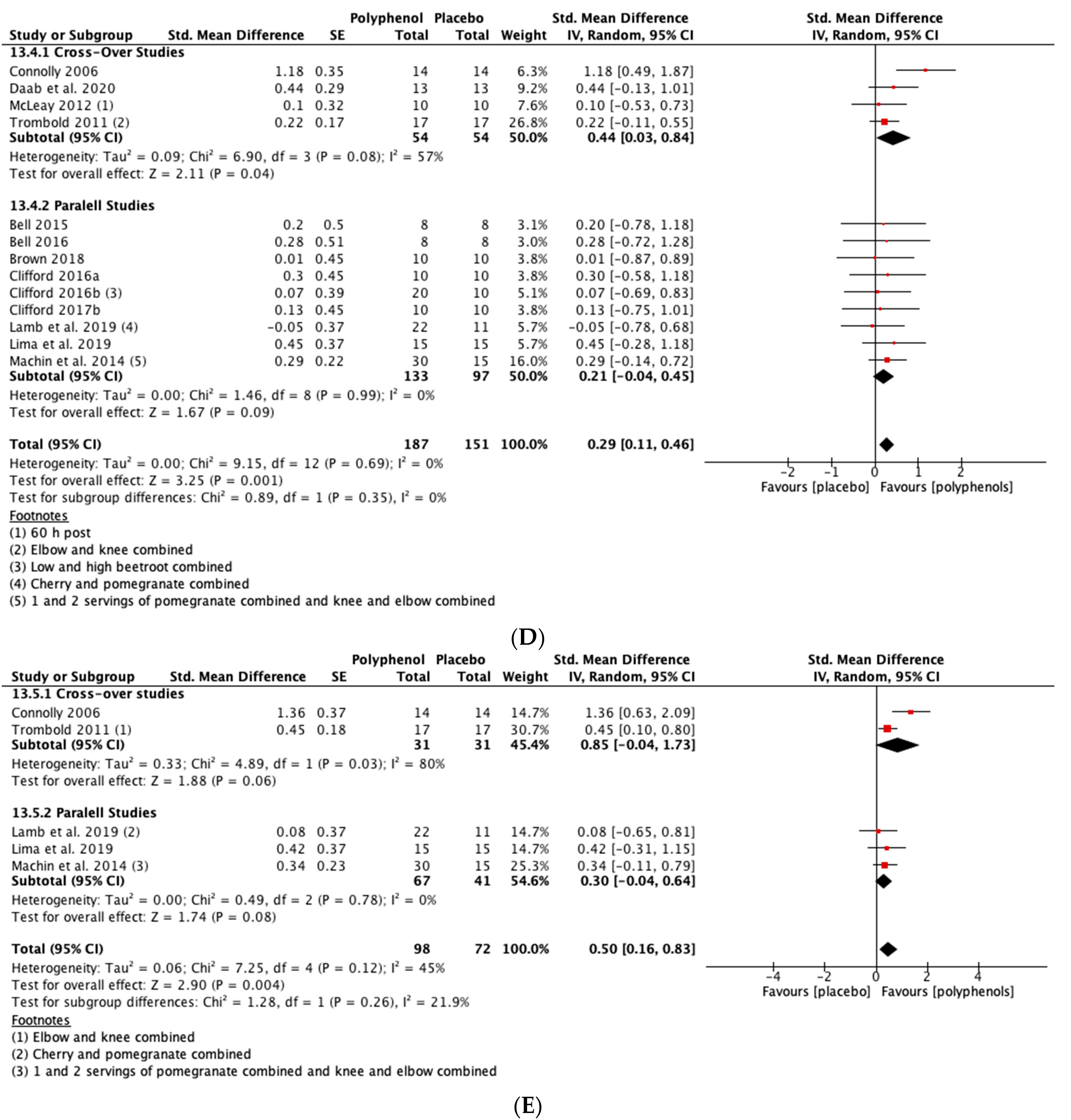
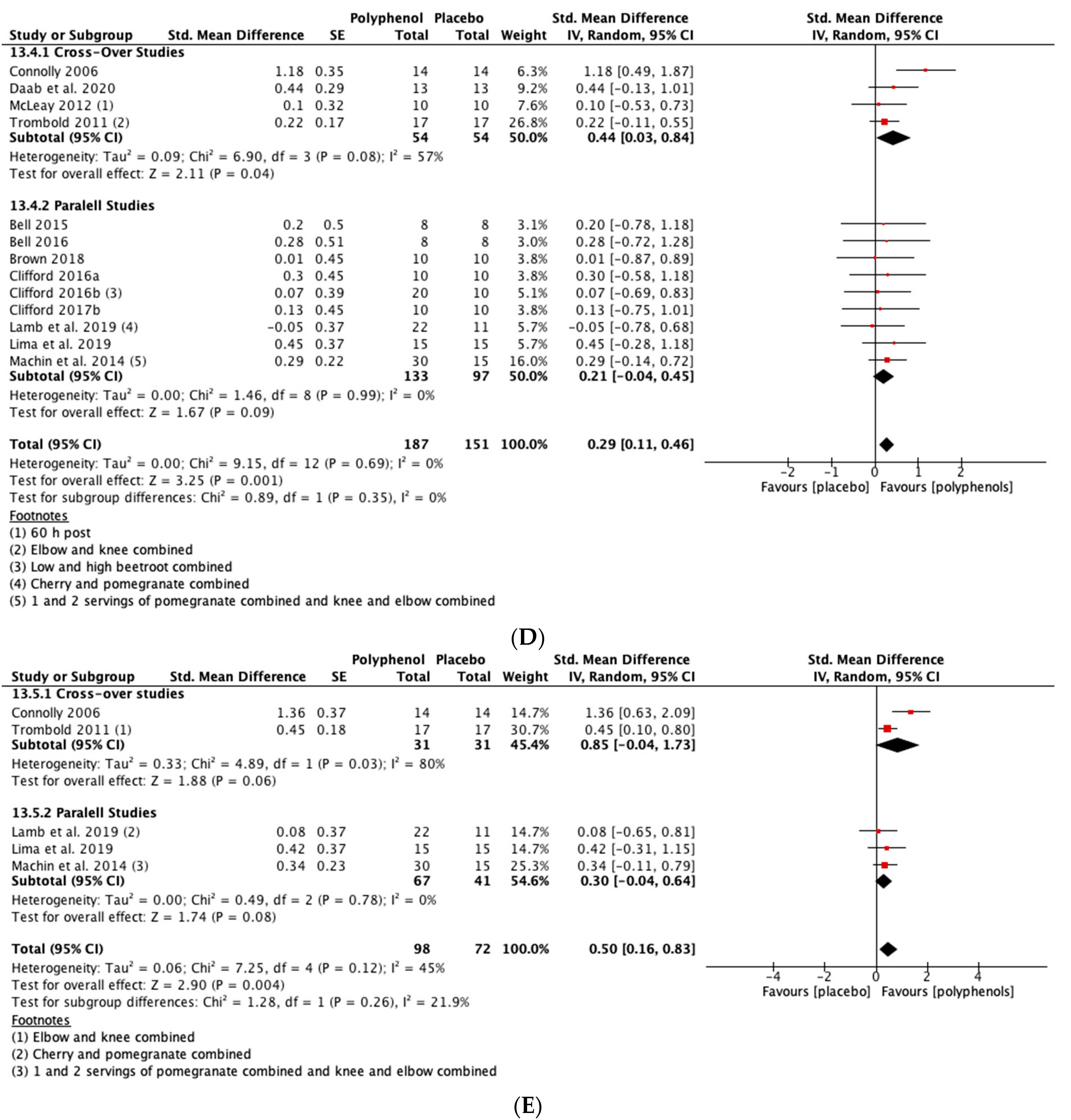
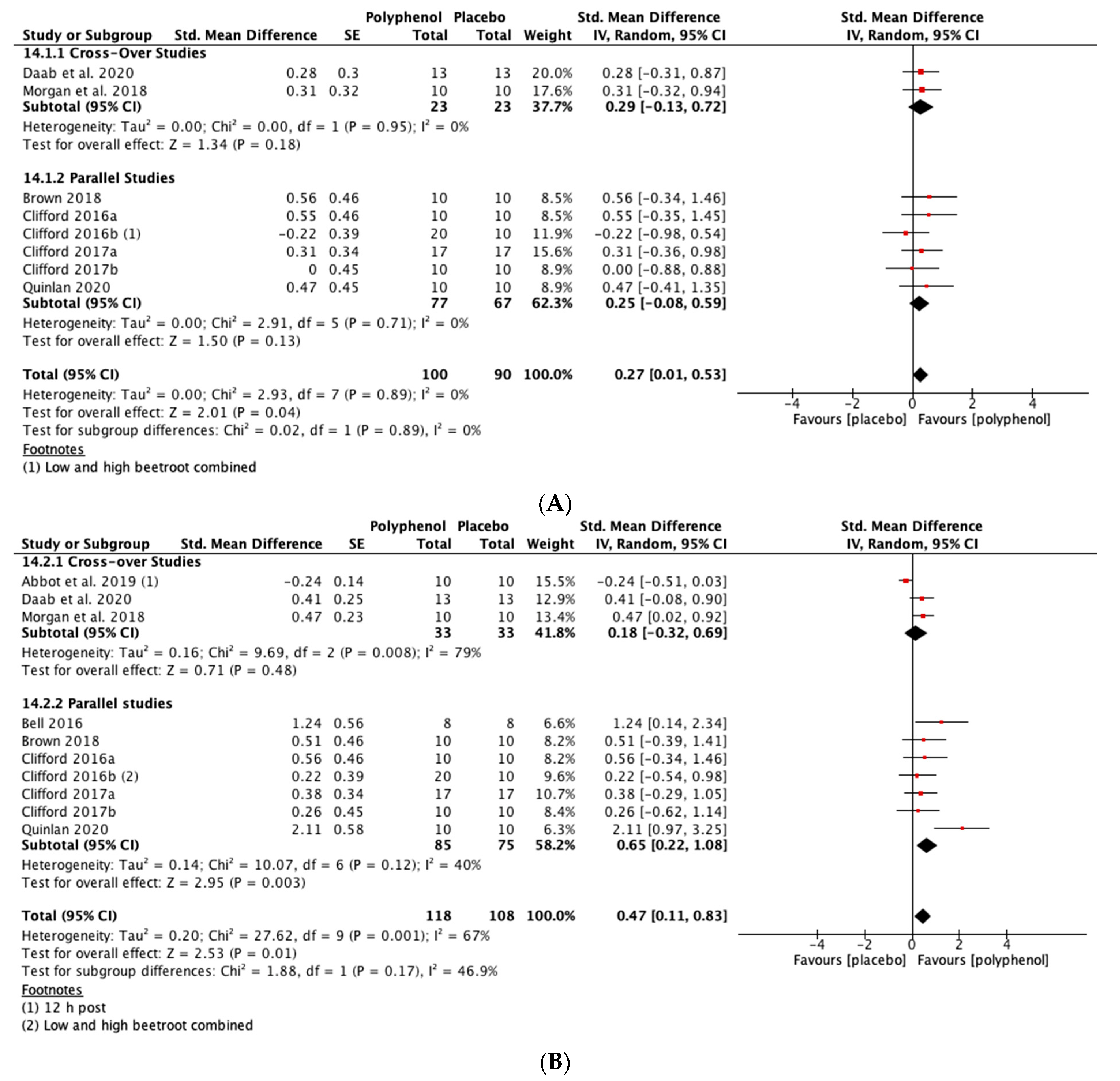
CMJ
Heterogeneity
Sensitivity Analysis
3.5.2. Secondary Outcomes
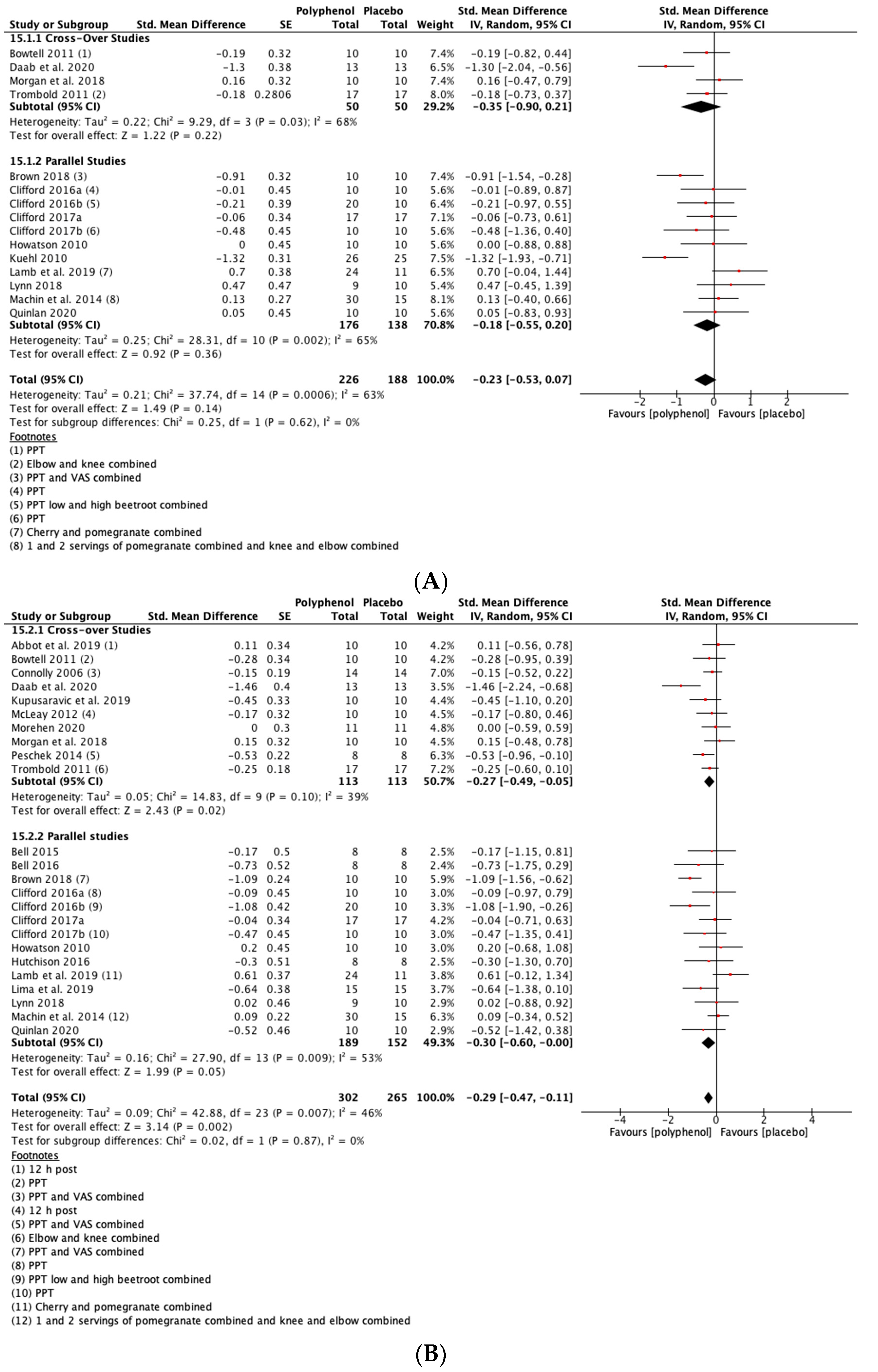
CK
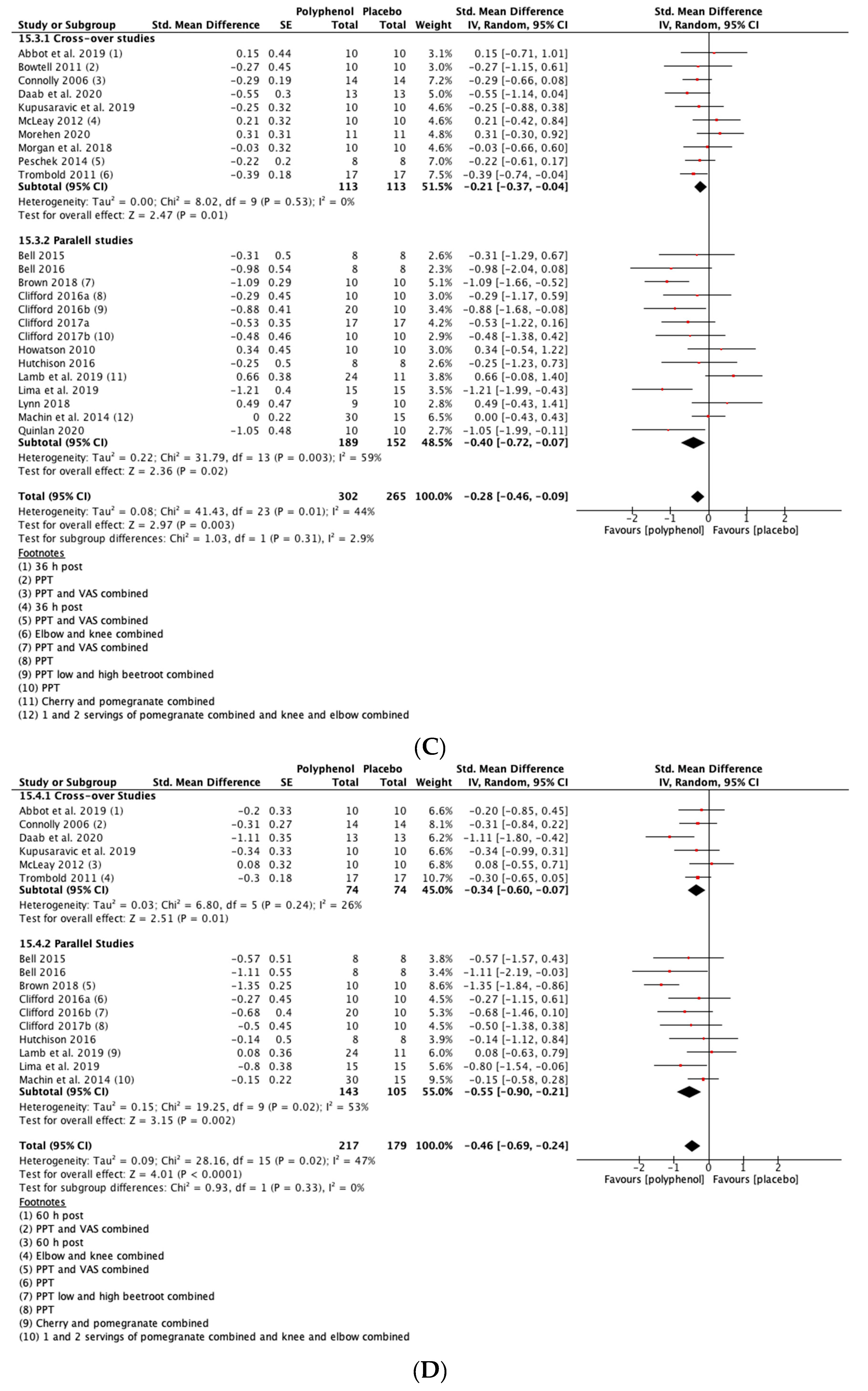
CRP
IL-6
PC
3.5.3. Analyses by Individual Polyphenol-Rich Foods
3.5.4. Comparison of Studies Based on Restriction of Dietary Polyphenol Intake
3.5.5. Quality of Evidence
4. Discussion
4.1. Mechanisms
4.2. Comparison with Other Reviews
4.3. Limitations
4.4. Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bowtell, J.; Kelly, V. Fruit-derived polyphenol supplementation for athlete recovery and performance. Sports Med. 2019, 49, 3–23. [Google Scholar] [CrossRef] [Green Version]
- Clarkson, P.M.; Hubal, M.J. Exercise-induced muscle damage in humans. Am. J. Phys. Med. Rehabil. 2002, 81, S52–S69. [Google Scholar] [CrossRef] [PubMed]
- Owens, D.J.; Twist, C.; Cobley, J.N.; Howatson, G.; Close, G.L. Exercise-induced muscle damage: What is it, what causes it and what are the nutritional solutions? Eur. J. Sport Sci. 2019, 19, 71–85. [Google Scholar] [CrossRef]
- Howatson, G.; van Someren, K.A. The prevention and treatment of exercise-induced muscle damage. Sports Med. 2008, 38, 483–503. [Google Scholar] [CrossRef] [PubMed]
- Morgan, D.L.; Proske, U. Popping sarcomere hypothesis explains stretch-induced muscle damage. Clin. Exp. Pharm. Physiol. 2004, 31, 541–545. [Google Scholar] [CrossRef]
- Fridén, J.; Sjöström, M.; Ekblom, B. Myofibrillar damage following intense eccentric exercise in man. Int. J. Sports Med. 1983, 4, 170–176. [Google Scholar] [CrossRef]
- Butterfield, T.A.; Best, T.M.; Merrick, M.A. The dual roles of neutrophils and macrophages in inflammation: A critical balance between tissue damage and repair. J. Athl. Train. 2006, 41, 457–465. [Google Scholar]
- Williamson, G. The role of polyphenols in modern nutrition. Nutr. Bull. 2017, 42, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Connolly, D.A.; McHugh, M.P.; Padilla-Zakour, O.I.; Carlson, L.; Sayers, S.P. Efficacy of a tart cherry juice blend in preventing the symptoms of muscle damage. Br. J. Sports Med. 2006, 40, 679–683; discussion 683. [Google Scholar] [CrossRef] [PubMed]
- Trombold, J.R.; Reinfeld, A.S.; Casler, J.R.; Coyle, E.F. The effect of pomegranate juice supplementation on strength and soreness after eccentric exercise. J. Strength Cond. Res. 2011, 25, 1782–1788. [Google Scholar] [CrossRef]
- Lynn, A.; Garner, S.; Nelson, N.; Simper, T.N.; Hall, A.C.; Ranchordas, M.K. Effect of bilberry juice on indices of muscle damage and inflammation in runners completing a half-marathon: A randomised, placebo-controlled trial. J. Int. Soc. Sports Nutr. 2018, 15, 1–8. [Google Scholar] [CrossRef] [Green Version]
- McLeay, Y.; Barnes, M.J.; Mundel, T.; Hurst, S.M.; Hurst, R.D.; Stannard, S.R. Effect of New Zealand blueberry consumption on recovery from eccentric exercise-induced muscle damage. J. Int. Soc. Sports Nutr. 2012, 9, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clifford, T.; Berntzen, B.; Davison, G.W.; West, D.J.; Howatson, G.; Stevenson, E.J. Effects of Beetroot Juice on Recovery of Muscle Function and Performance between Bouts of Repeated Sprint Exercise. Nutrients 2016, 8, 506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgan, P.T.; Wollman, P.M.; Jackman, S.R.; Bowtell, J.L. Flavanol-Rich Cacao Mucilage Juice Enhances Recovery of Power but Not Strength from Intensive Exercise in Healthy, Young Men. Sports 2018, 6, 159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahadoran, Z.; Mirmiran, P.; Jeddi, S.; Azizi, F.; Ghasemi, A.; Hadaegh, F. Nitrate and nitrite content of vegetables, fruits, grains, legumes, dairy products, meats and processed meats. J. Food Compos. Anal. 2016, 51, 93–105. [Google Scholar] [CrossRef]
- Kujala, T.S.; Vienola, M.S.; Klika, K.D.; Loponen, J.M.; Pihlaja, K. Betalain and phenolic compositions of four beetroot (Beta vulgaris) cultivars. Eur. Food Res. Technol. 2002, 214, 505–510. [Google Scholar] [CrossRef]
- Doma, K.; Gahreman, D.; Connor, J. Fruit supplementation reduces indices of exercise-induced muscle damage: A systematic review and meta-analysis. Eur. J. Sport Sci. 2021, 24, 562–579. [Google Scholar] [CrossRef]
- Warren, G.L.; Lowe, D.A.; Armstrong, R.B. Measurement tools used in the study of eccentric contraction-induced injury. Sports Med. 1999, 27, 43–59. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version; Cochrane: London, UK, 2021. [Google Scholar]
- Starbuck, C.; Eston, R.G. Exercise-induced muscle damage and the repeated bout effect: Evidence for cross transfer. Eur. J. Appl. Physiol. 2012, 112, 1005–1013. [Google Scholar] [CrossRef]
- RevMan 5.3 User Guide. Available online: https://training.cochrane.org/sites/training.cochrane.org/files/public/uploads/resources/downloadable_resources/English/RevMan_5.3_User_Guide.pdf (accessed on 24 June 2014).
- Sterne, J.A.C.; Savovic, J.; Page, M.J. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Altman, D.; Curtin, F.; Li, T.; Senn, S. Revised Cochrane Risk of Bias Tool for Randomized Trials (RoB 2.0) Additional Considerations for Cross-Over Trials 2016. 2021. Available online: https://www.unisa.edu.au/contentassets/72bf75606a2b4abcaf7f17404af374ad/rob2-0_indiv_main_guidance.pdf (accessed on 20 October 2016).
- Machin, D.R.; Christmas, K.M.; Chou, T.; Hill, S.C.; Van Pelt, D.W.; Trombold, J.R.; Coyle, E.F. Effects of differing dosages of pomegranate juice supplementation after eccentric exercise. Physiol. J. 2014, 2014. [Google Scholar] [CrossRef] [Green Version]
- Peschek, K.; Pritchett, R.; Bergman, E.; Pritchett, K. The effects of acute post exercise consumption of two cocoa-based beverages with varying flavanol content on indices of muscle recovery following downhill treadmill running. Nutrients 2014, 6, 50–62. [Google Scholar] [CrossRef] [Green Version]
- Clifford, T.; Bell, O.; West, D.J.; Howatson, G.; Stevenson, E.J. The effects of beetroot juice supplementation on indices of muscle damage following eccentric exercise. Eur. J. Appl. Physiol. 2016, 116, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Lamb, K.L.; Ranchordas, M.K.; Johnson, E.; Denning, J.; Downing, F.; Lynn, A. No effect of tart cherry juice or pomegranate juice on recovery from exercise-induced muscle damage in non-resistance trained men. Nutrients 2019, 11, 1593. [Google Scholar] [CrossRef] [Green Version]
- Taylor, K.S.; Mahtani, K.R.; Aronson, J.K. Combining and converting groups when extracting data for meta-analysis. BMJ Evid. Based Med. 2021, 26, 85–87. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: New York, NY, USA, 1988. [Google Scholar]
- Guyatt, G.H.; Thorlund, K.; Oxman, A.D. GRADE guidelines: 13. Preparing summary of findings tables and evidence profiles—Continuous outcomes. J. Clin. Epidemiol. 2013, 66, 173–183. [Google Scholar] [CrossRef]
- Cumming, G. Understanding the New Statistics: Effect Sizes, Confidence Intervals and Meta-Analyses; Routledge: East Sussex, UK, 2012. [Google Scholar]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Bowtell, J.L.; Sumners, D.P.; Dyer, A.; Fox, P.; Mileva, K.N. Montmorency cherry juice reduces muscle damage caused by intensive strength exercise. Med. Sci. Sports Exerc. 2011, 43, 1544–1551. [Google Scholar] [CrossRef] [Green Version]
- Clifford, T.; Allerton, D.M.; Brown, M.A.; Harper, L.; Horsburgh, S.; Keane, K.M.; Stevenson, E.J.; Howatson, G. Minimal muscle damage after a marathon and no influence of beetroot juice on inflammation and recovery. Appl. Physiol. Nutr. Metab. 2017, 42, 263–270. [Google Scholar] [CrossRef]
- Howatson, G.; McHugh, M.; Hill, J.; Brouner, J.; Jewell, A.; Van Someren, K.A.; Shave, R.; Howatson, S. Influence of tart cherry juice on indices of recovery following marathon running. Scand. J. Med. Sci. Sports 2010, 20, 843–852. [Google Scholar] [CrossRef]
- Kuehl, K.S.; Perrier, E.T.; Elliot, D.L.; Chesnutt, J.C. Efficacy of tart cherry juice in reducing muscle pain during running: A randomized controlled trial. J. Int. Soc. Sports Nutr. 2010, 7, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbott, W.; Brashill, C.; Brett, A.; Clifford, T. Tart cherry juice: No effect on muscle function loss or muscle soreness in professional soccer players after a match. Int. J. Sports Physiol. Perform. 2020, 15, 249–254. [Google Scholar] [CrossRef]
- Bell, P.G.; Walshe, I.H.; Davison, G.W.; Stevenson, E.J.; Howatson, G. Recovery facilitation with Montmorency cherries following high-intensity, metabolically challenging exercise. Appl. Physiol. Nutr. Metab. 2015, 40, 414–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bell, P.G.; Stevenson, E.; Davison, G.W.; Howatson, G. The effects of Montmorency tart cherry concentrate supplementation on recovery following prolonged, intermittent exercise. Nutrients 2016, 8, 441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, M.A.; Stevenson, E.J.; Howatson, G. Montmorency tart cherry (Prunus cerasus L.) supplementation accelerates recovery from exercise-induced muscle damage in females. Eur. J. Sport Sci. 2019, 19, 95–102. [Google Scholar] [CrossRef]
- Clifford, T.; Howatson, G.; West, D.J.; Stevenson, E.J. Beetroot juice is more beneficial than sodium nitrate for attenuating muscle pain after strenuous eccentric-bias exercise. Appl. Physiol. Nutr. Metab. 2017, 42, 1185–1191. [Google Scholar] [CrossRef] [Green Version]
- Daab, W.; Bouzid, M.A.; Lajri, M.; Bouchiba, M.; Saafi, M.A.; Rebai, H. Chronic beetroot juice supplementation accelerates recovery kinetics following simulated match play in soccer players. J. Am. Coll. Nutr. 2021, 40, 61–69. [Google Scholar] [CrossRef]
- Hutchison, A.T.; Flieller, E.B.; Dillon, K.J.; Leverett, B.D. Black currant nectar reduces muscle damage and inflammation following a bout of high-intensity eccentric contractions. J. Diet. Suppl. 2016, 13, 1–15. [Google Scholar] [CrossRef]
- Kupusarevic, J.; McShane, K.; Clifford, T. Cherry gel supplementation does not attenuate subjective muscle soreness or alter wellbeing following a match in a team of professional rugby union players: A pilot study. Sports 2019, 7, 84. [Google Scholar] [CrossRef] [Green Version]
- Lima, L.C.; Barreto, R.V.; Bassan, N.M.; Greco, C.C.; Denadai, B.S. Consumption of an anthocyanin-rich antioxidant juice accelerates recovery of running economy and indirect markers of exercise-induced muscle damage following downhill running. Nutrients 2019, 11, 2274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morehen, J.C.; Clarke, J.; Batsford, J.; Barrow, S.; Brown, A.D.; Stewart, C.E.; Morton, J.P.; Close, G.L. Montmorency tart cherry juice does not reduce markers of muscle soreness, function and inflammation following professional male rugby League match-play. Eur. J. Sport Sci. 2021, 21, 1003–1012. [Google Scholar] [CrossRef] [PubMed]
- Quinlan, R.; Hill, J.A. The efficacy of tart cherry juice in aiding recovery after intermittent exercise. Int. J. Sports Physiol. Perform. 2020, 15, 368–374. [Google Scholar] [CrossRef] [Green Version]
- Tashjian, R.Z.; Deloach, J.; Porucznik, C.A.; Powell, A.P. Minimal clinically important differences (MCID) and patient acceptable symptomatic state (PASS) for visual analog scales (VAS) measuring pain in patients treated for rotator cuff disease. J. Shoulder Elb. Surg. 2009, 18, 927–932. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Osoba, D.; Wu, A.W. Methods to explain the clinical significance of health status measures. Mayo Clin. Proc. 2002, 77, 371–383. [Google Scholar] [CrossRef]
- Manach, C.; Scalbert, A.; Morand, C.; Rémésy, C.; Jiménez, L. Polyphenols: Food sources and bioavailability. Am. J. Clin. Nutr. 2004, 79, 727–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baird, M.F.; Graham, S.M.; Baker, J.S.; Bickerstaff, G.F. Creatine-kinase-and exercise-related muscle damage implications for muscle performance and recovery. J. Nutr. Metab. 2012, 2012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brancaccio, P.; Maffulli, N.; Limongelli, F.M. Creatine kinase monitoring in sport medicine. Br. Med. Bull. 2007, 81, 209–230. [Google Scholar] [CrossRef]
- Sies, H. Total antioxidant capacity: Appraisal of a concept. J. Nutr. 2007, 137, 1493–1495. [Google Scholar] [CrossRef]
- Powers, S.K.; Smuder, A.J.; Kavazis, A.N.; Hudson, M.B. Experimental guidelines for studies designed to investigate the impact of antioxidant supplementation on exercise performance. Int. J. Sport Nutr. Exerc. Metab. 2010, 20, 2–14. [Google Scholar] [CrossRef] [Green Version]
- Halliwell, B.; Gutteridge, J.M. Free Radicals in Biology and Medicine; Oxford University Press: New York, NY, USA, 2015. [Google Scholar]
- Jajtner, A.R.; Hoffman, J.R.; Townsend, J.R. The effect of polyphenols on cytokine and granulocyte response to resistance exercise. Physiol. Rep. 2016, 4, e13058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hill, J.A.; Keane, K.M.; Quinlan, R.; Howatson, G. Tart cherry supplementation and recovery from strenuous exercise: A systematic review and meta-analysis. Int. J. Sport Nutr. Exerc. Metab. 2021, 31, 154–167. [Google Scholar] [CrossRef] [PubMed]
- Le, G.; Novotny, S.A.; Mader, T.L.; Greising, S.M.; Chan, S.S.; Kyba, M.; Lowe, D.A.; Warren, G.L. A moderate oestradiol level enhances neutrophil number and activity in muscle after traumatic injury but strength recovery is accelerated. J. Physiol. 2018, 596, 4665–4680. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Participant Characteristics at Baseline | Study Design | Exercise Intervention | Polyphenol Supplement | Dosage and Duration | Outcome Variables and Time of Measurement (h) |
|---|---|---|---|---|---|---|
| Abbot et al. 2019 [38)] | Professional male soccer players Age 19 ± 1 years Height 1.8 ± 0.6 m Mass 77.3 ± 6.4 kg n = 10 | Crossover | 90 min soccer match | Tart cherry juice Polyphenol content not stated | 2 × 30 mL concentrate for 3 days (morning of match until 36 h post-exercise) | DOMS (12, 36, 60) CMJ (12, 36, 60) |
| Bell et al. 2015 [39] | Male healthy trained cyclists Age 30 ± 8 years Height 181.1 ± 6.7 cm Mass 76.5 ± 9.2 kg O2peak 61.6 ± 10.4 mL·kg−1·min−1 n = 16 | Parallel | 109 min stochastic cycling | Montmorency tart cherry juice Per 1 mL 9.2 mg of anthocyanins (HPLC) Atlas Biosciences, Tuscon, Arizona, USA | 2 × 30 mL concentrate for 8 days (4 days pre-exercise, on the day of, and 3 days post-exercise) | MIVC (PE, 24, 48, 72) DOMS (PE, 24, 48, 72) CK (PE, 24, 48, 72) CRP (PE, 24, 48, 72) IL-6 (PE, 24, 48, 72) |
| Bell et al. 2016 [40] | Male semi-professional soccer players Age 25 ± 4 years Height 180.8 ± 7.4 cm Mass 81.9 ± 6.6 kg O2peak 54.9 mL·kg−1·min−1 n = 16 | Parallel | Loughborough intermittent shuttle test | Montmorency tart cherry juice Per 1000 mL 73.5 mg cyanidin-3-glucoside (HPLC) 178.8 mg of GAE (total phenols) 0.58 trolox equivalent (TEAC) Based on previous work from own laboratory (61) | 2 × 30 mL concentrate for 8 days (4 days pre-exercise, on the day of, and 3 days post-exercise) | MIVC (PE, 24, 48, 72) DOMS PE, 24, 48, 72) CMJ (PE, 24, 48, 72) CK (PE, 24, 48, 72) CRP (PE, 24, 48, 72) IL-6 (PE, 24, 48, 72) |
| Bowtell et al. 2011 [34] | Male well-trained participants Age 27.8 ± 1.6 years Height 1.76 ± 0.03 m Mass 81.3 ± 4.3 kg n = 10 | Crossover | 10 × 10 single leg extension | Montmorency tart cherry juice 275 mmol·L−1 trolox equivalents (ORAC) (Brunswick Laboratories, Southborough, USA) Per 1 mL 9.117 mg of anthocyanins: malvidin (4.696 mg) and cyanidin (3.346 mg) (HPLC) (Atlas, Biosciences, Tucson, Arizona, USA) | 2 × 30 mL concentrate for 10 days (7 days pre-exercise, on the day of, and 2 days post-exercise) | MIVC (PE, 24, 48) CK (24, 48) CRP (PE, 24, 48) PC (PE, 24, 48) |
| Brown, Stevenson and Howatson (2019) [41] | Female physically active females Age 19 ± 1 years Height 167 ± 6 cm Mass 61.4 ± 5.7 kg BMI 22.1 ± 1.9 kg m−2 n = 20 | Parallel | 15 × 30 m repeated sprints with 30 s rest | Montmorency tart cherry juice Per 1000 mL 73.5 mg cyanidin-3-glucoside (HPLC) 178.8 mg of GAE (total phenols) 0.58 trolox equivalent (TEAC) Based on previous work from own laboratory (61). | 2 × 30 mL concentrate for 8 days (4 days pre-exercise, on the day of, and 3 days post-exercise) | MIVC (PE, 24, 48, 72) DOMS (PE, 24, 48, 72) CMJ (PE, 24, 48, 72) CK (PE, 24, 48, 72) CRP, (PE, 24, 48, 72) |
| Clifford et al. 2016a [13] | Male collegiate team sport players Age 22 ± 2.5 years Height 1.80 ± 0.70 m Mass 75.1 ± 10.9 kg n = 20 | Parallel | 20 × 30 m sprints on day 1 and day 4 (72 h apart) | Beetroot juice Per 1000 mL 1606.9 ± 151 mg GAE (total phenols) 11.4 ± 0.2 mmol trolox equivalents (TEAC) (62). | 2 × 250 mL for 3 days (day of and 2 days post-exercise) | MIVC (PE, 24, 48, 72, 96) CMJ (PE, 24, 48, 72, 96) CK (PE, 24, 48, 72, 96) CRP (PE, 24, 48, 72, 96) PC (PE, 24, 48, 72, 96) |
| Clifford et al. 2016b [27] | Male recreational active participants Age 21.3 ± 4 years Height 178 ± 0.76 m Mass 75.6 ± 8.3 kg n = 30 | Parallel | 5 × 20 drop jumps | Beetroot juice (high 250 mL vs. low dose 125 mL) Per 250 mL 401.72 ± 37.72 mg GAE (total phenols) 2.85 ± 0.05 mmol trolox equivalents (DPPH) | 3 × servings on day of exercise and 2 × servings for two days post-exercise | MIVC, (PE, 24, 48, 72) CMJ (PE, 24 48, 72) CK (PE, 24, 48, 72) IL-6 (PE, 24, 48, 72) |
| Clifford et al. 2017a [35] | Recreational runners Age 40.5 ± 11 years Height 1.71 ± 0.08 cm Mass 70.3 ± 10.85 kg n = 34 (m = 21; f = 13) | Parallel | Druridge Bay Marathon (Northumbria, UK) | Beetroot juice (250 mL) Per 250 mL ~400 mg GAE (total phenols) ~3 mmol trolox equivalents (DPPH) (62). | 3 × servings on day of exercise and 2 × servings for two days post-exercise | MIVC (PE, 24, 48) DOMS (PE, 24, 48) CMJ (PE, 24, 48) CK (PE, 24, 48) CRP (PE, 24, 48) IL-6 (PE, 24, 48) |
| Clifford et al. 2017b [42] | Male healthy untrained participants Age 21.7 ± 2.3 years Height 178.0 ± 6.46 cm Mass 75.1 ± 10.13 kg n = 30 | Parallel | 5 × 20 drop jumps | Beetroot juice (250 mL) Per 250 mL ~400 mg GAE (total phenols) (62). | 3 × servings on day of exercise and 2 × servings for two days post-exercise | MIVC (PE, 24, 48, 72) CMJ (PE, 24, 48, 72) CK, (PE, 24, 48, 72) CRP (PE, 24, 48, 72) |
| Connoll, McHugh and Padilla Zakour 2006 (9) | Male Age 22 ± 4 y ears Height 1.78 ± 0.86 m Mass 90 ± 18 kg n = 16 | Crossover | 2 × 20 eccentric elbow contractions | Tart cherry juice and apple juice blend Per 12 fl oz 600 mg of GAE (total phenols) 40 mg of cyanidin-3-glucoside equivalents (pH differential) | 2 × 12 fl oz bottles for 8 days (3 days pre-exercise, on the day of, and 4 days post-exercise) | MIVC (24, 48, 72, 96) DOMS, (24, 48, 72, 96) |
| Daab et al. 2020 [43] | Male semi-professional soccer players Age 22.1 ± 0.56 years Height 178 ± 1.19 cm Mass 75.8 ± 5.58 kg n = 13 | Crossover | Loughborough intermittent shuttle test | Beetroot juice Polyphenol content not stated | 2 × 150 mL per day for 7 days (3 days pre-exercise, on the day of, and 3 days post-exercise) | MIVC (PE, 24, 48, 72) DOMS (PE, 24, 48, 72) CMJ (PE, 24, 48, 72) CK (PE, 24, 48, 72) CRP (PE, 24, 48, 72) |
| Howatson et al. 2010 [36] | Marathon runners Age 37.5 ± 9 years Height 1.76 ± 0.07 m Mass 73.3 ± 9.85 kg n = 20 (m = 13; f = 7) | Parallel | London Marathon (UK) | Tart cherry juice and apple juice blend 55 mmol·L−1 trolox equivalents (ORAC) Per 12 fl oz 600 mg of GAE (total phenols) 40 mg of cyanidin-3-glucoside equivalents (pH differential) (9). | 2 × 8 fl oz bottles for 8 days (5 days pre-exercise, on the day of, and 2 days post-exercise) | MIVC (PE, 24, 48) DOMS (PE, 24,48) CK (PE, 24, 48) CRP (PE, 24, 48) IL-6 (PE, 24 48) PC (PE, 24, 48) |
| Hutchison et al. 2016 [44] | Healthy participants Age 20.2 ± 0.6 years Height 165.75 ± 3 cm Mass 64.2 ± 5 kg n = 16 (m = 3; f = 13) | Parallel | 3 × 10 eccentric squats | Blackcurrant nectar 7340 μmol trolox equivalents (TEAC) Per 16 fl oz 193.25 mg malvidin glucosides (pH differential) 175.69 mg cyanidin glucosides (pH differential) | 16 fl oz bottle twice per day for 8 days (4 days pre-exercise, on the day of, and 3 days post-exercise) | DOMS (PE, 24, 48, 96) CK (PE, 24, 48, 96) IL-6 (PE, 24, 48, 96) |
| Kuehl et al. 2010 [37] | Healthy runners Age 35.8 ± 9.6 years n = 54 (m = 36; f = 18) | Parallel | Oregon Hood to Coast Relay Race (USA) | Montmorency tart cherry juice and apple juice blend Per 12 fl oz 600 mg of GAE (total phenols) 40 mg of cyanidin-3-glucoside equivalents (pH differential) (9). | 2 × 355 mL tart cherry juice for 8 days (7 days pre-exercise, on the day of the trial) | DOMS (PE) |
| Kupsaravic, McShane and Clifford. 2019 [45] | Elite male rugby union players Age 28 ± 4 years Height 1.88 ± 0.64 m Mass 106.8 ± 7.6 kg n = 10 | Crossover | Rugby Union match | Montmorency tart cherry juice Polyphenol content not stated | 2 × 30 mL concentrate for 5 days (2 days pre-exercise, on the day of, 2 days post-exercise) | DOMS (24, 48, 72) |
| Lamb et al. 2019 [28] | Male non-resistance trained Age 24 IQR 22,33 years BMI 25.6 ± 4 kg m−2 n = 36 | Parallel | 5 × 10 eccentric elbow contractions non dominant arm | Montmorency tart cherry juice and Pomegranate Wonderful juice Tart cherry juice per 30 mL 294.7 ± 14.9 mg GAE (total phenols) 7.7 ± 0.3 mg anthocyanins (pH differential) Pomegranate Wonderful per 250 mL 878.9 ± 92.7 mg GAE (total phenols) 49.4 ± 2.0 mg total anthocyanins (pH differential) | 2 × 30 mL of concentrate for 9 days (cherry) and 2 × 250 mL for 9 days (pomegranate) (4 days pre-exercise, on the day of, 4 days post-exercise) | MIVC (PE, 24, 48, 72, 96) DOMS (PE, 24, 48, 72, 96) CK (PE, 24, 48, 72, 96) |
| Lima et al. 2019 [46] | Healthy male physical education students Age 22.3 ± 2.6 years Height 176.6 ± 6.4 cm Mass 77.1 ± 10.5 kg n = 30 | Parallel | 30 min downhill run at 70% O2max | Anthocyanin-rich antioxidant juice that consisted of a mixture of clarified apple juice with plum, blueberry, maquiberry, raspberry and cranberry 67,680 μmol·mL−1 of trolox equivalents (ORAC) Per 240 mL 58 mg of anthocyanins | 2 × 240 mL for 9 days (4 days pre-exercise, on the day of, 4 days post-exercise) | MIVC (PE, 24, 48, 72. 96) DOMS (24, 48, 72, 96) CK (48, 96) |
| Lynn et al. 2018 [11] | Recreational runners Age 30.9 ± 10.53 years Height 1.74 ± 0.08 m Mass 71.4 ± 10.5 kg BMI 23.5 ± 2.45 kg m−2 n = 21 (m = 16; f = 5) | Parallel | Sheffield Half Marathon (UK) | Bilberry juice Per 200 mL 744.14 ± 81.75 mg of GAE (total phenols) 80.04 ± 3.51 mg of total anthocyanins (pH differential) | 2 × 200 mL for 8 days (5 days pre-exercise, on the day of, 2 days post-exercise) | DOMS (PE, 24, 48) CK (PE, 24, 48) CRP (PE, 24, 48) |
| Machin et al. 2014 [25] | Male non-resistance trained Age 22.3 ± 4.1 years Height 174.9 ± 6.2 cm Mass 73.8 ± 11.5 kg n = 45 | Parallel | 20 min of downhill running and 40 repetitions of bilateral eccentric elbow contractions | Pomegranate Wonderful juice (high 2 × 30 mL vs. low 1 × 30 mL) Per 30 mL 650 mg of GAE consisting of 95.5% ellagitannins, 3.5% ellagic acid, and 1% anthocyanins | 1 or 2 × servings for 8 days (3 days pre-exercise, on the day of, 4 days post-exercise) | MIVC (PE, 24, 48, 72, 96) DOMS (PE, 24, 48, 72, 96) |
| McLeay et al. 2012 [12] | Healthy recreational females Age 22 ± 1 years Height 167 ± 5 cm Mass 62 ± 8 kg n = 14 | Crossover | 3 × 100 eccentric knee extensions | Smoothie with New Zealand blueberries (200 g), banana (~50 g) and apple juice (200 mL) 5417 μmol trolox equivalents (ORAC) Per 100 mL 168 mg of GAE (total phenols) 96.6 mg of anthocyanins 26 mg of phenolic acid 10.2 mg of flavonoids | 3 × servings on the day of exercise and 1 × serving for 2 days post-exercise | MIVC (12, 36, 60) DOMS (12, 36, 60) CK (12, 36, 60) IL-6 (12, 36, 60) PC (12, 36, 60) |
| Morehen et al. 2020 [47] | Male Professional Rugby players Age 18 ± 1 years Height 182 ± 0.04 cm Mass 92.2 ± 8.6 kg n = 11 | Crossover | Rugby Union match | Montmorency tart cherry juice Per 30 mL 320 mg of anthocyanins | 2 × 30 mL concentrate per day for 7 days, (4 days pre-match, on the day of, 2 days post-match) | DOMS (24, 48) CMJ (48) IL-6 (PE, 48) |
| Morgan et al. 2018 [14] | Healthy recreational active males Age 22.8 ± 3.3 years Height 1.84 ± 0.59 cm Mass 85.3 ± 12 kg n = 10 | Crossover | Single leg extension 10 × 10 repetitions at 80% 1RM | Ecuadorian cacao juice (ZumaCacao®) Per 330 mL serving 154 mg of polyphenols 8 mg epicatechin 43 mg catechins 23 mg flavanols 12 mg proanthocyanidins HPLC -Atlas, Bioscience, Inc, Tucson, Arizona, USA | 330 mL per day for 10 days (7 days pre-exercise, on the day of, 2 days post-exercise) | MIVC (PE, 24, 48) DOMS (PE, 24, 48) CMJ (PE, 24, 48) CK (PE, 24, 48) CRP (PE, 24, 48) PC (PE, 24, 48) |
| Peschek et al. 2014 [26] | Male well trained runners and triathletes Age 24.6 ± 5.6 years Height 182.1 ± 6.3 cm Mass 73.4 ± 7 kg Body fat percentage 13.7 ± 5.1% n = 8 | Crossover | 30 min downhill run at 70% O2max | Unsweetened Cocoa Via consisted of cocoa powder, salt, and soy lecithin Per 240 mL 350 mg flavanols | 1 g·kg−1 of body weight of cocoa milk at 1 h and at 2 h post-exercise | MIVC (24, 48) DOMS (24, 48) CK (24, 48) |
| Quinlan and Hill 2020 [48] | Team sport recreational athletes Age 26.5 ± 4.5 years Height 175.3 ± 9.75 cm Mass 70.2 ± 12.85 kg Predicted O2peak 44.4 ± 8.1 mL·kg−1·min−1 n = 20 (m = 8; f = 12) | Parallel | Loughborough intermittent shuttle test followed by 12 × 20 m sprints | Montmorency tart cherry juice Polyphenol content not stated | 2 × 30 mL concentrate for 8 days (5 day pre-exercise, on the day of, 2 days post-exercise) | MIVC (PE, 24, 48) DOMS (PE, 24, 48) CMJ (PE, 24, 48) CK (PE, 24, 48) CRP (PE, 24, 48) |
| Trombold et al. 2011 [10] | Male recreational active Age 21.9 ± 2.4 years Height 179.1 ± 8.4 cm Mass 80.2 ± 7.5 kg n = 17 | Crossover | 3 × 20 eccentric elbow contractions, 6 × 10 eccentric knee contractions | Pomegranate Wonderful juice Per 1000 mL 1979 mg of tannins 384 mg of anthocyanins 121 mg of ellagic acid derivatives (Content obtained from the manufacturer) | 2 × 250 mL for 15 days (8 days pre-exercise, on the day of, 6 days post-exercise) | MIVC (PE, 24, 48, 72, 96) DOMS, (PE, 24, 48, 72, 96) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rickards, L.; Lynn, A.; Harrop, D.; Barker, M.E.; Russell, M.; Ranchordas, M.K. Effect of Polyphenol-Rich Foods, Juices, and Concentrates on Recovery from Exercise Induced Muscle Damage: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 2988. https://doi.org/10.3390/nu13092988
Rickards L, Lynn A, Harrop D, Barker ME, Russell M, Ranchordas MK. Effect of Polyphenol-Rich Foods, Juices, and Concentrates on Recovery from Exercise Induced Muscle Damage: A Systematic Review and Meta-Analysis. Nutrients. 2021; 13(9):2988. https://doi.org/10.3390/nu13092988
Chicago/Turabian StyleRickards, Lee, Anthony Lynn, Deborah Harrop, Margo E. Barker, Mark Russell, and Mayur K. Ranchordas. 2021. "Effect of Polyphenol-Rich Foods, Juices, and Concentrates on Recovery from Exercise Induced Muscle Damage: A Systematic Review and Meta-Analysis" Nutrients 13, no. 9: 2988. https://doi.org/10.3390/nu13092988
APA StyleRickards, L., Lynn, A., Harrop, D., Barker, M. E., Russell, M., & Ranchordas, M. K. (2021). Effect of Polyphenol-Rich Foods, Juices, and Concentrates on Recovery from Exercise Induced Muscle Damage: A Systematic Review and Meta-Analysis. Nutrients, 13(9), 2988. https://doi.org/10.3390/nu13092988