
Prenatal Vitamins and the Risk of Offspring Autism Spectrum Disorder: Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Study Identification and Selection
2.3. Quality Assessment
2.4. Data Synthesis and Analysis
2.5. Meta-Analysis
2.6. Sensitivity Analysis
3. Results
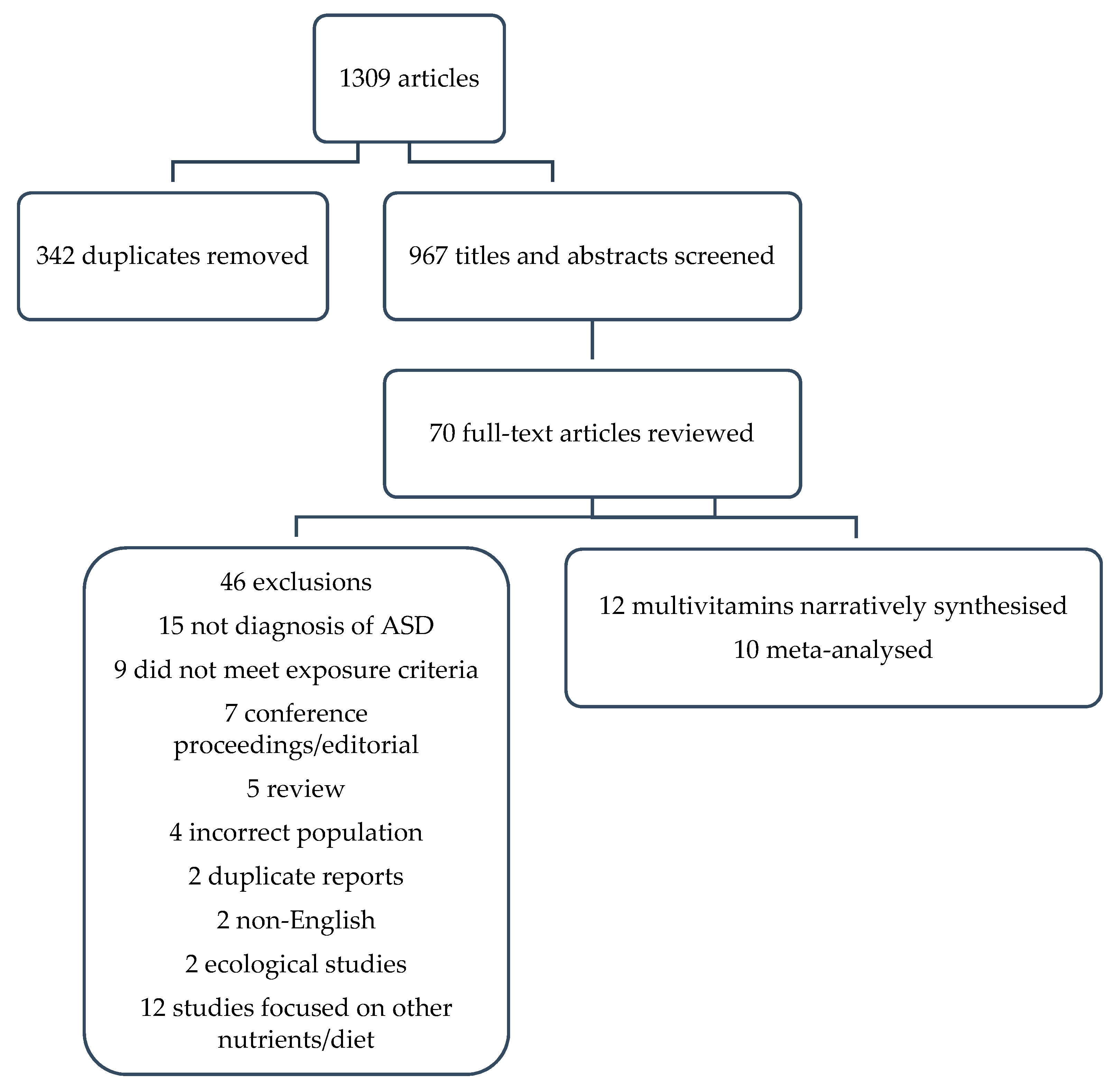
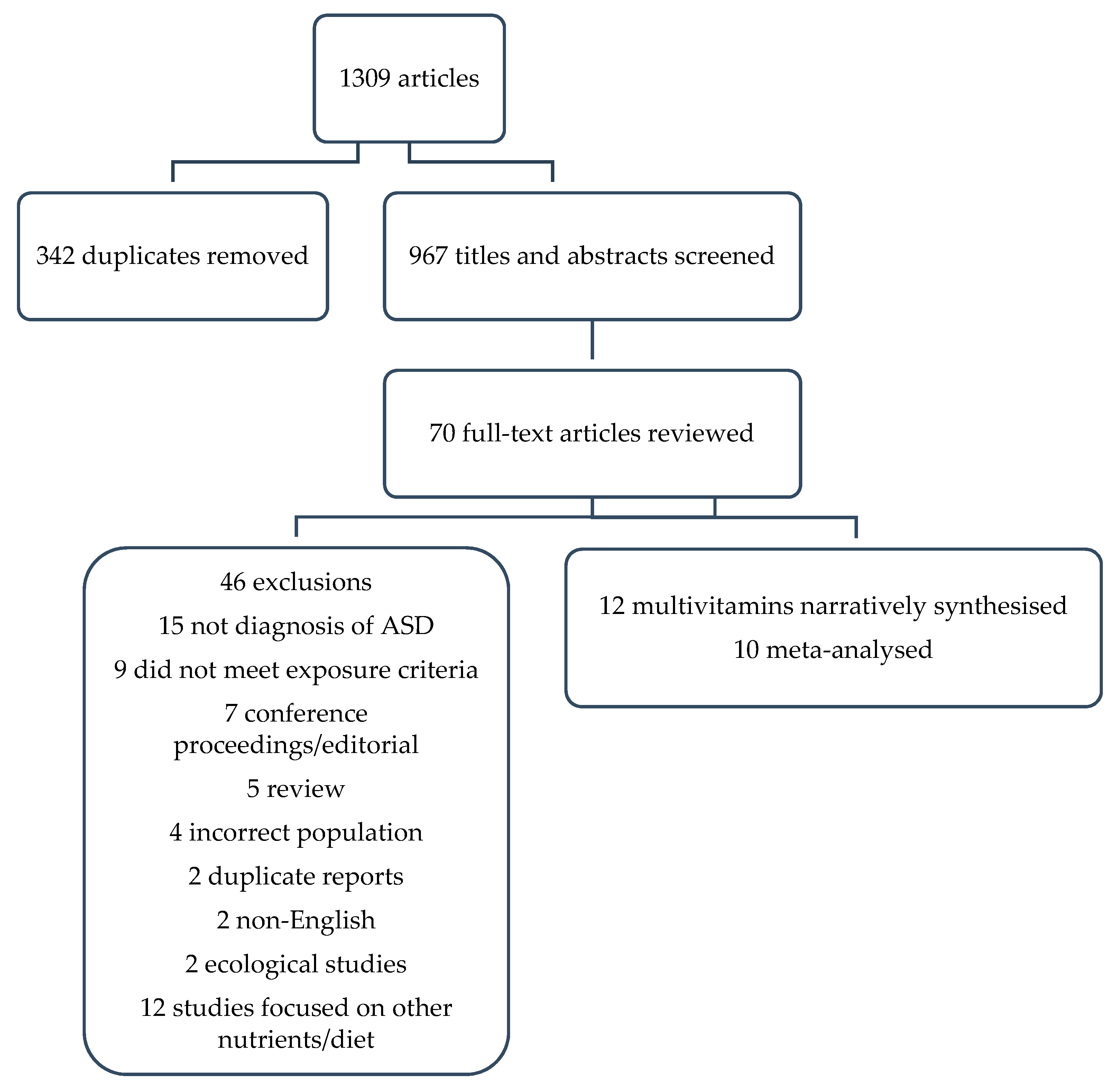
3.1. Identification of Studies
3.2. Quality Assessment
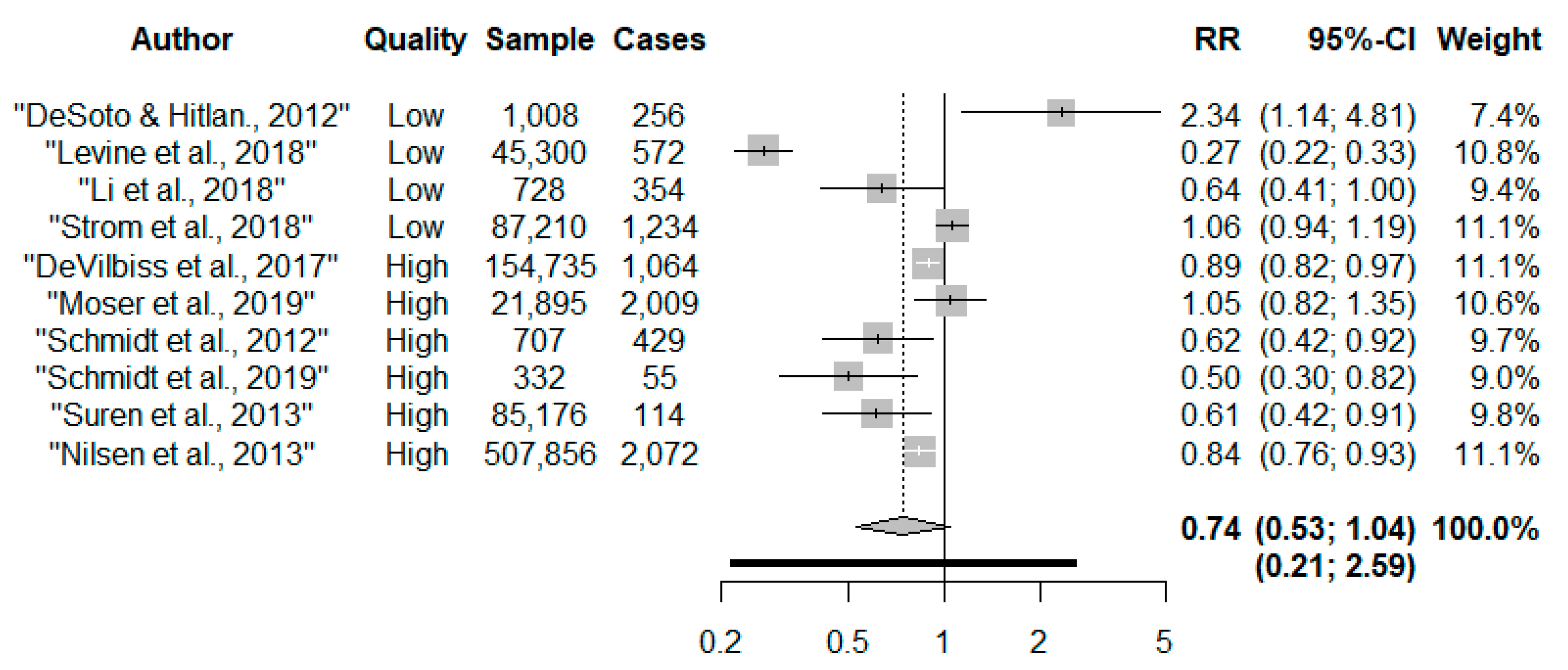
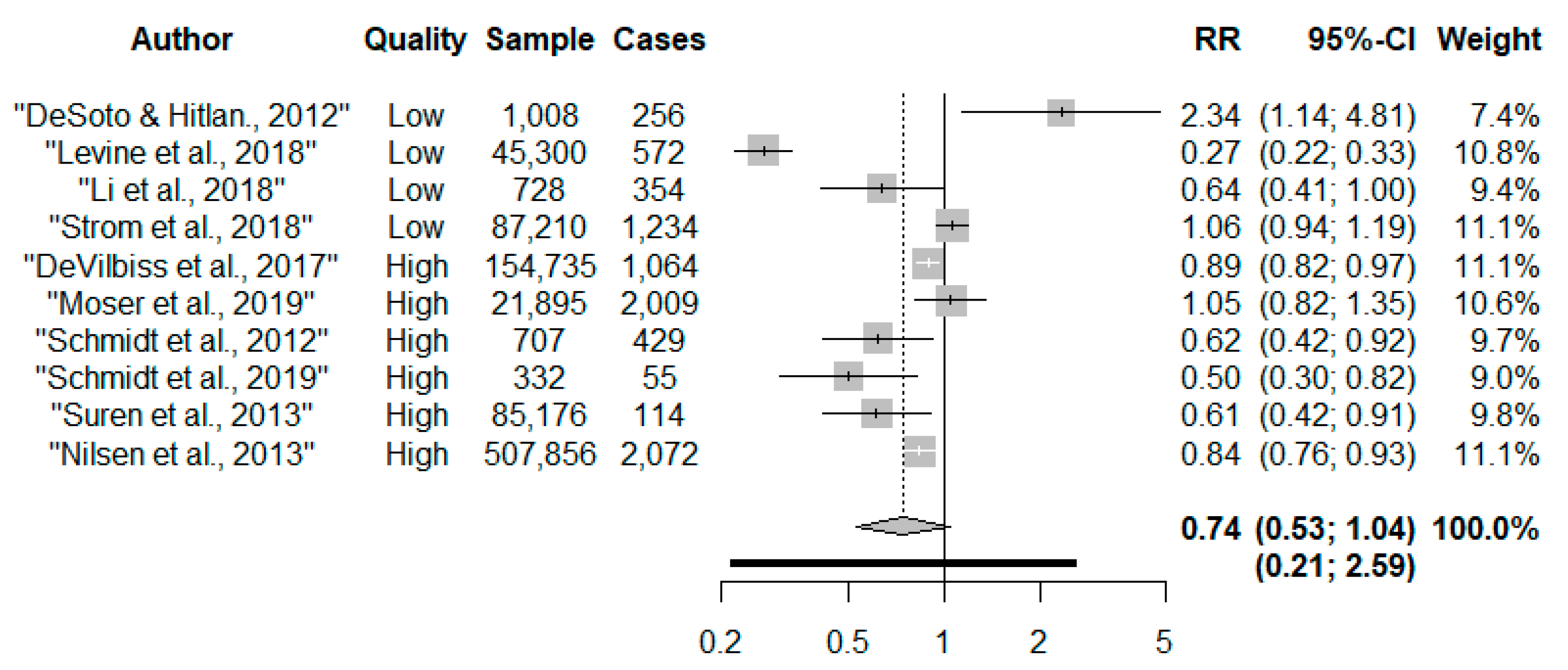
3.3. Meta-Analylic Results
Subgroup Analysis
3.4. Causal Approaches
4. Discussion
4.1. Alternative Causal Approaches
4.1.1. Multivariate Regression
4.1.2. Gene-Nutrient Interaction
4.1.3. Discordant Sibling Analysis
4.1.4. Negative Control
4.1.5. Triangulation
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. International Classification of Diseases and Related Health Problems; 11th rev., ICD-11; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Knapp, M.; Romeo, R.; Beecham, J. Economic cost of autism in the UK. Autism 2009, 13, 317–336. [Google Scholar] [CrossRef]
- Lyall, K.; Croen, L.; Daniels, J.; Fallin, M.D.; Ladd-Acosta, C.; Lee, B.K.; Park, B.Y.; Snyder, N.W.; Schendel, D.; Volk, H.; et al. The Changing Epidemiology of Autism Spectrum Disorders. Annu. Rev. Public Health 2017, 38, 81–102. [Google Scholar] [CrossRef] [Green Version]
- Li, M.; Francis, E.; Hinkle, S.N.; Ajjarapu, A.S.; Zhang, C. Preconception and Prenatal Nutrition and Neurodevelopmental Disorders: A Systematic Review and Meta-Analysis. Nutrients 2019, 11, 1628. [Google Scholar] [CrossRef] [Green Version]
- Guo, B.-Q.; Li, H.-B.; Zhai, D.-S.; Ding, S.-B. Maternal multivitamin supplementation is associated with a reduced risk of autism spectrum disorder in children: A systematic review and meta-analysis. Nutr. Res. 2019, 65, 4–16. [Google Scholar] [CrossRef]
- Kendall, J.M. Designing a research project: Randomised controlled trials and their principles. Emerg. Med. J. 2003, 20, 164–168. [Google Scholar] [CrossRef] [Green Version]
- Lawlor, D.A.; Tilling, K.; Smith, G.D. Triangulation in aetiological epidemiology. Int. J. Epidemiol. 2016, 45, 1866–1886. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Dekkers, O.M.; Vandenbroucke, J.P.; Cevallos, M.; Renehan, A.G.; Altman, D.G.; Egger, M. COSMOS-E: Guidance on conducting systematic reviews and meta-analyses of observational studies of etiology. PLoS Med. 2019, 16, e1002742. [Google Scholar] [CrossRef]
- Guo, B.Q.; Li, H.B.; Zhai, D.S.; Ding, S.B. Association of maternal prenatal folic acid intake with subsequent risk of autism spectrum disorder in children: A systematic review and meta-analysis. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2019, 94, 109650. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Grp, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.; Li, K.; Zhao, D.; Li, L. The association between maternal use of folic acid supplements during pregnancy and risk of autism spectrum disorders in children: A meta-analysis. Mol. Autism 2017, 8, 1–4. [Google Scholar] [CrossRef] [Green Version]
- McKenzie, D.P.; Thomas, C. Relative risks and odds ratios: Simple rules on when and how to use them. Eur. J. Clin. Investig. 2020, 50, e13249. [Google Scholar] [CrossRef] [PubMed]
- Riley, R.D.; Higgins, J.P.; Deeks, J.J. Interpretation of random effects meta-analyses. BMJ 2011, 342, d549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IntHout, J.; Ioannidis, J.P.A.; Rovers, M.M.; Goeman, J.J. Plea for routinely presenting prediction intervals in meta-analysis. BMJ Open. 2016, 6, e010247. [Google Scholar] [CrossRef] [Green Version]
- Gordon, M.; Lumley, T. Advanced Forest Plot Using ‘grid’ Graphics, December 12, 2020. R Package Version 1.10 ed.: CRAN. Available online: https://cran.r-project.org/web/packages/forestplot/forestplot.pdf (accessed on 23 July 2021).
- Duval, S.; Tweedie, R. Trim and Fill: A Simple Funnel-Plot-Based Method of Testing and Adjusting for Publication Bias in Meta-Analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Virk, J.; Liew, Z.; Olsen, J.; Nohr, E.A.; Catov, J.M.; Ritz, B. Preconceptional and prenatal supplementary folic acid and multivitamin intake and autism spectrum disorders. Autism 2016, 20, 710–718. [Google Scholar] [CrossRef] [PubMed]
- Strøm, M.; Granström, C.; Lyall, K.; Ascherio, A.; Olsen, S.F. Research letter: Folic acid supplementation and intake of folate in pregnancy in relation to offspring risk of autism spectrum disorder. Psychol. Med. 2018, 48, 1048–1054. [Google Scholar] [CrossRef] [Green Version]
- Raghavan, R.; Riley, A.W.; Volk, H.; Caruso, D.; Hironaka, L.; Sices, L.; Hong, X.; Wang, G.; Ji, Y.; Brucato, M.; et al. Maternal Multivitamin Intake, Plasma Folate and Vitamin B12 Levels and Autism Spectrum Disorder Risk in Offspring. Paediatr. Perinat. Epidemiol. 2018, 32, 100–111. [Google Scholar] [CrossRef]
- Tan, M.; Yang, T.; Zhu, J.; Li, Q.; Lai, X.; Li, Y.; Tang, T.; Chen, J.; Li, T. Maternal folic acid and micronutrient supplementation is associated with vitamin levels and symptoms in children with autism spectrum disorders. Reprod. Toxicol. 2020, 91, 109–115. [Google Scholar] [CrossRef]
- DeVilbiss, E.A.; Magnusson, C.; Gardner, R.M.; Rai, D.; Newschaffer, C.J.; Lyall, K.; Dalman, C.; Lee, B.K. Antenatal nutritional supplementation and autism spectrum disorders in the Stockholm youth cohort: Population based cohort study. Br. Med. J. 2017, 359, J4273. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, R.J.; Iosif, A.-M.; Angel, E.G.; Ozonoff, S. Association of Maternal Prenatal Vitamin Use With Risk for Autism Spectrum Disorder Recurrence in Young Siblings. JAMA Psychiatry 2019, 76, 391–398. [Google Scholar] [CrossRef]
- Suren, P.; Roth, C.; Bresnahan, M.; Haugen, M.; Hornig, M.; Hirtz, D.; Lie, K.K.; Lipkin, W.I.; Mangus, P.; Reichborn-Kjennerud, T.; et al. Association Between Maternal Use of Folic Acid Supplements and Risk of Autism Spectrum Disorders in Children. JAMA J. Am. Med Assoc. 2013, 309, 570–577. [Google Scholar] [CrossRef] [Green Version]
- Nilsen, R.M.; Gunnes, N.; Alsaker, E.R.; Bresnahan, M.; Hirtz, D.; Hornig, M.; Lie, K.K.; Lipkin, W.I.; Mangus, P.; Reichborn-Kjennerud, T.; et al. Analysis of self-selection bias in a population-based cohort study of autism spectrum disorders. Paediatr. Perinat. Epidemiol. 2013, 27, 553–563. [Google Scholar] [CrossRef] [Green Version]
- Levine, S.Z.; Kodesh, A.; Viktorin, A.; Smith, L.; Uher, R.; Reichenberg, A.; Sadin, S. Association of Maternal Use of Folic Acid and Multivitamin Supplements in the Periods Before and During Pregnancy with the Risk of Autism Spectrum Disorder in Offspring. JAMA Psychiatry 2018, 75, 176–184. [Google Scholar] [CrossRef] [Green Version]
- Moser, S.S.; Davidovitch, M.; Rotem, R.S.; Chodick, G.; Shalev, V.; Koren, G. High dose folic acid during pregnancy and the risk of autism; The birth order bias: A nested case-control study. Reprod. Toxicol. 2019, 89, 173–177. [Google Scholar] [CrossRef]
- Schmidt, R.J.; Tancredi, D.J.; Ozonoff, S.; Hansen, R.L.; Hartiala, J.; Allayee, H.; Schmidt, L.C.; Tassone, F.; Hertz-Picciotto, I. Maternal periconceptional folic acid intake and risk of autism spectrum disorders and developmental delay in the CHARGE (CHildhood Autism Risks from Genetics and Environment) case-control study. Am. J. Clin. Nutr. 2012, 96, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Desoto, M.C.; Hitlan, R.T. Synthetic folic acid supplementation during pregnancy may increase the risk of developing autism. J. Pediat. Biochem. 2012, 2, 251–261. [Google Scholar]
- Li., Y.-M.; Shen, Y.-D.; Li, Y.-J.; Xun, G.-L.; Liu, H.; Wu, R.-R.; Xia, K.; Zhao, J.-P.; Ou, J.-J. Maternal dietary patterns, supplements intake and autism spectrum disorders A preliminary case-control study. Medicine 2018, 97, e13902. [Google Scholar] [CrossRef]
- Iglesias Vazquez, L.; Canals, J.; Arija, V. Review and meta-analysis found that prenatal folic acid was associated with a 58% reduction in autism but had no effect on mental and motor development. Acta Paediatr. Int. J. Paediatr. 2019, 108, 600–610. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Sultan, S.; Glasziou, P.; Akl, E.A.; Alonso-Coello, P.; Atkins, D.; Kunz, R.; Brozek, J.; Montori, V.; et al. GRADE guidelines: 9. Rating up the quality of evidence. J. Clin. Epidemiol. 2011, 64, 1311–1316. [Google Scholar] [CrossRef]
- Virk, J.; Liew, Z.; Olsen, J.; Nohr, E.A.; Catov, J.M.; Ritz, B. Pre-conceptual and prenatal supplementary folic acid and multivitamin intake, behavioral problems, and hyperkinetic disorders: A study based on the Danish National Birth Cohort (DNBC). Nutr. Neurosci. 2018, 21, 352–360. [Google Scholar] [CrossRef] [Green Version]
- Scientific Committee on Food, Scientific Panel on Dietetic Products Nutrition and Allergies. Tolerable Upper Intake Levels for Vitamins and Minerals; European Food Safety Authority: Parma, Italy, 2006. [Google Scholar]
- Milman, N.; Byg, K.E.; Hvas, A.M.; Bergholt, T.; Eriksen, L. Erythrocyte folate, plasma folate and plasma homocysteine during normal pregnancy and postpartum: A longitudinal study comprising 404 Danish women. Eur. J. Haematol. 2006, 76, 200–205. [Google Scholar] [CrossRef]
- Ohrvik, V.; Lemming, E.W.; Nalsen, C.; Becker, W.; Ridefelt, P.; Lindroos, A.K. Dietary intake and biomarker status of folate in Swedish adults. Eur. J. Nutr. 2018, 57, 451–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilsen, R.M.; Vollset, S.E.; Monsen, A.L.; Ulvik, A.; Haugen, M.; Meltzer, H.M.; Magnus, P.; Ueland, P.M. Infant birth size is not associated with maternal intake and status of folate during the second trimester in Norwegian pregnant women. J. Nutr. Nutr. Epidemiol. 2010, 140, 572–579. [Google Scholar] [CrossRef]
- Pfeiffer, C.M.; Hughes, J.P.; Lacher, D.A.; Bailey, R.L.; Berry, R.J.; Zhang, M.; Yetley, E.A.; Rader, J.I.; Sempos,, C.T.; Johnson, C.L.; et al. Estimation of trends in serum and RBC folate in the US population from pre- to postfortification using assay-adjusted data from the NHANES 1988-2010. J. Nutr. 2012, 142, 886–893. [Google Scholar] [CrossRef] [PubMed]
- Wiens, D.; DeSoto, M.C. Is High Folic Acid Intake a Risk Factor for Autism?—A Review. Brain Sci. 2017, 7, 149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scientific Advisory Committee on Nutrition (SACN). Folic Acid: Updated SACN Recommendations; Public Health England: London, UK, 2017. [Google Scholar]
- Koren, G.; Moser, S.S. Does high-dose gestational folic acid increase the risk for autism? The birth order hypothesis. Med. Hypotheses 2019, 132, 109350. [Google Scholar] [CrossRef]
- Stephenson, J.H.N.; Hall, J.; Schoenaker, D.A.J.M.; Hutchinson, J.; Cade, J.E.; Poston, L.; Barrett, G.; Crozier, S.R.; Barker, M.; Kumaran, K.; et al. Before the beginning: Nutrition and lifestyle in the preconception period and its importance for future health. Lancet 2018, 391, 1830–1841. [Google Scholar] [CrossRef]
- Whitehouse, A.J.O.; Stanley, F.J. Is autism one or multiple disorders? Med. J. Aust. 2013, 198, 3. [Google Scholar] [CrossRef] [PubMed]
- Pu, D.; Shen, Y.; Wu, J. Association between MTHFR Gene Polymorphisms and the Risk of Autism Spectrum Disorders: A Meta-Analysis. Autism Res. 2013, 6, 384–392. [Google Scholar] [CrossRef]
- Frisell, T.; Oberg, S.; Kuja-Halkola, R.; Sjolander, A. Sibling Comparison Designs Bias from Non-Shared Confounders and Measurement Error. Epidemiology 2012, 23, 713–720. [Google Scholar] [CrossRef] [Green Version]
- Shi, X.; Miao, W.; Tchetgen, E.T.A. A Selective Review of Negative Control Methods in Epidemiology. Curr. Epidemiol. Rep. 2020, 7, 190–202. [Google Scholar] [CrossRef]
- Lyall, K.; Munger, K.L.; O’Reilly, E.J.; Santangelo, S.L.; Ascherio, A. Maternal Dietary Fat Intake in Association With Autism Spectrum Disorders. Am. J. Epidemiol. 2013, 178, 209–220. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.M. Relationship between Neonatal Vitamin D at Birth and Risk of Autism Spectrum Disorders: The NBSIB Study. J. Bone Miner. Res. 2018, 33, 458–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]

{kind=link}
{kind=link}
| Search String | Search Terms |
|---|---|
| Population | (Pregnancy OR Fetal development OR Prenatal).af. OR Fetal development/OR “fetal development”.af. OR “fetal programming”.af OR “fetal programing”.af |
| Exposure | NUTRITIONAL PHYSIOLOGICAL PHENOMENA OR Prenatal Nutritional Physiological Phenomena/OR Maternal nutritional physiological phenomena/OR DIET OR nutri* OR vitamin OR diet* OR mineral OR Nutritional Status |
| Study | Cases/Total Sample | RR | 95% CI | Quality of Evidence (GRADE) |
|---|---|---|---|---|
| 7 cohort/5 case-control | 8761/1,025,534 | 0.74 | 0.53, 1.04 | very low |
| Author/Study Design | Country/Cohort/Sample | Exposure Measure (S) | Outcome Measure | Covariates a | Results Effect Size Estimate and 95% CI | |
|---|---|---|---|---|---|---|
| Desoto and Hitlan, 2012 [29]/case-control | USA 256 cases and 752 controls, age range 6–12 years | Self-reported FA or multivitamin supplement use obtained from health records | ICD-9 | Child; anaemia, pica, sex, birth weight, birth order, year of birth, breast feeding, sex and FA interaction Maternal; age, poverty ratio, adequacy of prenatal care, cholesterol screen, pap smear, prenatal alcohol use, prenatal viral infections, lead exposure | Reference, no supplement use | |
| FA/multivitamin | ||||||
| HR 2.34 | 1.14, 4.82 | |||||
| DeVilbiss et al., 2017 [22]/population-based cohort and sibling case control | Sweden/Stockholm youth cohort 273,107/1064 cases age range 4–15 years | Self-reported multivitamin supplement use recorded by midwife at first booking | DSM-IV or ICD-10 | Child; sex, birth year, and years of residence in Stockholm County Maternal; country of birth, maternal education, disposable family income, age, parity, smoking, BMI at first antenatal visit, neurologic or psychiatric conditions before the child’s birth (anxiety disorders, autism, bipolar disorder, depression, intellectual disability, non-affective psychosis, stress related disorders, epilepsy), antiepileptics and antidepressants medication Sibling analysis child sex and birth year, maternal parity | Reference, no supplement use | |
| Multivitamin | ||||||
| OR 0.89 | 0.82, 0.97 | |||||
| Sibling analysis, multivitamin | ||||||
| OR 0.95 | 0.81, 1.13 | |||||
| Propensity score matching | ||||||
| OR 0.86 | 0.78, 0.95 | |||||
| Levine et al., 2018 [26]/nested case-control | Israel/Meuhedet population based register 572 cases and 45,300 controls average age 10 years (SD 1.4) | Pharmacy records, Multivitamins and/or FA supplements | ICD-9 | Child; sex, birth year Maternal; parity, socioeconomic status (high vs low), psychiatric diagnosis by childbirth, age Paternal psychiatric diagnosis, age | Reference, no supplement use | |
| FA/multivitamins | ||||||
| RR 0.27 | 0.22, 0.33 | |||||
| Negative control | ||||||
| Reference, no supplement use | ||||||
| Multivitamin use 2 years prior to pregnancy | ||||||
| 0.12 | 0.07, 0.20 | |||||
| Li et al., 2018 [30]/case control | China/Autism clinical and environmental database 354 cases and 374 controls, average age 4.5 years | Self-reported FA supplements | DSM-IV-TR | Child; age, premature birth, gender Maternal; pre-pregnancy BMI preconception and predelivery, mode of delivery Parental; age, education Dietary patterns were additionally adjusted for other dietary patterns FA and calcium supplements: were additionally adjusted for other supplements. | Reference, no supplement use | |
| FA | ||||||
| OR 0.64 | 0.41, 1.00 | |||||
| Moser et al., 2019 [27]/nested case-control | Israeli/Maccabi Healthcare Services 2009 cases and 19,886 controls | Dispensing records for FA with or without multivitamins supplements | DSM, version unreported | Child: sex, birth year, birth order Maternal: age, region of residence, poverty index, number of physician visits, diabetes mellitus, hypertension, cardiovascular disease, cancer, subfertility, epilepsy, antifolate medication (proguanil, methotrexate, sulfasalazine, sulphamethoxazole and trimethoprim, pyrimethamine, valproate, carbamazepine, phenytoin and phenobarbital) Final model adjusted for; maternal age, subfertility, number of physician visits, birth order, parity | Reference, ≤0.2 mg/day | |
| FA supplement | ||||||
| 0.2–<0.4 mg/day | ||||||
| OR 1.15 | 0.98, 1.24 | |||||
| 0.4–<1 mg/day | ||||||
| OR 1.10 | 0.98, 1.24 | |||||
| 1 < 3 mg/day | ||||||
| OR 1.14 | 0.98, 1.34 | |||||
| ≥3 mg/day | ||||||
| OR 1.01 | 0.60, 1.70 | |||||
| Raghavan et al., 2018 [20]/prospective cohort | USA/Boston Medical Centre 1257/86 cases, aged up to 9 year | Self-reported maternal multivitamin supplement use | ICD-9 | Child; sex, gestational age birth year Maternal; homocysteine, race, age, smoking status, diabetes, reduction, parity, MTHFR 677 genotype, BMI | Reference, multivitamins 2–5 times/week | |
| First trimester ≤ 2/week | ||||||
| HR 3.4 | 1.6, 7.2 | |||||
| >5/week | ||||||
| HR 2.3 | 1.2, 3.9 | |||||
| Second trimester ≤ 2/week | ||||||
| HR 3.8 | 1.8, 8.0 | |||||
| >5/week | ||||||
| HR 2.1 | 1.2, 3.6 | |||||
| Third trimester | ||||||
| ≤2/week | ||||||
| HR 3.5 | 1.7, 7.4 | |||||
| >5/week | ||||||
| HR 2.1 | 1.2, 3.6 | |||||
| Schmidt et al., 2019 [23]/prospective cohort | USA/Markers of Autism Risk in Babies: Learning Early Signs (MARBLES) 332/55 cases, average age 36.5 months | Self-reported multivitamin supplement use obtained through three telephone interviews | Autism Diagnostic Observation Schedule and DSM-5 | Child; birthplace, sex, year of birth Maternal; education, age, pre-pregnancy BMI, planned pregnancy, race/ethnicity, home ownership, insurance delivery type. Paternal; age Covariates in final model, maternal characteristics (education, age, insurance delivery type) and child characteristics (race) | Reference, no supplement use | |
| Multivitamin | ||||||
| RR 0.50 | ||||||
| Schmidt et al 2012 [28]/case control | USA/Childhood autism risks from genetics and environment (CHARGE) 429 cases and 278 controls age range 24–60 months | Self-reported obtained FA intake based on supplements, including multivitamin supplements, and fortified breakfast cereals, shakes and bars obtained via telephone interview | Health records and Autism Diagnostic Interview–Revised and the Autism Diagnostic Observation Schedule–Generic | Child; birth year, sex, race Maternal; race, age, education, pre-pregnancy BMI, birthplace, residing with a smoker, smoking status, alcohol consumption, other nutrients intakes (calcium, iron, vitamin A, B6, B12, C, D and E) Preeclampsia, type of delivery, vaginal bleeding during pregnancy, induced labour Paternal: age Covariates in final model; childbirth year and maternal education | Reference, no supplement use | |
| All strata combined | ||||||
| OR 0.62 | 0.42, 0.92 | |||||
| Strata by C/T genotypes | ||||||
| maternal CC | ||||||
| OR 1.20 | 0.61, 2.34 | |||||
| maternal CT/TT | ||||||
| OR 0.46 | 0.25, 0.85 | |||||
| child CC | ||||||
| OR 1.15 | 0.55, 2.38 | |||||
| child CT/TT | ||||||
| OR 0.48 | 0.27, 0.88 | |||||
| both mother & child | ||||||
| OR 1.29 | 0.54, 3.10 | |||||
| either mother or child CT/TT | ||||||
| OR 0.49 | 0.16, 1.50 | |||||
| both mother and child CT/TT | ||||||
| OR 0.30 | 0.10, 0.90 | |||||
| Suren et al., 2013 [24]/prospective cohort | Norway/Norwegian mother, father and child cohort (MoBa) 85,176/114 cases, mean age of 6.4 years | Self-reported questionnaire responses, multivitamin and mineral supplement, FA supplement | DSM-IV or ICD-10 | Child; birth year Maternal; planned pregnancy, smoking, BMI, parity, weight gain at 18 and 30 weeks Parental; education, age Covariates retained in final model; birth year, parity and maternal education | Reference, no supplement use | |
| FA/multivitamins | ||||||
| OR 0.61 | 0.41, 0.90 | |||||
| Negative control | ||||||
| Reference, no fish oils supplements | ||||||
| Fish oil supplements | ||||||
| OR 1.29 | 0.88, 1.89 | |||||
| Strom et al., 2017 [19]/prospective cohort | Denmark/Danish National Birth Cohort 87,210/1234 cases, age range 11–17 years | Self-reported folate/FA, vitamin and mineral supplement use, reported during GP interview | ICD-10 | Child; sex Maternal; age, parity, smoking, education, socioeconomic status (based on occupation and education), planned pregnancy, pre-pregnancy BMI Paternal; age | Reference, no supplement use | |
| FA/multivitamins | ||||||
| HR 1.06 | 0.94, 1.19 | |||||
| Tan et al., 2020 [21]/case- control | China 416 cases and 201 control mean age 4.68 years cases, 4.47 years controls | Self-reported FA or micronutrient supplements | DSM-5 | Child; age, sex, gestational age, birth weight Maternal; residence (rural/urban), labour mode Paternal; age Household; income | Reference, supplement use | |
| No FA supplements | ||||||
| 1.91 | 1.24, 2.93 | |||||
| No micronutrient supplements | ||||||
| 1.72 | 1.20, 2.47 | |||||
| Nilsen et al., 2013 [25]/population based cohort | Norway/Norwegian registry 507,856/2072 cases, mean age 7 years | Self-reported FA intake obtained via maternal health records | ICD-10 | Child; birth year Maternal; age, marital status, parity, hospital size Paternal; age | Reference, no supplement use | |
| FA | ||||||
| OR 0.86 | 0.78, 0.95 | |||||
| Study | Design | Sample Size Cases/Controls or Children (Cases) | Multivariate Regression/GEE | Causal Diagram | Propensity Score | Sibling Study | Negative Control | Genetic Studies |
|---|---|---|---|---|---|---|---|---|
| Folic acid/multivitamins | ||||||||
| Desoto and Hitlan, 2012 (taking supplements) | Case-control | 256/752 | ▼ | |||||
| DeVilbiss et al., 2017 (taking supplements) | Cohort | 273,107 (1064) | ▲ | ▲ | Δ | |||
| Levine et al., 2018 (taking supplements) | Cohort | 45,300 (572) | ▲ | ▲ b | ||||
| Li et al., 2018 (taking supplements) | Case-control | 354/374 | ▲ | |||||
| Moser et al., 2019 (taking supplements) | Case-control | 2009/19,886 | Δ | |||||
| Nilsen et al., 2013 (taking supplements) | Cohort | 507,856 (2072) | ▲ | |||||
| Raghavan et al., 2017 a (taking supplements < twice/week or taking supplements > five times/week) | Cohort | 1257 (86) | ▼ | |||||
| Schmidt et al., 2019 (taking supplements) | Cohort | 241 (55) | ▲ | |||||
| Schmidt et al., 2012 (taking supplements) | Case-control | 429/278 | ▲ | ▲ c | ||||
| Suren et al., 2013 (taking supplements) | Cohort | 85,176 (114) | ▲ | ∇ d | ||||
| Strom et al., 2017 (taking supplements) | Cohort | 87,210 (1234) | ∇ | |||||
| Tan et al., 2020 (not taking supplements) | Case-control | 416/201 | ▲ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Friel, C.; Leyland, A.H.; Anderson, J.J.; Havdahl, A.; Borge, T.; Shimonovich, M.; Dundas, R. Prenatal Vitamins and the Risk of Offspring Autism Spectrum Disorder: Systematic Review and Meta-Analysis. Nutrients 2021, 13, 2558. https://doi.org/10.3390/nu13082558
Friel C, Leyland AH, Anderson JJ, Havdahl A, Borge T, Shimonovich M, Dundas R. Prenatal Vitamins and the Risk of Offspring Autism Spectrum Disorder: Systematic Review and Meta-Analysis. Nutrients. 2021; 13(8):2558. https://doi.org/10.3390/nu13082558
Chicago/Turabian StyleFriel, Catherine, Alastair H. Leyland, Jana J. Anderson, Alexandra Havdahl, Tiril Borge, Michal Shimonovich, and Ruth Dundas. 2021. "Prenatal Vitamins and the Risk of Offspring Autism Spectrum Disorder: Systematic Review and Meta-Analysis" Nutrients 13, no. 8: 2558. https://doi.org/10.3390/nu13082558
APA StyleFriel, C., Leyland, A. H., Anderson, J. J., Havdahl, A., Borge, T., Shimonovich, M., & Dundas, R. (2021). Prenatal Vitamins and the Risk of Offspring Autism Spectrum Disorder: Systematic Review and Meta-Analysis. Nutrients, 13(8), 2558. https://doi.org/10.3390/nu13082558