
Endovascular Bariatric Surgery as Novel Minimally Invasive Technique for Weight Management in the Morbidly Obese: Review of the Literature

 , , , ,
, , , ,
Abstract
:1. Introduction
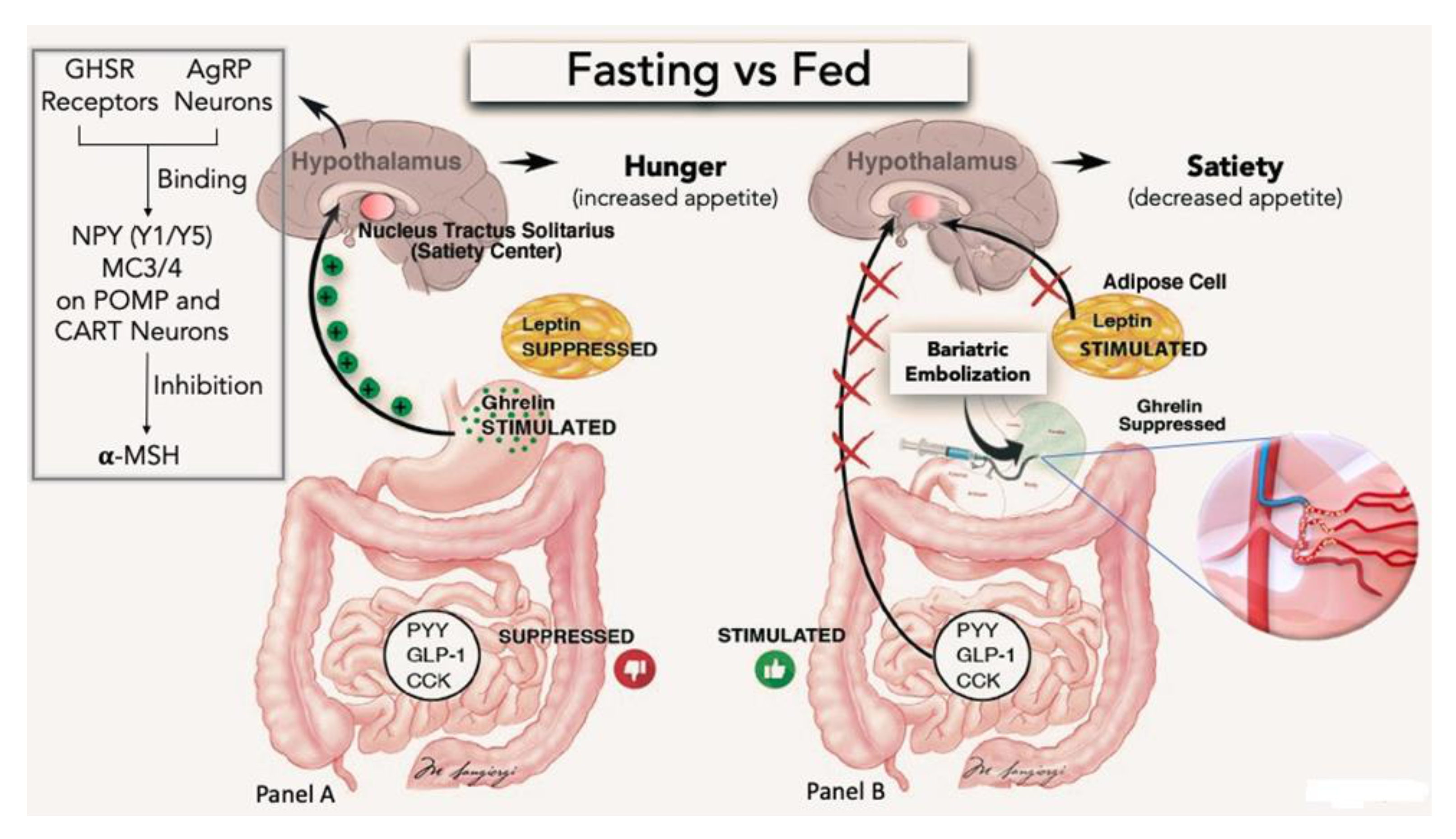
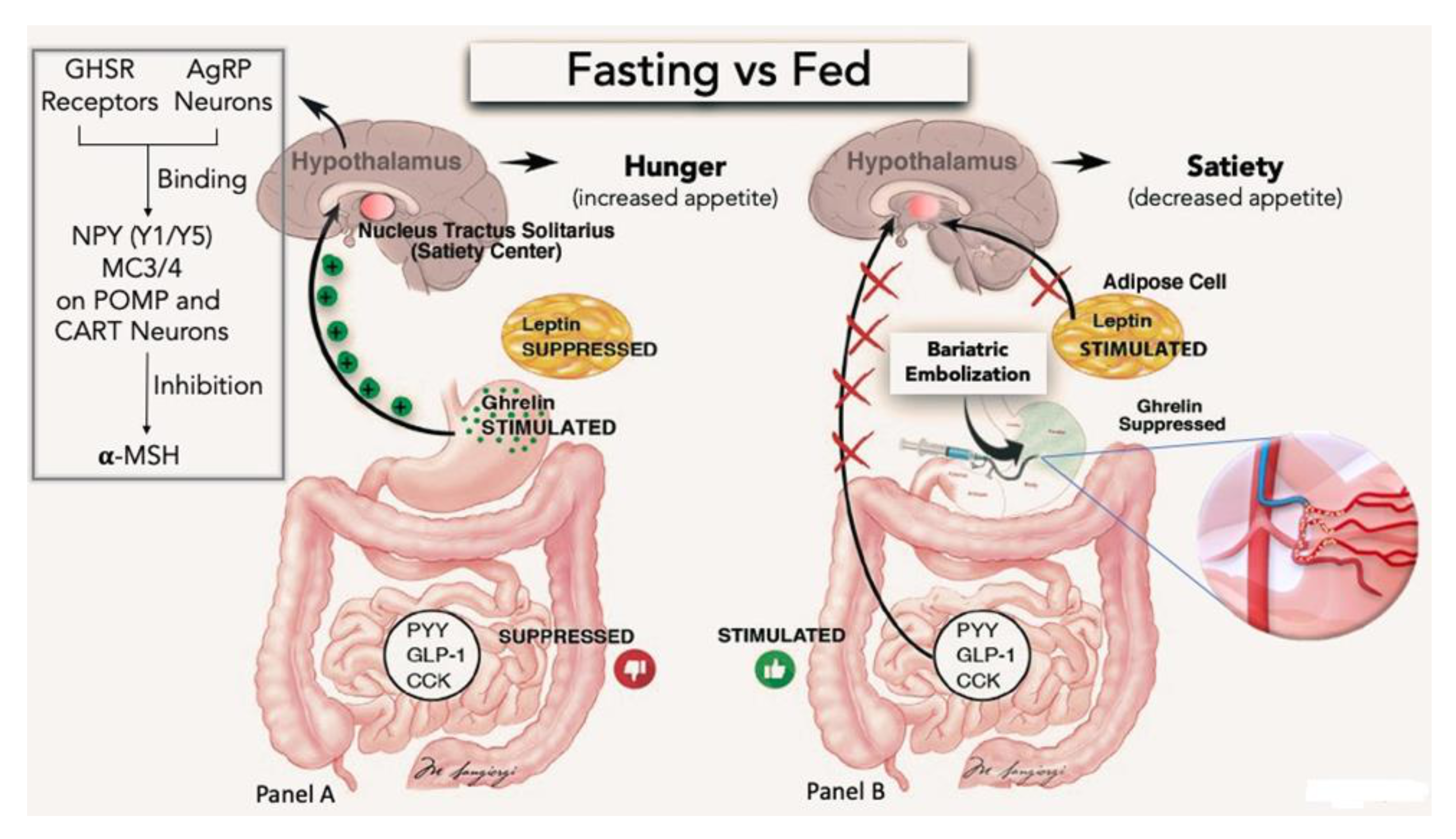
2. Pathophysiological Basis for EBS
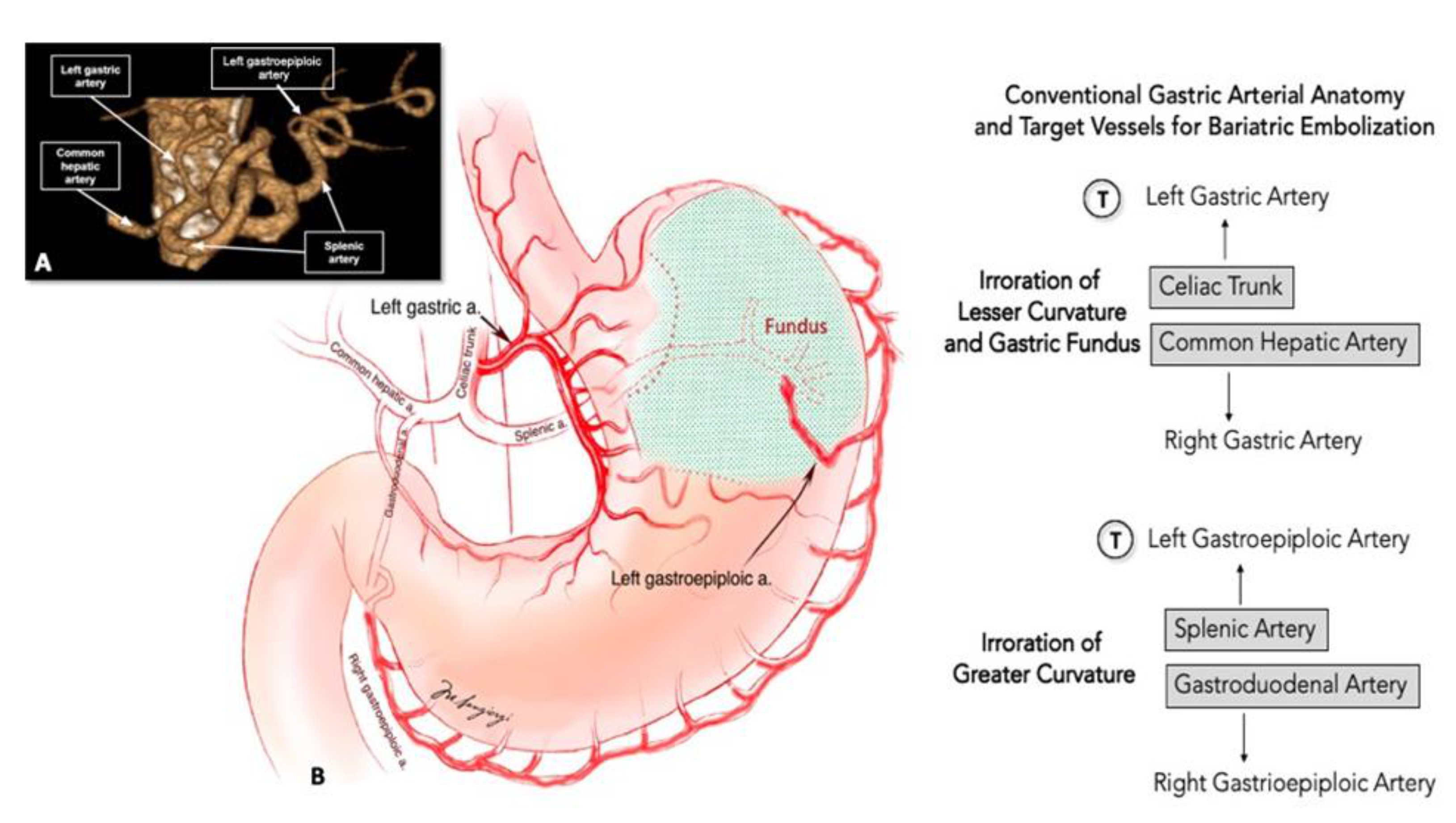
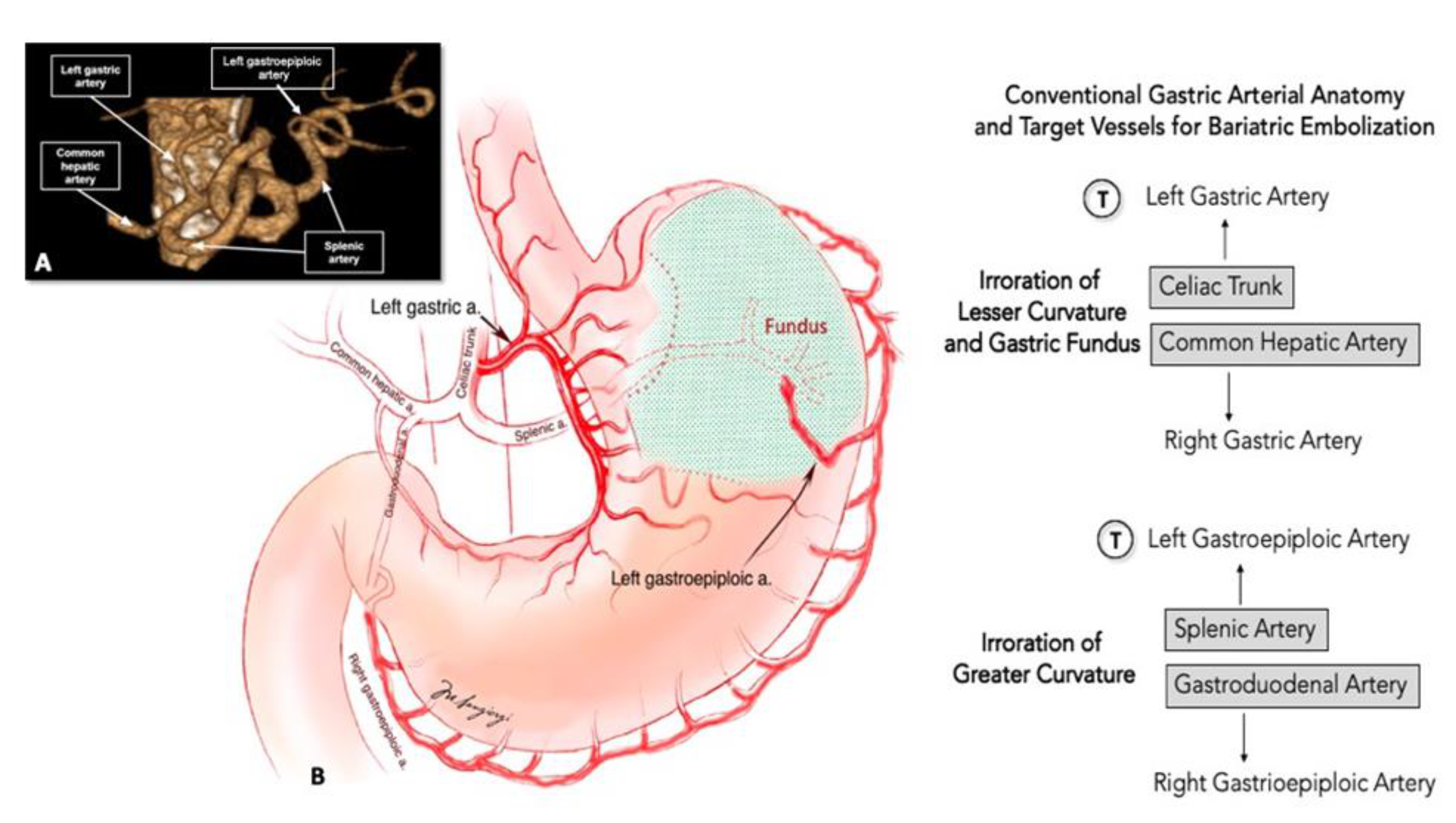
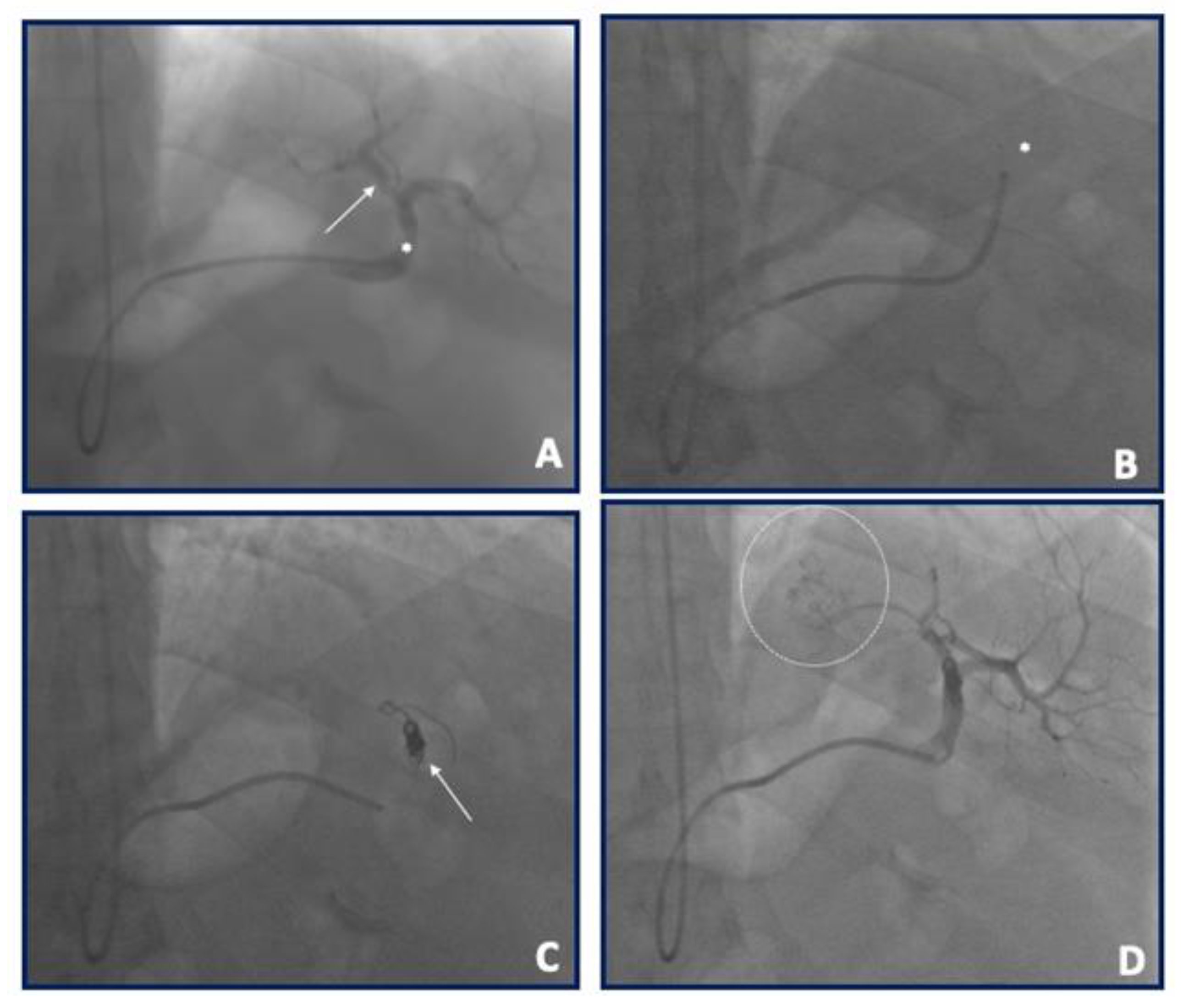
3. EBS Procedure
4. EBS Preclinical Evidence
5. EBS Human Clinical Evidence
6. Current and Future Perspectives
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Flegal, K.M.; Kit, B.K.; Orpana, H.; Graubard, B.I. Association of all-cause mortality with overweight and obesity using standard body mass index categories: A systematic review and meta-analysis. JAMA 2013, 309, 71–82. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.D.; Basu, A. Estimating the medical care costs of obesity in the united states: Systematic review, meta-analysis, and empirical analysis. Value Health 2016, 19, 602–613. [Google Scholar] [CrossRef] [Green Version]
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Obesity Society. Circulation 2014, 129, S102–S138. [Google Scholar] [CrossRef] [Green Version]
- Lupoli, R.; Lembo, E.; Saldalamacchia, G.; Avola, C.K.; Angrisani, L.; Capaldo, B. Bariatric surgery and long-term nutritional issues. World J. Diabetes 2017, 8, 464–474. [Google Scholar] [CrossRef]
- Fujioka, K. Follow-up of nutritional and metabolic problems after bariatric surgery. Diabetes Care 2005, 28, 481–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangan, A.; Le Roux, C.W.; Miller, N.G.; Docherty, N.G. Iron and Vitamin D/Calcium Deficiency after Gastric Bypass: Mechanisms Involved and Strategies to Improve Oral Supplement Disposition. Curr. Drug Metab. 2019, 20, 244–252. [Google Scholar] [CrossRef]
- Di Lorenzo, N.; Antoniou, S.A.; Batterham, R.L.; Busetto, L.; Godoroja, D.; Iossa, A.; Carrano, F.M.; Agresta, F.; Alarçon, I.; Azran, C.; et al. Clinical practice guidelines of the European Association for Endoscopic Surgery (EAES) on bariatric surgery: Update 2020 endorsed by IFSO-EC, EASO and ESPCOP. Surg. Endosc. 2020, 34, 2332–2358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bai, Z.-B.; Qin, Y.-L.; Deng, G.; Zhao, G.-F.; Zhong, B.-Y.; Teng, G.-J. Bariatric embolization of the left gastric arteries for the treatment of obesity: 9-month data in 5 patients. Obes. Surg. 2018, 28, 907–915. [Google Scholar] [CrossRef] [PubMed]
- Elens, S.; Roger, T.; Elens, M.; Rommens, J.; Sarafidis, A.; Capelluto, E.; Delcour, C. Gastric embolization as treatment for overweight patients; Ef-ficacy and safety. Cardiovasc. Interv. Radiol. 2019, 42, 513–519. [Google Scholar] [CrossRef]
- Hafezi-Nejad, N.; Bailey, C.R.; Weiss, C.R. Bariatric embolization: A narrative review of clinical data from human trials. Tech. Vasc. Interv. Radiol. 2020, 23, 100658. [Google Scholar] [CrossRef]
- Kipshidze, N.; Archvadze, A.; Bertog, S.; Leon, M.B.; Sievert, H. Endovascular bariatrics: First in humans study of gastric artery embolization for weight loss. JACC Cardiovasc. Interv. 2015, 8, 1641–1644. [Google Scholar] [CrossRef] [Green Version]
- Pirlet, C.; Ruzsa, Z.; Costerousse, O.; Nemes, B.; Merkely, B.; Poirier, P.; Bertrand, O.F. Transradial left gastric artery embolization to treat severe obesity: A pilot study. Catheter. Cardiovasc. Interv. 2019, 93, 365–370. [Google Scholar] [CrossRef]
- Syed, M.I.; Morar, K.; Shaikh, A.; Craig, P.; Khan, O.; Patel, S.; Khabiri, H. Gastric artery embolization trial for the lessening of appetite nonsurgically (GET LEAN): Six-month preliminary data. J. Vasc. Interv. Radiol. 2016, 27, 1502–1508. [Google Scholar] [CrossRef]
- Korbonits, M.; Goldstone, A.P.; Gueorguiev, M.; Grossman, A.B. Ghrelin—A hormone with multiple functions. Front. Neuroendocrinol. 2004, 25, 27–68. [Google Scholar] [CrossRef] [PubMed]
- Nakazato, M.; Murakami, N.; Date, Y.; Kojima, M.; Matsuo, H.; Kangawa, K.; Matsukura, S. A role for ghrelin in the central regulation of feeding. Nat. Cell Biol. 2001, 409, 194–198. [Google Scholar] [CrossRef]
- Duca, F.A.; Covasa, M. Current and emerging concepts on the role of periperal signals in the control of food intake and development of obesity. Br. J. Nutr. 2012, 108, 778–793. [Google Scholar] [CrossRef] [Green Version]
- Page, A.J.; Slattery, J.A.; Milte, C.; Laker, R.; O’Donnell, T.; Dorian, C.; Brierley, S.; Blackshaw, A. Ghrelin selectively reduces mechanosensitivity of upper gastrointestinal vagal afferents. Am. J. Physiol. Liver Physiol. 2007, 292, G1376–G1384. [Google Scholar] [CrossRef] [Green Version]
- Gunn, A.J.; Oklu, R. A preliminary observation of weight loss following left gastric artery embolization in humans. J. Obes. 2014, 2014, 185349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.J.; Raman, H.S.; Salter, A.; Ramaswamy, R.; Gunn, A.J.; Weiss, C.R.; Akinwande, O. Analysis of weight changes after left gastric artery embolization in a cancer-naive population. Diagn. Interv. Radiol. 2018, 24, 94–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arepally, A.; Barnett, B.; Montgomery, E.; Patel, T.H. Catheter-directed gastric artery chemical embolization for modulation of systemic ghrelin levels in a porcine model: Initial experience. Radiology 2007, 244, 138–143. [Google Scholar] [CrossRef]
- Arepally, A.; Barnett, B.; Patel, T.T.; Howland, V.; Boston, R.C.; Kraitchman, D.L.; Malayeri, A.A. Catheter-directed gastric artery chemical embolization suppresses systemic ghrelin levels in porcine model. Radiology 2008, 249, 127–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bawudun, D.; Xing, Y.; Liu, W.-Y.; Huang, Y.-J.; Ren, W.-X.; Ma, M.; Xu, X.-D.; Teng, G.-J. Ghrelin suppression and fat loss after left gastric artery em-bolization in canine model. Cardiovasc. Interv. Radiol. 2012, 35, 1460–1466. [Google Scholar] [CrossRef] [PubMed]
- Paxton, B.E.; Kim, C.Y.; Alley, C.L.; Crow, J.H.; Balmadrid, B.; Keith, C.G.; Kankotia, R.J.; Stinnett, S.; Arepally, A. Bariatric embolization for suppression of the hunger hormone ghrelin in a porcine model. Radiology 2013, 266, 471–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paxton, B.E.; Alley, C.L.; Crow, J.H.; Burchette, J.; Weiss, C.R.; Kraitchman, D.L.; Arepally, A.; Kim, C.Y. Histopathologic and immunohistochemical sequelae of bar-iatric embolization in a porcine model. J. Vasc. Interv. Radiol. 2014, 25, 455–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paxton, B.E.; Arepally, A.; Alley, C.L.; Kim, C.Y. Bariatric embolization: Pilot study on the impact of gastroprotective agents and arterial distribution on ulceration risk and efficacy in a porcine model. J. Vasc. Interv. Radiol. 2016, 27, 1923–1928. [Google Scholar] [CrossRef]
- Kim, J.M.; Kim, M.D.; Han, K.; Muqmiroh, L.; Kim, S.U.; Kim, G.M.; Kwon, J.; Pari, S., Jr.; Won, J.Y.; Lee, D.Y. Bariatric arterial embolization with non-spherical polyvinyl alcohol particles for ghrelin suppression in a swine model. Cardiovasc. Interv. Radiol. 2017, 40, 744–749. [Google Scholar] [CrossRef]
- Hafezi-Nejad, N.; Bailey, C.R.; Gunn, A.J.; Weiss, C.R. Weight loss after left gastric artery embolization: A systematic review and meta-analysis. J. Vasc. Interv. Radiol. 2019, 30, 1593–1603.e3. [Google Scholar] [CrossRef]
- Fu, Y.; Kraitchman, D.L. Rationale and preclinical data supporting bariatric arterial embolization. Tech. Vasc. Interv. Radiol. 2020, 23, 100656. [Google Scholar] [CrossRef]
- Weiss, C.R.; Abiola, G.O.; Fischman, A.M.; Cheskin, L.J.; Vairavamurthy, J.; Holly, B.P.; Akinwande, O.; Nwoke, F.; Paudel, K.; Belmustakov, S.; et al. Bariatric embolization of arteries for the treatment of obesity (BEAT Obesity) trial: Results at 1 year. Radiology 2019, 291, 792–800. [Google Scholar] [CrossRef]
- Zaitoun, M.M.; Basha, M.A.A.; Hassan, F.; Elsayed, S.B.; Farag, A.A.; Amer, M.; Aly, S.A.; Zaitoun, N. Left gastric artery embolization in obese, prediabetic patients: A pilot study. J. Vasc. Interv. Radiol. 2019, 30, 790–796. [Google Scholar] [CrossRef] [PubMed]
- Reddy, V.Y.; Neužil, P.; Musikantow, D.; Sramkova, P.; Rosen, R.; Kipshidze, N.; Kipshidze, N.; Fried, M. Transcatheter bariatric embolotherapy for weight reduction in obesity. JACC 2020, 76, 2305–2317. [Google Scholar] [CrossRef] [PubMed]
- Weiss, C.R.; Abiola, G.O.; Fischman, A.M.; Cheskin, L.J.; Vairavamurthy, J.; Holly, B.P.; Akinwande, O.; Nwoke, F.; Paudel, K.; Belmustakov, S.; et al. Bariatric embolization of arteries with imaging visible embolics (BEATLES) (BAE2). Clin. Trials.
- Davies, M.; Færch, L.; Jeppesen, O.K.; Pakseresht, A.; Pedersen, S.D.; Perreault, L.; Rosenstock, J.; Shimomura, I.; Viljoen, A.; Wadden, T.A.; et al. Semaglutide 2·4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): A randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. Lancet 2021, 397, 971–984. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/Year/REF. | Animal Model | N of Animals | Follow-Up | Absolute Weight Change (%) | Absolute Ghrelin Change (%) |
|---|---|---|---|---|---|
| Arepally 2007 [20] | Swine | 5 2 CTRL 4 LDSM 4 HDSM | 4 weeks | 8.6 increase 1.4 increase 1.4 increase | 15% increase 130% increase 60% decrease |
| Arepally 2008 [21] | Swine | 10 5 CTRL 5 SM | 4 weeks | 15.8 increase 7.8 increase | 10.1 increase 12.9 decrease |
| Bawudun 2012 [22] | Dog | 15 5 CTRL 5 EO 5 PVA | 8 weeks | 5 increase 5 decrease 10 decrease | 13.6 increase 15.8 decrease 30.1 decrease |
| Paxton 2013 [23] | Swine | 12 6 CTRL 6 MS | 8 weeks | 28 increase 10 increase | 30 increase 30 decrease |
| Paxton 2014 [24] | Swine | 12 6 CTRL 6 EO | 8 weeks | Not Reported Not Reported | Not Reported Not Reported |
| Paxton 2016 [25] | Swine | 22 6 CTRL 6 EA [8]5 EA [2]5 EA [1] | 4–8 weeks | 26.5 increase 8.7 increase 19.7 increase 23.0 increase | 19.9 increase 29.9 decrease 18.2 increase 234 increase |
| Kim 2017 [26] | Swine | 10 5 CTRL 5 PVA | 2 mos | 30% increase 27% increase | No change 40% decrease |
| Author/Year/REF | Study Design | N of pts | Follow-UpLength | Total Weight Loss (%) | Embolic Material |
|---|---|---|---|---|---|
| Kipshidze 2015 [11] | Prospective | 5 | 2 years | 22 kg (17.1%) | 300–500 μm BeadBlock embospheres |
| GET-LEAN 2016 [13] | Prospective | 4 | 6 months | 9.2 kg (8.5%) | 300–500 μm BeadBlock embospheres |
| Bai 2018 [8] | Prospective | 5 | 9 months | 12.9 kg (12.6%) | 500–710 μm PVA particles |
| Pirlet 2019 [12] | Prospective | 7 | 12 months | 13 kg (4.7%) | 300–500 μm PVA particles |
| Elens 2019 [9] | Prospective | 16 | 12 months | 8 kg (10%) | 500–700 μm Merit Medical embospheres |
| BEAT 2019 [29] | Prospective | 20 | 12 months | 7.6 kg (11.5%) | 300–500 μm Merit Medical embospheres |
| Zaitun 2019 [30] | Prospective (pre-diabetic) | 10 | 6 months | 9 kg (8.9%) | 300–500 μm Merit Medical embospheres |
| LOSEIT 2020 [31] | Randomized, sham-controlled | 40 | 12 months | 9.3 Kg (9.3%) | 300–500 μm BeadBlock microspheres |
| BEATLES 2023 [32]On-going Trial | Randomized, sham-controlled | 56 | 12 months | On-going trial | 100–200 µm radiopaque microspheres |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sangiorgi, G.M.; Cereda, A.; Porchetta, N.; Benedetto, D.; Matteucci, A.; Bonanni, M.; Chiricolo, G.; De Lorenzo, A. Endovascular Bariatric Surgery as Novel Minimally Invasive Technique for Weight Management in the Morbidly Obese: Review of the Literature. Nutrients 2021, 13, 2541. https://doi.org/10.3390/nu13082541
Sangiorgi GM, Cereda A, Porchetta N, Benedetto D, Matteucci A, Bonanni M, Chiricolo G, De Lorenzo A. Endovascular Bariatric Surgery as Novel Minimally Invasive Technique for Weight Management in the Morbidly Obese: Review of the Literature. Nutrients. 2021; 13(8):2541. https://doi.org/10.3390/nu13082541
Chicago/Turabian StyleSangiorgi, Giuseppe Massimo, Alberto Cereda, Nicola Porchetta, Daniela Benedetto, Andrea Matteucci, Michela Bonanni, Gaetano Chiricolo, and Antonino De Lorenzo. 2021. "Endovascular Bariatric Surgery as Novel Minimally Invasive Technique for Weight Management in the Morbidly Obese: Review of the Literature" Nutrients 13, no. 8: 2541. https://doi.org/10.3390/nu13082541