
Effect of Glutamine Supplementation on Muscular Damage Biomarkers in Professional Basketball Players

 ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Managing of Blood Samples
2.4. Determination of Muscle Damage Markers
2.5. Statistical Analysis
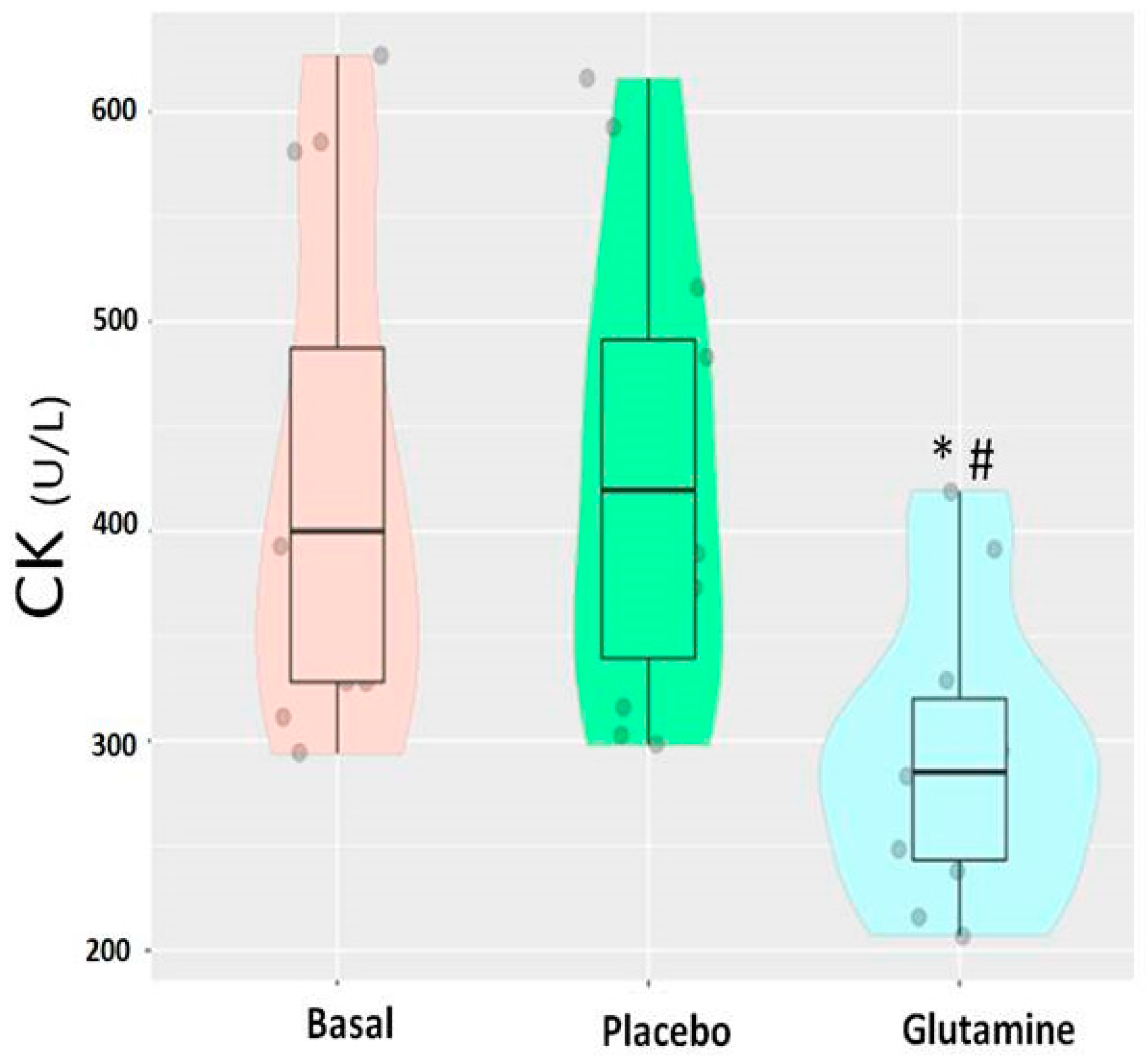
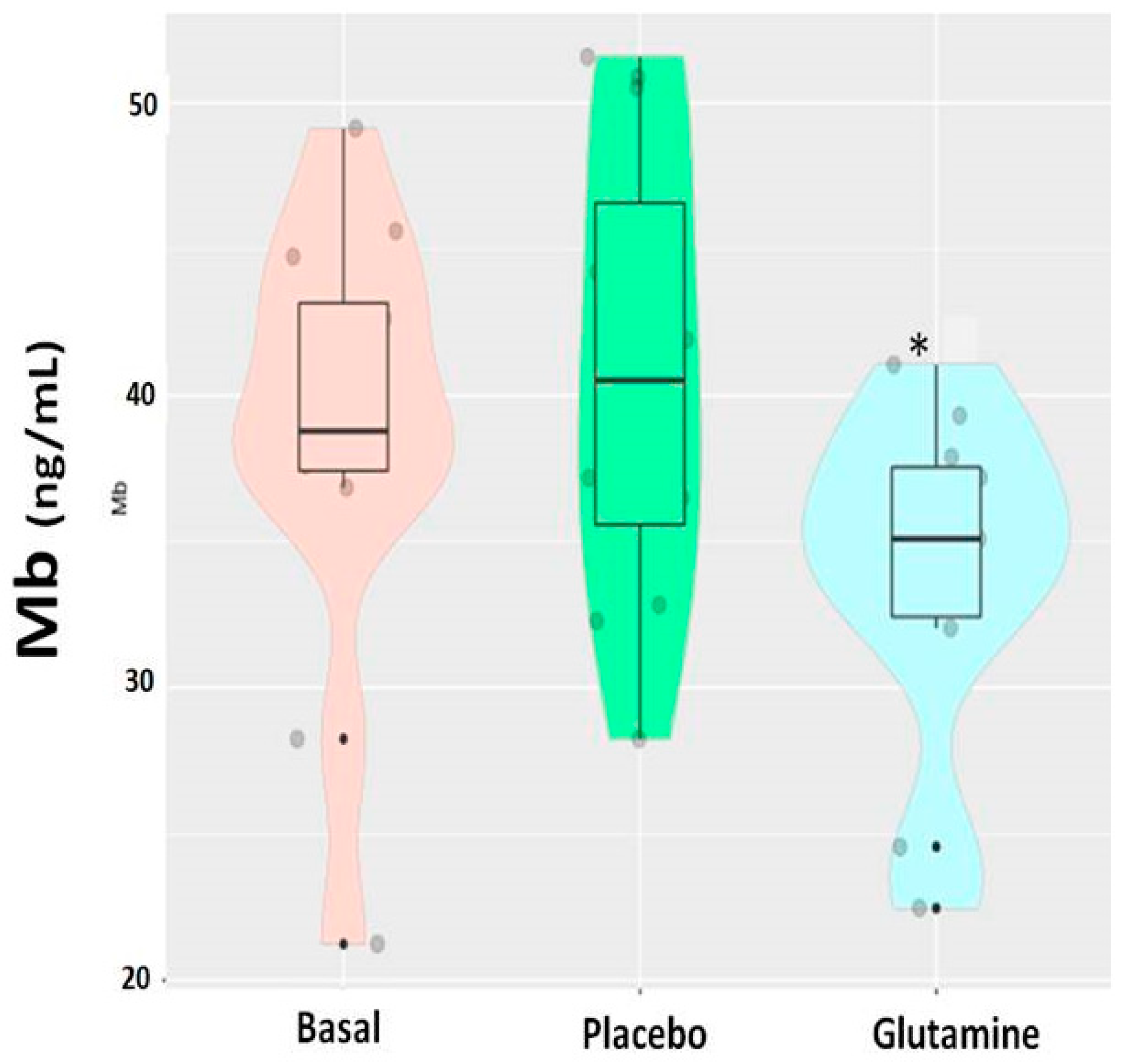
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Proske, U.; Morgan, D.L. Muscle damage from eccentric exercise: Mechanism, mechanical signs, adaptation and clinical applications. J. Physiol. 2001, 537, 333–345. [Google Scholar] [CrossRef]
- Howatson, G.; van Someren, K.A. The prevention and treatment of exercise-induced muscle damage. Sports Med. 2008, 38, 483–503. [Google Scholar] [CrossRef] [PubMed]
- Felig, P. Amino acid metabolism in man. Ann. Rev. Biochem. 1975, 44, 933–955. [Google Scholar] [CrossRef] [PubMed]
- Watford, M. Glutamine metabolism and function in relation to proline synthesis and the safety of glutamine and proline supplementation. J. Nutr. 2008, 138, 2003–2007. [Google Scholar] [CrossRef]
- Castell, L.M. Can glutamine modify the apparent immunodepression observed after prolonged, exhaustive exercise? Nutrition 2002, 18, 371–375. [Google Scholar] [CrossRef]
- Nieman, D.C. Exercise immunology: Nutritional countermeasures. Can. J. Appl. Physiol. 2001, 26, S45–S55. [Google Scholar] [CrossRef]
- Parry-Billings, M.; Budgett, R.; Koutedakis, Y.; Blomstrand, E.; Brooks, S.; Williams, C.; Calder, P.C.; Pilling, S.; Baigri, R.; Newsholme, E.A. Plasma amino acid concentrations in the overtraining syndrome: Possible effects on the immune system. Med. Sci. Sports Exerc. 1992, 24, 1353–1358. [Google Scholar] [CrossRef]
- Castell, L.M. Glutamine supplementation in vitro and in vivo, in exercise and in immunodepresion. Sports Med. 2003, 33, 323–345. [Google Scholar] [CrossRef]
- Kuhn, K.S.; Muscaritoli, M.; Wischmeyer, P.; Stehle, P. Glutamine as indispensable nutrient in oncology: Experimental and clinical evidence. Eur. J. Nutr. 2010, 49, 197–210. [Google Scholar] [CrossRef]
- Rahmani, F.N.; Farzaneh, E.; Damirchi, A.; Shamsi, M.A. Effect of L-glutamine supplementation on electromyographic activity of the quadriceps muscle injured by eccentric exercise. Iran. J. Basic Med. Sci. 2013, 16, 808–812. [Google Scholar]
- Street, B.; Byrne, C.; Eston, R. Glutamine supplementation in recovery from eccentric exercise attenuates strength loss and muscle soreness. J. Exerc. Sci. Fit. 2011, 9, 116–122. [Google Scholar] [CrossRef][Green Version]
- Castell, L.M.; Newsholme, E.A. The effects of oral glutamine supplementation on athletes after prolonged, exhaustive exercise. Nutrition 1997, 13, 738–742. [Google Scholar] [CrossRef]
- Gleeson, M.; Walsh, N.P.; Blannin, A.K.; Robson, P.J.; Cook, L.; Donnelly, A.E.; Day, S.H. The effect of severe eccentric exercise-induced muscle damage on plasma elastase, glutamine and zinc concentrations. Eur. J. Appl. Physiol. Occup. Physiol. 1988, 77, 543–546. [Google Scholar] [CrossRef]
- Nosaka, K.; Sacco, P.; Mawatari, K. Effects of amino acid supplementation on muscle soreness and damage. Int. J. Sport Nutr. Exerc. Metab. 2006, 16, 620–635. [Google Scholar] [CrossRef] [PubMed]
- MacLennan, P.A.; Brown, R.A.; Rennie, M.J. A positive relationship between protein synthetic rate and intracellular glutamine concentration in perfused rat skeletal muscle. FEBS Lett. 1987, 215, 187–191. [Google Scholar] [CrossRef]
- Wu, G.Y.; Thompson, J.R. The effect of glutamine on protein turnover in chick skeletal muscle in vitro. Biochem. J. 1990, 265, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Legault, Z.; Bagnall, N.; Kimmerly, D.S. The influence of oral L-glutamine supplementation on muscle strength recovery and soreness following unilateral knee extension eccentric exercise. Int. J. Sport Nutr. Exerc. Metab. 2015, 25, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Stojanovic, E.; Stojiljkovic, N.; Scanlan, A.T.; Dalbo, V.J.; Berkelmans, D.M.; Milanovic, Z. The activity demands and physiological responses encountered during basketball match-play: A systematic review. Sports Med. 2018, 48, 111–135. [Google Scholar] [CrossRef]
- Ziv, G.; Lidor, R. Vertical jump in female and male basketball players—A review of observational and experimental studies. J. Sci Med. Sport 2010, 13, 332–339. [Google Scholar] [CrossRef]
- Koo, G.H.; Woo, J.; Shin, K.O.; Kang, S. Effects of supplementation with BCAA and L-glutamine on blood fatigue factors and cytokines in juvenile athletes submitted to maximal intensity rowing performance. J. Phys. Ther. Sci. 2014, 26, 1241–1246. [Google Scholar] [CrossRef][Green Version]
- Ramezani-Ahmadi, A.; Rayyani, E.; Bahreini, M.; Mansoori, A. The effect of glutamine supplementation on athletic performance, body composition, and immune function: A systematic review and a meta-analysis of clinical trials. Clin. Nutr. 2019, 38, 1076–1091. [Google Scholar] [CrossRef]
- Amirato, G.R.; Borges, J.O.; Marques, D.L.; Santos, J.M.B.; Santos, C.A.F.; Andrade, M.S.; Furtado, G.E.; Rossi, M.; Luis, L.N.; Zambonatto, R.F.; et al. L-Glutamine supplementation enhances strength and power of knee muscles and improves glycemia control and plasma redox balance in exercising elderly women. Nutrients 2021, 13, 1025. [Google Scholar] [CrossRef] [PubMed]
- Spiteri, T.; Newton, R.U.; Binetti, M.; Hart, N.H.; Sheppard, J.M.; Nimphius, S. Mechanical determinants of faster change of direction and agility performance in female basketball athletes. J. Strength Cond. Res. 2015, 29, 2205–2214. [Google Scholar] [CrossRef] [PubMed]
- Spiteri, T.; Binetti, M.; Scanlan, A.T.; Dalbo, V.J.; Dolci, F.; Specos, C. Physical determinants of division 1 collegiate basketball, women’s national basketball league and women’s national basketball association athletes: With reference to lower body sidedness. J. Strength Cond. Res. 2019, 33, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Souglis, A.; Bogdanis, G.; Giannopoulou, I.; Papadopoulos, C.; Apostolidis, N. Comparison of inflammatory responses and muscle damage indices following a soccer, basketball, volleyball and handball game at an elite competitive level. Res. Sports Med. 2015, 23, 59–72. [Google Scholar] [CrossRef]
- Gleeson, M. Dosing and efficacy of glutamine supplementation in human exercise and sport training. J. Nutr. 2008, 138, 2045S–2049S. [Google Scholar] [CrossRef] [PubMed]
- Parry-Billings, M.; Evans, J.; Calder, P.C.; Newsholme, E.A. Does glutamine contribute to immunosuppression? Lancet 1990, 336, 523–525. [Google Scholar] [CrossRef]
- Rennie, M.J.; Edwards, R.H.; Krywawych, S.; Davies, C.T.; Halliday, D.; Waterlow, J.C.; Millward, D.J. Effect of exercise on protein turnover in man. Clin. Sci. 1981, 61, 627–639. [Google Scholar] [CrossRef]
- Coqueiro, A.Y.; Rogero, M.M.; Tirapegui, J. Glutamine as an anti-fatigue amino acid in sports nutrition. Nutrients 2019, 11, 863. [Google Scholar] [CrossRef]
- Newsholme, E.A.; Newsholme, P.; Curi, R. The role of the citric acid cycle in cells the immune system and its importance in sepsis, trauma and burns. Biochem. Soc. Symp. 1987, 54, 145–162. [Google Scholar]
- Parry-Billings, M.; Baigrie, R.; Lamont, P.; Morris, P.; Newsholme, E.A. Effects of major and minor surgery on plasma glutamine and cytokine levels. Arch. Surg. 1992, 127, 1237–1240. [Google Scholar] [CrossRef]
- Powell, H.; Castell, L.M.; Parry-Billings, M.; Desborough, J.P.; Hall, G.M.; Newsholme, E.A. Growth hormone suppression and glutamine flux associated with cardiac surgery. Clin. Physiol. 1994, 14, 569–580. [Google Scholar] [CrossRef]
- Paulsen, G.; Crameri, R.; Benestad, H.B.; Fjeld, J.G.; Morkrid, L.; Hallen, J.; Raastad, T. Time course of leukocyte accumulation in human muscle after eccentric exercise. Med. Sci. Sports Exerc. 2010, 42, 75–85. [Google Scholar] [CrossRef]
- Carrasco, G.A.; Van de Kar, L.D. Neuroendocrine pharmacology of stress. Eur. J. Pharmacol. 2003, 463, 235–272. [Google Scholar] [CrossRef]
- Córdova-Martinez, A.; Seco-Calvo, J.; Tur-Mari, J.A.; Abecia-Inchaurregui, L.C.; Echeverría-Orella, E.; Pons-Biescas, A. Testosterone and cortisol changes in professional basketball players through a season competition. J. Strength Cond. Res. 2010, 24, 1102–1108. [Google Scholar] [CrossRef] [PubMed]
- Engelmann, M.; Landgraf, R.; Wotjak, C.T. The hypothalamic-neurohypophysial system regulates the hypothalamic-pituitary-adrenal axis under stress: An old concept revisited. Front. Neuroendocrinol. 2004, 25, 132–149. [Google Scholar] [CrossRef]
- Peake, J.; Nosaka, K.; Suzuki, K. Characterization of inflammatory responses to eccentric exercise in humans. Exerc. Immunol. Rev. 2005, 11, 64–85. [Google Scholar] [PubMed]
- Kellmann, M. Preventing overtraining in athletes in high-intensity sports and stress/recovery monitoring. Scand. J. Med. Sci. Sports 2010, 20 (Suppl. S2), 95–102. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | B | G | P |
|---|---|---|---|
| LDH (U/L) | 374.2 ± 29.81 | 384.4 ± 47.70 | 396.8 ± 36.90 |
| AST (U/L) | 33.38 ± 4.43 | 30.13 ± 5.08 * | 33.08 ± 4.4 |
| ALT (U/L) | 24.8 ± 3.41 | 23.9 ± 2.72 | 25.42 ± 3.62 |
| Urea (mg/dL) | 43.8 ± 6.04 | 42.9 ± 5.98 | 42.58 ± 5.40 |
| Creatinine (mg/dL) | 1.25 ± 0.05 | 1.23 ± 0.04 | 1.29 ± 0.07 |
| TP (g/L) | 6.98 ± 0.56 | 7.08 ± 0.45 | 6.97 ± 0.49 |
| Parameter | B | G | P |
|---|---|---|---|
| Erythrocytes (106/uL) | 4.88 ± 4.32 | 4.86 ± 3.98 | 4.95 ± 4.51 |
| Hematocrit (%) | 44.56 ± 1.3 | 44.52 ± 1.9 | 44.75 ± 2.2 |
| Hemoglobin (g/dL) | 14.63 ± 0.56 | 14.54 ± 0.78 | 14.32 ± 0.62 |
| WBC (103/uL) | 6.13 ± 1.15 | 5.81 ± 0.98 | 6.73 ± 1.11 |
| Neutrophils (%) | 47.98 ± 7.2 | 59.31 ± 8.1 | 44.18 ± 4.5 |
| Neutrophils (103/uL) | 2.94 ± 0.25 | 3.02 ± 0.19 * | 3.64 ± 0.19 |
| Lymphocytes (%) | 46.76 ± 6.8 | 37.42 ± 5.1 *,# | 53.75 ± 5.7 |
| Lymphocytes(103/uL) | 2.87 ± 0.18 | 2.17 ± 0.15 | 2.94 ± 0.20 |
| Hormone | B | G | P |
|---|---|---|---|
| Cortisol (ug/dL) | 17.67 ± 2.5 | 17.21 ± 3.2 | 18.93 ± 3.4 |
| Testosterone (ng/dL) | 5.87 ± 1.11 | 5.98 ± 1.04 | 6.07 ± 0.98 |
| ACTH (pg/mL) | 78.7 ± 22.49 | 53.7 ± 22.90 *,# | 76.5 ± 23.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Córdova-Martínez, A.; Caballero-García, A.; Bello, H.J.; Pérez-Valdecantos, D.; Roche, E. Effect of Glutamine Supplementation on Muscular Damage Biomarkers in Professional Basketball Players. Nutrients 2021, 13, 2073. https://doi.org/10.3390/nu13062073
Córdova-Martínez A, Caballero-García A, Bello HJ, Pérez-Valdecantos D, Roche E. Effect of Glutamine Supplementation on Muscular Damage Biomarkers in Professional Basketball Players. Nutrients. 2021; 13(6):2073. https://doi.org/10.3390/nu13062073
Chicago/Turabian StyleCórdova-Martínez, Alfredo, Alberto Caballero-García, Hugo J Bello, Daniel Pérez-Valdecantos, and Enrique Roche. 2021. "Effect of Glutamine Supplementation on Muscular Damage Biomarkers in Professional Basketball Players" Nutrients 13, no. 6: 2073. https://doi.org/10.3390/nu13062073
APA StyleCórdova-Martínez, A., Caballero-García, A., Bello, H. J., Pérez-Valdecantos, D., & Roche, E. (2021). Effect of Glutamine Supplementation on Muscular Damage Biomarkers in Professional Basketball Players. Nutrients, 13(6), 2073. https://doi.org/10.3390/nu13062073